Everolimus-eluting stent versus bare-metal stent in elderly (≥ 75 years) versus non-elderly (b 75 years) patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention: Insights from the examination trial ☆ , ☆☆ Alfonso Ielasi a,1 , Salvatore Brugaletta b,1 , Antonio Silvestro a , Angel Cequier c,d , Andrés Iñiguez e , Antonio Serra f , Rosana Hernandez-Antolin g , Vicente Mainar h , Marco Valgimigli i , Pieter den Heijer j , Armando Bethencourt k , Nicolás Vazquez l , Patrick Serruys m , Manel Sabate b,2 , Maurizio Tespili a, ⁎ ,2 a Hospital “Bolognini” Seriate, Bergamo, Italy b University Hospital Clinic, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain c Heart Institute, University Hospital of Bellvitge, Barcelona, Spain d University Hospital of Bellvitge (IDIBELL), Barcelona, Spain e Hospital do Meixoeiro, Vigo, Spain f University Hospital of Sant Pau, Barcelona, Spain g University Hospital San Carlos, Madrid, Spain h Hospital General of Alicante, Alicante, Spain i University Hospital Ferrara, Ferrara, Italy j Amphia Ziekenhuis, Breda, The Netherlands k Hospital Son Dureta, Palma de Mallorca, Spain l Hospital Juan Canalejo, A Coruña, Spain m Erasmus Medical Center, Rotterdam, The Netherlands abstract article info Article history: Received 15 May 2014 Received in revised form 14 August 2014 Accepted 18 October 2014 Available online 22 October 2014 Keywords: Myocardial infarction Elderly Drug-eluting stent Outcome Background: The elderly (≥75 years) constitute a high-risk subset of patients who continue to have a poorer prognosis than non-elderly (b 75 years). Whether the effects of everolimus-eluting stent (EES) in ST-segment el- evation myocardial infarction (STEMI) are independent of age has not been reported. We investigated the out- comes following primary PCI (PPCI) with bare-metal stent (BMS) or EES in elderly vs. non-elderly STEMI patients. Methods: The EXAMINATION trial randomized 1498 STEMI patients to BMS or EES. The primary patient-oriented endpoint (POCE) was the combined of all-cause death, any-recurrent myocardial infarction (MI) and any- revascularization at 1-year. The secondary endpoint included the device-oriented combined (DOCE) of cardiac death, target-vessel MI and target-lesion revascularization. These endpoints and their components were com- pared between elderly and non-elderly. Results: Among patients enrolled in the trial, 245 (16.3%) were elderly, allocated to BMS (n = 132) or EES (n = 113), while the remaining 1253 (83.7%) were non-elderly, allocated to BMS (n = 615) or EES (n = 638). At 1-year, both the POCE and DOCE were observed more frequently in elderly vs. non-elderly group (24.5% vs. 10.5%, p b 0.001 and 15.9% vs. 5.1%, p b 0.001). Whereas in non-elderly, both POCE and DOCE were lower in EES vs. BMS (12.4% vs. 8.8%, p = 0.03 and 6.7% vs. 3.6%, p = 0.01), no differences were found in elderly, with a tendency for interaction between age and stent type for POCE (p = 0.05). On multivariate analysis age ≥75 years was an in- dependent predictor of POCE (HR 2.19 [95%CI 1.59–3.01], p b 0.0001) and DOCE (HR 2.42 [95%CI 1.60–3.7], p b 0.001) at 1-year. Conclusions: In STEMI patients undergoing PPCI, advanced age (≥75 years) is associated with worse outcomes. The beneficial effects of EES over BMS tended to be age-dependent. © 2014 Elsevier Ireland Ltd. All rights reserved. International Journal of Cardiology 179 (2015) 73–78 ☆ All the authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. ☆☆ There are no potential conflicts of interest or funding sources to disclose. ⁎ Corresponding author at: Division of Cardiology “Bolognini” Hospital, Via Paderno 21, 24068 Seriate (BG), Italy. E-mail address: [email protected] (M. Tespili). 1 Drs Ielasi and Brugaletta equally contributed to the manuscript and are co-first authors. 2 Drs Tespili and Sabatè shared the senior authorship. http://dx.doi.org/10.1016/j.ijcard.2014.10.038 0167-5273/© 2014 Elsevier Ireland Ltd. All rights reserved. Contents lists available at ScienceDirect International Journal of Cardiology journal homepage: www.elsevier.com/locate/ijcard

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

International Journal of Cardiology 179 (2015) 73–78
Contents lists available at ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
Everolimus-eluting stent versus bare-metal stent in elderly (≥75 years)versus non-elderly (b75 years) patients with ST-elevation myocardialinfarction undergoing primary percutaneous coronary intervention:Insights from the examination trial☆,☆☆
Alfonso Ielasi a,1, Salvatore Brugaletta b,1, Antonio Silvestro a, Angel Cequier c,d, Andrés Iñiguez e, Antonio Serra f,Rosana Hernandez-Antolin g, Vicente Mainar h, Marco Valgimigli i, Pieter den Heijer j, Armando Bethencourt k,Nicolás Vazquez l, Patrick Serruys m, Manel Sabate b,2, Maurizio Tespili a,⁎,2
a Hospital “Bolognini” Seriate, Bergamo, Italyb University Hospital Clinic, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spainc Heart Institute, University Hospital of Bellvitge, Barcelona, Spaind University Hospital of Bellvitge (IDIBELL), Barcelona, Spaine Hospital do Meixoeiro, Vigo, Spainf University Hospital of Sant Pau, Barcelona, Spaing University Hospital San Carlos, Madrid, Spainh Hospital General of Alicante, Alicante, Spaini University Hospital Ferrara, Ferrara, Italyj Amphia Ziekenhuis, Breda, The Netherlandsk Hospital Son Dureta, Palma de Mallorca, Spainl Hospital Juan Canalejo, A Coruña, Spainm Erasmus Medical Center, Rotterdam, The Netherlands
☆ All the authors take responsibility for all aspects of t☆☆ There are no potential conflicts of interest or funding
⁎ Corresponding author at: Division of Cardiology “BoE-mail address: [email protected] (M. Tespili).
1 Drs Ielasi and Brugaletta equally contributed to the m2 Drs Tespili and Sabatè shared the senior authorship.
http://dx.doi.org/10.1016/j.ijcard.2014.10.0380167-5273/© 2014 Elsevier Ireland Ltd. All rights reserved
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 15 May 2014Received in revised form 14 August 2014Accepted 18 October 2014Available online 22 October 2014Keywords:Myocardial infarctionElderlyDrug-eluting stentOutcome
Background: The elderly (≥75 years) constitute a high-risk subset of patients who continue to have a poorerprognosis than non-elderly (b75 years).Whether the effects of everolimus-eluting stent (EES) in ST-segment el-evation myocardial infarction (STEMI) are independent of age has not been reported. We investigated the out-comes following primary PCI (PPCI)with bare-metal stent (BMS) or EES in elderly vs. non-elderly STEMI patients.Methods: The EXAMINATION trial randomized 1498 STEMI patients to BMS or EES. The primary patient-orientedendpoint (POCE) was the combined of all-cause death, any-recurrent myocardial infarction (MI) and any-revascularization at 1-year. The secondary endpoint included the device-oriented combined (DOCE) of cardiacdeath, target-vessel MI and target-lesion revascularization. These endpoints and their components were com-pared between elderly and non-elderly.Results: Among patients enrolled in the trial, 245 (16.3%) were elderly, allocated to BMS (n = 132) or EES
(n = 113), while the remaining 1253 (83.7%) were non-elderly, allocated to BMS (n = 615) or EES (n = 638).At 1-year, both the POCE and DOCE were observed more frequently in elderly vs. non-elderly group (24.5% vs.10.5%, p b 0.001 and 15.9% vs. 5.1%, p b 0.001). Whereas in non-elderly, both POCE and DOCE were lower in EESvs. BMS (12.4% vs. 8.8%, p=0.03 and 6.7% vs. 3.6%, p= 0.01), no differenceswere found in elderly, with a tendencyfor interaction between age and stent type for POCE (p= 0.05). Onmultivariate analysis age≥75 years was an in-dependent predictor of POCE (HR 2.19 [95%CI 1.59–3.01], p b 0.0001) and DOCE (HR 2.42 [95%CI 1.60–3.7],p b 0.001) at 1-year.Conclusions: In STEMI patients undergoing PPCI, advanced age (≥75 years) is associated with worse outcomes. Thebeneficial effects of EES over BMS tended to be age-dependent.© 2014 Elsevier Ireland Ltd. All rights reserved.
he reliability and freedom from bias of the data presented and their discussed interpretation.sources to disclose.
lognini” Hospital, Via Paderno 21, 24068 Seriate (BG), Italy.
anuscript and are co-first authors.
.

74 A. Ielasi et al. / International Journal of Cardiology 179 (2015) 73–78
1. Introduction
Primary percutaneous coronary intervention (PPCI) represents thetherapy of choice in the setting of ST-segment elevation myocardial in-farction (STEMI) when it can be performed in a timely fashion by an ex-perienced team [1,2]. The refinement of interventional techniques andthe optimization of anti-platelet and antithrombotic therapy have sig-nificantly improved the outcomes of patients with STEMI [3–6].
Of note is that due to the aging of population in the developed coun-tries, the incidence of acute myocardial infarction has increased in elder-ly patients [7]. Despite improvements in outcomes of STEMI patients,elderly who have undergone PPCI have still a poorer prognosis thanyoung patients [8–10]. Suboptimal myocardial perfusion has been re-cently shown to contribute to poor outcome as well as the presence ofco-morbidities, more severe coronary artery disease (CAD), higher rateof access site complications,major bleeding and impaired left ventricularfunction [8–12].
Two recentmeta-analyses of STEMI patients treated by PPCI showedthat the implantation of a second generation cobalt–chromium (Co–Cr)everolimus eluting stent (EES) was associated with a substantial de-crease in the risk of target lesion revascularization (TLR) with no in-crease in very late stent-thrombosis (ST), compared with first-generation DES (sirolimus-eluting stent [SES], paclitaxel-eluting [PES])and bare-metal stent (BMS) [13,14]. No data are actually availableconcerning the safety and effectiveness of Co–Cr EES implantation inelderly STEMI patients.
The aim of the present analysis was therefore to assess the out-comes of second generation Co–Cr EES vs. Co–Cr BMS in elderly(≥75 years) vs. non-elderly (b75 years) STEMI patients enrolled inthe EXAMINATION (Evaluation of the Xience-V stent in Acute Myocar-dial INfArcTION) trial [15].
2. Methods
This is a post-hoc analysis study from the all-comer, multicentre, controlled, andrandomized, EXAMINATION trial (Evaluation of the Xience-V stent in Acute MyocardialINfArcTION) (NCT00828087). The EXAMINATION trial randomized 1:1 a total of 1498 pa-tientswith STEMI undergoing PPCI to EES (n=751) (Xience; Abbott Vascular, Santa Clara,CA) or Multilink Vision BMS (n = 747) (Abbott Vascular, Santa Clara, CA). The results ofthe EXAMINATION trial have been previously reported [16]. All participating centers sub-mitted and received the approval of their Medical Ethics Committee for the protocol andfor the informed consent. The study was conducted in compliance with the protocol, theDeclaration of Helsinki, BS EN ISO 14155 Part 1 and Part 2, and applicable local require-ments. All patients provided written informed consent. The EXAMINATION trial hasbeen funded by the Spanish Heart Foundation.
All STEMI patients within the first 48 h after the onset of symptoms who underwentPPCI were eligible for the study. Exclusion criteria were: age less than 18 years; pregnan-cy; patients with known intolerance to aspirin, clopidogrel, heparin, stainless steel, evero-limus or contrast material; patients on chronic treatment with anti-vitamin K agents; andSTEMI secondary to ST. The only anatomic exclusion criterion was the vessel size largerthan 4.0 mm or smaller than 2.25 mm. Importantly, there was no upper age limit for pa-tients inclusion [15]. For this sub-analysis, the cut-off of 75 years was chosen to identifyelderly patients, according to previous reports [17–20].
The primary endpoint of the study was the patient-oriented combined endpoint(POCE) of all-cause death, any recurrent MI and any repeat revascularization at 1 year[15]. Secondary endpoints of the study, analyzed at 1-year, included the device-orientedcombined endpoint (DOCE) of cardiac death, target-vessel myocardial infarction (TV-MI)and TLR, all cause and cardiac death; recurrentMI (WorldHealthOrganization extended def-inition); TLR; target vessel revascularization (TVR); ST (according to the Academic ResearchConsortium definitions); device and procedural success; major andminor bleeding [15]. De-tailed definitions of the endpoints have been reported elsewhere [15]. All clinical eventswereadjudicated by an independent Clinical Event Committee (Cardialysis, Rotterdam, TheNetherlands). Clinical, angiographic, procedural characteristics and 1-year outcomes wereanalyzed stratified by age (b75 vs. ≥75 years old) and stent type.
2.1. Statistical analysis
Categorical variables were expressed as number and percentage and were comparedby chi-square analysis or Fisher exact test, as appropriate. Continuous variables wereexpressed as mean ± standard deviation or median and interquartile range and werecompared by the t-test or Wilcoxon rank sum test, as appropriate.
Event analyses were displayed using Kaplan–Meier plots, and were compared withthe log-rank test. Power calculation showed that primary endpoint comparison was
80% powered to demonstrate any difference between the groups either in elderly(≥75 years) or in non-elderly (b75 years). Multivariable predictors of 1-year outcomeswere determined using Cox proportional hazards regression. A univariate analysis wasperformed in order to select the variables to be entered in the multivariate model withan entry of 0.1. The following variables were tested in the univariate analysis: age(≥75 years), arm of treatment, baseline Killip class, clinical condition, sex, diabetesmellitus, hypercholesterolemia, hypertension, TIMI flow pre-PCI, use of thrombectomydevice, use of IIb/IIIa inhibitors, ejection fraction, direct stenting, number of stents im-planted, body mass index, use of unfractionated heparin, bivalirudin, dual antiplatelettherapy (DAPT), stent diameter and length. The interaction between age and stent typewas tested in the proportional hazards model for the patient, device-oriented endpoints,all-cause and cardiac death, bleeding.
A two-tailed p-value b0.05was considered statistically significant. Statistical analyseswere performed with SPSS statistical package, version 20.0 (SPSS Inc., Chicago IL, USA).
3. Results
3.1. Baseline clinical characteristics
Among the 1498 patients enrolled in the trial, 245 (16.3%) patientswere classified as elderly (≥75 years-old) and were allocated to BMS(n = 132; 53.8%) or EES (n = 113; 46.1%). The remaining 1253 (83.7%)patientswere classified as non-elderly (b75 year-old) andwere allocatedto BMS (n= 615; 49.1%) or EES (n= 638; 50.9%). Baseline clinical char-acteristics of all patients according to age (b75 vs. ≥75 years) and stenttype (EES vs. BMS) are shown in Table 1. Overall, elderly patients weremore frequently female (35.1% vs. 13.4%, p b 0.001), with a lower bodymass index (26.43 ± 3.81 kg/m2 vs. 27.52 ± 3.81 kg/m2, p b 0.001) andejection fraction (47.85 ± 11.34% vs. 51.69 ± 10.17%, p b 0.001) ascompared to non-elderly. Furthermore, they had higher prevalence ofdiabetes (24.5% vs. 15.8%, p b 0.001), hypertension (67.3% vs. 44.7%,p b 0.001), prior stroke (4.9% vs. 1.5%, p = 0.001) and higher KillipClass at presentation (p b 0.001) than non-elderly patients.
3.2. Angiographic and procedural characteristics
Baseline angiographic and procedural characteristics of all patientsaccording to age (b75 vs. ≥75 years) and stent type (EES vs. BMS) areshown in Table 2.
Elderly patients received less frequently IIb/IIIa inhibitor (37.6% vs.55.3%, p b 0.001), thrombus-aspiration (58.4% vs. 66.5%, p = 0.015)and direct stenting (42.1% vs. 63.8%, p b 0.001) as compared to non-elderly. In addition they required a higher number of stent (1.48 ±0.72 vs. 1.37 ± 0.63, p = 0.011), generally smaller (3.12 ± 0.42 mmvs. 3.22 ± 0.46 mm, p = 0.003), longer (29.42 ± 15.21 mm vs.27.14 ± 13.73 mm, p = 0.02) and overlapped (32.7% vs. 25.9%,p = 0.02) as compared to non-elderly. Eventually, they showed moreoften impaired post-procedural TIMI flow (p = 0.02) and lack of ST-segment resolution (p = 0.04) compared to non-elderly group.
3.3. Clinical outcomes
At 1-year, 1090 (91.8%) non-elderly and 176 (76.9%) elderly patientswere on DAPT (p b 0.001).
One-year clinical outcomes are shown in Table 3. Overall, both thePOCE and the DOCE resulted significantly higher in elderly (24.5% vs.10.5%, p b 0.001 and 15.9% vs. 5.1%, p b 0.001, respectively) as comparedto non-elderly group. Overall, elderly patients had a higher incidence ofall cause (13.9% vs. 1.4%, p b 0.001) and cardiac death (12.7% vs. 1.1%,p b 0.001) compared to non-elderly. No significant differences wereobserved between the groups in terms of TV-MI (p = 0.51), TLR(p = 0.52), TVR (p = 0.59) and definite/probable ST (p = 0.52)while overall bleedings were more frequent in elderly vs. non-elderly(7.3% vs. 4.0%, p = 0.02).
Whereas in non-elderly patients both the POCE and the DOCE wereobserved more frequently in the BMS vs. the EES group (12.4% vs. 8.8%,p = 0.03 and 6.7% vs. 3.6%, p = 0.01, respectively), no significant
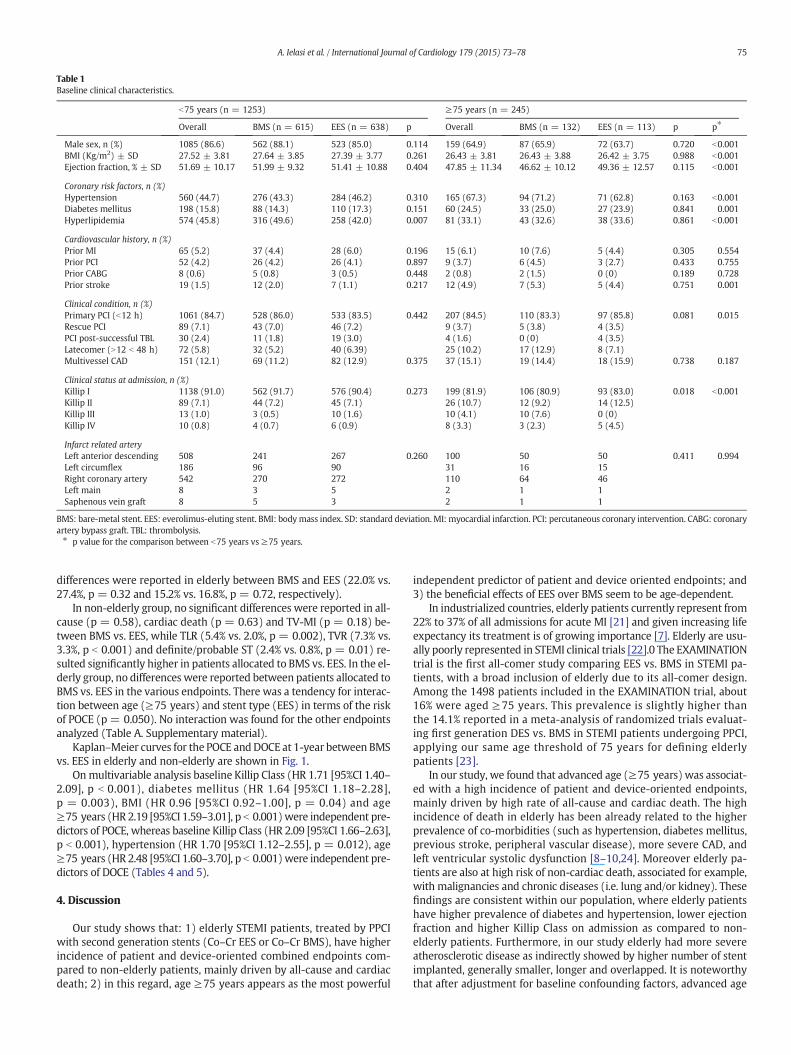
Table 1Baseline clinical characteristics.
b75 years (n = 1253) ≥75 years (n = 245)
Overall BMS (n = 615) EES (n = 638) p Overall BMS (n = 132) EES (n = 113) p p⁎
Male sex, n (%) 1085 (86.6) 562 (88.1) 523 (85.0) 0.114 159 (64.9) 87 (65.9) 72 (63.7) 0.720 b0.001BMI (Kg/m2) ± SD 27.52 ± 3.81 27.64 ± 3.85 27.39 ± 3.77 0.261 26.43 ± 3.81 26.43 ± 3.88 26.42 ± 3.75 0.988 b0.001Ejection fraction, % ± SD 51.69 ± 10.17 51.99 ± 9.32 51.41 ± 10.88 0.404 47.85 ± 11.34 46.62 ± 10.12 49.36 ± 12.57 0.115 b0.001
Coronary risk factors, n (%)Hypertension 560 (44.7) 276 (43.3) 284 (46.2) 0.310 165 (67.3) 94 (71.2) 71 (62.8) 0.163 b0.001Diabetes mellitus 198 (15.8) 88 (14.3) 110 (17.3) 0.151 60 (24.5) 33 (25.0) 27 (23.9) 0.841 0.001Hyperlipidemia 574 (45.8) 316 (49.6) 258 (42.0) 0.007 81 (33.1) 43 (32.6) 38 (33.6) 0.861 b0.001
Cardiovascular history, n (%)Prior MI 65 (5.2) 37 (4.4) 28 (6.0) 0.196 15 (6.1) 10 (7.6) 5 (4.4) 0.305 0.554Prior PCI 52 (4.2) 26 (4.2) 26 (4.1) 0.897 9 (3.7) 6 (4.5) 3 (2.7) 0.433 0.755Prior CABG 8 (0.6) 5 (0.8) 3 (0.5) 0.448 2 (0.8) 2 (1.5) 0 (0) 0.189 0.728Prior stroke 19 (1.5) 12 (2.0) 7 (1.1) 0.217 12 (4.9) 7 (5.3) 5 (4.4) 0.751 0.001
Clinical condition, n (%)Primary PCI (b12 h) 1061 (84.7) 528 (86.0) 533 (83.5) 0.442 207 (84.5) 110 (83.3) 97 (85.8) 0.081 0.015Rescue PCI 89 (7.1) 43 (7.0) 46 (7.2) 9 (3.7) 5 (3.8) 4 (3.5)PCI post-successful TBL 30 (2.4) 11 (1.8) 19 (3.0) 4 (1.6) 0 (0) 4 (3.5)Latecomer (N12 b 48 h) 72 (5.8) 32 (5.2) 40 (6.39) 25 (10.2) 17 (12.9) 8 (7.1)Multivessel CAD 151 (12.1) 69 (11.2) 82 (12.9) 0.375 37 (15.1) 19 (14.4) 18 (15.9) 0.738 0.187
Clinical status at admission, n (%)Killip I 1138 (91.0) 562 (91.7) 576 (90.4) 0.273 199 (81.9) 106 (80.9) 93 (83.0) 0.018 b0.001Killip II 89 (7.1) 44 (7.2) 45 (7.1) 26 (10.7) 12 (9.2) 14 (12.5)Killip III 13 (1.0) 3 (0.5) 10 (1.6) 10 (4.1) 10 (7.6) 0 (0)Killip IV 10 (0.8) 4 (0.7) 6 (0.9) 8 (3.3) 3 (2.3) 5 (4.5)
Infarct related arteryLeft anterior descending 508 241 267 0.260 100 50 50 0.411 0.994Left circumflex 186 96 90 31 16 15Right coronary artery 542 270 272 110 64 46Left main 8 3 5 2 1 1Saphenous vein graft 8 5 3 2 1 1
BMS: bare-metal stent. EES: everolimus-eluting stent. BMI: bodymass index. SD: standard deviation. MI: myocardial infarction. PCI: percutaneous coronary intervention. CABG: coronaryartery bypass graft. TBL: thrombolysis.⁎ p value for the comparison between b75 years vs ≥75 years.
75A. Ielasi et al. / International Journal of Cardiology 179 (2015) 73–78
differences were reported in elderly between BMS and EES (22.0% vs.27.4%, p = 0.32 and 15.2% vs. 16.8%, p = 0.72, respectively).
In non-elderly group, no significant differences were reported in all-cause (p = 0.58), cardiac death (p = 0.63) and TV-MI (p = 0.18) be-tween BMS vs. EES, while TLR (5.4% vs. 2.0%, p = 0.002), TVR (7.3% vs.3.3%, p b 0.001) and definite/probable ST (2.4% vs. 0.8%, p = 0.01) re-sulted significantly higher in patients allocated to BMS vs. EES. In the el-derly group, no differences were reported between patients allocated toBMS vs. EES in the various endpoints. There was a tendency for interac-tion between age (≥75 years) and stent type (EES) in terms of the riskof POCE (p = 0.050). No interaction was found for the other endpointsanalyzed (Table A. Supplementary material).
Kaplan–Meier curves for the POCE andDOCE at 1-year between BMSvs. EES in elderly and non-elderly are shown in Fig. 1.
Onmultivariable analysis baseline Killip Class (HR 1.71 [95%CI 1.40–2.09], p b 0.001), diabetes mellitus (HR 1.64 [95%CI 1.18–2.28],p = 0.003), BMI (HR 0.96 [95%CI 0.92–1.00], p = 0.04) and age≥75 years (HR 2.19 [95%CI 1.59–3.01], p b 0.001)were independent pre-dictors of POCE, whereas baseline Killip Class (HR 2.09 [95%CI 1.66–2.63],p b 0.001), hypertension (HR 1.70 [95%CI 1.12–2.55], p = 0.012), age≥75 years (HR 2.48 [95%CI 1.60–3.70], p b 0.001)were independent pre-dictors of DOCE (Tables 4 and 5).
4. Discussion
Our study shows that: 1) elderly STEMI patients, treated by PPCIwith second generation stents (Co–Cr EES or Co–Cr BMS), have higherincidence of patient and device-oriented combined endpoints com-pared to non-elderly patients, mainly driven by all-cause and cardiacdeath; 2) in this regard, age ≥75 years appears as the most powerful
independent predictor of patient and device oriented endpoints; and3) the beneficial effects of EES over BMS seem to be age-dependent.
In industrialized countries, elderly patients currently represent from22% to 37% of all admissions for acute MI [21] and given increasing lifeexpectancy its treatment is of growing importance [7]. Elderly are usu-ally poorly represented in STEMI clinical trials [22].0 The EXAMINATIONtrial is the first all-comer study comparing EES vs. BMS in STEMI pa-tients, with a broad inclusion of elderly due to its all-comer design.Among the 1498 patients included in the EXAMINATION trial, about16% were aged ≥75 years. This prevalence is slightly higher thanthe 14.1% reported in a meta-analysis of randomized trials evaluat-ing first generation DES vs. BMS in STEMI patients undergoing PPCI,applying our same age threshold of 75 years for defining elderlypatients [23].
In our study, we found that advanced age (≥75 years) was associat-ed with a high incidence of patient and device-oriented endpoints,mainly driven by high rate of all-cause and cardiac death. The highincidence of death in elderly has been already related to the higherprevalence of co-morbidities (such as hypertension, diabetes mellitus,previous stroke, peripheral vascular disease), more severe CAD, andleft ventricular systolic dysfunction [8–10,24]. Moreover elderly pa-tients are also at high risk of non-cardiac death, associated for example,with malignancies and chronic diseases (i.e. lung and/or kidney). Thesefindings are consistent within our population, where elderly patientshave higher prevalence of diabetes and hypertension, lower ejectionfraction and higher Killip Class on admission as compared to non-elderly patients. Furthermore, in our study elderly had more severeatherosclerotic disease as indirectly showed by higher number of stentimplanted, generally smaller, longer and overlapped. It is noteworthythat after adjustment for baseline confounding factors, advanced age

Table 2Baseline angiographic and procedural characteristics.
b75 years (n = 1253) ≥75 years (n = 245)
Overall BMS (n615) EES (n = 638) p Overall BMS (n = 132) EES (n = 113) p p⁎
TIMI flow pre-PCI, n (%)0 738 (59.1) 368 (60.1) 370 (58.1) 0.141 140 (58.3) 74 (57.4) 66 (59.5) 0.041 0.9321 96 (7.7) 53 (8.7) 43 (6.8) 19 (7.9) 5 (3.9) 14 (12.6)2 164 (13.1) 83 (13.6) 81 (12.7) 35 (14.6) 23 (17.8) 12 (10.8)3 251 (20.1) 108 (17.6) 143 (22.4) 46 (19.2) 27 (20.9) 19 (17.1)
TIMI flow post-PCI, n (%)0 20 (1.6) 9 (1.5) 11 (1.7) 0.976 6 (1.7) 2 (1.5) 4 (3.6) 0.478 0.0251 8 (0.6) 4 (0.7) 4 (0.6) 4 (1.7) 3 (2.3) 1 (0.9)2 43 (3.4) 22 (3.6) 21 (3.3) 16 (6.6) 7 (5.4) 9 (8.1)3 1181 (94.3) 579 (94.3) 602 (94.4) 215 (89.2) 118 (90.8) 97 (87.4)
Anticoagulation regimen, n (%)UFH 1017 (81.2) 495 (80.5) 522 (81.8) 0.547 172 (70.2) 95 (72.0) 77 (68.1) 0.514 b0.001LMWH 115 (9.2) 61 (9.9) 54 (8.5) 0.373 18 (7.3) 10 (7.6) 8 (7.1) 0.882 0.357Bivalirudin 81 (6.5) 46 (7.5) 35 (5.5) 0.151 24 (9.8) 10 (7.6) 14 (12.4) 0.206 0.062
Antiplatelet regimen, n (%)ASA pre-PCI 1166 (93.1) 576 (93.7) 590 (92.5) 0.411 222 (90.6) 118 (89.4) 104 (92.0) 0.480 0.180Clopidogrel pre-PCI 1191 (95.1) 584 (95.0) 607 (95.1) 0.882 227 (92.7) 122 (92.4) 105 (92.9) 0.882 0.127IIb/IIIa inhibitor 693 (55.3) 339 (55.1) 354 (55.5) 0.897 92 (37.6) 46 (34.8) 46 (40.7) 0.345 b0.001Thrombectomy, n (%) 833 (66.5) 404 (65.7) 429 (67.2) 0.561 143 (58.4) 77 (58.3) 66 (58.4) 0.991 0.015Direct stenting, n (%) 784 (63.8) 378 (63.1) 406 (64.4) 0.625 101 (42.1) 56 (42.7) 45 (41.3) 0.819 b0.001Post-dilatation, n (%) 186 (14.8) 79 (12.8) 107 (16.8) 0.051 35 (14.3) 24 (18.2) 11 (9.7) 0.060 0.822Overlapping stent, n (%) 324 (25.9) 161 (26.2) 163 (25.5) 0.799 80 (32.7) 45 (34.1) 35 (31.0) 0.604 0.028Stent implanted per patient, n ± SD 1.37 ± 0.63 1.37 ± 0.63 1.37 ± 0.64 0.951 1.48 ± 0.72 1.44 ± 0.66 1.54 ± 0.78 0.277 0.011Total stent length, mm ± SD 27.14 ± 13.73 26.75 ± 12.96 27.51 ± 14.43 0.330 29.42 ± 15.21 28.39 ± 14.1 30.63 ± 16.35 0.254 0.020Total stent length N30 mm, n (%) 330 (26.5) 153 (25.1) 177 (27.8) 0.287 86 (35.4) 45 (34.4) 41 (36.6) 0.714 0.005Maximal stent diameter, mm ± SD 3.22 ± 0.46 3.21 ± 0.46 3.23 ± 0.45 0.379 3.12 ± 0.42 3.10 ± 0.43 3.15 ± 0.41 0.418 0.003Maximal stent diameter N3 mm, n (%) 592 (47.5) 280 (46.0) 312 (49.0) 0.289 91 (37.4) 48 (36.6) 43 (38.4) 0.779 0.004
ST resolution post-PCI, n (%)N70% 732 (64.2) 370 (66.0) 362 (62.4) 0.213 120 (56.9) 68 (60.2) 52 (53.1) 0.298 0.044
BMS: bare-metal stent. EES: everolimus-eluting stent. PCI: percutaneous coronary intervention. UFH: unfractioned heparin. LMWH: lowmolecular weight heparin. ASA: aspirin. SD: stan-dard deviation.⁎ p value for the comparison between b75 years vs ≥75 years.
76 A. Ielasi et al. / International Journal of Cardiology 179 (2015) 73–78
(≥75 years) was still a strong independent predictor of patient and de-vice oriented endpoints.
In the setting of STEMI, our study represents the first evaluation onthe impact of a second generationDES on outcomes followingPPCI in el-derly patients. In particular, the use of EES does not appear to have thesame positive impact as compared to BMS either in elderly or in non-elderly. Limited and contrasting data are currently available concerningthe impact of advanced age on outcomes following DES implantation inpatients with stable angina or acute coronary syndromes. The recently
Table 3Clinical Outcomes at 1-year follow-up.
b75 years (n = 1253)
Overall BMS (n = 615) EES (n = 6
Primary end-point, n (%) 132 (10.5) 76 (12.4) 56 (8.8)Device-oriented end-point, n (%) 64 (5.1) 41 (6.7) 23 (3.6)
Death, n (%)All-cause 18 (1.4) 10 (1.6) 8 (1.3)Cardiac 14 (1.1) 6 (1.0) 8 (1.3)TV-myocardial infarction, n (%) 10 (0.8) 7 (1.1) 3 (0.5)Any Myocardial infarction, n (%) 12 (1.0) 8 (1.3) 4 (0.6)
Revascularization, n (%)Target lesion 46 (3.7) 33 (5.4) 13 (2.0)Target vessel 66 (5.3) 45 (7.3) 21 (3.3)Non-target vessel 67 (5.3) 32 (5.2) 35 (5.5)Definite/probable stent thrombosis, n (%) 20 (1.6) 15 (2.4) 5 (0.8)Bleeding 50 (4.0) 29 (4.7) 21 (3.3)Major 14 (1.1) 8 (1.3) 6 (0.9)Minor 38 (3.0) 23 (3.7) 15 (2.4)
BMS: bare-metal stent. EES: everolimus-eluting stent.⁎ p value for the comparison between b75 years vs. ≥75 years.
published XIMA trial showed that second-generation EES is associatedwith a lower incidence of MI and TVR, without an increased incidenceof major bleeding as compared to BMS in octogenarians with non-STEMI, unstable and stable angina. In contrast to this, our analysis didnot show any of these differences; this may be related not only to thefact that these endpoints are underpowered in our analysis, but also tothe fact that our analysis included only STEMI patients, who have differ-ent ischemic risks than those patients included in the XIMA trial [25].Consistently with our results, De Luca et al. recently demonstrated
≥75 years (n = 245)
38) p Overall BMS (n = 132) EES (n = 113) p p⁎
0.039 63 (24.5) 30 (22.0) 33 (27.4) 0.321 b0.0010.014 39 (15.9) 20 (15.2) 19 (16.8) 0.723 b0.001
0.580 34 (13.9) 16 (12.1) 18 (15.9) 0.390 b0.0010.639 31 (12.7) 15 (11.4) 16 (14.2) 0.512 b0.0010.184 3 (1.2) 2 (1.5) 1 (0.9) 0.655 0.5100.221 4 (1.6) 2 (1.5) 2 (1.8) 0.875 0.347
0.002 7 (2.9) 4 (3.0) 3 (2.7) 0.806 0.528b0.001 13 (5.3) 6 (4.5) 7 (6.2) 0.566 0.9800.824 14 (5.7) 9 (6.8) 5 (4.4) 0.421 0.8160.019 6 (2.4) 4 (3.0) 2 (1.8) 0.525 0.3500.198 18 (7.3) 10 (7.6) 8 (7.1) 0.892 0.0210.544 5 (2.4) 3 (2.3) 2 (2.7) 0.847 0.0970.152 13 (5.3) 7 (5.3) 6 (5.3) 0.998 0.073
Fig. 1.Kaplan–Meier curves show survival free from the patient-oriented combined endpoint of all-cause death, any-recurrentMI and any-revascularization at 1-year between BMS vs. EESin elderly and non-elderly (1A). Kaplan–Meier curves show survival free from the device-oriented combined endpoint of cardiac death, target-vessel myocardial infarction and TLR at 1-yearbetween BMS vs. EES in elderly and non-elderly (1B). EES: everolimus-eluting stent. BMS: bare-metal stent.
77A. Ielasi et al. / International Journal of Cardiology 179 (2015) 73–78
that advanced age (≥75 years) was associated with a significantlyhigher mortality without any protective effect of first generation DESon the risk of re-MI, TLR, and ST as compared to BMS [23]. Conversely,it is noteworthy that a sub-study of the HORIZONS-AMI trial, showedthat the effect of PES in reducing ischemia-driven TLR, was independentof age (b70 years vs. ≥70 years) up to 3-year follow-up [26]. Differ-ences in elderly threshold used (≥70 or ≥75 years), in sample sizeand in the follow-up length may help to explain the contrasting resultsbetween those studies. Our findings may emphasize the importance ofage-related co-morbidities with a subsequent high mortality stent-unrelated, which may obscure the advantages of EES over BMS in thispopulation and may be taken into consideration in the decision-making stent selection in elderly STEMI patients undergoing PPCI.
4.1. Limitations
This study is a post-hoc analysis of the EXAMINATION trial. Althoughthe primary endpoint was 80% powered to demonstrate any differencebetween stents groups, other endpoints are underpowered. Neverthe-less, these data currently represent the only ones on performance ofEES on elderly STEMI patients.
Table 4Independent predictors of the patient oriented endpoint at 1-year follow-up.
Hazard ratio (95% confidence interval) p-Value
Baseline Killip class 1.71 [95%CI 1.40–2.09] b0.001Diabetes mellitus 1.64 [95%CI 1.18–2.28] 0.003BMI 0.96 [95%CI 0.92–1.00] 0.049Age (≥75 years) 2.19 [95%CI 1.59–3.01] b0.001
BMI: body mass index.
Table 5Independent predictors of the device-oriented endpoint at 1-year follow-up.
Hazard ratio(95% confidence interval)
p-Value
BMS implanted at index procedure 1.46 [0.91–2.02] 0.128Baseline Killip class 2.09 [1.66–2.63] b0.001Hypertension 1.70 [1.12–2.55] 0.012Age (≥75 years) 2.48 [1.60–3.70] b0.001
5. Conclusions
Elderly (≥75 years) STEMI patients undergoing PPCI exhibit higherrate of patient and device oriented endpoints, mainly driven by higherrate of all-cause and cardiac death, even after adjustment for confound-ing factors, as compared to younger (b75 years) STEMI patients. Thebeneficial effects of EES over BMS appear to be age-dependent and inparticular less evident in elderly.
Disclosures
Dr Sabatè has received consultant and speaker fees from AbbottVascular, Medtronic, and Cordis J&J. Dr Valgimigli received an honorar-ium as a public speaker Terumo, The Medicines Company, Medtronic,Iroko, Merck, Abbott, Ely Lilly, AstraZeneca, Cordis, CID, and Bayer.Dr Brugaletta has received speaker fees from Abbott Vascular andAstraZeneca. Dr Ielasi has received speaker fees from Abbott Vascular.All other authors declare that they have no conflicts of interest.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.ijcard.2014.10.038.
References
[1] E.M. Antman, M. Hand, P.W. Armstrong, et al., 2007 focused update of the ACC/AHA2004 guidelines for the management of patients with ST-elevation myocardialinfarction: a report of the American College of Cardiology/American Heart Associa-tion Task Force on Practice Guidelines, J. Am. Coll. Cardiol. 51 (2008) 210–247.
[2] P.G. Steg, S.K. James, D. Atar, et al., ESC Guidelines for the management of acutemyocardial infarction in patients presenting with ST-segment elevation, Eur. HeartJ. 33 (2012) 2569–2619.
[3] G.W. Stone, B. Witzenbichler, G. Guagliumi, et al., Bivalirudin during primary PCI inacute myocardial infarction, N. Engl. J. Med. 358 (2008) 2218–2230.
[4] G. Montalescot, S.D. Wiviott, E. Braunwald, et al., Prasugrel compared with clopidogrelin patients undergoing percutaneous coronary intervention for ST-elevationmyocardi-al infarction (TRITON-TIMI 38): double-blind, randomised controlled trial, Lancet 373(2009) 723–731.
[5] P.G. Steg, S. James, R.A. Harrington, et al., Ticagrelor versus clopidogrel in patientswith ST-elevation acute coronary syndromes intended for reperfusion with primarypercutaneous coronary intervention: a Platelet Inhibition and Patient Outcomes(PLATO) trial subgroup analysis, Circulation 122 (2010) 2131–2141.
[6] G. De Luca, E.P. Navarese, H. Suryapranata, Ameta-analytic overview of thrombectomyduring primary angioplasty, Int. J. Cardiol. 166 (2012) 606–612.
[7] R.W. Yeh, S. Sidney, M. Chandra, M. Sorel, J.V. Selby, A.S. Go, Population trends in theincidence and outcomes of acute myocardial infarction, N. Engl. J. Med. 362 (2010)2155–2165.
[8] D.R. Holmes Jr., H.D. White, K.S. Pieper, S.G. Ellis, R.M. Califf, E.J. Topol, Effect of ageon outcome with primary angioplasty versus thrombolysis, J. Am. Coll. Cardiol. 33(1999) 412–419.

78 A. Ielasi et al. / International Journal of Cardiology 179 (2015) 73–78
[9] R.J. Goldberg, D. McCormick, J.H. Gurwitz, J. Yarzebski, D. Lessard, J.M. Gore, Age-related trends in short- and long-term survival after acute myocardial infarction: a20-year population-based perspective (1975–1995), Am. J. Cardiol. 82 (1998)1311–1317.
[10] G. De Luca, A.W. van 't Hof, J.P. Ottervanger, et al., Ageing, impaired myocardial per-fusion, and mortality in patients with ST-segment elevation myocardial infarctiontreated by primary angioplasty, Eur. Heart J. 26 (2005) 662–666.
[11] G. Guagliumi, G.W. Stone, D.A. Cox, et al., Outcome in elderly patients undergoingprimary coronary intervention for acute myocardial infarction: results from theControlled Abciximab and Device Investigation to Lower Late Angioplasty Complica-tions (CADILLAC) trial, Circulation 110 (2004) 1598–1604.
[12] I. Iakovou, T. Schmidt, E. Bonizzoni, et al., Incidence, predictors, and outcome ofthrombosis after successful implantation of drug-eluting stents, JAMA 293 (2005)2126–2130.
[13] T. Palmerini, G. Biondi-Zoccai, D. Della Riva, et al., Clinical outcomes with drug-eluting and bare-metal stents in patients with ST-segment elevation myocardialinfarction: evidence from a comprehensive network meta-analysis, J. Am. Coll.Cardiol. 62 (2013) 496–504.
[14] S. Bangalore, N. Amoroso, M. Fusaro, S. Kumar, F. Feit, Outcomes with various drug-eluting or bare metal stents in patients with ST-segment-elevation myocardial in-farction: a mixed treatment comparison analysis of trial level data from 34,068patient-years of follow-up from randomized trials, Circ. Cardiovasc. Interv. 6(2013) 378–390.
[15] M. Sabate, A. Cequier, A. Iniguez, et al., Rationale and design of the EXAMINATION trial:a randomised comparison between everolimus-eluting stents and cobalt–chromiumbare-metal stents in ST-elevation myocardial infarction, EuroIntervention 7 (2011)977–984.
[16] M. Sabate, A. Cequier, A. Iniguez, et al., Everolimus-eluting stent versus bare-metalstent in ST-segment elevation myocardial infarction (EXAMINATION): 1 year resultsof a randomised controlled trial, Lancet 380 (2012) 1482–1490.
[17] E. Braunwald, E.M. Antman, J.W. Beasley, et al., ACC/AHA guideline update for themanagement of patients with unstable angina and non-ST-segment elevation myo-cardial infarction—2002: summary article: a report of the American College ofCardiology/American Heart Association Task Force on Practice Guidelines (Committee
on the Management of Patients With Unstable Angina), Circulation 106 (2002)1893–1900.
[18] K.P. Alexander, L.K. Newby, P.W. Armstrong, et al., Acute coronary care in the elder-ly, part II: ST-segment-elevation myocardial infarction: a scientific statement forhealthcare professionals from the American Heart Association Council on ClinicalCardiology: in collaboration with the Society of Geriatric Cardiology, Circulation115 (2007) 2570–2589.
[19] F. Schiele, N. Meneveau, M.F. Seronde, et al., Changes in management of elderly pa-tients with myocardial infarction, Eur. Heart J. 30 (2009) 987–994.
[20] F. De Felice, R. Fiorilli, A. Parma, et al., Comparison of one-year outcome of patientsaged b75 years versus N/=75 years undergoing “rescue” percutaneous coronary in-tervention, Am. J. Cardiol. 108 (2011) 1075–1080.
[21] T. Bauer, O. Koeth, C. Junger, et al., Effect of an invasive strategy on in-hospital out-come in elderly patients with non-ST-elevation myocardial infarction, Eur. Heart J.28 (2007) 2873–2878.
[22] P.Y. Lee, K.P. Alexander, B.G. Hammill, S.K. Pasquali, E.D. Peterson, Representation ofelderly persons and women in published randomized trials of acute coronary syn-dromes, JAMA 286 (2001) 708–713.
[23] G. De Luca, M.T. Dirksen, C. Spaulding, et al., Impact of age on long-term outcomeafter primary angioplasty with bare-metal or drug-eluting stent (from the DESERTcooperation), Am. J. Cardiol. 112 (2013) 181–186.
[24] V.S. DeGeare, G.W. Stone, L. Grines, et al., Angiographic and clinical characteris-tics associated with increased in-hospital mortality in elderly patients withacute myocardial infarction undergoing percutaneous intervention (a pooledanalysis of the primary angioplasty in myocardial infarction trials), Am. J.Cardiol. 86 (2000) 30–34.
[25] A. de Belder, J.M. de la TorreHernandez, R. Lopez-Palop, et al., A prospective random-ized trial of everolimus-eluting stents versus bare metal stents in octogenarians:Xience or vision stents for the management of angina in the elderly — the XIMAtrial, J. Am. Coll. Cardiol. 63 (2014) 1371–1375.
[26] D. Dudek, R. Mehran, A. Dziewierz, et al., Impact of advanced age on the safety andeffectiveness of paclitaxel-eluting stent implantation in patients with ST-segmentelevation myocardial infarction undergoing primary angioplasty: the HORIZONS-AMI trial, Catheter. Cardiovasc. Interv. 82 (2013) 869–877.
Related Documents











