2015 AHLA Physicians and Hospitals Institute February 2 – 4, 2015 Carol W. Carden, CPA/ABV, ASA, CFE Mark Easterly, JD Exclusive Contracting and Incentivizing Quality in Your Hospitalist Program

Exclusive Contracting and Incentivizing Quality in Your Hospitalist Program
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Page 0
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Carol W. Carden, CPA/ABV, ASA, CFE
Mark Easterly, JD
Exclusive Contracting and
Incentivizing Quality in Your
Hospitalist Program
Page 1
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Objectives
• Understand the role of hospitalists and review the
growth of hospital medicine as a hospital-based
service
• Learn how to use hospitalist incentives to improve
quality, safety, and patient satisfaction
• Review case study
• Understand compensation and valuation
methodologies for hospitalist contracts

Page 2
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Page 3
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Hospitalists in Modern Health Care Delivery
• Hospital medicine has been the “Quiet
Revolution” in health care delivery
• AHA survey found that 83% of hospitals with
>200 beds have hospitalist programs.
Page 4
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Definition of a Hospitalist
• Term defined in 1996 NEJM article by Wachter/Goldman
from UCSF
• Hospitalists are hospital-based physicians that manage
medical inpatients
• An alternative to inpatient management by an office-
based PCP
Page 5
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Definition of a Hospitalist
The Society of Hospital Medicine
www.hospitalmedicine.org
Hospitalists are physicians whose primary
professional focus is the general medical care of
hospitalized patients. Their activities include
patient care, teaching, research, and leadership
related to Hospital Medicine.
Page 6
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Driving Forces Behind Growth of Hospital
Medicine Movement
• Changing approaches to delivery of care
– Managed care driven
• Need for efficient and cost-effective outpatient and
inpatient care
• Need for quality improvement
• Evolution of the internist away from hospital-based
practice
• Physician lifestyle expectations and demands

Page 7
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Hospitals Benefit from Hospitalists
• Physician champions for patient safety
and quality improvements
• Standardization of care
• Patient throughput and length of stay
management
• Decrease ED wait times
• Recruitment of medical staff
• Nursing satisfaction and retention
Page 8
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
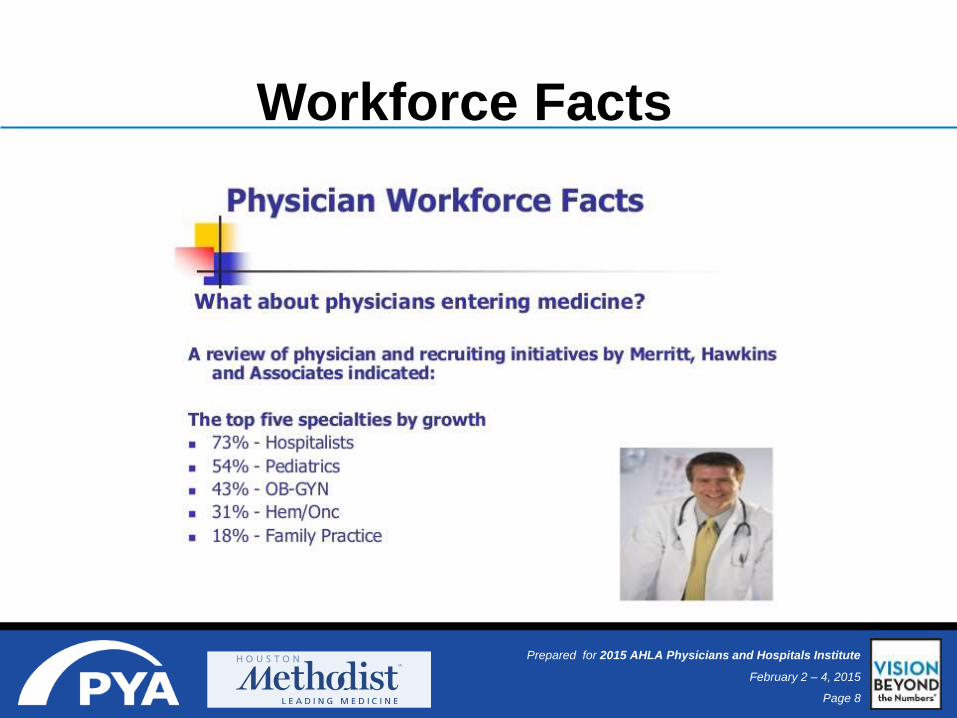
Workforce Facts

Page 9
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
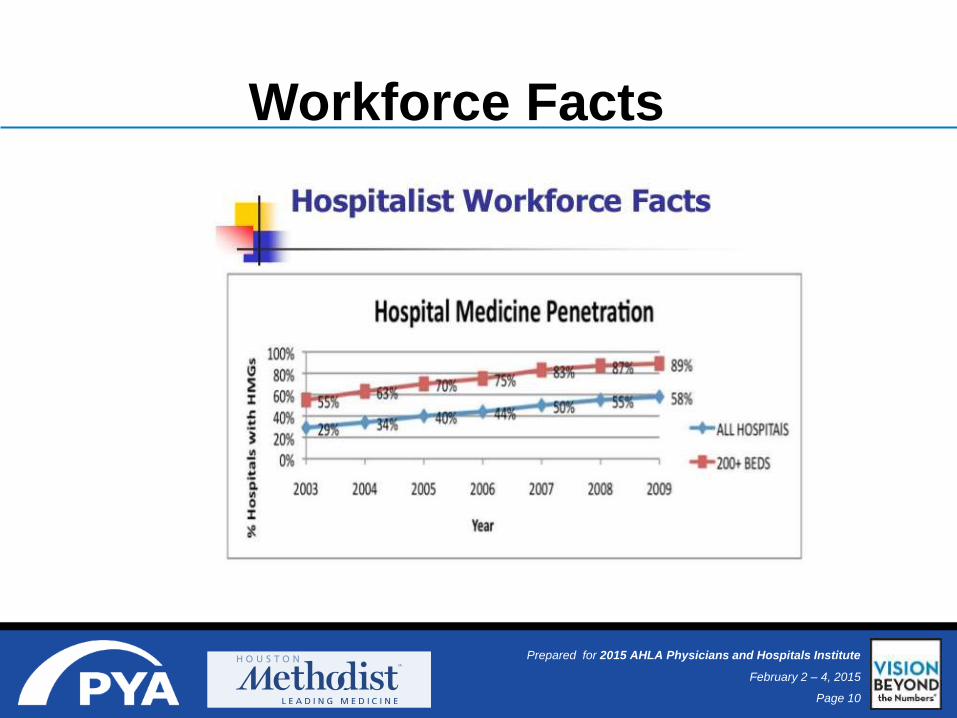
Workforce Facts
Page 10
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
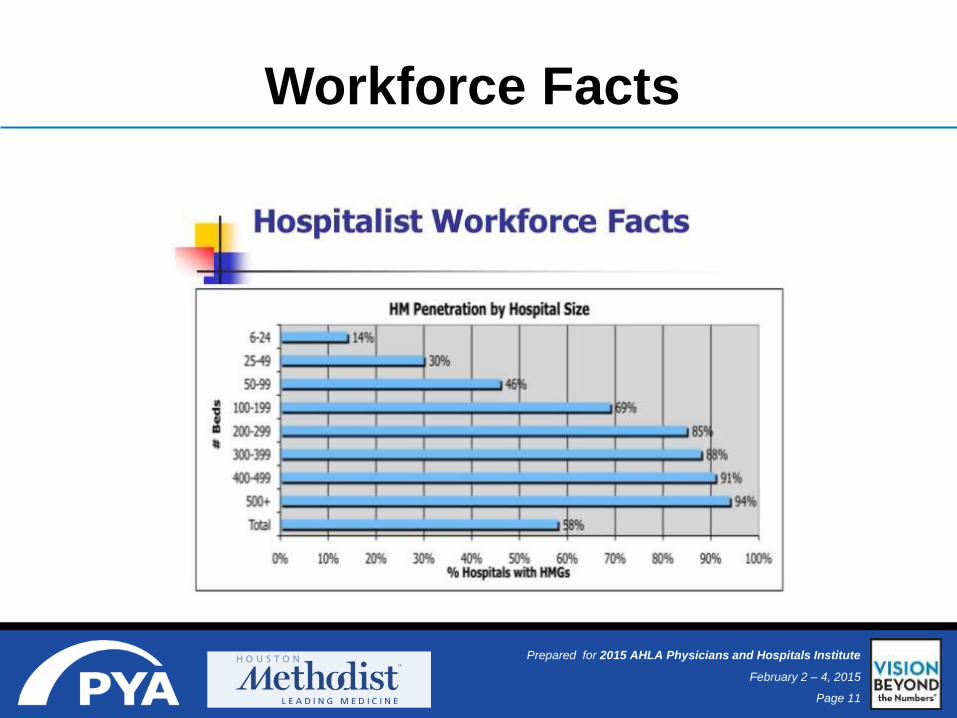
Workforce Facts
Page 11
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Workforce Facts

Page 12
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Workforce Facts
Page 13
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
National Providers
Page 14
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
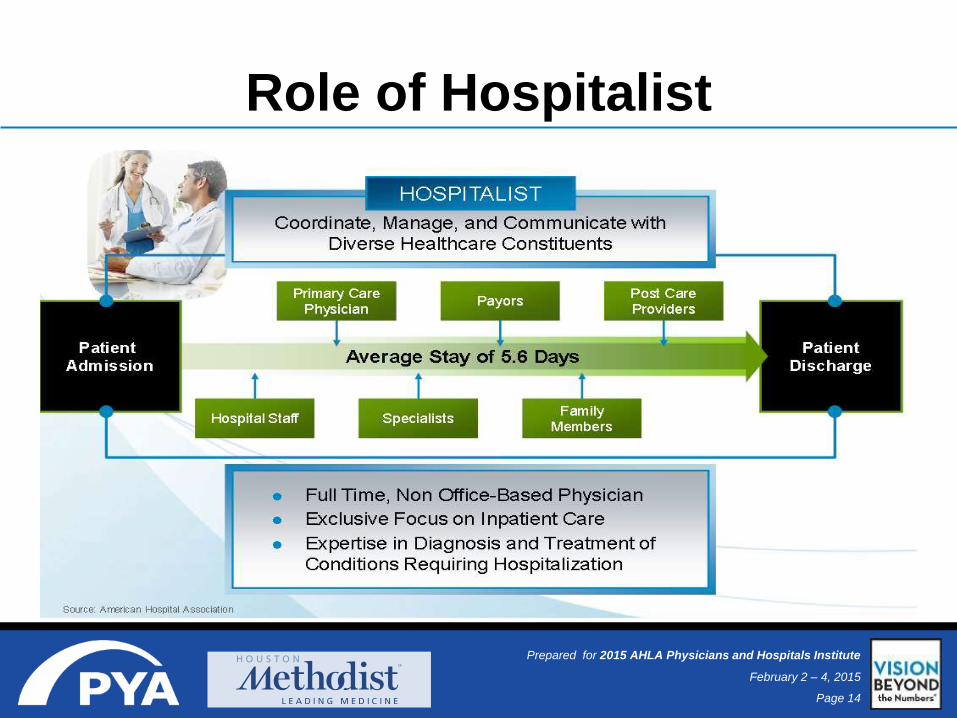
Role of Hospitalist

Page 15
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Medical Group-Based Programs
• Almost 90% of major multi-specialty medical groups have programs
• Many programs support multiple hospitals
• Cost savings are a strong motivation for using hospitalists
• Often at financial risk (e.g., capitation) for inpatient services
• Programs good at integrating care across multiple settings
• PCPs and hospitalists are partners in the medical group
• PCP can explain hospitalist role to the patient before admission
• The hospitalist can easily and frequently communicate with the PCP and
other MDs in the group (e.g, using an EMR)
• Smooth patient transfers to ECFs and rehab facilities because groups
often have contractual relationships with these providers
Page 16
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Academic Hospital-Based Programs
• Leading the hospitalist movement academic medicine
• Teaching is an important priority for these programs
• These hospitals often care for very sick patients
• Hospitalists’ role often requires significant coordination with a
range of sophisticated specialists
• Because of house staff/specialization:
• Hospitalists rarely perform procedures
• Hospitalists less likely to see patients in ICU, CCU, or ED
Page 17
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Community Hospital-Based Programs
• Represent the growth market for new hospitalist programs
• Virtually all hospitals with active plans to implement hospitalist
programs in the next 2 years are in this category
• Hospitalists have multi-dimensional responsibilities
• Admit some patients, admit and round on other patients, perform
consultations, do medical procedures, and see patients in the ICU,
CCU, and ED
• More likely to provide 24 hour, round-the-clock coverage
and to employ administrative and/or clinical support staff
Page 18
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Hospitalist Program Models
• Completely Open Medical Staff
– Any physician can apply for privileges as
hospitalist
• Partially Closed Staff
– Multiple providers but closed to new applicants
• Exclusive Staffing
– Private provider via PSA
– Employed providers via direct employment

Page 19
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Why Hospitalists for your Quality Improvement
Program?
• Physically present and
available
• Vested in hospital’s
success
• Volume/influence
• Contracted
– Employed or private
– Opportunity to exert
greater control

Page 20
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Steps
• Identify opportunity for your hospitalist program
• Determine: closed vs. open staff model
• Issue RFP
• Award contract(s)
• Work with physicians on developing quality metrics
• Value financial incentive
• Execute
• Measure and reward achievement

Page 21
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Legal Issues
• Stark
• Anti-kickback
• Civil Monetary Penalty Statue
• Tax exemption
• Anti-trust
Page 22
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Stark Law 42 U.S.C. §1395nn
• Personal services
exception
• Fair market value
exception
• Bona fide
employment

Page 23
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Stark Law 42 U.S.C. §1395nn
• Incentive Payment and Shared Savings Program
Exception (42 CFR §411.357(x))
• CMS proposed July 7, 2008
• “hospitals may sponsor quality-focused programs in
which objective improvements in quality or
individual patient care outcomes are rewarded with
payments to physicians responsible for the
improvements.”
• Not yet adopted as final rule

Page 24
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Stark Law 42 U.S.C. §1395nn
• Incentive Payment and Shared Savings Program
Exception (42 CFR §411.357(x))
– “In many cases, incentive payment and shared savings
programs can be structured to satisfy the requirements of
existing exceptions (e.g., bona fide employment, personal
services arrangements, fair market value compensation,
or indirect compensation).”
– “However, in other circumstances, the existing exceptions
to [Stark] may not be sufficiently flexible to protect
payments to physicians under incentive payment
programs.” 73 Fed. Reg. 38551

Page 25
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Request for Proposal
• Written RFP
• Clearly describe services, roles, and
objectives
• Set timetable for response
• Outline significant contract terms
• Include medical director or program leader
role?
• Local groups or include national providers?
Page 26
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Closing the Hospitalist Service
• Check applicable state law
• Check hospital and medical staff bylaws
• Check current contractual relationships
• How to define “hospitalists”
– Self declaration or delineation of privileges
– Ex. Hospitalists def. as Internal Medicine but no clinical
practice
• Action by hospital board of directors

Page 27
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Preparing the Exclusive Agreement
• Clearly define services, expectations and standards
• Exclusivity language: “Group shall be the exclusive provider of Hospitalist
Services at the Hospital”
• “Clean Sweep” provision: “Physician agrees that his or her Medical Staff
membership and privileges at the Hospital shall terminate at such time that (i) Physician is
no longer retained by Exclusive Group; (ii) the Hospital withdraws its approval of the
Physician as an approved provider; or (iii) the Exclusive Agreement is terminated.
Physician further agrees that, notwithstanding any rights to notice, hearing, and review that
may be established by Hospital Policies, Medical Staff bylaws, or by state law, the Hospital
has no duty to provide notice or hearing in the event the Medical Staff membership and
privileges of Physician are so terminated. Physician shall be deemed to have automatically
resigned Medical Staff membership and privileges at the Hospital under such
circumstances, and hereby waives any notice or hearing.”
• Include quality metrics and compensation set in advance
Page 28
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Quality Metrics
• Decide what to measure
• Set targets
• Generate and analyze reports
• Distill key indicators into dashboard
• Develop action plan for improvement and
achievement of metrics

Page 29
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Quality Metrics
• CMS Core Measures
• Mortality Index
• 30-day readmission rates
• Discharge before 11:00
a.m.
• Physician documentation
response time
• Patient satisfaction
(HCAHPS, Press Ganey)
Page 30
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Goals Effective Impact
Standardization for comparison across hospitals
National benchmark
Hospital accountability and incentive to improve quality
Demonstrate performance
Enhanced public accountability
Transparency and reporting
Quality Metrics
Page 31
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Quality Metrics

Page 32
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Point
Allocation
Benchmark
and Baseline Target
2014 Results
First
Quarter
Second
Quarter
Third
Quarter
Fourth
Quarter
Final
Results
1 - CORE MEASURES: Process of Care Weighted Value 40%
Heart Failure (HF)
Pneumonia
2 - CUSTOMER EXPERIENCE Weighted
Value 40%
Patient Satisfaction (Based on Press Ganey Scores)
Time Physician Spent with you 33%
Physician kept you informed 34%
Friendliness/courtesy of physician 33%
4 - MORTALITYWeighted
Value 20%
Sample
Quality Metrics
Page 33
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Other Possible Metrics• Medication reconciliation
• Physician throughput
• Provider satisfaction
– Primary care physician
– Specialist
• EHR adoption and Meaningful Use compliance
• ICD 10 compliance
• “Good Citizenship”
• Is it measurable? Is it legal?
Page 34
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Length of Stay (LOS)
• All hospitals measure.
• Direct bottom line impact
• Hospitalists in position to best influence LOS
• Caution against using LOS as an incentivized quality metric
• Civil Monetary Penalty statute implications 42 U.S.C. § 1320a-7a(b)
– Prohibits knowingly paying a physician an inducement to reduce or
limit the services provided to a federal health program beneficiary
– Potential $2,000 penalty on both hospital and physician
Page 35
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
CMP Rule • 1999 OIG Special Advisory Bulletin re: Gainsharing
– “OIG recognizes that hospitals have a legitimate interest in enlisting
physicians in the efforts to eliminate unnecessary costs. Savings that
do not affect the quality of care may be generated in many ways . . .
[including] reducing lengths of stay.” “Nonetheless, the plain
language of [CMP rule] prohibits tying physicians’ compensation to
reductions or limitation in items or services.”
• 2012 GAO Report to Congress: “Implementation of Financial Incentive
Programs Under Federal Fraud and Abuse Laws”
– “Financial inventive programs . . [and] payments from a hospital to a
physician designed to reward quality that lead to a reduction or
limitation or services furnished to hospital patients . . . Implicate the
CMP law.”
Page 36
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
CMP Rule
• OIG issues proposed rules October 3, 2014 (79 Fed. Reg. 59717)
– “The statute does not limit this prohibition to reductions or limitation of
medically necessary services.”
– “Given the changes in the practice of medicine over the years,
including collaborative efforts among providers and practitioners, and
the rise of widely-accepted clinical metrics, we are considering a
narrower interpretation of the term ‘reduce of limit services’ than we
have previously held.”
– Solicited comments on definition of “reduce or limit services” and
safeguards “to ensure the goal of the statute is met: to prevent
hospitals from paying physicians to discharge patients too soon.”

Page 37
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Case Study
Page 38
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Case Study
• 872 staffed beds
• Major academic medical center
• Internal medicine residency program
• Open staff model
– 5 employed hospitalists;
– 40+ private;
– 4 major groups; one affiliated with major multispecialty group
• 40% of all discharges from hospitalists
Page 39
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Case Study
Hospital Concerns:
• Physician handoff
• Use of consultants
• Quality improvement
• Unassigned ED admission
• Lack of control
• Maintaining existing provider relationships

Page 40
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Leadership
• Engaged Physicians
– Stakeholders formed Hospitalist Governance Council
– Individual Group Leaders
• Department of Medicine Chair
• Hospital Chief Quality Officer
• Hospital Administration
• Medical Executive Committee
• Board of Trustees

Page 41
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Case Study
• Hospitalist Governance Committee set performance
standards
• Hospital issues RFP
• HGC determines quality metrics
• Create dashboard
• External valuation for subsidy and financial incentive
• Board of Directors action to close service
• Execute contracts, measure performance
Page 42
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Performance Standards for Hospitalists
• Provide 24/365 in-house coverage (physicians/mid-level providers) for all patients
• Must personally see and examine patients within six hours of admission/observation
• Orders on chart within one hour of arrival on the floor
• Should alert HMH staff physicians on Day 1 that their patient has been admitted
• Brief discharge summaries on the day of discharge for next level of care
• Participate daily in care coordination rounds
• 100% core measures compliance
• Low Hospital Acquired Conditions (HAC) rate
• Define an acceptable overall Hospitalist Quality Index
• Consultants cannot bring on other consultants without approval of Attending
• No hospitalists can be responsible for the care of more than 25 patients/day
• No hospitalists can admit/observe more than 15 new patients in a 24-hour period

Page 43
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Performance Measure Dashboard
Page 44
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Case Study: Results
• Closed staff
• Several “co-exclusive” contracted hospitalist groups
– Mix of employed and private
• Unassigned ED coverage
• Quality measures with financial incentives
• Quarterly data reports and payment
• Functioning Hospitalist Governance Council

Page 45
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
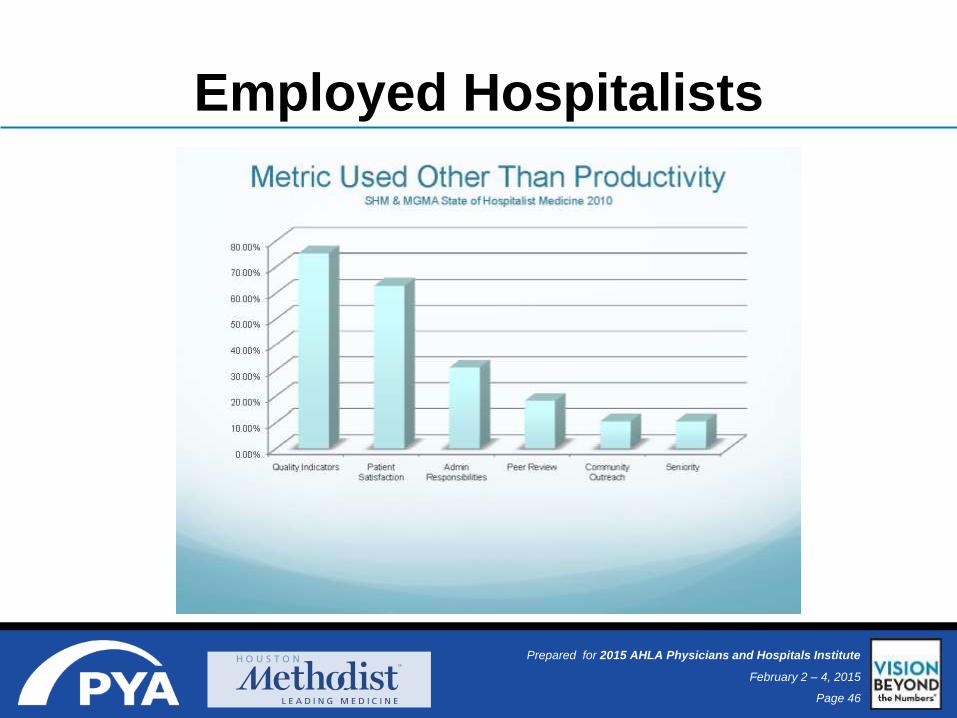
Employed Hospitalists
Page 46
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Employed Hospitalists

Page 47
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Economics of a Hospitalist Program
Predominant
mode of
payment is
shift based
Performance
incentives are
common
87% - 93% of
hospitalists
programs
require a
subsidy
• Average
subsidy is
$156,063
for adult
programs
• Average
subsidy is
$105,985
for pediatric
programs
Exclusive
arrangements
are common
Specialty
hospitalists
becoming
more common
• Critical
care/
intensivist
and
surgicalist

Page 48
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Fair Market Value Considerations
Key Concepts
Determined from the perspective of hypothetical buyers and
sellers without the ability to refer business to one another.
Reasonable knowledge of the relevant facts by both parties
Neither party is under compulsion to buy or sell services
Separate definitions for IRS and Stark/OIG purposes

Page 49
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Fair Market Value• IRS Definition1
– Fair market value (FMV) is defined as the price at which the property or service would change hands between a willing buyer and a willing seller, neither being under a compulsion to buy or sell and both having reasonable knowledge of the relevant facts”
• OIG/Stark Definitions2
– Fair Market Value: the value in arm’s-length transactions, consistent with the general market value
– General Market Value: the price that an asset would bring as the result of bona fide bargaining between well-informed buyers and sellers who are not otherwise in a position to generate business for the other party, or the compensation that would be included in a service agreement as the result of bona fide bargaining between well-informed parties to the agreement who are not otherwise in a position to generate business for the other party, on the date of acquisition of the asset or at the time of the service agreement. Usually, the fair market price is the price at which bona fide sales have been consummated for assets of like type, quality, and quantity in a particular market at the time of acquisition, or the compensation that has been included in bona fide service agreements with comparable terms at the time of the agreement, where the price or compensation has not been determined in any manner that takes into account the volume or value of anticipated or actual referrals
1 Treas. Reg. § 20.2031-1(b) (2005); Rev. Rul. 59-60, 1959-1 C.B.237. 2 42 C.F.R. § 411.351 (2011).

Page 50
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
COMMERCIAL REASONABLENESS
FAIR MARKET VALUE
Compliance Issues Regarding Hospital-
Physician Financial Relationships
Overall Arrangement
“WHY?”
SENSE CENTS
Range of Dollars Only
“HOW MUCH?”
Scope
Key Question
Page 51
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
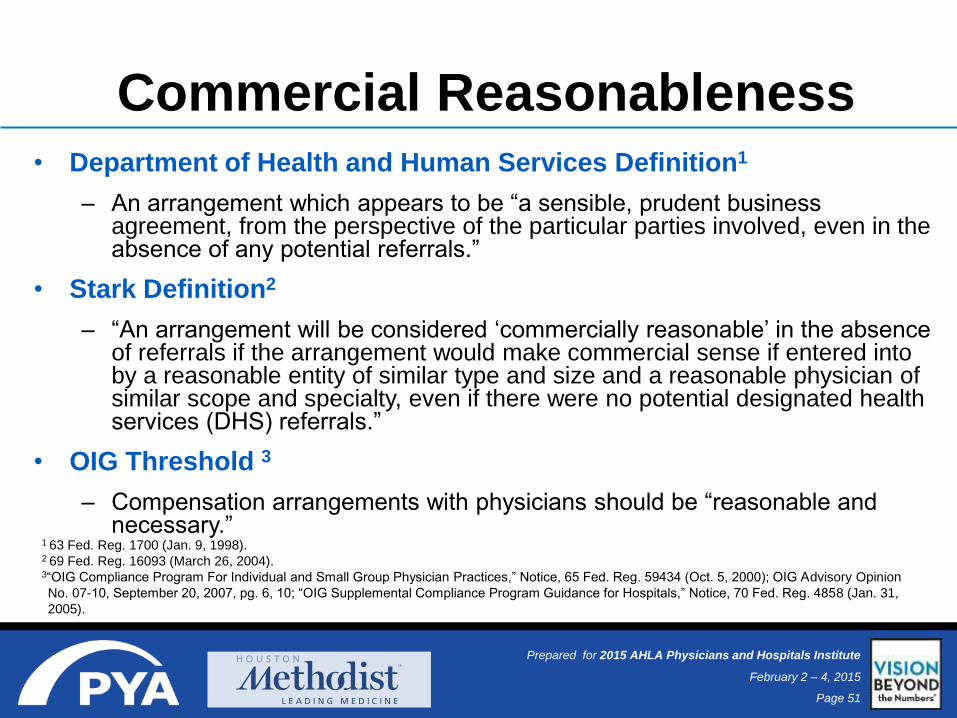
Commercial Reasonableness• Department of Health and Human Services Definition1
– An arrangement which appears to be “a sensible, prudent business agreement, from the perspective of the particular parties involved, even in the absence of any potential referrals.”
• Stark Definition2
– “An arrangement will be considered ‘commercially reasonable’ in the absence of referrals if the arrangement would make commercial sense if entered into by a reasonable entity of similar type and size and a reasonable physician of similar scope and specialty, even if there were no potential designated health services (DHS) referrals.”
• OIG Threshold 3
– Compensation arrangements with physicians should be “reasonable and necessary.”
1 63 Fed. Reg. 1700 (Jan. 9, 1998).2 69 Fed. Reg. 16093 (March 26, 2004).3“OIG Compliance Program For Individual and Small Group Physician Practices,” Notice, 65 Fed. Reg. 59434 (Oct. 5, 2000); OIG Advisory Opinion
No. 07-10, September 20, 2007, pg. 6, 10; “OIG Supplemental Compliance Program Guidance for Hospitals,” Notice, 70 Fed. Reg. 4858 (Jan. 31,
2005).

Page 52
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Factors in Determining CR
Business Purpose
Provider Analysis
Facility Analysis
Resource Analysis
Independence & Oversight
Commercial
Reasonableness
Determination

Page 53
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Commercial Reasonableness
Does the proposed service represent a reasonable necessity essential
to the functioning of the hospital?
Is the specific purpose of the service clearly identifiable and appropriately
defined?
Does the proposed service relate to the business and/or clinical plans
of the hospital?
Does the proposed service contribute to the hospital’s profits and/or the
development of a service line?
BUSINESS PURPOSE
Page 54
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Commercial Reasonableness
PROVIDER
ANALYSIS
Does the role require a physician to perform the services?
Does the role require a physician of a certain specialty to perform the
services?
Has the amount of time demanded of the physician in the proposed role
been considered?
Do any salary considerations exist related to providers of similar specialty
and experience in comparable organizations and positions?
PROVIDER ANALYSIS
Page 55
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Commercial Reasonableness
Is patient demand/number of hospital patients sufficient to justify the
service?
Are patient acuity levels such that the proposed service is necessary?
Do patient needs dictate the need for a separate and distinct physician
for the proposed services?
Is the size of the hospital and its relevant departments appropriate
for the proposed service?
FACILITY ANALYSIS

Page 56
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Commercial Reasonableness
Counsel
In – house
Outside
Valuation Firm
Internal
External
Internal
Management
Board
WHO DECIDES?

Page 57
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Factors Impacting Compensation
Payer mix
Productivity level
Many times measured by
encounter data
Supply/demand for
physicians in the local market
Hospitalists were the third
most highly recruited
specialty according to Merritt
Hawkins
Level of at-risk/incentive
compensation
Page 58
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Components of a Typical Subsidy
1
Fair market value
physician
compensation
2
Physician benefits
& malpractice
expense
3
Fair market
value MLP
compensation
4
MLP benefits &
malpractice
expense
5
Billing and
overhead
expense
6
Offset by
projected
collections
Page 59
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
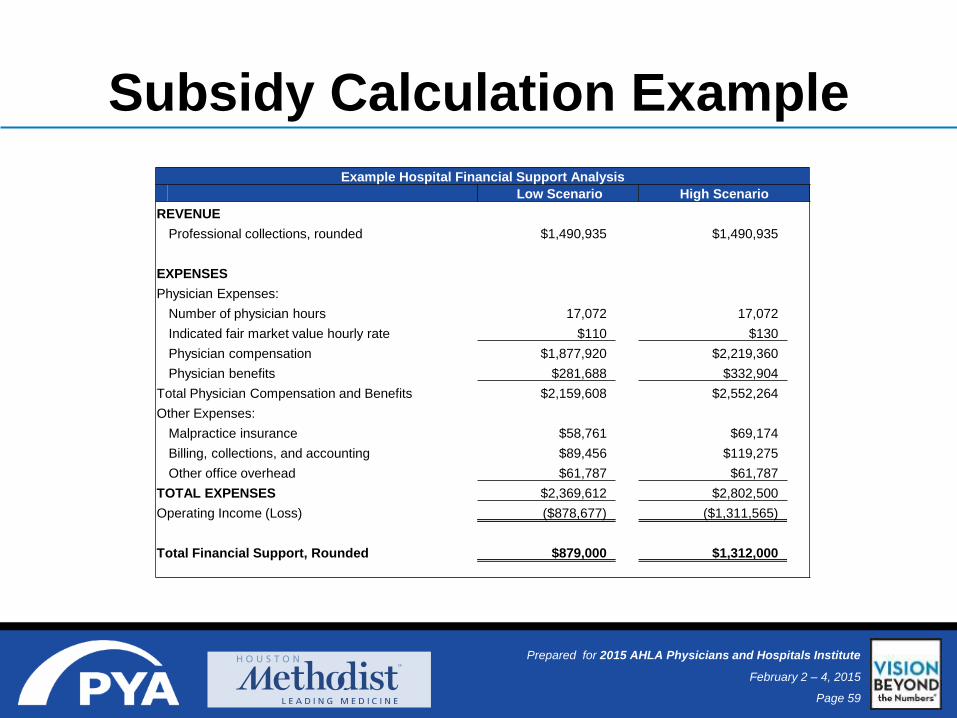
Subsidy Calculation Example
Example Hospital Financial Support Analysis
Low Scenario High Scenario
REVENUE
Professional collections, rounded $1,490,935 $1,490,935
EXPENSES
Physician Expenses:
Number of physician hours 17,072 17,072
Indicated fair market value hourly rate $110 $130
Physician compensation $1,877,920 $2,219,360
Physician benefits $281,688 $332,904
Total Physician Compensation and Benefits $2,159,608 $2,552,264
Other Expenses:
Malpractice insurance $58,761 $69,174
Billing, collections, and accounting $89,456 $119,275
Other office overhead $61,787 $61,787
TOTAL EXPENSES $2,369,612 $2,802,500
Operating Income (Loss) ($878,677) ($1,311,565)
Total Financial Support, Rounded $879,000 $1,312,000
Page 60
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Questions?
Page 61
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Web Resources
www.hospitalmedicine.org
www.pressganey.com
www.thefrontierproject.com
www.hhs.gov
www.qualitynet.org
www.hcahpsonline.org
www.hospitalcompare.hhs.gov
www.studergroup.com
Page 62
Prepared for 2015 AHLA Physicians and Hospitals Institute
February 2 – 4, 2015
Contact Information
Carol Carden, CPA/ABV, ASA
PYA
(800) 270-9629
www.pyapc.com
http://twitter.com/carolcardenpya
Mark Easterly, JD
Houston Methodist
(713) 441-2571
www.houstonmethodist.org
Related Documents











