Transcribed Notes Wednesday - 10/22/14 Last class we spoke about contractility and the ejection fraction. What does contractility mean? It relies on calcium ; you get more calcium in and you get a stronger force of contraction. This is different from starling’s law where you get a stronger force of contraction because the ventricles have been stretched and the fibers have been aligned properly. Understand that when we are talking about stretch of the ventricle, within physiological ranges, it usually is true that the more the ventricle stretches the stronger the force of contraction is… but in somebody who has a weak or sickened heart where they get into a volume overload situation where they are in heart failure, their ventricles will start to dilate much further than they normally would and when that happens you will take the fibers out of the optimal alignment and overstretch the skeletal muscle and contractile force goes down. What is the ejection fraction? Percentage of the end diastolic volume that is represented by the stroke volume; EF= SV/EDV. It is essentially saying to you: when the ventricles contract, what fraction of the end diastolic volume are they able to eject? Normal = 60-65%. Ejection fraction is important because it is an indicator of cardiac health; when somebody is in heart failure, his or her ejection fraction will start to fall. If their ejection fraction starts to fall… that means that they are leaving more blood in the ventricles with each cycle and that can cause dilation which leads to heart failure. (EX: During maximal exercise, the ejection fraction can rise to about 90%; so that would mean if your end diastolic volume was 100mls, your stroke volume would be 90 mls, and the end systolic volume would be 10 mls.) *KNOW HOW TO CALCULATE THIS, I WILL SEND YOU A LIST OF ANY CALCULATIONS YOU NEED TO KNOW*

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Transcribed NotesWednesday - 10/22/14
Last class we spoke about contractility and the ejection fraction.
What does contractility mean? It relies on calcium; you get more calcium in and you get a stronger force of contraction. This is different from starling’s law where you get a stronger force of contraction because the ventricles have been stretched and the fibers have been aligned properly. Understand that when we are talking about stretch of the ventricle, within physiological ranges, it usually is true that the more the ventricle stretches the stronger the force of contraction is… but in somebody who has a weak or sickened heart where they get into a volume overload situation where they are in heart failure, their ventricles will start to dilate much further than they normally would and when that happens you will take the fibers out of the optimal alignment and overstretch the skeletal muscle and contractile force goes down.
What is the ejection fraction? Percentage of the end diastolic volume that is represented by the stroke volume; EF= SV/EDV. It is essentially saying to you: when the ventricles contract, what fraction of the end diastolic volume are they able to eject? Normal = 60-65%. Ejection fraction is important because it is an indicator of cardiac health; when somebody is in heart failure, his or her ejection fraction will start to fall. If their ejection fraction starts to fall… that means that they are leaving more blood in the ventricles with each cycle and that can cause dilation which leads to heart failure. (EX: During maximal exercise, the ejection fraction can rise to about 90%; so that would mean if your end diastolic volume was 100mls, your stroke volume would be 90 mls, and the end systolic volume would be 10 mls.) *KNOW HOW TO CALCULATE THIS, I WILL SEND YOU A LIST OF ANY CALCULATIONS YOU NEED TO KNOW*
CLICK QUESTION:Patient has an EDV of 100 mls, and an ESV of 40 mls. What is the
ejection fraction?1. 40%2. 50%3. 60%4. 80%
Inotropic agents
So inotropicity refers to contractility. So if a drug is a positive inotropic agent what do you think that does to the contractility? It increases it. Negative inotropic agents decrease contractility. CALCIUM is the only thing that can
increase contractility so it should make sense to you that positive inotropic agents do something to increase intracellular calcium levels and negative inotropic agents would do something to decrease calcium levels.
Positive inotropic agents o Epinephrine and Norepinephrine are positive inotropes
due to their actions on beta-receptors. They elevate cyclicAMP and the effect of that is an opening of calcium channels. So when norepi and epinephrine are around calcium channels open and you get more calcium influx into the cell and a stronger force of contraction because of that. These two also increase heart rate as well so they have really big effects on cardiac output because they increase both heart rate and stroke volume.
o Glucagon stimulates cyclicAMP formation, which would have the effect of opening up calcium channels.
o Digitalis increases intracellular calcium. You would tend to believe that if the sympathetic nervous
system stimulates contractility, then it must be the case that the parasympathetic nervous system decreases contractility… if the parasympathetic nervous system could it probably would… But it turns out that the parasympathetic nervous system doesn’t have a lot of innervation on the ventricles.
Negative Inotropic agents o Remember beta-blockers? It should make sense to you
that negative inotropic agents would block beta 1 receptors in the heart, and by doing so they would decrease levels of intracellular calcium and decrease contractility.
o Calcium-channel blockers are another class of drugs—(Again… because cardiac muscle relies on calcium from external sources that occurs through the entry through voltage gated calcium channels) if you block those voltage gated calcium channels, you block calcium entry and block the amount of calcium in the cell, which will lower contractility.
Cardiac Preload and Afterload
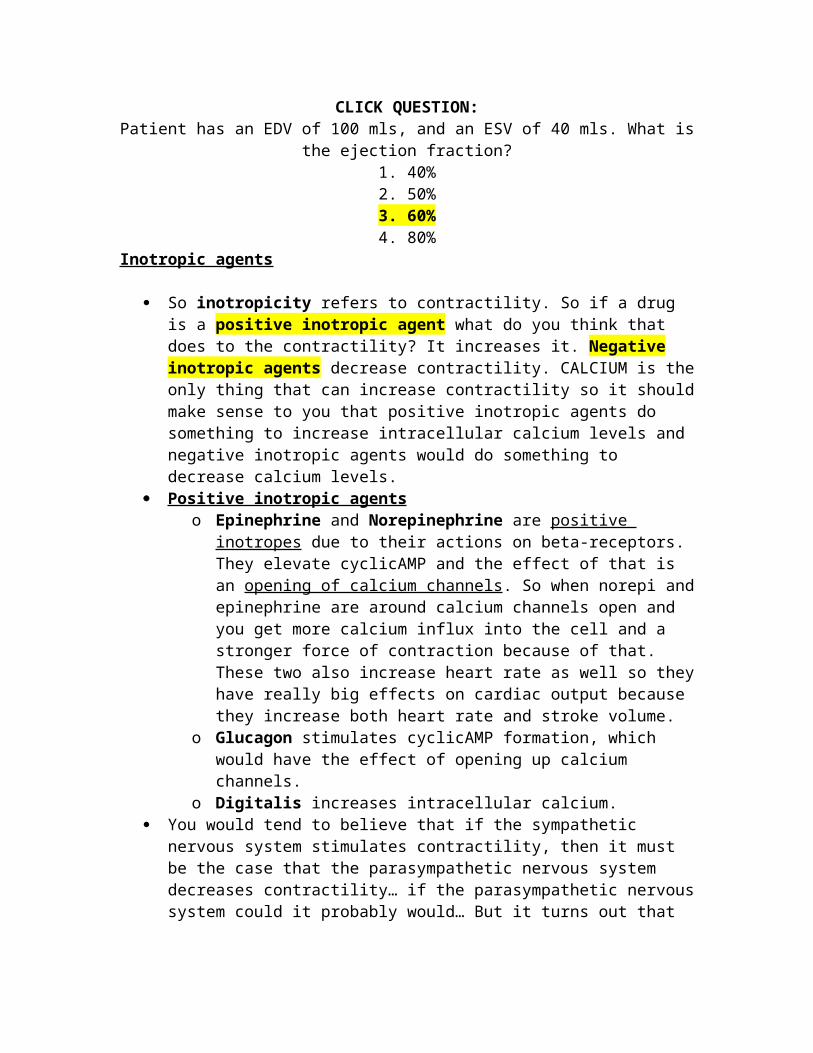
Preload = end diastolic volume; the load that’s on the ventricles before they
contract. Afterload = it is essentially the amount of pressure that the
heart has to generate in order to get the blood moving out the
aortic semilunar valve. In other words, it is the load that is opposing the ventricle. Think about it this way: when does the aortic semilunar valve open? When ventricular pressure is greater than aortic pressure. So afterload really can be thought of as aortic pressure because the higher the aortic pressure is... what can you say about the workload the ventricles have to do to get the blood ejected? It’s gonna have to generate more pressure and more work. So afterload really is aortic pressure and is also approximated by mean pressure. The main determinant of afterload is total peripheral resistance (to be discussed). Do you understand that when vessels are very constricted, that pressure goes up? That is because blood pressure is essentially the force that the blood is exerting on the vessel walls, so if you contain that blood in a smaller space… there is more force against the vessel wall. So when blood vessels constrict, pressure goes up. Total peripheral resistance is like the net sum of how constricted all the vessels across the body are.
For example: People that drive a million miles an hour and cut people off. Well some guy was honking his horn at somebody behind me and was yelling out of his window, and he came around and screeched his tires and jumped out of his car and went running out. Well people like that… what happens to them if they don’t get into a car accident? They usually have a heart attack and this is why. Their total peripheral resistance is through the roof. Their vessels are all constricted which means that their blood pressure will increase like crazy. If their aortic pressure is really high, what is their heart gonna have to do to try to get blood out the aorta? The heart is gonna have to contract really forcefully. So years and years and years of that puts this huge load on the heart and the heart gets weakened and tired. This force that the ventricles have to generate or have to overcome to get the blood moving out the aorta, or quite simply the aortic pressure is afterload. Afterload is essentially the force the heart has to work against to get blood moving or the pressure that the heart has to work against to get the blood ejected and delivered to the body. So that guys blood
pressure is probably sky high and his aortic pressure as well, which means that his afterload is high. This means that his heart is working like crazy just to try to meet the demands of the body. After 15-20 years of being a psycho like this you can expect someone’s heart to fail. So the goal here is to keep afterload as low as we possibly can.
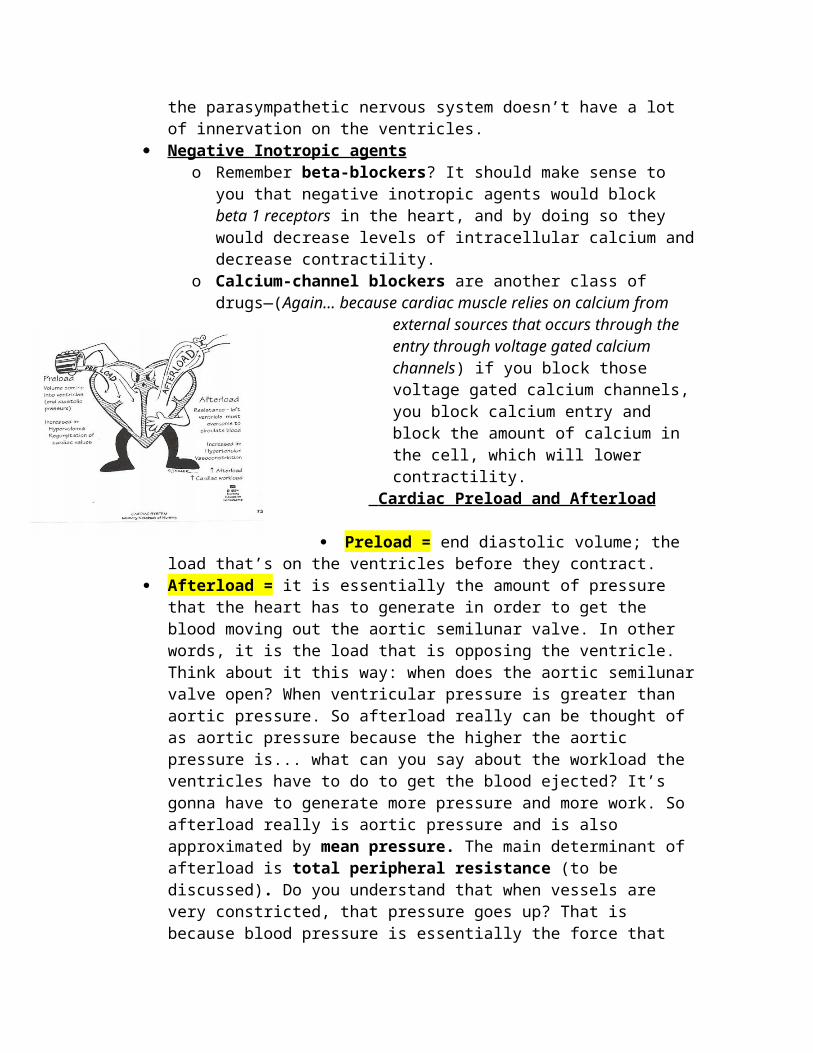
< --- This is just to remind you that you can’t get blood moving out the aorta and delivered to the body until the ventricles exceed aortic pressure. So if the aortic pressure was way higher than the ventricular pressure, the heart is gonna have to work much harder to generate more pressure. If the heart cannot work harder, it is gonna delay the time
that it takes for the semilunar valve to open and the time that you have for ejection is gonna be reduced.
You guys probably know that blood pressure recommendations are 120/80. Nobody ever worried too much until you had 140/90. Now the recommendations have changed and they want everyone blood pressure below 120/80 and if youre higher than that they will tell you to start dieting and exercising. The reason for it is because they found that vene small elevations in pressure over the long term have very harmful effects on the heart and the vasculature, which can lead to diseases.
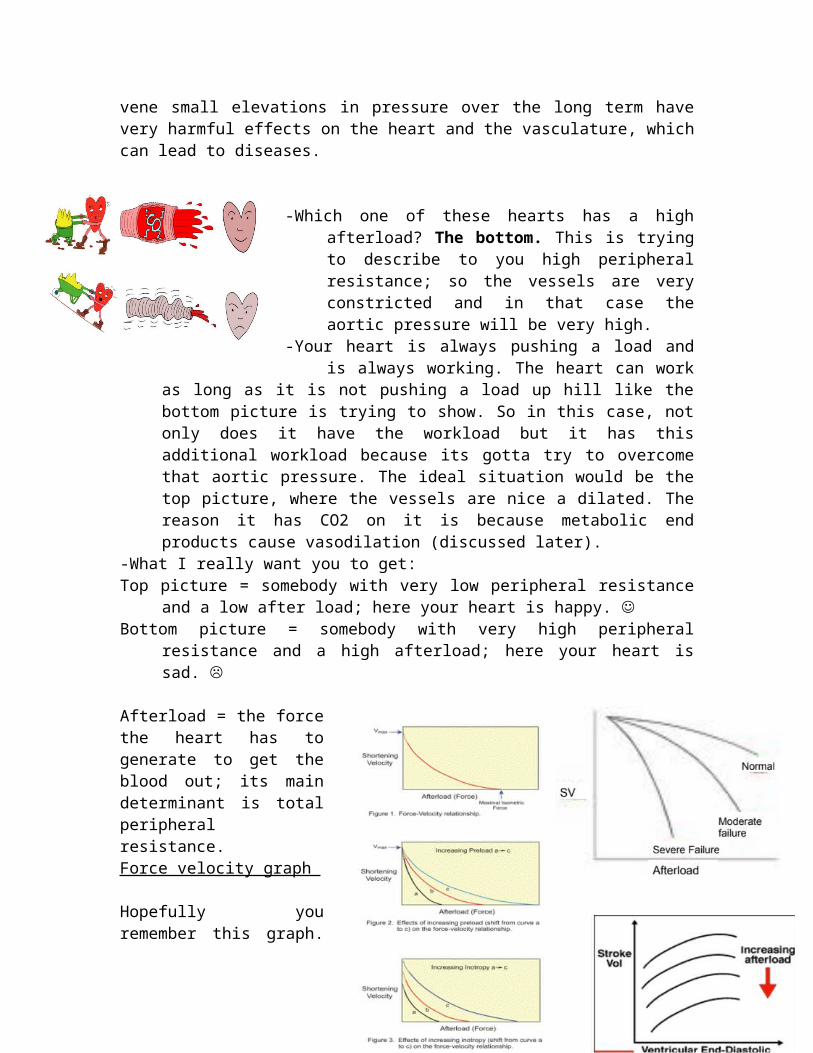
-Which one of these hearts has a high afterload?
The bottom. This is trying to describe to you high peripheral resistance; so the vessels are very constricted and in that case the aortic pressure will be very high.
-Your heart is always pushing a load and is always working. The heart can work as long as it is not pushing a load up hill like the bottom picture is trying to show. So in this case, not
only does it have the workload but it has this additional workload because its gotta try to overcome that aortic pressure. The ideal situation would be the top picture, where the vessels are nice a dilated. The reason it has CO2 on it is because metabolic end products cause vasodilation (discussed later).
-What I really want you to get: Top picture = somebody with very low peripheral resistance and a low
after load; here your heart is happy. Bottom picture = somebody with very high peripheral resistance and a
high afterload; here your heart is sad.
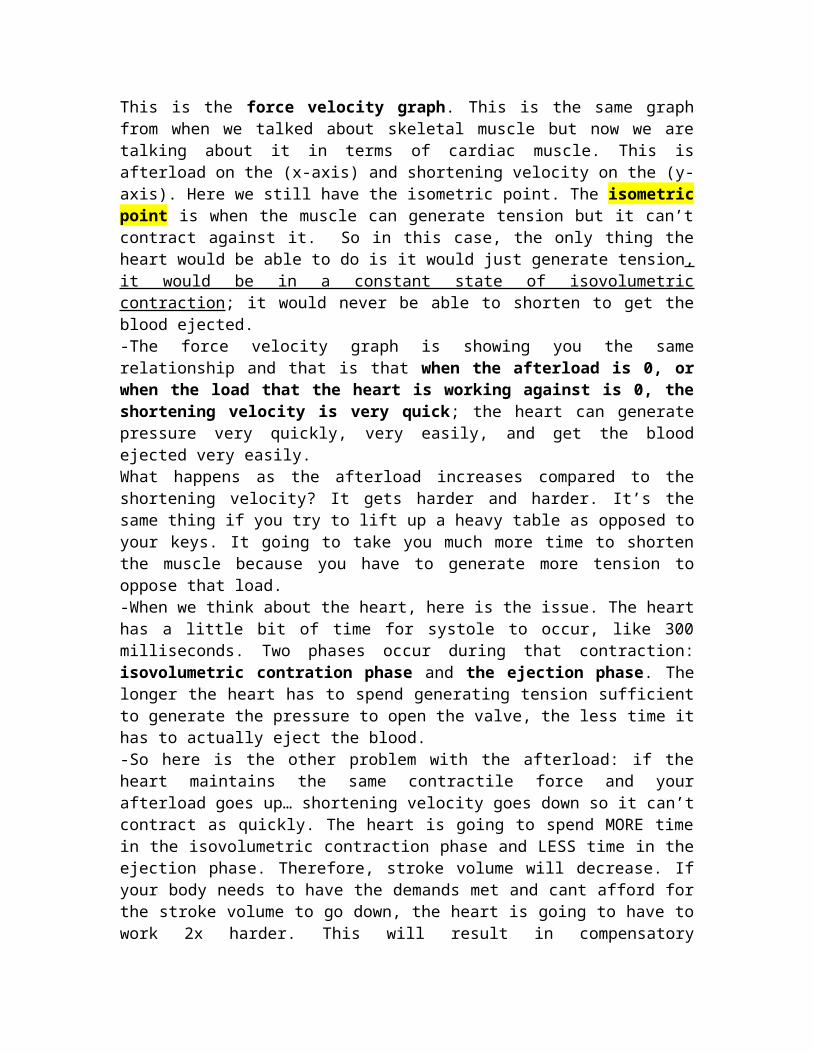
Afterload = the force the heart has to generate to get the blood out; its main determinant is total peripheral resistance. Force velocity graph
Hopefully you remember this graph. This is the force velocity graph. This is the same graph from when we talked about skeletal muscle but now we are talking about it in terms of cardiac muscle. This is
afterload on the (x-axis) and shortening velocity on the (y-axis). Here we still have the isometric point. The isometric point is when the muscle can generate tension but it can’t contract against it. So in this case, the only thing the heart would be able to do is it would just generate tension, it would be in a constant state of isovolumetric contraction; it would never be able to shorten to get the blood ejected.-The force velocity graph is showing you the same relationship and that is that when the afterload is 0, or when the load that the heart is working against is 0, the shortening velocity is very quick; the heart can generate pressure very quickly, very easily, and get the blood ejected very easily. What happens as the afterload increases compared to the shortening velocity? It gets harder and harder. It’s the same thing if you try to lift up a heavy table as opposed to your keys. It going to take you much more time to shorten the muscle because you have to generate more tension to oppose that load. -When we think about the heart, here is the issue. The heart has a little bit of time for systole to occur, like 300 milliseconds. Two phases occur during that contraction: isovolumetric contration phase and the ejection phase. The longer the heart has to spend generating tension sufficient to generate the pressure to open the valve, the less time it has to actually eject the blood. -So here is the other problem with the afterload: if the heart maintains the same contractile force and your afterload goes up… shortening velocity goes down so it can’t contract as quickly. The heart is going to spend MORE time in the isovolumetric contraction phase and LESS time in the ejection phase. Therefore, stroke volume will decrease. If your body needs to have the demands met and cant afford for the stroke volume to go down, the heart is going to have to work 2x harder. This will result in compensatory hypertrophy, but we can’t do it forever and over time the heart will start to fail.
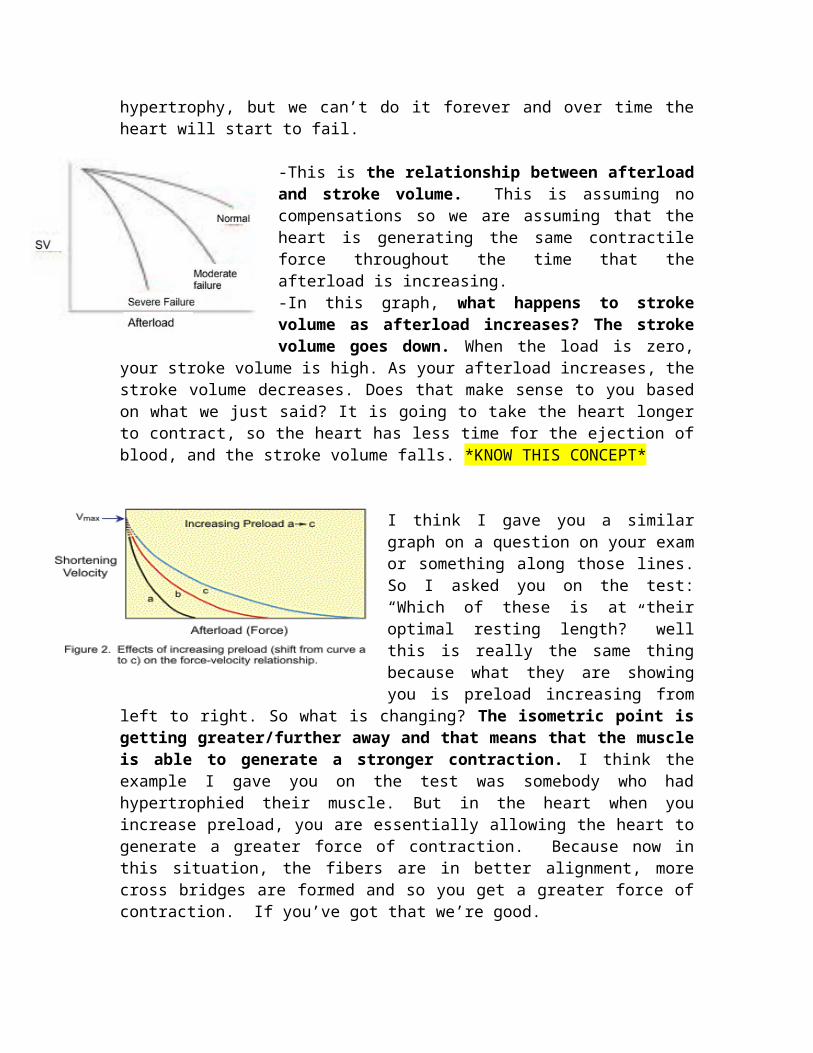
-This is the relationship between afterload and stroke volume. This is assuming no compensations so we are assuming that the heart is generating the same contractile force throughout the time that the afterload is increasing. -In this graph, what happens to stroke volume as afterload increases? The stroke volume goes down. When the load is zero, your stroke volume is high. As your afterload increases, the stroke volume decreases. Does that make sense to you based on what we just said? It is going to take
the heart longer to contract, so the heart has less time for the ejection of blood, and the stroke volume falls. *KNOW THIS CONCEPT*
I think I gave you a similar graph on a question on your exam or something along those lines. So I asked you on the test: “Which of these is at their optimal resting length?” well this is really the same thing because what they are showing you is preload increasing from left to right. So what is changing? The isometric point is getting greater/further away and
that means that the muscle is able to generate a stronger contraction. I think the example I gave you on the test was somebody who had hypertrophied their muscle. But in the heart when you
increase preload, you are essentially allowing the heart to generate a greater force of contraction. Because now in this situation, the fibers are in better alignment, more cross bridges are formed and so you get a greater force of contraction. If you’ve got that we’re good.
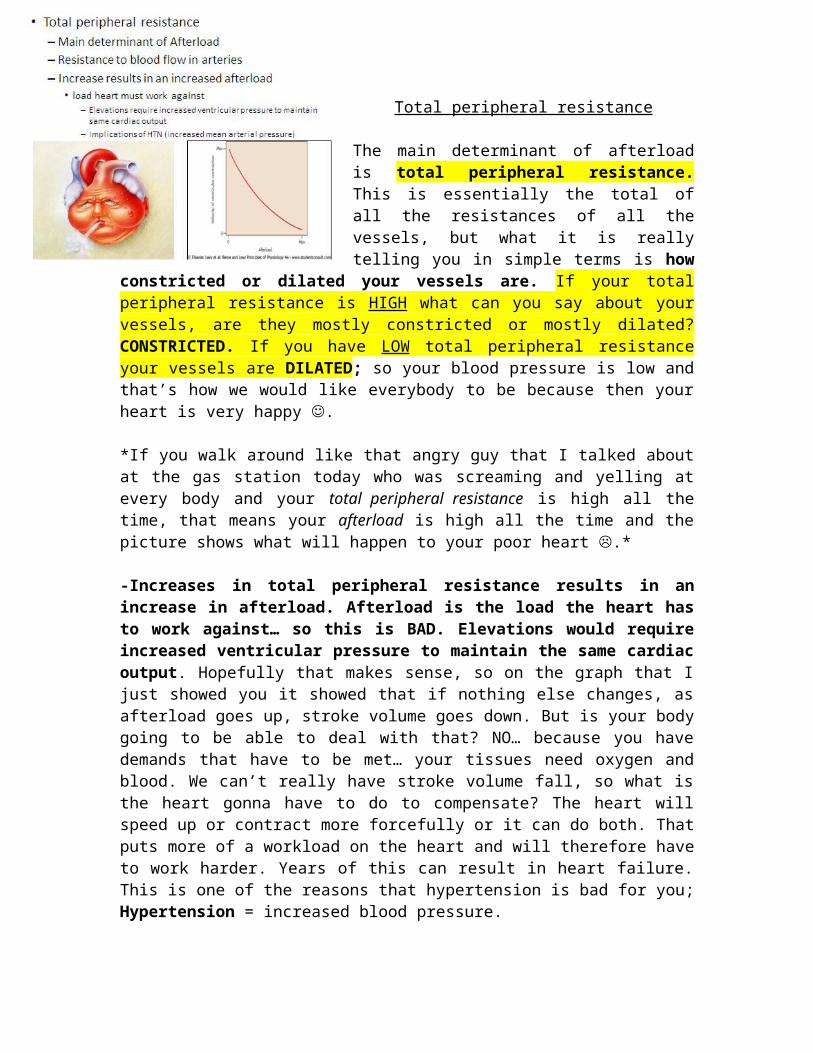
Total peripheral resistance
The main determinant of afterload is total peripheral resistance. This is essentially the total of all the resistances
of all the vessels, but what it is really telling you in simple terms is how constricted or dilated your vessels are. If your total peripheral resistance is HIGH what can you say about your vessels, are they mostly constricted or mostly dilated? CONSTRICTED. If you have LOW total peripheral resistance your vessels are DILATED; so your blood pressure is low and that’s how we would like everybody to be because then your heart is very happy .
*If you walk around like that angry guy that I talked about at the gas station today who was screaming and yelling at every body and your total peripheral resistance is high all the time, that means your afterload is high all the time and the picture shows what will happen to your poor heart .*
-Increases in total peripheral resistance results in an increase in afterload. Afterload is the load the heart has to work against… so this is BAD. Elevations would require increased
ventricular pressure to maintain the same cardiac output. Hopefully that makes sense, so on the graph that I just showed you it showed that if nothing else changes, as afterload goes up, stroke volume goes down. But is your body going to be able to deal with that? NO… because you have demands that have to be met… your tissues need oxygen and blood. We can’t really have stroke volume fall, so what is the heart gonna have to do to compensate? The heart will speed up or contract more forcefully or it can do both. That puts more
of a workload on the heart and will therefore have to work harder. Years of this can result in heart failure. This is one of the reasons that hypertension is bad for you; Hypertension = increased blood pressure.
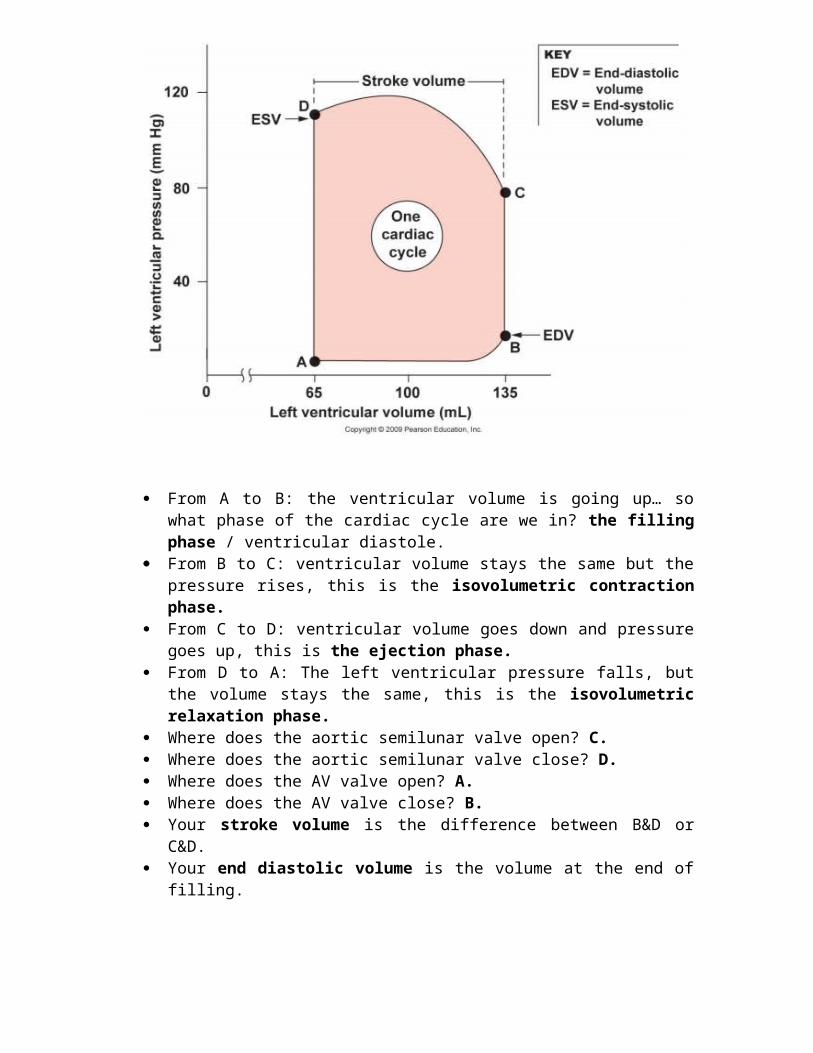
From A to B: the ventricular volume is going up… so what phase of the cardiac cycle are we in? the filling phase / ventricular diastole.
From B to C: ventricular volume stays the same but the pressure rises, this is the isovolumetric contraction phase.
From C to D: ventricular volume goes down and pressure goes up, this is the ejection phase.
From D to A: The left ventricular pressure falls, but the volume stays the same, this is the isovolumetric relaxation phase.
Where does the aortic semilunar valve open? C. Where does the aortic semilunar valve close? D. Where does the AV valve open? A. Where does the AV valve close? B. Your stroke volume is the difference between B&D or C&D. Your end diastolic volume is the volume at the end of filling.
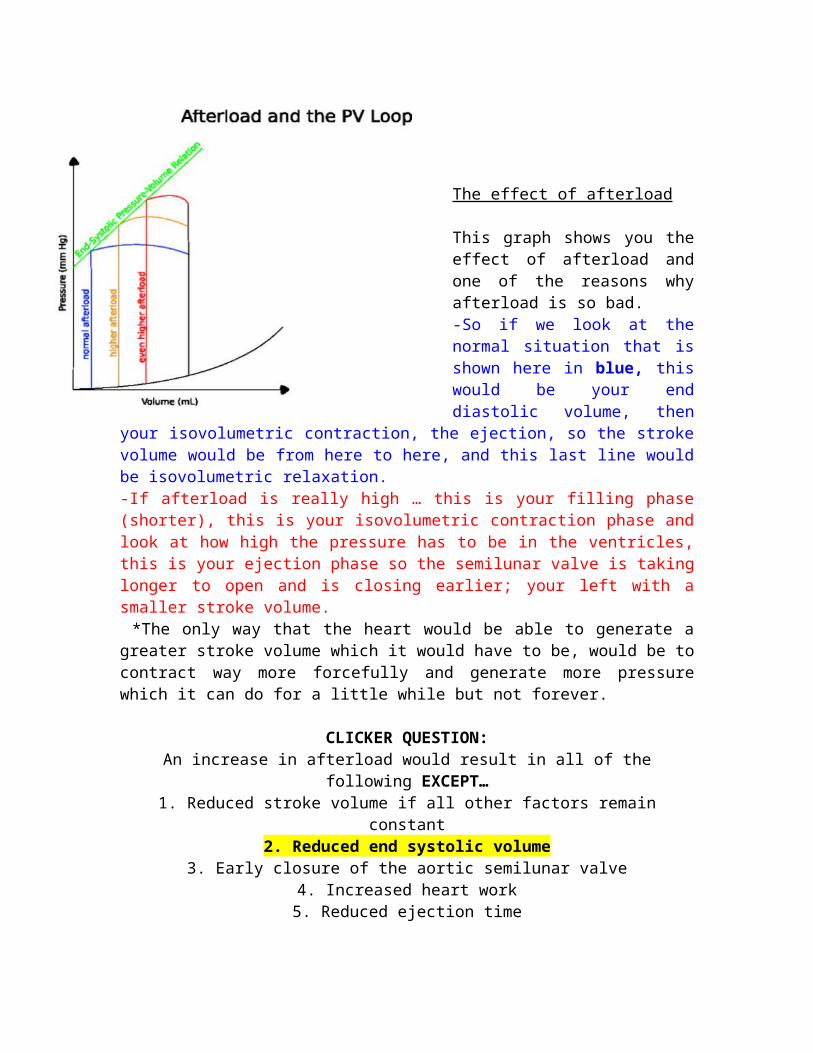
The effect of afterload
This graph shows you the effect of afterload and one of the reasons why afterload is so bad. -So if we look at the normal situation that is shown here in blue, this would be your end diastolic volume, then your isovolumetric contraction, the ejection, so the stroke volume would be
from here to here, and this last line would be isovolumetric relaxation. -If afterload is really high … this is your filling phase (shorter), this is your isovolumetric contraction phase and look at how high the pressure has to be in the ventricles, this is your ejection phase so the semilunar valve is taking longer to open and is closing earlier; your left with a smaller stroke volume. *The only way that the heart would be able to generate a greater stroke volume which it would have to be, would be to contract way more forcefully and generate more pressure which it can do for a little while but not forever.
CLICKER QUESTION:An increase in afterload would result in all of the following EXCEPT…
1. Reduced stroke volume if all other factors remain constant2. Reduced end systolic volume
3. Early closure of the aortic semilunar valve4. Increased heart work5. Reduced ejection time
EXPLANATION: 1. This is true. You will have a reduced stroke volume if you increase the afterload.
2. You would not have a reduced end systolic volume if you increase the afterload because
the blood is going to stay in the ventricle due to increased afterload. You would expect your end systolic volume to increase because you would
have more blood left in the ventricle.3. You will have early closure of the aortic semilunar valve based on the graph I just
showed you. The valve takes long to open and closes early.
4. You would have increased heart work.5. You would have reduced time for ejection.
Venous return
Venous return which is preload. The venous return is the blood coming back to the heart from the venous circulation so that is gonna affect the end diastolic volume because it directly gives rise to the EDV.
Venous pressure drives blood back to the heart (to be discussed). Venous pressure is fairly low but its turns out that the pressure in the small veins is greater than the pressure in the vena cava; that ends up driving flow back to the heart. Veins are thin walled structures. They exhibit a lot of compliance meaning they can distend/expand very easily. They are capacitance vessels because this distension allows them to kind of store a lot of blood; veins are holding a large fraction of the blood volume.
The veins hold 70% of blood volume in a resting individual. So while you are sitting here at rest, the majority of your blood volume is actually in your venous circulation. The mean venous pressure is very low about 2 mmHg; this is the average pressure across the venous circulation. It is a low-pressure low resistance pathway.
Arteries are resistance vessels. Arteries are a high-pressure high resistance pathway. The mean arterial pressure is high about 80-100 mmHg.*The difference of this high arterial pressure and low venous pressure is part of what helps drive the whole circuit because blood moves from high pressure to low pressure.
Factors that aid venous return:
When you think about it, it’s not a big deal to think about blood coming from the head to the heart because that’s easy... But if the veins have such low pressure, how do you get the blood from your feet back to your heart...Valves: veins have valves in them; that means that the blood can only move in one direction and it can only move back to the heart.Skeletal muscle pump: the veins sit in between the skeletal muscles and when you contract your skeletal muscles, the venous return is facilitated because the veins have valves and when the veins are squeezed the blood can only move back towards the heart.Respiratory pump: when you take a breath in your diaphragm flattens, right? So the contraction of the diaphragm flattening actually helps to squeeze on some of the veins in that area as well.Pressure gradient: blood moves from high pressure to low pressure. The pressure in the venules (the small veins right after you come from the capillaries then you enter these small veins), their pressure is about 10 mmHg; The pressure in the vena cava is only 1 mmHg. So that pressure gradient of 9 mmHg FAVORS blood flow back towards the vena cava.
Pressure gradient “story”:
So blood goes from the arteries arterioles capillaries the capillaries have an arteriole and venous side from the venous side of the capillary blood enters venules a.k.a small veins bigger veins vena cava. We are trying to get blood from the venules to the vena cava.
The reason the right atria becomes important is because the right atria is where the vena cava dump into. So that right atria vena cava junction… whatever the pressure is in the right atria it is very similar in the vena cava. So when I talk about right atrial pressure you can think of it as being the same as the pressure in the vena cava.
So if the pressure is 10mmHg here in the venules, and the pressure is 2 mmHg in the vena cava, how does that favor the movement of blood? Back towards the vena cava. You get it? When you breathe in, that lowers right atrial pressure, which also lowers the pressure in the vena cava. So if you take in a breath and instead of this being 2 mmHg now it is 1 mmHg, you have helped venous return because this pressure gradient is now greater.
The bigger this pressure gradient is, the more you are facilitating venous return. Here is the issue: if somebody has right-sided heart failure that’s when blood starts backing up in the ventricles, and then it backs up into the atria, and then its gonna back up into the vena cava… whats gonna happen to the pressure in the vena cava? It is gonna go up so if it goes up to 8 mmHg you will
reduce venous return. So anything that increases right atrial pressure impairs venous return or makes it difficult for that blood to make it back.
*** So we have valves so the blood can only move in one direction. We have a skeletal muscle pump which means as you contract your muscles the veins get compressed and that helps drive blood back to the heart. We have this pressure gradient, and again when you breathe in deeply, it decreases this right atrial pressure which facilitates venous return. The diaphragm also helps with venous return because when it flattens it squeezes the abdominal area and that helps to push blood back (Respiratory pump). ***
Exercise greatly increases venous return. When you exercise you’ve got skeletal muscle activity, you’re breathing deeply… all of those things together help to facilitate venous return. These factors help end diastolic volume go up because you mobilize a lot of that blood.
CLICKER QUESTION:Which of the following would reduce venous return?
1. Brisk walking2. Right sided heart failure
3. Increased pressure in venules4. Rapid and deep breathing
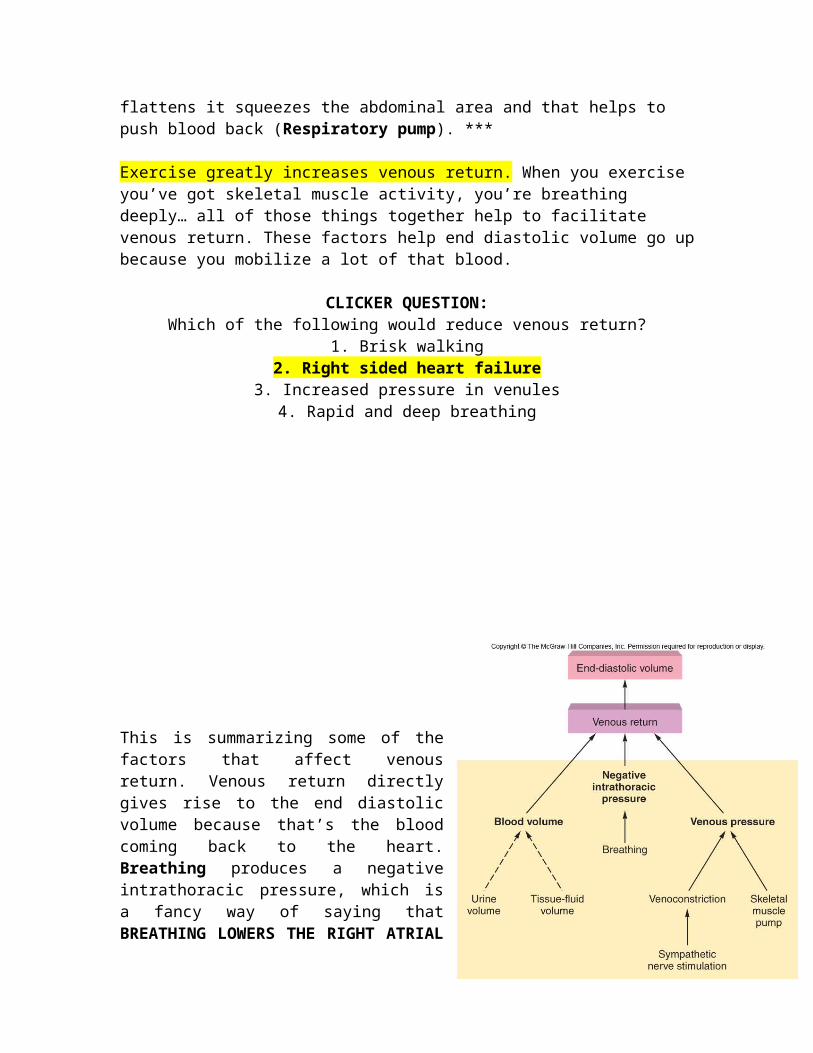
This is summarizing some of the factors that affect venous return. Venous return directly gives rise to the end diastolic volume because that’s the blood coming back to the heart. Breathing produces a negative intrathoracic pressure, which is a fancy way of saying that BREATHING LOWERS THE
RIGHT ATRIAL PRESSURE. The more blood volume you have, in most cases, the more your venous return will be because you’ve got more blood in the entire system. The skeletal muscle pump will increase venous pressure, constrict those vessels and cause the blood to move back towards the heart. Sympathetic nerve stimulation can also cause the veins to constrict; since the veins have valves in them when you squeeze them you move the blood back towards the heart.
Chemoreceptors
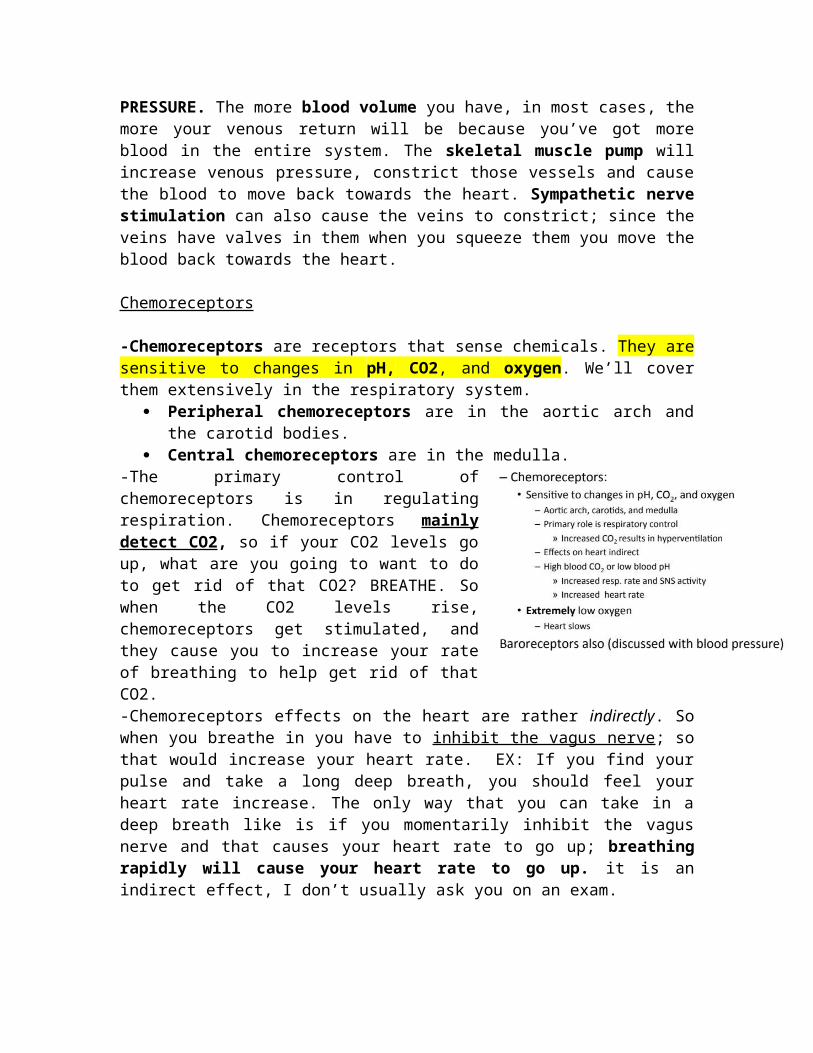
-Chemoreceptors are receptors that sense chemicals. They are sensitive to changes in pH, CO2, and oxygen. We’ll cover them extensively in the respiratory system.
Peripheral chemoreceptors are in the aortic arch and the carotid bodies.
Central chemoreceptors are in the medulla. -The primary control of chemoreceptors is in regulating respiration. Chemoreceptors mainly detect CO2, so if your CO2 levels go up, what are you going to want to do to get rid of that CO2? BREATHE. So when the CO2 levels rise, chemoreceptors get stimulated, and they cause you to increase your rate of breathing to help get rid of that CO2.-Chemoreceptors effects on the heart are rather indirectly. So when you breathe in you have to inhibit the vagus nerve; so that would increase your heart rate. EX: If you find your pulse and take a long deep breath, you should feel your heart rate increase. The only way that you can take in a deep breath like is if you momentarily inhibit the vagus nerve and that causes your heart rate to go up; breathing rapidly will cause your heart rate to go up. it is an indirect effect, I don’t usually ask you on an exam.-High blood CO2 or low blood pH will increase respiratory rate and will indirectly increase heart rate based on what we just spoke about.-EXTREMELY low oxygen (dangerously low, like you’re gonna die low oxygen), will slow the heart rate down.
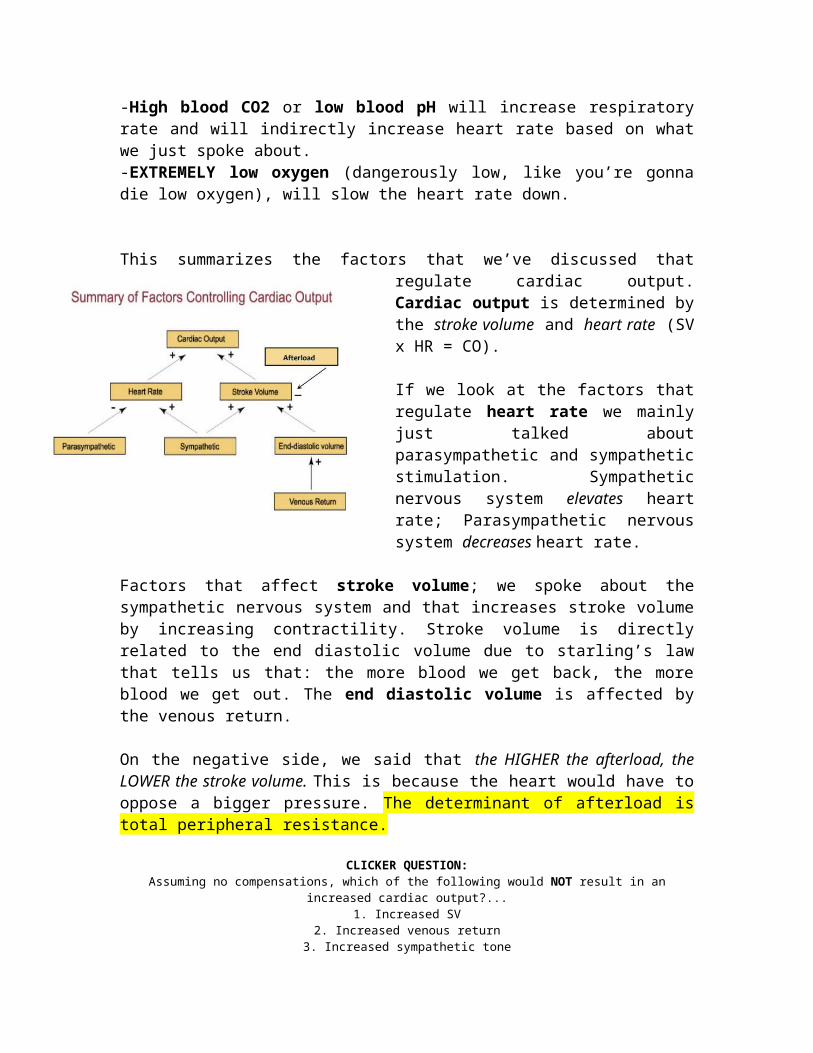
This summarizes the factors that we’ve discussed that regulate cardiac output. Cardiac output is determined by the stroke volume and heart rate (SV x HR = CO).
If we look at the factors that regulate heart rate we mainly just talked about parasympathetic and sympathetic stimulation. Sympathetic nervous system elevates heart rate; Parasympathetic nervous system
decreases heart rate.
Factors that affect stroke volume; we spoke about the sympathetic nervous system and that increases stroke volume by increasing contractility. Stroke volume is directly related to the end diastolic volume due to starling’s law that tells us that: the more blood we get back, the more blood we get out. The end diastolic volume is affected by the venous return.
On the negative side, we said that the HIGHER the afterload, the LOWER the stroke volume. This is because the heart would have to oppose a bigger pressure. The determinant of afterload is total peripheral resistance.
CLICKER QUESTION:Assuming no compensations, which of the following would NOT result in an increased cardiac
output?...1. Increased SV
2. Increased venous return3. Increased sympathetic tone
4. Increased total peripheral resistanceEXPLANATION: Increased total peripheral resistance would INCREASE afterload and
cardiac output would fall. Blood Pressure
Blood Volume
-Our blood pressure is affected by our blood volume. So when people have high blood pressure they tell them to maintain a low salt diet, because sodium increases your blood osmolarity and that will cause you to hold water in your blood stream which will increase your blood volume which will increase your blood pressure.
-Blood pressure is the force that the blood is exerting on the vessel walls. The more blood volume you have contained within that space the more pressure it’s going to be. -We are made up of 60% water:
2/3 of that water are found within cells. 1/3 of that water is found as extra
cellular fluid. o (80%) of it is interstitial fluido (20%) of that extra cellular fluid is
within our blood
Google says: “Interstitial fluid, also known as tissue fluid, is a liquid — made mostly of water — that fills up the space between the cells of most organisms.”
-Water moves pretty freely between compartments because we have aquaporins allover the place (water channels). If there is a difference in osmolarity between the interstitial space and cells, water will move to equilibrate that and it occurs very rapidly and it occurs until the osmolarity of both compartments are the same. It is the osmotic pressures and hydrostatic pressures that determine this.
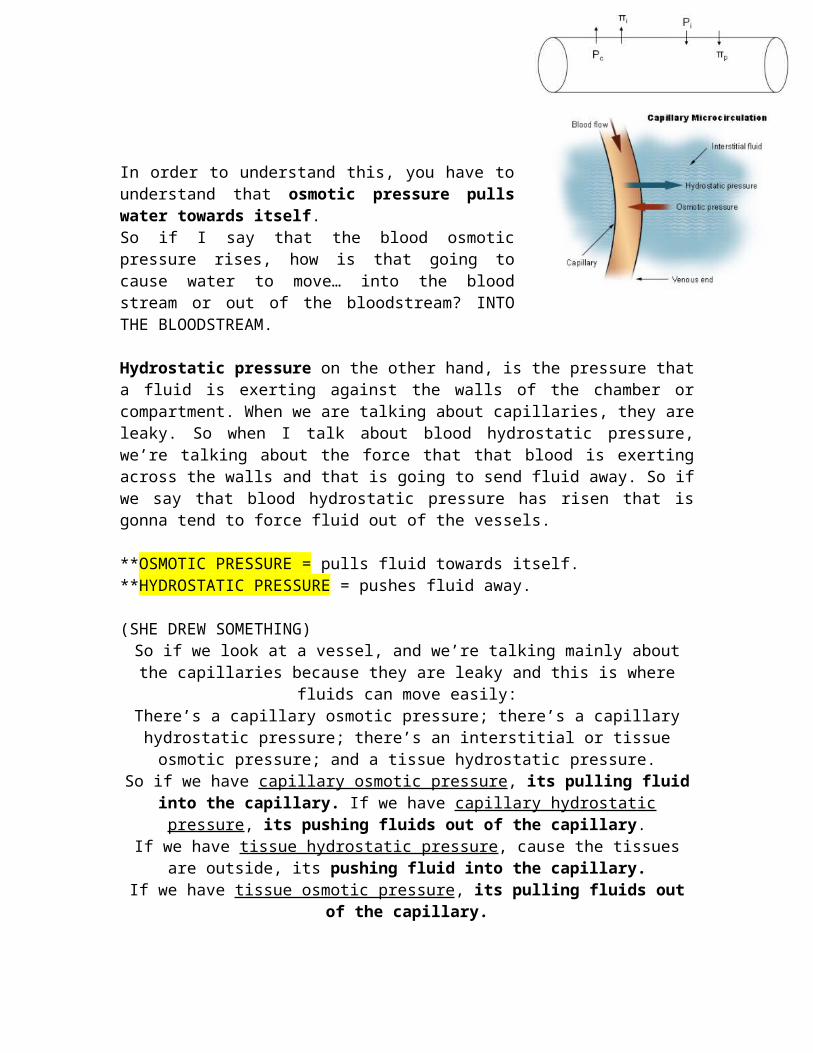
In order to understand this, you have to understand that osmotic pressure pulls water towards itself. So if I say that the blood osmotic pressure rises, how is that going to cause water to move… into the blood stream or out of the bloodstream? INTO THE BLOODSTREAM.
Hydrostatic pressure on the other hand, is the pressure that a fluid is exerting against the walls of the chamber or compartment. When we are talking about capillaries, they are leaky. So when I talk about blood hydrostatic pressure, we’re talking about the force that that blood is exerting across the walls and that is going to send fluid away. So if we say that blood hydrostatic pressure has risen that is gonna tend to force fluid out of the vessels.
**OSMOTIC PRESSURE = pulls fluid towards itself.**HYDROSTATIC PRESSURE = pushes fluid away.
(SHE DREW SOMETHING)So if we look at a vessel, and we’re talking
mainly about the capillaries because they are leaky and this is where fluids can move easily:There’s a capillary osmotic pressure; there’s a
capillary hydrostatic pressure; there’s an interstitial or tissue osmotic pressure; and a
tissue hydrostatic pressure.So if we have capillary osmotic pressure, its pulling fluid into the capillary. If we have capillary hydrostatic pressure, its pushing
fluids out of the capillary.If we have tissue hydrostatic pressure, cause the tissues are outside,
its pushing fluid into the capillary.If we have tissue osmotic pressure, its pulling fluids out of the
capillary.
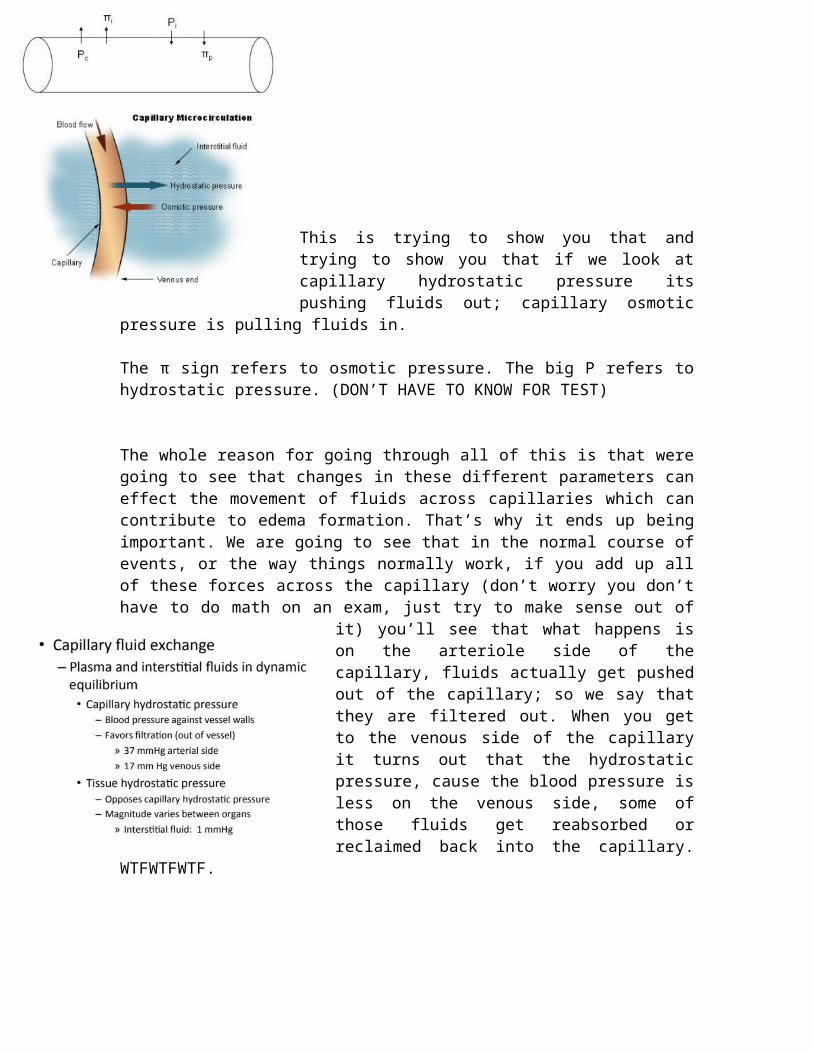
This is trying to show you that and trying to show you that if we look at capillary hydrostatic pressure its pushing fluids out; capillary osmotic pressure is pulling fluids in.
The π sign refers to osmotic pressure. The big P refers to hydrostatic pressure. (DON’T HAVE TO KNOW FOR TEST)
The whole reason for going through all of this is that were going to see that changes in these different parameters can effect the movement of fluids across capillaries which can contribute to edema formation. That’s why it ends up being important. We are going to see that in the normal course of events, or the way things normally work, if you add up all of these forces across the capillary (don’t worry you don’t have to do math on an exam, just try to make sense out of it) you’ll see that what happens is on the arteriole side of the capillary, fluids actually get pushed out of the capillary; so we say that they are filtered out. When you get to the venous side of the capillary it turns out that the hydrostatic pressure, cause the blood pressure is less on the venous side, some of those fluids get reabsorbed or reclaimed back into the capillary. WTFWTFWTF.
The plasma and interstitial fluids are in dynamic equilibrium that means that these forces can cause fluids to move until everything kind of equilibrates.
Capillary hydrostatic pressure = the blood pressure against the vessel walls. It favors filtration or the movement of fluids out of the vessel.
Pressure is higher on the arterial side and lower on the venous side.As we go from the arteriole side of the capillaries to the venous side of the capillaries, this
hydrostatic pressure falls that’s because blood pressure in general falls as you move from arteries to veins.
Tissue hydrostatic pressure = the magnitude varies between organs but it is usually very, very low. That is because there aren’t many plasma proteins out there or any proteins to contribute to it.
Colloid osmotic pressure is the osmotic pressure of the blood; It is the osmotic
pressure that is exerted by the plasma proteins.
Interstitial osmotic pressure = the osmotic pressure of the interstitial space; it is also called tissue osmotic pressure.
The net filtration pressure will determine how fluids move. The forces that are pushing fluids out of the vessel are the capillary hydrostatic pressure and the interstitial osmotic pressure. The forces that are holding fluids into the vessel are the capillary osmotic pressure and the interstitial hydrostatic pressure. The way that you figure out if fluids are
being filtered/pushed out of the capillary or if they are being absorbed/coming back in, is by adding up all these forces.
EX (just for clarification):
With these pressures we want to know are fluids being filtered out of the capillary or are they being resorbed by the capillary. So how do you do it. You figure out which are holding fluids in the capillary and which are pulling fluids out of the capillary and then you just add them up.Capillary hydrostatic pressure: 10 (OUT)
Capillary osmotic pressure: 15 (IN)Tissue hydrostatic pressure: 30 (IN)Tissue osmotic pressure: 12 (OUT)
45 mmHg favoring reabsorption (pulling fluids in)22 mmHg favoring filtration (pushing fluids out) How are fluids moving? Into the vessel with a reabsorption pressure of 23 mmHg. (45-22 =23) If both numbers were the same then there would be no fluid movement and everything is at equilibrium because everything would be balanced.
This is showing you what the numbers actually are in the body. In a normal individual, on the
arterial side of the capillary, we have the capillary hydrostatic pressure at 37 mmHg. The interstitial osmotic pressure is 0. Then we have the forces holding fluids into the capillary so the capillary osmotic pressure is 25 mmHg and the hydrostatic pressure of the interstitial space is 1 mmHg. This is all on the arterial side.
When we get to the venous side, everything is exactly the same except the capillary hydrostatic pressure, instead of being 37 mmHg, is only 17 mmHg here. So if we calculate the net filtration pressure here for the arterial side, we find that we have more forces pushing fluids out on the arterial side; and the difference between them is 11 mmHg. So we have a net filtration pressure (fluids are moving out of the capillary) of 11mmHg.
If we then add up the pressures on the venous side of the capillary (again: everything here is the same, but the hydrostatic pressure of the blood is less) we find out that in that case we have more forces holding fluids in, and we call it a reabsorption pressure of 9 mmHg.
So what this tells us is that as fluids move from the arterial side of the capillary to the venous side, the following happens: fluids are
filtered out on the arterial side, and they are then reclaimed on the venous side. So that’s good because if everything was just filtered, what would happen if we didn’t bring it back? You would have accumulation of interstitial fluid, which is EDEMA (bad). However, this reabsorption that occurs on the venous side is not 100%; the venous side doesn’t reabsorb 100% of the fluids that were filtered on the arterial side of the capillary; the venous side takes up 85% of what is filtered. The remaining 15% is picked up by the lympathics, which enters the lympathic circulation and ultimately dumps into the bloodstream.
***SO WHAT YOU NEED TO KNOW FOR ME FOR THIS***
IF WE CHANGE ANY ONE OF THESE FORCES, HOW DOES IT AFFECT THE MOVEMENT OF FLUIDS?
So if capillary hydrostatic pressure would rise… what would that do?
Push water out, so that would favor filtration; that would favor edema formation.
If capillary osmotic pressure were to rise, that would inhibit edema formation.
If tissue hydrostatic pressure were to rise, that would also inhibit edema formation.
If tissue osmotic pressure were to rise, that would favor edema formation.
CLICKER QUESTION:An increase in capillary hydrostatic pressure would…
1. Increase capillary filtration2. Decrease capillary filtration3. No effect capillary filtration
EXPLANATION: Capillary hydrostatic pushes away so it would increase capillary filtration. That would favor edema because you are putting it out into the interstitial
space.
CLICKER QUESTION:An increase in capillary osmotic pressure would be expected to…
1. Increase capillary filtration2. Decrease capillary filtration
3. No effect capillary filtrationEXPLANATION: Decrease it and that would inhibit edema formation.
CLICKER QUESTION:
Liver failure would be expected to result in which of the following…
1. Increase blood volume2. Result in interstitial fluid
accumulation3. Increase blood clotting
4. Increase blood hydrostatic pressure
EXPLANATION: It would result in interstitial fluid accumulation but why, what is it changing? Low albumin, which lowers the blood
osmotic pressure. The capillary osmotic pressure would decline; so you would have fluids exiting which would favor edema formation in the interstitial space.
This we said:Fluids leave the aterial end via filtration, and are returned on the venous side; This is due to reduction of the hydrostatic pressure. In other words, the capillary hydrostatic pressure declines as you go from the arterial side of the capillary to the venous side of the capillary.
I said to you that this allows for the reclamation of 85% of the fluids that are filtered, but it doesn’t get all of them and we need to get all of them otherwise we are going to have edema formation, so the lympathics pick up the remaining 15%.
Lymphatic capillaries are what pick up that interstitial fluid. Once it gets into the lymphatic system we call it lymph.
This slide is about the lympathic system. She read it word for word; just know the slide.
This is showing you these lymphatic capillaries. They kind of intersperse themselves amongst the capillary beds. Hopefully that makes sense to you because we said that this is where the filtration is occurring, so we need them out here to be able to pick up that filtrate.
This is trying to show you the organization or kind of how they are able to do this. These lymphatic capillaries have these valves in them. So the way that it works is that when fluid starts to accumulate out here, it will come in through these valves and then as this vessel get full, it will pinch the valve closed so that they don’t take anymore until that moves forward.
The lymphatic ducts is a merging of lymph capillaries. I’m not gonna ask you about that cause its anatomy. All these lymphatic vessels are doing is their taking that interstitial fluid that was filtered that wasn’t able picked
up/absorbed and is ultimately returning it back to the bloodstream.
<<<<<< FOR YOUR INFO.
Related Documents











