EVIDENCIA Y EXPERIENCIA CON ERIBULINA EN CÁNCER DE MAMA METASTÁSICO Dra. Noelia Martínez Jáñez Hospital Ramón y Cajal

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EVIDENCIA Y EXPERIENCIA CON ERIBULINA EN CÁNCER DE MAMA METASTÁSICO
Dra. Noelia Martínez JáñezHospital Ramón y Cajal

INTRODUCCIÓN

BREAST CANCER IS THE MOST DIAGNOSED AND LEADING CAUSE OF CANCER DEATH IN EUROPEAN WOMEN
Accounts for 30% of new cancer cases and 17% of cancer deaths in European women
Ferlay J, Parkin D et al. Eur J Cancer. 2010;46:765–781
Incidence Mortality
Estimated number of cases, women, thousands (Europe, 2008)

EPIDEMIOLOGÍA DEL CÁNCER DE MAMA EN ESPAÑA
27.500 cs/año50,9 cs/100.000 hab/año
↓ 1-3 % anual~ 6300 / año
INCIDENCIA
PREVALENCIA
MORTALIDAD
Factores ambientales
Dco precozRecursos dcos y terapeúticos
Supervivencia a 5 años: 83%100.000 pats ?
1990 2000 2010

CÁNCER DE MAMA AVANZADO: AÚN UN PROBLEMA CLÍNICO
Enfermedad localizada
1ª L
R.I.P.
2ª L
3ª L
4ª L
5ª L
6ª L
7ª L………nª L
Enfermedad avanzada
Enfermedad avanzada
Enfermedad avanzada
Enfermedad avanzada
Enfermedad avanzada
Enfermedad avanzada
Enfermedad avanzada
Adyuvancia
NeoadyuvanciaCURACIÓN
2,5 años
20-50%6-10%

AVANCE DE TRATAMIENTOS
Pre-anthracyclines● CMF, CMFVP
Anthracyclines● Combinations
– AC, FAC, AVCMF, FEC, CEF
● Sequence and alternating, dose intensity, dose density, high-dose chemotherapy
Taxanes (paclitaxel/docetaxel)● Integration in chemotherapy strategies
New Agents (gemcitabine, capecitabine, ixabepilone*, eribulin)● Sequential monotherapy
● Combinations
Biological modifiers (trastuzumab, bevacizumab, lapatinib)● Integration in chemotherapy strategies
A = doxorubicin; C = cyclophosphamide; E = epirubicin; F = 5-fluorouracil; M = methotrexate; MBC = metastatic breast cancer; P = prednisone; V = vincristineGiordano S, Buzdar A et al. Cancer. 2004;100:44–52; US Food and Drug Administration. What's new from the Office of Hematology Oncology Products. 2011
1970s
1980s
1990s
2000s
*Not approved in EU (approved in Switzerland)

ERIBULINA

A Phase III, Open-label, Randomized, Multicenter Study Of Eribulin Mesylate Versus Capecitabine In Patients With Locally Advanced Or Metastatic Breast Cancer Previously Treated With Anthracyclines And Taxane

INTRODUCCIÓN MECANISMO DE ACCIÓN

¿QUE ES LA ERIBULINA?
* Eribulin = E7389 = ER-086526 = B1939 = NSC 707389
Halichondria okadai

MECANISMO DE ACCIÓN
Growing microtubule
Shortening microtubule
MicrotubulePolymerization
MTOC
Eribulin has no effect on microtubule shortening
2
Eribulin Eribulin inhibits microtubule growth1
3 Eribulin causes globular tubulin aggregates
Eribulin
Globular tubulin aggregates
MicrotubuleDepolymerization
MicrotubuleDynamics
MTOC

MECANISMO DE ACCIÓN
Growing microtubule
Shortening microtubule
MicrotubulePolymerization
MTOC
Eribulin has no effect on microtubule shortening
2
Eribulin Eribulin inhibits microtubule growth1
3 Eribulin causes globular tubulin aggregates
Eribulin
Globular tubulin aggregates
MicrotubuleDepolymerization
MicrotubuleDynamics
MT drawing created by M. Asada, TRL, Eisai; later adapted by B. Littlefield, ERI Jordan et al., 2005)

ESTUDIOS CLÍNICOS



EMBRACE STUDY DESIGN
• Locally recurrent or MBC• 2-5 prior chemotherapies
• Progression ≤6 months of last chemotherapy
• Neuropathy ≤grade 2• ECOG ≤2
Eribulin mesylate1.4 mg/m2, 2-5 min IV
Day 1, 8 q21 days
Treatment of Physician’s Choice (TPC)
Any monotherapy (chemotherapy, hormonal, biological)* or
supportive care only†
Randomization 2:1
• PFS• ORR• Safety
• Overall survival
Primary endpoint
Secondary endpoints
Stratification:– Geographical region, prior capecitabine, HER2/neu status
Global, randomized, open-label Phase III trial (Study 305)
Patients (N=762)
− ≥2 for advanced disease− Prior anthracycline and
taxane
* Approved for treatment of cancer†Or palliative treatment or radiotherapy administered according to local practice, if applicableECOG, Eastern Cooperative Oncology Group; IV, intravenous; PFS, progression-free survival; HER2/neu, human epidermal growth factor receptor 2
THE PRIMARY ENDPOINT : OVERALL SURVIVAL
Progression-free survival
● Protocol pre-specified
● Assessed from randomisation to the earliest date of progression or death (or censored as per OS)
● Stratified log-rank (ITT and PP population)
Tumour response
● ORR and DOR were protocol pre-specified, CBR was not
● Tumour response was assessed using RECIST every 8 weeks (+1 week) until progression
● Investigator and independent review
● ORR assessed using exact Pearson Clopper two-sided 95% CI in patients with measurable disease per RECIST(version 1.0)
Overall survival
● Primary analysis planned at 411 (50%) events (but actually took place at 422 (55%) events)– Updated analysis conducted at 589 (77%)
events
● Determined from date of randomisation to death, or last date known alive (censored)
● Stratified log-rank by randomisation parameters (ITT population)
Safety
● Assessed according to NCI CTCAE criteria (version 3.0)
18
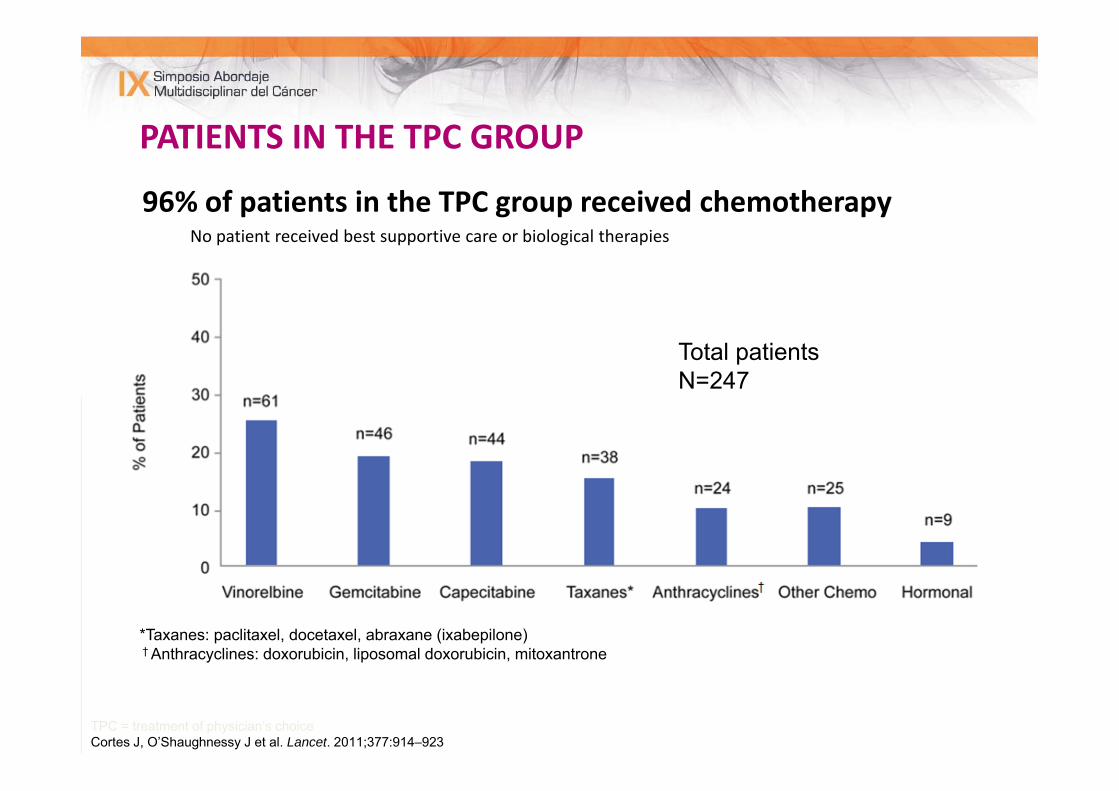
PATIENTS IN THE TPC GROUP
96% of patients in the TPC group received chemotherapyNo patient received best supportive care or biological therapies
*Taxanes: paclitaxel, docetaxel, abraxane (ixabepilone)† Anthracyclines: doxorubicin, liposomal doxorubicin, mitoxantrone
TPC = treatment of physician’s choiceCortes J, O’Shaughnessy J et al. Lancet. 2011;377:914–923
Total patients N=247

Eribulin n=508
TPC n=254
TotalN=762
Median age, years (range) 55 (28–85) 56 (27–81) 55 (27–85)
Ethnic origin, %
White 93 92 92
Black 4 6 4
Asian/Pacific Islander 1 1 1
Other 3 2 3
Geographical region, %
Region 1. North America, Western Europe, Australia 64 64 64
Region 2. Eastern Europe, Russia 25 25 25
Region 3. Latin America, South Africa 11 11 11
ECOG PS, %
0 43 41 42
1 48 50 49
2 8 9 8
BASELINE CHARACTERISTICS

TUMOUR CHARACTERISTICSEribulinn=508
TPCn=254
Total N=762
ER/PgR status, %
ER and/or PgR+ 64 64 64
ER and/or PgR- 24 25 25
ER/PgR/HER-2 negative, % 18 20 19
HER-2 status, %
Negative 73 76 74
Positive 16 16 16
Number of organs involved, %
1 17 14 16
2 34 32 33
3 29 30 29
≥4 20 24 22
Most common metastatic sites, %
Bone 60 62 61
Liver 58 63 60
Lymph nodes 43 46 44
Lung 39 37 38

PRIOR CHEMOTHERAPY REGIMENS
Eribulin, % n=508
TPC, %n=254
Total, % N=762
Number of prior chemotherapy regimens*1 <1 0 <1
2 13 12 13
3 35 33 34
4 (median) 33 31 32
5 17 20 18
>6 3 4 3
Prior capecitabine, % 73 74 73
*Received for the treatment of locally recurrent or metastatic breast cancer
TPC = treatment of physician’s choiceCortes J, O’Shaughnessy J et al. Lancet. 2011;377:914–923

MEDIAN DURATION OF ERIBULIN TREATMENT
Eribulinn=503
TPC Chemotherapy
n=238
Drug exposureMedian duration of exposure, months (range)≥5 cycles, % (range)
3.9 (0.7–16.3) 59 (1–23)
2.1 (0.03–21.2)NA
Dose interruptions, %Dose delays, %Dose reductions, %
64929
94126
Patients were treated with eribulin or TPC until disease progression, unacceptable toxicity, patient/physician request to discontinue or serious protocol non‐compliance
NA = not applicable; TPC = treatment of physician’s choiceCortes J, O’Shaughnessy J et al. Lancet. 2011;377:914–923
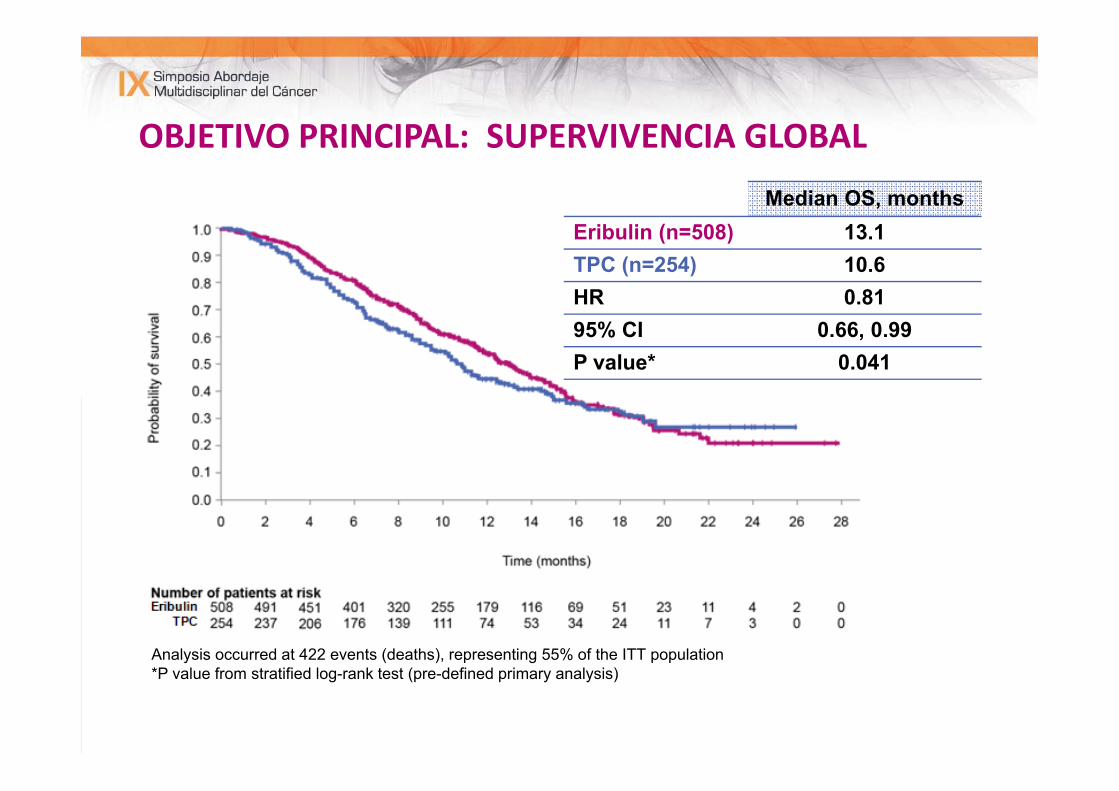
OBJETIVO PRINCIPAL: SUPERVIVENCIA GLOBAL
Analysis occurred at 422 events (deaths), representing 55% of the ITT population*P value from stratified log-rank test (pre-defined primary analysis)
Median OS, monthsEribulin (n=508) 13.1TPC (n=254) 10.6HR 0.8195% CI 0.66, 0.99P value* 0.041

UPDATED OS ANALYSIS : 75% PATIENTS
Analysis occurred at 589 events (deaths), representing 77% of the ITT population*Nominal P value from stratified log-rank test
Median OS, monthsEribulin (n=508) 13.2TPC (n=254) 10.5HR 0.8195% CI 0.67, 0.96P value* 0.014

SURVIVAL BENEFIT WITH ERIBULIN VS TPC
≤3 chemotherapy regimens previously
received
>3 chemotherapy regimens previously
receivedOS, months (95% CI)
Eribulin-treated patients13.3
(12.0, 14.9)n=362
11.7(9.3, 12.5)
n=106
TPC-treated patients10.7
(9.3, 12.5])n=162
10.0(6.3, 18.0])
n=51
Median survival difference, months 2.6 1.7
P value 0.039 0.607
Hazard ratio (95% CI) 0.774(0.606, 0.988)
0.899(0.600, 1.348)

OBJETIVO SECUNDARIO: SLP
● PFS (PP population) was longer with eribulin vs TPC, reaching statistical significance by both independent (P=0.02) and investigator review (P<0.001)
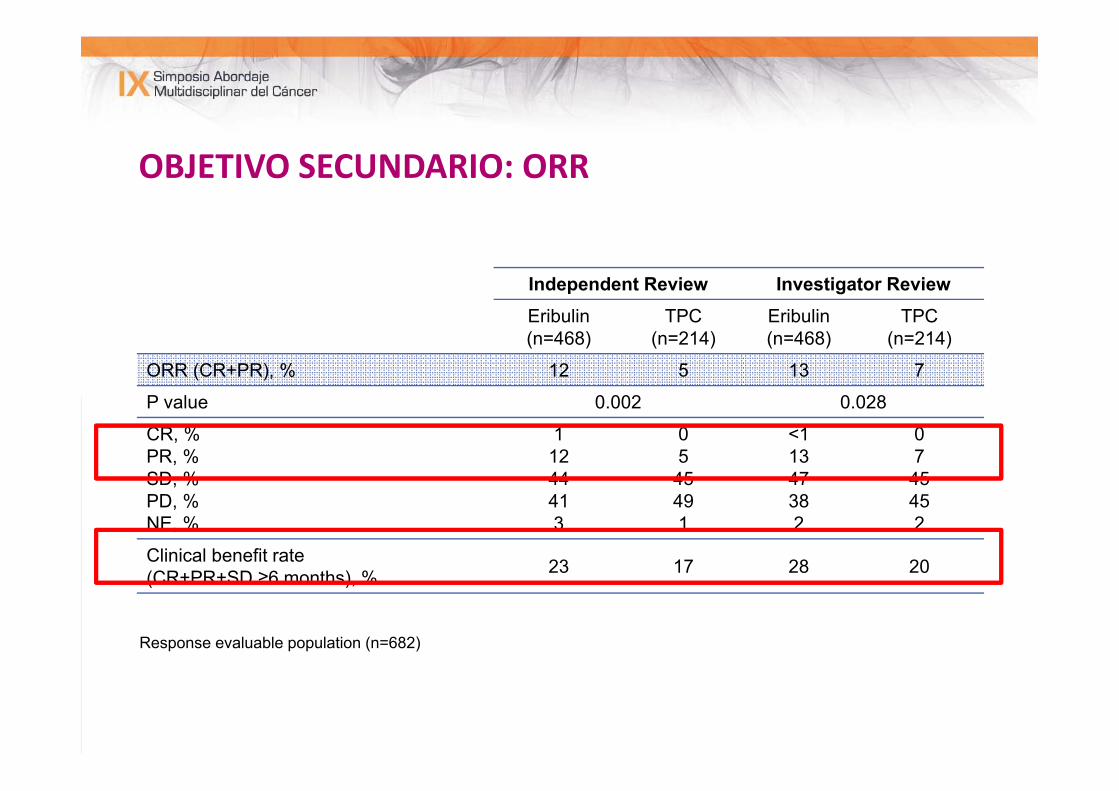
OBJETIVO SECUNDARIO: ORR
Independent Review Investigator ReviewEribulin (n=468)
TPC(n=214)
Eribulin (n=468)
TPC(n=214)
ORR (CR+PR), % 12 5 13 7
P value 0.002 0.028
CR, %PR, %SD, %PD, %NE, %
11244413
05
45491
<11347382
07
45452
Clinical benefit rate (CR+PR+SD ≥6 months), % 23 17 28 20
Response evaluable population (n=682)

OVERALL INCIDENCE OF ADVERSE EVENT
AE, % Eribulin(n=503)
TPC(n=247)
All AEs 99 93
Serious AEs 25 26
AEs leading to
interruption 5 10
discontinuation 13 15
dose reduction 17 16
dose delay 35 32
Fatal AEs 4 7
Fatal AEs (treatment-related) 1 1

HAEMATOLOGICAL ADVERSE EVENT
• Febrile neutropenia occurred with eribulin (5%) and TPC (2%)• Neutropenia was managed with dose delays, dose reductions and G‐
CSF • Administration of prophylactic G‐CSF was not permitted in the study• <1% of eribulin patients discontinued treatment due to
haematological AEs
Eribulin (n=503) TPC (n=247)All
Grades Grade 3 Grade 4 All Grades
Grade 3 Grade 4
Haematological, %
Neutropenia 52 21 24 30 14 7
Leucopenia 23 12 2 11 5 1
Anaemia 19 2 <1 23 3 <1
Cortes J, O’Shaughnessy J et al. Lancet. 2011;377:914–923

NON‐HAEMATOLOGICAL ADVERSE EVENTS
Eribulin (n=503) TPC (n=247)
All Grades Grade 3 Grade 4 All Grades Grade 3 Grade 4
Non-haematological, %
Asthenia/fatigue 54 8 1 40 10 0
Alopecia* 45 N/A N/A 10 N/A N/A
Nausea 35 1 0 28 2 0
Peripheral neuropathy† 35 8 <1 16 2 0
Constipation 25 1 0 21 1 0
Arthralgia/myalgia 22 <1 0 12 1 0
Pyrexia 21 <1 0 13 <1 0
Weight decrease 21 1 0 14 <1 N/A
Cortes J, O’Shaughnessy J et al. Lancet. 2011;377:914–923
CONCLUSIONES
– La eribulina mejora la SG de forma significativa, en las mujeres pretratados de CBM en comparación con otra citotóxica disponible.
– El beneficio parece mayor, en los pacientes que han recibido menos regimenes de QT.
– EL perfil de toxicidad es manejable y AES son los comúnmente asociados con la quimioterapia
La dosis recomendada de eribulina como la solución 1.23mg/m2 (equivalente al mesilato de eribulina 1.4 mg/m2)
días 1-8/21 días


CASO CLÍNICO
• 65 años .
• Abril 1995
•CDI pT1b pNo(0/13)M0. HR negativos. •SEGUIMIENTO
CASO CLÍNICO
HERCEPTIN 1 año
•Octubre 2003: Recaída supraclavicular izquierda
•Septiembre 2008: Progresión ósea
DOCETAXEL- XELODA 6 meses → Xeloda + zometa
• Agosto 2009: RECAIDA HEPÁTICA Y PG ÓSEA
• Octubre 2009:
CASO CLíNICO
Paclitaxel 150 mg/m2 + gPaclitaxel 150 mg/m2 + gGemcitabina 1500 mg/m2 + Bevacizumab 7.5 mg/kg
ZOMETA
Myocet 60 mg/m2 +Gencitabina 1500 mg/m2 + Bevacizumab 7.5 mg/kg
ZOMETA
3 meses…Tto de mantemimiento:
Avastin+zometa+arimidex+zoladex

• Marzo 2011: PG hepática.
• Junio 2011: PG Hepática
CASO CLÍNICO
ILP 13 meses: TAMOXIFENO
CDDP‐VINORELBINA

CASO CLíNICO
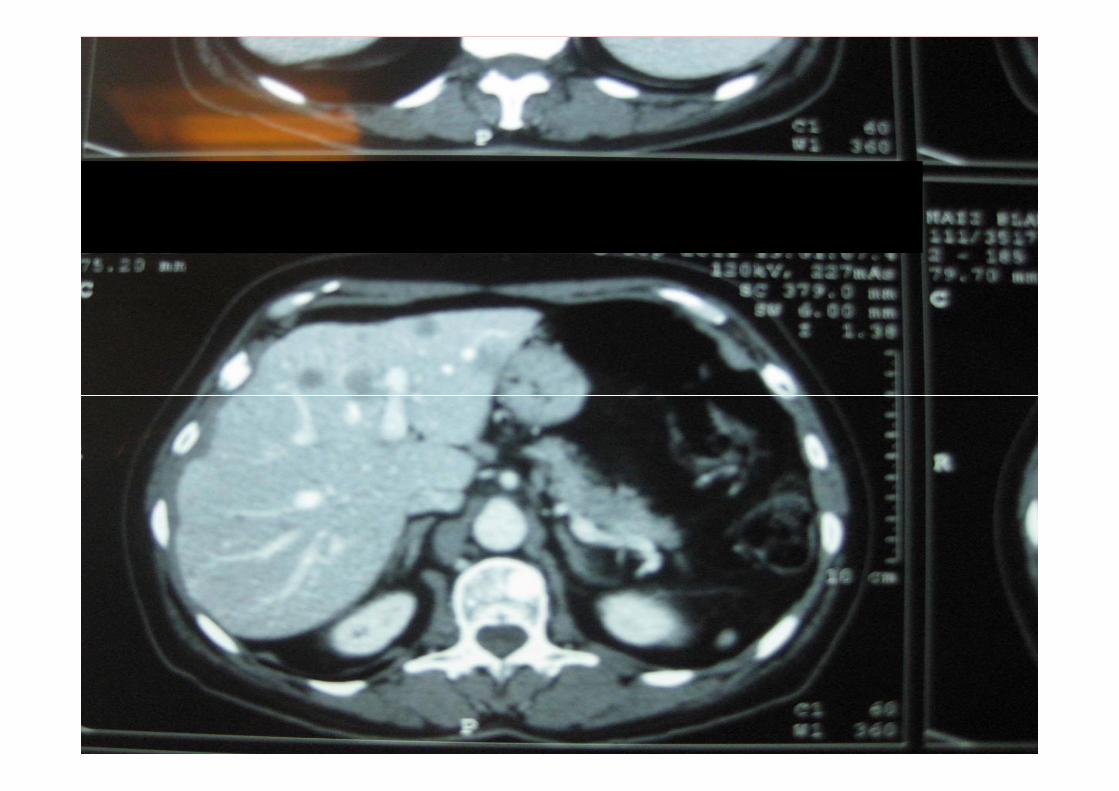

7º Línea
Tras 3 ciclos….




CASO CLÍNICO• Tras 7 meses de tratamiento… nueva progresión hepática en Abril 2012 hepática…

EXPERIENCIA EN EL H. RAMÓN Y CAJAL‐20 pacientes: >3º línea. Media 4‐8 líneas.‐Respuestas parciales o EE, con una media duración de 6 meses.
‐ EXCELENTE TOLERANCIA:‐ Astenia grado I‐ Neuropatía sensitiva a partir del 4‐5º ciclo REVERSIBLE.
‐ Neutropenia grado I ó II, tras 1º parte: 1 vial G‐CSF día +3.




A Phase III, Open-label, Randomized, Multicenter Study Of Eribulin Mesylate Versus Capecitabine In Patients With
Locally Advanced Or Metastatic Breast Cancer Previously Treated With
Anthracyclines And TaxanesPeter A. Kaufman,1 Ahmad Awada,2 Christopher Twelves,3
Louise Yelle,4 Edith A. Perez,5 Jantien Wanders,6Martin S. Olivo,7 Yi He,7 Corina E. Dutcus,7 Javier Cortes8
1Norris Cotton Cancer Center, Dartmouth-Hitchcock Medical Center, Lebanon, NH, USA; 2Medical Oncology Clinic, Jules Bordet Institute, Brussels, Belgium; 3Leeds Institute of
Molecular Medicine and St James’s Institute of Oncology, Leeds, UK; 4Department of Medicine, University of Montreal, Montreal, Canada; 5Mayo Medical Clinic, Jacksonville, FL, USA;
6Eisai Ltd, Hatfield, UK; 7Eisai Inc., Woodcliff Lake, NJ, USA; 8Vall D’Hebron University Hospital, Barcelona, Spain

STUDY RATIONALE
• Capecitabine is a widely used therapy in MBC, including 1st‐, 2nd‐ and 3rd‐line setting for MBC• Approved for the treatment of patients with MBC whose disease is resistant to
both paclitaxel and an anthracycline‐containing regimen
†At least two prior chemotherapy regimens for advanced disease including an anthracycline and a taxane Cortes et al. Lancet 2011;377:914-23This presentation is the intellectual property of the author.
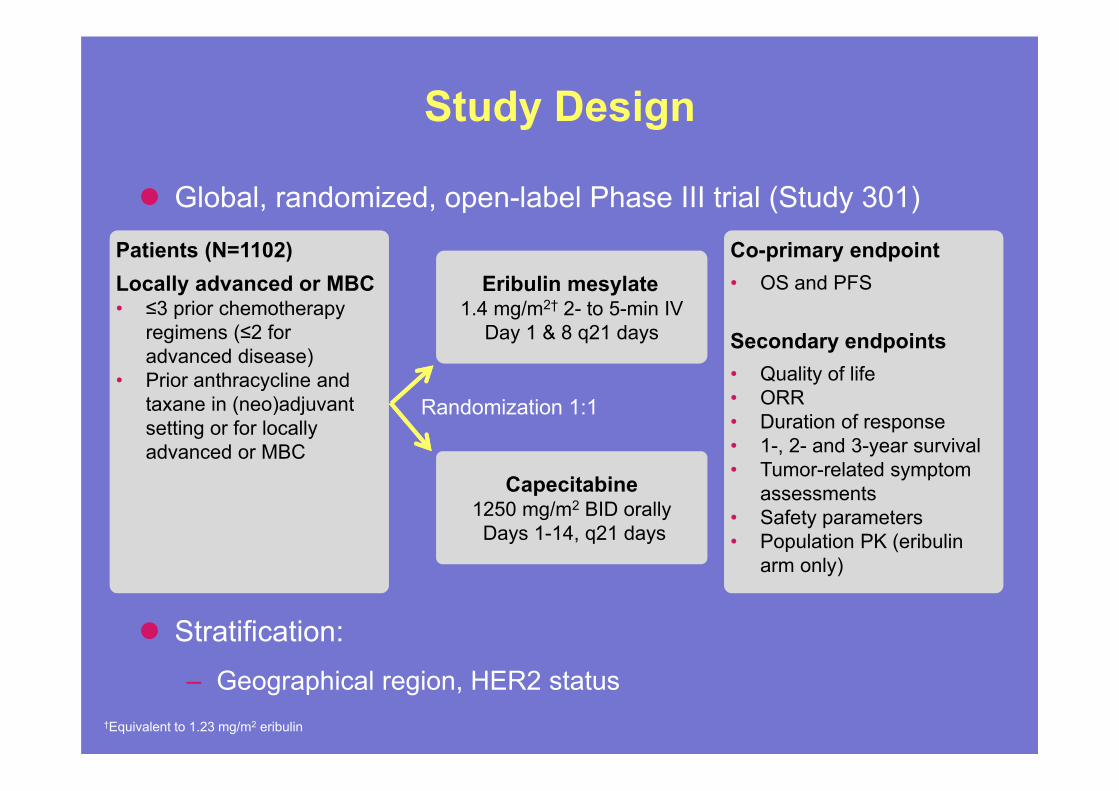
Study Design
Global, randomized, open-label Phase III trial (Study 301)
Stratification:– Geographical region, HER2 status
†Equivalent to 1.23 mg/m2 eribulin
Capecitabine1250 mg/m2 BID orallyDays 1-14, q21 days
Eribulin mesylate1.4 mg/m2† 2- to 5-min IV
Day 1 & 8 q21 days
Randomization 1:1
Co-primary endpoint• OS and PFS
Secondary endpoints• Quality of life• ORR• Duration of response• 1-, 2- and 3-year survival• Tumor-related symptom
assessments • Safety parameters • Population PK (eribulin
arm only)
Co-primary endpoint• OS and PFS
Secondary endpoints• Quality of life• ORR• Duration of response• 1-, 2- and 3-year survival• Tumor-related symptom
assessments • Safety parameters • Population PK (eribulin
arm only)
Patients (N=1102)Locally advanced or MBC• ≤3 prior chemotherapy
regimens (≤2 for advanced disease)
• Prior anthracycline and taxane in (neo)adjuvant setting or for locally advanced or MBC
Patients (N=1102)Locally advanced or MBC• ≤3 prior chemotherapy
regimens (≤2 for advanced disease)
• Prior anthracycline and taxane in (neo)adjuvant setting or for locally advanced or MBC

STATISTICAL PLAN: ANALYSIS OF CO‐PRIMARY ENDPOINTS
• Primary pre‐defined analyses in the ITT population• Two‐sided, stratified log‐rank test stratified for HER2 and geographic region;
HR based on Cox regression model
• 1,100 patients planned enrolment. OS determination, 905 events (final analysis, 82% events) sufficient for 90% probability if the HR <= 0.8 (Type I error = 0.04)
• Two planned interim analyses of OS: 453 and 603 deaths
• Final analysis would be declared positive if either• OS with eribulin is significantly better vs capecitabine (p≤0.0372) • PFS (independent review) with eribulin is significantly better vs capecitabine
(p≤0.01) and HR for OS (eribulin/capecitabine) is <1
San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center – December 4-8, 2012
This presentation is the intellectual property of the author.

PATIENT AND DISEASE CHARACTERISTICS
ITT population†Determined by independent assessment; missing patients for sites of disease were 1% for eribulin and 1% for capecitabine ‡Assays carried out and defined locally Unknown patients for eribulin and capecitabine were: HER2 status 17% and 16% ; ER status 11% and 10%; PR status 12% and 12%, respectively
Eribulin (n=554) Capecitabine (n=548)
Median age (range) 54.0 (24‐80) 53.0 (26‐80)
ECOG performance, % 0 45 42
1 53 55
2+ 2 3
Number of prior chemotherapy regimens for advanced disease, %
0 21 19
1 50 53
2 28 27
>2 1 1
Sites of disease†, % Visceral 84 88
Non‐visceral only 15 11
HER2 status‡, % Positive 16 15
Negative 68 69
ER status‡, % Positive 47 51
Negative 42 39
PR status‡, % Positive 41 43
Negative 47 45
Triple (ER/PR/HER2) negative, % 27 25
San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center – December 4-8, 2012
This presentation is the intellectual property of the author.
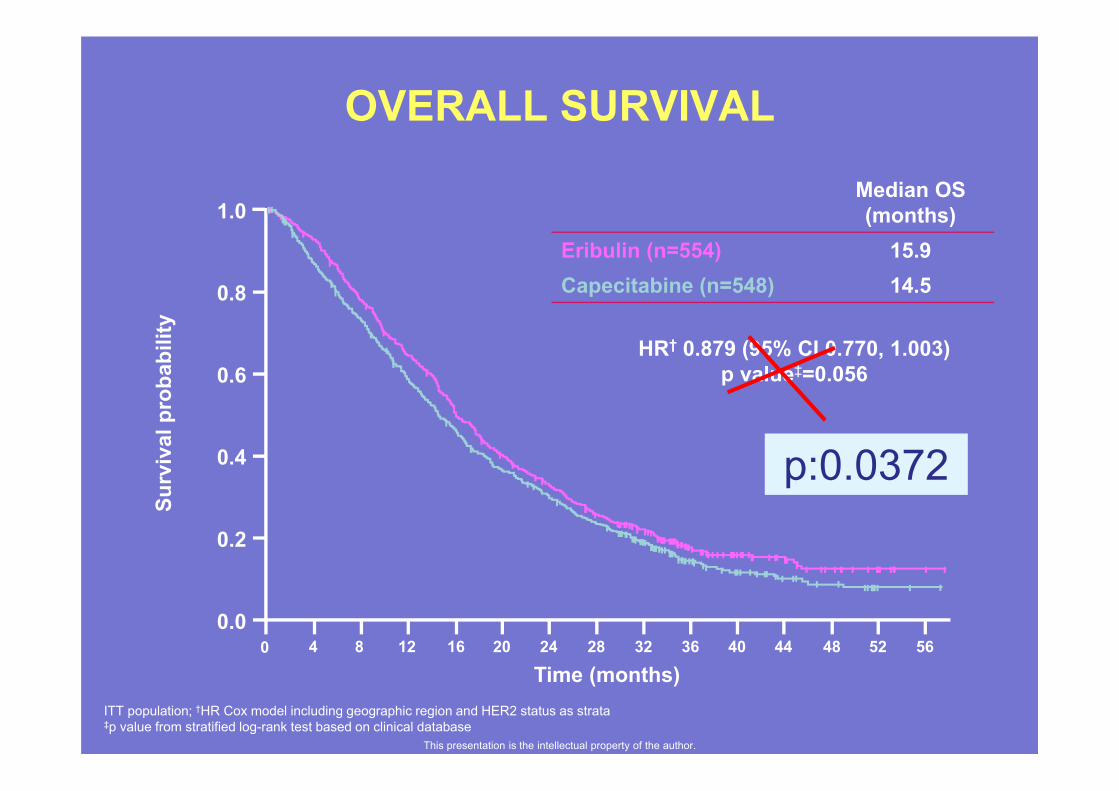
OVERALL SURVIVALSu
rviv
al p
roba
bilit
y
Time (months)0
0.0
0.2
0.4
0.6
0.8
1.0
56524844403632282420161284
HR† 0.879 (95% CI 0.770, 1.003)p value‡=0.056
Median OS (months)
Eribulin (n=554) 15.9Capecitabine (n=548) 14.5
ITT population; †HR Cox model including geographic region and HER2 status as strata‡p value from stratified log-rank test based on clinical database
This presentation is the intellectual property of the author.
p:0.0372

HR† 0.977 (95% CI 0.857, 1.114) p value‡=0.736
HR† 1.079 (95% CI 0.932, 1.250) p value‡=0.305
Time (months)
Investigator ReviewIndependent Review
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
pro
babi
lity
Time (months)0 4 8 12 16 20 24 28 32 36 40 44 0 4 8 12 16 20 24 28 32
1.0
0.8
0.6
0.4
0.2
0.0Su
rviv
al p
roba
bilit
y36 40 44
ITT population; †HR Cox model including geographic region and HER2 status as strata‡p value from stratified log-rank test based on clinical database
Median (months)
Eribulin (n=554) 4.1
Capecitabine (n=548) 4.2
Median (months)
Eribulin (n=554) 4.2
Capecitabine (n=548) 4.1
PROGRESSION-FREE SURVIVAL
This presentation is the intellectual property of the author.

RESPONSE RATES
STUDY MEDICATION EXPOSURE
ADVERSE EVENTS

Overall 0.879 (0.770, 1.003) 15.9 14.5
HER2 status
Positive 0.965 (0.688, 1.355) 14.3 17.1
Negative 0.838 (0.715, 0.983) 15.9 13.5
ER status
Positive 0.897 (0.737, 1.093) 18.2 16.8
Negative 0.779 (0.635, 0.955) 14.4 10.5
Triple negative
Yes 0.702 (0.545, 0.906) 14.4 9.4
No 0.927 (0.795, 1.081) 17.5 16.6
Subgroup HR (95% CI) Eribulin CapecitabineMedian (months)
ITT population
Overall Survival By Receptor Status
0.2 0.5 1.0 2 5
n=755
n=449
n=284
Favors eribulin Favors capecitabineThis presentation is the intellectual property of the author.
CONCLUSIONES
Este estudio no demuestra una superioridad estadísticamente significativa de eribulina vs capecitabina en la SG o la SLP
La mediana de SG: eribulin15.9 meses, capecitabine14.5 mes
HR, 0,879 (IC del 95%: 0,770, 1,003)
Eribulina y capecitabina tiene una actividad similar.
Subgrupos de pacientes pueden tener un mayor beneficio terapéutico con eribulina triple negativo, ER negativo, HER2 negativo.

• La eribulina es un fármaco imprescindible en nuestras mujeres con CMM politratadas.
• El ÚNICO fármaco que mejora la SUPERVIVENCIA GLOBAL, en monoterapia.
• Utilización de forma PRECÓZ.• Presenta una excelente tolerancia, con pocos efectos adversos, que son manejables.
• Es un fármaco equivalente a la capecitabina, en mujeres con CMM y tratamiento precoz.

Related Documents











