Janet Pettit DNP, NNP-BC, VA-BC Janet Pettit DNP, NNP-BC, VA-BC

Evidence-Based Approaches to Elimination of Neonatal CLABSI
Jan 15, 2016
Evidence-Based Approaches to Elimination of Neonatal CLABSI. Janet Pettit DNP, NNP-BC, VA-BC. Disclosures. Argon Medical California Childrens Services NICU HAI Collaborative PDI. Objectives. At the conclusion of the presentation, the participant will be able to: - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Janet Pettit DNP, NNP-BC, VA-BCJanet Pettit DNP, NNP-BC, VA-BC

Argon MedicalCalifornia Childrens Services NICU HAI
CollaborativePDI

At the conclusion of the presentation, the participant will be able to:
Identify common components of insertion bundles used for central lines in neonatesIdentify three controversial components of maintenance bundles used for central lines in neonatesList three care processes with proven efficacy in decreasing CLABSIDistinguish two avenues beyond the insertion and maintenance bundles that have proven success in reducing and sustaining CLABSI reduction efforts





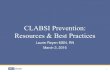
CLABSI RATES CA RNICU COLLABORATIVES- PHASES 1-3: 2006-2011 (2nd QTR)
-1.0
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
J an-06
Apr-0
6
J ul-0
6
Oct-06
J an-07
Apr-0
7
J ul-0
7
Oct-07
J an-08
Apr-0
8
J ul-0
8
Oct-08
J an-09
Apr-0
9
J ul-0
9
Oct-09
J an-10
Apr-1
0
J ul-1
0
Oct-10
J an-11
Apr-1
1
CLA
BSI/
1000
line
day
s
BASELINEN=13
PHASE 1N=13
FOLLOW-UPN=13
PHASE 2N=22
PHASE 3N=14
New CDC Definition
BASELINEN=14


CPQCC HAI Toolkit
NICU Teams




Insertion Maintenance Leadership Diagnosis
Go to website for information about bundlehttp://www.dhcs.ca.gov/ProvGovPart/initiatives/nqi/Pages/default.aspx

Maximum sterile barrier precautionsDisinfect skin with chlorhexidine or povidone
iodineDedicated team for placement & careAll supplies for procedure at bedsideHand hygiene performedInsertion checklist usedStaff empowered to stop non emergent
procedure if sterility breached

BarriersPrevious product labeling restricted use if < 2 months
of age.Updated product labeling January 2012: Use with care
in premature infants or infants under 2 months of age. These products may cause irritation or chemical burns.
Skin reactionsAbsorptionFear of the unknown
FacilitatorsEmerging evidence
Improved CLABSI reductionMinimal reactions
Adjusting use based on gestation & chronologic ageNo toxicity associated with the minimal absorptionRealization that all skin antiseptics problematic
More than half of NICUs in US are using

Should practice extend to all lines?Daily assessment of catheter needReview dressing integrity & cleanlinessUse closed system for infusion, blood sampling & medication administrationAssemble & connect infusion tubing using aseptic or sterile technique. Use consistent tubing configuration

Disinfect injection port with alcohol or chlorhexidine/alcohol for 15 seconds & allow to dry.Use of alcohol port protectors
Hand hygiene performed & clean gloves worn for catheter entry
Use prefilled, flush containing syringesStaff empowered to stop the line in non-
emergent procedure if sterility breached

Can the catheter be removed?
• Daily assessment & documentation of catheter need – Joint Commission NPSG.07.04.01 & CA requirement
• Plan for removal• Key times for removal to lessen risk

PRN change recommendedRoutine change intervals
Remove blood & drainage
Not intactUse sterile technique
Dressing typeTransparent vs. gauzeTransparent: allows direct
visualization and requires fewer changes, but no other demonstrated clinical advantage.
20

Definition of “closed”Infusion, blood
withdrawal, med administration
Close all or only central catheters

Entry point to catheter kept out of bed
Needleless connector capped with syringe at all times
System changed along with other infusion tubing
Part of Aly, 2005 bundle & adopted by many NICUs
22

Bundle componentAly 2005 & othersLack of standardization
Sterile vs aseptic techniqueResource availability
1-2 personnelSet-up carts/stationsConsistent tubing
configurationsProcedural checklist
Frequency of change

Ryder et al. Microscopic Evaluation of Microbial Colonization on Needleless Connectors. 2009. APIC Poster Presentation

Alcohol
CHG/alcohol
31% don’t
clean!


Increase contamination of vials & ampules when prepared in ward vs pharmacy Van Grafhorst Critical Care Med 2002.
Syringe contamination
Nurse filled vs. prefilled
27

The Line


Administrative involvement & support for zero HAIsEngage staff with feedback
Posting days since last CLABSIPosting rates of CLABSI
Perform investigation of each CLABSI/BSISurveillance activities for critical processes
Hand hygieneLine management and entryOff unit proceduresStop the line support
Trained personnel to perform specialized maintenance activities

Helps to ensure quality of care Means to monitor compliance
with policy Multidepartmental personnel
monitor adherence to policy Unit-based Hospital-based
Correct problem behavior while its occurring
Reward proper behavior





Developed by CCS CLABSI Prevention Collaborative

Developed by CCS CLABSI Prevention Collaborative



NHSN criteriaCulturing techniques

Feeding tubes & practices
# Line entries
Respiratory care practices
Skin assessment & # punctures

The way in which Each individual pays attention to and performs their job
PLUS
The way All individuals inter-relate, interact, and communicate while working, ultimately determines the sustainability of high quality, safe health care.


Questions: [email protected]

Chaiyakunapruk, N., Veenstra, D. L., Lipsky, B. A., & Saint, S. (2002). Chlorhexidine compared with povidone-iodine solution for vascular catheter-site care: a meta-analysis. Ann Intern Med, 136(11), 792-801. doi: 200206040-00007 [pii]
Curry, S., Honeycutt, M., Goins, G., & Gilliam, C. (2009). Catheter-associated bloodstream infections in the NICU: getting to zero. Neonatal network : NN, 28(3), 151-155.
Marschall J., Mermel, L. A., Classen, D., Arias, K. M., Podgorny, K., & Yokoe, D. S. (2008). Strategies to prevent central line associated bloodstream infections in acute care hospitals. Infection Control and Hospital Epidemiology, 29, S22-30.
Mullany, L., Darmstadt, G. L., & TielschJ. M. (2006). Safety and impact of chlorhexidine antisepsis interventions for improving neonatal health in developing countries. Pediatric Infectious Disease Journal, 25, 665-675.
O'Grady, N. P., Alexander, M., Burns, L. A., Dellinger, E. P., Garland, J., Heard, S. O., . . . (HICPAC)., H. I. C. P. A. C. (2011). 2011 Guidelines for the Prevention of Intravascular Catheter-Related Infections 1-83. Retrieved from Centers for Disease Control and Prevention website: http://www.cdc.gov/hicpac/bsi/bsi-guidelines-2011.html
Payne, N. R., Carpenter, J. H., Badger, G. J., Horbar, J. D., & Rogowski, J. (2004). Marginal increase in cost and excess length of stay associated with nosocomial bloodstream infections in surviving very low birth weight infants. Pediatrics, 114, 348-355.

Pettit, J. & Wyckoff, M. M. (2007). Peripherally inserted central catheter: Guidelines for practice. Glenview, IL: The National Association of Neonatal Nurses.
Powers, R. J., & Wirtschafter, D. W. (2010). Decreasing central line associated bloodstream infection in neonatal intensive care. Clinics in perinatology, 37(1), 247-272. doi: 10.1016/j.clp.2010.01.014
Suresh, G. K., & Edwards, W. H. (2012). Central line-associated bloodstream infections in neonatal intensive care: changing the mental model from inevitability to preventability. American journal of perinatology, 29(1), 57-64. doi: 10.1055/s-0031-1286182
Wirtschafter, D. D., Pettit, J., Kurtin, P., Dalsey, M., Chance, K., Morrow, H. W., . . . Kloman, S. (2010). A statewide quality improvement collaborative to reduce neonatal central line-associated blood stream infections. [Multicenter Study]. Journal of perinatology : official journal of the California Perinatal Association, 30(3), 170-181. doi: 10.1038/jp.2009.172
Zingg, W., Imhof, A., Maggiorini, M., Stocker, R., Keller, E., & Ruef, C. (2009). Impact of a prevention strategy targeting hand hygiene and catheter care on the incidence of catheter-related bloodstream infections. Critical care medicine, 37(7), 2167-2173; quiz 2180. doi: 10.1097/CCM.0b013e3181a02d8f
Related Documents