Professional Assignment Thesis, 2010 (Module III.1 and III.2) Evidence Based Guideline for the Conservative Treatment of the Posterior Ankle Impingement Syndrome in Professional Ballet Dancers European School of Physiotherapy, Hogeschool van Amsterdam (HvA), Tafelbergweg 51, Amsterdam, The Netherlands. February 2011 The Authors of the Guideline T. Soler, R. Jezerskyte Banfi, L. Katsman

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Professional Assignment Thesis, 2010 (Module III.1 and III.2)
Evidence Based Guideline for the Conservative
Treatment of the Posterior Ankle Impingement
Syndrome in Professional Ballet Dancers
European School of Physiotherapy, Hogeschool van Amsterdam (HvA), Tafelbergweg 51, Amsterdam, The Netherlands.
February 2011
The Authors of the Guideline
T. Soler, R. Jezerskyte Banfi, L. Katsman
2
Preface
This guideline is a part of the professional assignment thesis created for the curriculum of the European
School of Physiotherapy.
The authors of the guideline are: Tamara Soler, Ruta Jezerskyte-Banfi and Leon Katsman.
This guideline is intended to assist physiotherapists in creating the treatment plan for the posterior ankle
impingement syndrome (PAIS) in professional ballet dancers.
At the end of the guideline the reader will find a summary of the scientific literature regarding the conservative
treatment modalities, as well as authors‟ recommendations for the use of each modality.
It is the authors‟ hope, that the reader will be able to use this guideline in clinical practice and that further
research will be instigated in order to create the specific evidence based protocol for the conservative
treatment of the PAIS in professional ballet dancers.
Conte
nts
3
Contents
Preface ............................................................................................................................................................... 2
Contents ............................................................................................................................................................. 3
A. Introduction ..................................................................................................................................................... 4
A.1 Target group ............................................................................................................................................. 4
A.2 Problem definition ..................................................................................................................................... 4
A.3 What is PAIS?........................................................................................................................................... 4
A.4 The role of the physiotherapist ................................................................................................................. 5
A.5 General Treatment ................................................................................................................................... 5
B. Diagnostic Process......................................................................................................................................... 6
B.1 Introduction ............................................................................................................................................... 6
B.2 Screening .................................................................................................................................................. 6
B.3 History-taking ............................................................................................................................................ 7
B.4 Examination .............................................................................................................................................. 7
B.5 Differential diagnosis ................................................................................................................................ 7
B.6 Assessment tools...................................................................................................................................... 8
B.7 Analysis .................................................................................................................................................... 9
B.8 Conclusion ................................................................................................................................................ 9
B.9 Treatment plan.......................................................................................................................................... 9
C. Therapeutic Process ...................................................................................................................................... 9
C.1 Therapeutic methods .............................................................................................................................. 10
C.2 Evaluation ............................................................................................................................................... 18
C.3 Preventing the PAIS ............................................................................................................................... 19
Acknowledgements........................................................................................................................................... 19
References ....................................................................................................................................................... 20
Supplements ..................................................................................................................................................... 22
Supplement 1. Conclusions and recommendations .................................................................................... 22
Supplement 2. Assessment tools .................................................................................................................. 27
A. In
troductio
n
4
A. Introduction
This guideline has been developed according to the request of the Health team members working at Het
Nationale Ballet (HNB) in the Netherlands, and is a consecutive product following the literature review and
expert consensus produced by the authors of this guideline. The main objective of the guideline for the
physiotherapists was to enhance the health, training, well-being and performance of professional ballet
dancers suffering from the Posterior Ankle Impingement Syndrome (PAIS). Particular need for an evidence-
based guideline was noted by the authors while reviewing the literature and interviewing experts in the dance
field. The absence of an adequate research, as well as the lack of unanimous agreement between
physiotherapists regarding the conservative treatment plan for PAIS, inspired the authors to engage in the
process of a guideline creation. Furthermore, the significance of such guideline lies in the necessity for
dancers, physiotherapists, ballet and insurance companies to acquire a transparent way of working while
creating and evaluating the conservative treatment plan for PAIS.
The advice and recommendations discussed in this guideline create an evidence based outline of the most
common modalities used by physiotherapists for the conservative treatment of PAIS, in order to assist the
reduction of symptoms and to achieve prior activity level of a professional ballet dancer.
A.1 Target group
This guideline is intended for physiotherapists with different specializations (manual therapists, sports
physiotherapists, etc.) that treat professional ballet dancers with PAIS after an acute or chronic episode. In
addition to the specific background knowledge about dancers‟ activity and injury pathomechanics, mastered
by physiotherapists working in the field, the guideline is designed to be used as a complementary tool when
creating an effective treatment plan for professional dancers suffering from PAIS.
A.2 Problem definition
The scientific literature and physiotherapy experts working with dancers indicate that professional ballet
dancers are often predisposed to the PAIS, due to the specific ballet technique demands. Nevertheless, the
treatment of this pathology is lacking a comprehensive and complete guideline.
A.3 What is PAIS?
PAIS is defined as a clinical disorder in which the posterior ankle pain occurs during forced plantar flexion
position. In professional ballet dancers it is typically a chronic problem of insidious onset. In addition, onset of
symptoms can be secondary to a precipitating injury to other anatomical structures around the ankle
(Maquirriai 2005, Robinson 2007).
Pathological entities involved in PAIS are generally categorized as osseous or soft tissue. Osseous
impingement involves displaced os trigonum, hypertrophic posterior talar process, loose body and/or a
prominent superior calcaneal tuberosity (van Dijk, 2006, Peace et al. 2004). Soft tissue impingement involves
thickening or calcification of the posterior tibiotalar capsule and postraumatic scar tissue. Secondary
A. In
troductio
n
5
involvement of the Flexor Hallucis Longus (FHL) tendonitis (“Dancer‟s tendinitis”), Achilles tendinitis, and
tarsal tunnel syndrome or osteochondral lesion can often mimic PAIS (Bureau et al. 2000).
A.3.1 Epidemiological data
No precise epidemiology records of PAIS exist for neither the general nor professional ballet dancers
population. “A great amount of weight-bearing plantar flexion of the ankle especially in the „demi-pointe‟
and in „pointe‟ positions is a crucial component of classical ballet technique, therefore it is considered to
be one of the major factors evoking and exacerbating PAIS (Russell et al. 2010).
A.3.2 Diagnosis
Diagnosis of PAIS is based on clinical history and physical examination. In professional ballet dancers it
is typically a chronic problem of insidious onset. In addition, onset of symptoms can be secondary to a
precipitating injury to other anatomical structures around the ankle (Robinson, 2007). The most
commonly seen features of PAIS in professional ballet dancers include pain during activity in the
posterolateral or posteromedial aspect of the ankle (especially during „relevé‟ movement), swelling,
grinding sensation (during forced plantarflexion), reduced joint mobility and impaired physical activity as
well as participation.
Differential diagnosis is usually performed with additional laboratory examination tools such as
radiography, CT scan, MRI or an arthroscopy. The physicians and physiotherapists may consider
radiographic examinations to confirm the diagnosis, therefore optimizing the therapy.
A.4 The role of the physiotherapist
Physiotherapy can play an important role in different stages of the rehabilitation process in professional
dancers with PAIS. Primarily, guiding the dancer through the course of pain alleviation and teaching how to
cope with the actual situation. During the rehabilitation process, assistance and special competencies of sport
physiotherapists, physiotherapists or manual therapists working in the dance field are necessary.
Physiotherapy cannot always have a good prognosis, especially, when osseous structures are involved (e.g.
Os Trigonum). Nevertheless, the consequences of the disorder, such as decrease of muscle strength, lack of
ankle stability, core muscle weakness and postural or functional alignment can be avoided and/or improved by
physiotherapy.
Furthermore, an efficient communication is essential between the Health team members, dancers,
choreographers, teachers and company directors in order to recognize limitations and to provide the best
treatment possible.
A.5 General Treatment
No specifically structured conservative treatment for PAIS is as yet known. In everyday practice, the treatment
plan often involves the use of several modalities simultaneously. A combination of exercise therapy, manual
therapy, technique re-education, ankle and core stability training is performed. A more detailed description of
the various modalities and timeline used, are provided in the evidence based review developed by the authors
of the guideline.
B.
Dia
gnostic P
rocess
6
B. Diagnostic Process
B.1 Introduction
Assessing the severity and nature of the dancer‟s complaint and the possibility to modify it by applying
physiotherapy is the main objective of the diagnostic process. The PAIS diagnosis is based on clinical history
and physical examination. The initial assessment must first concentrate on impairments of body functions and
body structure, after which the focus will shift to limitations of activities and restrictions of participation, and
finally to the influence of environmental and personal factors. A very important aspect of the initial assessment
is the detection of red and yellow flags. Such screening process has to be performed by the physiotherapist,
and in case a red or yellow flag is found, a dancer has to be referred to an appropriate specialist.
B. 2 Screening
During the screening process an indication for physiotherapy is examined. The physiotherapist assesses the
dancer‟s pattern of complaints and symptoms and the possible presence of yellow and red flags. Yellow flags
are indications of psychosocial and behavioral risk factors for the persistence and/or deterioration of the
dancer‟s health problems. Red flags are patterns of signs or symptoms (alarm signals) that may indicate
serious pathology (e.g. fracture), necessitating further medical diagnostics. It is of great importance for the
physiotherapist to be able to recognize the typical pattern of complaints of the PAIS and the ankle in general,
in order to decide whether there are specific red flags that do not fit with this pattern. In case a red flag is
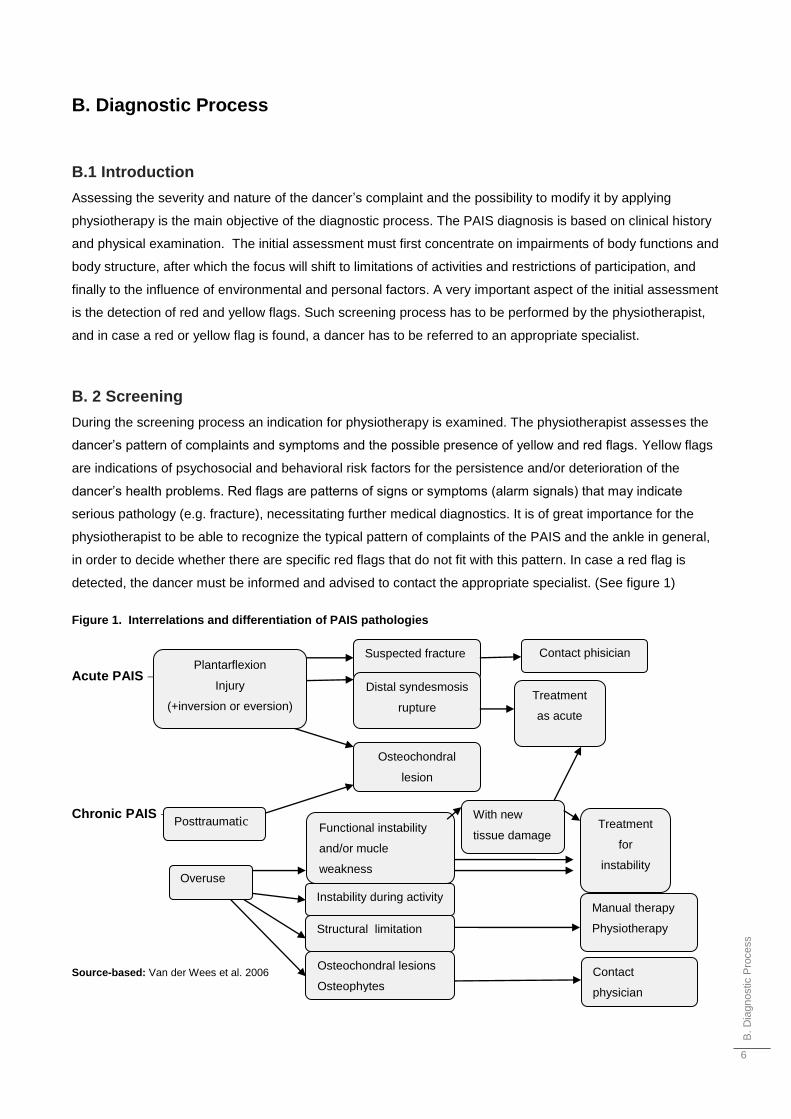
detected, the dancer must be informed and advised to contact the appropriate specialist. (See figure 1)
Figure 1. Interrelations and differentiation of PAIS pathologies
Acute PAIS →
Chronic PAIS →
Source-based: Van der Wees et al. 2006
Contact phisician Plantarflexion
Injury
(+inversion or eversion)
Suspected fracture
Distal syndesmosis
rupture
Osteochondral
lesion
Posttraumatic
Overuse
Functional instability
and/or mucle
weakness
Instability during activity
Structural limitation
With new
tissue damage
Treatment
as acute
Treatment
for
instability
Manual therapy
Physiotherapy
Osteochondral lesions
Osteophytes
Contact
physician
B.
Dia
gnostic P
rocess
7
B.3 History-taking
History-taking considers questions related to the causative factors involved (e.g. an old inversion trauma or
pain and swelling after an acute plantar hyperflexion event), development of the complaint over time and the
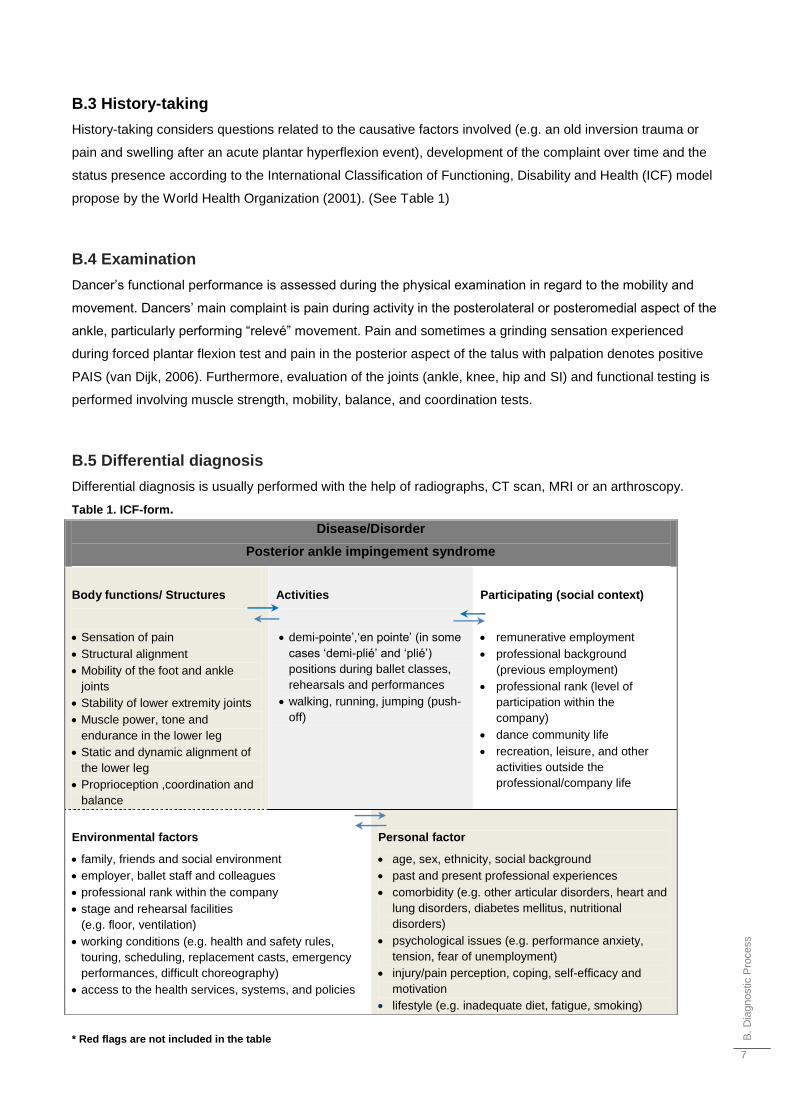
status presence according to the International Classification of Functioning, Disability and Health (ICF) model
propose by the World Health Organization (2001). (See Table 1)
B.4 Examination
Dancer‟s functional performance is assessed during the physical examination in regard to the mobility and
movement. Dancers‟ main complaint is pain during activity in the posterolateral or posteromedial aspect of the
ankle, particularly performing “relevé” movement. Pain and sometimes a grinding sensation experienced
during forced plantar flexion test and pain in the posterior aspect of the talus with palpation denotes positive
PAIS (van Dijk, 2006). Furthermore, evaluation of the joints (ankle, knee, hip and SI) and functional testing is
performed involving muscle strength, mobility, balance, and coordination tests.
B.5 Differential diagnosis
Differential diagnosis is usually performed with the help of radiographs, CT scan, MRI or an arthroscopy.
Table 1. ICF-form.
* Red flags are not included in the table
Disease/Disorder
Posterior ankle impingement syndrome
Body functions/ Structures
Sensation of pain
Structural alignment
Mobility of the foot and ankle
joints
Stability of lower extremity joints
Muscle power, tone and
endurance in the lower leg
Static and dynamic alignment of
the lower leg
Proprioception ,coordination and
balance
Activities
demi-pointe‟,„en pointe‟ (in some
cases „demi-plié‟ and „plié‟)
positions during ballet classes,
rehearsals and performances
walking, running, jumping (push-
off)
Participating (social context)
remunerative employment
professional background
(previous employment)
professional rank (level of
participation within the
company)
dance community life
recreation, leisure, and other
activities outside the
professional/company life
Environmental factors
family, friends and social environment
employer, ballet staff and colleagues
professional rank within the company
stage and rehearsal facilities
(e.g. floor, ventilation)
working conditions (e.g. health and safety rules,
touring, scheduling, replacement casts, emergency
performances, difficult choreography)
access to the health services, systems, and policies
Personal factor
age, sex, ethnicity, social background
past and present professional experiences
comorbidity (e.g. other articular disorders, heart and
lung disorders, diabetes mellitus, nutritional
disorders)
psychological issues (e.g. performance anxiety,
tension, fear of unemployment)
injury/pain perception, coping, self-efficacy and
motivation
lifestyle (e.g. inadequate diet, fatigue, smoking)
B.
Dia
gnostic P
rocess
8
B.6 Assessment tools
See some of the models for the questionnaires, below in the Supplement 2 (Appendix section).
● Forced plantar flexion test
The passive forced plantarflexion test should be performed with repetitive quick passive hyperplantarflexion
movements in a patient sitting with the knee flexed at 90˚. The test can be repeated in slight external rotation
or slight internal rotation of the foot on the tibia. The investigator can apply a rotational movement on the point
of maximal plantarflexion, thereby „„grinding‟‟ the posterior talar process/os trigonum between tibia and
calcaneus. A negative test rules out a posterior impingement syndrome. A positive test, in combination with
pain on posterolateral palpation, should be followed by a diagnostic infiltration. (van Dijk 2006, expert
opinions, 2010)
● The Pain Questionnaire (SEFIP) for Dancers
The SEFIP form is intended primarily for professional dancers but can also be used for dance students on
various courses, dance teachers and others who dance regularly and with relatively high intensity. Certain
words might have to be adjusted, e.g. “production” may be replaced with another suitable term better
reflecting the activity concerned. (Ramel 1999)
● The Foot & Ankle Disability Index (FADI) Sport Score
The Foot and Ankle Disability Index (FADI) Sport is a self-report instrument which was designed to assess the
functional limitations related to foot and ankle conditions while assessing tasks that are essential for sport.
FADI Sport has a total point value of 32 points. It is scored as percentages, with 100% representing no
dysfunction. (Martin et al 2009)
● Visual-Analogue-Scale Foot and Ankle (VAS FA)
Visual-Analogue-Scale Foot and Ankle has the following features: a questionnaire based on 20 questions
requiring purely subjective answers; three different question categories (pain, n = 4; function, n = 11; other
complaints n = 5); Visual-Analogue-Scale (VAS) based rating; computerized evaluation. (Richter et al. 2006)
● Patient Specific Complaints (PSC)
With the help of this instrument the dancer is asked to select three activities that he/she consider to be the
most important. The difficulties caused by performing these activities are scored on three separate 100 mm
Visual Analogue Scales (VAS) ( Source-based: Keun et al. 2004)
● Functional Evaluative Tests For Dance
The Functional Evaluative Tests for Dance instrument was developed by Liederbach (1994) in the Harkness
Center for Dance Injuries. It provides the basis for functional evaluation of static dance postures. Each
position has specific criteria to assess in determining the ability of the dancer to achieve and maintain static
postures. The Evaluation Criteria are to be use as guidelines for observing the dancer with respect to key
elements of each Position/Action. Dynamic evaluation is usually carried out after the clinician is satisfied with
C.
Th
era
peutic P
rocess
9
the dancer‟s ability to maintain static postures. The physiotherapists may go directly to dynamic evaluation if
they are familiar with the dancer‟s performance, rehearsal, training, and injury history ( Brinson and Dick
1996).
● The Healthier Dancer questionnaire
Using the Healthier Dancer questionnaire different aspects of dancers‟ health, well-being and injury can be
assessed (Brinson and Dick 1996).
B.7 Analysis
Information collected during the phases of diagnostic process defines dancer‟s complains in terms of
impairments of body functions and structures, limitations in activities and participation, as well as
environmental and personal factors. Establishing a physiotherapy diagnosis and assessing the indication for
physiotherapy are the main objectives.
B.8 Conclusion
After answering the below mentioned questions, the physiotherapist and the dancer should discuss the
individual treatment goals and create a treatment plan.
Questions to be answered:
● What is the physiotherapy diagnosis?
● Is physiotherapy indicated?
● Can the dancer be treated according to the guideline?
B.9 Treatment plan
The treatment plan is made according to prioritized physiotherapy goals. The physiotherapist must discuss the
treatment plan with the dancer in order to agree on the future goals. The overall objective of the treatment
must be connected with the specific help seeking question of a dancer. Since rest is a very important factor in
the healing process, going back to activity should be regulated and gradual in order to prevent „over-loading‟.
C. Therapeutic Process
The objectives for the therapeutic process are set to optimize dancer‟s functions, activities, and participation.
On the basis of the physiotherapy diagnosis, the treatment plan is formulated, discussed with the dancer and
adjusted accordingly. The physiotherapist and the dancer should discuss the level of expected outcome and
make necessary adjustments regarding dancers‟ specific requirements. The treatment plan should contain
treatment goals (SMART), timeline, modalities and preferably evidence based practice. The treatment process
should be re-evaluated and adjusted regularly. The importance of preventing injury recurrence must be
emphasized.
C.
Th
era
peutic P
rocess
10
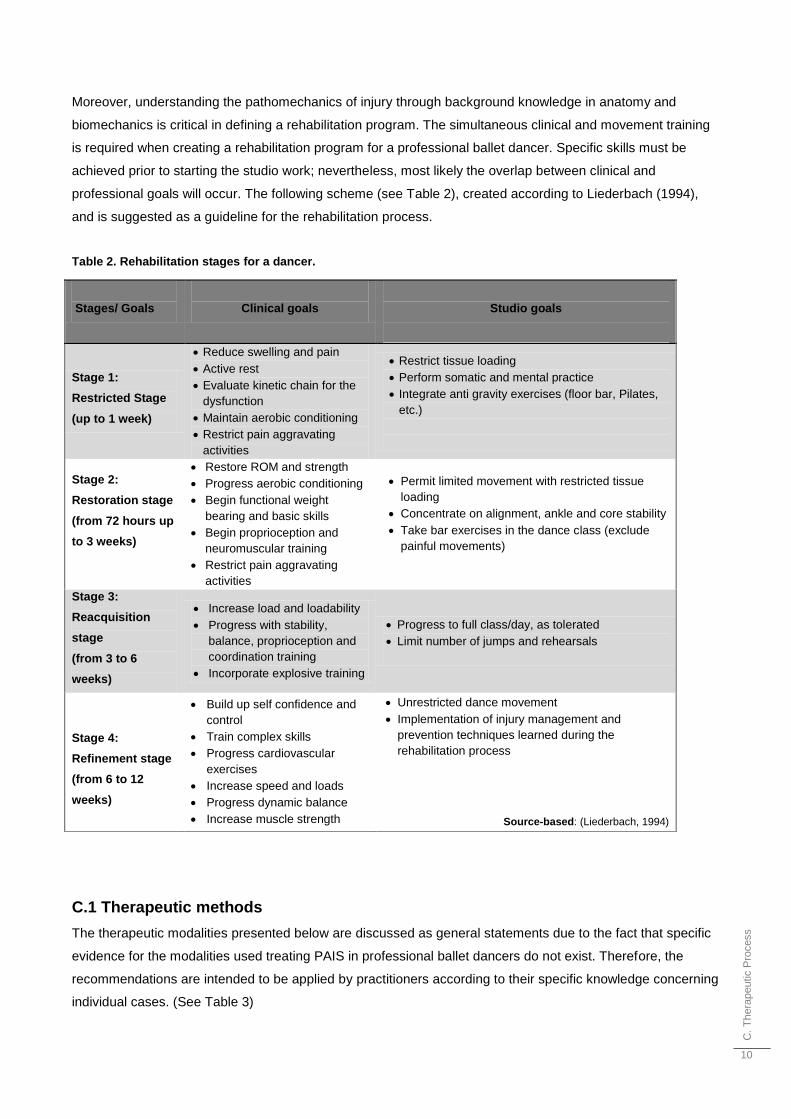
Moreover, understanding the pathomechanics of injury through background knowledge in anatomy and
biomechanics is critical in defining a rehabilitation program. The simultaneous clinical and movement training
is required when creating a rehabilitation program for a professional ballet dancer. Specific skills must be
achieved prior to starting the studio work; nevertheless, most likely the overlap between clinical and
professional goals will occur. The following scheme (see Table 2), created according to Liederbach (1994),
and is suggested as a guideline for the rehabilitation process.
Table 2. Rehabilitation stages for a dancer.
C.1 Therapeutic methods
The therapeutic modalities presented below are discussed as general statements due to the fact that specific
evidence for the modalities used treating PAIS in professional ballet dancers do not exist. Therefore, the
recommendations are intended to be applied by practitioners according to their specific knowledge concerning
individual cases. (See Table 3)
Stages/ Goals
Clinical goals
Studio goals
Stage 1:
Restricted Stage
(up to 1 week)
Reduce swelling and pain
Active rest
Evaluate kinetic chain for the
dysfunction
Maintain aerobic conditioning
Restrict pain aggravating
activities
Restrict tissue loading
Perform somatic and mental practice
Integrate anti gravity exercises (floor bar, Pilates,
etc.)
Stage 2:
Restoration stage
(from 72 hours up
to 3 weeks)
Restore ROM and strength
Progress aerobic conditioning
Begin functional weight
bearing and basic skills
Begin proprioception and
neuromuscular training
Restrict pain aggravating
activities
Permit limited movement with restricted tissue
loading
Concentrate on alignment, ankle and core stability
Take bar exercises in the dance class (exclude
painful movements)
Stage 3:
Reacquisition
stage
(from 3 to 6
weeks)
Increase load and loadability
Progress with stability,
balance, proprioception and
coordination training
Incorporate explosive training
Progress to full class/day, as tolerated
Limit number of jumps and rehearsals
Stage 4:
Refinement stage
(from 6 to 12
weeks)
Build up self confidence and
control
Train complex skills
Progress cardiovascular
exercises
Increase speed and loads
Progress dynamic balance
Increase muscle strength
Unrestricted dance movement
Implementation of injury management and
prevention techniques learned during the
rehabilitation process
Source-based: (Liederbach, 1994)
C.
Th
era
peutic P
rocess
11
● Manual therapy
Physiotherapists frequently use passive mobilizations of the ankle joints for the treatment of ballet dancers or
athletes with PAIS (expert opinions, 2010). The current research does not provide enough information about
the manual therapy interventions specifically for acute or chronic PAIS, nevertheless, there is evidence for the
efficacy of this treatment, when combined with multimodal or exercise therapy, in cases of acute ankle injuries
(Brantingham et al. 2009, Bleakley et al. 2008, van der Wees et al. 2006, van der Wees et al. 2006).
The authors recommend passive mobilizations of the ankle joints for the treatment of professional ballet
dancers with PAIS in order to reduce pain and regain mobility before starting active exercise therapy (expert
opinions, 2010). Furthermore, manually guided active ROM exercises (extrinsic feedback) are recommended
when treating PAIS in order to stimulate intrinsic feedback encouraging the correct movement patterns (expert
opinions, 2010). Additionally, active manipulations using McKenzie Belt technique are suggested.
Ankle stability exercises
Research shows that lack of stability in the ankle can be improved with Whole body vibration training (WBVT)
which is a new rehabilitation method that has been linked with improving balance and muscle function. WBVT
improved static balance and Star Excursion Balance Test (SEBT) scores amongst dancers exhibiting ankle
instability (Cloak 2010). Likewise, elastic resistance exercises are shown to improve balance in subjects with
or without history of lateral ankle sprains (Hak 2009). Evidence shows that daily ankle disk training assists in
preventing ankle sprains (Arnold 2004). Balance training protocols have consistently been shown to improve
postural stability in subjects with chronic ankle instability (CAI) (Holmes 2009).
The authors of the guideline strongly recommend ankle stability exercises for the conservative treatment of
PAIS in professional ballet dancers when acute or CAI is present.
Stretching exercises for the ankle
According to the research both, jogging and static stretching exercises appear to be beneficial to individuals
participating in sports activities. It is of importance to note, that for the decrease of muscle stiffness, dynamic
stretching series while running were more effective than static stretching at the ankle joint (McNair 1996).
Looking at stretching more deeply, research shows greater increase in active ROM compared to passive
ROM when micro stretching is performed (Wyon and Matthew, 2009). Furthermore, it is important to note that
young dancers with a tendency to have very lax joint structures should be identified early and advised against
overstretching (Reid 1988).
The authors recommend active resistance and dynamic stretching exercises for the conservative treatment of
PAIS in professional ballet dancers who present no chronic or structural ankle instability.
Proprioception/ Neuromuscular training
Proprioception is not commonly assessed in dancers (Batson 2009). Nevertheless, it is important to examine
it, as a minimal proprioceptive deficit can compromise finely tuned motor control, increasing the risk of injury.
Batson (2009) suggest that a proprioceptive deficit undetected, can lead to adaptations in alignment, localized
weakness, and altered central motor programming. Therefore, “if proprioception is insufficiently recovered
after injury the dancer may lack confidence to move fully and safely” (Batson 2009).
C.
Th
era
peutic P
rocess
12
The studies mention below suggested that retraining proprioception after injury must address different levels.
According to Batson (2009), proprioception should be trained at the level of central nervous system, reflex
spinal level, brain stem level, and cortical level to guarantee a good recovery. Therefore, a combination of
proprioceptive exercises like wobble boards, Pilates reformer training, plyometric training and mini-trampoline
exercises with additional challenges of body positioning, range of motion (ROM), and cognitive- and manual
interference would be recommended (Batson 2009, Willardson 2007). Other factors (positive feedback
concerning the performance, increase of the dancers‟ autonomy, and encouraging an external focus) and
techniques (Alexander Technique, Feldenkrais Awareness through Movement, and Body-Mind Centering)
should also be considered to refine visual and proprioceptive feedback. Batson (2009) describes that
increased muscular efficiency and higher retention of rehabilitation benefits are shown when somatic practices
are combined with manual therapies.
van der Wees et al. (2006) suggest that proprioception should be trained across the full ROM, in order to
activate the mechanoreceptors under specific angles as well; this is particularly relevant to the ROM after
mobilizations.
According to Zech et al. (2010) balance training should be emphasized, as it is shown to be effective for
postural and neuromuscular control of the ankle.
The Royal Dutch Society for Physical Therapy (Koninklijk Nederlands Genootschap voor Fysiotherapie-
KNGF) guideline for acute ankle sprain describes that wobble board exercises alone are insufficient to train all
aspects of proprioception. Therefore, they recommend the use of functional Daily Life Activities (ADL) or sport
specific types of exercises.
Further high-quality clinical trials are needed to enhance the evidence base and to help physical therapists to
select effective and more specific strategies for dancers, during neuromuscular training.
The authors strongly recommend proprioception training in which the combination of functional and activity
related exercises are considered.
Endurance training
Dance is a very demanding form of physical activity. Especially, since dance has a high degree of physical
exertion, the concept of aerobic capacity becomes very important factor over a significant period of time
(Brinson and Dick, 1996). A dancer is required to have strong aerobic foundations in order to meet the
required workload (Twitchett et al. 2009). Efficient aerobic capacity is necessary to guarantee an improved
performance, reduce the risk of injury and therefore prolong dancers‟ careers.
The authors recommend emphasizing endurance training for the conservative treatment of PAIS in
professional ballet dancers. Furthermore, endurance training must be incorporated in the rehabilitation
process in the first stages, in order to prevent the decrease of dancers‟ aerobic capacity and therefore to
maintain the loadability
Strength training
The recent review by Koutedakis et al. (2009) noted that there is no scientific evidence available
recommending the use of different strength training regimens for different dance styles. However, amongst
other causes, reduced muscular strength accounts for injuries that are of greater severity in dancers
(Koutedakis et al. 2009, Brinson and Dick 1996). Van der Wees et al. (2006) indicates that strength training
C.
Th
era
peutic P
rocess
13
promotes the recovery in cases of functional instability of the ankle. According to expert opinions, strength
training for the ankle is frequently used in practice when treating PAIS in professional ballet dancers.
Plyometric training is proved to enhance ankle functional stability (Ismail et al. 2010).
Therefore, the authors are of the opinion that strengthening exercises for the ankle and foot (in combination
with the strengthening exercises for the kinetic chain) are recommended when treating PAIS in professional
ballet dancers. Furthermore, the authors recommend additional implementation of plyometric training in order
to improve ankle functional stability.
● Core stability exercises
Scientific literature recognizes the fact that strength and stability exercises for core muscles are the key
components in training programs for athletes (Bliss et al. 2005, Behm et al. 2010). It also emphasizes the
relationship between the core stability and incidence in the lower extremity injuries (Bliss et al. 2005, Willson
et al. 2005). Nevertheless, despite the popularity of core training, there is a lack of scientific studies conducted
to validate its benefits for athletes (Willardson, 2007).
The existing studies agree that the phase of training and the specific health status of an athlete should be
considered when recommending core stability exercises (Willardson, 2007). Furthermore, as mentioned in the
review by Behm et al. (2010), training programs preparing the athletes for a variety of alternating postures and
external forces, must incorporate the destabilizing component into the exercise regiment. It has been
suggested that the foundation for core stability exercises in elite athletes should be formed by round-based
free-weight exercises with moderate levels of instability (Behm et al. 2010).
Guidelines for initiating point training in ballet students (Weiss et al. 2009) recommend delaying point work in
cases where the student has weak trunk or pelvic (core) musculature. According to the expert opinions
(2010), core stability exercises are often used in practice when treating professional ballet dancers with PAIS.
The authors suggest core stability training as a part of an exercise program for the conservative treatment of
PAIS in professional ballet dancers. Core stability training should be considered in a specific phase of the
rehabilitation process in order to reduce the load and to enhance the control in the lower extremities. Pilates
and Yoga exercises can be used as supplementary components of core stability training (Omkar et al. 2009,
Emery et al. 2010).
Kinetic chain exercises
Identification of the kinetic chain dysfunctions, which are responsible for the functional biomechanical
deficiencies, is an important factor when establishing treatment plan for PAIS in professional dancers (expert
opinions, 2010). Kinetic chain deficits which can be detected during functional testing and must be treated in
order to prevent the risk of failed rehabilitation or predispose a dancer to further injury (Macintyre 2000).
According to Geraci et al. (2005), a long-term successful outcome and prevention of re-injury are more likely
to occur if the focus of rehabilitation is on the restoration of the functional kinetic chain, rather than on a
specific injured tissue. The review by Seto and Brewster (1994) recommended the use of open and closed
kinetic chain exercises in order to improve proprioception and function after foot or ankle injuries. Closed
kinetic chain exercises are considered to be an integral part of accelerated knee/leg rehabilitation programs
due to their effect on increasing effectiveness of rehabilitation protocols (Kibler 2000, Lutz 1993).
C.
Th
era
peutic P
rocess
14
The authors recommend early identification of deficiencies in the kinetic chain and implementation of closed
kinetic chain exercises in the early phases of the conservative treatment of PAIS in professional ballet
dancers.
Ice therapy
Research showed to have no clear answers about the use of ice therapy for pain and swelling reduction after
an acute ankle sprain. Icepacks are not an effective method to reduce swelling and pain (van der Wees 2006),
even though the KNGF Guidelines recommend the use of icepacks and compression, combined with rest and
elevation (RICE) during the acute phase, to enhance patient sense of well-being. Bleakley et al. (2004) found
no evidence of optimal treatment results of ice for closed soft- tissue injuries.
Further control trials are needed to provide evidence-based guidelines in the treatment of acute soft-tissue
injuries.
The authors suggest that more research must be conducted regarding the effects of cryotherapy for the
conservative treatment of PAIS in professional ballet dancers. Nevertheless, the authors recommend the use
of protection measures, icepacks and compression, combined with rest and elevation (PRICE) during the
acute phase, in order to enhance patient sense of well-being.
Taping
The use of taping techniques or braces has been shown to reduce and prevent the risk of reoccurrence of the
ankle sprain in high-risk sports. Expert opinions and literature point out the positive effect of taping on
proprioception and muscle activity stimulation on stabilization of the ankle in ballet dancers with overuse
syndrome. Geyer et al. (1993) showed that applying tape leads to significant changes in muscle activity as
well as height and antagonist reflex patterns. These changes were particularly obvious in dancers with
unstable ankle and metatarsal joints. KNGF guidelines for the acute ankle sprain suggest that as a treatment
modality, taping technique have a negative effect on functional stability in the long run.
Therefore, the authors recommend the use of taping only in specific situations: preventing injury re-
occurrence, the first phases while returning to activity or under high performance demands. Taping must be
used as a preventive tool and not as a substitute for other treatment modalities such as ankle stabilization
exercises or self awareness.
Orthotics
In practice, the use of insoles is occasionally considered during the conservative treatment of PAIS in dancers
(expert opinions, 2010). Healthcare professionals prescribe foot orthoses (FOs) for treatment and prevention
of lower limb injuries. Tourné et al. (2010) showed that plantar orthotics is considered during conservative
treatment for CAI to treat any static disorders such as hindfoot varus or a flat foot valgus. These disorders can
contribute to future ankle traumatic inversion injuries and alter the proprioceptive control. According to
Douglas (2007) athletes with CAI showed a consistent loss of balance or postural control. The research
revealed positive effects of foot orthoses on postural control.
The authors do not recommend the direct use of orthotics for the conservative treatment of PAIS in
professional ballet dancers, although it is occasionally used in everyday practice for the general population.
C.
Th
era
peutic P
rocess
15
Nevertheless, the authors recommend the use of the orthotics in case there is a static disorder present,
limiting the function, activity or participation of the dancer (such as hindfoot varus or flat foot valgus).
Massage
Massage therapy is used as a stress reduction technique and to enhance recovery of ballet dancers in daily
practice more than a preventive or as a modality to restore injury (Nadia et al. 2010). Massage is also
contraindicated during the acute phase of an injury, as it can increase swelling and bleeding in the tissue,
prolonging the recovery time. Scientific literature is insufficient to conclude whether massage facilitates
recovery from a fatiguing effort. Both, tissue healing and a psychological effect of massage are areas that may
prove to be promising with further research (Moraska 2005).
The authors remark the need for further research for sports massage, especially well-designed studies,
involving therapists specifically trained to administer this type of therapy.
Furthermore, the authors recommend the use of specific massage techniques for the conservative treatment
of PAIS in professional ballet dancers only when there is a need to release muscle tension or to enhance
patient sense of well-being.
● Electrotherapy
There is no conclusive evidence to support the use of electrotherapy while treating professional ballet dancers
with PAIS. The evidence for the use of electrotherapy in sports related ankle injuries is only marginal as well
(Clijsen et al. 2007, van der Wees et al. 2006).
Therefore, the authors do not recommend the use of this therapeutic modality for the conservative treatment
of PAIS in professional ballet dancers, due to no additional value to the healing process.
Ultrasound
There is little and no high quality evidence available to support the use of ultrasound therapy for
musculoskeletal conditions of the lower limb (Shanks et al. 2010, Robertson and Baker, 2001), nevertheless,
this therapy continues to be widely used as an adjunct modality by physiotherapists (Wong et al. 2007). The
authors neither encourage nor discourage the use of ultrasound therapy for the conservative treatment of
PAIS in professional ballet dancers.
Acupuncture
Although acupuncture is not performed by physiotherapists, it was chosen by the authors of the guideline as
an additional modality, due to the suggestion from one of the interviewed experts. The effect of acupuncture
on pain and the use of this therapy for dancers remain controversial. According to the study carried by Vested
et al. (2009) no significant analgesic effect of acupuncture was found. Furthermore, the research suggested
that regarding the relation between acupuncture and pain, the psychological impact of the treatment remains
unclear. Kelly (2009) presents the benefit of acupuncture for patients with specific disorders such as: low back
pain, neck pain, chronic idiopathic, headache, migraine and knee osteoarthritis, although suggestions for
other conditions are still recommended.
C.
Th
era
peutic P
rocess
16
The use of acupuncture for pain reduction remains unclear according to the scientific literature. Despite no
evidence found concerning acupuncture specifically for PAIS, to the authors‟ knowledge this modality is
frequently used in the rehabilitation process of dancers for pain reduction.
Therefore, the authors neither encourage nor discourage the use of acupuncture for the conservative
treatment of PAIS in professional ballet dancers.
Ballet technique re-education
The strong connection between specific ballet dance related injuries and faulty technique or poor
biomechanics, in combination with other risk factors, is a common fact in professional dance practice
(Solomon et al. 2000, expert opinions, 2010). The dance research emphasizes neuromuscular re-education in
order to minimize the re-occurrence of injury and to accelerate the return to full ballet activity. Furthermore,
imagery and kinesthetic awareness are reported to have an effect on the relationship and alignment of
skeletal parts, by changing habitual neuromuscular patterns (Krasnow 2001).
The authors recommend emphasizing ballet technique re-education for the conservative treatment of PAIS in
professional ballet dancers in order to prevent the risk of reinjury and to enhance the full return to ballet
activity.
Load and loadability
The overtraining syndrome (OTS) is a common feature in elite athletes as well as in professional ballet
dancers. Because of the complexity, a combination of excessive training demands and other biologic,
psychological, and social stressors, OTS is difficult to measure (Purvis et al., 2010). Scientific dance research
shows that the risk of injuries increases due to the fatigue and overload (Brinson and Dick, 1996). The
prevention of overtraining and fatigue in a professional ballet setting can be avoided by introducing the
periodization model which is being widely used in sports (Wyon, 2010). Moreover, the use of the
multidimensional load/carriability model developed by The Nederlands Paramedisch Instituut (Hagenaars et
al. 2002) can help the physiotherapists to monitor the balance between dancers work load and his/her
loadability. The Healthy Dancer Diary (HDD), developed by Jacques van Rossum and Hanno van der Loo
bureau Adphys for the Amsterdam School of the Arts (The Netherlands) is a tool for dancers to get a better
understanding about the relationship between the physical and mental conditions (the loadability), and the
rehearsals or performances (the load). Healthcare practitioners could benefit from implementation of such a
tool, because it would allow them to design suitable prevention programs as well as diagnose and treat
injuries more effectively.
Therefore, the authors recommend graduated workloads, periodization and well scheduled rest/activity
periods in order to avoid fatigue and OTS.
The use of a multidimensional load/carriability model is suggested in order to monitor the balance between a
dancers work load and his/her loadability.
Additionally, the authors suggest implementation of a web-based training diary for dancers (HDD),
● Communication, information and advice
According to Lai et al. (2008) and expert opinions (2010), medical practitioners rarely communicate with each
other concerning a dancer. Furthermore, the lack of communication, concerning injured dancers, between

C.
Th
era
peutic P
rocess
17
dance teachers, choreographers, and company directors may also have negative a effect on the recovery
process. Therefore, developing appropriate and effective systems of communication, interaction, and mutual
understanding will assist the dancer in regaining and maintaining health (Solomon et al. 2000).
Numerous research studies emphasize the importance of information provided to the dancers, teachers and
choreographers about the anatomy, physiology, psychology, nutrition and dance bio-mechanics as it can
provide a valuable tool for assessing fitness level, controlling overtraining (“burnout”), improving ballet
technique and therefore preventing injuries (Koutedakis et al. 2008). In the Netherlands, significant efforts
were made by the physiotherapists (e.g. Willemsen T. book “Anatomy and Injuries” (2007) to inform dancers
about their own bodies and their susceptibility to injury.
Additionally, scientific research studies (Kromhout and Butzin, 1993, Kulik 1994) have shown that the use of
instructional software for physical education purposes improves learning time and, in addition, promotes
greater motivation and enjoyment of the students (Mohnsen 2001).
The authors recommend incorporating information and advice concerning the PAIS in the conservative
treatment plan for PAIS in professional ballet dancers, therefore improving the communication between the
Health team members, ballet staff and dancers.
In the authors opinion information and advice should consider the following arguments:
the specific pathology of PAIS;
the consequences of the pathology for the dancer in terms of functions, activities and participation;
the relation between the load and the dancers loadability given a specific situation (information about the
activity restriction and/or dosage);
the dancers injury perception and coping style;
the work place environment and professional demands;
implementing the multimedia instructional programs in order to make the provided information or advice
more appealing for the dancers.
C.
Th
era
peutic P
rocess
18
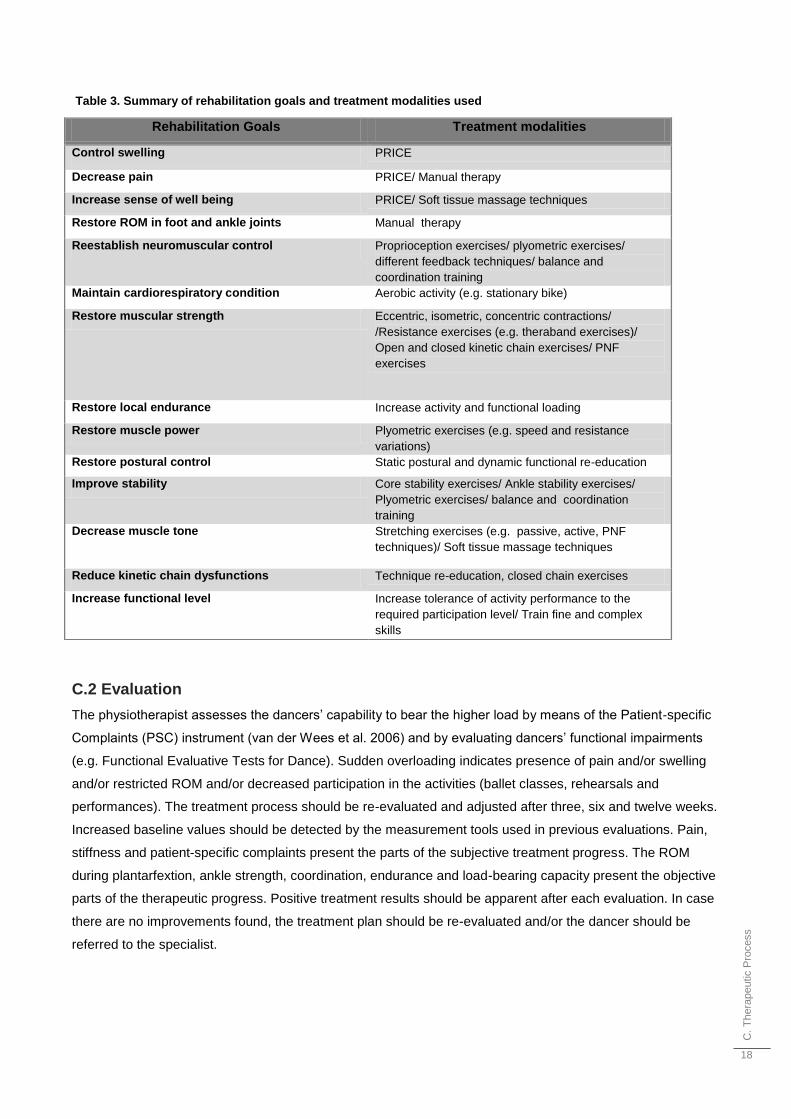
Table 3. Summary of rehabilitation goals and treatment modalities used
C.2 Evaluation
The physiotherapist assesses the dancers‟ capability to bear the higher load by means of the Patient-specific
Complaints (PSC) instrument (van der Wees et al. 2006) and by evaluating dancers‟ functional impairments
(e.g. Functional Evaluative Tests for Dance). Sudden overloading indicates presence of pain and/or swelling
and/or restricted ROM and/or decreased participation in the activities (ballet classes, rehearsals and
performances). The treatment process should be re-evaluated and adjusted after three, six and twelve weeks.
Increased baseline values should be detected by the measurement tools used in previous evaluations. Pain,
stiffness and patient-specific complaints present the parts of the subjective treatment progress. The ROM
during plantarfextion, ankle strength, coordination, endurance and load-bearing capacity present the objective
parts of the therapeutic progress. Positive treatment results should be apparent after each evaluation. In case
there are no improvements found, the treatment plan should be re-evaluated and/or the dancer should be
referred to the specialist.
Rehabilitation Goals Treatment modalities
Control swelling PRICE
Decrease pain PRICE/ Manual therapy
Increase sense of well being PRICE/ Soft tissue massage techniques
Restore ROM in foot and ankle joints Manual therapy
Reestablish neuromuscular control Proprioception exercises/ plyometric exercises/
different feedback techniques/ balance and
coordination training
Maintain cardiorespiratory condition Aerobic activity (e.g. stationary bike)
Restore muscular strength Eccentric, isometric, concentric contractions/
/Resistance exercises (e.g. theraband exercises)/
Open and closed kinetic chain exercises/ PNF
exercises
Restore local endurance Increase activity and functional loading
Restore muscle power Plyometric exercises (e.g. speed and resistance
variations)
Restore postural control Static postural and dynamic functional re-education
Improve stability Core stability exercises/ Ankle stability exercises/
Plyometric exercises/ balance and coordination
training
Decrease muscle tone Stretching exercises (e.g. passive, active, PNF
techniques)/ Soft tissue massage techniques
Reduce kinetic chain dysfunctions Technique re-education, closed chain exercises
Increase functional level Increase tolerance of activity performance to the
required participation level/ Train fine and complex
skills
Acknow
ledgem
ents
19
C.3 Preventing the PAIS
The physiotherapist should inform and give advice to the dancer about the specific measures (preferably
evidence-based) necessary to avoid the reoccurrence of symptoms. The dancer should be advised to monitor
the balance between load and personal loadability, to use the supportive devices (tape or bandage) only
during high level activities (performances) and wear the footwear after work that permits ultimate comfort for
the ankle (Willemsen 2007). Instruction to continue varied exercise training in addition to the dancers usual
activities after the therapy process is accomplished should be given as well.
Acknowledgements
The authors want to express their gratitude to the following:
the client, Aina Bilkins and Ronald Klassen (HNB), for their continuous encouragement and assistance;
the coach, RMT. RPT. Rolf Hoogland for his guidance provided during the review writing process;
John ten Kulve, Ted Willemsen, Anita Radier, Marleen Grol, Rob Oskam, Jan Simons and MD, PhD. C.Niek
van Dijk for their indispensible collaboration during the project.
Special thanks go to the external advisors: Ana Aguilar, Aurelija Galvelyte, Juncal Roman and Vasiliki Folia.
Refe
rences
20
References
1. Arnold BL, Docherty CL. Low-Load Eversion Force Sense,
Self-Reported Ankle Instability, and Frequency of Giving
Way. Journal of Athletic Training 2006;41(3):233–238
2. Batson G. Updtae on Proprioception: Considerations for
Dance Education. Journal of Dance Medicine & Science.
2009;13 (2):35-41
3. Behm DG, Drinkwater EJ, Willardson JM, Cowley PM. The
use of instability to train the core musculature. Applied
Physiology, Nutrition and Metabolism. 2010 Feb; 35(1):91-
108.
4. Bleakley CM, McDonough SM, MacAuley DC. Some
conservative strategies are effective when added to
controlled mobilization with external support after acute
ankle sprain: a systematic review. Australian Journal of
Physiotherapy. 2008; 54(1):7-20.
5. Bleakley C, McDonough S, MacAuley D. The use of ice in
the treatment of acute soft-tissue injury: a systematic
review of randomized controlled trials. The American
Journal of Sports Medicine. 2004;32(1):251-261
6. Bliss LS, Teeple P. Core stability: the centerpiece of any
training program. Current Sports Medicine Reports.
2005;4(3):179-83.
7. Brantingham JW, Globe G, Pollard H, Hicks M, Korporaal
C, Hoskins W. Manipulative therapy for lower extremity
conditions: expansion of literature review. Journal of
Manipulative Physio Therapy. 2009 Jan;32(1):53-71
8. Brinson P, Dick F. Fit to Dance?.United Kingdom: Calouste
Gulbenkian Foundation; 1996. p. 61-68
9. Clijsen R, Taeymans J, Clarys P, Cabri J.
Sportphysiotherapy interventions in acute inversion trauma:
evidence based?.Sportverletz Sportschaden.
2007;21(2):71-6
10. Cloak R, Nevill AM, Clarke F, Day S, Wyon MA. Vibration
training improves balance in unstable ankles. International
Journal of Sports Medecine. 2010;31(12):894-900
11. Douglas H. Effects of Foot Orthoses on Patients with
Chronic Ankle Instability. Journal of the American Podiatric
Medical Association. 2007; 97 (1) :19-30
12. Emery K, De Serres SJ, McMillan A, Côté JN. The effects
of a Pilates training program on arm-trunk posture and
movement. Clinical Biomechanics (Bristol, Avon).
2010;25(2):124-30
13. Geyer M, Bergmann C, Siebert W. Overuse syndrome in
ballet: study of the effect of a tape bandage of the upper
ankle joint with motion analysis.Sportverletz Sportschaden.
1993;7(2):78-83.
14. Geraci MC Jr, Brown W.Evidence-based treatment of hip
and pelvic injuries in runners.Phys Med Rehabil Clin N Am.
2005;16(3):711-47Hagenaars LH, Bernards AT,
Oostendorp RA. The multidimensional load/carriability
model. Amersfoort, Nederlands: Dutch National Institute of
Allied Health Professions; 2002.
15. Gürsel Y, Ulus Y, Bilgiç A, Dinçer G, van der Heijden GJ.
Adding ultrasound in the management of soft tissue
disorders of the shoulder: a randomized placebo-controlled
trial. Physical Therapy. 2004;84(4):336-43.
16. Han K, Ricard M, Fellingham G. Effects of a 4-week
exercise program on balance using elastic tubing as a
perturbation force for individuals with a history of ankle
sprains. The Journal of Orthopaedic and Sports Physical
Therapy 2009;39(4):246-255
17. Holmes A, Delahunt E. Treatment of common deficits
associated with chronic ankle instability. Sports Med.
2009;39(3):207-24
18. Hughes T, Rochester P. The effects of proprioceptive
exercise and taping on proprioception in subjects with
functional ankle instability: a review of the literature.
Physical Therapy in Sport. 2008;9(3):136-147
19. Ismail M, Ibrahim M, Youssef E, Shorbagy K. Plyometric
training versus resistive exercises after acute lateral ankle
sprain. Foot and Ankle International. 2010 Jun;31(6):523-
30
20. Kelly R. Acupuncture for pain. Am Fam Physician.
2009;80(5):481-4.
21. Keus SH,.Hendriks HJ, Bloem BR, Bredero-Cohen AB,
Goede CT,van Haaren M. KNGF Guidelines for physical
therapy in patients with parkinson disease. 2004;114 (3).
22. Kibler WB. Closed kinetic chain rehabilitation for sports
injuries. Phys Med Rehabil Clin N Am. 2000;11(2):369-84.
23. Koutedakis Y, Clarke F, Wyon M, Aways D, Owolabi E.
Muscular Strength: Applications for Dancers. Medical
Problems of Performing Artists, 2009;24(4):157
24. Koutedakis Y, Owolabi EO, Apostolos M. Dance
biomechanics: a tool for controlling health, fitness, and
training. Journal of Dance Medicine & Science.
2008;12(3):83-90
25. Krasnow D, Monasterio R, Chatfield S. Emerging
Concepts of Posture and Alignment. [online]. 2001 [cited
2011 Jan 1]. Available from:
http://www.med.nyu.edu/hjd/harkness/assets/functional_e
valuative_tests_revised.pdf
26. Kromhout O.M, Butzin S.M. Integrating Computers into the
Elementary School Curriculum: an evaluation of nine
Project CHILD model schools. Journal of Research on
Computing in Education. 1993; 26: 55-69.
27. Kulik A. Meta-analytic studies of findings on computer-
based instruction. In: Baker EL, Harold F. Technology
assessment in education and training. United States:
O'NeilUniversity of Michigan; 1994. p. 26.
28. Kurer. The Foot & Ankle Disability Index (FADI) Score -
Sports Module. www.orthopaedicscores.com [online]. 2006
[cited 2011 Jan 1]. Available from:
http://www.orthopaedicscore.com/scorepages/foot_and_an
kle_disability_index_fadi_sport.html
29. Liederbach M. Functional Evaluative Tests For Dance.
[online]. 1994 [cited 2011 Jan 1]. Available from:
http://www.med.nyu.edu/hjd/harkness/assets/functional_ev
aluative_tests_revised.pdf
30. Lynch S, Renström P.Treatment of acute lateral ankle
ligament rupture in the athlete. Conservative versus
surgical treatment. Sports Med. 1999;27(1):61-71.
31. Lutz GE, Palmitier RA, An KN and Chao EY. Comparison
of tibiofemoral joint forces during open-kinetic-chain and
closed-kinetic-chain exercises. The Journal of Bone and
Joint Surgery. 1993;75(5):732-739
32. Macintyre J, Joy E.Foot and ankle injuries in dance.Clin
Sports Med. 2000 Apr;19(2):351-68.
33. Martin RL, Burdett RG, Irrgang JJ. Development of the Foot
and Ankle Disability Index (FADI) J Orthop Sports Phys
Ther. 1999;29 . Available from:
http://www.orthopaedicscore.com/scorepages/foot_and_an
kle_disability_index_fadi.html
34. McKeon P, Hertel J.Systematic review of postural control
and lateral ankle instability, part II: is balance training
clinically effective?. J Athl Train. 2008 May-Jun;43(3):305-
15
35. McNair PJ, Stanley SN. Effect of passive stretching and
jogging on the series elastic muscle stiffness and range of
Refe
rences
21
motion of the ankle joint. British Journal of Sports Medicine.
1996;30:313-317.
36. Mohnsen B. Using Instructional Software to Meet National
Physical Education Standards. The Journal of Physical
Education, Recreation & Dance. 2001; vol 72
37. Moraska A. Sports massage. A comprehensive review. J
Sports Med Phys Fitness. 2005; Sep;45(3):370-80.
38. Nadia S, Critchfield B. First Aid for Dancers.International
Association for Dance Medicine and Science. 2010Omkar
S, Vishwas S, Tech B. Yoga techniques as a means of core
stability training. Journal of Bodywork and Movement
Therapies. 2009;13(1):98-103.
39. Purvis D, Gonsalves S, Deuster PA. Physiological and
psychological fatigue in extreme conditions: overtraining
and elite athletes. 2010; 2(5):442-50.
40. Ramel E. Self-Estimated Functional Inability because of
Pain. [online]. 2001 [cited 2011 Jan 1]. Available from:
http://www.prevent.se/Documents/prevent.se/arbetsmiljoar
bete/systematiskt%20arbetmiljoarbete/hjalpdokument/hjalp
dokument_scen_eng_dancers_self-estimated.pdf
41. Reid DC. Prevention of hip and knee injuries in ballet
dancers. Sports Medecine. 1988;6(5):295-307
42. Richter M. Prof. Dr. Martinus Richter. [online]. 2004 [cited
2011 Jan 1]. Available from: http://www.foot-
trauma.org/uk/vase.htm
43. Richter M, Zech S, Geerling J, Frink M, Knobloch K, Krettek
C. New foot and ankle outcome score: Questionnaire
based, subjective, Visual-Analogue-Scale, validated and
computerized.Foot and ankle surgery. 2006;12
44. Robertson V ,Baker K. A Review of Therapeutic
Ultrasound: Effectiveness Studies. Physical Therapy. 2001;
81(7) 1339-1350
45. Shanks P, Curran M, Fletcher P, Thompson R. The
effectiveness of therapeutic ultrasound for musculoskeletal
conditions of the lower limb: A literature review.
2010;20(4):133-9.
46. Seto JL, Brewster CE. Treatment approaches following foot
and ankle injury. Clin Sports Med. 1994;13(4):695-718
47. Solomon R, Brown T, Gerbino PG, Micheli LJ. The young
dancer. 2000;19(4):717-39.
48. Twitchett EA, Koutedakis Y, Wyon MA. Physiological
fitness and professional classical ballet performance: a
brief review. Journal of Strength Conditioning Research.
2009;23(9):2732-40
49. Tourné Y, Besse JL, Mabit C. Chronic ankle instability.
Which tests to assess the lesions? Which therapeutic
options?. Orthop Traumatol Surg Res. 2010;96(4):433-46.
50. Van der Wees PJ, Lenssen AF, Hendriks EJ, Stomp DJ,
Dekker J, de Bie RA. Effectiveness of exercise therapy and
manual mobilisation in ankle sprain and functional
instability: a systematic review. Australian Journal of
Physiotherapy. 2006;52(1):27-37.
51. Van der Wees J, Lenssen A, Feijts Y, Bloo H, van Moorse
S, Ouderland R et al. KNGF Guideline for Physical Therapy
in patients with acute ankle sprain - Practice Guidelines.
2006;5 (116)
52. Van Der Windt DA, Van Der Heijden GJ, Van Den Berg
SG, Ter Riet G, De Winter AF, Bouter LM. Ultrasound
therapy for acute ankle sprains. Cochrane Database
Systematic Review. 2002;(1):CD001250.
53. Van Dijk N, Anterior and Posterior Ankle Impingement. Foot
Ankle Clin N Am. 2006;11:663–683
54. Vested M,Gøtzsche P, HróbjartssonG A. Acupuncture
treatment for pain: systematic review of randomised clinical
trials with acupuncture, placebo acupuncture, and no
acupuncture .2009; 338:3115
55. Weiss D, Rist R, Grossman G. When Can I Start Pointe
Work? Guidelines for Initiating Pointe Training. Reprinted
from the Journal of Dance Medicine & Science.
2009;13(3):90-92
56. Wewers ME, Lowe NK. A critical review of visual
analogue scales in the measurement of clinical
phenomena. Research in Nursing & Health 2007;
13(4):227–236
57. World Health Organization. [online]. [last update January
2011]. URL:
http://www.who.int 58. Willardson J. Core stability training: applications to sports
conditioning programs..J Strength Cond Res. 2007
;21(3):979-85.
59. Willemsen T. Anatomy and injuries. 1st ed. Amsterdam,
Nederlands: Obey Willemsen; 2007. p. 121-130
60. Willson JD, Dougherty CP, Ireland ML, Davis IM. Core
Stability and Its Relationship to Lower Extremity Function
and Injury. Journal of the American Academy of
Orthopaedic Surgeons,2005;13(5):316-325.
61. Wong RA, Schumann B, Townsend R, Phelps CA. A
survey of therapeutic ultrasound use by physical therapists
who are orthopaedic certified specialists. Physical Therapy.
2007;87(8):986-94.
62. Wyon M.Preparing to perform: periodization and danceJ
Dance Med Sci. 2010;14(2):67-72.
63. Wyon, Matthew; Felton, Lee; Galloway, Shaun. A
Comparison of Two Stretching Modalities on Lower-Limb
Range of Motion Measurements in Recreational Dancers.
Journal of Strength & Conditioning Research:
2009;23(7):2144-2148.
64. Zech A, Hübscher M, Vogt L, Banzer W, Hänsel F, Pfeifer
K. J Athl Train. Balance training for neuromuscular control
and performance enhancement: a systematic review.
2010;45(4):392-403.
Supple
me
nts
22
Supplements
Supplement 1. Conclusions and recommendations
Explanation of evidence levels
The levels of evidence used on the conclusions of the guideline have been defined in Dutch national
agreements (EBRO/CBO) and used as well by KNGF- guidelines.
Four levels of evidence are distinguished depending on the quality of the studies on which they are based:
Level 1: a study of A1 quality, or at least two independent studies of A2 quality
Level 2: one study of A2 quality or at least two independent studies of B quality
Level 3: one study of B or C quality
Level 4: expert opinion
Quality categories
A1 Systematic review including at least two independent studies of A2 quality
A2 Randomized double-blind comparative clinical trial of sound quality and sufficient size
B Comparative studies not meeting all the quality criteria mentioned under A2 (including case-control studies
and cohort studies)
C Non-comparative studies
D Opinions of experts, e.g. physical therapist interviewed by the authors of this guideline.
Conservative treatment plan of PAIS for professional ballet dancers
Manual Therapy
The authors of the guideline recommend passive mobilizations of the ankle joints for the treatment of professional
ballet dancers with PAIS in order to improve pain and regain mobility before starting active exercise therapy
(expert opinions). Furthermore, manually guided active ROM exercises (extrinsic feedback) are recommended
when treating PAIS in order to stimulate intrinsic feedback encouraging the correct movement patterns (expert
opinions). Additionally, active manipulations using McKenzie Belt technique are suggested. (level 1), (level 4)
Quality of evidence A1: (Brantingham et al. 2009, Bleakley et al. 2008, van der Wees et al. 2006, van der Wees et al.
2006)
Quality of evidence D: expert opinions, 2010
Stability exercise of the ankle
The authors of the guideline strongly recommend ankle stability exercises for the conservative treatment of PAIS
in professional ballet dancers when acute or chronic ankle instability is diagnosed.(level 1)
Quality of evidence A1: (McKeon et al., 2008)
Quality of evidence C: (Cloak et al, 2010, Hank et al., 2009, Arnold et al 2006, Holmes et al., 2009)
Supple
me
nts
23
Stretching exercises of the ankle
The authors of the guideline recommend active resistance and dynamic stretching exercises for the conservative
treatment of PAIS in professional ballet dancers who present no chronic or structural ankle instability.
Quality of evidence A1: (Wyon et al., 2009)
Quality of evidence A2: (Nair et al, 1996)
Quality of evidence C: (Reid, 1988)
Proprioception/ neuro muscular training
The authors of the guideline strongly recommend proprioception training in which the combination of functional
and activity related exercises are considered. Further high-quality clinical trials are needed to enhance the
evidence base and to help physical therapists to select effective and more specific strategies for dancers during
neuromuscular training.
Quality of articles A1: ( Willardson 2007, Zech et al. 2010, van der Wees et al. 2006)
Quality of articles C: (Batson 2009)
Endurance training
The authors of the guideline recommend emphasizing endurance training for the conservative treatment of PAIS
in professional ballet dancers. Furthermore, endurance training must be incorporated in the rehabilitation process
from the first stages, in order to prevent the decrease of the dancers‟ aerobic capacity and therefore to maintain
the loadability. (level 1), (level 3)
Quality of evidence C: (Brinson and Dick, 1996)
Quality of evidence A1: (Twitchett, 2009)
Strength training
The authors of the guideline are of the opinion that strengthening exercises for the ankle and foot (in combination
with the strengthening exercises for the kinetic chain) should be recommended while treating PAIS in
professional ballet dancers. Furthermore, the authors of the guideline recommend additional implementation of
plyometric training in order to improve ankle functional stability. (level 1), (level 3), (level 4)
Quality of evidence A1: (van der Wees et al. 2006, Koutedakis et al. 2009)
Quality of evidence B: ( Ismail et al. 2010)
Quality of evidence C: (Brinson and Dick 1996)
Quality of evidence D: expert opinions, 2010
Core stability exercises
The authors of the guideline suggest core stability training as part of an exercise program for the conservative
treatment of PAIS in professional ballet dancers. Core stability training should be considered in a specific phase
of the rehabilitation process in order to reduce the load and to enhance the control in the lower extremities.
Specific Pilates or Yoga exercises can be used as supplementary components of core stability training. (level 1),
(level3)
Supple
me
nts
24
Quality of evidence A1: (Willardson et al. 2007)
Quality of evidence B: (Emery et al. 2010)
Quality of evidence C: (Bliss et al. 2005, Behm et al. 2010, Willson et al. 2005, Weiss et al. 2009, Omkar et al. 2009)
Kinetic chain exercises
The authors of the guideline recommend early identification of deficiencies in the kinetic chain and
implementation of closed kinetic chain exercises in the early phases of the conservative treatment of PAIS in
professional ballet dancers. (level 1), (level 3), (level 4)
Quality of evidence A1: (Macintyre 2000, Geraci et al.2005, Seto and Brewster 1994, Kibler 2000)
Quality of evidence C: (Lutz, 1993)
Quality of evidence D: expert opinions, 2010
Ice therapy
The authors of the guideline suggest that more research must be conducted regarding the effects of cryotherapy
for the conservative treatment of PAIS in professional ballet dancers. Nevertheless, the guideline recommends
the use of protection measures, icepacks and compression, combined with rest and elevation (PRICE) during the
acute phase, in order to enhance patient sense of well-being. (level 1)
Quality of articles A1: (van der Wees et al. 2006, Bleakley et al. 2004)
Taping
● The authors recommend the use of taping in specific situations: preventing injury re-occurrence, the first phases
while returning to activity or under a high performance demands. (level 3)
Quality of articles C: (Geyer et al., 1993)
● Taping must be used as a preventive tool and not as a substitute for other treatment modalities such as ankle
stabilization exercises or self awareness. (level 1)
Quality of articles A1: (van der Wees et al. 2006)
Orthotics
● The authors do not recommend the direct use of orthotics for the conservative treatment of PAIS in professional
ballet dancers, although it is occasionally used in everyday practice for the general population. Nevertheless, the
authors recommend the use of the orthotics in case there is a static disorder present, limiting the function, activity
or participation of the dancer (such as if hindfoot varus or a flat foot valgus is present). (level 1),(level 3),(level 4)
Quality of articles A1: (Douglas 2007)
Quality of articles C: (Tourné et al. 2010)
Quality of articles D: expert opinions, 2010
Supple
me
nts
25
Massage
The authors of this guideline remark the need for further research into sports massage, especially well-designed
studies utilizing therapists specifically trained to administer this type of therapy. Furthermore, the authors
recommend the use of specific massage techniques for the conservative treatment of PAIS in professional ballet
dancers only when there is a need to release muscle tension or to enhance patient sense of well-being. (level 1),
(level 3)
Quality of evidence A1: (Moraska 2005)
Quality of evidence C: (Nadia et al, 2010)
Electrotherapy
The authors of the guideline do not recommend the use of this therapeutic modality for the conservative
treatment of PAIS in professional ballet dancers, due to no additional value to the healing process. (level 1)
Quality of evidence A1: (Clijsen et al. 2007, van der Wees et al. 2006)
Ultrasound
The authors neither encourage nor discourage the use of ultrasound therapy for the conservative treatment of
PAIS in professional ballet dancers. (level 1), (level 3)
Quality of evidence A1 :(Robertson and Baker 2001, Shanks et al. 2010)
Quality of evidence C: (Wong et al. 2007)
Acupuncture
● The authors neither encourage nor discourage the use of acupuncture for the conservative treatment of PAIS in
professional ballet dancers, as the use of acupuncture for pain reduction remains unclear according to the
scientific literature. Despite no evidence found concerning acupuncture specifically for PAIS, to the authors‟
knowledge this modality is frequently used in the rehabilitation process of dancers for pain management. (level 1)
(level 4).
Quality of articles A1: (Kelly 2009, Vested et al. 2009)
Quality of evidence D: expert opinions, 2010
Technique re-education
The authors of the guideline recommend emphasizing ballet technique re-education for the conservative
treatment of PAIS in professional ballet dancers in order to prevent the risk of reinjury and to enhance the full
return to ballet activity. (level 3), (level 4)
Quality of evidence C: (Solomon et al. 2000)
Quality of evidence D: expert opinions, 2010
Supple
me
nts
26
Load and loadability
The authors of the guideline recommend graduated workloads, the periodization and well scheduled rest/activity
periods in order to avoid fatigue and OTS. (level 1), (level 3)
Quality of evidence A1: (Purvis et al. 2010)
Quality of evidence C: (Brinson and Dick 1996)
Quality of evidence A1: (Wyon 2010)
The use of a multidimensional load/carriability model is suggested in order to monitor the balance between
dancers work load and his/her loadability. (Hagenaars et al. 2002)
The authors of the guideline suggest implementation of a web-based training diary for dancers (HDD).(Laws
2009)
Communication, information and advice
The authors of the guideline recommend incorporating information and advice concerning the PAIS in the
conservative treatment plan for PAIS in professional ballet dancers, therefore improving the communication
between the Health team members, ballet staff and dancers. (level 3)
Quality of evidence C: (Solomon et al. 2000, Koutedakis et al. 2008, Willemsen, 2007)
Additionally, the authors of the guideline encourage the use of instructional software for physical education purposes in
order to promote greater motivation and enjoyment for dancers while learning about the PAIS (Kromhout and Butzin 1993,
Kulik 1994, Mohnsen, 2001).
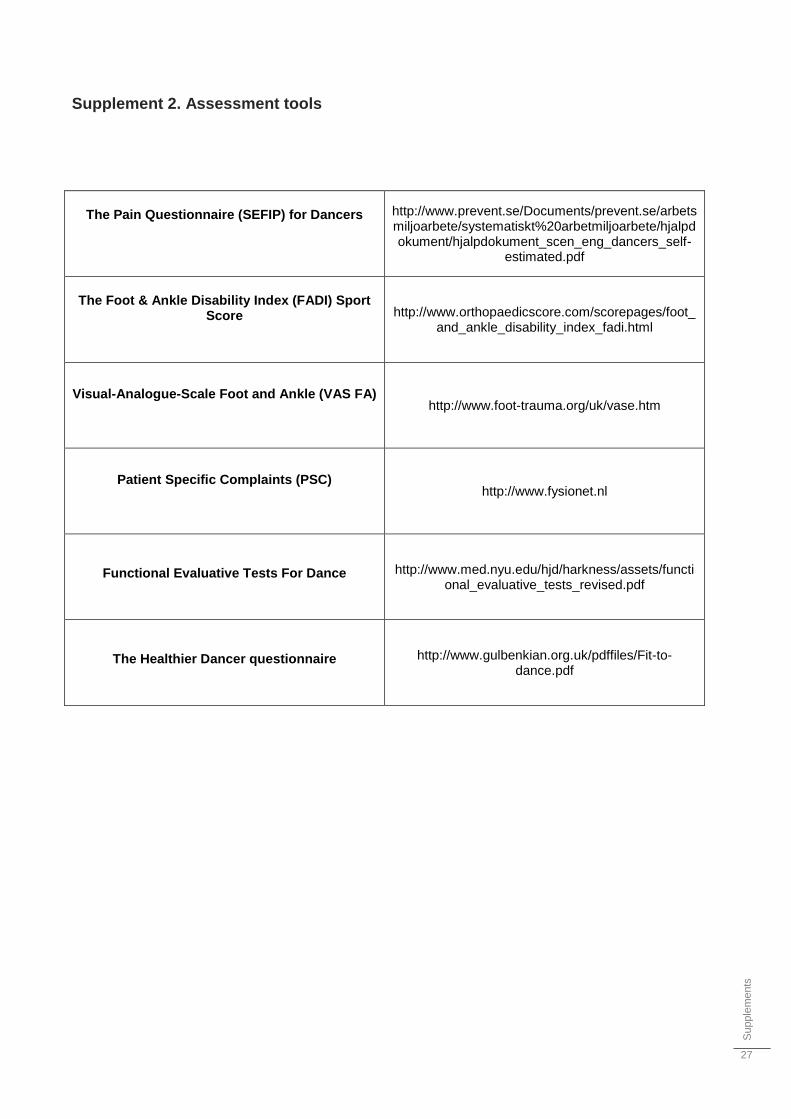
Supple
me
nts
27
Supplement 2. Assessment tools
The Pain Questionnaire (SEFIP) for Dancers
http://www.prevent.se/Documents/prevent.se/arbetsmiljoarbete/systematiskt%20arbetmiljoarbete/hjalpdokument/hjalpdokument_scen_eng_dancers_self-
estimated.pdf
The Foot & Ankle Disability Index (FADI) Sport
Score
http://www.orthopaedicscore.com/scorepages/foot_and_ankle_disability_index_fadi.html
Visual-Analogue-Scale Foot and Ankle (VAS FA)
http://www.foot-trauma.org/uk/vase.htm
Patient Specific Complaints (PSC)
http://www.fysionet.nl
Functional Evaluative Tests For Dance http://www.med.nyu.edu/hjd/harkness/assets/functional_evaluative_tests_revised.pdf
The Healthier Dancer questionnaire http://www.gulbenkian.org.uk/pdffiles/Fit-to-dance.pdf
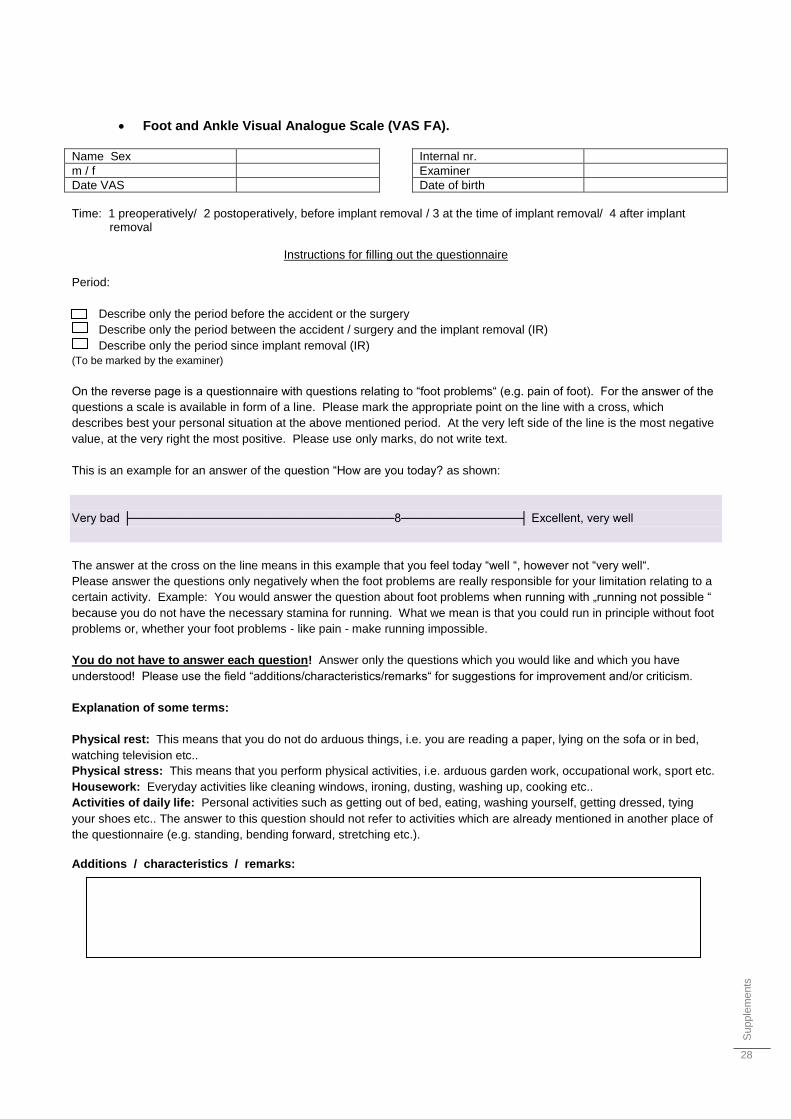
Supple
me
nts
28
Foot and Ankle Visual Analogue Scale (VAS FA).
Name Sex
m / f
Date VAS
Internal nr.
Examiner
Date of birth
Time: 1 preoperatively/ 2 postoperatively, before implant removal / 3 at the time of implant removal/ 4 after implant
removal
Instructions for filling out the questionnaire Period:
Describe only the period before the accident or the surgery
Describe only the period between the accident / surgery and the implant removal (IR)
Describe only the period since implant removal (IR)
(To be marked by the examiner)
On the reverse page is a questionnaire with questions relating to “foot problems“ (e.g. pain of foot). For the answer of the
questions a scale is available in form of a line. Please mark the appropriate point on the line with a cross, which
describes best your personal situation at the above mentioned period. At the very left side of the line is the most negative
value, at the very right the most positive. Please use only marks, do not write text.
This is an example for an answer of the question “How are you today? as shown:
Very bad ├───────────────────────────────8──────────────┤ Excellent, very well
The answer at the cross on the line means in this example that you feel today “well “, however not “very well“.
Please answer the questions only negatively when the foot problems are really responsible for your limitation relating to a
certain activity. Example: You would answer the question about foot problems when running with „running not possible “
because you do not have the necessary stamina for running. What we mean is that you could run in principle without foot
problems or, whether your foot problems - like pain - make running impossible.
You do not have to answer each question! Answer only the questions which you would like and which you have
understood! Please use the field “additions/characteristics/remarks“ for suggestions for improvement and/or criticism.
Explanation of some terms:
Physical rest: This means that you do not do arduous things, i.e. you are reading a paper, lying on the sofa or in bed,
watching television etc..
Physical stress: This means that you perform physical activities, i.e. arduous garden work, occupational work, sport etc.
Housework: Everyday activities like cleaning windows, ironing, dusting, washing up, cooking etc..
Activities of daily life: Personal activities such as getting out of bed, eating, washing yourself, getting dressed, tying
your shoes etc.. The answer to this question should not refer to activities which are already mentioned in another place of
the questionnaire (e.g. standing, bending forward, stretching etc.).
Additions / characteristics / remarks:
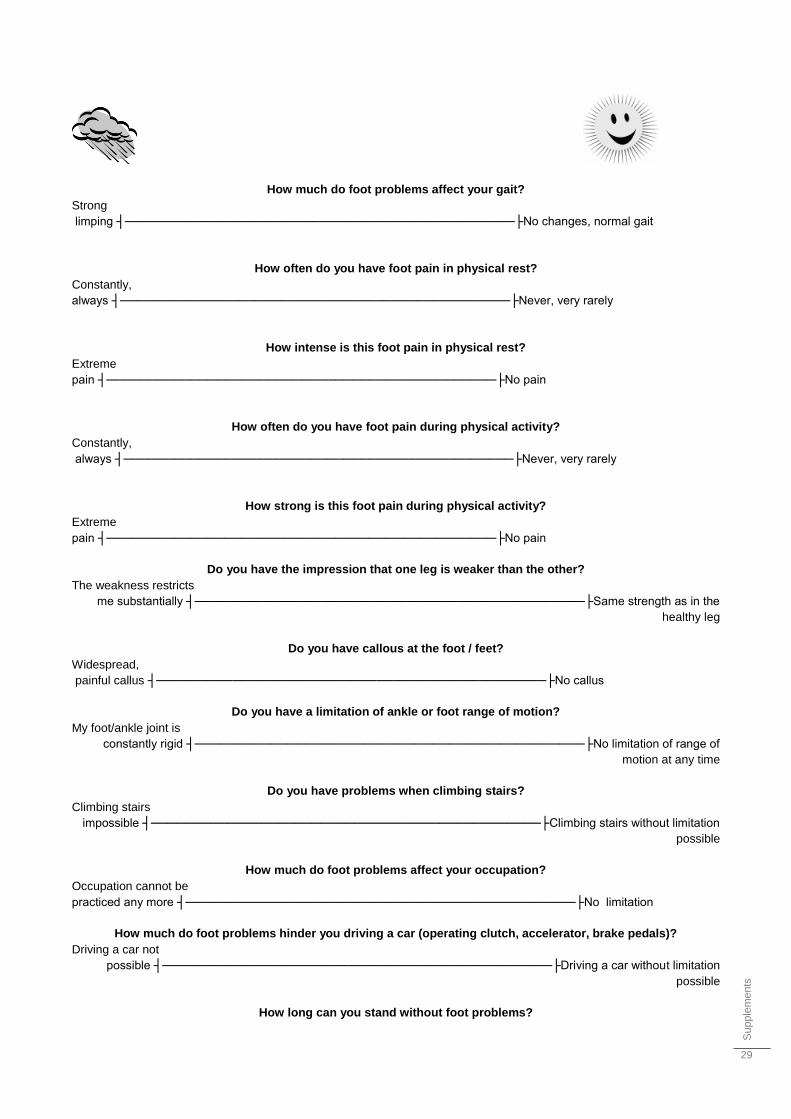
Supple
me
nts
29
How much do foot problems affect your gait?
Strong
limping ┤──────────────────────────────────────────────├No changes, normal gait
How often do you have foot pain in physical rest?
Constantly,
always ┤──────────────────────────────────────────────├Never, very rarely
How intense is this foot pain in physical rest?
Extreme
pain ┤──────────────────────────────────────────────├No pain
How often do you have foot pain during physical activity?
Constantly,
always ┤──────────────────────────────────────────────├Never, very rarely
How strong is this foot pain during physical activity?
Extreme
pain ┤──────────────────────────────────────────────├No pain
Do you have the impression that one leg is weaker than the other?
The weakness restricts
me substantially ┤──────────────────────────────────────────────├Same strength as in the
healthy leg
Do you have callous at the foot / feet?
Widespread,
painful callus ┤──────────────────────────────────────────────├No callus
Do you have a limitation of ankle or foot range of motion?
My foot/ankle joint is
constantly rigid ┤──────────────────────────────────────────────├No limitation of range of
motion at any time
Do you have problems when climbing stairs?
Climbing stairs
impossible ┤──────────────────────────────────────────────├Climbing stairs without limitation
possible
How much do foot problems affect your occupation?
Occupation cannot be
practiced any more ┤──────────────────────────────────────────────├No limitation
How much do foot problems hinder you driving a car (operating clutch, accelerator, brake pedals)?
Driving a car not
possible ┤──────────────────────────────────────────────├Driving a car without limitation
possible
How long can you stand without foot problems?
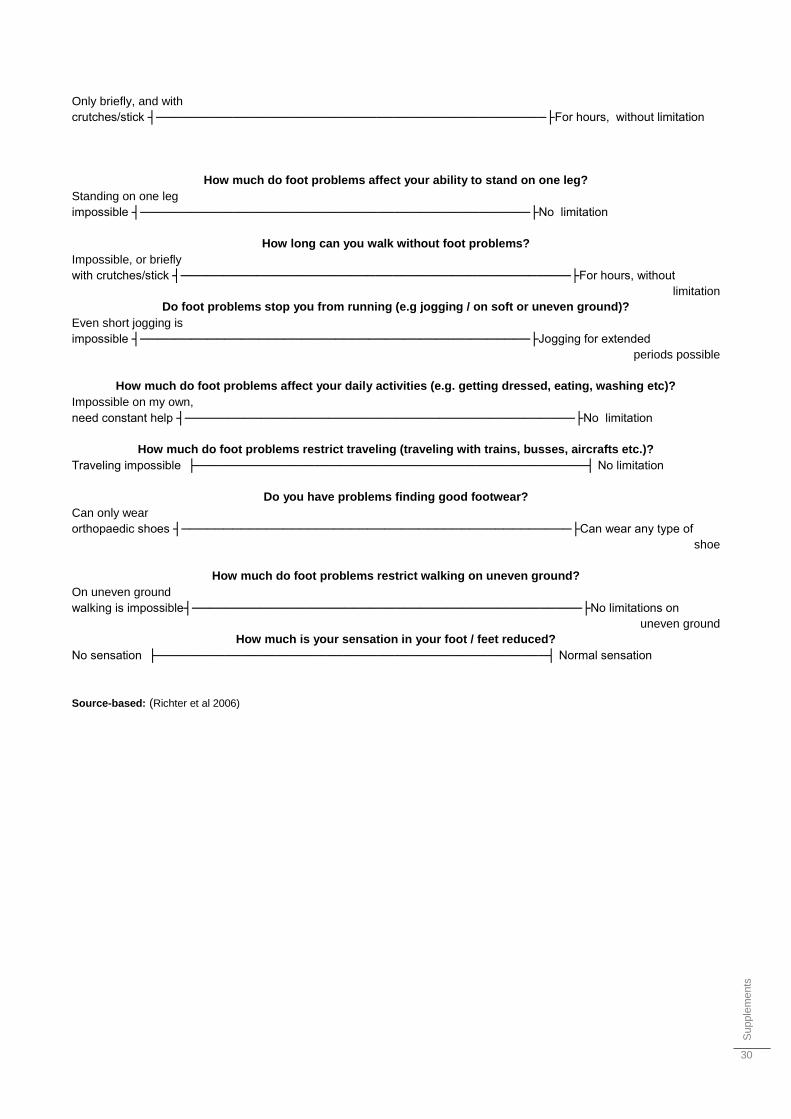
Supple
me
nts
30
Only briefly, and with
crutches/stick ┤──────────────────────────────────────────────├For hours, without limitation
How much do foot problems affect your ability to stand on one leg?
Standing on one leg
impossible ┤──────────────────────────────────────────────├No limitation
How long can you walk without foot problems?
Impossible, or briefly
with crutches/stick ┤──────────────────────────────────────────────├For hours, without
limitation
Do foot problems stop you from running (e.g jogging / on soft or uneven ground)?
Even short jogging is
impossible ┤──────────────────────────────────────────────├Jogging for extended
periods possible
How much do foot problems affect your daily activities (e.g. getting dressed, eating, washing etc)?
Impossible on my own,
need constant help ┤──────────────────────────────────────────────├No limitation
How much do foot problems restrict traveling (traveling with trains, busses, aircrafts etc.)?
Traveling impossible ├──────────────────────────────────────────────┤ No limitation
Do you have problems finding good footwear?
Can only wear
orthopaedic shoes ┤──────────────────────────────────────────────├Can wear any type of
shoe
How much do foot problems restrict walking on uneven ground?
On uneven ground
walking is impossible┤──────────────────────────────────────────────├No limitations on
uneven ground
How much is your sensation in your foot / feet reduced?
No sensation ├──────────────────────────────────────────────┤ Normal sensation
Source-based: (Richter et al 2006)
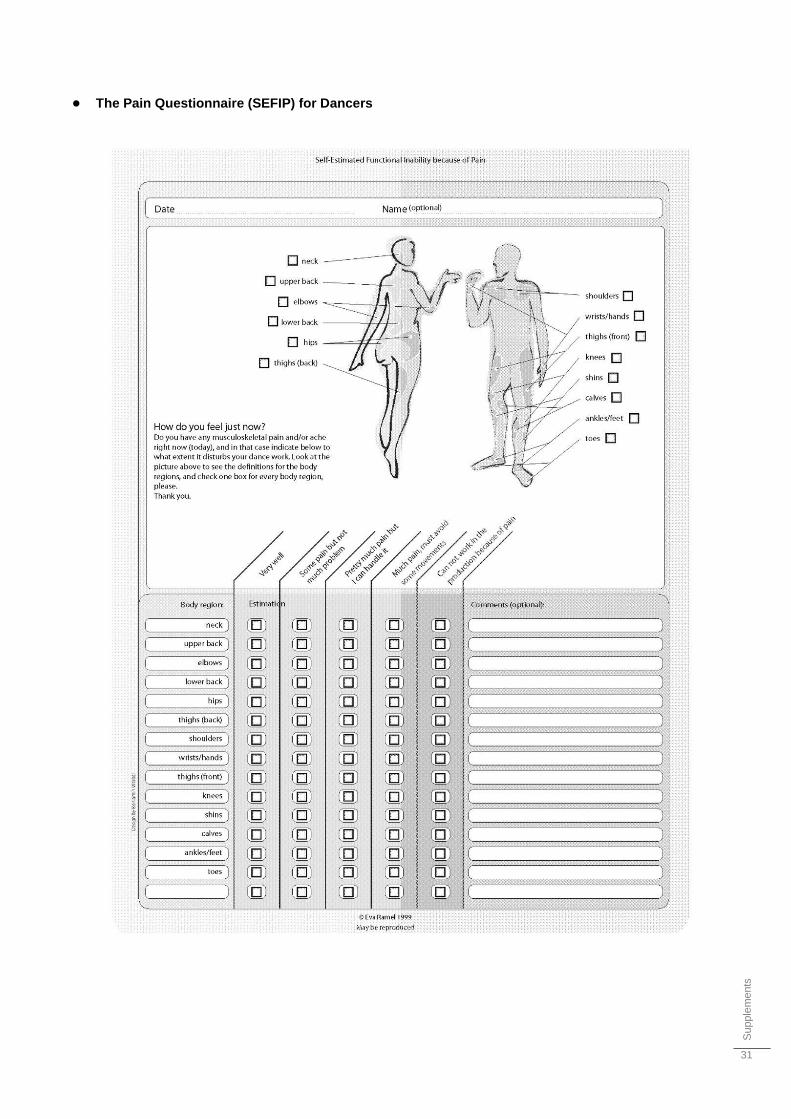
Supple
me
nts
31
● The Pain Questionnaire (SEFIP) for Dancers
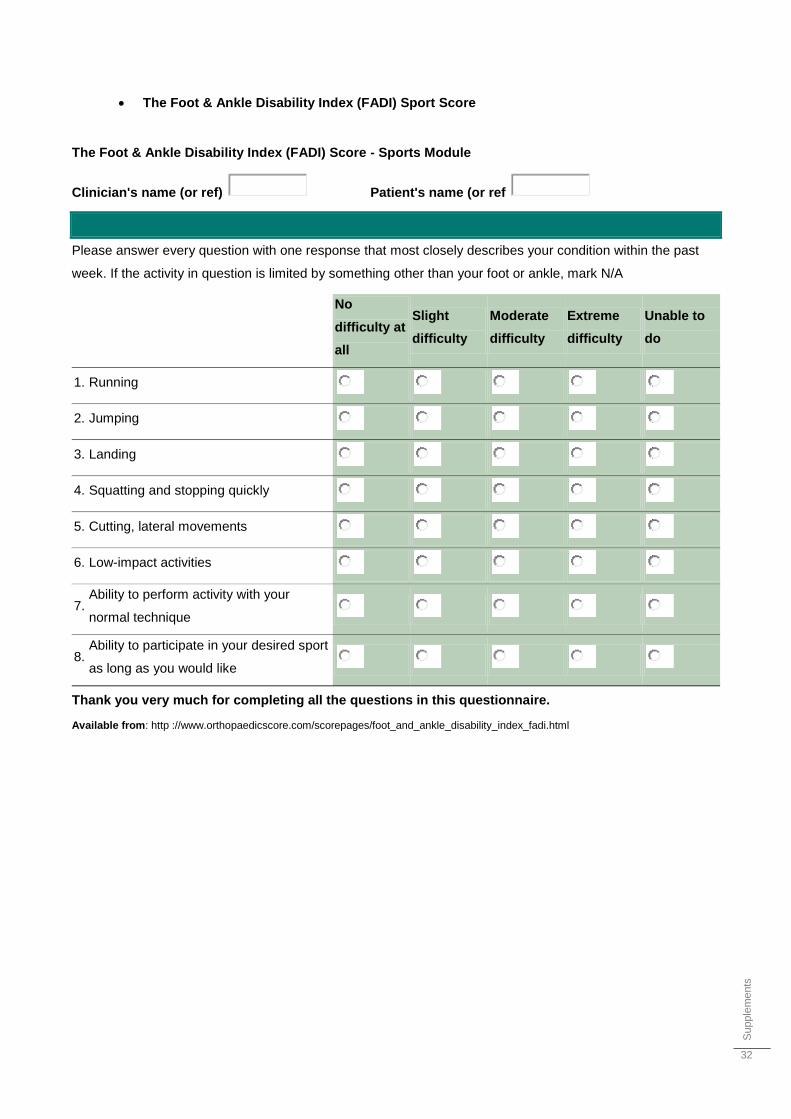
Supple
me
nts
32
The Foot & Ankle Disability Index (FADI) Sport Score
The Foot & Ankle Disability Index (FADI) Score - Sports Module
Clinician's name (or ref) Patient's name (or ref
Please answer every question with one response that most closely describes your condition within the past
week. If the activity in question is limited by something other than your foot or ankle, mark N/A
No
difficulty at
all
Slight
difficulty
Moderate
difficulty
Extreme
difficulty
Unable to
do
1. Running
2. Jumping
3. Landing
4. Squatting and stopping quickly
5. Cutting, lateral movements
6. Low-impact activities
7. Ability to perform activity with your
normal technique
8. Ability to participate in your desired sport
as long as you would like
Thank you very much for completing all the questions in this questionnaire.
Available from: http ://www.orthopaedicscore.com/scorepages/foot_and_ankle_disability_index_fadi.html
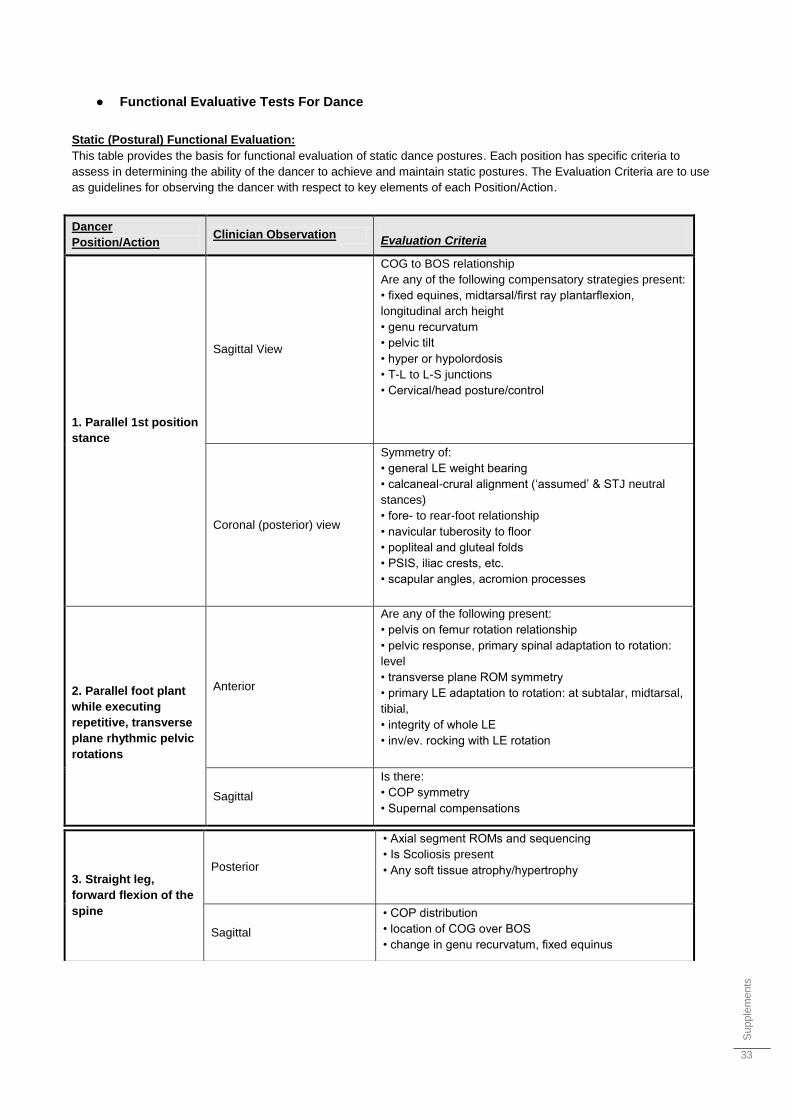
Supple
me
nts
33
● Functional Evaluative Tests For Dance
Static (Postural) Functional Evaluation:
This table provides the basis for functional evaluation of static dance postures. Each position has specific criteria to
assess in determining the ability of the dancer to achieve and maintain static postures. The Evaluation Criteria are to use
as guidelines for observing the dancer with respect to key elements of each Position/Action.
Dancer
Position/Action Clinician Observation
Evaluation Criteria
1. Parallel 1st position
stance
Sagittal View
COG to BOS relationship
Are any of the following compensatory strategies present:
• fixed equines, midtarsal/first ray plantarflexion,
longitudinal arch height
• genu recurvatum
• pelvic tilt
• hyper or hypolordosis
• T-L to L-S junctions
• Cervical/head posture/control
Coronal (posterior) view
Symmetry of:
• general LE weight bearing
• calcaneal-crural alignment („assumed‟ & STJ neutral
stances)
• fore- to rear-foot relationship
• navicular tuberosity to floor
• popliteal and gluteal folds
• PSIS, iliac crests, etc.
• scapular angles, acromion processes
2. Parallel foot plant
while executing
repetitive, transverse
plane rhythmic pelvic
rotations
Anterior
Are any of the following present:
• pelvis on femur rotation relationship
• pelvic response, primary spinal adaptation to rotation:
level
• transverse plane ROM symmetry
• primary LE adaptation to rotation: at subtalar, midtarsal,
tibial,
• integrity of whole LE
• inv/ev. rocking with LE rotation
Sagittal
Is there:
• COP symmetry
• Supernal compensations
3. Straight leg,
forward flexion of the
spine
Posterior
• Axial segment ROMs and sequencing
• Is Scoliosis present
• Any soft tissue atrophy/hypertrophy
Sagittal
• COP distribution
• location of COG over BOS
• change in genu recurvatum, fixed equinus
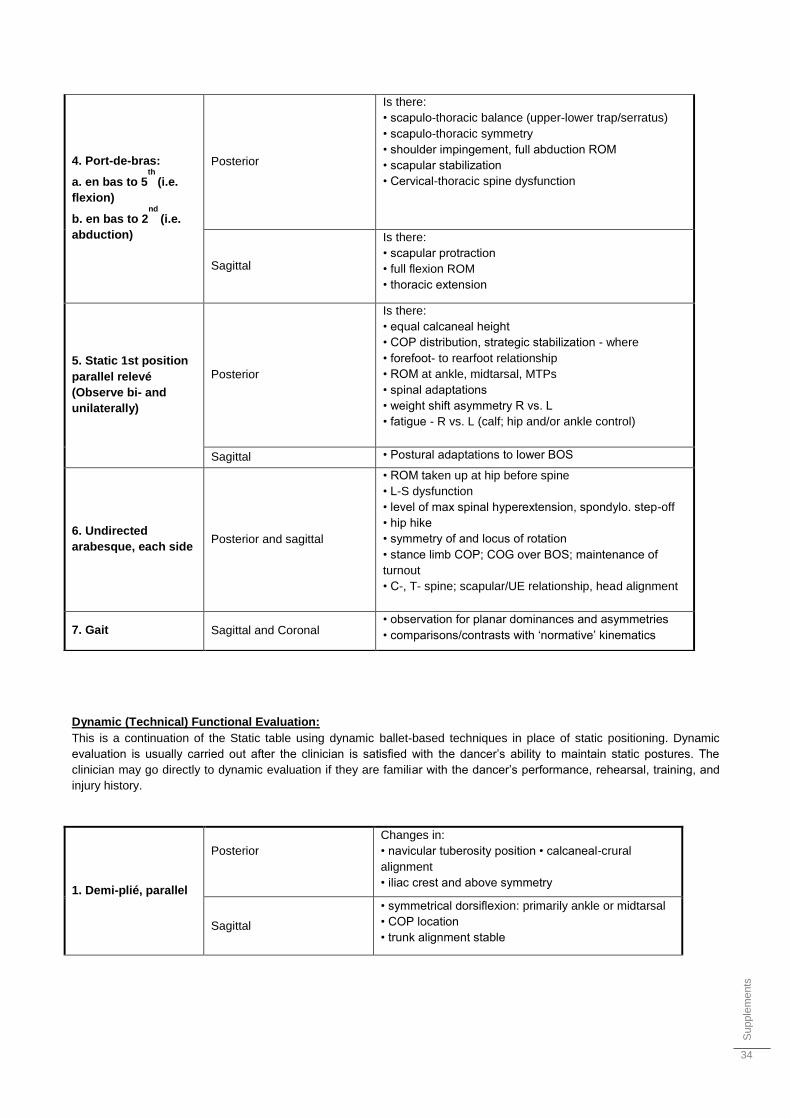
Supple
me
nts
34
Dynamic (Technical) Functional Evaluation:
This is a continuation of the Static table using dynamic ballet-based techniques in place of static positioning. Dynamic
evaluation is usually carried out after the clinician is satisfied with the dancer‟s ability to maintain static postures. The
clinician may go directly to dynamic evaluation if they are familiar with the dancer‟s performance, rehearsal, training, and
injury history.
1. Demi-plié, parallel
Posterior
Changes in:
• navicular tuberosity position • calcaneal-crural
alignment
• iliac crest and above symmetry
Sagittal
• symmetrical dorsiflexion: primarily ankle or midtarsal
• COP location
• trunk alignment stable
4. Port-de-bras:
a. en bas to 5th
(i.e.
flexion)
b. en bas to 2nd
(i.e.
abduction)
Posterior
Is there:
• scapulo-thoracic balance (upper-lower trap/serratus)
• scapulo-thoracic symmetry
• shoulder impingement, full abduction ROM
• scapular stabilization
• Cervical-thoracic spine dysfunction
Sagittal
Is there:
• scapular protraction
• full flexion ROM
• thoracic extension
5. Static 1st position
parallel relevé
(Observe bi- and
unilaterally)
Posterior
Is there:
• equal calcaneal height
• COP distribution, strategic stabilization - where
• forefoot- to rearfoot relationship
• ROM at ankle, midtarsal, MTPs
• spinal adaptations
• weight shift asymmetry R vs. L
• fatigue - R vs. L (calf; hip and/or ankle control)
Sagittal • Postural adaptations to lower BOS
6. Undirected
arabesque, each side Posterior and sagittal
• ROM taken up at hip before spine
• L-S dysfunction
• level of max spinal hyperextension, spondylo. step-off
• hip hike
• symmetry of and locus of rotation
• stance limb COP; COG over BOS; maintenance of
turnout
• C-, T- spine; scapular/UE relationship, head alignment
7. Gait Sagittal and Coronal • observation for planar dominances and asymmetries
• comparisons/contrasts with „normative‟ kinematics
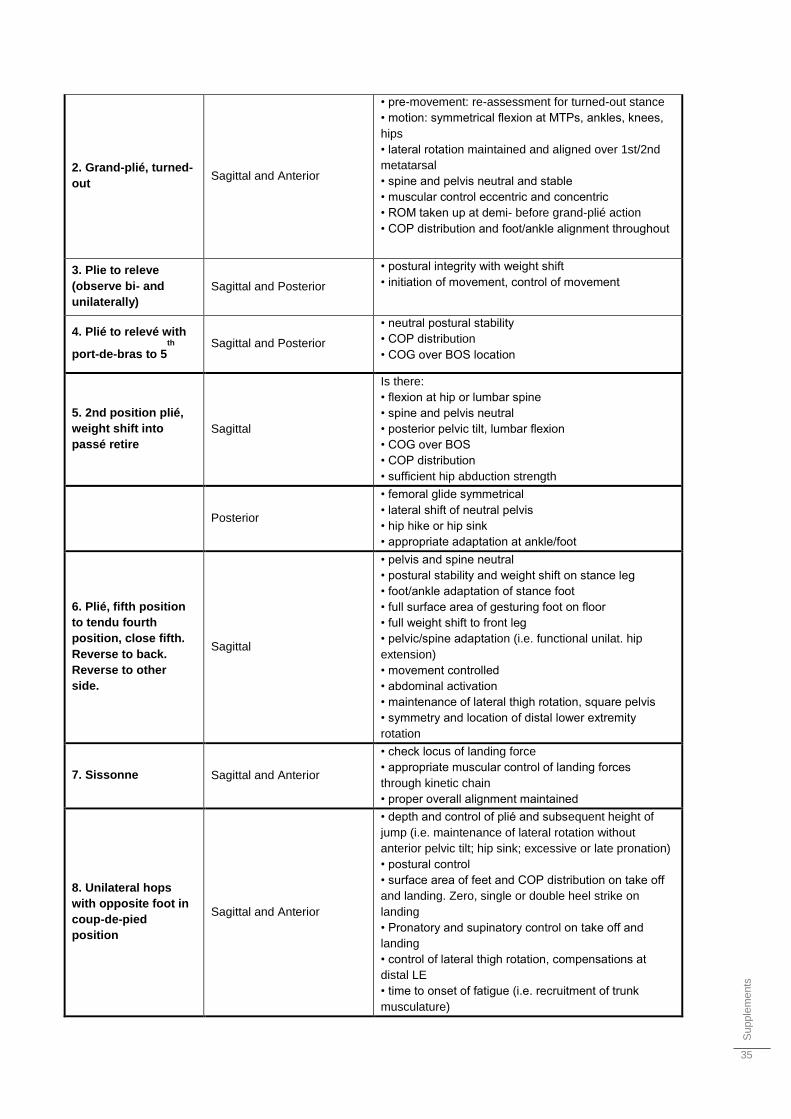
Supple
me
nts
35
2. Grand-plié, turned-
out Sagittal and Anterior
• pre-movement: re-assessment for turned-out stance
• motion: symmetrical flexion at MTPs, ankles, knees,
hips
• lateral rotation maintained and aligned over 1st/2nd
metatarsal
• spine and pelvis neutral and stable
• muscular control eccentric and concentric
• ROM taken up at demi- before grand-plié action
• COP distribution and foot/ankle alignment throughout
3. Plie to releve
(observe bi- and
unilaterally)
Sagittal and Posterior
• postural integrity with weight shift
• initiation of movement, control of movement
4. Plié to relevé with
port-de-bras to 5th
Sagittal and Posterior
• neutral postural stability
• COP distribution
• COG over BOS location
5. 2nd position plié,
weight shift into
passé retire
Sagittal
Is there:
• flexion at hip or lumbar spine
• spine and pelvis neutral
• posterior pelvic tilt, lumbar flexion
• COG over BOS
• COP distribution
• sufficient hip abduction strength
Posterior
• femoral glide symmetrical
• lateral shift of neutral pelvis
• hip hike or hip sink
• appropriate adaptation at ankle/foot
6. Plié, fifth position
to tendu fourth
position, close fifth.
Reverse to back.
Reverse to other
side.
Sagittal
• pelvis and spine neutral
• postural stability and weight shift on stance leg
• foot/ankle adaptation of stance foot
• full surface area of gesturing foot on floor
• full weight shift to front leg
• pelvic/spine adaptation (i.e. functional unilat. hip
extension)
• movement controlled
• abdominal activation
• maintenance of lateral thigh rotation, square pelvis
• symmetry and location of distal lower extremity
rotation
7. Sissonne Sagittal and Anterior
• check locus of landing force
• appropriate muscular control of landing forces
through kinetic chain
• proper overall alignment maintained
8. Unilateral hops
with opposite foot in
coup-de-pied
position
Sagittal and Anterior
• depth and control of plié and subsequent height of
jump (i.e. maintenance of lateral rotation without
anterior pelvic tilt; hip sink; excessive or late pronation)
• postural control
• surface area of feet and COP distribution on take off
and landing. Zero, single or double heel strike on
landing
• Pronatory and supinatory control on take off and
landing
• control of lateral thigh rotation, compensations at
distal LE
• time to onset of fatigue (i.e. recruitment of trunk
musculature)
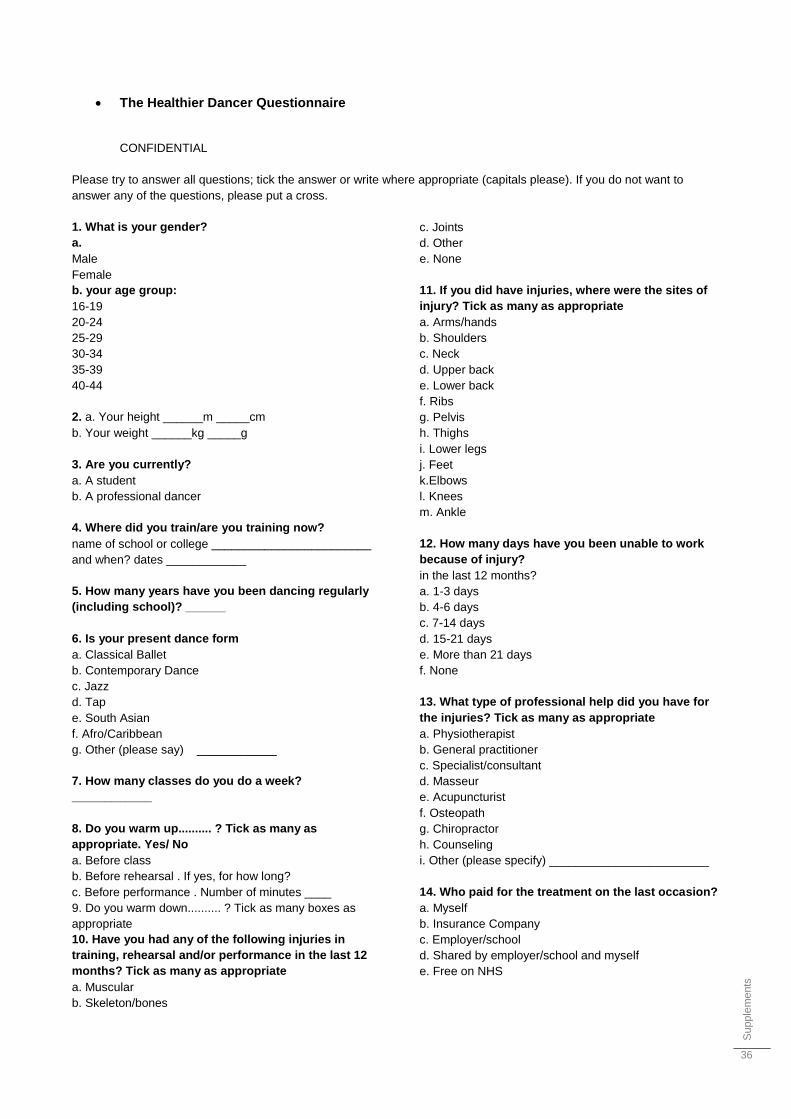
Supple
me
nts
36
The Healthier Dancer Questionnaire
CONFIDENTIAL
Please try to answer all questions; tick the answer or write where appropriate (capitals please). If you do not want to
answer any of the questions, please put a cross.
1. What is your gender?
a.
Male
Female
b. your age group:
16-19
20-24
25-29
30-34
35-39
40-44
2. a. Your height ______m _____cm
b. Your weight ______kg _____g
3. Are you currently?
a. A student
b. A professional dancer
4. Where did you train/are you training now?
name of school or college ________________________
and when? dates ____________
5. How many years have you been dancing regularly
(including school)? ______
6. Is your present dance form
a. Classical Ballet
b. Contemporary Dance
c. Jazz
d. Tap
e. South Asian
f. Afro/Caribbean
g. Other (please say) ____________
7. How many classes do you do a week?
____________
8. Do you warm up.......... ? Tick as many as
appropriate. Yes/ No
a. Before class
b. Before rehearsal . If yes, for how long?
c. Before performance . Number of minutes ____
9. Do you warm down.......... ? Tick as many boxes as
appropriate
10. Have you had any of the following injuries in
training, rehearsal and/or performance in the last 12
months? Tick as many as appropriate
a. Muscular
b. Skeleton/bones
c. Joints
d. Other
e. None
11. If you did have injuries, where were the sites of
injury? Tick as many as appropriate
a. Arms/hands
b. Shoulders
c. Neck
d. Upper back
e. Lower back
f. Ribs
g. Pelvis
h. Thighs
i. Lower legs
j. Feet
k.Elbows
l. Knees
m. Ankle
12. How many days have you been unable to work
because of injury?
in the last 12 months?
a. 1-3 days
b. 4-6 days
c. 7-14 days
d. 15-21 days
e. More than 21 days
f. None
13. What type of professional help did you have for
the injuries? Tick as many as appropriate
a. Physiotherapist
b. General practitioner
c. Specialist/consultant
d. Masseur
e. Acupuncturist
f. Osteopath
g. Chiropractor
h. Counseling
i. Other (please specify) ________________________
14. Who paid for the treatment on the last occasion?
a. Myself
b. Insurance Company
c. Employer/school
d. Shared by employer/school and myself
e. Free on NHS
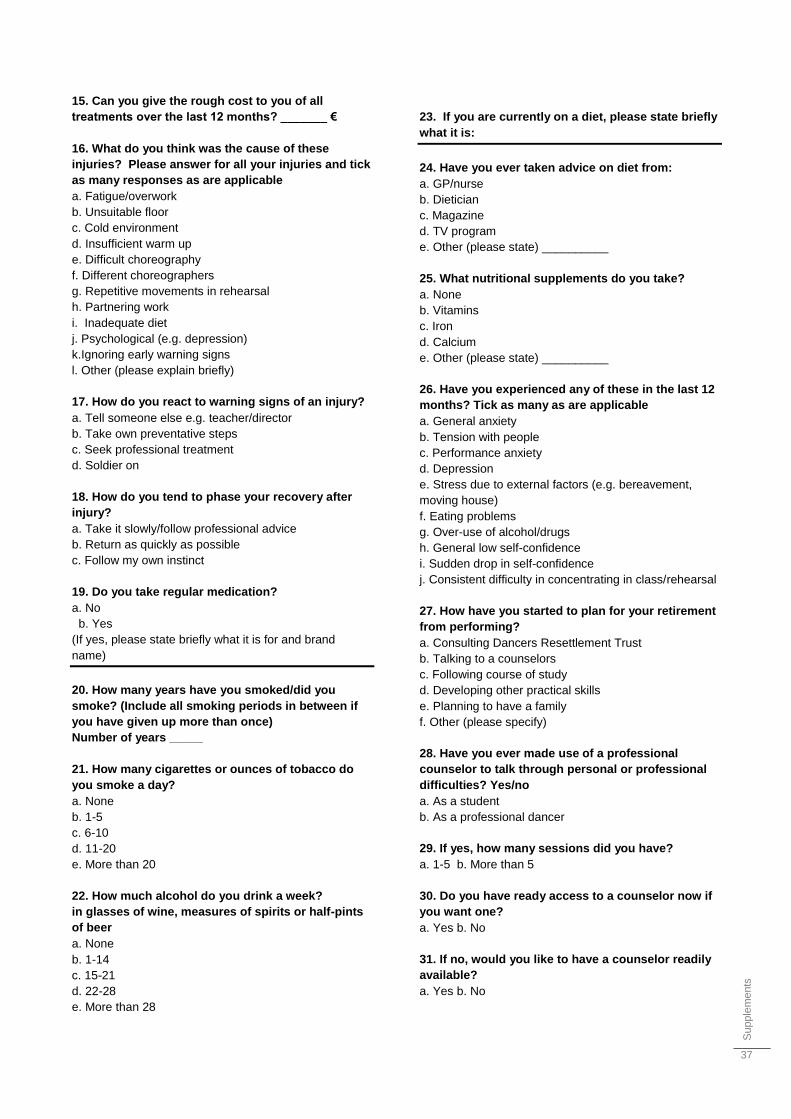
Supple
me
nts
37
15. Can you give the rough cost to you of all
treatments over the last 12 months? _______ €
16. What do you think was the cause of these
injuries? Please answer for all your injuries and tick
as many responses as are applicable
a. Fatigue/overwork
b. Unsuitable floor
c. Cold environment
d. Insufficient warm up
e. Difficult choreography
f. Different choreographers
g. Repetitive movements in rehearsal
h. Partnering work
i. Inadequate diet
j. Psychological (e.g. depression)
k.Ignoring early warning signs
l. Other (please explain briefly)
17. How do you react to warning signs of an injury?
a. Tell someone else e.g. teacher/director
b. Take own preventative steps
c. Seek professional treatment
d. Soldier on
18. How do you tend to phase your recovery after
injury?
a. Take it slowly/follow professional advice
b. Return as quickly as possible
c. Follow my own instinct
19. Do you take regular medication?
a. No
b. Yes
(If yes, please state briefly what it is for and brand
name)
20. How many years have you smoked/did you
smoke? (Include all smoking periods in between if
you have given up more than once)
Number of years _____
21. How many cigarettes or ounces of tobacco do
you smoke a day?
a. None
b. 1-5
c. 6-10
d. 11-20
e. More than 20
22. How much alcohol do you drink a week?
in glasses of wine, measures of spirits or half-pints
of beer
a. None
b. 1-14
c. 15-21
d. 22-28
e. More than 28
23. If you are currently on a diet, please state briefly
what it is:
24. Have you ever taken advice on diet from:
a. GP/nurse
b. Dietician
c. Magazine
d. TV program
e. Other (please state) __________
25. What nutritional supplements do you take?
a. None
b. Vitamins
c. Iron
d. Calcium
e. Other (please state) __________
26. Have you experienced any of these in the last 12
months? Tick as many as are applicable
a. General anxiety
b. Tension with people
c. Performance anxiety
d. Depression
e. Stress due to external factors (e.g. bereavement,
moving house)
f. Eating problems
g. Over-use of alcohol/drugs
h. General low self-confidence
i. Sudden drop in self-confidence
j. Consistent difficulty in concentrating in class/rehearsal
27. How have you started to plan for your retirement
from performing?
a. Consulting Dancers Resettlement Trust
b. Talking to a counselors
c. Following course of study
d. Developing other practical skills
e. Planning to have a family
f. Other (please specify)
28. Have you ever made use of a professional
counselor to talk through personal or professional
difficulties? Yes/no
a. As a student
b. As a professional dancer
29. If yes, how many sessions did you have?
a. 1-5 b. More than 5
30. Do you have ready access to a counselor now if
you want one?
a. Yes b. No
31. If no, would you like to have a counselor readily
available?
a. Yes b. No
Supple
me
nts
38
32. Do you feel that your vocational training
prepared/is preparing?
you adequately for your life as a dancer?
a. Yes b. No c. More or less
33. If not, how could it be/have been better?
34. In what ways do you think a free or reduced-cost
health and injury service for dancers could best
contribute to solving physical and psychological
problems?
Related Documents











