Evidence-based Practice Integrate best current evidence with clinical expertise and patient/family preferences and values for delivery of optimal health care www.qsen.org 1

Evidence-based Practice Integrate best current evidence with clinical expertise and patient/family preferences and values for delivery of optimal health.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Evidence-based Practice
Integrate best current evidence with clinical expertise and patient/family preferences and values for delivery of optimal health care
www.qsen.org
1
Who is Betty Neuman’s “Client”?
An individual, a family, a group or a community.
Continuous exchanges between the client system and the environment
The model is Wholistic—looks at all aspects of the client’s five key variables and how each impacts and is impacted by the other.
2
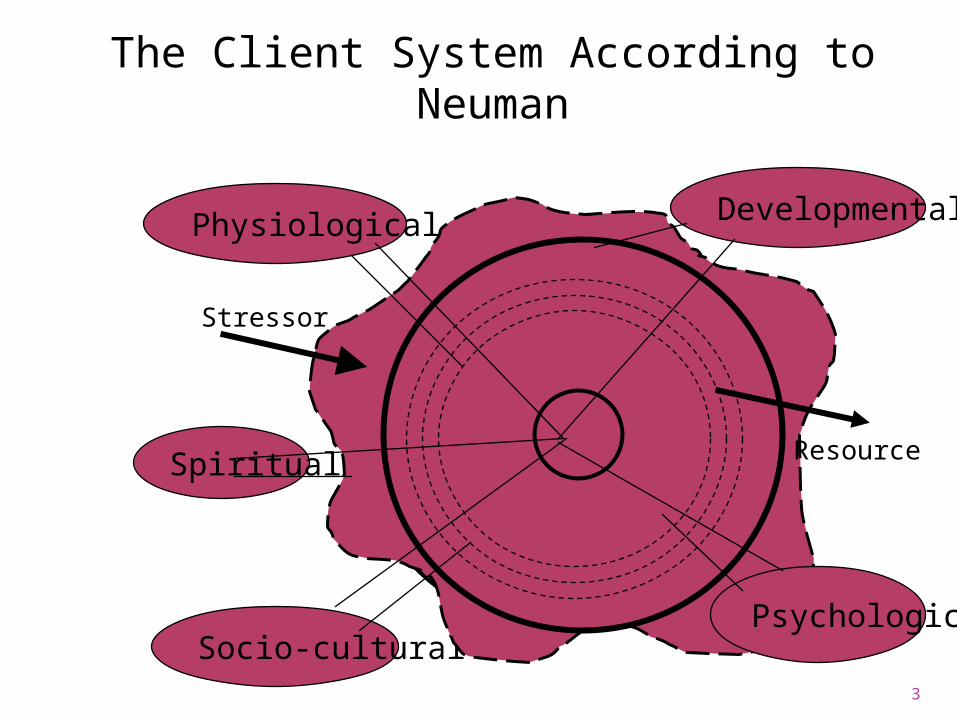
The Client System According to Neuman
Physiological Developmental
Spiritual
Socio-culturalPsychological
Stressor
Resource
3
How can we apply NSM to family?
Family as core What are family strengths?
(FLD) Individual systems as
Stressors Resources
4
What makes a family healthy?
5
What are risk factors to a family’s health?
6
Potential ND for families
Decisional conflict Compromised family coping Disabled family coping Ineffective family Therapeutic
regimen management Interrupted Family processes Readiness for enhanced Family
Coping
7
Stressors of Hospitalization
Fear Separation – family & peers Feelings of loss of control Regression common
8
Infant & Toddlers
Separation anxiety (6-30 months)3 phases
Protest:
Despair:
Detachment:
9F
Toddlers
React to any intrusive procedure the same
Developing autonomy Rituals and routines
10
Preschool
Less obvious separation anxiety
Fears mutilation Literal interpretation of words Like familiar routines & rituals Magical thinking
11
School-Age
Some separation anxiety Fears:
Body disability & death Dependence /loss of control
Ask relevant questions Understand cause and effect
12
Adolescent
Separation Body & body image Control important
13
Playroom
A safe area NO Intrusive procedures Not for administering
medications. Therapeutic Play
14
Risk for Falls
Who’s at risk? “Humpty Dumpty”
®assessment tool Individualized plan of care
4 siderails up not a restraint, it’s safety.
Communicate Educate
15
Risk for Impaired Skin Integrity Who’s at risk? (i.e. “risk factors”) Braden Q Scale
Mobility Activity Sensory Perception Moisture Friction-Shear Nutrition Tissue perfusion and oxygenation
16
Pain
Subjective and personal “an unpleasant sensory and emotional
experience… Associated with actual or potential
tissue damage” QSEN competencies on patient-
centered care: “Demonstrate comprehensive understanding of the concepts of pain and suffering, including physiologic models of pain & comfort.” (www.qsen.org)
17
Myths about Pain
Neonates do not experience pain.* Children have no memory of pain.* Correct amount of pain for a specific
injury or procedure* Parent’s exaggerate. Children tell you about pain. Children become addicted to
narcotics easier.* Narcotics cause respiratory
depression easier in children.*18
Influences on Pain Assessment
Previous experience with pain Developmental level
Ex: language ability Young infants: generalized
response – not able to localize. Type of pain – acute or chronic Parental response to child's pain
19
Behavioral Indicators
Restless, agitated
Difficult to distract
Irritability Facial grimacing Posturing
Drawing up knees
Anorexia Lethargy Sleep
disturbances
20
SpiritualitySpiritus
Meaning Value Transcendence Connecting Becoming
21
Spiritual Assessment
Religion: system of practices Culture – strong influence on
spirituality
Professional responsibility Collaborative
22
Spiritual Assessment of Children
Infant: sense of trust Toddler: rituals & routines Pre-school: concept of God concrete
family’s beliefs & customs important
School-age: good vs evil; help receiving love, hope, forgiveness
Adolescents: need for meaning & purpose in life.
Listen
23

Nursing Dx
Spiritual Distress Risk for Spiritual Distress Readiness for enhanced
Spiritual well-being
24
Chronic Illness
McKinney : a chronic illness or condition is one that is: long term Does not resolve spontaneously Usually without complete cure frequently has residual
characteristics that limit ADL &/or require adaptation or special assistance.
25
Needs of Family /Caregiver
Illness a family experience Reduce physical & emotional
burdens Provide knowledge & skill Resources for support Promote healthy coping Help prepare for impending
death 26
Caregiver role strain
Stages of caregiving http://www.alsa.org
Caregiver and care recipient at risk when caregiver overloaded.
27
Perception of Death: Infants & Toddlers
Lack understanding of concept
Greatest fear is separation No sense of time Reaction to loss of caregiver
28
Perception of Death: preschoolers
Death temporary & reversible Magical thinking Behaviors: Questions
29
Perception of Death: School-age
Death irreversible By age 10, universality Behaviors:
30
Perception of Death: Adolescent
Death irreversible, universal, inevitable
Personal, but distant Better understanding illness &
death Behaviors:
31
Nursing Care
Be available Personal beliefs & expectations Time & attention to the dying
child. Recognize need to talk Pain control, oral care, privacy Information Allow family members time
32
Children with Special Needs
Visual Impairment
Hearing Impairment
Language Aphonic
Neurologic impairment
Chronic illness Congenital
disability Developmental
delay or disability
33
Etiology
Hereditary- 5% Early embryonic alterations Early Intrauterine /neonatal
conditions Acquired childhood Environmental problems Unknown
34
35
Congenital Hypothyroidism
A deficiency of thyroid hormone present at birth.
Screening: 2-6 days after birth Untreated: severe mental
retardation. Primary prevention (of negative
outcome): lifelong thyroid supplements
36
F
Down Syndrome
Small square head Upward slant to eyes Flat nasal bridge Protruding tongue Hyperflexibility, muscle weakness Wide space between big & 2nd toes
37
Down Syndrome-higher incidence of:
Congenital heart malformations Frequent respiratory tract infections Thyroid disorders incidence of leukemia Atlantoaxial instability
38
Nursing Care
Early detection Developmental level Strengths vs. disabilities Support parents Encourage socialization Appropriate therapy
39
Nursing Care
Promote optimal growth & development
Behavior modification program Anticipatory guidance
40
Safety Concerns
Poor short-term memory Learn at a slower rate Physical problems w/mobility
41
Related Documents











