Evidence‐based for automated ventilation ? François LELLOUCHE, MD, PhD Centre de recherche de l’Institut Universitaire de Cardiologie et de Pneumologie de Québec 2 ème Journée Internationale de Ventilation Mécanique

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Evidence‐based for automated ventilation ?
François LELLOUCHE, MD, PhDCentre de recherche de l’Institut Universitaire de Cardiologie et de Pneumologie de Québec
2ème Journée Internationale de Ventilation Mécanique

CONFLITS D’INTERÊT
‐ Contrat avec Drager medical (frais de déplacement pour l'étude canadienne sur SmartCare)
‐ Contrat de recherche avec Hamilton médical pour mener l'évaluation d’Intellivent(salaire de l'assistant de recherche)
‐ Programme de recherche sur l’automatisation de la ventilation et de l'oxygène :
Fondation Canadienne pour l’Innovation (Fonds des Leaders)/FRSQ
‐ Président d'un compagnie R&D (OXYNOV’) qui développe des systèmes automatisés
pour l’oxygénothérapie et la ventilation mécanique
Pourquoi des modes automatisés en ventilation mécanique ?
SmartCare: Ajustement de l’aide inspiratoire, sevrage automatiséRésultats de l’étude pilote WEAN
Intellivent: Ventilation mécanique automatiséeÉvaluation en post‐opératoire de chirurgie cardiaqueDonnées récentes chez des patients médicaux
PLAN
Évaluation des nouveaux modes, quels critères ?
VACI
VPAC
Automode
VCVAC
SIMV
VAPS
VA
VS
PA
VCRP
Autoflow
APV
VS-AI-Vt mini
VAC+ VACI+VPC
VPSSPAP
MMV
VAIV
VIV APRV
VS-PPV
BIPAP
BILEVEL
VPL
ATC
TC
ASVPPS
PAV
PC
PAC
PACI
AI
CPAP
IPAP
EPAP
PSV
ASB
VPC
PRVC
NAVA Intellivent
SmartCare
Intellivent
SmartCare
PAV
NAVA
Recherche en ventilation mécanique
Physiologie +++++ARDS +++++Sevrage ventilatoire +++++Ventilation non invasive +++++
Nouveaux modes…….
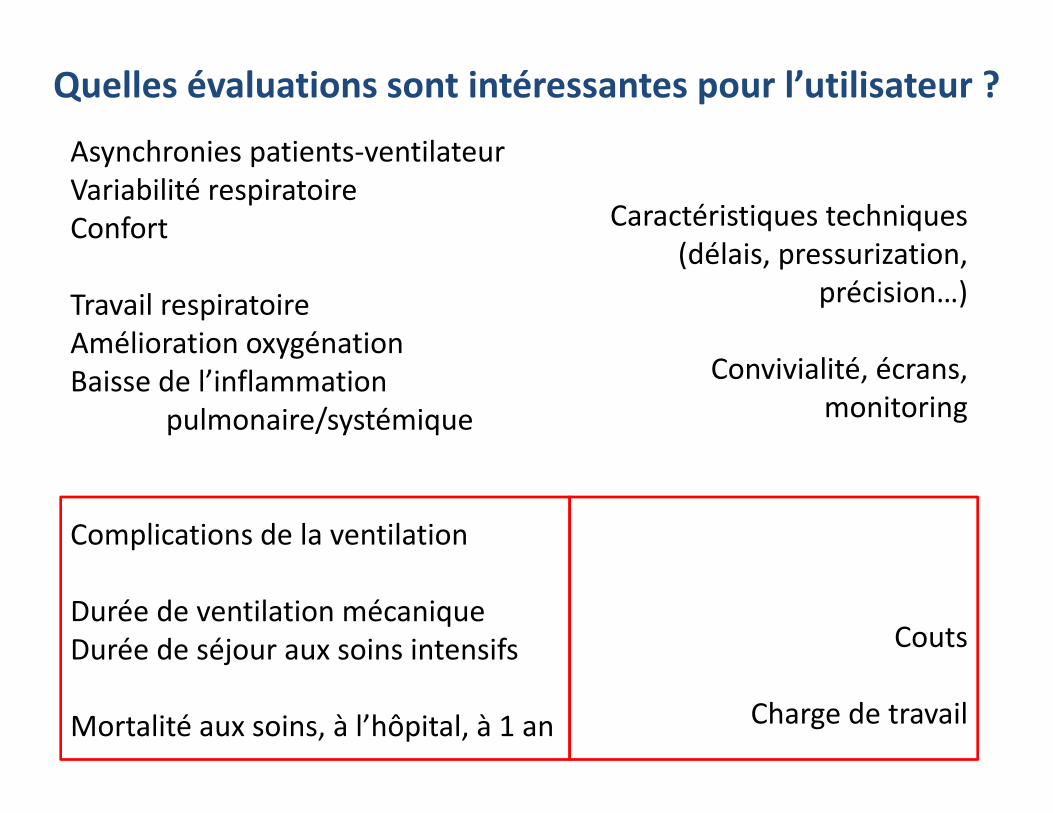
Quelles évaluations sont intéressantes pour l’utilisateur ?
Asynchronies patients‐ventilateurVariabilité respiratoireConfort
Travail respiratoireAmélioration oxygénationBaisse de l’inflammation
pulmonaire/systémique
Complications de la ventilation
Durée de ventilation mécaniqueDurée de séjour aux soins intensifs
Mortalité aux soins, à l’hôpital, à 1 an
Caractéristiques techniques(délais, pressurization,
précision…)
Convivialité, écrans, monitoring
Couts
Charge de travail
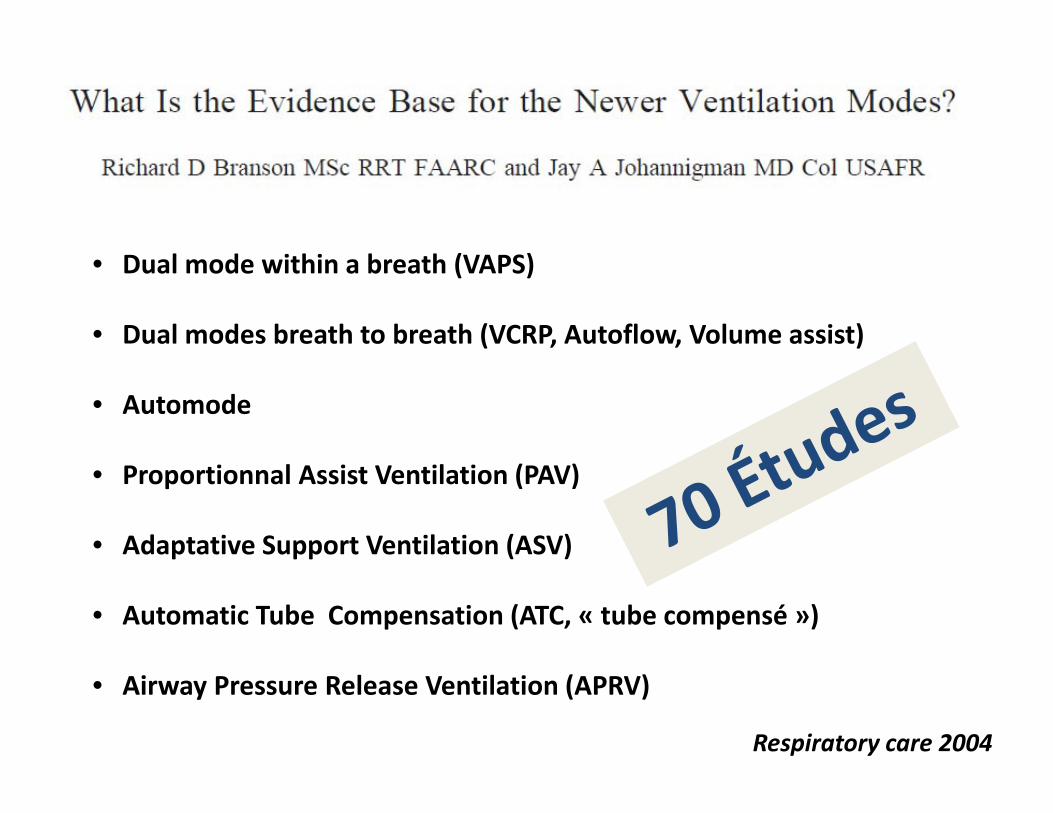
Respiratory care 2004
• Dual mode within a breath (VAPS)
• Dual modes breath to breath (VCRP, Autoflow, Volume assist)
• Automode
• Proportionnal Assist Ventilation (PAV)
• Adaptative Support Ventilation (ASV)
• Automatic Tube Compensation (ATC, « tube compensé »)
• Airway Pressure Release Ventilation (APRV)
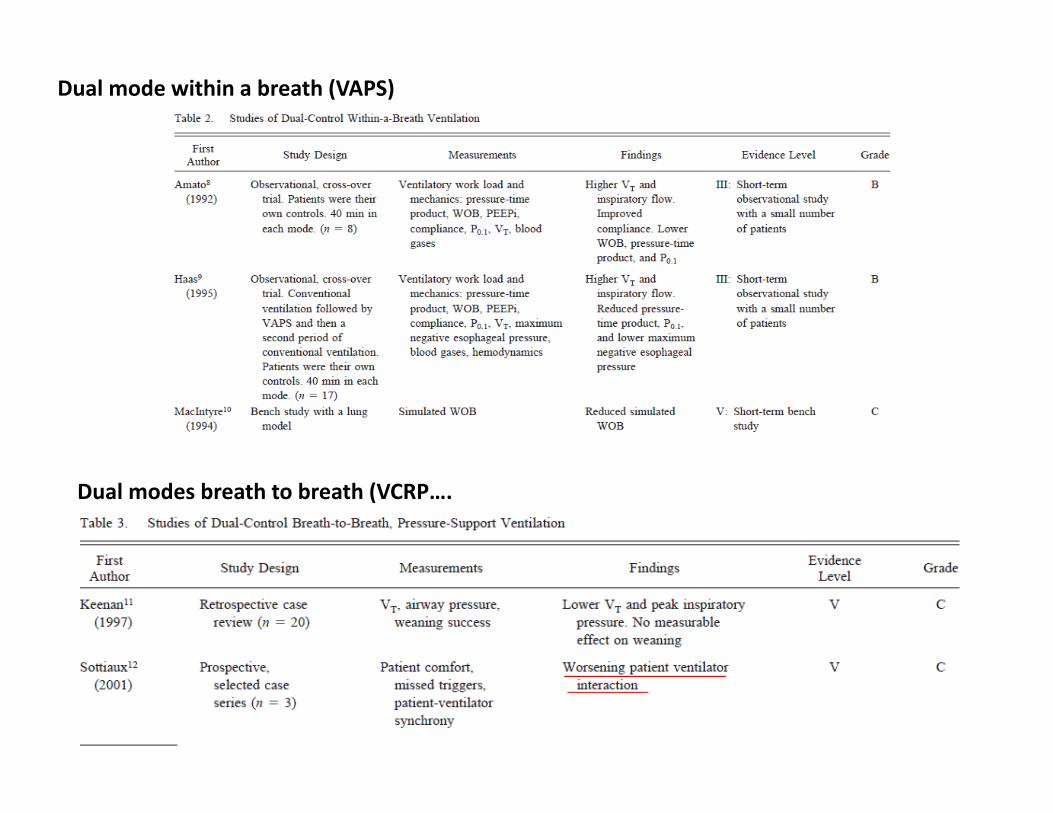
Dual mode within a breath (VAPS)
Dual modes breath to breath (VCRP….
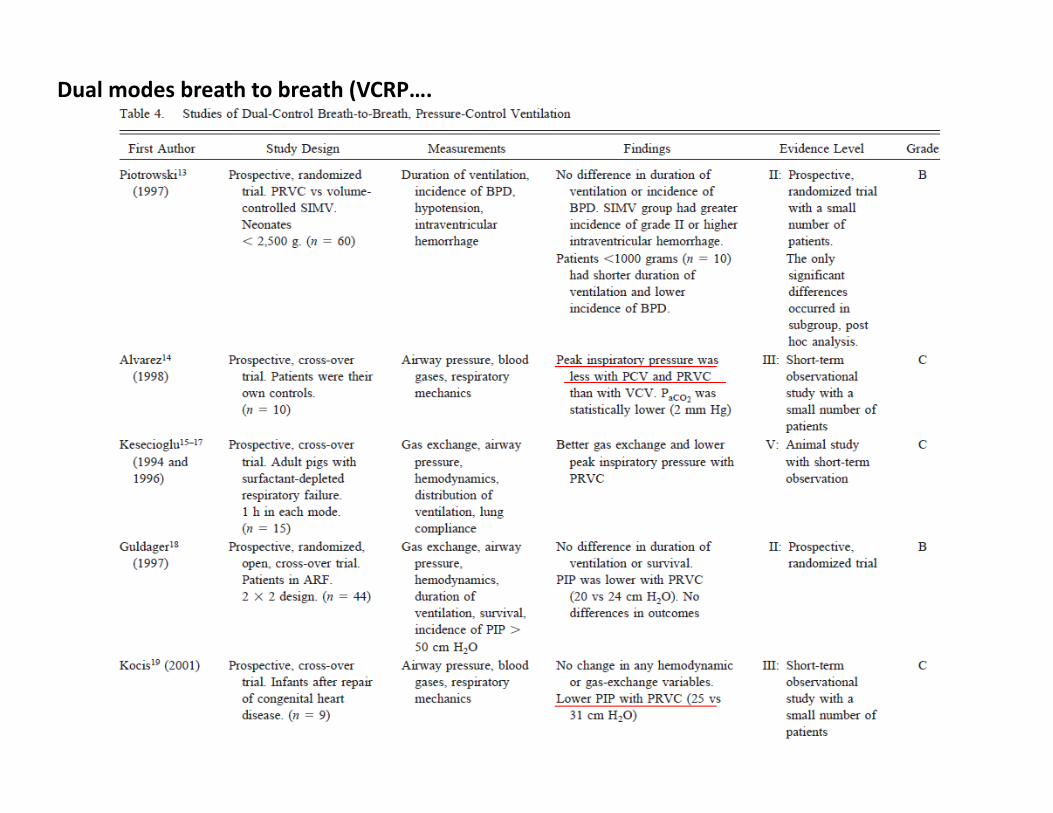
Dual modes breath to breath (VCRP….
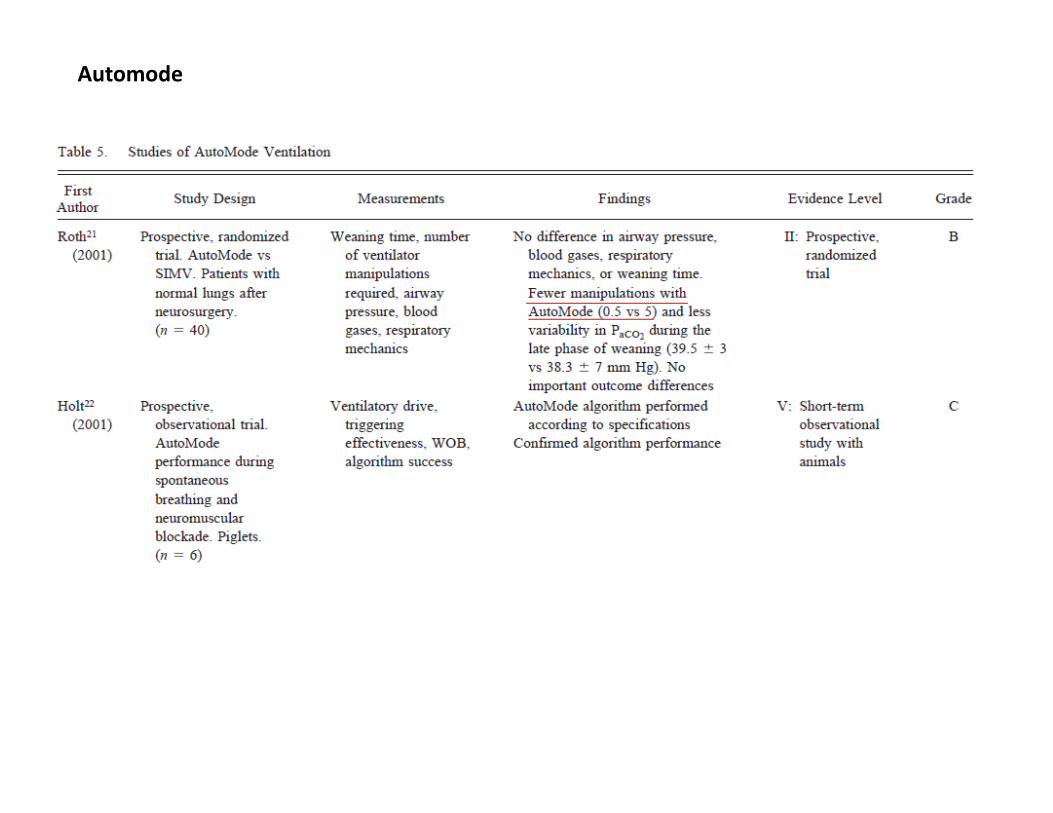
Automode
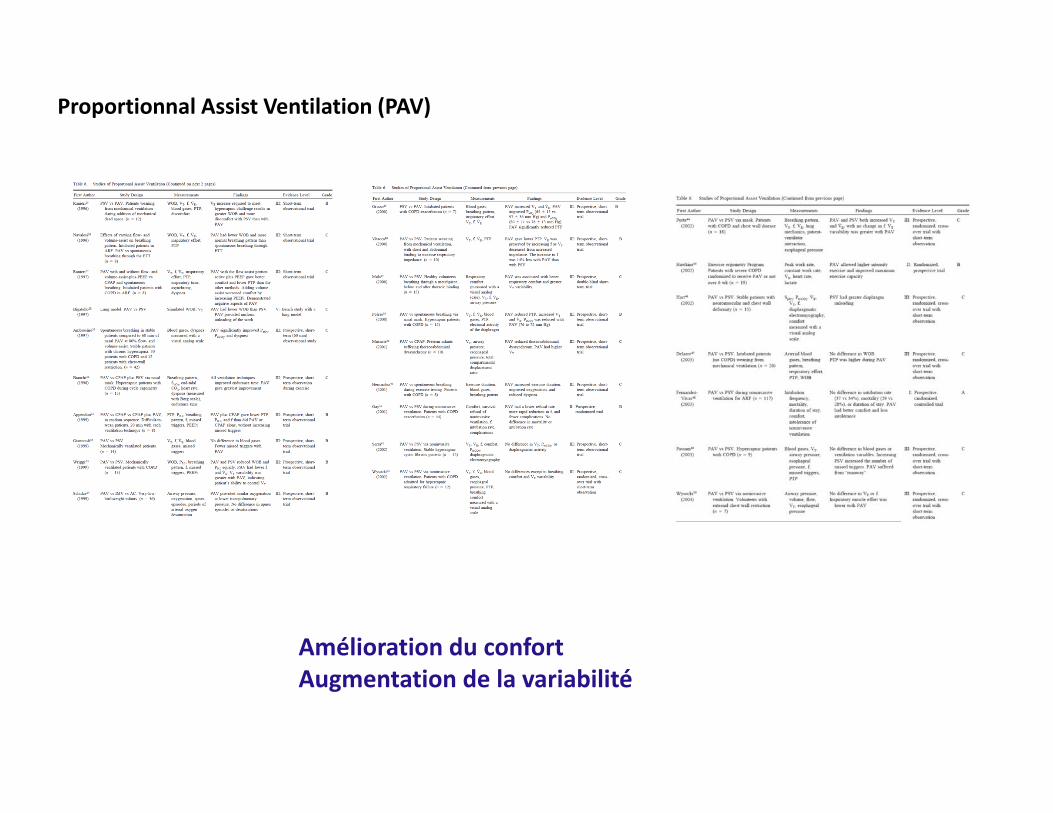
Proportionnal Assist Ventilation (PAV)
Amélioration du confortAugmentation de la variabilité
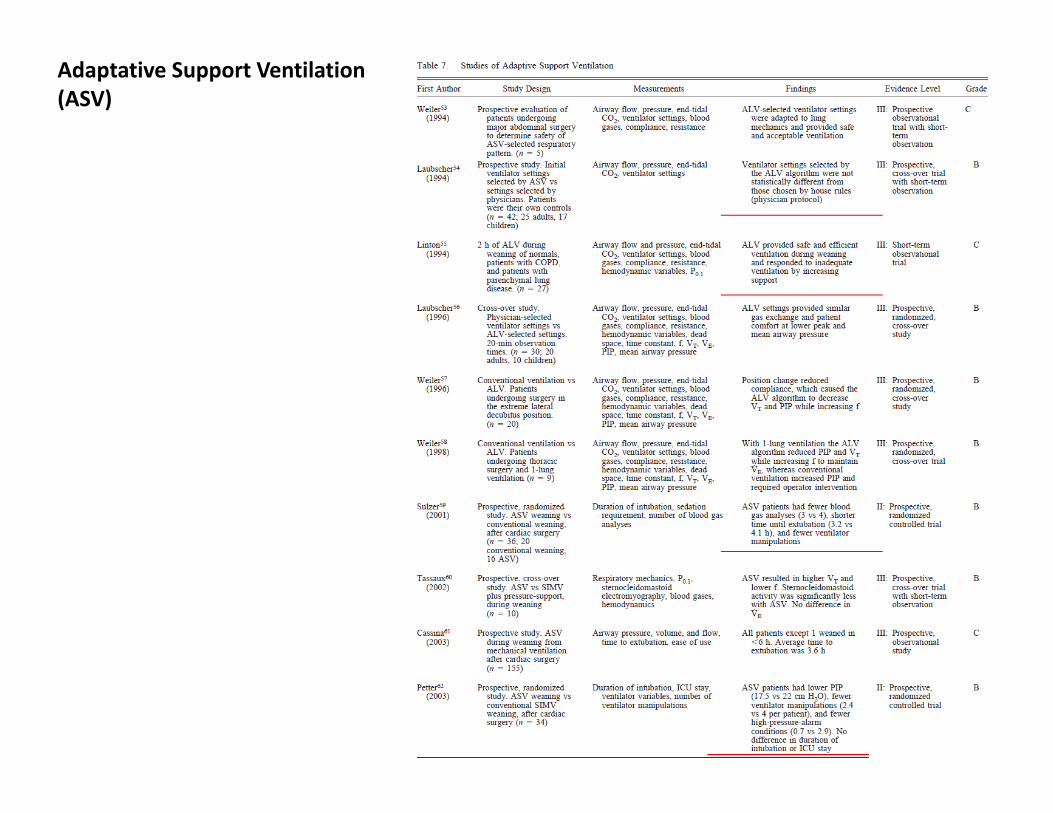
Adaptative Support Ventilation (ASV)
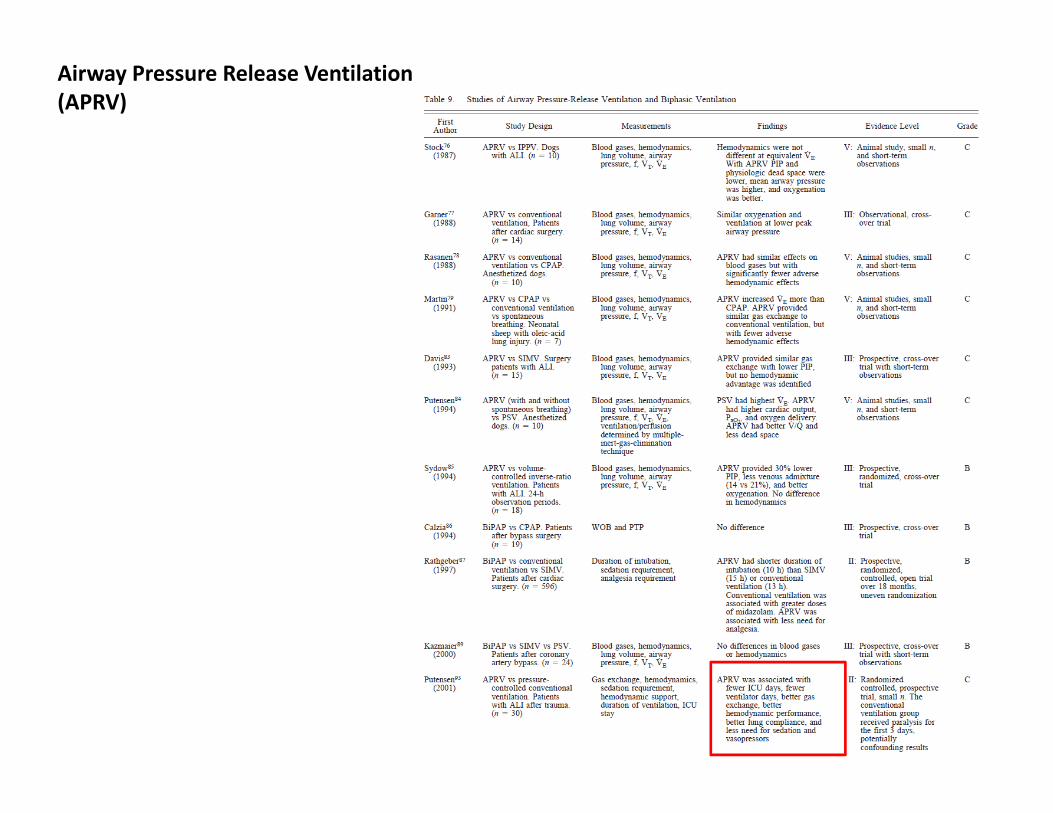
Airway Pressure Release Ventilation (APRV)
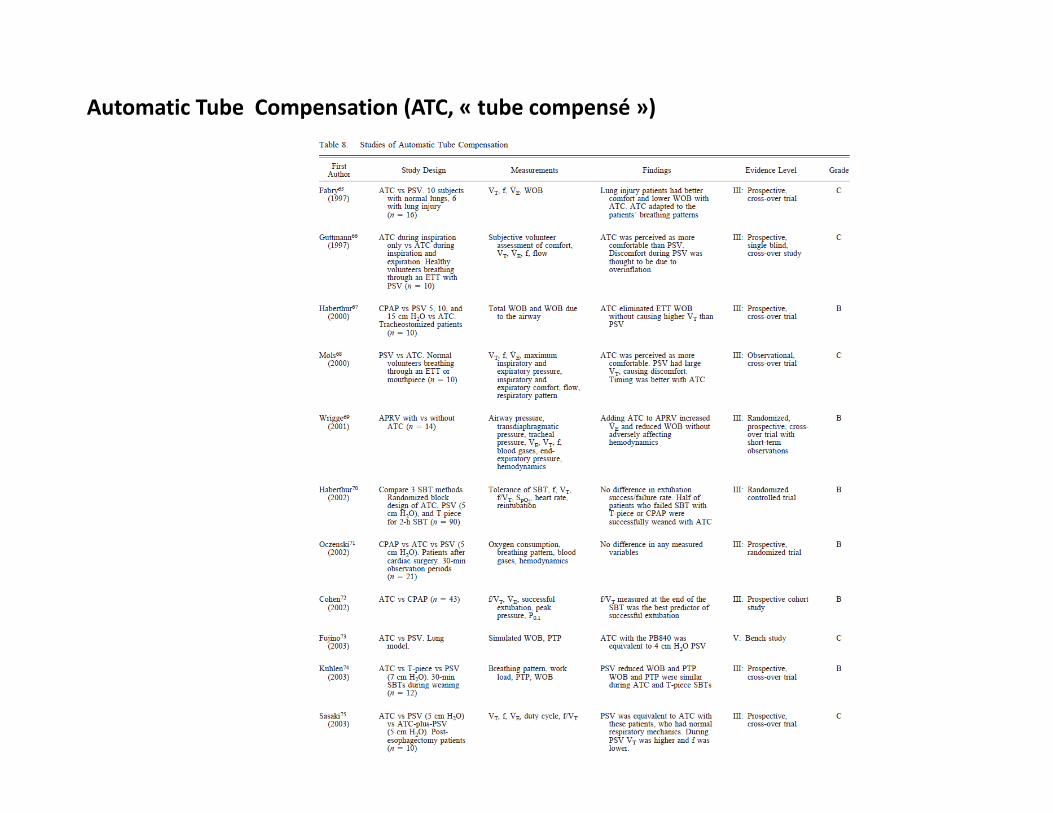
Automatic Tube Compensation (ATC, « tube compensé »)
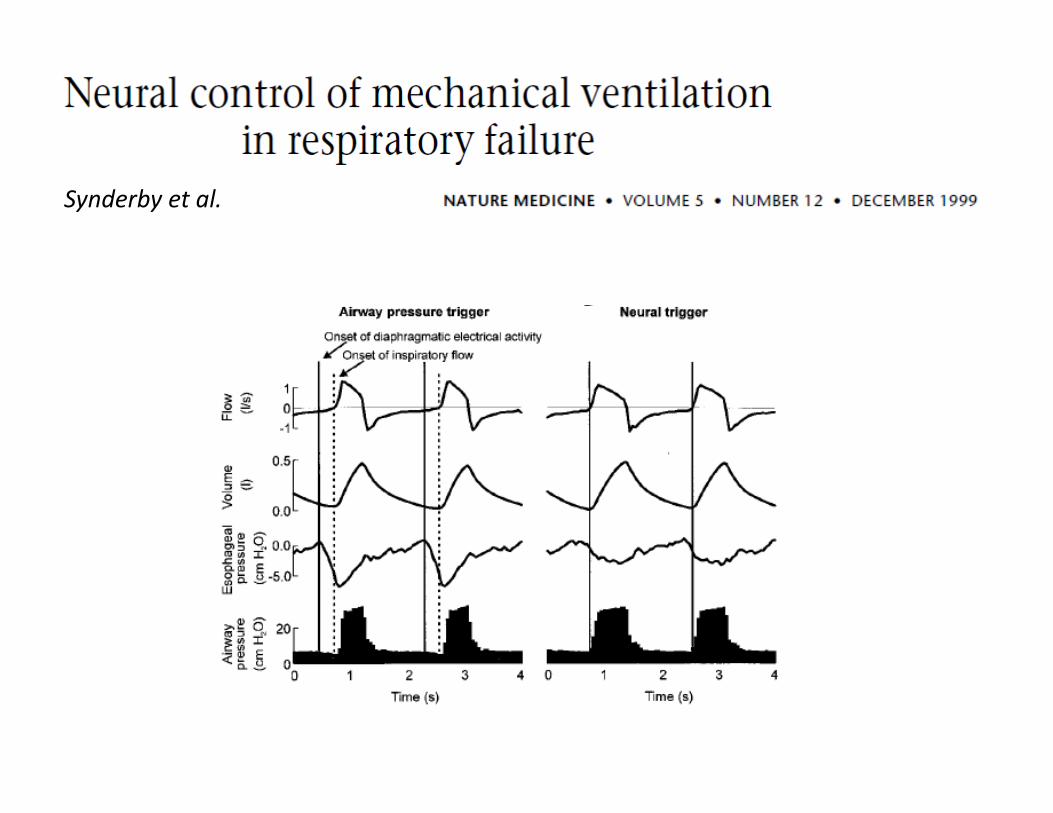
Synderby et al.
Synderby et al.
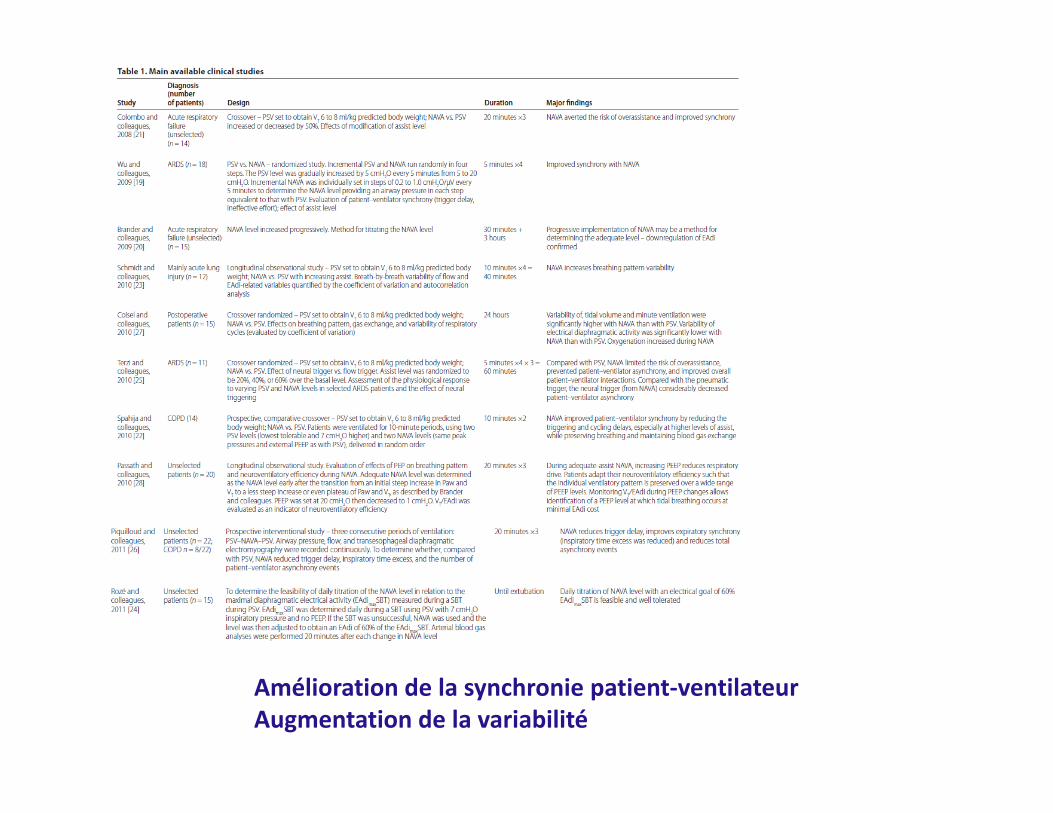
Amélioration de la synchronie patient‐ventilateurAugmentation de la variabilité
RECHERCHE EVALUANT LES « NOUVEAUX MODES »
Peu de données concluantes pour les critères d’évaluation importants:
‐ Durée de VM, durée de séjour, mortalité…‐ Au plan économique (charge de travail)
Beaucoup d’études
Pourquoi des modes automatisés en ventilation mécanique ?
SmartCare: Ajustement de l’aide inspiratoire, sevrage automatiséRésultats de l’étude pilote WEAN
Intellivent: Ventilation mécanique automatiséeRésultats de l’étude CLOSER 1
PLAN
Évaluation des nouveaux modes, quels critères ?
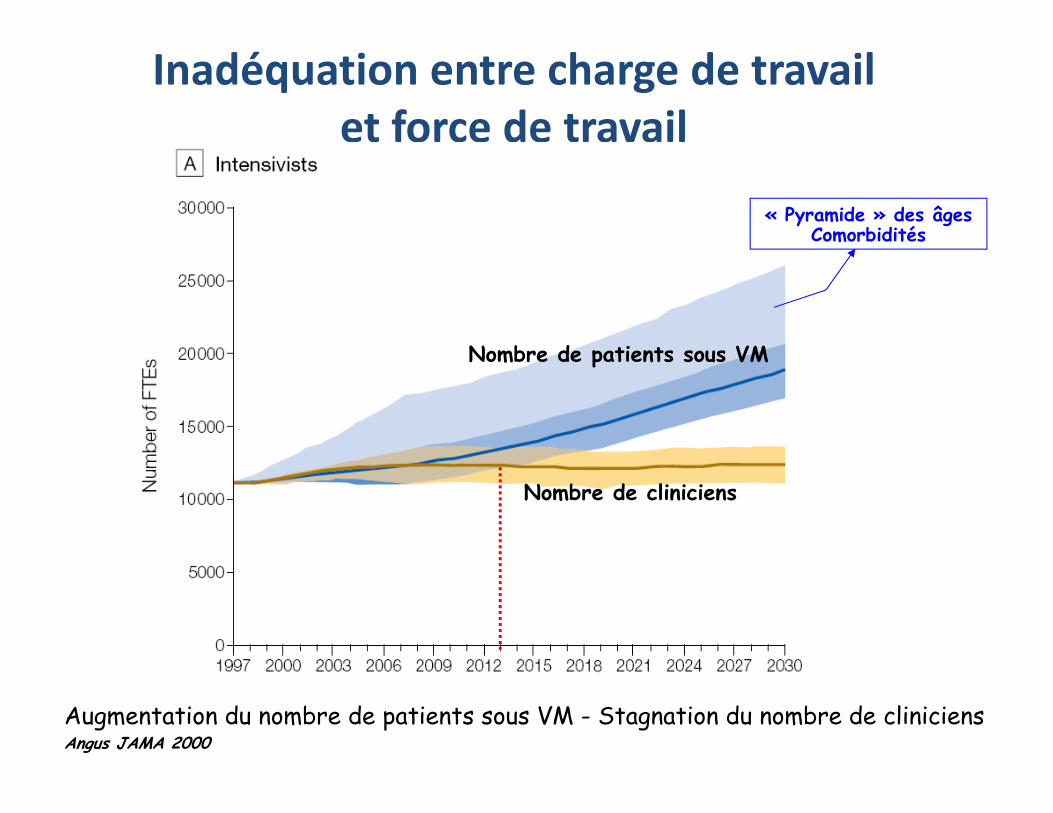
Inadéquation entre charge de travail et force de travail
Augmentation du nombre de patients sous VM - Stagnation du nombre de cliniciens Angus JAMA 2000
Nombre de patients sous VM
Nombre de cliniciens
« Pyramide » des âgesComorbidités
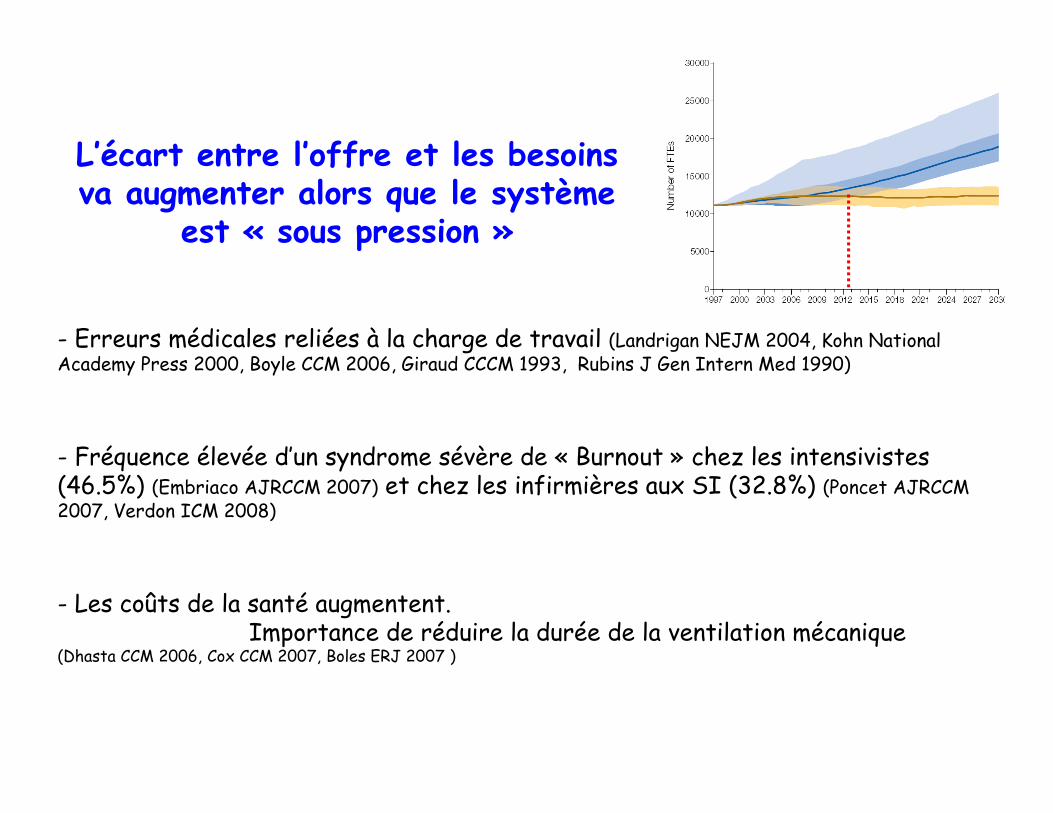
L’écart entre l’offre et les besoins va augmenter alors que le système
est « sous pression »
- Erreurs médicales reliées à la charge de travail (Landrigan NEJM 2004, Kohn National Academy Press 2000, Boyle CCM 2006, Giraud CCCM 1993, Rubins J Gen Intern Med 1990)
- Fréquence élevée d’un syndrome sévère de « Burnout » chez les intensivistes(46.5%) (Embriaco AJRCCM 2007) et chez les infirmières aux SI (32.8%) (Poncet AJRCCM 2007, Verdon ICM 2008)
- Les coûts de la santé augmentent. Importance de réduire la durée de la ventilation mécanique
(Dhasta CCM 2006, Cox CCM 2007, Boles ERJ 2007 )
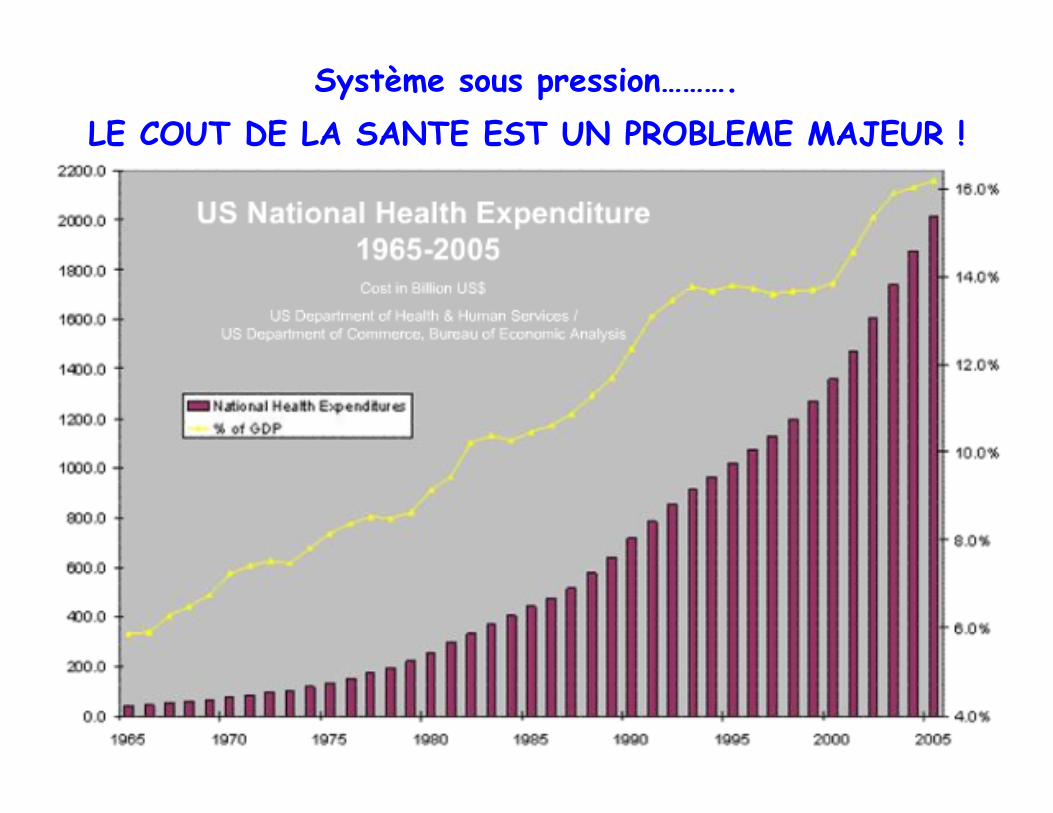
Système sous pression……….LE COUT DE LA SANTE EST UN PROBLEME MAJEUR !

Système sous pression……….LE COUT DE LA SANTE EST UN PROBLEME MAJEUR !
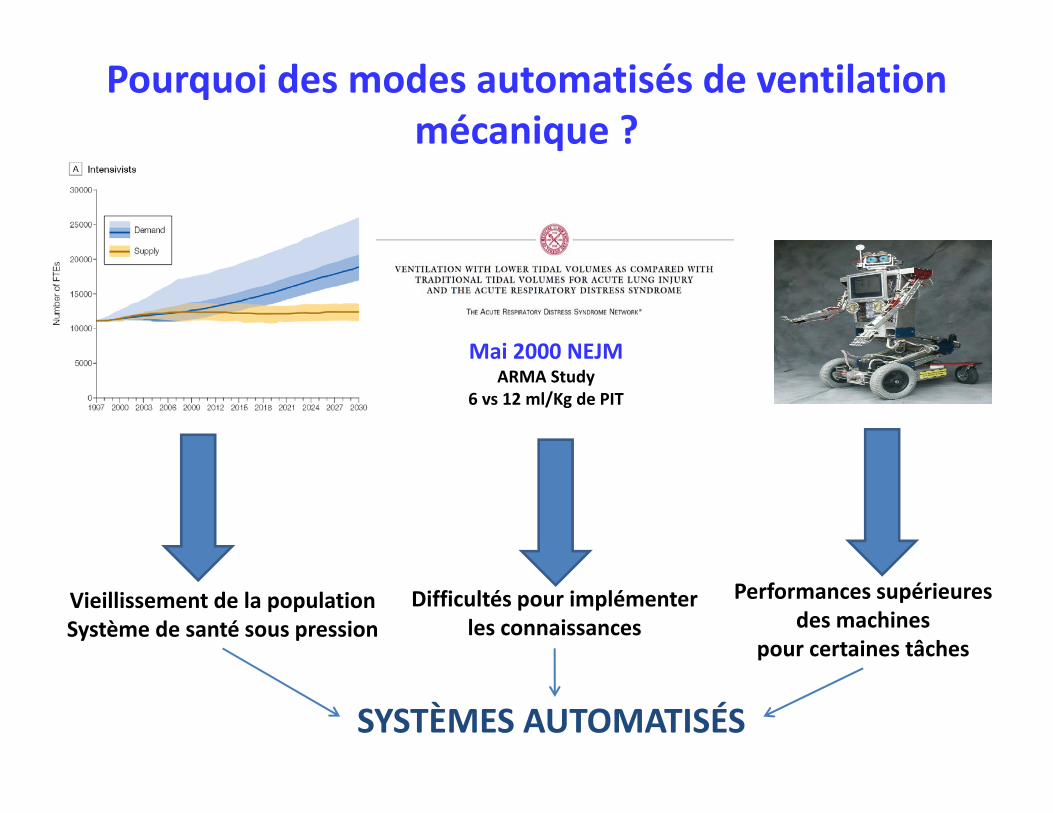
Mai 2000 NEJMARMA Study
6 vs 12 ml/Kg de PIT
Difficultés pour implémenter les connaissances
SYSTÈMES AUTOMATISÉS
Performances supérieures des machines
pour certaines tâches
Vieillissement de la populationSystème de santé sous pression
Pourquoi des modes automatisés de ventilation mécanique ?
Pourquoi des modes automatisés en ventilation mécanique ?
SmartCare: Ajustement de l’aide inspiratoire, sevrage automatiséRésultats de l’étude pilote WEAN
Intellivent: Ventilation mécanique automatiséeRésultats de l’étude CLOSER 1
PLAN
Évaluation des nouveaux modes, quels critères ?
Control
Patient Monitor Alarms
Ventilateur en aide inspiratoire
Control
Patient Monitor Alarms
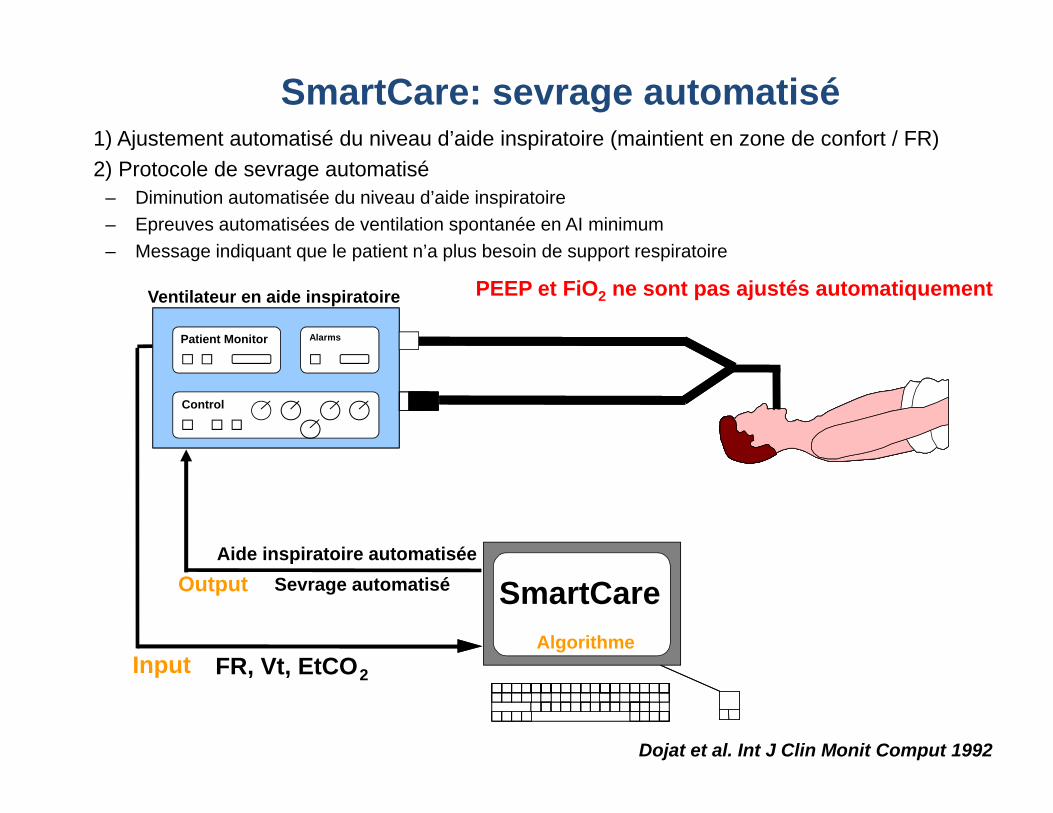
SmartCare: sevrage automatisé1) Ajustement automatisé du niveau d’aide inspiratoire (maintient en zone de confort / FR)2) Protocole de sevrage automatisé
– Diminution automatisée du niveau d’aide inspiratoire– Epreuves automatisées de ventilation spontanée en AI minimum– Message indiquant que le patient n’a plus besoin de support respiratoire
FR, Vt, EtCO2Input
Aide inspiratoire automatiséeSevrage automatiséOutput Automatic
WeaningSystem
SmartCareAlgorithme
Dojat et al. Int J Clin Monit Comput 1992
PEEP et FiO2 ne sont pas ajustés automatiquement
02468
1012141618
0:00 0:28 0:57 1:26 1:55 2:24 2:52
Time (h:min)
Leve
l of P
ress
ure
supp
ort (
cmH
2O
)
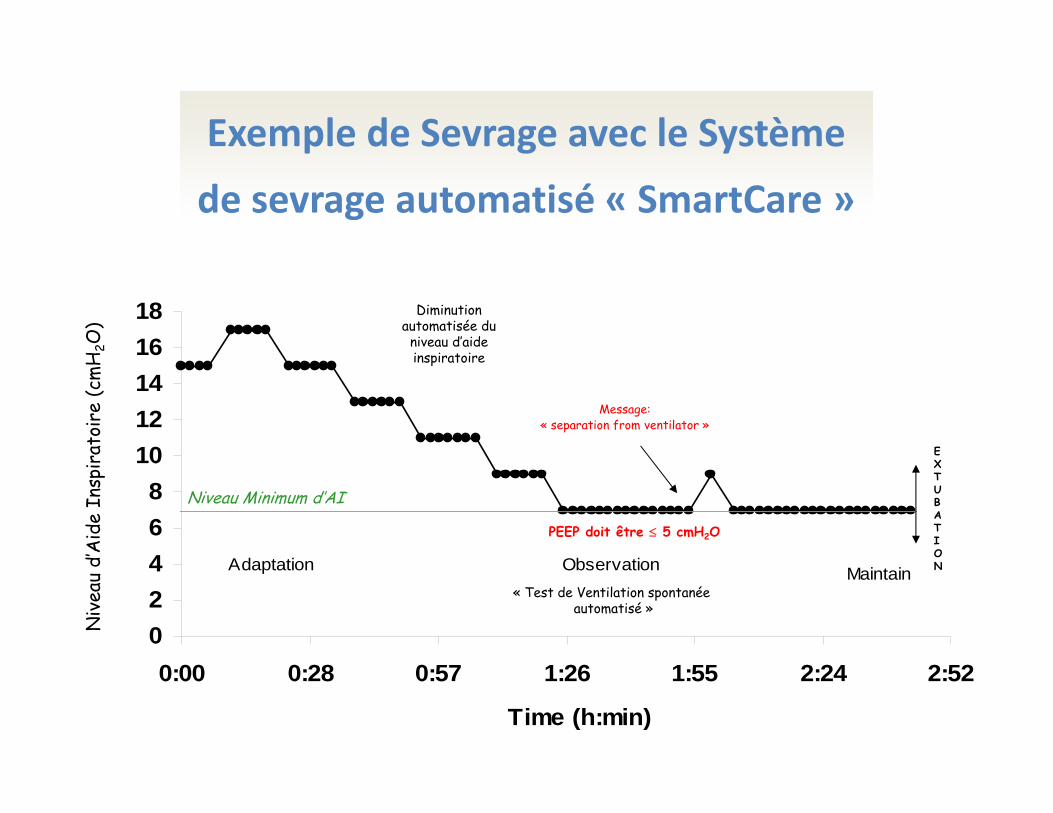
Observation MaintainAdaptation
Niveau Minimum d’AI
« Test de Ventilation spontanée automatisé »
EXTUBATION
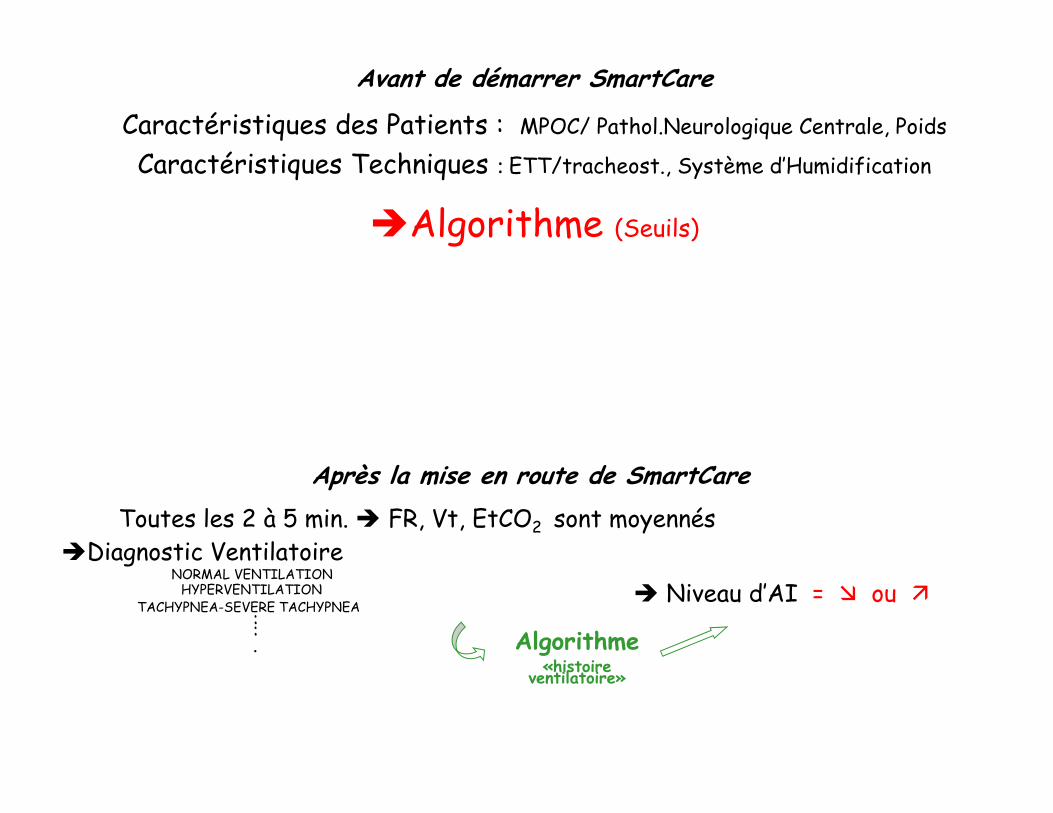
Après la mise en route de SmartCareToutes les 2 à 5 min. FR, Vt, EtCO2 sont moyennés
Diagnostic VentilatoireNORMAL VENTILATION
HYPERVENTILATIONTACHYPNEA-SEVERE TACHYPNEA
::. Algorithme
«histoire ventilatoire»
Niveau d’AI = ou
Diminution automatisée du
niveau d’aide inspiratoire
Message: « separation from ventilator »
PEEP doit être 5 cmH2O
Avant de démarrer SmartCare
Caractéristiques des Patients : MPOC/ Pathol.Neurologique Centrale, Poids
Caractéristiques Techniques : ETT/tracheost., Système d’Humidification
Algorithme (Seuils)
Exemple de Sevrage avec le Système de sevrage automatisé « SmartCare »
Niv
eau
d’A
ide
Insp
irat
oire
(cm
H2O
)
02468
1012141618
0:00 0:28 0:57 1:26 1:55 2:24 2:52
Time (h:min)
Leve
l of P
ress
ure
supp
ort (
cmH
2O
)
Observation MaintainAdaptation
Niveau Minimum d’AI
« Test de Ventilation spontanée automatisé »
EXTUBATION
Diminution automatisée du
niveau d’aide inspiratoire
Message: « separation from ventilator »
PEEP doit être 5 cmH2O
Avant de démarrer SmartCare
Caractéristiques des Patients : MPOC/ Pathol.Neurologique Centrale, Poids
Caractéristiques Techniques : ETT/tracheost., Système d’Humidification
Algorithme (Seuils)
Niv
eau
d’A
ide
Insp
irat
oire
(cm
H2O
)
Après la mise en route de SmartCareToutes les 2 à 5 min. FR, Vt, EtCO2 sont moyennés
Diagnostic VentilatoireNORMAL VENTILATION
HYPERVENTILATIONTACHYPNEA-SEVERE TACHYPNEA
::. Algorithme
«histoire ventilatoire»
Niveau d’AI = ou
02468
1012141618
0:00 0:28 0:57 1:26 1:55 2:24 2:52
Time (h:min)
Leve
l of P
ress
ure
supp
ort (
cmH
2O
)
Observation MaintainAdaptation
Niveau Minimum d’AI
« Test de Ventilation spontanée automatisé »
EXTUBATION
Diminution automatisée du
niveau d’aide inspiratoire
Message: « separation from ventilator »
PEEP doit être 5 cmH2O
Niv
eau
d’A
ide
Insp
irat
oire
(cm
H2O
)
Exemple de Sevrage avec le Système de sevrage automatisé « SmartCare »
0
10
20
30
40
50
60
70
1
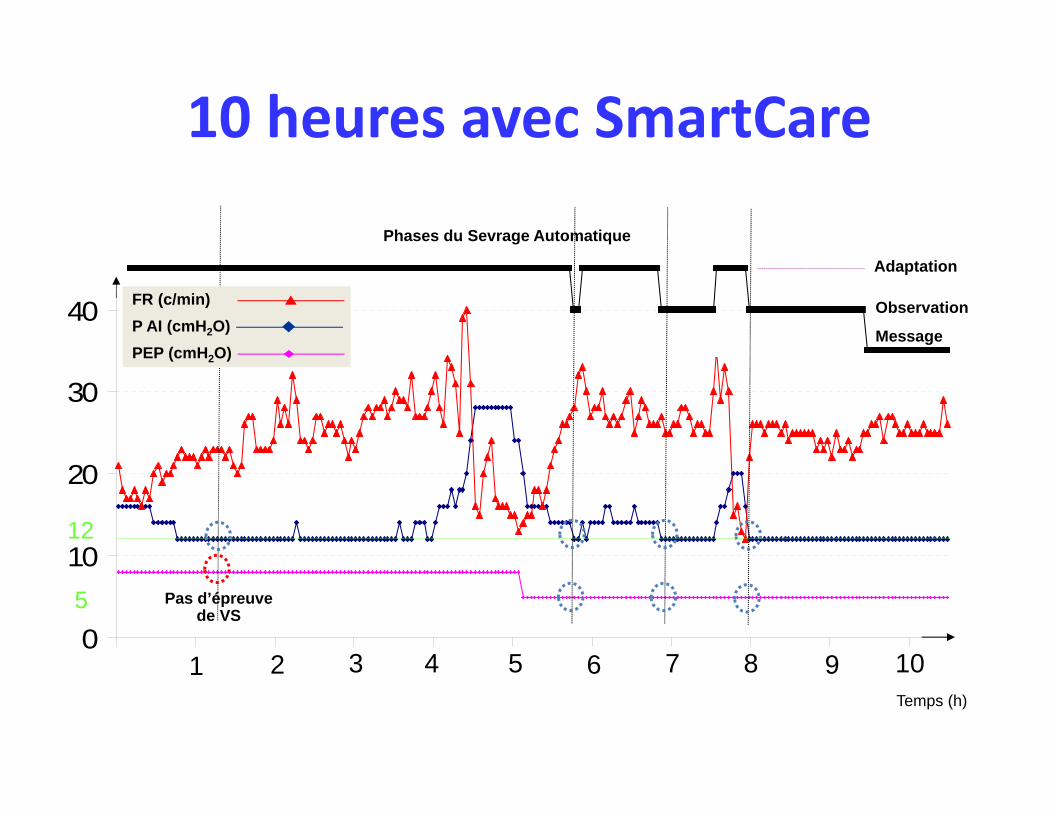
Diagnostic Respiratoire/Niveau d’assistance
Phases du Sevrage Automatique
Adaptation
Observation
Message
72 3 4 5 6 8 9 10Temps (h)
12
5
Epreuve VS n° 1
Epreuve VS n° 2
Epreuve VS n° 3
Sur-Assistance
Sous-Assistance
Pas d’épreuve de VS
FR (c/min)P AI (cmH2O)PEP (cmH2O)
10 heures avec SmartCare
0
10
20
30
40
50
60
70
1
Diagnostic Respiratoire/Niveau d’assistance
Phases du Sevrage Automatique
Adaptation
Observation
Message
72 3 4 5 6 8 9 10Temps (h)
12
5
Epreuve VS n° 1
Epreuve VS n° 2
Epreuve VS n° 3
Sur-Assistance
Sous-Assistance
Pas d’épreuve de VS
FR (c/min)P AI (cmH2O)PEP (cmH2O)
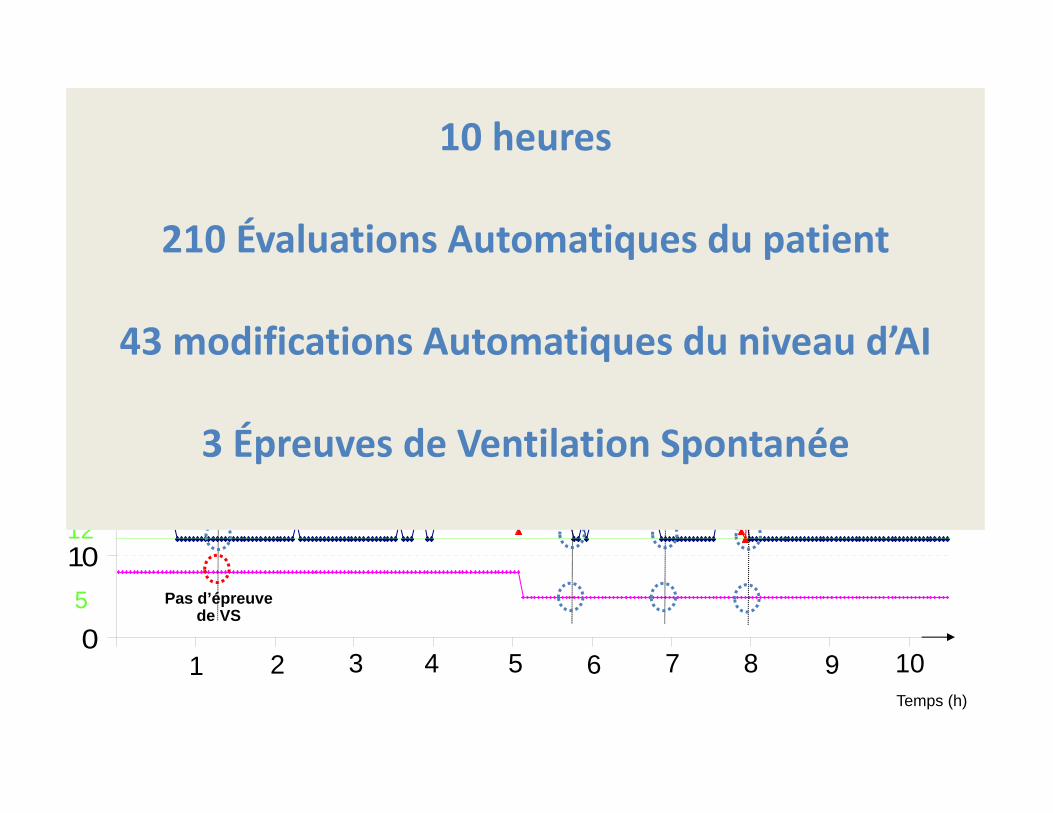
10 heures avec SmartCare10 heures
210 Évaluations Automatiques du patient
43 modifications Automatiques du niveau d’AI
3 Épreuves de Ventilation Spontanée
10 heures
210 Évaluations Automatiques du patient
43 modifications Automatiques du niveau d’AI
3 Épreuves de Ventilation Spontanée
Y E S
N O
Y E S N O
Y E S
E X T U B A T I O N
N O
Y E S
Y E S
N O
M e c h a n i c a l v e n t i l a t i o nQ u e s t i o n a t l e a s t 2 t i m e s a d a y :
W e a n i n g p o s s i b l e ?
I n i t i a t i o n o f w e a n i n g• S t o p o r l o w e r i n g o f s e d a t i o n• L e v e l o f P r e s s u r e S u p p o r t : 2 0 c m H 2 O
Q u e s t i o n a t l e a s t 2 t i m e s a d a y : S p o n t a n e o u s b r e a t h i n g t e s t f e a s i b l e ?
P S l e v e l 2 0 c m H 2 O a b o v e P E E P > 6 0 m i n u t e s ?
N OP a t i e n t w e a n e d b u t e x t u b a t i o n n o t p o s s i b l e
- L e v e l o f c o n s c i o u s n e s s O K- E f f i c i e n t s w a l l o w i n g- E f f i c i e n t c o u g h
E x t u b a t i o n p o s s i b l e ?
S p o n t a n e o u s b r e a t h i n g t e s t d u r i n g 3 0 'F i r s t c h o i c e : P r e s s u r e s u p p o r t 1 0 c m H 2 O , ± P E E P 5 c m H 2 OO t h e r c h o i c e s : - T - p i e c e t r i a l- C P A P , f l o w 3 0 l / m i n . P E E P 5 c m H 2 O
E x t u b a t i o n c r i t e r i a p r e s e n t ?
E x t u b a t i o n c r i t e r i a ( a l l m u s t b e p r e s e n t )- R e s p i r a t o r y r a t e 3 0 / '- P u l s e < 1 2 0 / '- S y s t . A B P < 1 8 0 a n d > 9 0 m m H g- N o h e m o d y n a m i c i n s t a b i l i t y- P a O 2 8 . 5 k P a a n d F I O 2 0 . 4 0- p H > 7 . 3 0
A d a p t a t i o n o f P S
a n d / o r P E E P l e v e l
S p o n t a n e o u s b r e a t h i n g t e s t f e a s i b l e i f a f t e r 6 0 ' w i t hP S 2 0 c m H 2 O , P E E P 5 c m H 2 O ( a l l m u s t b e
p r e s e n t ) :- R e s p i r a t o r y r a t e 3 0 / '- T i d a l v o l u m e 6 m l / k g- N o h e m o d y n a m i c i n s t a b i l i t y- S p O 2 9 0 % a n d F I O 2 0 . 4 0- N o o t h e r c o n t r a - i n d i c a t i o n
W e a n i n g p o s s i b l e i f a l l f o l l o w i n g c r i t e r i a a r e p r e s e n t :- I m p r o v e m e n t o f c o n d i t i o n h a v i n g l e d t o i n t u b a t i o n - A b s e n c e o f u n c o n t r o l l e d s e v e r e i n f e c t i o n- C o r r e c t i o n o f m e t a b o l i c d i s o r d e r s- A d e q u a t e h e m o g l o b i n l e v e l - N o h e m o d y n a m i c i n s t a b i l i t y- P a O 2 > 8 . 5 k P a w i t h F I O 2 0 . 4 0 a n d P E E P 5 c m H 2 O
Y E S
N O
Y E S N O
Y E S
E X T U B A T I O N
N O
Y E S
Y E S
N O
M e c h a n i c a l v e n t i l a t i o nQ u e s t i o n a t l e a s t 2 t i m e s a d a y :
W e a n i n g p o s s i b l e ?
I n i t i a t i o n o f w e a n i n g• S t o p o r l o w e r i n g o f s e d a t i o n• L e v e l o f P r e s s u r e S u p p o r t : 2 0 c m H 2 O
Q u e s t i o n a t l e a s t 2 t i m e s a d a y : S p o n t a n e o u s b r e a t h i n g t e s t f e a s i b l e ?
P S l e v e l 2 0 c m H 2 O a b o v e P E E P > 6 0 m i n u t e s ?
N OP a t i e n t w e a n e d b u t e x t u b a t i o n n o t p o s s i b l e
- L e v e l o f c o n s c i o u s n e s s O K- E f f i c i e n t s w a l l o w i n g- E f f i c i e n t c o u g h
E x t u b a t i o n p o s s i b l e ?
S p o n t a n e o u s b r e a t h i n g t e s t d u r i n g 3 0 'F i r s t c h o i c e : P r e s s u r e s u p p o r t 1 0 c m H 2 O , ± P E E P 5 c m H 2 OO t h e r c h o i c e s : - T - p i e c e t r i a l- C P A P , f l o w 3 0 l / m i n . P E E P 5 c m H 2 O
E x t u b a t i o n c r i t e r i a p r e s e n t ?
E x t u b a t i o n c r i t e r i a ( a l l m u s t b e p r e s e n t )- R e s p i r a t o r y r a t e 3 0 / '- P u l s e < 1 2 0 / '- S y s t . A B P < 1 8 0 a n d > 9 0 m m H g- N o h e m o d y n a m i c i n s t a b i l i t y- P a O 2 8 . 5 k P a a n d F I O 2 0 . 4 0- p H > 7 . 3 0
A d a p t a t i o n o f P S
a n d / o r P E E P l e v e l
S p o n t a n e o u s b r e a t h i n g t e s t f e a s i b l e i f a f t e r 6 0 ' w i t hP S 2 0 c m H 2 O , P E E P 5 c m H 2 O ( a l l m u s t b e
p r e s e n t ) :- R e s p i r a t o r y r a t e 3 0 / '- T i d a l v o l u m e 6 m l / k g- N o h e m o d y n a m i c i n s t a b i l i t y- S p O 2 9 0 % a n d F I O 2 0 . 4 0- N o o t h e r c o n t r a - i n d i c a t i o n
W e a n i n g p o s s i b l e i f a l l f o l l o w i n g c r i t e r i a a r e p r e s e n t :- I m p r o v e m e n t o f c o n d i t i o n h a v i n g l e d t o i n t u b a t i o n - A b s e n c e o f u n c o n t r o l l e d s e v e r e i n f e c t i o n- C o r r e c t i o n o f m e t a b o l i c d i s o r d e r s- A d e q u a t e h e m o g l o b i n l e v e l - N o h e m o d y n a m i c i n s t a b i l i t y- P a O 2 > 8 . 5 k P a w i t h F I O 2 0 . 4 0 a n d P E E P 5 c m H 2 O
W e a n i n g p r o c e s s c a n b e g i n i f :
T h e c a u s e o f t h e r e s p i r a t o r y f a i l u r e i s p a r t i a l l y o r c o m p l e t e l y c o n t r o l l e d , i n c l u d i n g a
S p O 2 9 0 % u n d e r F I O 2 0 . 5 a n d P E E P 5 c m H 2 O
H e m o d y n a m i c s t a b i l i t y ( S y s t o l i c B l o o d P r e s s u r e b e t w e e n 9 0 a n d 1 6 0 m m H g + P u l s e
b e t w e e n 6 0 a n d 1 2 5 / m i n u t e + a b s e n c e o f u n c o n t r o l l e d a r r h y t h m i a s )
T e m p e r a t u r e < 3 9 ° C
H a e m o g l o b i n 8 g / d L
A b s e n c e o f s i g n i f i c a n t h y d r o - e l e c t r o l y t e s a b n o r m a l i t i e s
P a t i e n t s c a n f o l l o w s i m p l e s o r d e r s a n d t h e r e i s n o t n e e d f o r h i g h d o s e o f s e d a t i v e s
F o r n e u r o l o g i c a l p a t i e n t s :
G l a s c o w C o m a S c a l e > 8 , I n t r a - C r a n i a l P r e s s u r e < 2 0 m m H g , C e r e b r a l P e r f u s i o n
P r e s s u r e > 6 0 m m H g
T h o s e p a t i e n t s w h o a c c o m p l i s h t h e s e c r i t e r i a w i l l f o l l o w a s p o n t a n e o u s b r e a t h i n g t e s t ( 2 h o u r s
T t u b e o r P r e s s u r e S u p p o r t V e n t i l a t i o n w i t h 7 c m H 2 O o f p r e s s u r e s u p p o r t a n d P o s i t i v e E n d
E x p i r a t o r y P r e s s u r e 5 c m H 2 O ) . N o t o l e r a n c e t o s p o n t a n e o u s b r e a t h i n g t e s t w i l l b e
c o n s i d e r e r i f :
R e s p i r a t o r y R a t e > 3 5 b p m + c l i n i c a l m a n i f e s t a t i o n *
H y p o x e m i a ( P a O 2 < 6 0 m m H g u n d e r O 2 f l o w 4 L / m i n )
A c i d o s i s ( p H 7 . 3 )
* C l i n i c a l m a n i f e s t a t i o n s : S y s t o l i c B l o o d P r e s s u r e 1 6 0 m m H g o r 9 0 m m H g , H e a r t R a t e
1 4 0 b p m o r a u g m e n t a t i o n o f 2 5 % o f b a s e l i n e , n e w a r r h y t h m i a , l o w e r c o n s c i e n c e l e v e l ,
s w e a t i n g o r a g i t a t i o n .
1 . P a t i e n t s w i l l b e e x t u b a t e d i f t h e y s u c c e s s f u l l y c o m p l e t e t h e 2 h o u r s s p o n t a n e o u s
b r e a t h i n g t r i a l a n d t h e y h a v e a n a d e q u a t e c o u g h
2 . F o r p a t i e n t s t h a t d o n o t t o l e r a t e t h e s p o n t a n e o u s b r e a t h i n g t e s t , w e a n i n g w i l l c o n t i n u e
o n P r e s s u r e S u p p o r t V e n t i l a t i o n . P r e s s u r e S u p p o r t w i l l b e a d j u s t e d t o a c h i e v e a
r e s p i r a t o r y f r e q u e n c y o f 2 5 - 3 0 b p m a n d a g o o d c l i n i c a l a d a p t a t i o n . P r e s s u r e S u p p o r t
w i l l b e d i m i n i s h e d a s s o o n a s p o s s i b l e f o l l o w i n g p a t i e n t ’ s c l i n i c a l t o l e r a n c e . P a t i e n t s
w i l l b e e x t u b a t e d i f t o l e r a t i n g l o w P r e s s u r e S u p p o r t l e v e l s ( n e x t t o 1 0 c m H 2 O ) w i t h
l o w P E E P l e v e l s ( 5 c m H 2 O ) i f c l i n i c a l t o l e r a n c e a n d c o u g h a r e a d e q u a t e .
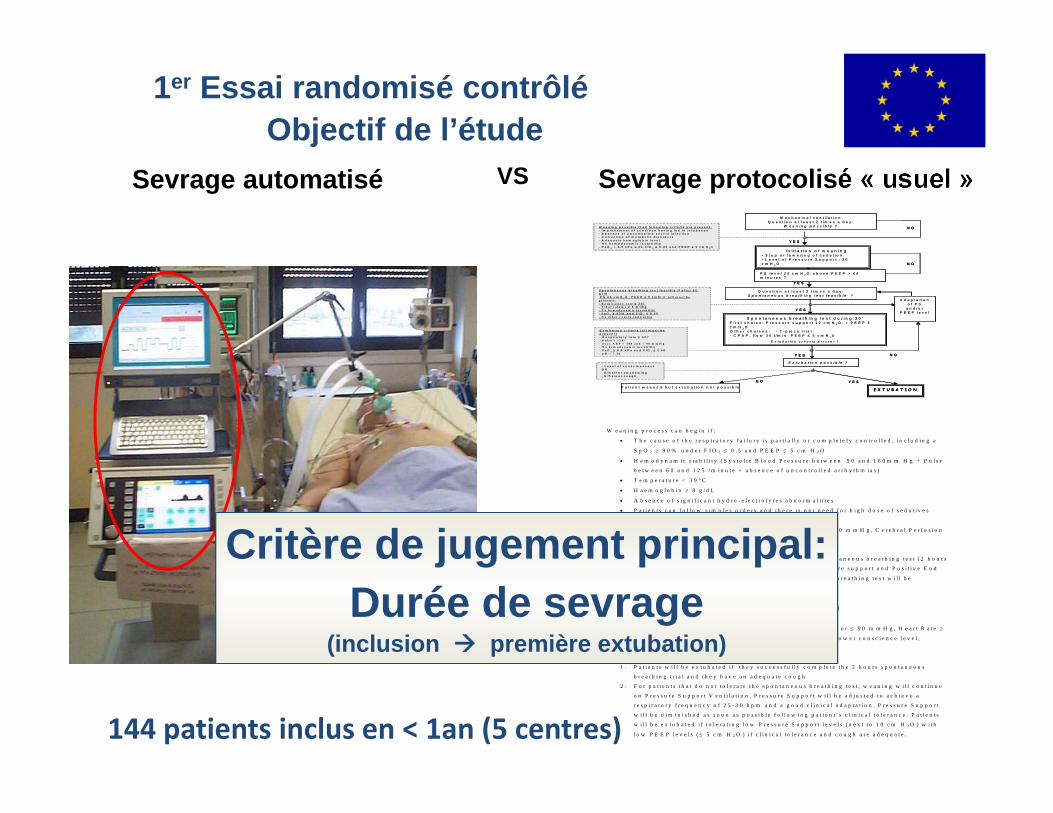
1er Essai randomisé contrôléObjectif de l’étude
Sevrage automatisé Sevrage protocolisé « usuel »VS
Critère de jugement principal: Durée de sevrage
(inclusion première extubation)
144 patients inclus en < 1an (5 centres)
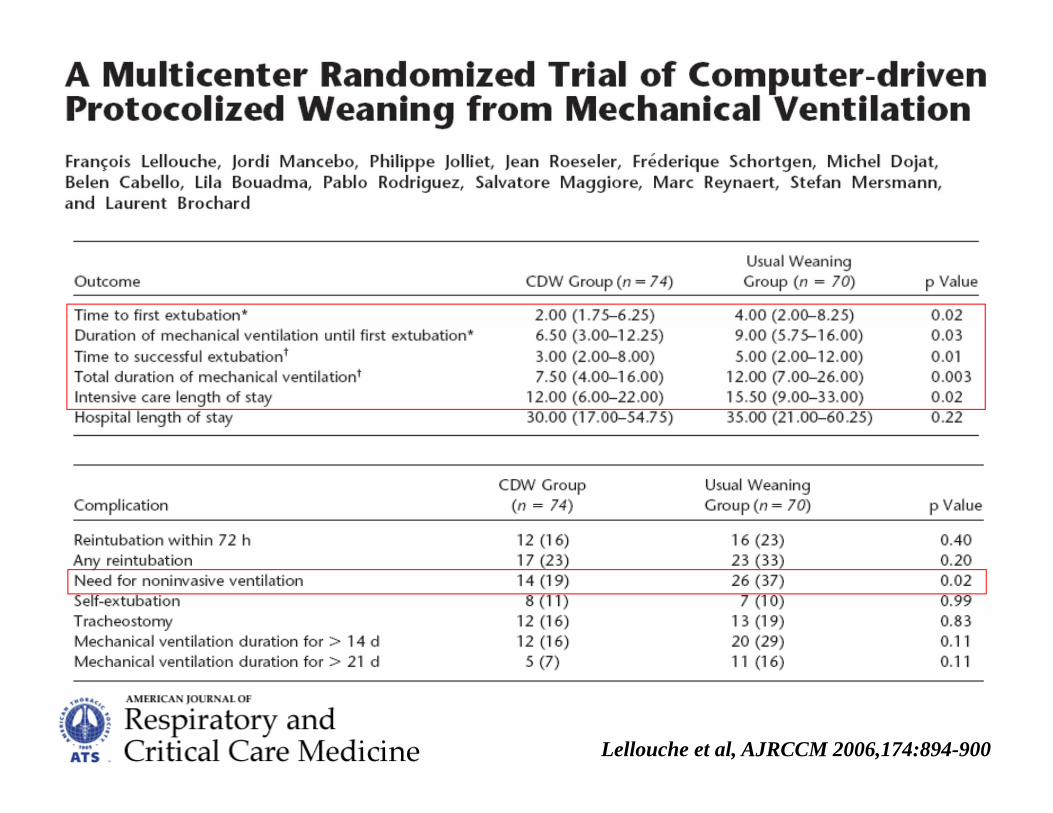
Lellouche et al, AJRCCM 2006,174:894-900
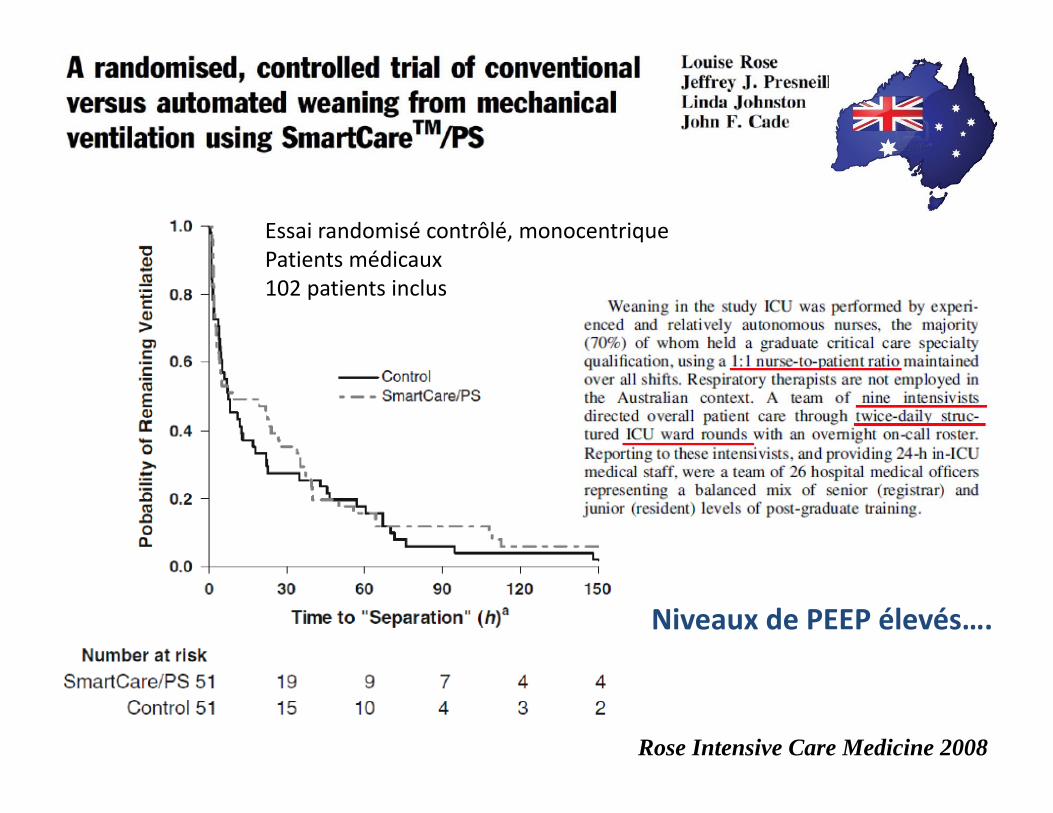
Rose Intensive Care Medicine 2008
Essai randomisé contrôlé, monocentriquePatients médicaux102 patients inclus
Niveaux de PEEP élevés….
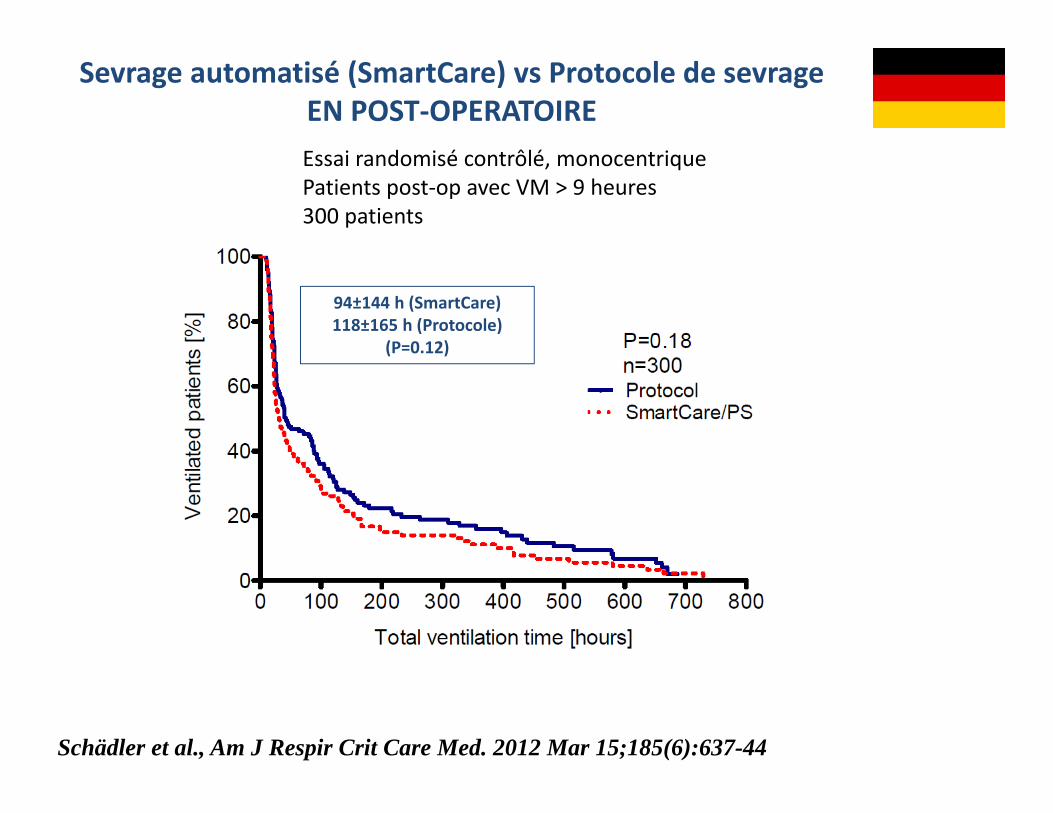
Sevrage automatisé (SmartCare) vs Protocole de sevrageEN POST‐OPERATOIREEssai randomisé contrôlé, monocentriquePatients post‐op avec VM > 9 heures300 patients
94±144 h (SmartCare)118±165 h (Protocole)
(P=0.12)
Schädler et al., Am J Respir Crit Care Med. 2012 Mar 15;185(6):637-44
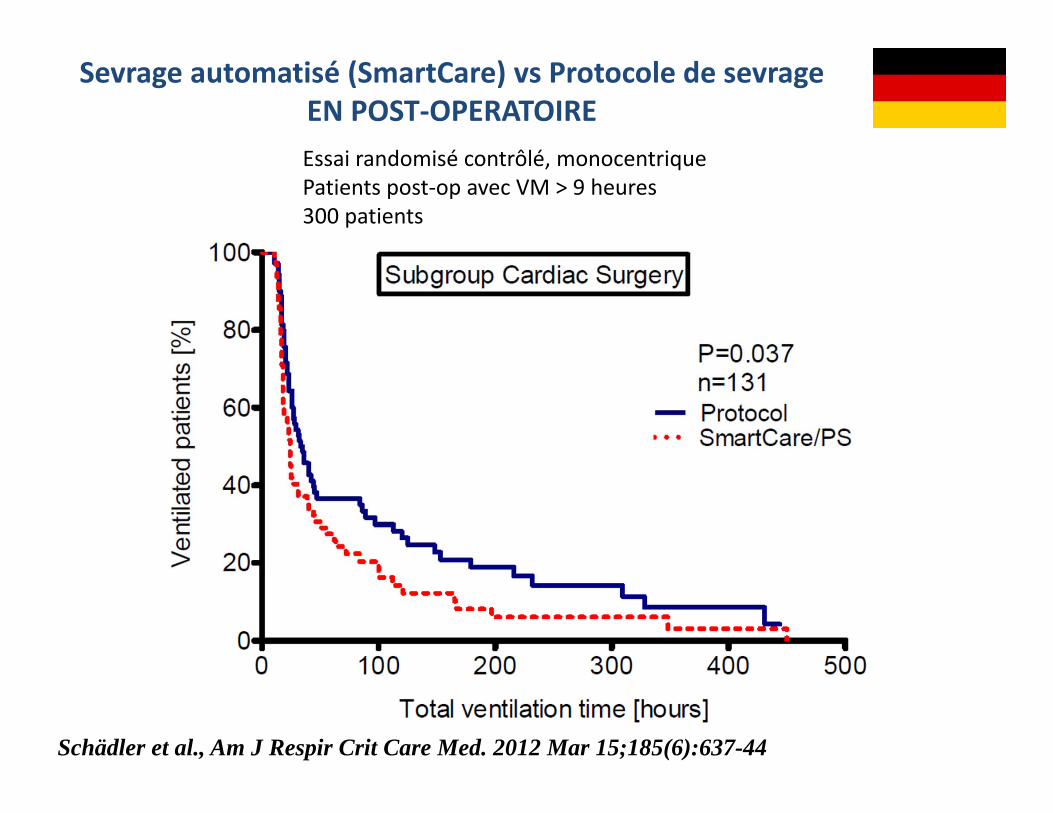
Sevrage automatisé (SmartCare) vs Protocole de sevrageEN POST‐OPERATOIREEssai randomisé contrôlé, monocentriquePatients post‐op avec VM > 9 heures300 patients
Schädler et al., Am J Respir Crit Care Med. 2012 Mar 15;185(6):637-44
WEAN Etude piloteCo-PI: K.Burns/F.Lellouche
Essai randomisé contrôlé, multicentrique, PILOTE
9 soins intensifs adultes
Sevrage automatisé (SmartCare) vs. Sevrage protocolisé
KE Burns, MO Meade, MR Lessard, L Hand, Q Zhou, SP Keenan and F Lellouche AJRCCM 2013
Population: Patients adultes nécessitant plus de 24 h de VM • Inclus à la phase précoce du sevrage• Dès que les patients tolèrent l’aide inspiratoire• Inclus si les patients échouent au test de VS ou en l’absence de critères de VS
Interventions: Sevrage automatisé (SmartCare™) vs Sevrage protocolisé (protocole écrit)
Commun aux 2 groupes: mode aide inspiratoire, évaluation des critères de VS, échelle PEEP/FiO2, protocole de sédation, critères d’extubation/réintubation, critères de VNI en cas de détresse post‐extubation.
Critère de jugement principal: Compliance et acceptance aux protocoles de sevrage et de sédation
Méthode
Variable Automated Weaning(n=50)
ProtocolizedWeaning(n=43)
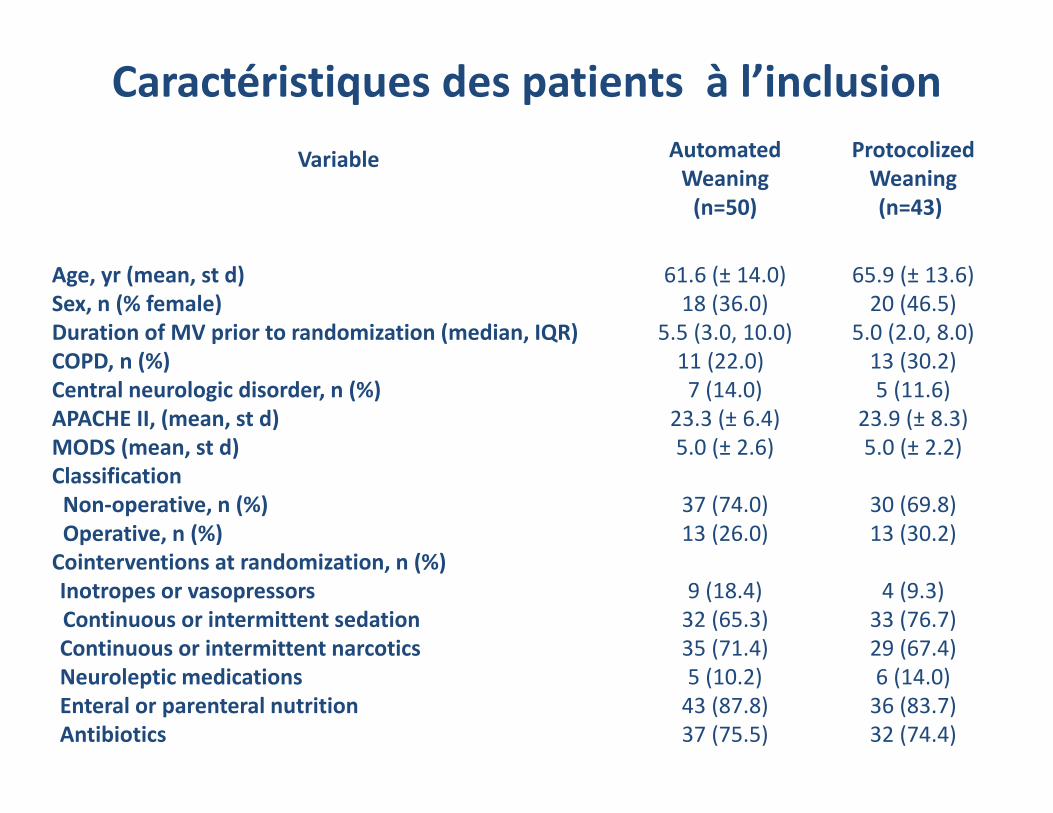
Age, yr (mean, st d) 61.6 (± 14.0) 65.9 (± 13.6)Sex, n (% female) 18 (36.0) 20 (46.5)Duration of MV prior to randomization (median, IQR) 5.5 (3.0, 10.0) 5.0 (2.0, 8.0)COPD, n (%) 11 (22.0) 13 (30.2)Central neurologic disorder, n (%) 7 (14.0) 5 (11.6)APACHE II, (mean, st d) 23.3 (± 6.4) 23.9 (± 8.3)MODS (mean, st d) 5.0 (± 2.6) 5.0 (± 2.2)ClassificationNon‐operative, n (%) Operative, n (%)
37 (74.0)13 (26.0)
30 (69.8)13 (30.2)
Cointerventions at randomization, n (%)Inotropes or vasopressorsContinuous or intermittent sedationContinuous or intermittent narcoticsNeuroleptic medicationsEnteral or parenteral nutritionAntibiotics
9 (18.4)32 (65.3)35 (71.4)5 (10.2)43 (87.8)37 (75.5)
4 (9.3)33 (76.7)29 (67.4)6 (14.0)36 (83.7)32 (74.4)
Caractéristiques des patients à l’inclusion
Automated Weaning(n=50)
ProtocolizedWeaning(n=43)
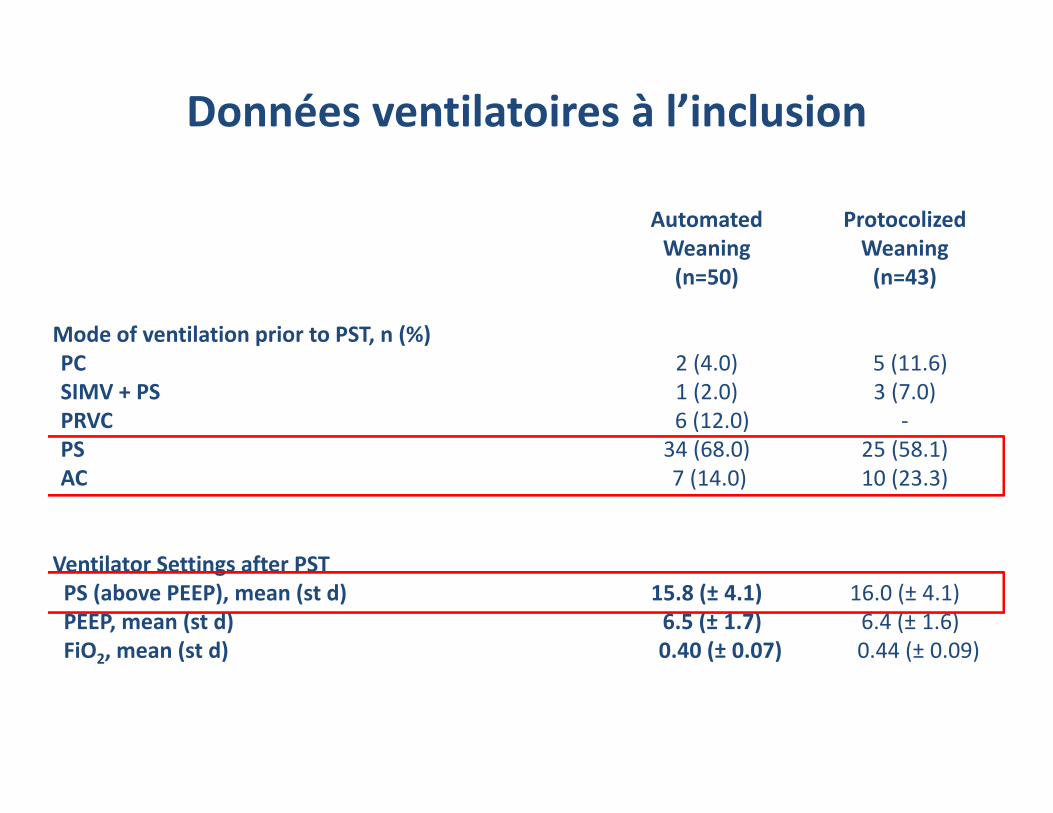
Mode of ventilation prior to PST, n (%)PC SIMV + PS PRVC PS AC
2 (4.0)1 (2.0)6 (12.0)34 (68.0)7 (14.0)
5 (11.6)3 (7.0)
‐25 (58.1)10 (23.3)
Ventilator Settings after PSTPS (above PEEP), mean (st d) PEEP, mean (st d) FiO2, mean (st d)
15.8 (± 4.1)6.5 (± 1.7)0.40 (± 0.07)
16.0 (± 4.1)6.4 (± 1.6)0.44 (± 0.09)
Données ventilatoires à l’inclusion
Weaning and Sedation Protocols Automated Weaning(n=50)
ProtocolizedWeaning(n=43)
p‐value
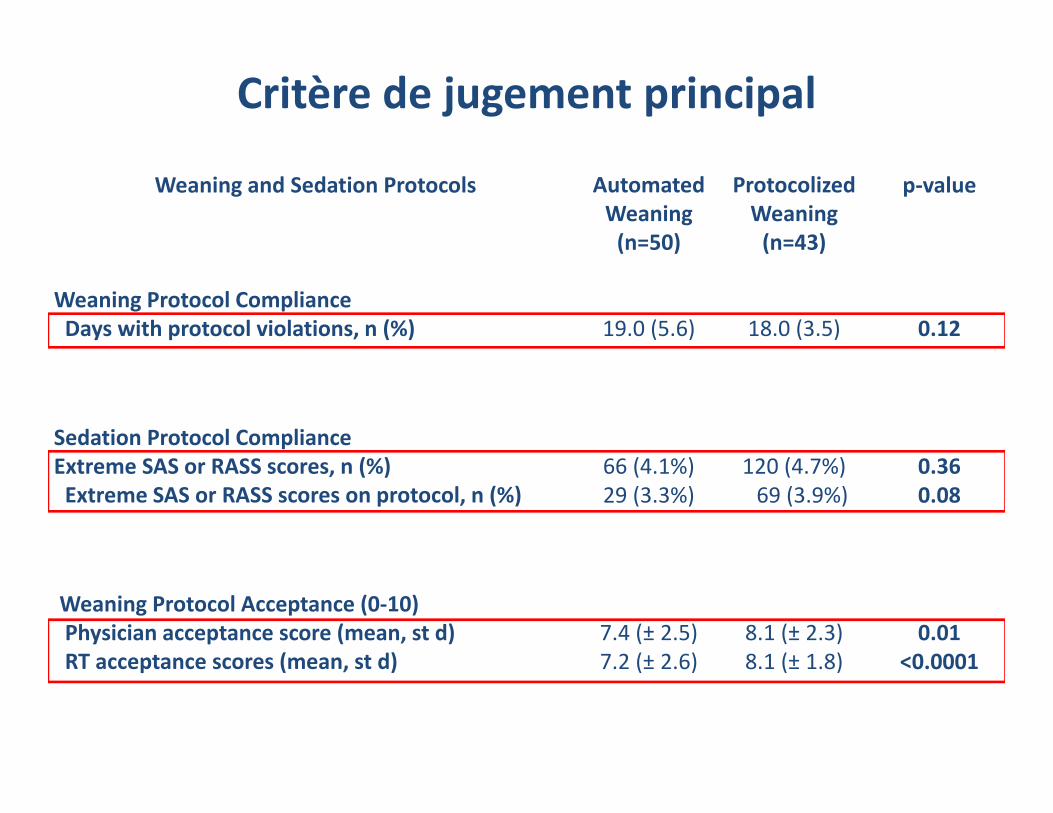
Weaning Protocol ComplianceDays with protocol violations, n (%) 19.0 (5.6) 18.0 (3.5) 0.12
Sedation Protocol ComplianceExtreme SAS or RASS scores, n (%)Extreme SAS or RASS scores on protocol, n (%)
66 (4.1%)29 (3.3%)
120 (4.7%)69 (3.9%)
0.360.08
Weaning Protocol Acceptance (0‐10)Physician acceptance score (mean, st d)RT acceptance scores (mean, st d)
7.4 (± 2.5)7.2 (± 2.6)
8.1 (± 2.3)8.1 (± 1.8)
0.01<0.0001
Critère de jugement principal
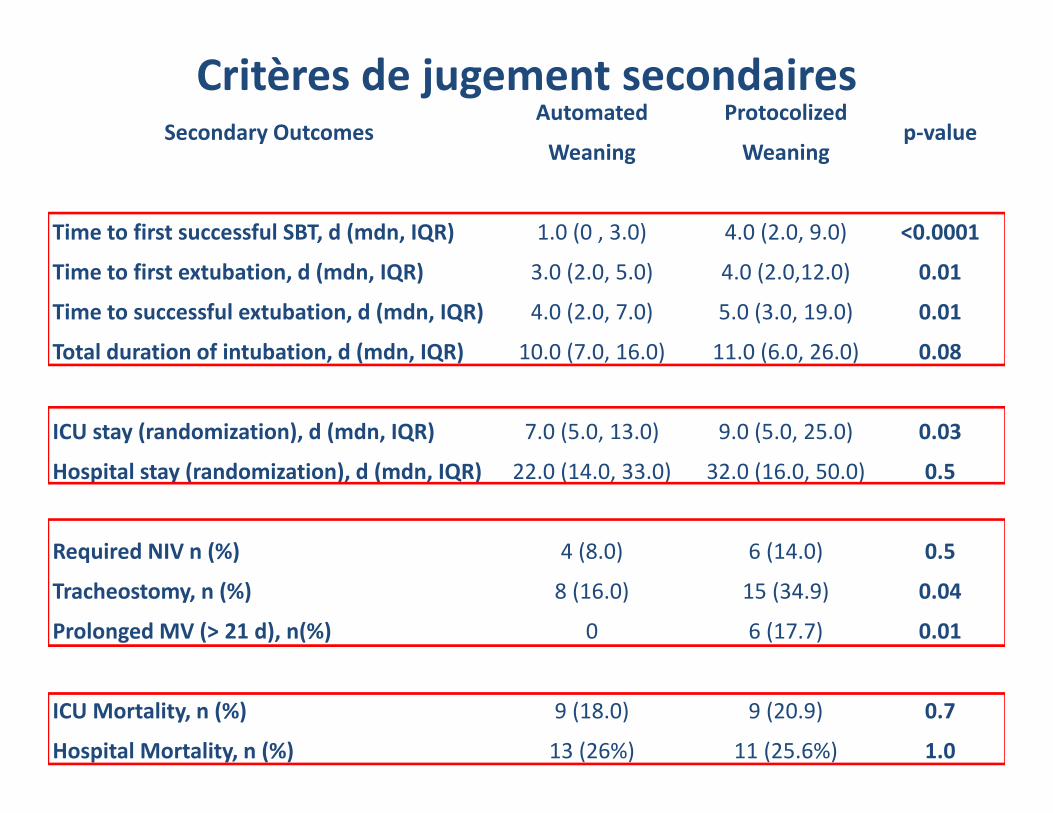
Secondary OutcomesAutomated
Weaning
Protocolized
Weaningp‐value
Time to first successful SBT, d (mdn, IQR) 1.0 (0 , 3.0) 4.0 (2.0, 9.0) <0.0001
Time to first extubation, d (mdn, IQR) 3.0 (2.0, 5.0) 4.0 (2.0,12.0) 0.01
Time to successful extubation, d (mdn, IQR) 4.0 (2.0, 7.0) 5.0 (3.0, 19.0) 0.01
Total duration of intubation, d (mdn, IQR) 10.0 (7.0, 16.0) 11.0 (6.0, 26.0) 0.08
ICU stay (randomization), d (mdn, IQR) 7.0 (5.0, 13.0) 9.0 (5.0, 25.0) 0.03
Hospital stay (randomization), d (mdn, IQR) 22.0 (14.0, 33.0) 32.0 (16.0, 50.0) 0.5
Required NIV n (%) 4 (8.0) 6 (14.0) 0.5
Tracheostomy, n (%) 8 (16.0) 15 (34.9) 0.04
Prolonged MV (> 21 d), n(%) 0 6 (17.7) 0.01
ICU Mortality, n (%) 9 (18.0) 9 (20.9) 0.7
Hospital Mortality, n (%) 13 (26%) 11 (25.6%) 1.0
Critères de jugement secondaires
Méta‐analyse à venir ……
SmartCare™ versus Non‐automated Weaning Strategies for Critically Ill Adults:
A Systematic Review and Meta‐analysis.
Karen EA Burns, Francois Lellouche, Rosane Nisenbaum, Martin Lessard and Jan O. Friedrich
LIMITATIONS DU SMARTCARE
Limitations de l’Aide Inspiratoire: dans certaines populations Tube en T > AIAsynchronies avec certaines populations (MPOC)
Un seul paramètre ajusté automatiquement
Pourquoi des modes automatisés en ventilation mécanique ?
SmartCare: Ajustement de l’aide inspiratoire, sevrage automatiséRésultats de l’étude pilote WEAN
PLAN
Intellivent: Ventilation mécanique automatiséeRésultats de l’étude CLOSER 1 (post‐op chirurgie cardiaque)Données chez des patients médicaux
Évaluation des nouveaux modes, quels critères ?
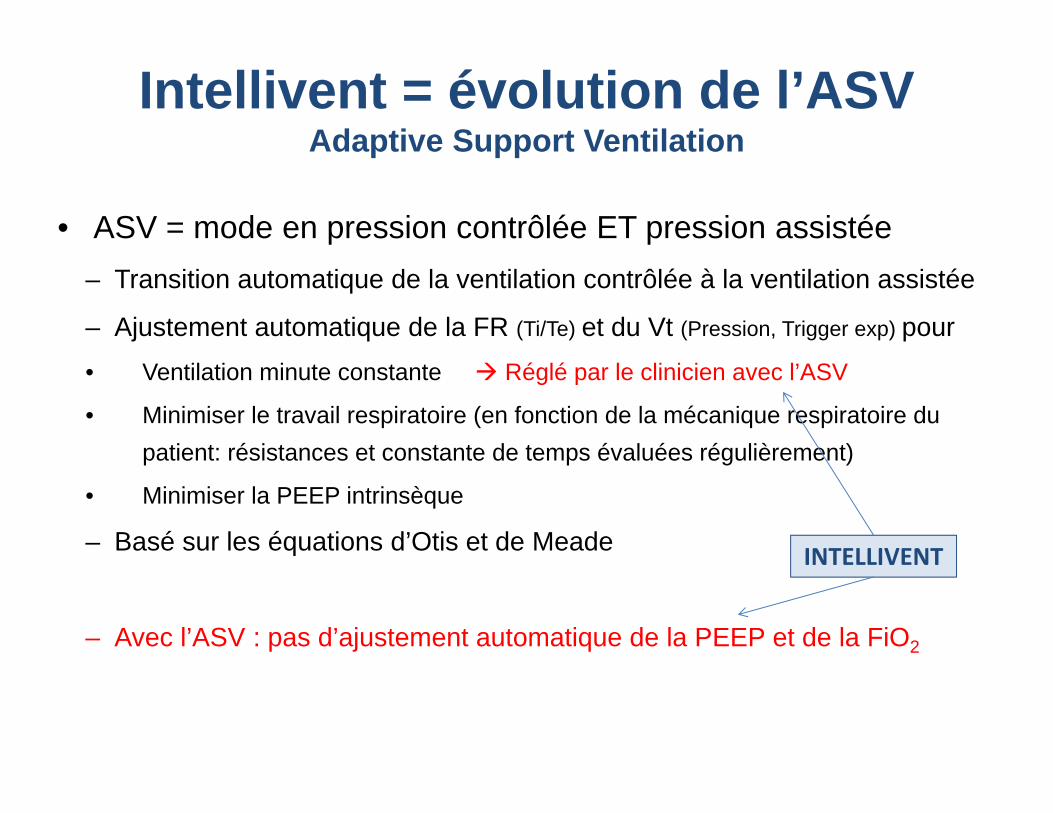
Intellivent = évolution de l’ASVAdaptive Support Ventilation
• ASV = mode en pression contrôlée ET pression assistée– Transition automatique de la ventilation contrôlée à la ventilation assistée
– Ajustement automatique de la FR (Ti/Te) et du Vt (Pression, Trigger exp) pour • Ventilation minute constante Réglé par le clinicien avec l’ASV
• Minimiser le travail respiratoire (en fonction de la mécanique respiratoire du patient: résistances et constante de temps évaluées régulièrement)
• Minimiser la PEEP intrinsèque
– Basé sur les équations d’Otis et de Meade
– Avec l’ASV : pas d’ajustement automatique de la PEEP et de la FiO2
INTELLIVENT
Control
Patient Monitor Alarms
Ventilateur
Control
Patient Monitor Alarms
PatientPatient
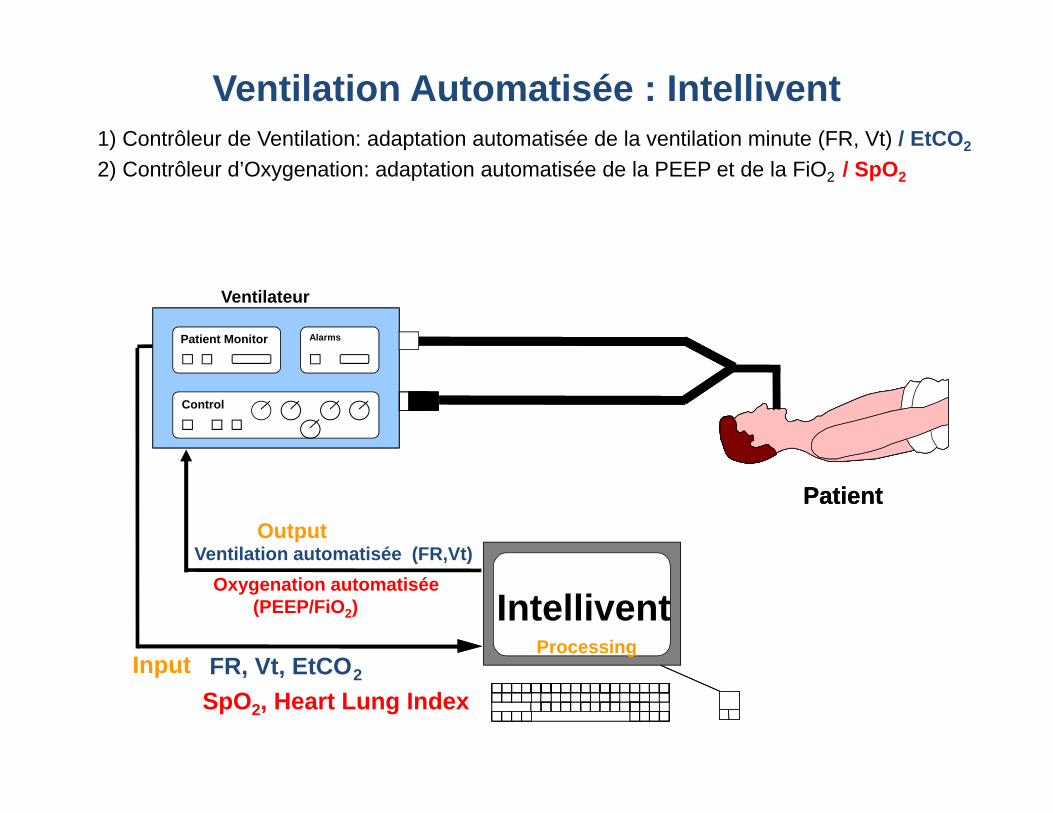
Ventilation Automatisée : Intellivent1) Contrôleur de Ventilation: adaptation automatisée de la ventilation minute (FR, Vt) / EtCO2
2) Contrôleur d’Oxygenation: adaptation automatisée de la PEEP et de la FiO2 / SpO2
FR, Vt, EtCO2Input
Ventilation automatisée (FR,Vt)Oxygenation automatisée
(PEEP/FiO2)
Output
AutomaticWeaningSystemIntellivent
Processing
SpO2, Heart Lung Index
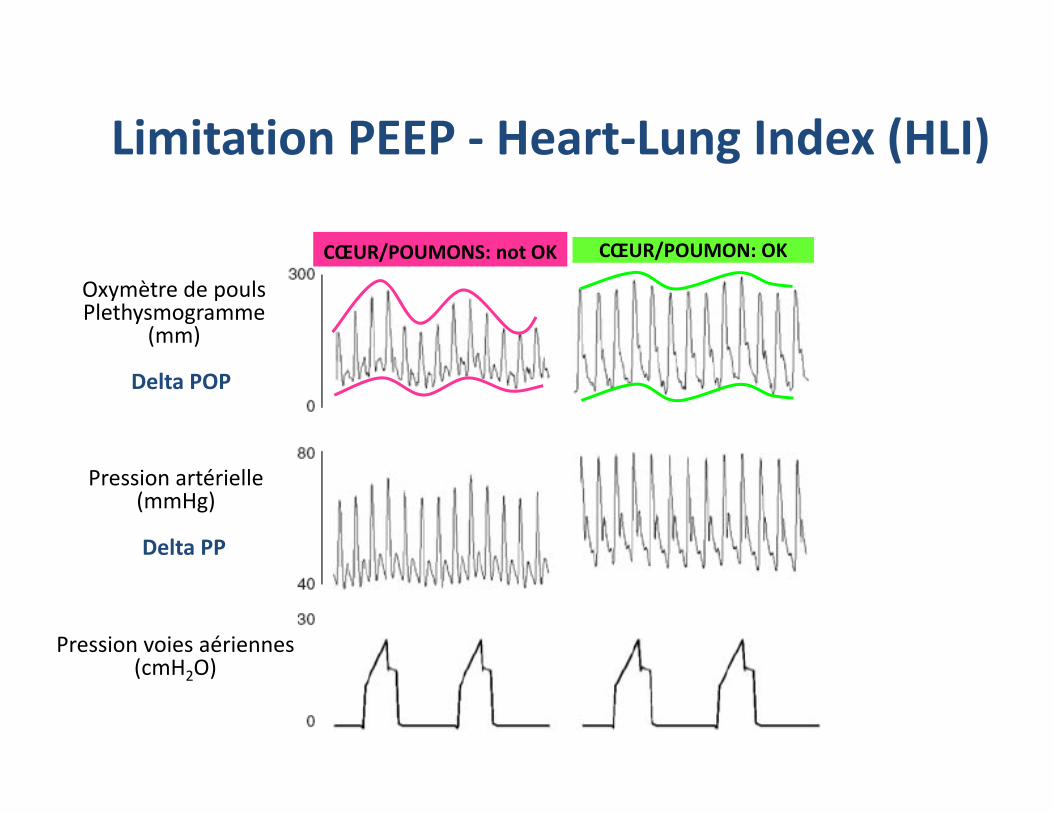
Limitation PEEP ‐ Heart‐Lung Index (HLI)
CŒUR/POUMONS: not OK CŒUR/POUMON: OK
Oxymètre de poulsPlethysmogramme
(mm)
Pression artérielle(mmHg)
Pression voies aériennes(cmH2O)
Delta POP
Delta PP
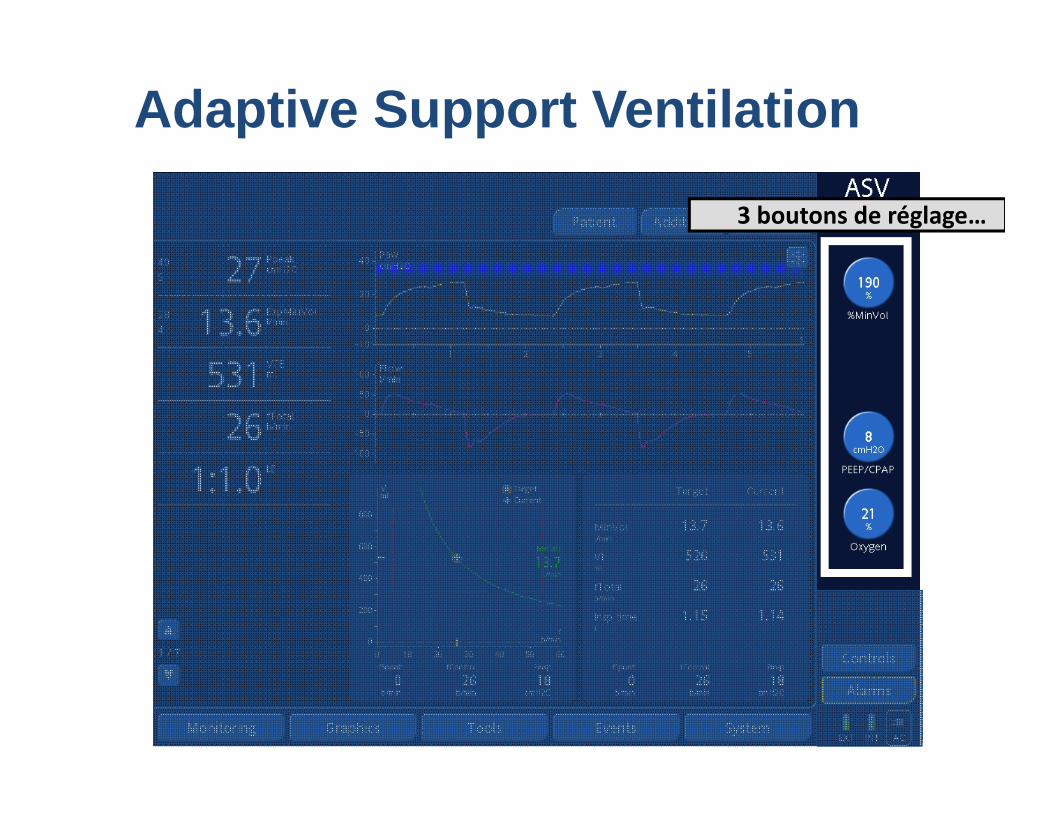
Adaptive Support Ventilation
3 boutons de réglage…
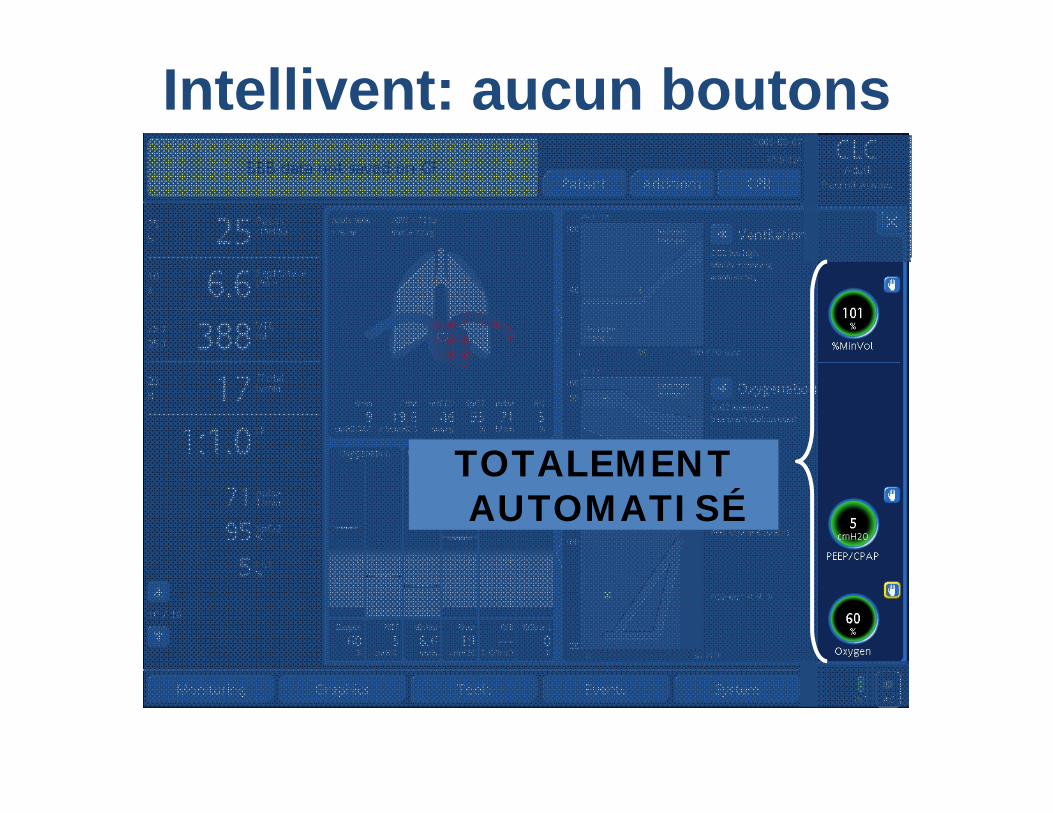
Intellivent: aucun boutons
TOTALEMENT AUTOMATISÉ
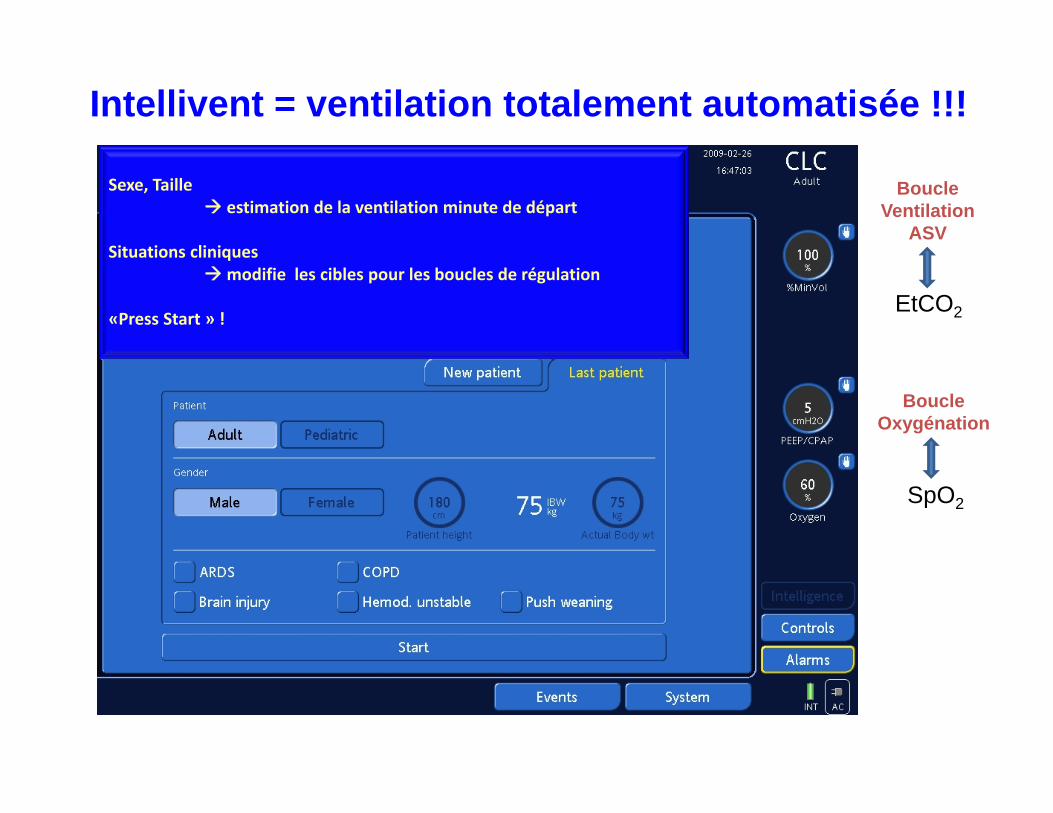
Intellivent = ventilation totalement automatisée !!!
Sexe, Taille estimation de la ventilation minute de départ
Situations cliniquesmodifie les cibles pour les boucles de régulation
«Press Start » !
Boucle Ventilation
ASV
Boucle Oxygénation
EtCO2
SpO2
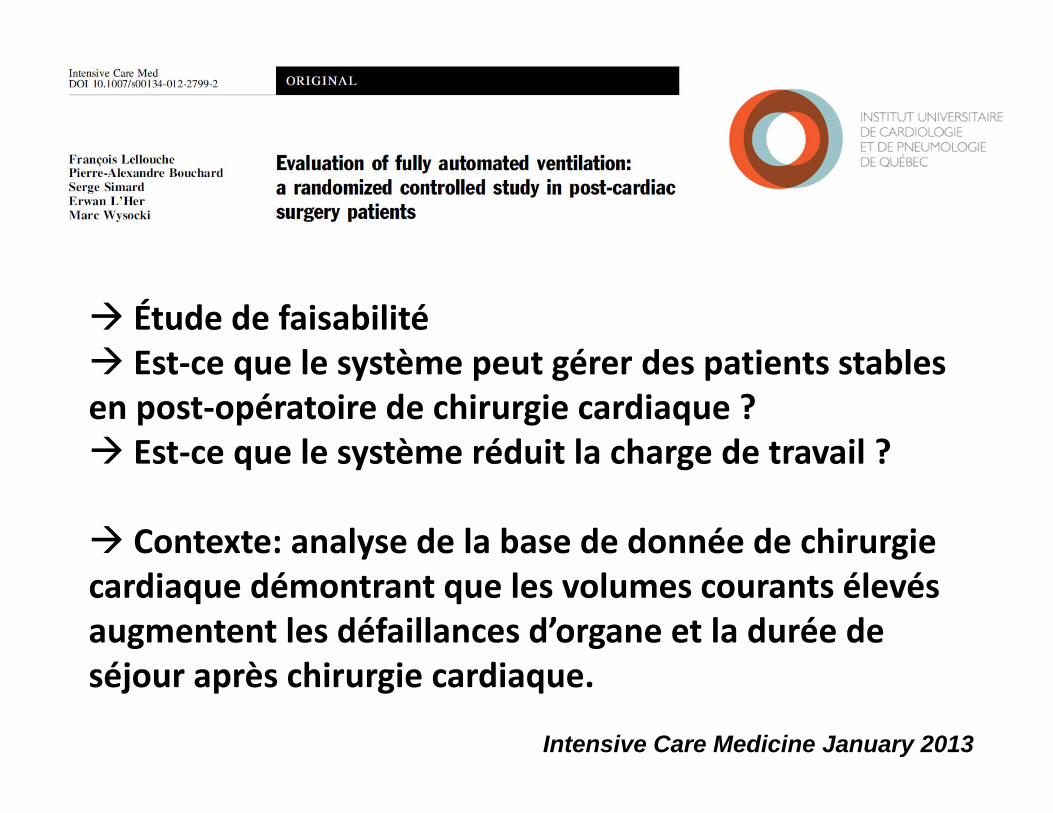
Étude de faisabilité Est‐ce que le système peut gérer des patients stables en post‐opératoire de chirurgie cardiaque ? Est‐ce que le système réduit la charge de travail ?
Contexte: analyse de la base de donnée de chirurgie cardiaque démontrant que les volumes courants élevés augmentent les défaillances d’organe et la durée de séjour après chirurgie cardiaque.
Intensive Care Medicine January 2013
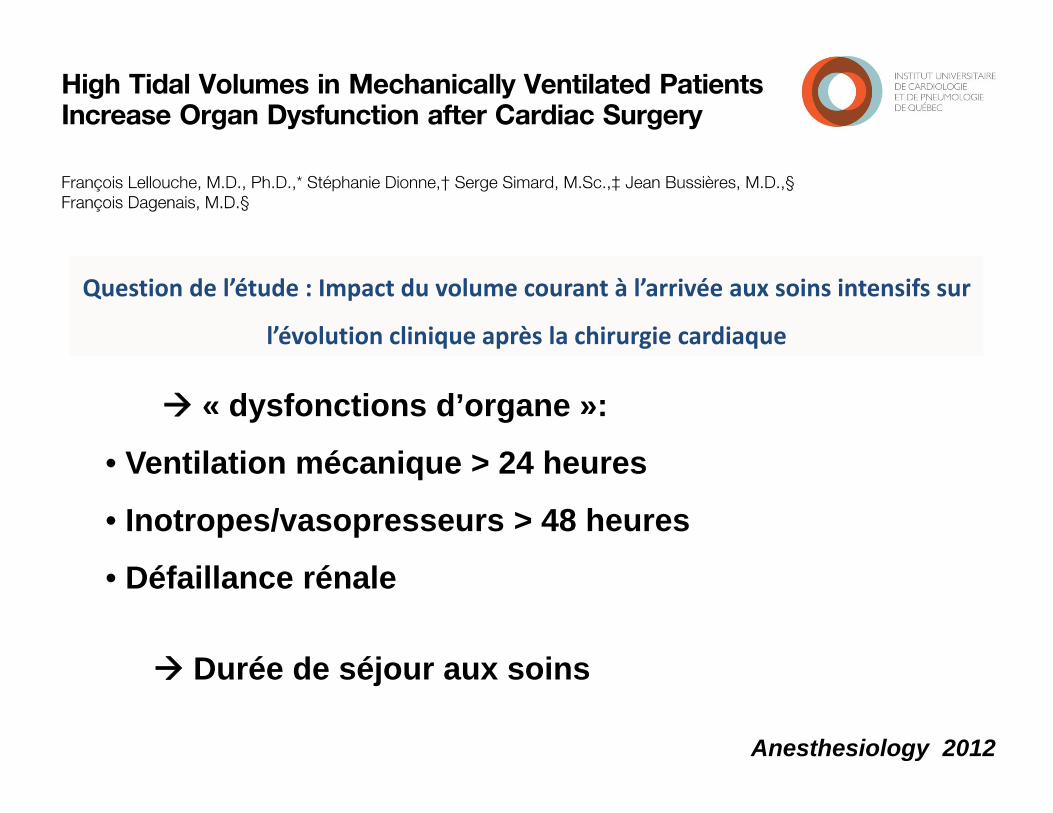
Anesthesiology 2012
Question de l’étude : Impact du volume courant à l’arrivée aux soins intensifs sur
l’évolution clinique après la chirurgie cardiaque
« dysfonctions d’organe »:
• Ventilation mécanique > 24 heures
• Inotropes/vasopresseurs > 48 heures
• Défaillance rénale
Durée de séjour aux soins
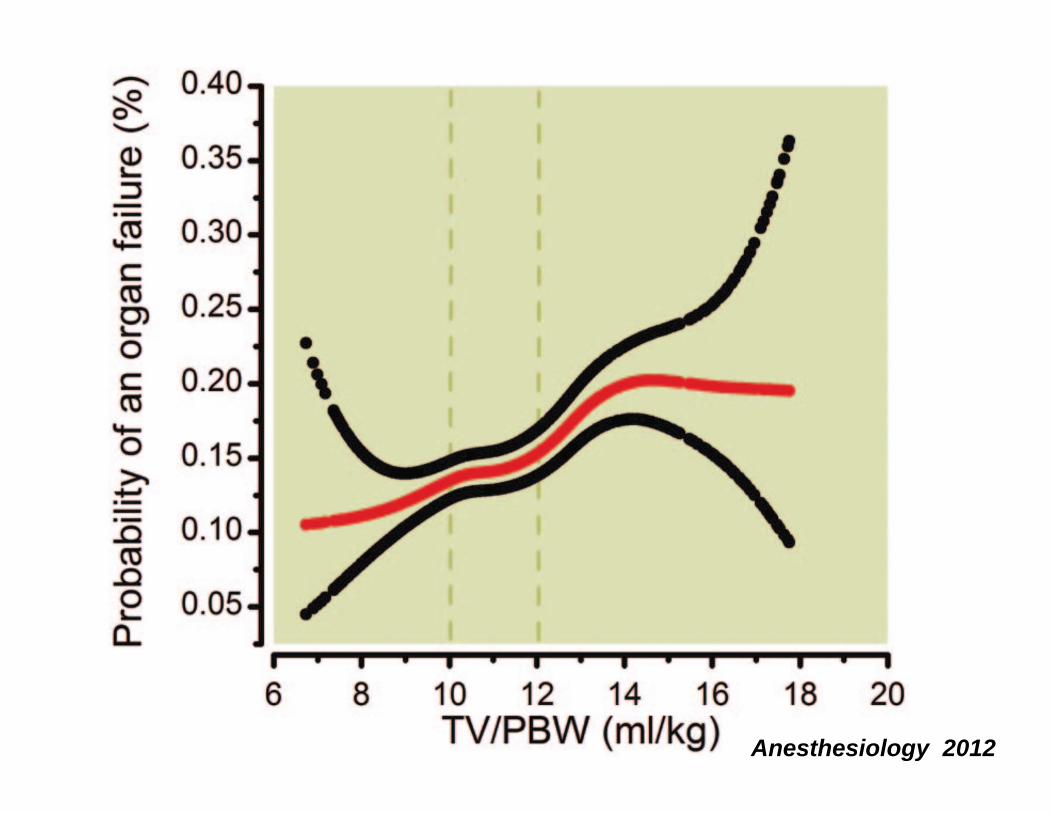
Anesthesiology 2012
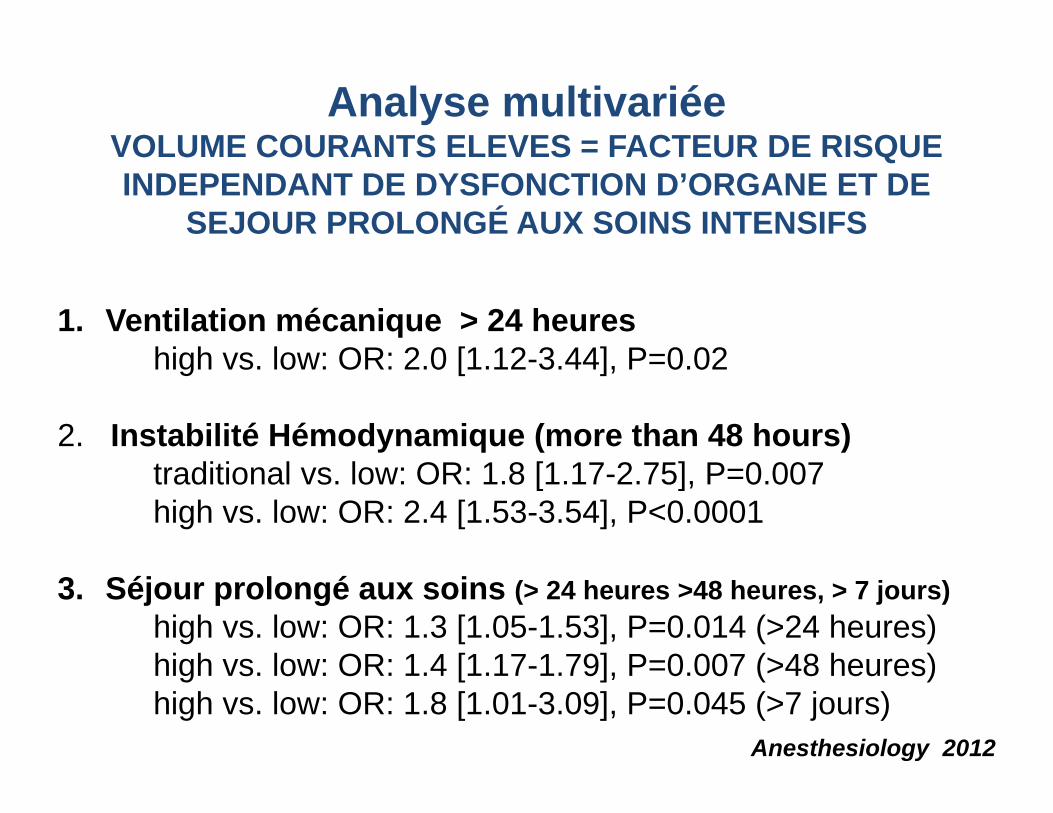
1. Ventilation mécanique > 24 heureshigh vs. low: OR: 2.0 [1.12-3.44], P=0.02
2. Instabilité Hémodynamique (more than 48 hours)traditional vs. low: OR: 1.8 [1.17-2.75], P=0.007 high vs. low: OR: 2.4 [1.53-3.54], P<0.0001
3. Séjour prolongé aux soins (> 24 heures >48 heures, > 7 jours)high vs. low: OR: 1.3 [1.05-1.53], P=0.014 (>24 heures)high vs. low: OR: 1.4 [1.17-1.79], P=0.007 (>48 heures)high vs. low: OR: 1.8 [1.01-3.09], P=0.045 (>7 jours)
Analyse multivariéeVOLUME COURANTS ELEVES = FACTEUR DE RISQUE INDEPENDANT DE DYSFONCTION D’ORGANE ET DE
SEJOUR PROLONGÉ AUX SOINS INTENSIFS
Anesthesiology 2012
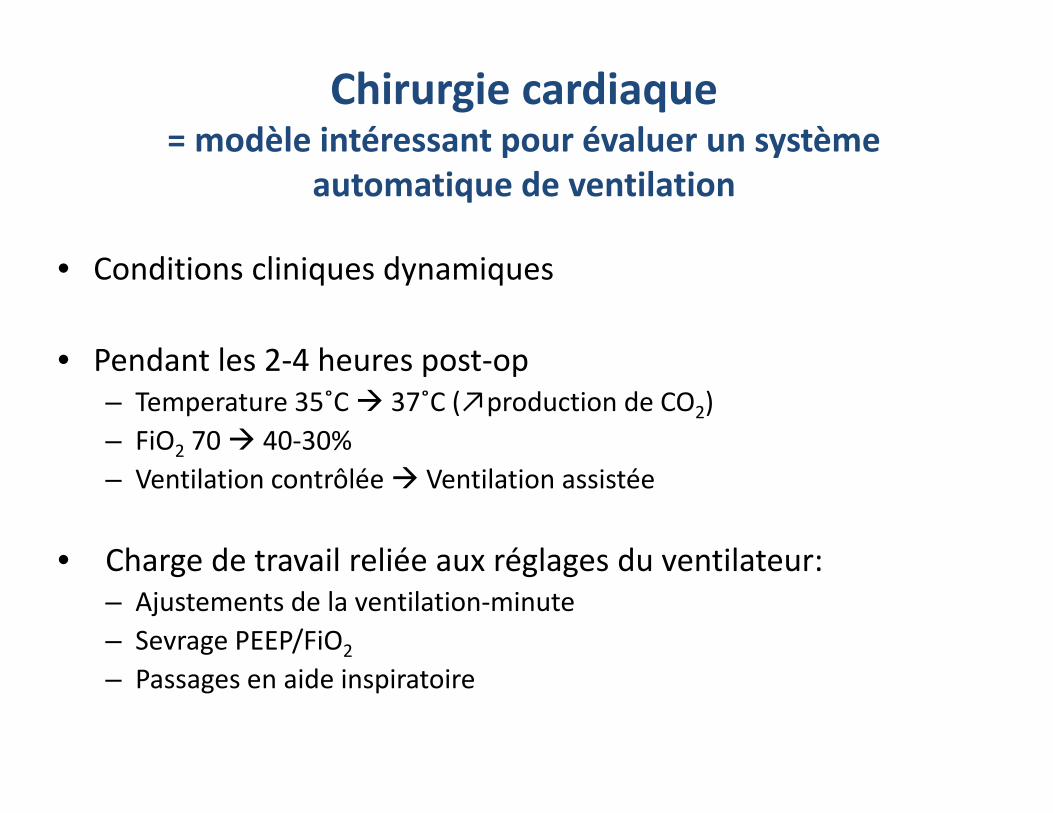
Chirurgie cardiaque= modèle intéressant pour évaluer un système
automatique de ventilation
• Conditions cliniques dynamiques
• Pendant les 2‐4 heures post‐op– Temperature 35˚C 37˚C (↗production de CO2)– FiO2 70 40‐30%– Ventilation contrôlée Ventilation assistée
• Charge de travail reliée aux réglages du ventilateur: – Ajustements de la ventilation‐minute– Sevrage PEEP/FiO2
– Passages en aide inspiratoire
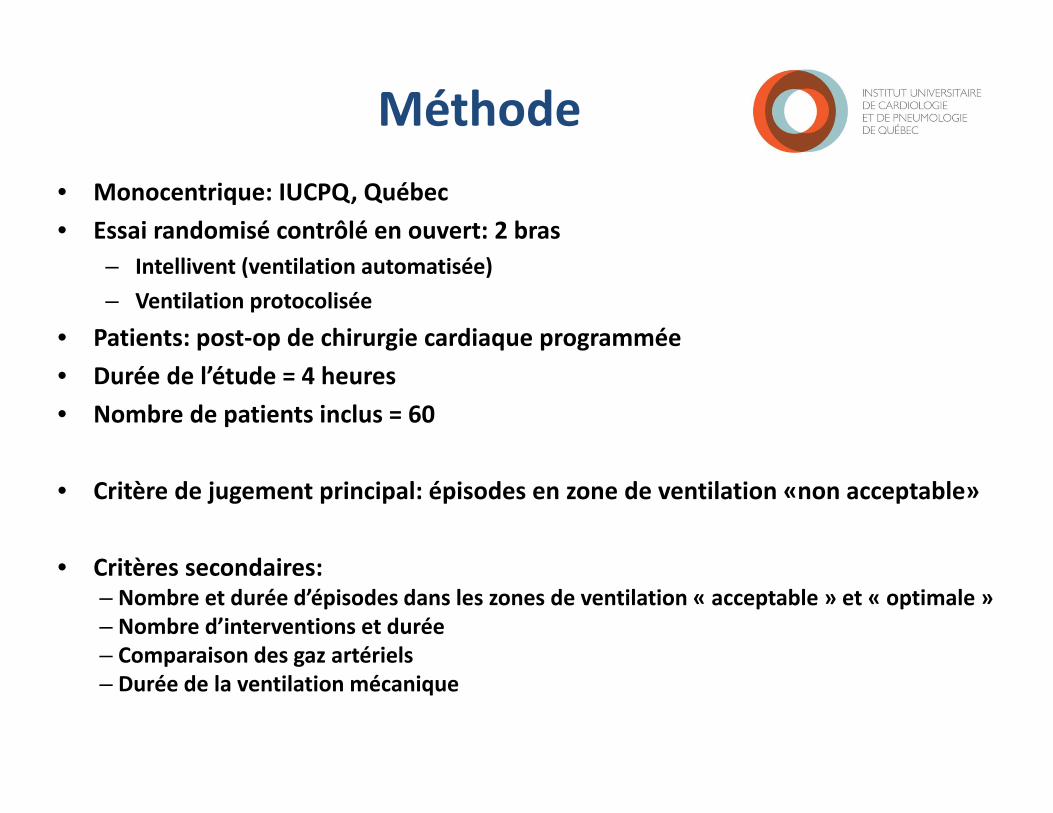
Méthode• Monocentrique: IUCPQ, Québec• Essai randomisé contrôlé en ouvert: 2 bras
– Intellivent (ventilation automatisée)– Ventilation protocolisée
• Patients: post‐op de chirurgie cardiaque programmée• Durée de l’étude = 4 heures• Nombre de patients inclus = 60
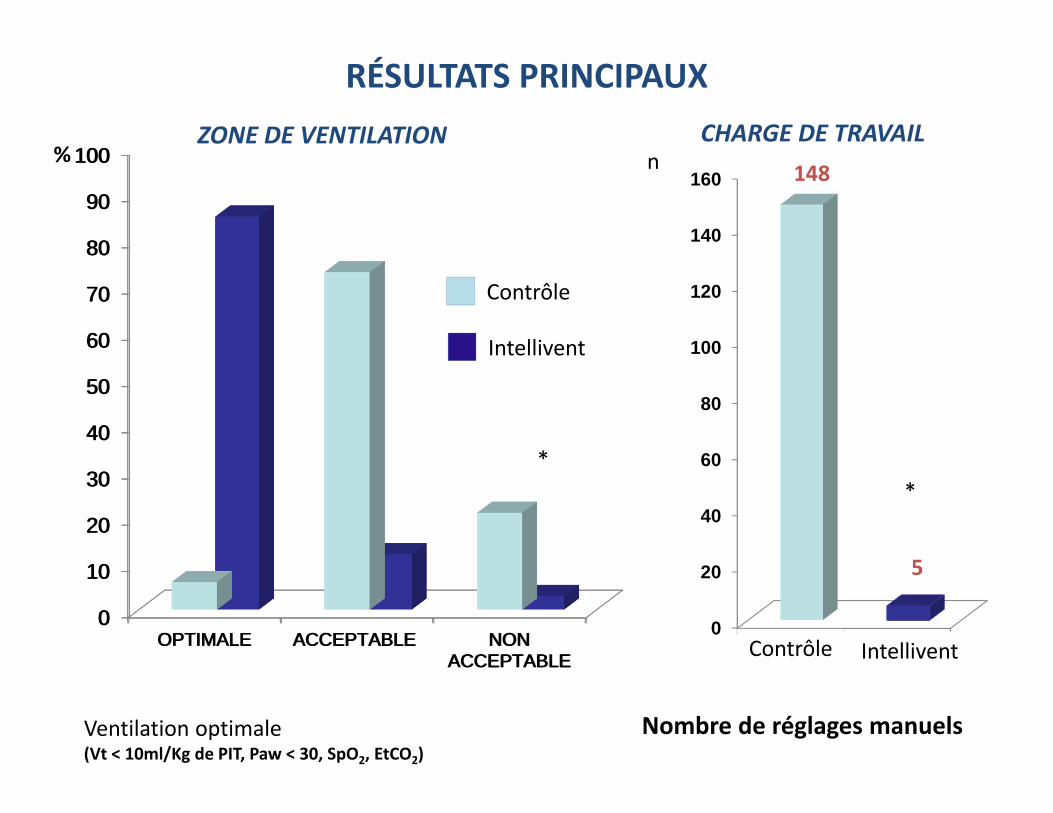
• Critère de jugement principal: épisodes en zone de ventilation «non acceptable»
• Critères secondaires: – Nombre et durée d’épisodes dans les zones de ventilation « acceptable » et « optimale »– Nombre d’interventions et durée– Comparaison des gaz artériels– Durée de la ventilation mécanique
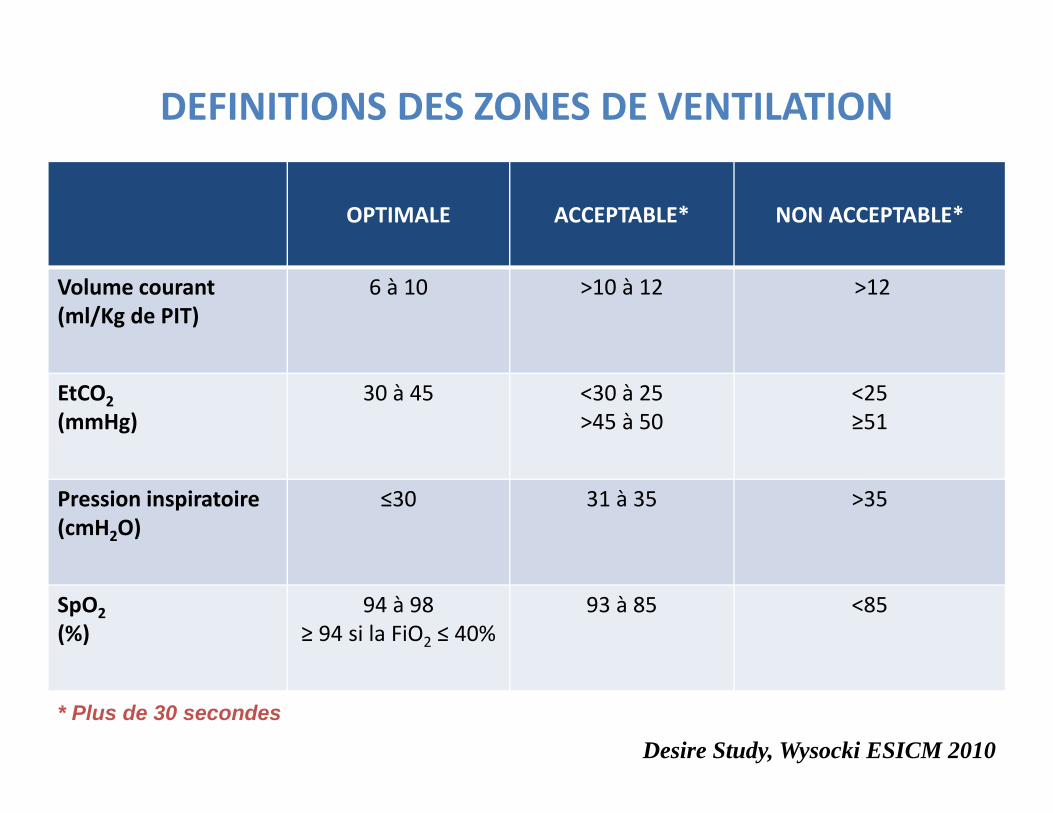
DEFINITIONS DES ZONES DE VENTILATION
OPTIMALE ACCEPTABLE* NON ACCEPTABLE*
Volume courant(ml/Kg de PIT)
6 à 10 >10 à 12 >12
EtCO2(mmHg)
30 à 45 <30 à 25>45 à 50
<25≥51
Pression inspiratoire(cmH2O)
≤30 31 à 35 >35
SpO2(%)
94 à 98≥ 94 si la FiO2 ≤ 40%
93 à 85 <85
* Plus de 30 secondes
Desire Study, Wysocki ESICM 2010
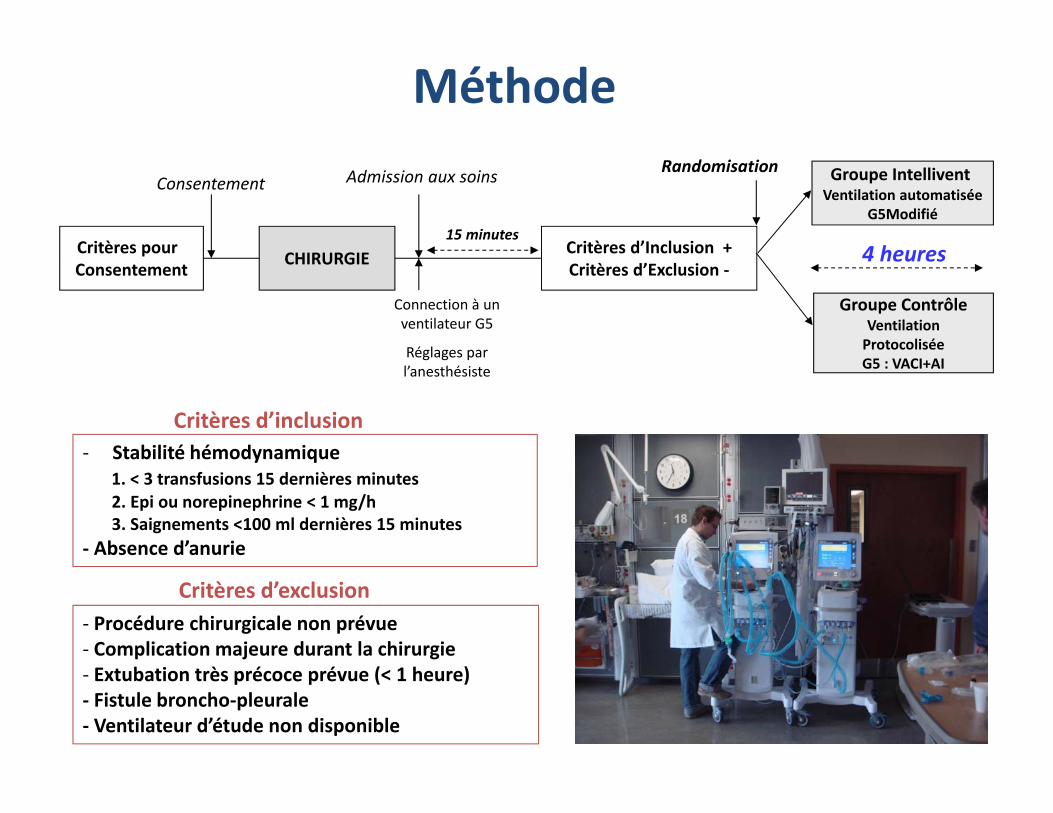
Critères pour Consentement CHIRURGIE Critères d’Inclusion +
Critères d’Exclusion ‐
Consentement Admission aux soins
Connection à un ventilateur G5
Réglages par l’anesthésiste
15 minutes
Groupe IntelliventVentilation automatisée
G5Modifié
Groupe ContrôleVentilationProtocoliséeG5 : VACI+AI
Randomisation
4 heures
‐ Stabilité hémodynamique 1. < 3 transfusions 15 dernières minutes2. Epi ou norepinephrine < 1 mg/h3. Saignements <100 ml dernières 15 minutes
‐ Absence d’anurie
‐ Procédure chirurgicale non prévue‐ Complication majeure durant la chirurgie‐ Extubation très précoce prévue (< 1 heure)‐ Fistule broncho‐pleurale‐ Ventilateur d’étude non disponible
Critères d’inclusion
Critères d’exclusion
Méthode
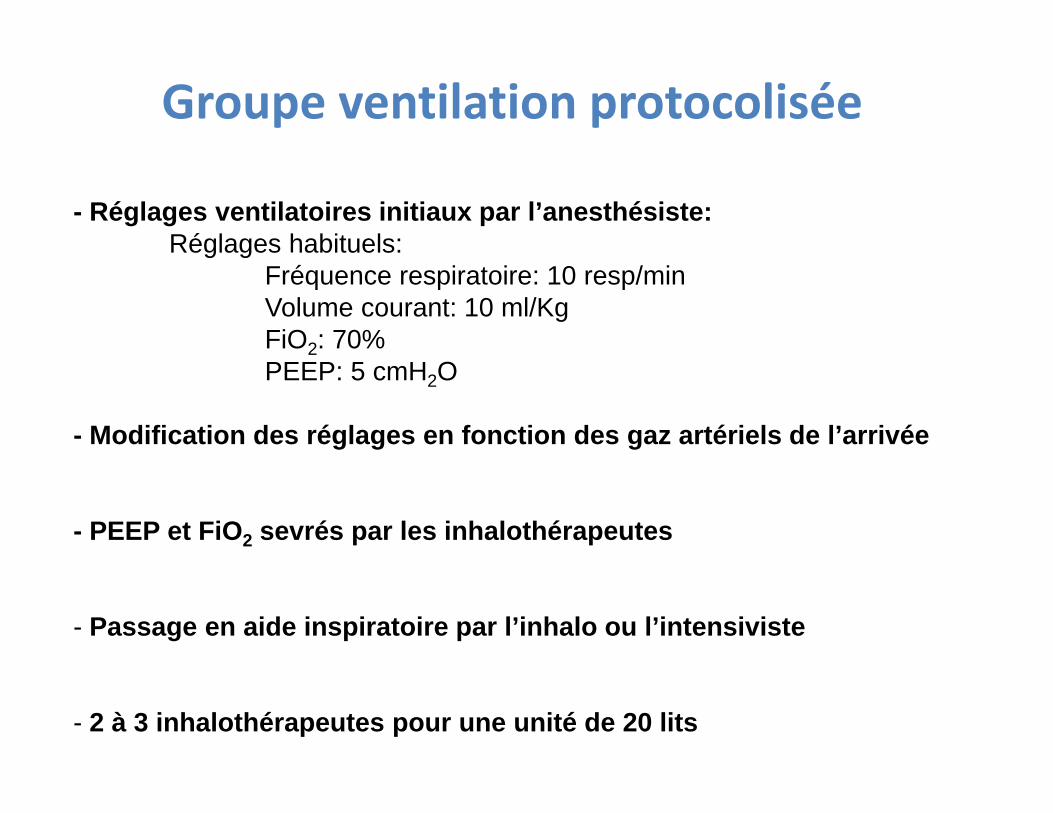
- Réglages ventilatoires initiaux par l’anesthésiste: Réglages habituels:
Fréquence respiratoire: 10 resp/minVolume courant: 10 ml/KgFiO2: 70%PEEP: 5 cmH2O
- Modification des réglages en fonction des gaz artériels de l’arrivée
- PEEP et FiO2 sevrés par les inhalothérapeutes
- Passage en aide inspiratoire par l’inhalo ou l’intensiviste
- 2 à 3 inhalothérapeutes pour une unité de 20 lits
Groupe ventilation protocolisée
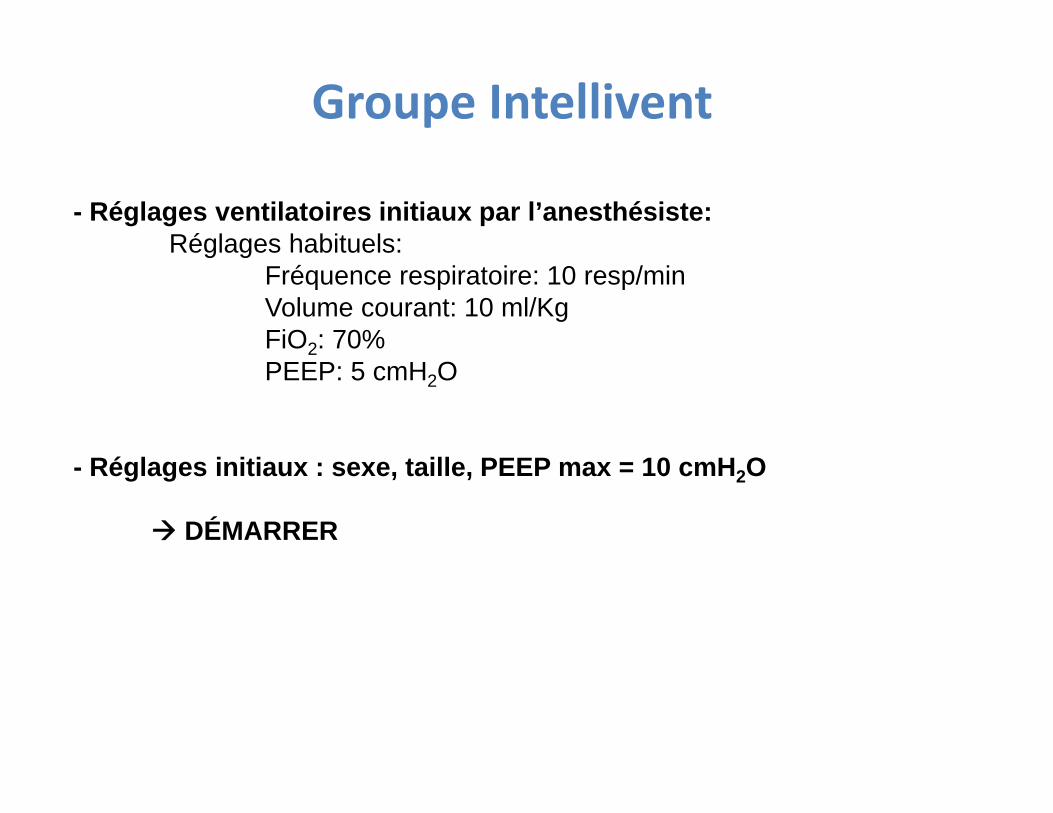
- Réglages ventilatoires initiaux par l’anesthésiste: Réglages habituels:
Fréquence respiratoire: 10 resp/minVolume courant: 10 ml/KgFiO2: 70%PEEP: 5 cmH2O
- Réglages initiaux : sexe, taille, PEEP max = 10 cmH2O
DÉMARRER
Groupe Intellivent
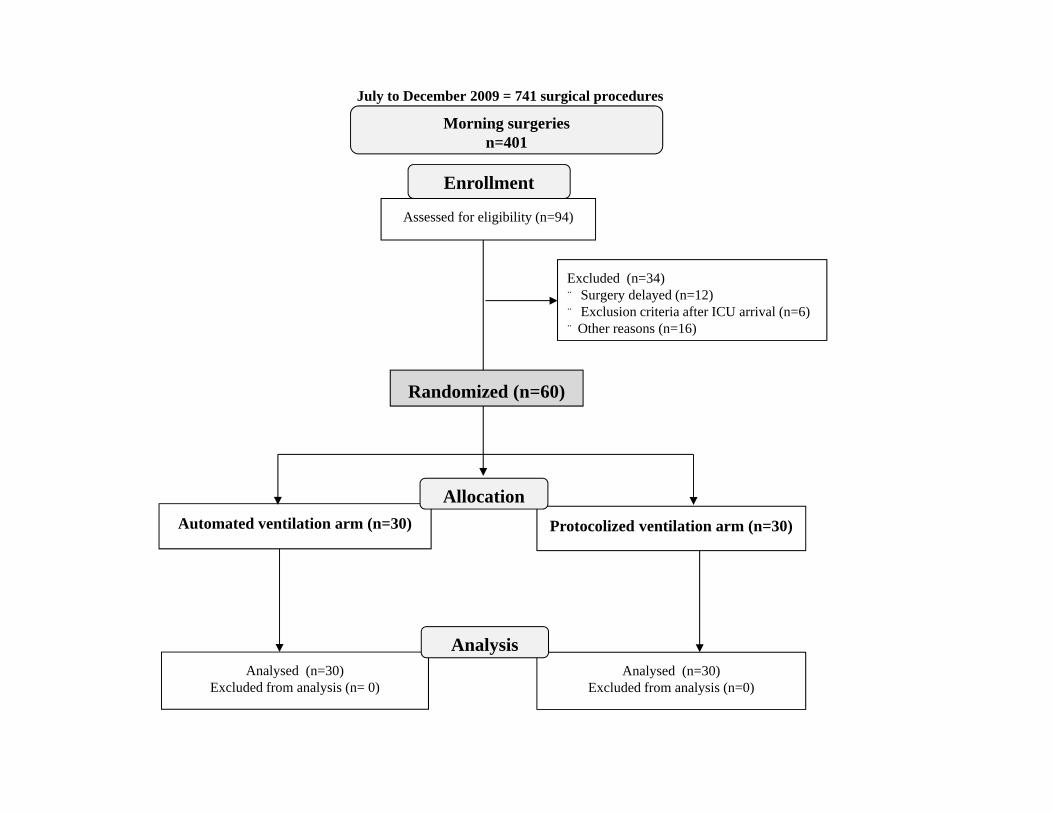
Assessed for eligibility (n=94)
Randomized (n=60)
Enrollment
Analysed (n=30)Excluded from analysis (n=0)
Analysed (n=30)Excluded from analysis (n= 0)
Automated ventilation arm (n=30) Protocolized ventilation arm (n=30)
Allocation
Analysis
Excluded (n=34)¨ Surgery delayed (n=12)¨ Exclusion criteria after ICU arrival (n=6)¨ Other reasons (n=16)
Morning surgeriesn=401
July to December 2009 = 741 surgical procedures
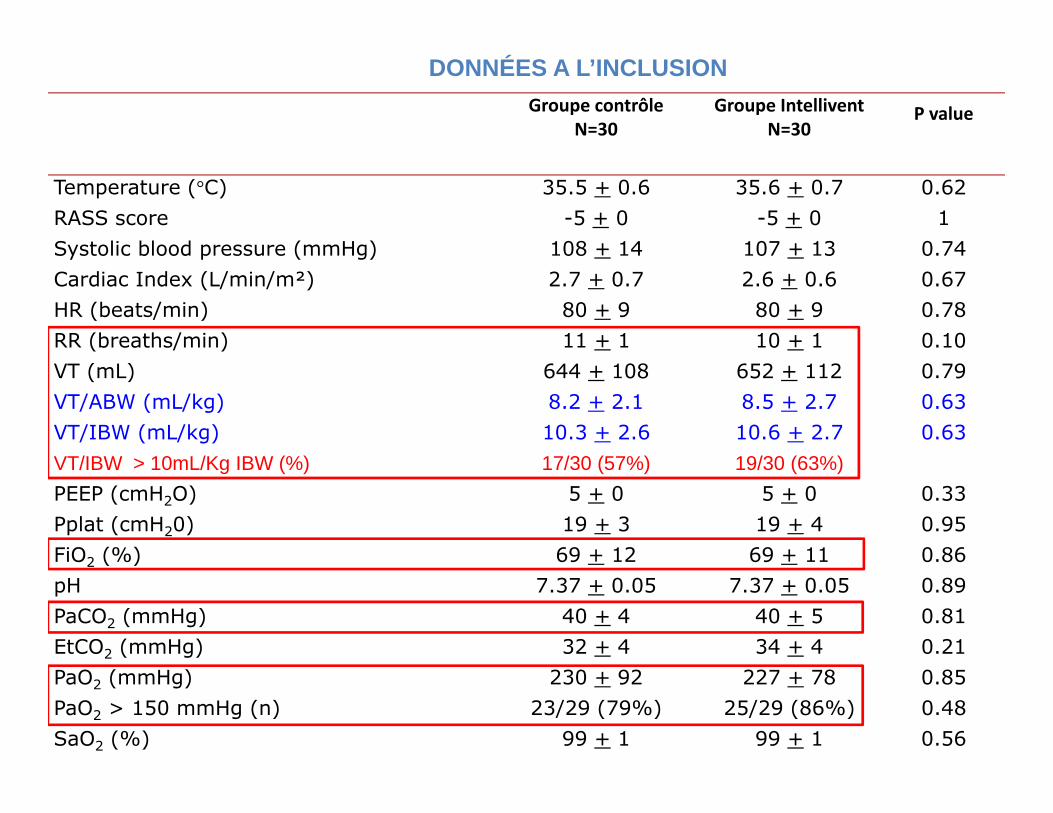
Groupe contrôleN=30
Groupe IntelliventN=30
P value
Temperature (°C) 35.5 + 0.6 35.6 + 0.7 0.62
RASS score -5 + 0 -5 + 0 1
Systolic blood pressure (mmHg) 108 + 14 107 + 13 0.74
Cardiac Index (L/min/m²) 2.7 + 0.7 2.6 + 0.6 0.67
HR (beats/min) 80 + 9 80 + 9 0.78
RR (breaths/min) 11 + 1 10 + 1 0.10
VT (mL) 644 + 108 652 + 112 0.79
VT/ABW (mL/kg) 8.2 + 2.1 8.5 + 2.7 0.63
VT/IBW (mL/kg) 10.3 + 2.6 10.6 + 2.7 0.63
VT/IBW > 10mL/Kg IBW (%) 17/30 (57%) 19/30 (63%)PEEP (cmH2O) 5 + 0 5 + 0 0.33
Pplat (cmH20) 19 + 3 19 + 4 0.95
FiO2 (%) 69 + 12 69 + 11 0.86
pH 7.37 + 0.05 7.37 + 0.05 0.89
PaCO2 (mmHg) 40 + 4 40 + 5 0.81
EtCO2 (mmHg) 32 + 4 34 + 4 0.21
PaO2 (mmHg) 230 + 92 227 + 78 0.85
PaO2 > 150 mmHg (n) 23/29 (79%) 25/29 (86%) 0.48
SaO2 (%) 99 + 1 99 + 1 0.56
DONNÉES A L’INCLUSION
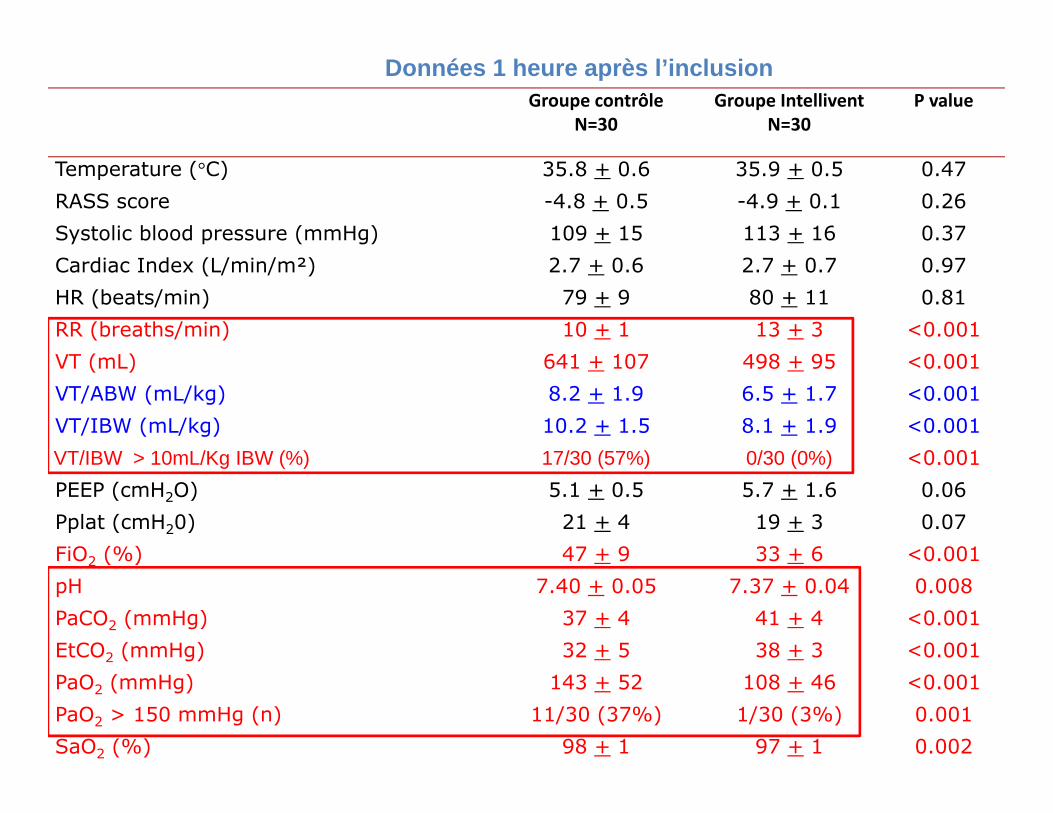
Groupe contrôleN=30
Groupe IntelliventN=30
P value
Temperature (°C) 35.8 + 0.6 35.9 + 0.5 0.47
RASS score -4.8 + 0.5 -4.9 + 0.1 0.26
Systolic blood pressure (mmHg) 109 + 15 113 + 16 0.37
Cardiac Index (L/min/m²) 2.7 + 0.6 2.7 + 0.7 0.97
HR (beats/min) 79 + 9 80 + 11 0.81
RR (breaths/min) 10 + 1 13 + 3 <0.001
VT (mL) 641 + 107 498 + 95 <0.001
VT/ABW (mL/kg) 8.2 + 1.9 6.5 + 1.7 <0.001
VT/IBW (mL/kg) 10.2 + 1.5 8.1 + 1.9 <0.001
VT/IBW > 10mL/Kg IBW (%) 17/30 (57%) 0/30 (0%) <0.001
PEEP (cmH2O) 5.1 + 0.5 5.7 + 1.6 0.06
Pplat (cmH20) 21 + 4 19 + 3 0.07
FiO2 (%) 47 + 9 33 + 6 <0.001
pH 7.40 + 0.05 7.37 + 0.04 0.008
PaCO2 (mmHg) 37 + 4 41 + 4 <0.001
EtCO2 (mmHg) 32 + 5 38 + 3 <0.001
PaO2 (mmHg) 143 + 52 108 + 46 <0.001
PaO2 > 150 mmHg (n) 11/30 (37%) 1/30 (3%) 0.001
SaO2 (%) 98 + 1 97 + 1 0.002
Données 1 heure après l’inclusion
0
10
20
30
40
50
60
70
80
90
100
OPTIMALE ACCEPTABLE NONACCEPTABLE
Groupe Controle
Groupe Intellivent
RÉSULTATS PRINCIPAUX
0
10
20
30
40
50
60
70
80
90
100
OPTIMALE ACCEPTABLE NONACCEPTABLE
Groupe Controle
Groupe Intellivent
%
0
20
40
60
80
100
120
140
160
GroupeControle
GroupeIntellivent
n
Nombre de réglages manuels
148
5
Contrôle
Intellivent
Contrôle Intellivent
Ventilation optimale (Vt < 10ml/Kg de PIT, Paw < 30, SpO2, EtCO2)
**
ZONE DE VENTILATION CHARGE DE TRAVAIL
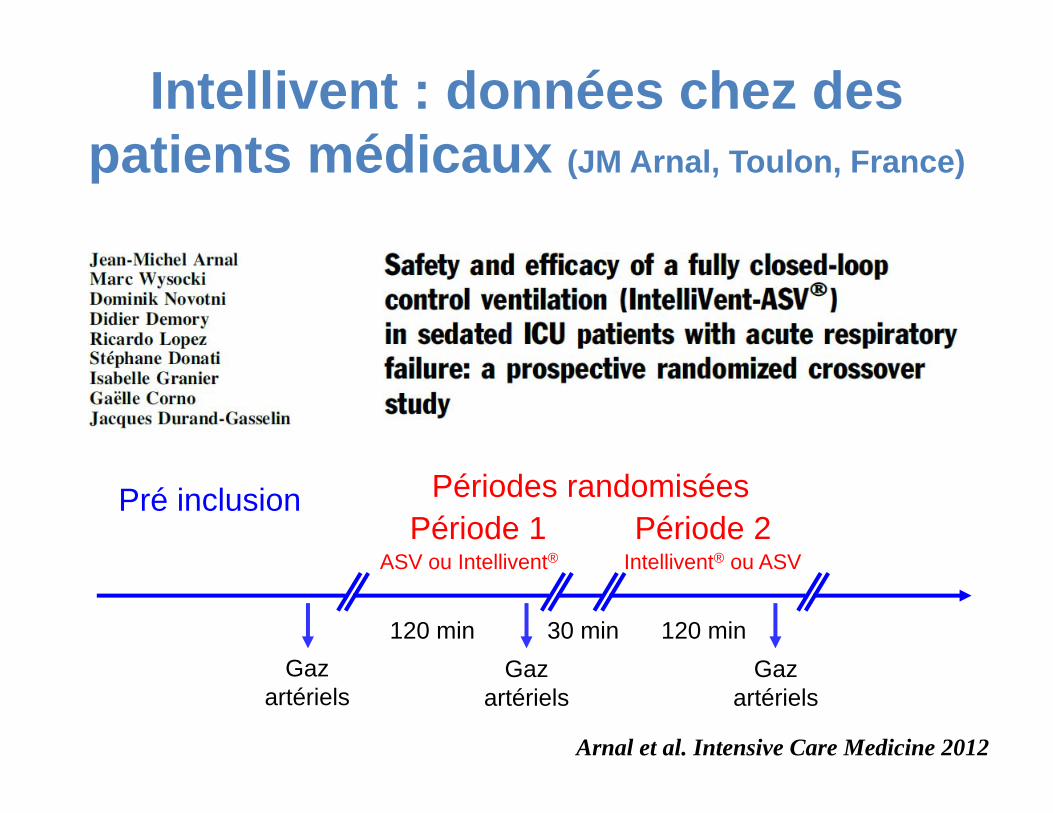
Intellivent : données chez des patients médicaux (JM Arnal, Toulon, France)
Pré inclusion Périodes randomiséesPériode 1 Période 2
ASV ou Intellivent® Intellivent® ou ASV
120 min 30 min 120 minGaz
artériels
Arnal et al. Intensive Care Medicine 2012
Gaz artériels
Gaz artériels
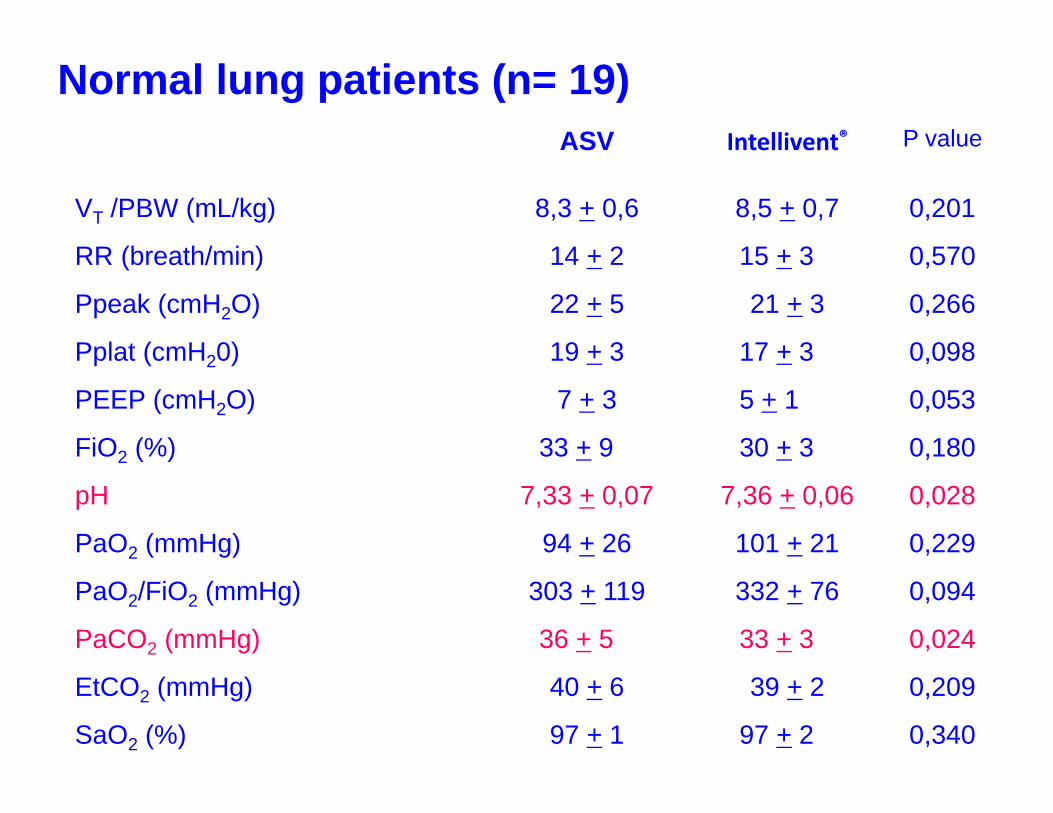
ASV Intellivent® P value
VT /PBW (mL/kg) 8,3 + 0,6 8,5 + 0,7 0,201
RR (breath/min) 14 + 2 15 + 3 0,570
Ppeak (cmH2O) 22 + 5 21 + 3 0,266
Pplat (cmH20) 19 + 3 17 + 3 0,098
PEEP (cmH2O) 7 + 3 5 + 1 0,053
FiO2 (%) 33 + 9 30 + 3 0,180
pH 7,33 + 0,07 7,36 + 0,06 0,028
PaO2 (mmHg) 94 + 26 101 + 21 0,229
PaO2/FiO2 (mmHg) 303 + 119 332 + 76 0,094
PaCO2 (mmHg) 36 + 5 33 + 3 0,024
EtCO2 (mmHg) 40 + 6 39 + 2 0,209
SaO2 (%) 97 + 1 97 + 2 0,340
Normal lung patients (n= 19)
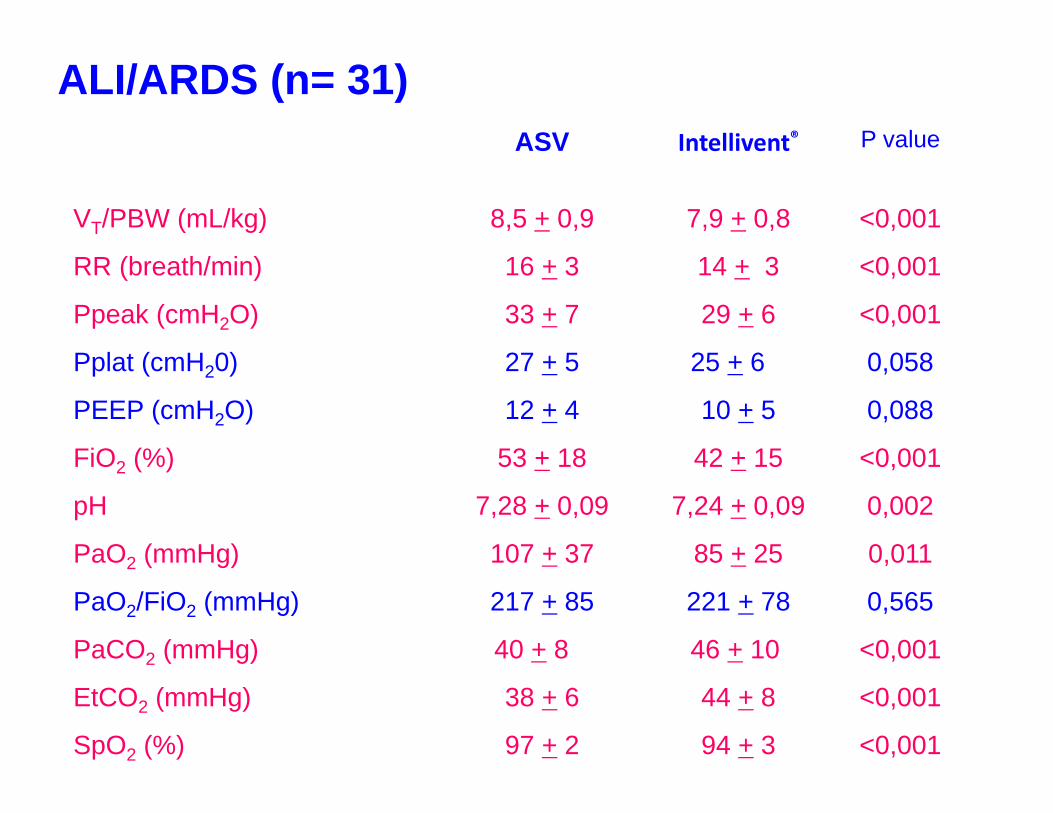
ASV Intellivent® P value
VT/PBW (mL/kg) 8,5 + 0,9 7,9 + 0,8 <0,001
RR (breath/min) 16 + 3 14 + 3 <0,001
Ppeak (cmH2O) 33 + 7 29 + 6 <0,001
Pplat (cmH20) 27 + 5 25 + 6 0,058
PEEP (cmH2O) 12 + 4 10 + 5 0,088
FiO2 (%) 53 + 18 42 + 15 <0,001
pH 7,28 + 0,09 7,24 + 0,09 0,002
PaO2 (mmHg) 107 + 37 85 + 25 0,011
PaO2/FiO2 (mmHg) 217 + 85 221 + 78 0,565
PaCO2 (mmHg) 40 + 8 46 + 10 <0,001
EtCO2 (mmHg) 38 + 6 44 + 8 <0,001
SpO2 (%) 97 + 2 94 + 3 <0,001
ALI/ARDS (n= 31)
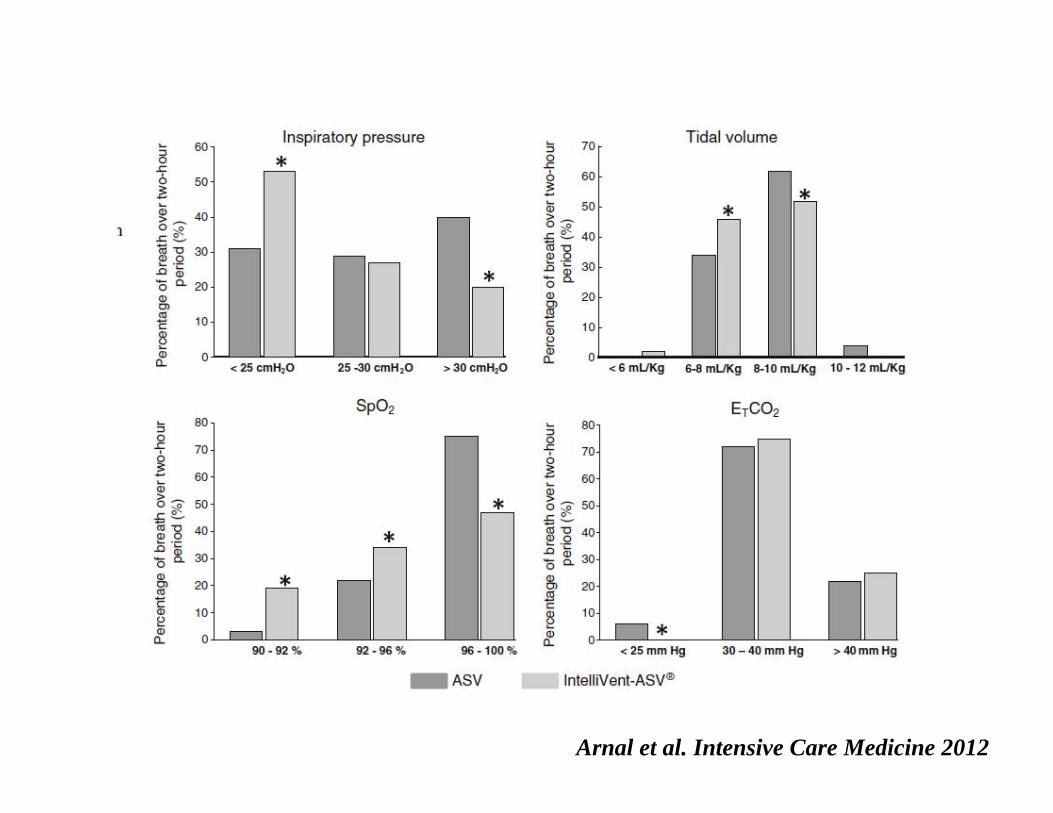
Arnal et al. Intensive Care Medicine 2012
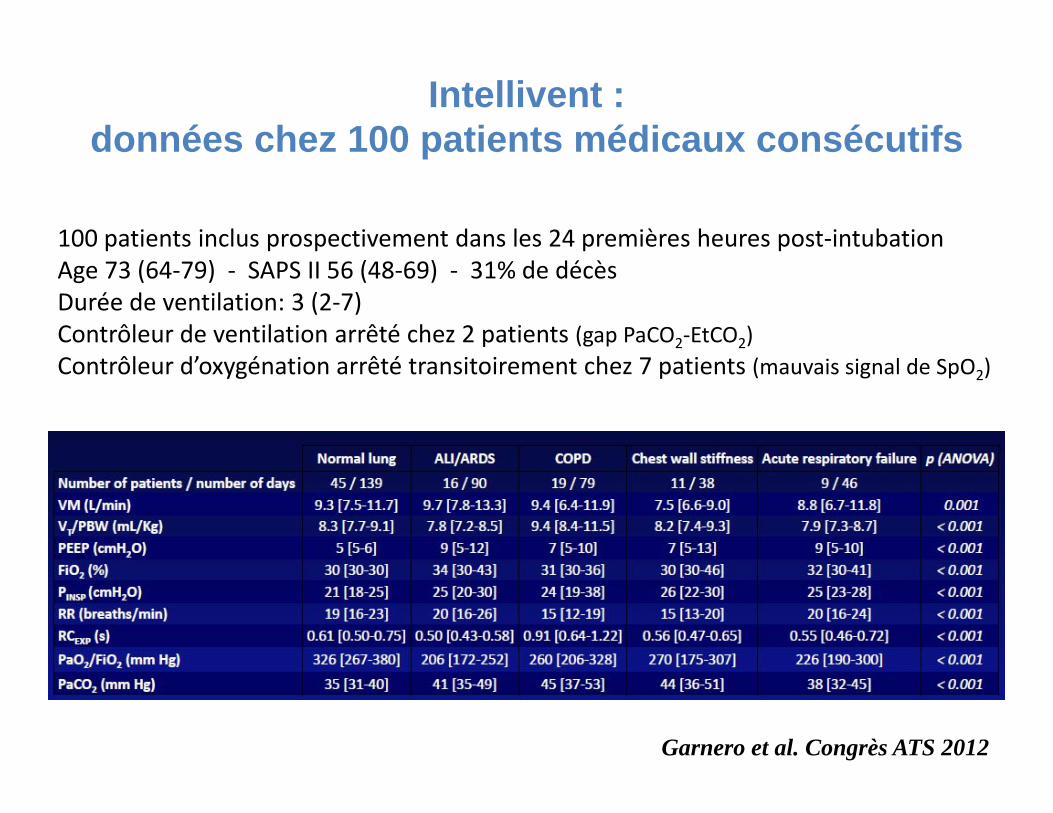
Garnero et al. Congrès ATS 2012
Intellivent : données chez 100 patients médicaux consécutifs
100 patients inclus prospectivement dans les 24 premières heures post‐intubationAge 73 (64‐79) ‐ SAPS II 56 (48‐69) ‐ 31% de décèsDurée de ventilation: 3 (2‐7)Contrôleur de ventilation arrêté chez 2 patients (gap PaCO2‐EtCO2)Contrôleur d’oxygénation arrêté transitoirement chez 7 patients (mauvais signal de SpO2)
LIMITATIONS DE L’INTELLIVENT
EtCO2 gradient augmenté en cas de bas débit
ARDS pas 6 ml/Kg PIT
PAS ASSEZ D’ÉVALUATION CLINIQUE
Conclusions: Automatisation de la ventilation mécanique
=> nombreux avantages
Sevrage automatisé => plusieurs études positives ou « équivalence »
Ventilation totalement automatisée=> premiers résultats encourageants avec une
population spécifique et sur une courte durée=> Données récentes encourageantes dans une
population médicale variée=> Nécessité de réaliser d’autres études
Résultats encourageants avec systèmes de 1ère génération

MERCI !
Related Documents











![[tel-00667286, v1] Asynchronies patient-ventilateur au ...](https://static.cupdf.com/doc/110x72/62af6d3eac61fa74611406a7/tel-00667286-v1-asynchronies-patient-ventilateur-au-.jpg)