REGULAR ARTICLE Evaluation of the automated coagulation analyzer SysmexR CA-7000 Florence Fischer, Anny Appert-Flory, Didier Jambou, Pierre Toulon * De´partementdTHe´matologie, CHU, Ho ˆpital de Cimiez, 4 avenue de la Reine Victoria, BP 1179, F-06003 Nice Cedex, France Received 1 February 2005; received in revised form 18 April 2005; accepted 6 June 2005 Available online 10 August 2005 Abstract The SysmexR CA-7000 is a fully automated multiparameter hemostasis analyzer equipped with a photo-optical clot detection unit and a cap-piercing system. It is designed to perform coagulation tests as well as chromogenic and immunologic assays. It was evaluated in a coagulation laboratory of a university hospital with respect to its technical characteristics in the determination of routine coagulation (prothrombin time, activated partial thromboplastin time, fibrinogen and single coagulation factors), chromogenic (antithrombin, and anti-FXa activity) and immunologic assays (von Willebrand factor). The intra-assay and inter-assay coefficients of variation (CV) were below 5% for most parameters both in the normal and in the pathological range (exceptions: intra-assay CV = 5.2% for the fibrinogen and 5.1% for antithrombin in the low range of concentrations; and inter-assay CV = 5.7% and 7.2% for clotting factors V and VII levels in the normal ranges, and in the range from 6.1% to 7.8% for anti-FXa activity). No significant interference could be demonstrated with hemolytic and icteric samples as demonstrated by results similar to those obtained using a mechanical clot detection-based analyzer (STAR). No carryover was detected in alternating measurements of heparinized (1.0 IU/mL unfractionated heparin) and normal plasma samples. The results of the different coagulation, chromogenic and immunologic assays obtained with the CA-7000 analyzer were well correlated with those obtained on the STAR analyzer (r in the range from 0.885 to 0.990). Our results demonstrated that using the CA-7000 analyzer, routine coagulation testing can be performed with satisfactory precision and the same applied to more specialized and specific tests such as single factor activity or antigen concentration. D 2005 Elsevier Ltd. All rights reserved. 0049-3848/$ - see front matter D 2005 Elsevier Ltd. All rights reserved. doi:10.1016/j.thromres.2005.06.012 Abbreviations: APTT, activated partial thromboplastin time; AT, antithrombin; CV, coefficient of variation; INR, international normalized ratio; PT, prothrombin time; vWF:Ag, von Willebrand factor antigen. * Corresponding author. Tel.: +33 4 92 03 42 07; fax: +33 4 92 03 42 12. E-mail address: [email protected] (P. Toulon). KEYWORDS Analyzer; Coagulation; Evaluation; SysmexR CA-7000 Thrombosis Research (2006) 117, 721 — 729 intl.elsevierhealth.com/journals/thre

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
intl.elsevierhealth.com/journals/thre
REGULAR ARTICLE
Evaluation of the automated coagulation analyzerSysmexR CA-7000
Florence Fischer, Anny Appert-Flory, Didier Jambou, Pierre Toulon*
Departement dTHematologie, CHU, Hopital de Cimiez, 4 avenue de la Reine Victoria, BP 1179,F-06003 Nice Cedex, France
Received 1 February 2005; received in revised form 18 April 2005; accepted 6 June 2005Available online 10 August 2005
0049-3848/$ - see front matter D 200doi:10.1016/j.thromres.2005.06.012
Abbreviations: APTT, activated panormalized ratio; PT, prothrombin tim* Corresponding author. Tel.: +33 4 9E-mail address: toulon.p@chu-nice
KEYWORDSAnalyzer;Coagulation;Evaluation;SysmexR CA-7000
Abstract The SysmexR CA-7000 is a fully automated multiparameter hemostasisanalyzer equipped with a photo-optical clot detection unit and a cap-piercingsystem. It is designed to perform coagulation tests as well as chromogenic andimmunologic assays. It was evaluated in a coagulation laboratory of a universityhospital with respect to its technical characteristics in the determination of routinecoagulation (prothrombin time, activated partial thromboplastin time, fibrinogenand single coagulation factors), chromogenic (antithrombin, and anti-FXa activity)and immunologic assays (von Willebrand factor). The intra-assay and inter-assaycoefficients of variation (CV) were below 5% for most parameters both in the normaland in the pathological range (exceptions: intra-assay CV=5.2% for the fibrinogenand 5.1% for antithrombin in the low range of concentrations; and inter-assayCV=5.7% and 7.2% for clotting factors V and VII levels in the normal ranges, and inthe range from 6.1% to 7.8% for anti-FXa activity). No significant interference couldbe demonstrated with hemolytic and icteric samples as demonstrated by resultssimilar to those obtained using a mechanical clot detection-based analyzer (STAR).No carryover was detected in alternating measurements of heparinized (1.0 IU/mLunfractionated heparin) and normal plasma samples. The results of the differentcoagulation, chromogenic and immunologic assays obtained with the CA-7000analyzer were well correlated with those obtained on the STAR analyzer (r in therange from 0.885 to 0.990). Our results demonstrated that using the CA-7000analyzer, routine coagulation testing can be performed with satisfactory precisionand the same applied to more specialized and specific tests such as single factoractivity or antigen concentration.D 2005 Elsevier Ltd. All rights reserved.
Thrombosis Research (2006) 117, 721—729
5 Elsevier Ltd. All rights reserved.
rtial thromboplastin time; AT, antithrombin; CV, coefficient of variation; INR, internationale; vWF:Ag, von Willebrand factor antigen.2 03 42 07; fax: +33 4 92 03 42 12..fr (P. Toulon).

F. Fischer et al.722
Introduction
The increasing coagulation tests volume and theeconomical pressure for tight personal andreagents budgets have raised interest in automatedcoagulation analyzers [1]. The current generationof coagulation analyzers is fully automated. Theircapabilities include primary tube sampling, cappiercing, automatic rerun, and dilution capabili-ties. They can perform basic coagulation tests suchas the prothrombin time (PT) or the activatedpartial thromboplastin time (APTT) as well as moresophisticated coagulation, chromogenic and immu-nologic assays [2,3] using smaller sample andreagent volumes than the manual techniques.
We, here, report an evaluation of the newanalyzer SysmexR CA-7000 in the routine practice.The evaluation addressed several issues includingease of operation, methodologies availability,reagent and patients sample on-board capabilities,ability to perform automatic dilution, and valida-tion of performances.
Materials and methods
Description of the SysmexR CA-7000analyzer
The SysmexR CA-7000 analyzer (TOA MedicalElectronics Co., Kobe, Japan and commercializedin France by Dade Behring, Paris la Defense) is afully automated stand-alone multiparameter coag-ulation analyzer with robotics capabilities. The clotdetection is made using photo-optical technology.Clotting, chromogenic and immunologic assays canbe performed in a true random fashion. Primarytubes are preceded to the instrument with the helpof samples racks (10 tubes per rack, with apossibility to mix closed and open tubes at onceon the same rack). A maximum of 100 samples canbe loaded at once with a true positive identifica-tion but without an auto-positioning of the barcodelabels. In addition, 5 positions on the sample partare devoted to STAT samples. The analyzer isequipped with a second-generation cap-piercingneedle for the transfer of plasma from the closedprimary tubes to secondary tubes located on asample rotor within the analyzer, from whichsamples are further transferred by 2 separatepipettors (one dedicated to single reagent-assaysand one to multiple reagents-assays). It could bementioned that the volume of plasma transferredfrom the primary tube to the secondary tube isdefined by the analyzer according to the originally
prescribed tests and the possibility to perform anyprogrammed reflex test. The intermediate tube isthen discarded when all of these tests are finished.So, if any rerun or additional test would berequired, the primary tube has to be inserted againin the analyzer with a new sampling procedurefrom the primary tube to a new secondary tube.
Using the software available at the time of theevaluation (n800-17), 56 different tests with 6programable steps can be adapted on the machine.There are a total of 58 positions available on 10racks for reagents and control samples which arepositively identified by barcode. Four racks (namedR1—R4) are dedicated to the starting reagents,three racks (named R5—R7) to intermediatereagents, one rack (named F) to the single-factordeficient plasmas and two racks (named C1 and C2)to control and standard plasma samples. Thenumber of positions available are different on eachrack (n =5, 6, or 8) as well as the volume ofaccepted vials (5, 15, or 50 mL). Fourteen of thesepositions are under constant magnetic stirringagitation. All are maintained at +12 8C. In addition,buffers and wash solution are displayed in acarrousel inside the analyzer. Five pipettors areavailable for the distribution of reagents i.e. onefor the distribution of factor-deficient plasmas, one(heated) for intermediate reagents, and three (twoheated) for the starting reagents that are specificfor thromboplastin and APTT reagent. The analyzeris totally open and convenient barcode printingfacilities are provided allowing positive identifica-tion of reagents other than those from DadeBehring. The instrument has the software capabil-ities for automatic reflex testing and is able to runmultiple assays at various dilutions simultaneouslywith an on-screen presentation of factor parallel-ism testing. The LIS interface is based on the bi-directional host-query-ASTM protocol. Finally, themaintenance is usually limited to a daily automaticprocedure which lasts 4 min and does not requirethe presence of a technician. In the case of highactivity, it is recommended by the manufacturer toproceed twice a day.
Evaluated samples
The lyophilized plasma samples Coag Norm andCoag Path were from Diagnostica Stago (Asnieres,France). In addition, plasma samples referred tothe laboratory for routine coagulation testing werealso evaluated. Venous blood was collected intoevacuated tubes containing 0.128 M sodium citrate(1 vol./9 vol.) (Vacutainer, Becton-Dickinson, LePont de Claix, France). At the time of the study,this citrate concentration was still widely used

Evaluation of the automated coagulation analyzer SysmexR CA-7000 723
despite international recommendations to use the0.109 M sodium citrate concentration [4]. Plasmawas obtained by centrifugation (�2) at 2500 �gand +12 8C for 15 min and was stored frozen inaliquots at �80 8C until evaluated.
Reagents and assay procedures
The reagents and the calibrators (brand name andmanufacturer) used in the present study are de-tailed in Table 1, as well as the tests methodology.All assays were performed according to the manu-facturer specifications and the standard laboratorymethods. Prothrombin time (PT) was initiated byadding 100 AL of a thromboplastin solution to 50 AL37 8C-prewarmed plasma sample. Activated partialthromboplastin time (APTT) was initiated by adding50 AL of a 0.025 mol/L calcium chloride solution to amixture of 50 AL APTTreagent and 50 AL plasma thatwas incubated at 37 8C for 240 s. Two different APTTreagents were evaluated using the same assayprocedure on the CA-7000, that differed from thenature of the activator i.e. micronized silica forAPTT-1 and kaolin for APTT-2. Fibrinogen wasmeasured according to Clauss [5]. For clottingfactor V (FV) and factor VII (FVII) measurement,50 AL of FV-depleted (or FVII-depleted) plasma wasadded to 50 AL of plasma diluted 1:10 in the Owren-Koller buffer (Diagnostica Stago). After a 240-sincubation at 37 8C, final measurement was takenafter the addition of 100 AL of PT reagent. For themeasurement of clotting factor VIII (FVIII), 50 AL ofFVIII-depleted plasma was added to 50 AL of plasmadiluted 1:10 in Owren-Koller buffer and 50 AL ofAPTT reagent (CK Prest). After a 240-s incubation at37 8C, final measurement was taken after theaddition of 50 AL of a 0.025 mol/L calcium chloridesolution. The anti-activated factor X (anti-FXa)activity was measured by adding 50 AL of plasmadiluted 1 :2 in a 0.025 mol/L sodium chloride
Table 1 Reagents and calibrators used in hemostasis anal
Test Reagent (Manufacturer) Calibra
PT Neoplastine CI10 (Diagnostica Stago) UnicaliAPTT-1 PTT automate (Diagnostica Stago Non-apAPTT-2 CK Prest (Diagnostica Stago) Non-apFibrinogen Fibrinogen 5 (Diagnostica Stago) UnicaliFactor V FV deficient (Diagnostica Stago) Standa
Neoplastin CI10 (Diagnostica Stago)Factor VII FVII deficient (Diagnostica Stago) Standa
Neoplastine CI10 (Diagnostica Stago)Factor VIII Hemolab Cofac VIII (BioMerieux) Standa
CK Prest (Diagnostica Stago)Anti-FXa activity Chromopep Heparin 6 (Biogenic) HeparipAntithrombin Stachrom ATIII (Diagnostica Stago) CaliplavWF:Ag Liatest vWF (Diagnostica Stago) VWF ca
solution into 125 AL of a 2.5 mg/mL chromogenicsubstrate (pNAPEP 1032) solution that was specificfor FXa. After a 240-s incubation at 37 8C, theoptical density was recorded at 405 nm after adding125 AL of a 2.5 Ag/mL FXa solution. The antithrom-bin (AT) activity was assayed by adding 100 AL of an11.3 nKat/mL thrombin solution into 100 AL ofplasma diluted 1:20 in Owren-Koller buffer. After a60-s incubation at 37 8C, the optical density wasrecorded at 405 nm after adding 100 AL of a 1.4Amol/mL chromogenic substrate (CBS 61.50) solu-tion that was specific for thrombin. The von Will-ebrand factor antigen (vWF:Ag) concentration wasmeasured by adding 150 AL of a suspension of latexmicroparticules sensitized by antibodies againstvWF into 150 AL of plasma diluted 1:3 in Owren-Koller buffer that was incubated at +37 8C for 240 s.
Clotting times for FV, FVII, FVIII, and fibrinogenwere plotted on specific reference curves thatwere generated by the analyzer, allowing thecalculation of corresponding analyte concentra-tion. Anti-FXa activity and AT activity assays usedchromogenic methods and similarly, the change inoptical density measured at 405 nm was plotted ona specific reference curve that was generated bythe instrument. The same applied to the vWF:Agconcentration that was evaluated using an immuno-turbidimetric assay. In all assay procedure, anautomatic dilution was programmed in the casesof levels outside the calibration curve.
Evaluation procedure
The intra-assay precision was determined forcoagulation assays (PT, APTT, fibrinogen, FV, FVII,and FVIII), chromogenic (anti-FXa activity and AT)and immunologic assays (vWF:Ag) by evaluatingpools of fresh plasma samples in the normal and inthe pathological range at least 10 times consecu-tively (in the same run). The inter-assay precision
yzer comparison studies
tor (Manufacturer) Methodology
brator (Diagnostica Stago) Coagulationplicable Coagulationplicable Coagulationbrator (Diagnostica Stago) Coagulationrd human plasma ORKL (Dade Behring) Coagulation
rd human plasma ORKL (Dade Behring) Coagulation
rd human plasma ORKL (Dade Behring) Coagulation
ep standard (Biopep) Chromogenicsma (BioMerieux) Chromogeniclibrator (Diagnostica Stago) Immuno-turbidimetry

F. Fischer et al.724
was determined by evaluating frozen and lyophi-lized plasma samples every day for at least 10consecutive days (for most parameters). Thecarryover was investigated by measuring APTTalternatively in normal plasma and normal plasmaspiked with heparin up to 1.0 IU/mL (finalconcentration) 10 times consecutively. Finally,the results of different assays obtained on theCA-7000 were compared to that obtained using thesame reagents on the STAR analyzer (DiagnosticaStago, Asnieres, France). The aim of the latterinvestigation was to compare values obtained byusing photo-optical clot detection (CA-7000) withthose obtained by using mechanical clot detection(STAR) particularly in plasmas with abnormaloptical characteristics such as haemolytic andicteric samples.
Statistical analysis
Results were expressed as the mean values withstandard deviations when the data were normallydistributed. Otherwise, results were expressed asthe median values with ranges. The Student t-test(in the case of normally distributed data), theWilcoxon’s matched pairs T-test and the Spear-man’s coefficient of rank correlation (both in thecase of non-normally distributed data) were usedwhen required. Comparison of the results obtainedon the two instruments was made according toBland and Altman [6].
Results
Intra-assay precision
As shown in Table 2, the intra-assay coefficients ofvariation (CV) were below 5% for most parametersboth in the normal and in the pathological range
Table 2 Intra-assay precision of the CA-7000 analyzer
Test Unit Fres
PT (%) % 70.8APTT-1 (PTT automate) s 38.0APTT-2 (CK Prest) s 43.0Fibrinogen g/L 3.10Factor V % NDFactor VII % NDFactor VIII % NDAnti-FXa activity* IU/mL 0.55Antithrombin % NDvWF:Ag % 69.2
The same lyophilized or frozen normal or abnormal sample was evalgiven as the mean values with standard deviation with the coeffici
ND: not done. *: 2 plasmas containing different anti-Xa levels were
except for the fibrinogen and AT in the low range ofconcentrations (5.2% and 5.1% respectively).
Inter-assay precision
As shown in Table 3, the inter-assay CV were below5% for most parameters measured in lyophilizedplasma samples both in the normal and in thepathological range, except for FV and FVII levels inthe normal ranges (5.7% and 7.2% respectively),and for anti-FXa activity (in the range from 6.1% to7.8%). The results obtained in frozen samples wereof the same magnitude order for PT and fibrinogen,whereas higher CVs were obtained for APTT i.e.7.8% for a normal plasma and 5.1% for an abnormalplasma.
Carryover
To evaluate the amount of carryover of heparin,APTT-1 was measured in a normal plasma runbefore and after a plasma sample spiked withunfractionated heparin (1.0 IU/mL final concentra-tion). No prolongation of APTT of normal plasmawas detected in alternating measurements of thesetwo plasma samples 10 times consecutively.
Throughput
When the single test mode was chosen, 257 PTweremeasured per hour. When the panel mode (PT induplicate and APTT+fibrinogen in single determi-nation) was selectioned, the throughput was 80samples per hour corresponding to 318 tests perhour.
Correlation with the STAR analyzer
The results of the different clotting, chromogenicand immunologic assays obtained with the CA-
h normal plasma Fresh abnormal plasma
F0.8 (1.1%); n =11 39F0.3 (0.8%); n =11F0.4 (1.1%); n =11 61.9F0.7 (1.1%); n =11F0.4 (0.9%); n =11 NDF0.05 (1.6%); n =11 1.75F0.09 (5.2%); n =10
64.3F2.0 (3.1%); n =1155.7F1.4 (2.6%); n =1161.3F0.9 (1.4%); n =10
F0.02 (3%); n =11 0.86F0.01 (1.6%); n =1166.3F3.4 (5.1%); n =21
F0.6 (0.9%); n =13 ND
uated n times simultaneously (in the same run). The results areent of variation (in percent).
investigated.
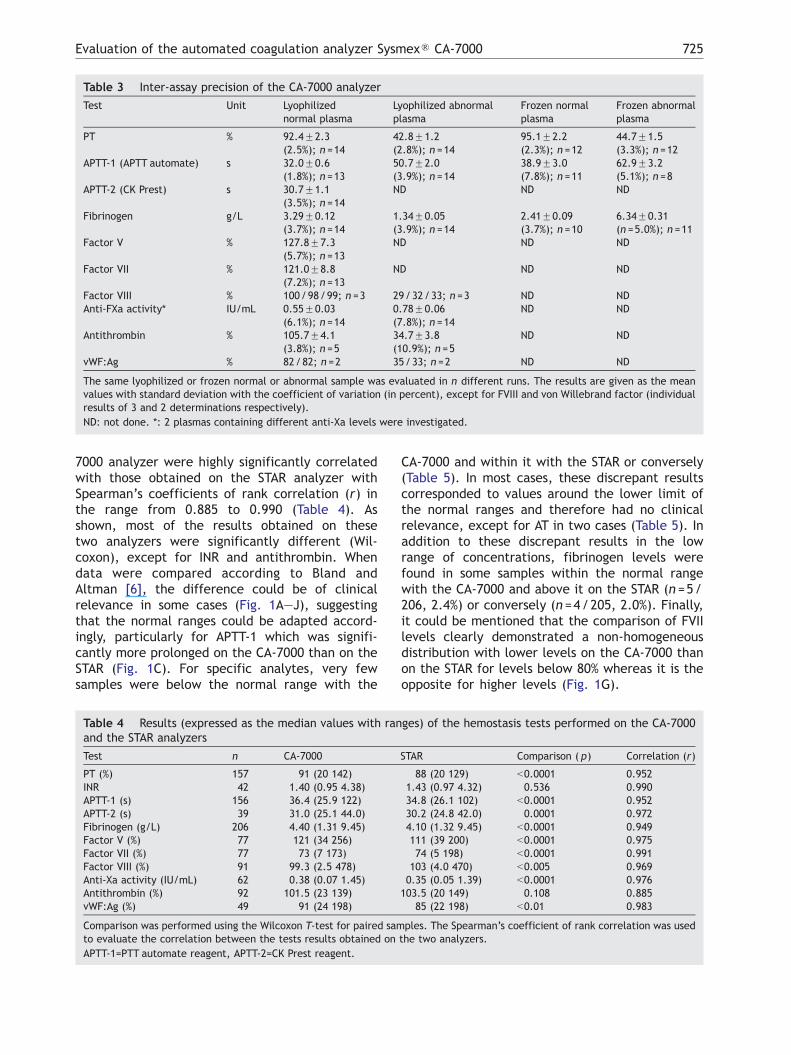
Table 3 Inter-assay precision of the CA-7000 analyzer
Test Unit Lyophilizednormal plasma
Lyophilized abnormalplasma
Frozen normalplasma
Frozen abnormalplasma
PT % 92.4F2.3(2.5%); n =14
42.8F1.2(2.8%); n =14
95.1F2.2(2.3%); n =12
44.7F1.5(3.3%); n =12
APTT-1 (APTT automate) s 32.0F0.6(1.8%); n =13
50.7F2.0(3.9%); n =14
38.9F3.0(7.8%); n =11
62.9F3.2(5.1%); n =8
APTT-2 (CK Prest) s 30.7F1.1(3.5%); n =14
ND ND ND
Fibrinogen g/L 3.29F0.12(3.7%); n =14
1.34F0.05(3.9%); n =14
2.41F0.09(3.7%); n =10
6.34F0.31(n =5.0%); n =11
Factor V % 127.8F7.3(5.7%); n =13
ND ND ND
Factor VII % 121.0F8.8(7.2%); n =13
ND ND ND
Factor VIII % 100/98/99; n =3 29/32/33; n =3 ND NDAnti-FXa activity* IU/mL 0.55F0.03
(6.1%); n =140.78F0.06(7.8%); n =14
ND ND
Antithrombin % 105.7F4.1(3.8%); n =5
34.7F3.8(10.9%); n =5
ND ND
vWF:Ag % 82/82; n =2 35/33; n =2 ND ND
The same lyophilized or frozen normal or abnormal sample was evaluated in n different runs. The results are given as the meanvalues with standard deviation with the coefficient of variation (in percent), except for FVIII and von Willebrand factor (individualresults of 3 and 2 determinations respectively).
ND: not done. *: 2 plasmas containing different anti-Xa levels were investigated.
Evaluation of the automated coagulation analyzer SysmexR CA-7000 725
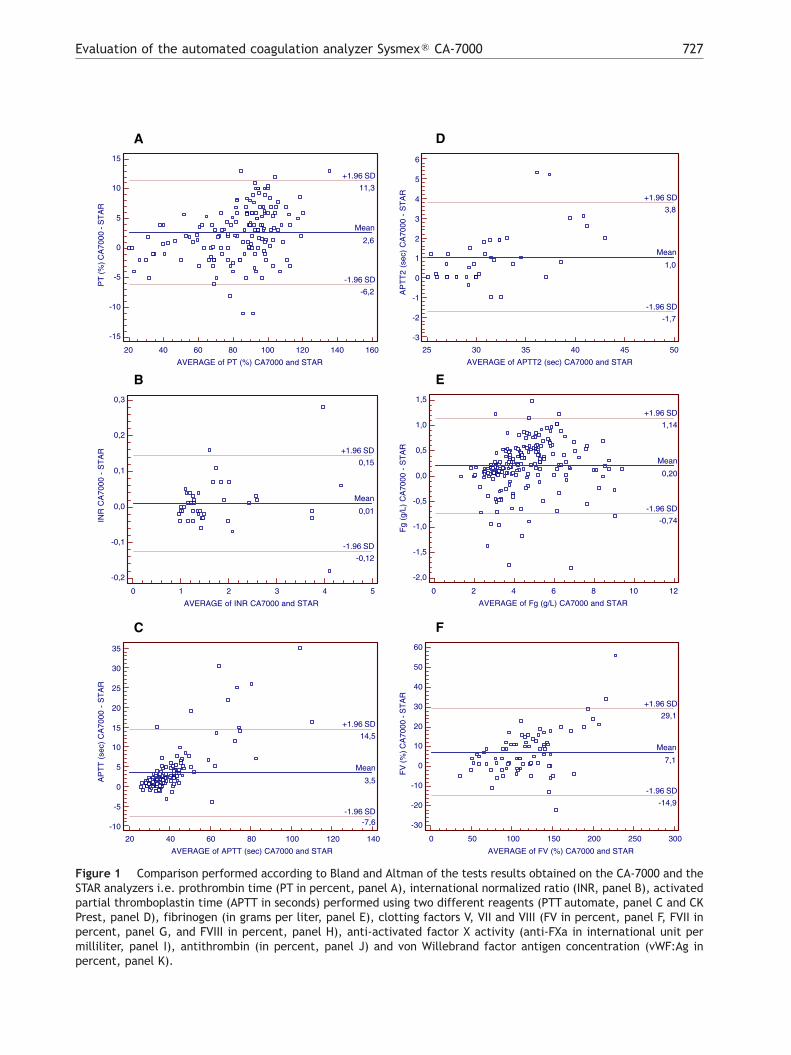
7000 analyzer were highly significantly correlatedwith those obtained on the STAR analyzer withSpearman’s coefficients of rank correlation (r) inthe range from 0.885 to 0.990 (Table 4). Asshown, most of the results obtained on thesetwo analyzers were significantly different (Wil-coxon), except for INR and antithrombin. Whendata were compared according to Bland andAltman [6], the difference could be of clinicalrelevance in some cases (Fig. 1A—J), suggestingthat the normal ranges could be adapted accord-ingly, particularly for APTT-1 which was signifi-cantly more prolonged on the CA-7000 than on theSTAR (Fig. 1C). For specific analytes, very fewsamples were below the normal range with the
Table 4 Results (expressed as the median values with ranand the STAR analyzers
Test n CA-7000
PT (%) 157 91 (20 142)INR 42 1.40 (0.95 4.38)APTT-1 (s) 156 36.4 (25.9 122)APTT-2 (s) 39 31.0 (25.1 44.0)Fibrinogen (g/L) 206 4.40 (1.31 9.45)Factor V (%) 77 121 (34 256)Factor VII (%) 77 73 (7 173)Factor VIII (%) 91 99.3 (2.5 478)Anti-Xa activity (IU/mL) 62 0.38 (0.07 1.45)Antithrombin (%) 92 101.5 (23 139)vWF:Ag (%) 49 91 (24 198)
Comparison was performed using the Wilcoxon T-test for paired samto evaluate the correlation between the tests results obtained on
APTT-1=PTT automate reagent, APTT-2=CK Prest reagent.
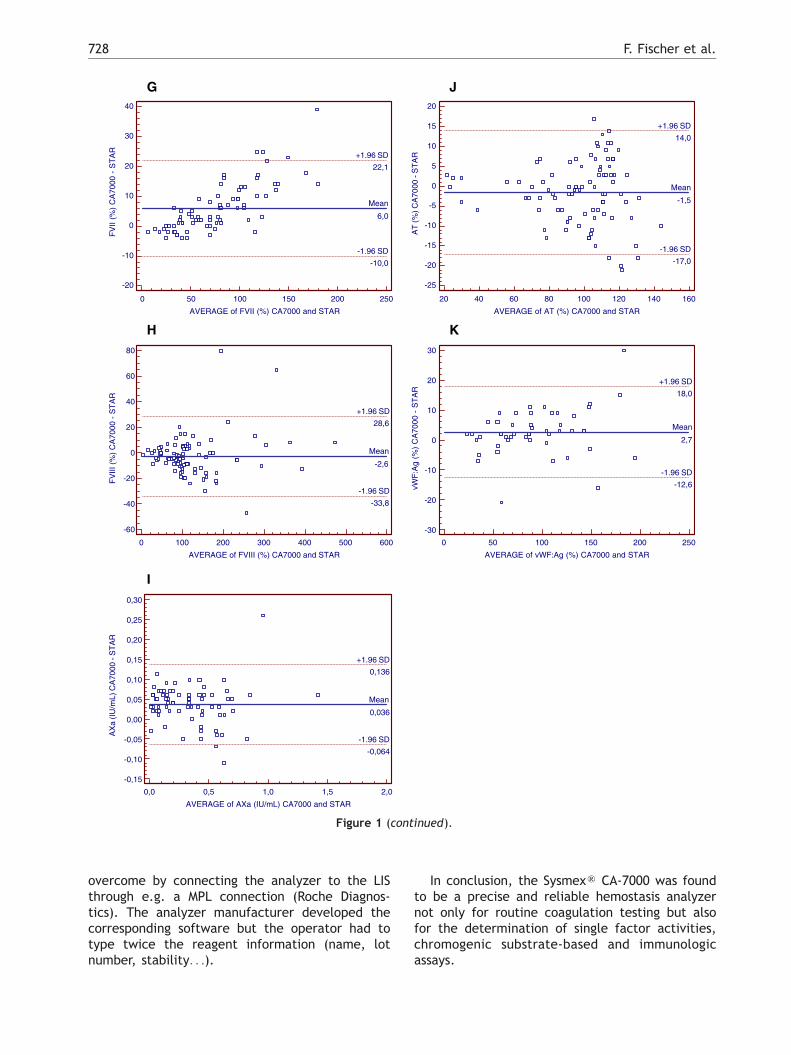
CA-7000 and within it with the STAR or conversely(Table 5). In most cases, these discrepant resultscorresponded to values around the lower limit ofthe normal ranges and therefore had no clinicalrelevance, except for AT in two cases (Table 5). Inaddition to these discrepant results in the lowrange of concentrations, fibrinogen levels werefound in some samples within the normal rangewith the CA-7000 and above it on the STAR (n =5/206, 2.4%) or conversely (n =4/205, 2.0%). Finally,it could be mentioned that the comparison of FVIIlevels clearly demonstrated a non-homogeneousdistribution with lower levels on the CA-7000 thanon the STAR for levels below 80% whereas it is theopposite for higher levels (Fig. 1G).
ges) of the hemostasis tests performed on the CA-7000
STAR Comparison ( p) Correlation (r)
88 (20 129) b0.0001 0.9521.43 (0.97 4.32) 0.536 0.99034.8 (26.1 102) b0.0001 0.95230.2 (24.8 42.0) 0.0001 0.9724.10 (1.32 9.45) b0.0001 0.949111 (39 200) b0.0001 0.97574 (5 198) b0.0001 0.991
103 (4.0 470) b0.005 0.9690.35 (0.05 1.39) b0.0001 0.976
103.5 (20 149) 0.108 0.88585 (22 198) b0.01 0.983
ples. The Spearman’s coefficient of rank correlation was usedthe two analyzers.
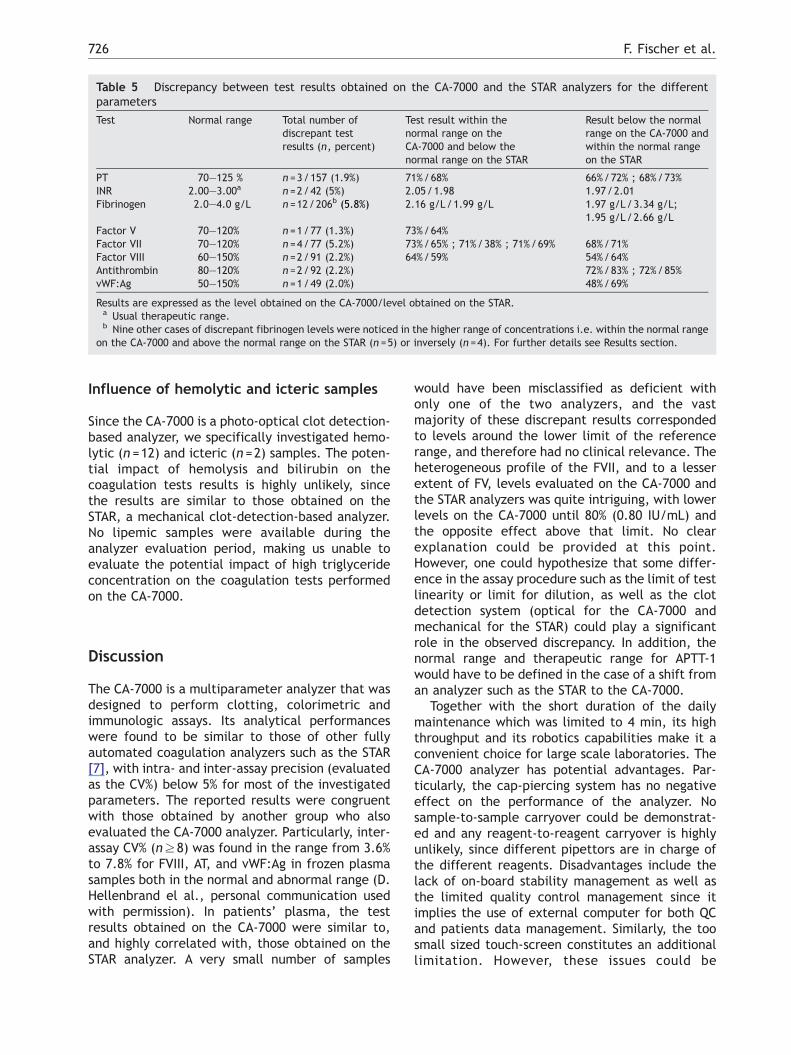
Table 5 Discrepancy between test results obtained on the CA-7000 and the STAR analyzers for the differentparameters
Test Normal range Total number ofdiscrepant testresults (n, percent)
Test result within thenormal range on theCA-7000 and below thenormal range on the STAR
Result below the normalrange on the CA-7000 andwithin the normal rangeon the STAR
PT 70—125 % n =3/157 (1.9%) 71%/68% 66%/72% ; 68%/73%INR 2.00—3.00a n =2/42 (5%) 2.05/1.98 1.97/2.01Fibrinogen 2.0—4.0 g/L n =12/206b (5.8%) 2.16 g/L/1.99 g/L 1.97 g/L/3.34 g/L;
1.95 g/L/2.66 g/LFactor V 70—120% n =1/77 (1.3%) 73%/64%Factor VII 70—120% n =4/77 (5.2%) 73%/65% ; 71%/38% ; 71%/69% 68%/71%Factor VIII 60—150% n =2/91 (2.2%) 64%/59% 54%/64%Antithrombin 80—120% n =2/92 (2.2%) 72%/83% ; 72%/85%vWF:Ag 50—150% n =1/49 (2.0%) 48%/69%
Results are expressed as the level obtained on the CA-7000/level obtained on the STAR.a Usual therapeutic range.b Nine other cases of discrepant fibrinogen levels were noticed in the higher range of concentrations i.e. within the normal range
on the CA-7000 and above the normal range on the STAR (n =5) or inversely (n =4). For further details see Results section.
F. Fischer et al.726
Influence of hemolytic and icteric samples
Since the CA-7000 is a photo-optical clot detection-based analyzer, we specifically investigated hemo-lytic (n =12) and icteric (n =2) samples. The poten-tial impact of hemolysis and bilirubin on thecoagulation tests results is highly unlikely, sincethe results are similar to those obtained on theSTAR, a mechanical clot-detection-based analyzer.No lipemic samples were available during theanalyzer evaluation period, making us unable toevaluate the potential impact of high triglycerideconcentration on the coagulation tests performedon the CA-7000.
Discussion
The CA-7000 is a multiparameter analyzer that wasdesigned to perform clotting, colorimetric andimmunologic assays. Its analytical performanceswere found to be similar to those of other fullyautomated coagulation analyzers such as the STAR[7], with intra- and inter-assay precision (evaluatedas the CV%) below 5% for most of the investigatedparameters. The reported results were congruentwith those obtained by another group who alsoevaluated the CA-7000 analyzer. Particularly, inter-assay CV% (nz8) was found in the range from 3.6%to 7.8% for FVIII, AT, and vWF:Ag in frozen plasmasamples both in the normal and abnormal range (D.Hellenbrand el al., personal communication usedwith permission). In patients’ plasma, the testresults obtained on the CA-7000 were similar to,and highly correlated with, those obtained on theSTAR analyzer. A very small number of samples
would have been misclassified as deficient withonly one of the two analyzers, and the vastmajority of these discrepant results correspondedto levels around the lower limit of the referencerange, and therefore had no clinical relevance. Theheterogeneous profile of the FVII, and to a lesserextent of FV, levels evaluated on the CA-7000 andthe STAR analyzers was quite intriguing, with lowerlevels on the CA-7000 until 80% (0.80 IU/mL) andthe opposite effect above that limit. No clearexplanation could be provided at this point.However, one could hypothesize that some differ-ence in the assay procedure such as the limit of testlinearity or limit for dilution, as well as the clotdetection system (optical for the CA-7000 andmechanical for the STAR) could play a significantrole in the observed discrepancy. In addition, thenormal range and therapeutic range for APTT-1would have to be defined in the case of a shift froman analyzer such as the STAR to the CA-7000.
Together with the short duration of the dailymaintenance which was limited to 4 min, its highthroughput and its robotics capabilities make it aconvenient choice for large scale laboratories. TheCA-7000 analyzer has potential advantages. Par-ticularly, the cap-piercing system has no negativeeffect on the performance of the analyzer. Nosample-to-sample carryover could be demonstrat-ed and any reagent-to-reagent carryover is highlyunlikely, since different pipettors are in charge ofthe different reagents. Disadvantages include thelack of on-board stability management as well asthe limited quality control management since itimplies the use of external computer for both QCand patients data management. Similarly, the toosmall sized touch-screen constitutes an additionallimitation. However, these issues could be
A
20 40 60 80 100 120 140 160
AVERAGE of PT (%) CA7000 and STAR
15
10
5
0
-5
-10
-15
PT
(%) C
A70
00 -
ST
AR
Mean
2,6
-1.96 SD
-6,2
+1.96 SD
11,3
B
0 1 2 3 4 5
AVERAGE of INR CA7000 and STAR
0,3
0,2
0,1
0,0
-0,1
-0,2
INR
CA
7000
- S
TA
R
Mean
0,01
-1.96 SD
-0,12
+1.96 SD
0,15
C
20 40 60 80 100 120 140
AVERAGE of APTT (sec) CA7000 and STAR
35
30
25
20
15
10
5
0
-5
-10
AP
TT
(se
c) C
A70
00 -
ST
AR
Mean
3,5
-1.96 SD-7,6
+1.96 SD
14,5
D
25 30 35 40 45 50
AVERAGE of APTT2 (sec) CA7000 and STAR
6
5
4
3
2
1
0
-1
-2
-3
AP
TT
2 (s
ec)
CA
7000
- S
TA
R
Mean
1,0
-1.96 SD
-1,7
+1.96 SD
3,8
E
0 2 4 6 8 10 12
AVERAGE of Fg (g/L) CA7000 and STAR
1,5
1,0
0,5
0,0
-0,5
-1,0
-1,5
-2,0
Fg
(g/L
) C
A70
00 -
ST
AR
Mean
0,20
-1.96 SD
-0,74
+1.96 SD
1,14
F
0 50 100 150 200 250 300
AVERAGE of FV (%) CA7000 and STAR
60
50
40
30
20
10
0
-10
-20
-30
FV
(%) C
A70
00 -
ST
AR
Mean
7,1
-1.96 SD
-14,9
+1.96 SD
29,1
Figure 1 Comparison performed according to Bland and Altman of the tests results obtained on the CA-7000 and theSTAR analyzers i.e. prothrombin time (PT in percent, panel A), international normalized ratio (INR, panel B), activatedpartial thromboplastin time (APTT in seconds) performed using two different reagents (PTT automate, panel C and CKPrest, panel D), fibrinogen (in grams per liter, panel E), clotting factors V, VII and VIII (FV in percent, panel F, FVII inpercent, panel G, and FVIII in percent, panel H), anti-activated factor X activity (anti-FXa in international unit permilliliter, panel I), antithrombin (in percent, panel J) and von Willebrand factor antigen concentration (vWF:Ag inpercent, panel K).
Evaluation of the automated coagulation analyzer SysmexR CA-7000 727
G
0 50 100 150 200 250
AVERAGE of FVII (%) CA7000 and STAR
40
30
20
10
0
-10
-20
FV
II (%
) C
A70
00 -
ST
AR
Mean
6,0
-1.96 SD
-10,0
+1.96 SD
22,1
H
0 100 200 300 400 500 600
AVERAGE of FVIII (%) CA7000 and STAR
80
60
40
20
0
-20
-40
-60
FV
III (
%)
CA
7000
- S
TA
R
Mean
-2,6
-1.96 SD
-33,8
+1.96 SD
28,6
I
0,0 0,5 1,0 1,5 2,0
AVERAGE of AXa (IU/mL) CA7000 and STAR
0,30
0,25
0,20
0,15
0,10
0,05
0,00
-0,05
-0,10
-0,15
AX
a (I
U/m
L) C
A70
00 -
ST
AR
Mean
0,036
-1.96 SD
-0,064
+1.96 SD
0,136
J
20 40 60 80 100 120 140 160
AVERAGE of AT (%) CA7000 and STAR
20
15
10
5
0
-5
-10
-15
-20
-25
AT
(%) C
A70
00 -
ST
AR
Mean
-1,5
-1.96 SD
-17,0
+1.96 SD
14,0
K
0 50 100 150 200 250
AVERAGE of vWF:Ag (%) CA7000 and STAR
30
20
10
0
-10
-20
-30
vWF
:Ag
(%)
CA
7000
- S
TA
R
Mean
2,7
-1.96 SD
-12,6
+1.96 SD
18,0
Figure 1 (continued).
F. Fischer et al.728
overcome by connecting the analyzer to the LISthrough e.g. a MPL connection (Roche Diagnos-tics). The analyzer manufacturer developed thecorresponding software but the operator had totype twice the reagent information (name, lotnumber, stability. . .).
In conclusion, the SysmexR CA-7000 was foundto be a precise and reliable hemostasis analyzernot only for routine coagulation testing but alsofor the determination of single factor activities,chromogenic substrate-based and immunologicassays.

Evaluation of the automated coagulation analyzer SysmexR CA-7000 729
Acknowledgements
The authors wish to thank D. Hellenbrand, R. vanOerle and K. Hamulyak (Department of Hematolo-gy, University Hospital, Maastricht, The Nether-lands) for allowing us to report their unpublishedresults. We are indebted to the technicians fromthe Department of Hematology (Hopital de Cimiez,Nice, France) for expert technical assistance duringthe analyzer evaluation.
References
[1] Walenga JM, Fareed J. Automation and quality control in thecoagulation laboratory. Clin Lab Med 1994;14:709–28.
[2] Aiach M, Leon M, Michaud A, Capron L. Adaptation ofsynthetic peptide substrate-based assays on a discreteanalyzer. Semin Thromb Hemost 1983;9:206–16.
[3] Amiral J, Adalbert B, Adam M. Application of enzymeimmunoassays to coagulation testing. Clin Chem 1994;30:1512–6.
[4] WHO. Guidelines for thromboplastin and plasma used tocontrol oral anticoagulant therapy. WHO Technical Reportseries 1999;889:64–93.
[5] Clauss A. Gerinnungsphysiologische Schnellmethode zurBestimmung des Fibrinogens. Acta Haematol 1957;17:237–46.
[6] Bland JM, Altman DJ. Statistical methods for assessingagreement between two methods of clinical measurement.Lancet 1986;1:307–10.
[7] Flanders MM, Crist R, Safapour S, Rodgers GM. Evaluation andperformance characteristics of the STA-R coagulation ana-lyzer. Clin Chem 2002;48:1622–4.
Related Documents











