ISSN : 0970 2067 rt7r*. b afmeOlci n "o2l i n, .yg Official Publication of Indian Association of Biomedical Scientists (IABMS)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ISSN : 0970 2067
rt7r*. b afmeOlci n "o2l
i n, .yg
Official Publication of
Indian Association ofBiomedical Scientists (IABMS)
1l
BIOMEDICIITEVoL 33 No. 4: (October - December) 2013
Contents
Tbpics andAuthors Page (s)
tr. Past presidents of IABMS.. 458
m. Review/ SpecialArticles
1. Thermography in Orthodontics - A review 459-462Kishorekumar S., Faisal Tajir, Gnanashanmugam K., Saravanan B., Mahalakshmi K.and SivakumarM.
2. Frogry affair: Are frogs threatened and endangered species? -AReview 463467\ Rathinasamy Sheeladevi and Loganathan Sundareswaran
IV. ResearchPapers
3. Correlation of homocysteine concentrations with severity of coronrry arterT disease 46H72Harish Rao B', Govindaraju V and Manjunath CN
4. Comparitive evaluation of two dilferent staining methods for detection of Helicobacterpyloritn gastric biopsles 473475
ManjulaAVagarali, Sharada C Metgud and Supnya
5. Isol,etion oforal aerobic and anaerobic bacteria from seliva and subgingival plaque samples inchronic periodontitis patients. 476482
S.Jayaram,Bahawath Singb Balagurunathan and S.P.K. Kennedy Babu
6. Role of magnesium in cerebrovascular accident CVApatients 483-486
Shrabani Mohanty, Roopa Murgod and Venkata Bharatkumar Pinnelli
7. Adiponectin, inflammatory and lipid profile in healthy obese young adults of an Urban populationin South Indie-Across sectiond study. 487493
Smita S Sonoli, Anil Malleshappa and V.A.Kothiwale
8. Association between Ilomocysteine and Ischemia ModifiedAlbumin (IMA), lipids & inflammationbiomarkers in obese pnemenopausel women. 494-500
K. Malleshappa" P. Rajasekhar and C.Nandini
9. Aberrant crypt formation in colon of albino rats following oral administretion of orlistat 501-505
Nidhi Singh, Sl.Jethani, RK. Rohatgi, Uuhi Kalra, Deepa Singh, Alka Aggarwal and Aksh Dubey.
10. A comparative study ofinsulin resistance among prehypertensiye and normd subjects. 506-510
Bharath T, Roopakala M S and Manjula P.
11. I)oes prenatal testosterone have a role in development ofcerebral palsy? 511-514Sudhakar. H.H., Veena Umesh. B., Vennila Palanivelu. M. and Riyaz. H.
12. Study of occipitalization of aflas with focus on embryological basis, evolution,paleopatholory and clinical aspects. 515-519
VivekaS andSudhaMJ
13. Evaluation of total serum alpha-l-antitrypsin aafl lifsmin E in smoker and non smokerchronic obstructive pu[nonary disease patients. 520-525
Benazeer Jadhav, J. S. Bardapurkar, V. R. Bhagwat and S. J. Bardapurkar.
14. Effect of dietary n-3 polyunsetureted fatty acids (PUFA) formulations on lipid metabolism in albino rat. 52G532Nagabhushan Reddy M and Basha Mohideen Md
15. Few minutes a day for exencise: Comparative study of CRP, oxidant antioxidant status in COPD:Selfs good, supervised can be great 533-536
Shah Mohammad Abbas Waseem , Zuber Ahmad and Najmul Islam.
16. Serum and salivary alkaline phosphatase level ln smokers and its correlation withcommunity periodontal index for treatment need (CPITN score) -Apilot study. 537-539
Baishali Saha S.C.Chandraselfiaran and Bhagavad Gita.
17. The study of spiromefy tests in healthy male and female adults with respect to bodymass index end waist to hip ratio. 540-544
K.K. Kasturi.
wn w. hio m e dicin e o nlin e. org Biomedicine - VoL 33 No. 4: 201j
VRB
Highlight
520 Biomedicine: 2013; $G): 520 - 525
Evaluation of total serum alpha-l-antitrypsin and Vitamin E in smoker and nonsmoker chronic obstructive pulmonary disease patients.
'Benazeer Jadhav, 'J. S. Bardapurkar, 'V. R. Bhagwat and 'S. J..Bardapurkar.rDeparment of Biochemistry, SBH Govt. Medical College, Dhule, Maharashta,INDIA.
2Dept. of Biochemistry, Govt. Medical College and Hospital, Aurangaba4 INDIA.'Shree nursing Home, Sanmitra Colony, Aurangabad, INDIA.
@eceived:27.08.2013 Revised:02.10.2013 Accepted: 15.10.2013)
Corresponding author
Dr. Benazeer Jadhav. Email: j [email protected]
AbstractIntroduction: Chronic obstructive putmonary disease (COPD) is a health problem with increasing severity, as
erposure to risk fabtors such as cigarette smoke, pollution is inevitable. Oxidant-antioxidant imbalance causeercess of oxidative burden leading to lung tissue damage. Presently, diagnosis of COPD is based on impairedlungfunctiontests.Aims: This study was aimed to measure serum levels of total alpha 1 antitrypsin (alAI), a serine protease-inhibitor and lipophilic antioxidant vitamin E in various stages of COPD and to correlate them with BMI andookingstatus.Materials and Methods: The study involved 100 stable COPD patients grouped in to four stages based onGOLD criterion (FEVI% predicted). Serum levels of total alpha I antitrypsin (olAI), a serine protease-inhibitor and lipophilic antioxidant vitamin E in various stages of COPD were assessed and correlated with BMImdsmokingstatus.Results: Total alAI showed increasing trend while vitamin E levels showed decreasing trend across the stagesof COPD. Mean cllAT is higher while mean vitamin E level is lower in active smokers than non smokers and ex-mokers. olAI showed weak negative correlation (r: -0.3, p<0.05) while Vitamin E has significant positiveorrelation (r : 0. 6, p<0. 05) with FEV I % predicted.Conclusion: Raised olAI and lowervitamin E levels, indicate excess of oxidative stress in smokers and theyhve shown opposing trend across the stages of COPD. alAI may serve as potential biomarkers in COPDpathophysiology.fey words : COPD, serum vitamin E, serum total ol AT.
htroduction
llhronic O
I (coPD) i\-/increasingrisk factors such as cigarette smoke, pollutioncombined with increasing life expectancy makes
COPD a major epidemic in near future. A study byJindal et al. (l) showed the prevalence of COPD as
4.1, and prevalence ratio as2.65:1 in smoker and nonsmokers in India (1,2), clearly emphasizing COPDas the upcoming health problem in India. COPD isdefined as a group of diseases charactenzed byairflow limitation that is not fully reversible. Theairflow limitation is progressive and associated with
www. bio m e dicin eo nlin e. org
an abnormal inflammatory response of ltrng tonoxious particles or gases. The concept of abnormalinflammatory response and progressive naflre ofairflow limitation has instigated interest in severalworkers to study the underlying cellular andbiochemical mechanisms in etiopathogenesis ofCOPD (3, 4). The diagnosis of COPD is primarilybased on lung function tests. Key parameters
measured are forced expiratory volume in I second(FEVI) and forced vital capacity (FVC). ReducedFEVIIFVC ratio is considered as the most sensitiveindex for early airway obstnrction in COPD (5).GOLD guidelines propose a classification of diseas'e
severity into four stages primarily based onFEvlYopredicted (3). The staging is based on the
Biomedicine - VoL 33 No. 4: 2013
VRB
Highlight
Benazeer Jadhav et aL: Evaluation of totaf,.......... patients
fimctional impairment only. It overlooks the cellularchanges and inflammatory markers in the lung andperipheral tissue as biomarkers of diseasepathogenesis (6). Exposure to smoke is one of thefrequent histories found in COPD patients. It isreported that more than 90% COPD patients arecurent or ex-smokers, while only 10-15 % of these
smokers develop COPD. This could be due tovariation in individual's susceptibility towardsenvironmental and genetic factors to develop thedisease (7).Smoke exposure is the initiating eventthat recruits and activates inflammatory celts in thealveoli and lower respiratory tract (8). This increases
the local inflammation in the pulmonarycompartment and lead to excess oxidative burden (8,9). This oxidative burden is counteracted normally byvarious protective biomolecules like alpha-l -
antitrypsin (alAI), a serine protease inhibitor and
lipophilic antioxidant Vitamin E. More than 95%protection against neutrophil elastase is given byolAI and thus the pulmonary elastic recoil ispreserved in respiratory tract (10, I l). Lung tissue isrich in the lipid content owing to the presence ofsnrfactant, and lipophilic antioxidant Vitamin E isintegral component of surfactant (12). Moreovervitamin E has long half life endowing the lung tissue
in combating oxidative stress. So the two parameters
are particularly important in pulmonary tissue ( I 3).
Aim
The aim of the present study was to estimate senrmtotal olAI and Vitamin E in COPD patients and tofind out correlation between these parameters and
Itmg firnction tests, if any and to compare the resultsin smoker and non-smoker COPD patients.
Material andMethods
This cross sectional study was performed in theDepartment of Biochemistry, Government MedicalCollego, Aurangabad, in collaboration with Shree
Nursing Home and the Department of Medicine,Government Medical Colle Ea, Aurang abad, duringMay 2009 to July 2009. 100 diagnosed patients ofCOPD attending Medicine OPD were enrolled in thestudy, following institutional ethical committee
www. bi o m e di cin e o n lin e" o r g
s2t
pennission and guidelines. Patients with acuteinfections like URTI, inflammations and otherchronic diseases like exacerbation of COPD, CCFand anemia were excluded. Stable COPD patients(smokers or non-smokers) were randomly includedin the study, as they come to Medicine OPD.Puhnonary firnction tests were carried out in themonring hours which involved measurement ofFEVI% predicted, FVC etc. Patients were groupedinto four stages based upon 'FEVI % predicted'according to GOLD guidelines. Stage I has the value<80o/o, in stage II it varies between 50 -80%, while instage III it varies between 30 -50o and stage [V has<30oh ofpredicted value or is equal to SUo/obut signsof right heart failure or respiratory failure arepositive. In all stages FEVI/FVC ratio is (0.7 (Table
l) (3). Further patients are divided into three groups
according to their smoking stafus, and again groupedinto four stages based on GOLD criterion. BMI ofpatients was calculated by using formula height (rn')divided by weight (kg). Five ml of venous blood wascollected at random in plain bulb from each patientfor estimation of serum total alAf and Vitamin Elevels. The biochemical and clinical parameters werecompared among COPD patients themselves based
onstages ofCOPD.
Estimation of total alAI in serum was done byquantitative immuneturbidimetric method by usingready to use reagent test kit obtained fromSPINREACT Computy, Spain. Tests were done as
per manufacturer's guidelines on fully automatedchemistry analyzer XL 640 (TransAsia B iomedicals,Mumbai). Estimation of vitamin E was done byB aker and Frank method ( 1 5 ) usingspectrophotometer (Thermo Spectronic, UK) at 530IIIII.
Statistical analysis was done using graph pad and
SPSS -17 softrvare. AI.IOVA test was employed tofind out significance of the difference in the mean
values of biochemical parameters across variousstages of COPD and various groups according tosmoking status.
Biomedicine - VoL 33 No. 4: 2013
s22 Benazeer Jadhat et aL: Evaluation of total.......... patients
Table I GOLD classilication of COPD patients.
GOLD Stage Severity Spirometry0
1
2
3
4
At risk
MildModerate
Severe
Very severe
Normal
FEVIIFVC< 0.7 and FEVl<-8Oo/o predicted
FEVI/FVC< 0.7 and FEVI : 50-80 % predicted
FEVI/FVC< 0.7 and FEV1:30-50% predicted
FEVIIFVC<0.7 and FEVI <30oh predicted or FEV1< 50opredicted with respiratory failure or signs of right heartfailure.
Table 2 Distribution of smoker, non-smoker and ex-smoker COPDpatients in various COPD stages.
N Stage I Stage II Stage m Stage IVFEVI% Pred
Non smokers
Ex smokers
Active smokers
Total Patients
78 x 7.127
5
I00
6
59.97 + 9.16
t2t603
31
40.67 + 5.90
t8t904
4l
25.05 + 6.69
4
t701
22
39
53
08
100
* p value (<0.05) statistically significant
Table 3 Serum olAT, Vit E, BMI in studied groups of COPD patients inrelation with COPD stages.
Reference Stage I Stage II Stage III Stage IV01AI mgoh
VitEmgYoBMI
90-200
0.5- I .8
149 + 16* 163 +21*1.60 + 0.15* 1.20 + 0.24*
22.19 + 5.13 22.39 + 4.ll
180 +22* 190 t33*0.88 + 0.25* 0.62 *,0.26*
21 .06 + 5.53 18 r 3.0
Biochemical parametes in COPD stages+cl-AT -+-Yn-E
I ,"o-# !Y
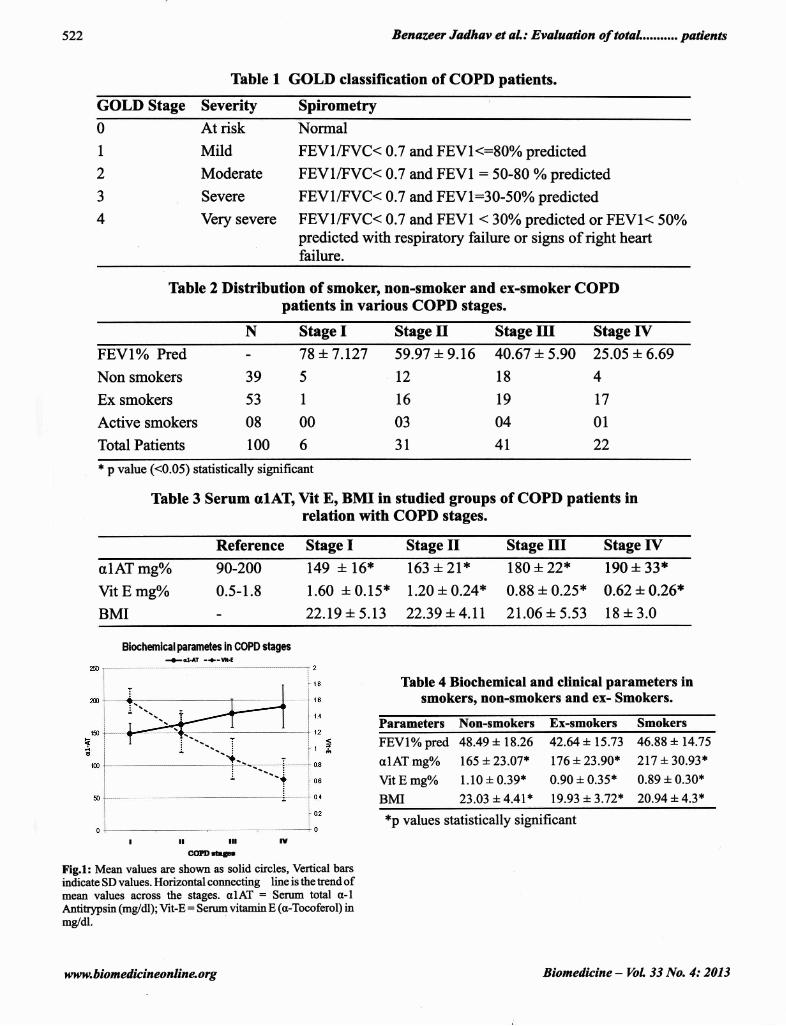
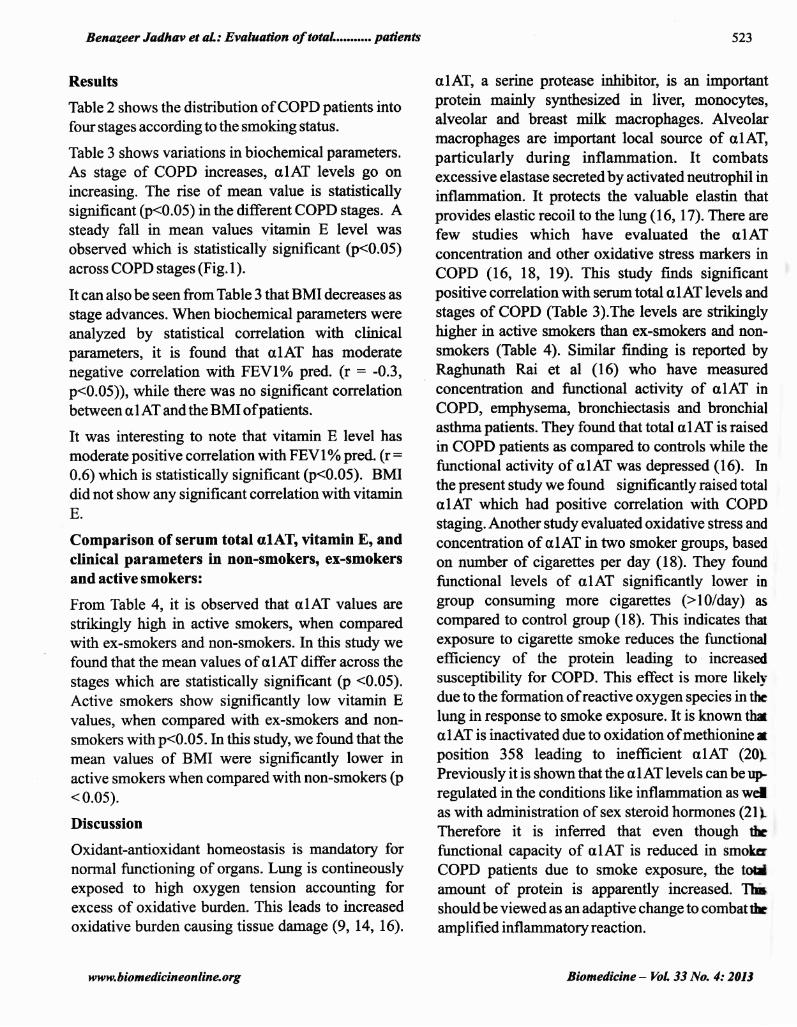
Fig.l: Mean values are shown as solid circles, Venical barsindicate SD values. Horizontal connecting line is the trend ofmean values across the stages. olAf _ Serum total o-lAntitfrpsin (mg/dl); Vit-E - Senrm vitamin E (o-Tocoferol) inmg/dl.
tttwty. b i o m e di c in e o n lin e. o r g
Table 4 Biochemical and clinical parameters insmokers, non-smokers and ex- Smokers.
Parameters Non-smokers Ex-smokers Smokers
FEVIo/o pred 48.49 + 18.26 42.64 +. 15.13
alAI mgo/o 165 *23.07* 176 +23.90*
Vit E mg%o l.l0 + 0.39* 0.90 + 0.35*
BMI 23.03 + 4.4t* 19.93 + 3.72*
46.88 + 14.75
217 + 30.93*
0.89 + 0.30*
20.94 + 4.3**p values statistically significant
Biomedicine - VoL 33 No. 4: 2013
Benazeer Jadhat et aL: Evaluation of total.....o..o pafients
Results
Thble 2 shows the distribution of COPD patients intofotrr stages according to the smoktng stafus.
Table 3 shows variations in biochemical parameters.
As stage of COPD increases, olAI levels go onincreasing. The rise of mean value is statisticallysignificant (p<0.05) in the different COPD stages. Asteady fall in mean values vitamin E level wasobserved which is statistically significant (p<0.05)across COPD stages (Fig. l).
It can also be seen from Table 3 that BMI decreases as
stage advances. When biochemical parameters wereanalyzed by statistical correlation with clinicalparameters, it is found that olAf has moderatenegative correlation with FEVI% pred. G - -0.3,p<0.05)), while there was no sigdficant correlationbetween CI,lAT and the BMI ofpatients.
It was interesting to note that vitamin E level has
moderate positive correlation with FEVI%pred. (r -0.6) which is statistically significant (p<0.05). BMIdid not show any significant correlation with vilaminE.
Comparison of serum total alAT, vitamin E, andclinical parameters in non-smokers, ex-smokersand active smokers:
From Table 4, it is observed that alAf values are
strikingly high in active smokers, when comparedwith ex-smokers and non-smokers. In this study wefound that the mean values of alAI differ across the
stages which are statistically significant (p <0.05).
Active smokers show significantly low vitamin Evalues, when compared with ex-smokers and non-
smokers with p<0.05. In this study, we found that the
mean values of BMI were significantly lower inactive smokers when compared with non-smokers (p< 0.05).
Discussion
Oxidant-antioxidant homeostasis is mandatory fornorrnal firnctioning of organs. Lung is contineouslyexposed to high oxygen tension accounting forexcess of oxidative burden. This leads to increased
oxidative burden causing tissue damage (9, L4, 16).
www. bi o m e di cin e o n I in e. org
523
ulAI, a serine protease inhibitor, is an importantprotein mainly slmthesized in liver, monocytes,alveolar and breast milk macrophages. Alveolarmacrophages are important local source of alAI,particularly during inflamrnation. It combatsexcessive elastase secreted by activated neutrophil ininflarnmation. It protects the valuable elastin thatprovides elastic recoil to the lung (16, l7). There arefew studies which have evaluated the alATconcentration and other oxidative stress markers inCOPD (L6, 18, 19). This study finds significantpositive correlation with serum total olAI levels and
stages of COPD (Table 3).The levels ate strikinglyhigher in active smokers than ex-smokers and non-smokers (Table 4). Similar finding is reported byRaghunath Rai et al (16) who have measured
concenffation and functional activity of alAI inCOPD, erphysema, bronchiectasis and bronchialasthmapatients. They found that total olAf is raised
in COPD patients as compared to controls while thefirnctional activity of olAf was depressed (16). Inthe present study we found significantly raised totalalAI which had positive correlation with COPDstaging. Another study evaluated oxidative stress and
concentration of alAI in two smoker groups, based
on number of cigarettes per day (18). They foundfunctional levels of alAf significantly lower ingroup consuming more cigarettes (>10/day) as
compared to control group (18). This indicates thaexposure to cigarette smoke reduces the fimctionalefficiency of the protein leading to increased
susceptibility for COPD. This effect is more likelydue to the formation of reactive oxygen species in ttrclung in response to smoke exposrrre. It is known thxolAI is inactivated due to oxidation ofmethionine trposition 358 leading to inefficient olAT (20L
Previously it is shown that the ulAI levels can b. r+regulated in the conditions like inflammation as welas with administration of sex steroid hormones (21 tTherefore it is inferred that even though fufunctional capacity of ulAT is reduced in smokcr
COPD patients due to smoke exposure, the to&J
amount of protein is apparently increased. Thishouldbe viewed as an adaptive change to combatthamplified infl ammatory reaction.
Biomedicine - VoL 3i No. 4: 2013

524
In this study, it is observed that the mean values ofvitamin E levels fall progressively and significantlyas the stage of COPD advances (Fig. l). There are
significantly low levels of serum vitamin E in activesmoker as compared to non smokers and ex smokers,(Table 4) these results are in congruence with past
studies. Raghunath Rai et al, (16) have demonstratedlow vitamin E levels in patients with COPD as
compared to controls (16).Similar results werereported by Eric Pacht (22) who measured vitamin Ehvels in broncho-alveolar lavage fluid, serum,macrophages in smokers and non-smokers. He foundvitamin E levels are lower in smokers as compared tox)n- smokers (22). This can be explained on the basisof increasing oxidation of vitamin E to its inactivenetabolites due to excess of oxidative burden inrtive smoker COPD patients. This study reports fallh BMI as the stage advances (Table 3). Thisobservation indicates only the systemic involvementpevalent in COPD. There is no direct relationship ofBMI and changes in other biochemical parameters
studied in COP patients. The findings of this studysrggest that the biochemical parameters such as
senrm total ulAT and vitamin E levels may have
some role in pathophysiolory of the disease. The
finding may also help in assessing disease severityand prognosis in response to therapeuticinterventions in the COPD.
Limitations
It is imperative to state the limitation of this study.
The functional status of the protein i.e. alAI is notassessed. Measurement of firnctional activity ofolAI in different stages of COPD would have been
more informative.
Conclusion
This is a cross sectional study carried out involvingCOPD patients who were diagnosed on spirometry.
They are gfouped into four stages based upon the
FEV \%predicted which is the firnctional indicator ofairflow obstruction. We estimated serum levels oftotal ulAI and vitamin E and clinicalparameters likeBMI, FEVI% predicted. The mean levels of alATwere found to be higher as stage of COPD advanced.
www. biom edicin e o nlin e. org
Benazeer Jadhav et aL: Evaluation of total......... pafients
The levels were significantly higher in currentsmokers as compared to ex-smokers and nonsmokers. This could be due to inactivation of proteinby oxidative stress, and up regulation of synthesis soas to combat excess oxidative burden, hence thelevels oftotal olAT might have been raised in spite oflower activity of protein. Vitamin E is majorlipophilic antioxidant compound which plays vitalrole in dealing with oxidative stress in lung. Thestudy found significant fall in mean level of thisdietary antioxidant vitamin E. Significant lowermean levels were found in active smokers as
compared to ex- smokers and non smokers. Thepresent study clearly accenfuates the importance ofulAI and vitamin E as the protective mechanisms tocombat excess oxidative stress in COPD. Henco,these parameters should be considered as thepotential biomarkers of COPD. They can be used toassess the proglosis of COPD during therapy, as theirmean leve1s vary with cellular events in relation withCOPD stage.
Declaration of Interests
We declare that there are no conflicts oflnterests.
Acknowledgements
We express our sincere thanks to Dr. R. J. Shende fornecessary administrative help in the successful
completion ofthe work.
References
1. Viegi G, ScogRamiglio A, Baldacci S, Pistelli, F and
Carrozzi, L. Epidemiology of chronic obstructivepulmonary disease (COPD). Respiration . 2001 ; 68 ( 1 ) :4- I 9.
2. Jindal S K, Aggarwal A N, Chaudhry K, Chhabra S K,D'Souza GA, Guph D, Katiyar S K, Kumar R, Shah B and
VijayanV K. Asthma Epidemiology Study Group. Amulticentric study on epidemiology of chronic obstructivepulmonary disease and its relationship with tobacco
smoking and environmental tobacco smoke exposure.
Indian J Chest Dis Allied Sci .2006;48 ( l):23-29 .
3. Executive Sunrmtr!, Global Strategy for the Diagnosis,Management, and prevention of COPD; http:llwww.goldcopd.com, updated 2005, Last accessed on 2005.
4. Bames P J. Mediators of chronic obstructive pulmonary
disease. Phannacol Rev. 2004;56(a): 515-548.5. Reilly J J, Silvennan E K, Shapiro S D. Chronic Obstructive
Pulmonay Disease. In: Harrison's Principles of internal
medicine, vol 2,16* edn., Kasper D I, Braunwald E, FauciA
Biomedicine - VoL 33 No. 4: 2013
Benazeer Jadhav et aL: Evoluation of totaf,.......... patients
S, Hauser S L, Longo D I, Jameson J L, editors, McGrawHill, New York City ; 2005: I 548- 1552.
6. Rufino R and Lapa DeSilva J R. Cellular and biochemicalbasis of chronic obstnrctive pulmonary disease. J B Ras
Pneumol. 200 6; 32(24): I -8.7. Kelly F J. Vitamins and respiratory disease: antioxidant
micronutrients in puhnonary health and disease. Proc NutrSoc. 2005; 64(4): 510-526.
8. Oudijk E J, Lammers J W and Koenderman L. Systemicinflammation in chronic obstnrctive pulmonary disease. EurRespir J .. 2003 ; Suppl; 46: 5s- I 3s.
9. Van Eeden S 4 Yeung A, Qtrinlam K and Hogg J C.
Systemic response to ambient particulate matter: relevance
to chronic obstructive pulmonary disease. Proc Am ThoracSoc. 2005;2(l):61-67 .
10. GadekJE, Fells GA, ZirnmemanRlandCrystalRc. Roleof connective tissue proteases in the pathogenesis ofchronicinflammatory lung disease. Environ Health Perspect. 1984;55:297-306.
11. Gadek J E and Pacht E R. Pathogenesis of hereditaryemphysema and replacement therapy for alpha l -antitrypsindeficiency Insight into the more common forms ofemphysema. Chest. 1996; I I 0(6/Suppl) : 2485-2505.
12. Kolleck I, Sinha P and Riistow B. Vitamin E as an
antioxidant ofthe lung: mechanisms ofvitaminE deliverytoalveolar tlpe tr cells. Am J Respir Crit Care Med. 2002;166(t2Pt2):562-66.
13. Schiinemann H J, Grant B J, Freudenheim I L, Muti RBrowne R W, Drake J A, Klocke R A, Trevisan M. Therelation of sertrm levels of antioxidant vitamins C and E,
retinol and carotenoids with pulmonary firnction in the
general population. Am J Respir Crit Care Med. 2001;163(s): 1246-t2ss.
52s
14. Kluchov6 Z,Pefr6sov6 D, Joppa P, DorkovilZ and Tk6coviR. The association between oxidative stress and obstructive
' ltrng impairment inpatients with COPD. Physiol Res. 2007;56 (1): 5l-56.
15. Baker H and Frank O. Clinical vitaminology, methods and
interpritatiorxr. Interscience hrblishers, John Wiley and
Sons rnc.r NewYork; I 968; 172.16. Raghunath Rai, ffid Phadke M. Plasma anti protease status
in different respiratory disorders. Ind J Clin Biochem 2006;2t(2): t6tltil.
17. Kalsheker N and Morgan K. Molecular biology andrespiratory disease The alpha 1 antitlpsin gene and
chronic lung disease. Thorax. I 990; 45( I 0): 7 59-7 64.18. Sayyad A K Deshpande K H, Suryakar A N, Ankush R D
and IGtkam RV. Oxidative stress & senrm al-Antifiypsinin smokers. Ind J Clin Biochem. 2008; B @):37 5-377 .
19. Somayajulu G L, Raja R D and Reddy P P. Senrm ol-Antitrypsin in smokers & non smokers. Ind J Clin Biochem.t996;11(l): 70-72.
20. Moreno J J and Pryor W A. Inactivation of alphalproteinase inhibitor by peroxpitrite. Chem. Res. Toxicol.1992;s (3): 42s43t.
21. Mornex J R Chytil-Weir A, Martinet Y, Cotrfirey M,LeCocq J P and Crystal R G. Expression of the alpha-lantitypsin gene in mononuclear phagocytes of normal and
alpha-l-antitlpsin deficient individuals. J Clin Invest.1986; 77 (6): t9s2-1961.
Z2.Pacht E & Ikseki H, Mohammed J R, Cornwell D G and
Davis W B. Deficiency of vitamin E in the alveolar fluid ofcigarette smokers Influence on alveolar macrophage
cytotoxicity. J Clin Invest. I 9 86; 7 7 (3): 7 89 -7 9 6.
tt wtv. bi o m e di cin e o n lin e. o r g Biomedicine - YoL 33 No. 4: 2013
Related Documents











