Please cite this article in press as: Aakre I, et al. Excessive iodine intake and thyroid dysfunction among lactating Saharawi women. J Trace Elem Med Biol (2014), http://dx.doi.org/10.1016/j.jtemb.2014.09.009 ARTICLE IN PRESS G Model JTEMB-25613; No. of Pages 6 Journal of Trace Elements in Medicine and Biology xxx (2014) xxx–xxx Contents lists available at ScienceDirect Journal of Trace Elements in Medicine and Biology jou rn al homepage: www.elsevier.de/jtemb Nutrition Excessive iodine intake and thyroid dysfunction among lactating Saharawi women Inger Aakre a,b,∗ , Trine Bjøro c,d , Ingrid Norheim e , Tor A. Strand b,f , Ingrid Barikmo a , Sigrun Henjum a a Department of Health Nutrition and Management, Faculty of Health Sciences, Oslo and Akershus University College, Oslo, Norway b Department of Global Public Health and Primary Care, Faculty of Medicine and Dentistry, University of Bergen, Bergen, Norway c Department of Medical Biochemistry, Oslo University Hospital, Oslo, Norway d Institute of Clinical Medicine, University of Oslo, Oslo, Norway e Department of Endocrinology, Morbid Obesity and Preventive Medicine, Oslo University Hospital, Oslo, Norway f Medical Microbiology, Department of Laboratory Medicine, Medical Services Division, Innlandet Hospital Trust, Lillehammer, Norway a r t i c l e i n f o Article history: Received 6 August 2014 Accepted 24 September 2014 Keywords: Iodine excess Lactating women Thyroid dysfunction Breast milk iodine Urinary iodine a b s t r a c t Objectives: Excessive iodine intake may lead to thyroid dysfunction, which may be particularly harmful during pregnancy and lactation. The main objective was to describe iodine status and the prevalence of thyroid dysfunction among lactating women in areas with high iodine (HI) and very high iodine (VHI) concentrations in drinking water. Design and methods: A cross-sectional survey was performed among 111 lactating women in the Saharawi refugee camps, Algeria. Breast milk iodine concentration (BMIC), urinary iodine concentration (UIC) and the iodine concentration in the most commonly consumed foods/drinks were measured. A 24-h dietary recall was used to estimate iodine intake. Thyroid hormones and antibodies were measured in serum. Results: Median UIC, BMIC and iodine intake across both areas was 350 g/L, 479 g/L and 407 g/day, respectively. In multiple regression analyses, we discovered that being from VHI area was associated with higher UIC and BMIC. BMIC was also positively associated with iodine intake. Thyroid dysfunction and/or positive thyroid antibodies were found in 33.3% of the women, of which 18.9% had hypothyroidism and 8.1% had hyperthyroidism and 6.3% had positive antibodies with normal thyroid function. Elevated thy- roid antibodies were in total found in 17.1%. We found no difference in distribution of thyroid dysfunction or positive antibodies between HI and VHI areas. BMI, BMIC and elevated thyroglobulin (Tg) predicted abnormal thyroid function tests. Conclusions: The high prevalence of thyroid dysfunction may be caused by excessive iodine intake over several years. © 2014 Elsevier GmbH. All rights reserved. Introduction Adequate iodine intake is essential for synthesis of thyroid hor- mones, which are critical in several metabolic processes in the body [1]. Iodine intake both below and above the recommended ref- erence is associated with thyroid disease [2]. Iodine deficiency is still a global health issue, but there has been remarkable progress Laboratories used for analyses: Nutritional Intervention Research Unit in Cape Town, South Africa, National Institute of Nutrition and Seafood Research in Norway, Central Laboratory, Oslo University Hospital, Norway. ∗ Corresponding author at: HEL, Inger Aakre, Oslo and Akershus University College, Postboks 4 St. Olavs plass, 0130 Oslo, Norway. Tel.: +47 48132574. E-mail addresses: [email protected], [email protected] (I. Aakre). towards eliminating iodine deficiency disorders [3]. Iodine excess, on the other hand, has become more prevalent over the last decade, and the number of countries with excessive iodine intake, indicated by median urinary iodine excretion of ≥300 g/L, has doubled from 5 to 10 [4]. Iodine-induced thyroid dysfunction as a result of iodine excess may lead to both hypo- and hyperthyroidism [5]. Iodine status is a particularly important issue for pregnant and lactating women, since their nutritional status affects the child in utero and through breastfeeding, which may lead to impaired neurological child development [4,6]. An upper limit for iodine intake has not yet been established for lactating women [7], but high iodine con- centrations in breast milk caused by excessive iodine intakes have been described [8,9]. However, as far as we know, there are no stud- ies examining iodine status and thyroid function among lactating women with chronically high iodine intake. http://dx.doi.org/10.1016/j.jtemb.2014.09.009 0946-672X/© 2014 Elsevier GmbH. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

J
N
ES
ISa
b
c
d
e
f
a
ARA
KILTBU
I
m[es
TC
P
h0
ARTICLE IN PRESSG ModelTEMB-25613; No. of Pages 6
Journal of Trace Elements in Medicine and Biology xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Journal of Trace Elements in Medicine and Biology
jou rn al homepage: www.elsev ier .de / j temb
utrition
xcessive iodine intake and thyroid dysfunction among lactatingaharawi women�
nger Aakrea,b,∗, Trine Bjøroc,d, Ingrid Norheime, Tor A. Strandb,f, Ingrid Barikmoa,igrun Henjuma
Department of Health Nutrition and Management, Faculty of Health Sciences, Oslo and Akershus University College, Oslo, NorwayDepartment of Global Public Health and Primary Care, Faculty of Medicine and Dentistry, University of Bergen, Bergen, NorwayDepartment of Medical Biochemistry, Oslo University Hospital, Oslo, NorwayInstitute of Clinical Medicine, University of Oslo, Oslo, NorwayDepartment of Endocrinology, Morbid Obesity and Preventive Medicine, Oslo University Hospital, Oslo, NorwayMedical Microbiology, Department of Laboratory Medicine, Medical Services Division, Innlandet Hospital Trust, Lillehammer, Norway
r t i c l e i n f o
rticle history:eceived 6 August 2014ccepted 24 September 2014
eywords:odine excessactating womenhyroid dysfunctionreast milk iodinerinary iodine
a b s t r a c t
Objectives: Excessive iodine intake may lead to thyroid dysfunction, which may be particularly harmfulduring pregnancy and lactation. The main objective was to describe iodine status and the prevalence ofthyroid dysfunction among lactating women in areas with high iodine (HI) and very high iodine (VHI)concentrations in drinking water.Design and methods: A cross-sectional survey was performed among 111 lactating women in the Saharawirefugee camps, Algeria. Breast milk iodine concentration (BMIC), urinary iodine concentration (UIC) andthe iodine concentration in the most commonly consumed foods/drinks were measured. A 24-h dietaryrecall was used to estimate iodine intake. Thyroid hormones and antibodies were measured in serum.Results: Median UIC, BMIC and iodine intake across both areas was 350 �g/L, 479 �g/L and 407 �g/day,respectively. In multiple regression analyses, we discovered that being from VHI area was associated withhigher UIC and BMIC. BMIC was also positively associated with iodine intake. Thyroid dysfunction and/orpositive thyroid antibodies were found in 33.3% of the women, of which 18.9% had hypothyroidism and8.1% had hyperthyroidism and 6.3% had positive antibodies with normal thyroid function. Elevated thy-
roid antibodies were in total found in 17.1%. We found no difference in distribution of thyroid dysfunctionor positive antibodies between HI and VHI areas. BMI, BMIC and elevated thyroglobulin (Tg) predictedabnormal thyroid function tests.Conclusions: The high prevalence of thyroid dysfunction may be caused by excessive iodine intake overseveral years.© 2014 Elsevier GmbH. All rights reserved.
ntroduction
Adequate iodine intake is essential for synthesis of thyroid hor-ones, which are critical in several metabolic processes in the body
Please cite this article in press as: Aakre I, et al. Excessive iodine intaTrace Elem Med Biol (2014), http://dx.doi.org/10.1016/j.jtemb.2014.0
1]. Iodine intake both below and above the recommended ref-rence is associated with thyroid disease [2]. Iodine deficiency istill a global health issue, but there has been remarkable progress
� Laboratories used for analyses: Nutritional Intervention Research Unit in Capeown, South Africa, National Institute of Nutrition and Seafood Research in Norway,entral Laboratory, Oslo University Hospital, Norway.∗ Corresponding author at: HEL, Inger Aakre, Oslo and Akershus University College,ostboks 4 St. Olavs plass, 0130 Oslo, Norway. Tel.: +47 48132574.
E-mail addresses: [email protected], [email protected] (I. Aakre).
ttp://dx.doi.org/10.1016/j.jtemb.2014.09.009946-672X/© 2014 Elsevier GmbH. All rights reserved.
towards eliminating iodine deficiency disorders [3]. Iodine excess,on the other hand, has become more prevalent over the last decade,and the number of countries with excessive iodine intake, indicatedby median urinary iodine excretion of ≥300 �g/L, has doubled from5 to 10 [4]. Iodine-induced thyroid dysfunction as a result of iodineexcess may lead to both hypo- and hyperthyroidism [5]. Iodinestatus is a particularly important issue for pregnant and lactatingwomen, since their nutritional status affects the child in utero andthrough breastfeeding, which may lead to impaired neurologicalchild development [4,6]. An upper limit for iodine intake has notyet been established for lactating women [7], but high iodine con-
ke and thyroid dysfunction among lactating Saharawi women. J9.009
centrations in breast milk caused by excessive iodine intakes havebeen described [8,9]. However, as far as we know, there are no stud-ies examining iodine status and thyroid function among lactatingwomen with chronically high iodine intake.

IN PRESSG ModelJ
2 s in Medicine and Biology xxx (2014) xxx–xxx
hoa[
tiw
S
S
DSfirtarw
[wdti
ww
M
swtIor
amApI
dafnsa
(tsui(Ma
Table 1Reference ranges used for thyroid function tests.
Blood constitutes Reference levelsa
TSH 0.5–3.5 mlU/LFT4 9.0–21.0 pmol/LFT3 2.7–6.3 pmol/LTgAb <50 kU/LTPOAb <50 kU/LTg <78 �g/LTRAb <1.8 kU/L
ARTICLETEMB-25613; No. of Pages 6
I. Aakre et al. / Journal of Trace Element
The participants in this survey were Saharawi refugees whoave been settled in the Algerian refugee camps since 1975. Previ-us surveys have reported endemic goitre among Saharawi womennd children, probably due to iodine excess from ground water10,11].
The main objective of this paper is to describe iodine status andhe prevalence of thyroid dysfunction among lactating women liv-ng in areas of high iodine (HI) water and very high iodine (VHI)
ater.
ubjects and methods
ubjects
This cross-sectional study was conducted from October toecember 2010 in four different districts, all belonging to theaharawi refugee camps [12]. Lactating women and their childrenrom 0 to 7 months of age were the target group. A list of beneficiar-es was used to estimate the number of women in each of the fourefugee camps. The main objective of the project was to estimatehe prevalence of thyroid dysfunction in the population. Assuming
precision of ±5 percentage points around the prevalence estimateequired a sample size of approximately 100 women, as determinedith EpiInfo Statcalc, version 7.1.3.
The selection procedure was done by convenience sampling13] at health stations in the camps, and all of the eligible womenho accepted the invitation to participate were included until theesired number of participants was reached. We asked 153 womeno participate, and 111 met the inclusion criteria and accepted thenvitation.
Our data was analysed according to two areas within the campsith high iodine (HI) and very high iodine (VHI) in the drinkingater, as discovered in a previous study [14].
ethods
Spot urine samples were collected from all participants andtored at −20 ◦C until analysed. Twelve samples of public waterere collected in each area (n = 24). Analyses of iodine concentra-
ion in urine and water samples were performed at the Nutritionalntervention Research Unit in Cape Town, South Africa, by meansf manual acid digestion followed by the Sandell–Kolthoff reaction,ecorded spectrophotometrically [15].
Breast-milk samples were collected from all participants, andnimal-milk samples were collected from all households with ani-al milk available (n = 47). All milk samples were stored at −20 ◦C.nalyses of iodine content in milk were performed by the Cou-led Plasma-Mass Spectrometry method (ICP-MS) at the National
nstitute of Nutrition and Seafood Research in Norway [16].A 24-h dietary recall of iodine-rich foods and drinks was con-
ucted. The quantities consumed were assessed by the weighedmounts of the estimated intake using similar or same types ofood/drink on an electronic scale (Capere, Insjön, Sweden) to theearest 0.001 kg. Dietary variables were processed in Excel (ver-ion 14.0) using iodine concentration from the respective iodinenalyses for calculating iodine intake.
Blood samples were drawn in plastic clot activator gel tubesBD Vacutainer SST II, Oxford, UK) and kept at 5 ◦C until cen-rifuged and separated from the blood pellet within 2 h. Serumamples were stored in transfer tubes and kept frozen at −20 ◦Cntil analysed at the Central Laboratory, Oslo University Hospital
Please cite this article in press as: Aakre I, et al. Excessive iodine intaTrace Elem Med Biol (2014), http://dx.doi.org/10.1016/j.jtemb.2014.0
n Norway. Thyrotropin (TSH), free thyroxine (FT4), free triiodideFT3) and thyrotropin receptor antibodies (TRAb) were analysed on
odul E, Roche with CV < 7%; thyroglobulin (Tg) was analysed withn in-house time-resolved immunofluorometric assay (TR-IFMA)
a Used at Oslo University Hospital in Norway. For TSH also published by Bjoroet al. [18].
Auto-Delfia as previously described [17]; Tg antibodies (TgAb)were determined by Anti-TGn Kryptor from BRAHMS; and thyroidperoxidase antibodies (TPOAb) were measured with ImmunoCAPThyroid Peroxidase from Thermo Scientific, all with CV < 10%.
Reference ranges established at Oslo University Hospital andin the Norwegian HUNT study [18] were used for assessingthyroid dysfunction and are presented in Table 1. Overt hypothy-roidism was defined as TSH > 3.5 mIU/L and FT4 < 9 pmol/L, orTSH > 10 mIU/L and FT4 below the first quartile of this sample(<12 pmol/L). Subclinical hypothyroidism was defined at a TSHlevel of >3.5 mIU/L and <10 mIU/L with FT4 within the refer-ence range (9–21 pmol/L). Overt hyperthyroidism was defined asTSH < 0.5 mIU/L and FT4 and/or FT3 (T3 toxicosis) higher than theupper reference range. Subclinical hyperthyroidism was defined asTSH < 0.5 mIU/L and both FT4 and FT3 within the reference values.Positive antibodies were defined by TPOAb levels >50 kU/L and/orTgAb levels >50 kU/L. Due to interference of TgAb in the Tg assay[19], elevated Tg was assessed only in participants with Tg valuesabove the upper reference and who were TgAb negative.
The participants answered a pre-coded questionnaire concern-ing background variables. The questionnaire and 24-h dietaryrecall were administered by interview in the local language, Has-saniya. Body weight was measured using a UNICEF digital platformscale (SECA 890, Hamburg, Germany) and height was measuredto the nearest 0.1 cm using a portable UNICEF length board. TheWorld Health Organisation (WHO) body mass index (BMI) (kg/m2)was used to classify underweight, normal weight, overweightand obesity, defined by BMI < 18.5 kg/m2, BMI = 18.5–24.9 kg/m2,BMI = 25.0–29.9 kg/m2 and BMI ≥ 30 kg/m2, respectively.
Ethics approval for the survey was given by the Regional Com-mittees for Medical and Health Research Ethics in Norway andby the Saharawi Ministry of Public Health. Informed consent wasobtained both orally and in writing from all participants. It wasemphasised that refusal to participate or withdrawal from the sur-vey would not have any negative consequences for the participants.
Statistics
Data were entered and analysed using SPSS version 21 (SPSSInc., Chicago). Normally distributed data were expressed as mean(±SD). Variables that did not adhere to a normal distribution wereexpressed as median and interquartile range (IQR). Differencesbetween HI and VHI areas, as well as differences between womenwith and without thyroid dysfunction and positive antibodies,were tested using Student’s t-test for normally distributed data,Mann–Whitney U test for skewed data and Pearson’s Chi-squaretest for categorical data.
UIC and BMIC were used as dependent variables in multi-ple linear regression analyses. Due to skewed distributions, both
ke and thyroid dysfunction among lactating Saharawi women. J9.009
dependent variables were log2 transformed. UIC and BMIC wereexamined for associations with each other and the following vari-ables: area, Tg, estimated iodine intake, age of woman, age ofchildren and exclusively breastfeeding. For BMIC, breastfeeding
ARTICLE IN PRESSG ModelJTEMB-25613; No. of Pages 6
I. Aakre et al. / Journal of Trace Elements in Medicine and Biology xxx (2014) xxx–xxx 3
Table 2Characteristics of lactating women from HI and VHI areasa (n = 111).
Characteristics HI (n = 56) VHI (n = 55) p Total (n = 111)
Age, years 31.5 ± 5.7 31.3 ± 6.1 31.4 ± 5.9No. of children 2.9 ± 1.6 3.3 ± 2.1 3.1 ± 1.9Height, cm 157.2 ± 5.2 155.7 ± 5.6 156.5 ± 5.4Weight, kg 66.6 ± 10.2 65.6 ± 13.2 65.9 ± 11.7BMI, kg/m2 26.9 ± 3.7 26.9 ± 5.4 26.9 ± 4.6
<18.5 1 [1.8] 2 [3.6] 3 [2.7]18.5–24.9 16 [28.6] 17 [30.9] 33 [29.7]25.0–29.9 28 [50.0] 20 [36.4] 48 [43.2]≥30 11 [19.6] 16 [29.1] 27 [24.3]
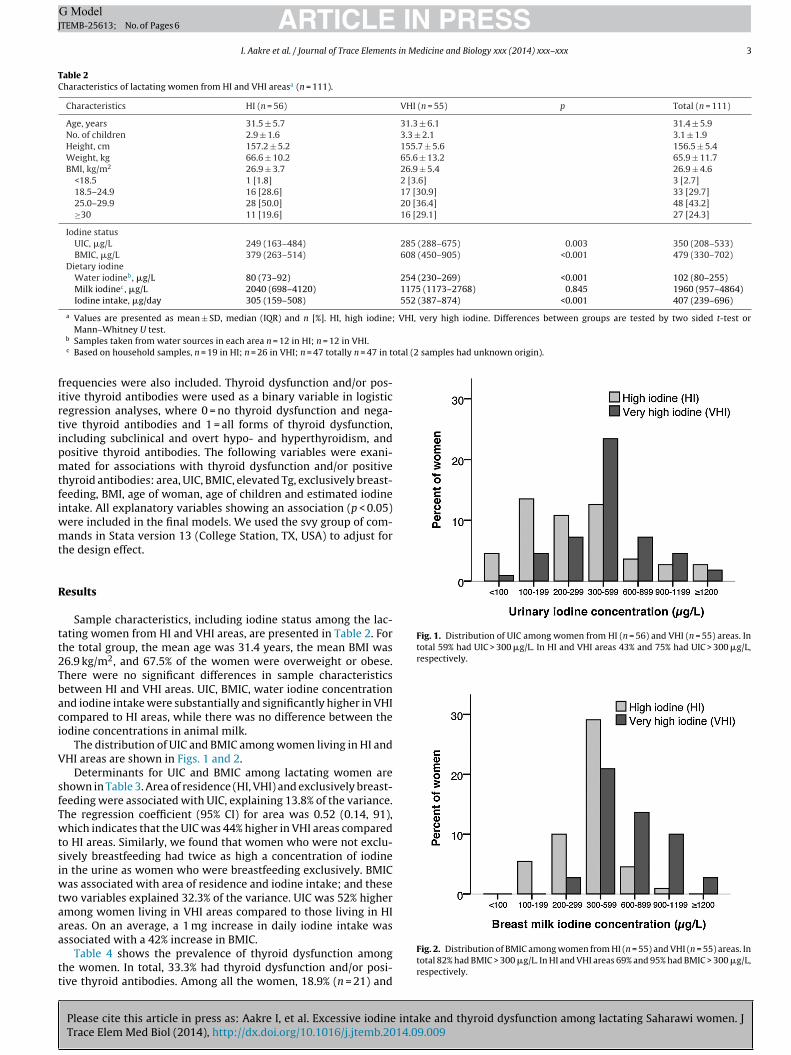
Iodine statusUIC, �g/L 249 (163–484) 285 (288–675) 0.003 350 (208–533)BMIC, �g/L 379 (263–514) 608 (450–905) <0.001 479 (330–702)
Dietary iodineWater iodineb, �g/L 80 (73–92) 254 (230–269) <0.001 102 (80–255)Milk iodinec, �g/L 2040 (698–4120) 1175 (1173–2768) 0.845 1960 (957–4864)Iodine intake, �g/day 305 (159–508) 552 (387–874) <0.001 407 (239–696)
a Values are presented as mean ± SD, median (IQR) and n [%]. HI, high iodine; VHI, very high iodine. Differences between groups are tested by two sided t-test or
otal (2 samples had unknown origin).
firtipmtfiwmt
R
tt2Tbaci
V
sfTwtsiwtaaa
tt
Fig. 1. Distribution of UIC among women from HI (n = 56) and VHI (n = 55) areas. Intotal 59% had UIC > 300 �g/L. In HI and VHI areas 43% and 75% had UIC > 300 �g/L,respectively.
Mann–Whitney U test.b Samples taken from water sources in each area n = 12 in HI; n = 12 in VHI.c Based on household samples, n = 19 in HI; n = 26 in VHI; n = 47 totally n = 47 in t
requencies were also included. Thyroid dysfunction and/or pos-tive thyroid antibodies were used as a binary variable in logisticegression analyses, where 0 = no thyroid dysfunction and nega-ive thyroid antibodies and 1 = all forms of thyroid dysfunction,ncluding subclinical and overt hypo- and hyperthyroidism, andositive thyroid antibodies. The following variables were exani-ated for associations with thyroid dysfunction and/or positive
hyroid antibodies: area, UIC, BMIC, elevated Tg, exclusively breast-eeding, BMI, age of woman, age of children and estimated iodinentake. All explanatory variables showing an association (p < 0.05)
ere included in the final models. We used the svy group of com-ands in Stata version 13 (College Station, TX, USA) to adjust for
he design effect.
esults
Sample characteristics, including iodine status among the lac-ating women from HI and VHI areas, are presented in Table 2. Forhe total group, the mean age was 31.4 years, the mean BMI was6.9 kg/m2, and 67.5% of the women were overweight or obese.here were no significant differences in sample characteristicsetween HI and VHI areas. UIC, BMIC, water iodine concentrationnd iodine intake were substantially and significantly higher in VHIompared to HI areas, while there was no difference between theodine concentrations in animal milk.
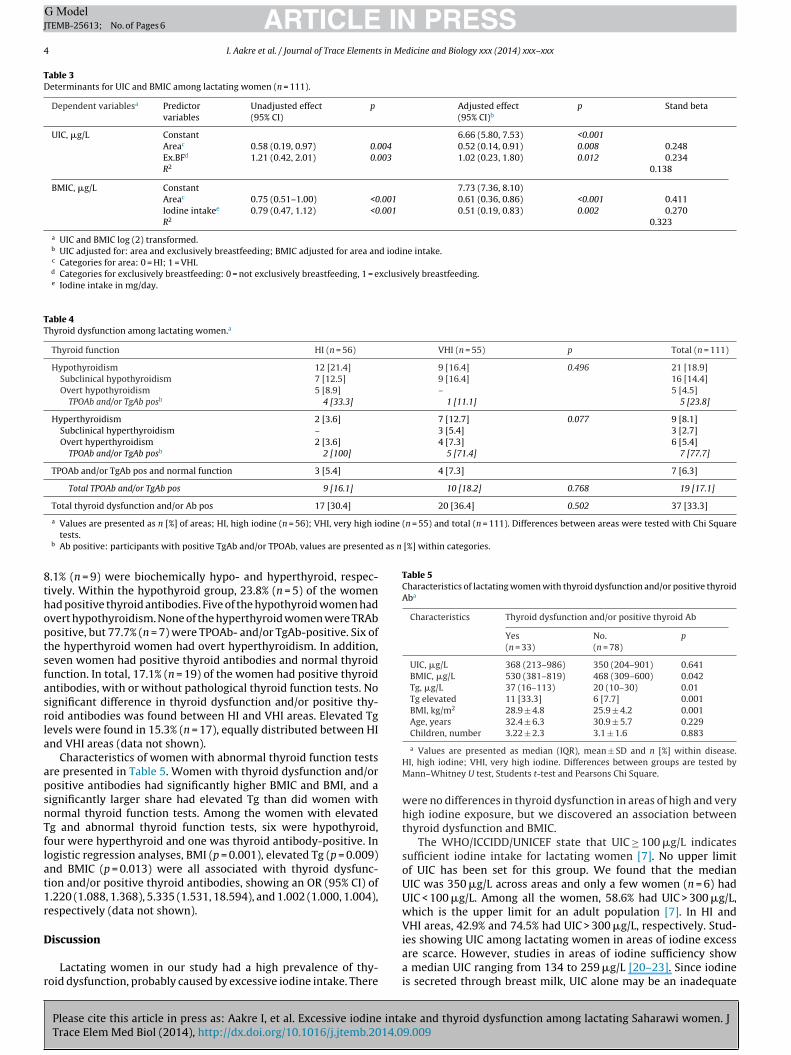
The distribution of UIC and BMIC among women living in HI andHI areas are shown in Figs. 1 and 2.
Determinants for UIC and BMIC among lactating women arehown in Table 3. Area of residence (HI, VHI) and exclusively breast-eeding were associated with UIC, explaining 13.8% of the variance.he regression coefficient (95% CI) for area was 0.52 (0.14, 91),hich indicates that the UIC was 44% higher in VHI areas compared
o HI areas. Similarly, we found that women who were not exclu-ively breastfeeding had twice as high a concentration of iodinen the urine as women who were breastfeeding exclusively. BMIC
as associated with area of residence and iodine intake; and thesewo variables explained 32.3% of the variance. UIC was 52% highermong women living in VHI areas compared to those living in HIreas. On an average, a 1 mg increase in daily iodine intake was
Please cite this article in press as: Aakre I, et al. Excessive iodine intake and thyroid dysfunction among lactating Saharawi women. JTrace Elem Med Biol (2014), http://dx.doi.org/10.1016/j.jtemb.2014.09.009
ssociated with a 42% increase in BMIC.Table 4 shows the prevalence of thyroid dysfunction among
he women. In total, 33.3% had thyroid dysfunction and/or posi-ive thyroid antibodies. Among all the women, 18.9% (n = 21) and
Fig. 2. Distribution of BMIC among women from HI (n = 55) and VHI (n = 55) areas. Intotal 82% had BMIC > 300 �g/L. In HI and VHI areas 69% and 95% had BMIC > 300 �g/L,respectively.
ARTICLE IN PRESSG ModelJTEMB-25613; No. of Pages 6
4 I. Aakre et al. / Journal of Trace Elements in Medicine and Biology xxx (2014) xxx–xxx
Table 3Determinants for UIC and BMIC among lactating women (n = 111).
Dependent variablesa Predictorvariables
Unadjusted effect(95% CI)
p Adjusted effect(95% CI)b
p Stand beta
UIC, �g/L Constant 6.66 (5.80, 7.53) <0.001Areac 0.58 (0.19, 0.97) 0.004 0.52 (0.14, 0.91) 0.008 0.248Ex.BFd 1.21 (0.42, 2.01) 0.003 1.02 (0.23, 1.80) 0.012 0.234R2 0.138
BMIC, �g/L Constant 7.73 (7.36, 8.10)Areac 0.75 (0.51–1.00) <0.001 0.61 (0.36, 0.86) <0.001 0.411Iodine intakee 0.79 (0.47, 1.12) <0.001 0.51 (0.19, 0.83) 0.002 0.270R2 0.323
a UIC and BMIC log (2) transformed.b UIC adjusted for: area and exclusively breastfeeding; BMIC adjusted for area and iodine intake.c Categories for area: 0 = HI; 1 = VHI.d Categories for exclusively breastfeeding: 0 = not exclusively breastfeeding, 1 = exclusively breastfeeding.e Iodine intake in mg/day.
Table 4Thyroid dysfunction among lactating women.a
Thyroid function HI (n = 56) VHI (n = 55) p Total (n = 111)
Hypothyroidism 12 [21.4] 9 [16.4] 0.496 21 [18.9]Subclinical hypothyroidism 7 [12.5] 9 [16.4] 16 [14.4]Overt hypothyroidism 5 [8.9] – 5 [4.5]
TPOAb and/or TgAb posb 4 [33.3] 1 [11.1] 5 [23.8]
Hyperthyroidism 2 [3.6] 7 [12.7] 0.077 9 [8.1]Subclinical hyperthyroidism – 3 [5.4] 3 [2.7]Overt hyperthyroidism 2 [3.6] 4 [7.3] 6 [5.4]
TPOAb and/or TgAb posb 2 [100] 5 [71.4] 7 [77.7]
TPOAb and/or TgAb pos and normal function 3 [5.4] 4 [7.3] 7 [6.3]
Total TPOAb and/or TgAb pos 9 [16.1] 10 [18.2] 0.768 19 [17.1]
Total thyroid dysfunction and/or Ab pos 17 [30.4] 20 [36.4] 0.502 37 [33.3]
dine (n = 55) and total (n = 111). Differences between areas were tested with Chi Square
d as n [%] within categories.
8thoptsfasrla
apsnTflat1r
D
r
Table 5Characteristics of lactating women with thyroid dysfunction and/or positive thyroidAba
Characteristics Thyroid dysfunction and/or positive thyroid Ab
Yes(n = 33)
No.(n = 78)
p
UIC, �g/L 368 (213–986) 350 (204–901) 0.641BMIC, �g/L 530 (381–819) 468 (309–600) 0.042Tg, �g/L 37 (16–113) 20 (10–30) 0.01Tg elevated 11 [33.3] 6 [7.7] 0.001BMI, kg/m2 28.9 ± 4.8 25.9 ± 4.2 0.001Age, years 32.4 ± 6.3 30.9 ± 5.7 0.229Children, number 3.22 ± 2.3 3.1 ± 1.6 0.883
a Values are presented as n [%] of areas; HI, high iodine (n = 56); VHI, very high iotests.
b Ab positive: participants with positive TgAb and/or TPOAb, values are presente
.1% (n = 9) were biochemically hypo- and hyperthyroid, respec-ively. Within the hypothyroid group, 23.8% (n = 5) of the womenad positive thyroid antibodies. Five of the hypothyroid women hadvert hypothyroidism. None of the hyperthyroid women were TRAbositive, but 77.7% (n = 7) were TPOAb- and/or TgAb-positive. Six ofhe hyperthyroid women had overt hyperthyroidism. In addition,even women had positive thyroid antibodies and normal thyroidunction. In total, 17.1% (n = 19) of the women had positive thyroidntibodies, with or without pathological thyroid function tests. Noignificant difference in thyroid dysfunction and/or positive thy-oid antibodies was found between HI and VHI areas. Elevated Tgevels were found in 15.3% (n = 17), equally distributed between HInd VHI areas (data not shown).
Characteristics of women with abnormal thyroid function testsre presented in Table 5. Women with thyroid dysfunction and/orositive antibodies had significantly higher BMIC and BMI, and aignificantly larger share had elevated Tg than did women withormal thyroid function tests. Among the women with elevatedg and abnormal thyroid function tests, six were hypothyroid,our were hyperthyroid and one was thyroid antibody-positive. Inogistic regression analyses, BMI (p = 0.001), elevated Tg (p = 0.009)nd BMIC (p = 0.013) were all associated with thyroid dysfunc-ion and/or positive thyroid antibodies, showing an OR (95% CI) of.220 (1.088, 1.368), 5.335 (1.531, 18.594), and 1.002 (1.000, 1.004),espectively (data not shown).
Please cite this article in press as: Aakre I, et al. Excessive iodine intaTrace Elem Med Biol (2014), http://dx.doi.org/10.1016/j.jtemb.2014.0
iscussion
Lactating women in our study had a high prevalence of thy-oid dysfunction, probably caused by excessive iodine intake. There
a Values are presented as median (IQR), mean ± SD and n [%] within disease.HI, high iodine; VHI, very high iodine. Differences between groups are tested byMann–Whitney U test, Students t-test and Pearsons Chi Square.
were no differences in thyroid dysfunction in areas of high and veryhigh iodine exposure, but we discovered an association betweenthyroid dysfunction and BMIC.
The WHO/ICCIDD/UNICEF state that UIC ≥ 100 �g/L indicatessufficient iodine intake for lactating women [7]. No upper limitof UIC has been set for this group. We found that the medianUIC was 350 �g/L across areas and only a few women (n = 6) hadUIC < 100 �g/L. Among all the women, 58.6% had UIC > 300 �g/L,which is the upper limit for an adult population [7]. In HI andVHI areas, 42.9% and 74.5% had UIC > 300 �g/L, respectively. Stud-
ke and thyroid dysfunction among lactating Saharawi women. J9.009
ies showing UIC among lactating women in areas of iodine excessare scarce. However, studies in areas of iodine sufficiency showa median UIC ranging from 134 to 259 �g/L [20–23]. Since iodineis secreted through breast milk, UIC alone may be an inadequate

ING ModelJ
s in Me
iwmtbowpoibTdi0cdm
rmfdattIm[
Vcittphsatsnocm
rhteoiCpetwadoocofpt
between BMIC and thyroid dysfunction and positive antibodies,
ARTICLETEMB-25613; No. of Pages 6
I. Aakre et al. / Journal of Trace Element
ndicator of iodine nutrition among lactating women. Among allomen, median BMIC was 479 �g/L, and in HI and VHI areas,edian BMIC was 379 �g/L and 608 �g/L, respectively. According
o Laurberg and Andersen [24], iodine content in breast milk shoulde approximately 135 �g/L in women consuming the daily rec-mmended iodine intake. High BMIC is reported in Asian cultureshere iodine rich seaweed soup is commonly consumed in theostpartum period [8]. Two Korean studies show central measuresf 2529 �g/L and 892 �g/L in the breast milk of women consum-ng iodine-rich seaweed soup [9,25]. Excessive iodine intake fromreast milk can result in subclinical hypothyroidism for infants [9].he WHO recommends a daily iodine intake of 90 �g/day for chil-ren aged 0–2 years. The median iodine intake for the children
n our study would be 380 �g/day if mean breast milk intake is.8 L/day, a level which is high above the recommended intake forhildren. Even though no upper limit has been defined for infants,ifferent studies suggest that high iodine intake among childrenay result in adverse health consequences [26,27].The iodine intake in both areas was high. Based on a 24-h dietary
ecall, we found that water, camel milk and goat milk were theajor dietary iodine sources. This coincides with previous findings
rom the refugee camps [14]. Iodine concentration in animal milkid not correspond with water iodine in HI and VHI areas, since thenimal milk was imported from different areas within and outsidehe camps. The median iodine intake was 407 �g/day, and almostwice as high in VHI (552 �g/day) areas as in HI (305 �g/day) areas.n both areas, the iodine intake was much higher than the recom-
ended daily intake of 250 �g/day set by the WHO/ICCIDD/UNICEF7].
In the multiple regression analyses, we found that area (HI andHI) predicted both UIC and BMIC, confirming that water iodineoncentration probably is the most important determinant for theodine concentration, as reported by others [26,28]. We also foundhat UIC was lower in women who were exclusively breastfeedinghan in those who were not. This is probably due to increased milkroduction in those who exclusively breastfed their children andence had more iodine excreted through their breast milk. Othertudies have similar results, where the degree of lactation was neg-tively associated with UIC [11,29,30]. Andersen et al. [31] foundhat UIC is dependent on fluid intake whereas BMIC is not. Our studyhowed a positive association between BMIC and iodine intake, butot between UIC and iodine intake. In a survey where high dosesf iodine were given to lactating women, BMIC increased signifi-antly while UIC remained stable, suggesting that BMIC might beore sensitive than UIC to iodine intake [32].In total, 33.3% of the women in our study had pathological thy-
oid function tests and/or positive thyroid antibodies. Biochemicalypo- and hyperthyroidism was found in 18.9% and 8.1%, respec-ively. Laurberg et al. [33] discovered in their study among thelderly that thyroid hypofunction was more prevalent in an areaf high iodine intake compared to an area of low or adequateodine intake. In an area of chronically high iodine exposure amonghinese adult men and women, Teng et al. [34] found that therevalence of hypo- and hyperthyroidism, including Graves’ dis-ase, was 8.1% and 3.4%, respectively, which is a lower numberhan found in our study. However, in these studies, both men andomen have been evaluated. Our study included only women, who
re known to have a higher prevalence than men of thyroid disor-ers. The women in our study had all recently given birth and somef the women might have had postpartum thyroid dysfunction. Inur study, 17.1% of the women had positive thyroid antibodies, indi-ating autoimmune aetiology of the thyroid dysfunction in many
Please cite this article in press as: Aakre I, et al. Excessive iodine intaTrace Elem Med Biol (2014), http://dx.doi.org/10.1016/j.jtemb.2014.0
f them. This is a high incidence compared to data in the reviewrom Nicholson et al. [35], showing that the global prevalence ofostpartum thyroid dysfunction varied from 4.4% in Asia to 5.7% inhe United States.
PRESSdicine and Biology xxx (2014) xxx–xxx 5
Studies in both humans and animals have discovered thatan increase in iodine intake enhances thyroid autoimmunity[33,36–38]. The prevalence of both thyroid dysfunction and thyroidautoimmunity was high in our study, but we found no signifi-cant difference between HI and VHI areas. However, this may beexplained by the fact that the iodine exposure in both HI and VHIareas are high and all the women have probably been exposed tohigh iodine in drinking water and milk for several years. Other stud-ies have observed a positive correlation with prevalence of overthypothyroidism and positive antibodies [33,39]. We found thatthyroid dysfunction (hypo- and hyperthyroidism) was significantlycorrelated (p < 0.001) to positive antibodies (data not shown).
We found a significant difference in BMIC between women withnormal and abnormal thyroid function tests. This indicates thatBMIC might be a better indicator for iodine status in lactatingwomen than is UIC, as suggested by Leung et al. [32]. Serum Tghas been reported to be an indicator for both iodine deficiencyand excess [40]. In women with thyroid dysfunction, we found37% with elevated Tg (>78 �g/L). Median Tg was 37 �g/L amongwomen with thyroid dysfunction and/or positive thyroid antibod-ies and was significantly higher among women with normal thyroidfunction (median Tg 20 �g/L), indicating either increased volumeof the thyroid gland or increased leakage of Tg from the gland, dueeither to TSH stimulation or increased secretion of thyroid hor-mones.
Two thirds of the women in our study were overweight or obese.The mean BMI was 26.9 kg/m2, and 24% had BMI > 30 kg/m2. Theassociation between a small elevation in TSH and an increase inBMI has earlier been reported [41,42]. In our study, the womenwith thyroid dysfunction had a substantially higher BMI than thewomen with normal thyroid function tests.
Strengths and limitations
The strength of our study is the high rate of participation amongthe women and the relatively large amount of data obtained [43].However, a random sample was not feasible to obtain becauseof the difficult living situation of the refugees. The conditions inthe refugee camps are quite similar, sharing the same food aidprogrammes, water sources and health care services. There arealso small differences in socioeconomic variables [44]. We used24-h recall for assessing iodine intake. Only the most iodine richfoods/drinks were included in the 24 h recall, which was waterand animal milk. Other foods and drinks may have contributed tothe total iodine intake. In addition there is likely that water iodineintake is underestimated, since all water used for cooking purposesmay not have been captured. The power to detect statistical asso-ciations between dietary intake and health outcomes is generallylimited. We assessed thyroid dysfunction biochemically, using ref-erence ranges defined at our laboratory and in a well-characterizedbut quite different population in Norway [18]. Reference rangesmay be different in populations due to variations in nutritionalstatus and genetics, and also due to methodological differences. Acontrol group in a similar area with adequate iodine status wouldhave been advantageous.
Conclusions
Our data indicate that BMIC might be a good indicator foriodine status among lactating women. We also found an association
ke and thyroid dysfunction among lactating Saharawi women. J9.009
which indicate that thyroid dysfunction, may be caused by exces-sive iodine intake. The high prevalence of thyroid dysfunction andthe chronically high intake of iodine might have adverse healthconsequences for the women and their children.
ING ModelJ
6 s in M
F
lNE
C
A
fisf
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ARTICLETEMB-25613; No. of Pages 6
I. Aakre et al. / Journal of Trace Element
unding
This study was supported by Oslo and Akershus University Col-ege, Department of Health, Nutrition and Management, and theorwegian Church Aid. TAS was funded by a grant from the South-astern Norway Regional Health Authority (grant no. 2012090).
onflict of interest
None declared.
cknowledgements
We would like to thank the Saharawi Health Authorities and oureldworkers for all of their support and cooperation throughout theurvey. We also would like to thank Lisbeth Dahl and Pieter Joosteor conducting the iodine analyses in milk, water and urine.
eferences
[1] Vanderpas J. Nutritional epidemiology and thyroid hormone metabolism. AnnuRev Nutr 2006;26:293–322.
[2] Laurberg P, Cerqueira C, Ovesen L, Rasmussen LB, Perrild H, Andersen S, et al.Iodine intake as a determinant of thyroid disorders in populations. Best PractRes Clin Endocrinol Metab 2010;24:13–27.
[3] Pearce EN, Andersson M, Zimmermann MB. Global iodine nutrition: where dowe stand in 2013. Thyroid 2013;23:523–8.
[4] Zimmermann BM. Iodine deficiency and excess in children: worldwide statusin 2013. Endocr Pract 2013;11:1–27.
[5] Leung AM, Braverman LE. Consequences of excess iodine. Nat Rev Endocrinol2014;10:136–42.
[6] Zimmermann BM. The role of iodine in human growth and development. SemCell Dev Biol 2011;22:645–52.
[7] WHO. Assessment of iodine deficiency disorders and monitoring their elimi-nation. A guide for programme managers. 2nd ed. World Health Organisation,International Council for Control of Iodine Deficiency Disorders, United NationsChildren’s Fund; 2007.
[8] Rhee SS, Braverman LE, Pino S, He X, Pearce EN. High iodine content of Koreanseaweed soup: a health risk for lactating women and their infants. Thyroid2011;21:927–8.
[9] Chung HR, Shin CH, Yang SW, Choi CW, Kim BI. Subclinical hypothyroidism inKorean preterm infants associated with high levels of iodine in breast milk. JClin Endocrinol Metab 2009;94:4444–7.
10] Henjum S, Barikmo I, Gjerlaug AK, Mohamed-Lehabib A, Oshaug A, Strand TA,et al. Endemic goitre and excessive iodine in urine and drinking water amongSaharawi refugee children. Publ Health Nutr 2010;13:1472–7.
11] Henjum S, Barikmo I, Strand TA, Oshaug A, Torheim LE. Iodine-induced goitreand high rates of anaemia among Saharawi refugee women. Publ Health Nutr2011;15:1512–8.
12] SMH, NCA and AUC. Prevalence of goitre and evaluation of food intake amongSaharawi refugees in camps in Tindouf, Algeria. Saharawi Ministry of Health,Department of Health, Norwegian Church Aid, Akershus University College;2008.
13] Gibson RS. Sampling protocols. In: Principles of nutritional assessment. NewYork: Oxford University Press; 2005. p. 9–11.
14] Barikmo I, Henjum S, Dahl L, Oshaug A, Torheim LE. Environmental implicationof iodine in water, milk and other foods used in Saharawi refugee camps inTindouf, Algeria. J Food Compos Anal 2011;24:637–41.
15] Jooste LP, Strydom E. Methods for determination of iodine in urine and salt.Best Pract Res Clin Endocrinol Metab 2010;24:77–88.
16] Dahl L, Johansson L, Julshamn K, Meltzer HM. The iodine content of Norwegianfoods and diets. Publ Health Nutr 2004;7:569–76.
17] Sigstad E, Heilo A, Paus E, Holgersen K, Grøholt K, Jørgensen L, et al. The useful-ness of detecting thyroglobulin in fine-needle aspirates from patients with necklesions using a sensitive thyroglobulin assay. Diagn Cytopathol 2007;35:761–7.
18] Bjoro T, Holmen J, Kruger O, Midthjell K, Hunstad K, Schreiner T, et al. Prevalenceof thyroid disease, thyroid dysfunction and thyroid peroxidase antibodies in a
Please cite this article in press as: Aakre I, et al. Excessive iodine intaTrace Elem Med Biol (2014), http://dx.doi.org/10.1016/j.jtemb.2014.0
large, unselected population. The Health Study of Nord-Trondelag (HUNT). EurJ Endocrinol 2000;143:639–47.
19] Spencer C, Fatemi S. Thyroglobulin antibody (TgAb) methods – strengths,pitfalls and clinical utility for monitoring TgAb-positive patients with differen-tiated thyroid cancer. Best Pract Res Clin Endocrinol Metab 2013;27:701–12.
[
PRESSedicine and Biology xxx (2014) xxx–xxx
20] Wang Y, Zhang Z, Ge P, Wang Y, Wang S. Iodine status and thyroid functionof pregnant, lactating women and infants (0–1 yr) residing in areas with aneffective Universal Salt Iodization program. Asia Pacif J Clin Nutr 2009;18:34.
21] Temple VJ, Haindapa B, Turare R, Masta A, Amoa AB, Ripa P. Status of iodinenutrition in pregnant and lactating women in national capital district, PapuaNew Guinea. Asia Pacif J Clin Nutr 2006;15:533.
22] Azizi F. Iodine nutrition in pregnancy and lactation in Iran. Publ Health Nutr2007;10:1596–9.
23] Ordookhani A, Pearcet NE, Hedayati M, Mirmiran P, Salimi S, Azizi F, et al.Assessment of thyroid function and urinary and breast milk iodine concen-trations in healthy newborns and their mothers in Tehran. Clin Endocrinol2007;67:175–9.
24] Laurberg P, Andersen LS. Breast milk – a gateway to iodine-dependent braindevelopment. Nat Rev Endocrinol 2014:10.
25] Moon S, Kim J. Iodine content of human milk and dietary iodine intake of Koreanlactating mothers. Int J Food Sci Nutr 1999;50:165–71.
26] Sang Z, Chen W, Shen J, Tan L, Zhao N, Liu H, et al. Long-term exposure toexcessive iodine from water is associated with thyroid dysfunction in children.J Nutr 2013;143:2038–43.
27] Zimmermann MB, Ito Y, Hess SY, Fuijeda K, Molinari L. High thyroid vol-ume in children with excess dietary iodine intakes. Am J Clin Nutr 2005;81:840–4.
28] Lv S, Wang Y, Xu D, Rutherford S, Chong Z, Du Y, et al. Drinking water con-tributes to excessive iodine intake among children in Hebei, China. Eur J ClinNutr 2013;67:961–5.
29] Schulze K, West K, Gautschi L, Dreyfuss M, LeClerq S, Dahal B, et al. Seasonalityin urinary and household salt iodine content among pregnant and lactatingwomen of the plains of Nepal. Eur J Clin Nutr 2003;57:969–76.
30] Eltom A, Eltom M, Elnagar B, Elbagir M, Gebre-Medhin M. Changes in iodinemetabolism during late pregnancy and lactation: a longitudinal study amongSudanese women. Eur J Clin Nutr 2000;54:429–33.
31] Andersen SL, Møller M, Laurberg P. Iodine concentrations in milk and in urineduring breastfeeding are differently affected by maternal fluid intake. Thyroid2014;24:764–72.
32] Leung AM, Braverman LE, He X, Heeren T, Pearce EN. Breast milk iodineconcentrations following acute dietary iodine intake. Thyroid 2012;22:1176–80.
33] Laurberg P, Pedersen MK, Hreidarsson A, Sigfusson N, Iversen E, Knudsen RP.Iodine intake and the pattern of thyroid disorders: a comparative epidemio-logical study of thyroid abnormalities in the elderly in Iceland and in Jutland,Denmark. J Clin Endocrinol Metab 1998;83:756–69.
34] Teng W, Shan Z, Teng X, Guan H, Li Y, Teng D, et al. Effect of iodine intake onthyroid diseases in China. New Engl J Med 2006;354:2783–93.
35] Nicholson WK, Robinson KA, Smallridge RC, Ladenson PW, Powe NR. Preva-lence of postpartum thyroid dysfunction: a quantitative review. Thyroid2006;16:573–82.
36] Teng X, Shan Z, Teng W, Fan C, Wang H, Guo R. Experimental study on the effectsof chronic iodine excess on thyroid function, structure, and autoimmunity inautoimmune-prone NOD.H2h4 mice. Clin Exp Med 2009;9:51–9.
37] Barin J, Talor M, Sharma R, Rose N, Burek C. Iodination of murine thyroglobulinenhances autoimmune reactivity in the NOD.H2h4 mouse. Clin Exp Immunol2005;142:251–9.
38] Alsayed A, Gad AM, Abdel-Baset H, Abdel-Fattah A, Ahmed A, Azab A. Excess uri-nary iodine is associated with autoimmune subclinical hypothyroidism amongEgyptian women. Endocr J 2008;55:601–5.
39] Roos A, Links TP, de Jong-van den Berg LT, Gans RO, Wolffenbuttel BH,Bakker SJ. Thyroid peroxidase antibodies, levels of thyroid stimulating hor-mone and development of hypothyroidism in euthyroid subjects. Eur J InternMed 2010;21:555–9.
40] Zimmermann MB, Aeberli I, Andersson M, Assey V, Yorg JAJ, Jooste P, et al.Thyroglobulin is a sensitive measure of both deficient and excess iodine intakesin children and indicates no adverse effects on thyroid function in the UIC rangeof 100–299 �g/L: a UNICEF/ICCIDD Study Group report. J Clin Endocrinol Metab2013;98:1271–80.
41] Bjergved L, Jørgensen T, Perrild H, Laurberg P, Krejbjerg A, Ovesen L, et al. Thy-roid function and body weight: a community-based longitudinal study. PLOSONE 2014:9.
42] Åsvold BO, Bjøro T, Vatten LJ. Association of serum TSH with high bodymass differs between smokers and never-smokers. J Clin Endocrinol Metab2009;94:5023–7.
43] Andersen S, Karmisholt J, Pedersen KM, Laurberg P. Reliability of studies ofiodine intake and recommendations for number of samples in groups and in
ke and thyroid dysfunction among lactating Saharawi women. J9.009
individuals. Brit J Nutr 2008;99:813–8.44] WFP, MDM, NCA. & AUC. Nutritional and food security survey among the
Saharawi refugees in camps in Tindouf, Algeria, October 2008. World FoodProgramme, Medicos del Mundo, Norwegian Church Aid, Akershus UniversityCollege; 2008.
Related Documents