ORIGINAL ARTICLE Evaluation of sFas in serum and follicular fluid during ovarian stimulation for assisted reproduction Ayman Nady Abdelmeged a, * , Yasser Ibrahim Ali b , Diaa Eldin Elmoghazi a , Mostafa Kamel Eissa a a Department of Obstetrics and Gynecology and Minia Infertility Research Unit, Minia University, Egypt b IVF Unit, Schleswig Holstein University, Germany Received 4 May 2010; accepted 22 December 2010 Available online 21 January 2011 KEYWORDS sFas; IVF; ICSI Abstract Objectives: To measure the level of sFas in serum and follicular fluid (FF) from infertile women undergoing exogenous gonadotropin stimulation as a part of IVF/ICSI cycles and to study its correlation with oocyte maturation, fertilization, and embryo quality. Materials and methods: Serum and FF samples were obtained from 55 patients at the time of trans- vaginal oocyte retrieval after ovulation induction for assisted reproduction. sFas levels in the serum and FF were measured in duplicate by a solid phase enzyme-linked immunosorbent assay (ELISA). E2 levels were measured by an enzyme immunoassay. Results: There was no statistically significant correlation between age and sFas levels in serum (p = 0.84, r = 0.35) or follicular fluid (p = 0.75, r = 0.36). It was observed that the levels of sFas in serum and FF varies with different patients’ diagnosis. There was a statistically significant increase in sFas levels in both serum (p = 0.023, r = 0.08) and FF (p = 0.014, r = 0.01) in patients with uterine causes of infertility (subseptate uterus and previ- ous myomectomy) compared with those having other causes of infertility. sFas were detected in low concentration in serum and FF in patients with male factor and idiopathic causes of infertility (Fig. 1). A positive correlation was found between the sFas levels in the serum and those in the FF (p = 0.01, r = 0.91) (Fig. 2). However, no correlation was found between the levels of sFas and * Corresponding author. Mobile: +20 0103622245. E-mail address: [email protected] (A.N. Abdelmeged). 1110-5690 Ó 2011 Middle East Fertility Society. Production and hosting by Elsevier B.V. All rights reserved. Peer review under responsibility of Middle East Fertility Society. doi:10.1016/j.mefs.2010.12.012 Production and hosting by Elsevier Middle East Fertility Society Journal (2011) 16, 50–55 Middle East Fertility Society Middle East Fertility Society Journal www.mefsjournal.com www.sciencedirect.com

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Middle East Fertility Society Journal (2011) 16, 50–55
Middle East Fertility Society
Middle East Fertility Society Journal
www.mefsjournal.comwww.sciencedirect.com
ORIGINAL ARTICLE
Evaluation of sFas in serum and follicular fluid
during ovarian stimulation for assisted reproduction
Ayman Nady Abdelmeged a,*, Yasser Ibrahim Ali b, Diaa Eldin Elmoghazi a,
Mostafa Kamel Eissa a
a Department of Obstetrics and Gynecology and Minia Infertility Research Unit, Minia University, Egyptb IVF Unit, Schleswig Holstein University, Germany
Received 4 May 2010; accepted 22 December 2010Available online 21 January 2011
*
E
11
ho
Pe
do
KEYWORDS
sFas;
IVF;
ICSI
Corresponding author. Mob
-mail address: elnadyayman70
10-5690 � 2011 Middle E
sting by Elsevier B.V. All rig
er review under responsibilit
i:10.1016/j.mefs.2010.12.012
Production and ho
ile: +20
74@yah
ast Ferti
hts reser
y of Mid
sting by E
Abstract Objectives: To measure the level of sFas in serum and follicular fluid (FF) from infertile
women undergoing exogenous gonadotropin stimulation as a part of IVF/ICSI cycles and to study
its correlation with oocyte maturation, fertilization, and embryo quality.
Materials and methods: Serum and FF samples were obtained from 55 patients at the time of trans-
vaginal oocyte retrieval after ovulation induction for assisted reproduction. sFas levels in the serum
and FF were measured in duplicate by a solid phase enzyme-linked immunosorbent assay (ELISA).
E2 levels were measured by an enzyme immunoassay.
Results: There was no statistically significant correlation between age and sFas levels in serum
(p= 0.84, r = �0.35) or follicular fluid (p= 0.75, r = �0.36).It was observed that the levels of sFas in serum and FF varies with different patients’ diagnosis.
There was a statistically significant increase in sFas levels in both serum (p= 0.023, r = 0.08) and
FF (p= 0.014, r = 0.01) in patients with uterine causes of infertility (subseptate uterus and previ-
ous myomectomy) compared with those having other causes of infertility. sFas were detected in low
concentration in serum and FF in patients with male factor and idiopathic causes of infertility
(Fig. 1).
A positive correlation was found between the sFas levels in the serum and those in the FF
(p= 0.01, r = 0.91) (Fig. 2). However, no correlation was found between the levels of sFas and
0103622245.
oo.com (A.N. Abdelmeged).
lity Society. Production and
ved.
dle East Fertility Society.
lsevier

Evaluation of sFas in serum and follicular fluid during ovarian stimulation 51
the levels of estradiol in the serum (p= 0.427, r= �0.03). There was a significant correlation
between the number of fertilized oocytes and the level of sFas in the serum (p= 0.013,
r = �0.42) (Fig. 3).There was no correlation between the number of fertilized oocytes and the level of sFas in FF
(p= 0.168, r = �0.40). However, a significant correlation between the levels of sFas in the serum
of pregnant (n= 11) and non-pregnant women (n= 44) was observed (p= 0.045, r = 0.90)
(Fig. 4).
Conclusions: A lower level of sFas in serum was associated with a higher pregnancy rates. This may
be attributed to the presence of good fertilized oocytes. The above phenomena may suggest that low
levels of sFas in serum may be associated with improved implantation of fertilized oocytes or may
prevent damage to the embryo. Lower levels of sFas seem to support embryo implantation.
� 2011 Middle East Fertility Society. Production and hosting by Elsevier B.V. All rights reserved.
1. Introduction
Follicular atresia is an important negatively selective degener-
ative process during mammalian ovarian follicular growth anddevelopment (1) and is believed to involve granulosa cell deathby apoptosis (2).
Human Fas, is a 45-kDa transmembrane glycoprotein of
325 amino acids with a signal sequence at the NH2-terminusand belongs to the tumour necrosis factor (TNF) family (3).FasL, with no signal sequence at the NH2-terminus, has a do-
main of hydrophobic amino acids in the middle of the mole-cule, indicating it is a type II membrane protein with itsCOOH-terminal region outside of the cell (4). When FasL
binds to Fas on the surface, apoptosis is initiated (5).Although several intracellular molecules including B-cell
lymphoma/leukemia 2 (Bcl-2) (6), Bcl-2 associated x protein
(Bax) (7), and cysteinyl-aspartate specific proteinases (Caspas-es) (8) have been shown to be directly involved in the regula-tion of this process, recent studies into the cellular andmolecular events leading to granulosa cell apoptosis have sug-
gested that death pathways mediated by Fas antigen may becentral in the induction of follicular atresia (9).
However, these studies did not examine the expression of
Fas during antral follicular development and failed to detectFas ligand in granulosa cells. As a result, information on dy-namic changes in Fas and Fas ligand protein expression during
follicular development and atresia remains to be investigated.Furthermore, many studies have been carried out into the
morphological and biochemical characteristics of atreticfollicles. These characteristics include detachment and degener-
ation of the granulosa cell layer (10), fragmentation of the basallamina (11), reduced DNA synthesis (12), decreased estrogenproduction and decreased gonadotropin binding (13).
Analysis of follicular fluid in combination with serum re-flects autocrine and paracrine factors regulating ovarian folli-culogenesis along with systemic endocrine dynamics (14).
Therefore, it is logic to assume that the level of the solubleapoptotic factors in serum and follicular fluid from womenundergoing IVF/ICSI cycles may have an implication on the
outcome of these cycles particularly oocyte maturation, fertil-ization, and embryo quality.
2. Aim of the work
To measure the level of sFas in serum and follicular fluid frominfertile women undergoing exogenous gonadotropin stimula-
tion as a part of IVF/ICSI cycles and to study its correla-tion with oocyte maturation, fertilization, and embryoquality.
3. Materials and methods
Women included in this study were recruited from those
attending IVF unit in Schleswig Holstein University betweenApril 2007 and May 2009. Written informed consent was ob-tained from each patient. Consent forms and protocols were
approved by the local Ethics Committee.Serum and FF samples were obtained from 55 patients at
the time of transvaginal oocyte retrieval after controlled ovar-
ian stimulation for in vitro fertilization (IVF), intracyto-plas-matic sperm injection (ICSI). The age of these patientsranges from 26 to 41 with a mean age of 35.56 years.
All patients underwent controlled ovarian stimulation with
a combination of GnRH agonist and recombinant (r) FSH,using a long protocol for IVF/ICSI treatment.
During the standard long protocol for pituitary suppression,
GnRH agonist (0.1 mg Decapeptyl; Ferring, Germany) wasadministered S.C. from day 21 of the previous cycle followedby FSH. On cycle day 3, 150 IU of daily S.C. injections with re-
combinant FSH (Follitropin, Gonal F; Serono, Germany) wasbegun.
Ovarian response was monitored by the serum E2 concen-
tration and measuring the diameter of developing follicles bytransvaginal ultrasonography.
Once the leading follicle reached P18 mm in diameter andthe level of 17-b estradiol was adequately increased (but still
less than 3000 pg/ml in the serum), 10,000 IU of hCG wasadministered intramuscularly.
Follicles were aspirated 36 h after administration of hCG.
On the day of oocyte retrieval, 5 ml blood was obtained froman antecubital vein, centrifuged for 15 min at speed of 800 · gat 5 �C, shock frozen and kept at �80 �C until assayed.
Follicular fluid was obtained from mature oocyte-bearingfollicles dealt with in the same way as blood samples, andstored at �80 �C until assayed.
3.1. Measurement of sFas in serum and follicular fluid
sFas levels in the serum and FF were measured in duplicate(the system was programmed to give the middle value) by a so-
lid phase enzyme-linked immunosorbent assay (ELISA) usingthe Quantikine sFas kit (R&D System Inc., Germany).
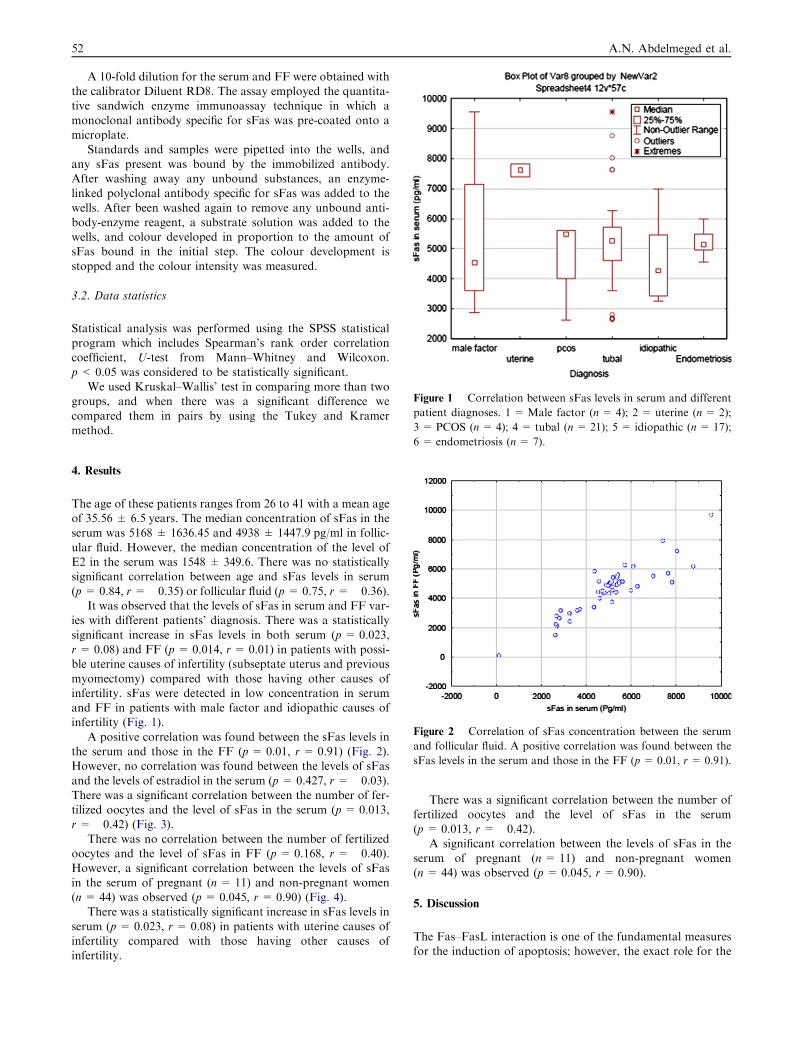
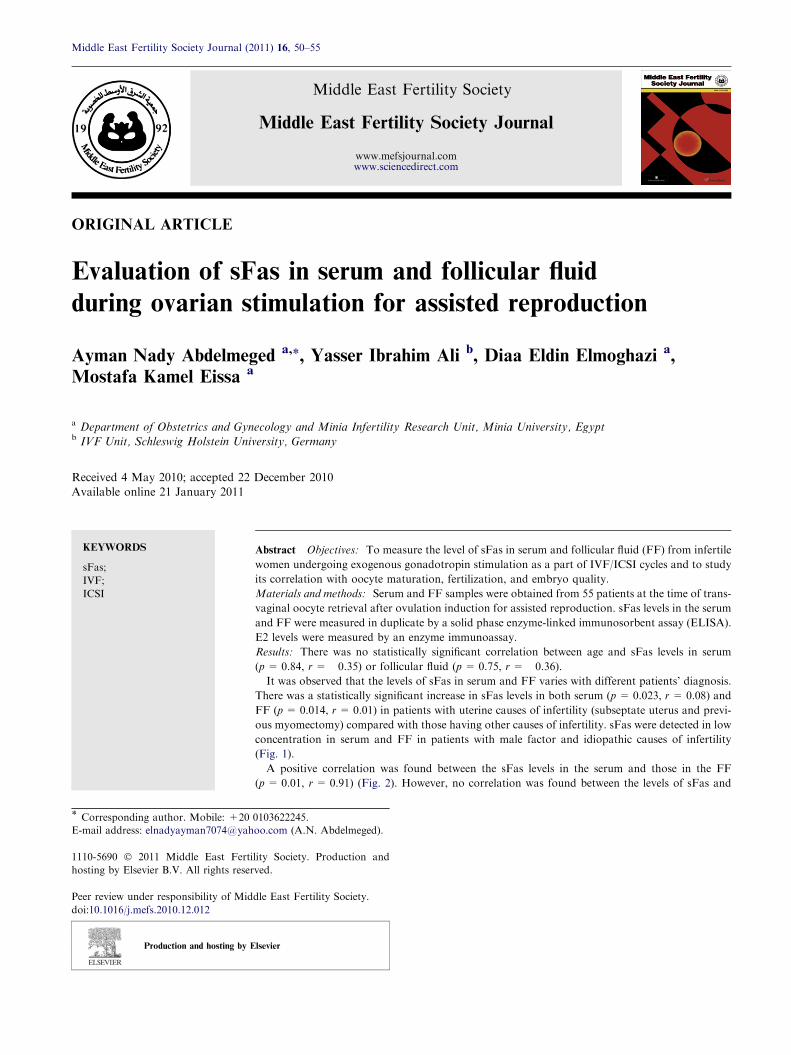
Figure 1 Correlation between sFas levels in serum and different
patient diagnoses. 1 =Male factor (n= 4); 2 = uterine (n= 2);
3 = PCOS (n= 4); 4 = tubal (n= 21); 5 = idiopathic (n= 17);
52 A.N. Abdelmeged et al.
A 10-fold dilution for the serum and FF were obtained withthe calibrator Diluent RD8. The assay employed the quantita-tive sandwich enzyme immunoassay technique in which a
monoclonal antibody specific for sFas was pre-coated onto amicroplate.
Standards and samples were pipetted into the wells, and
any sFas present was bound by the immobilized antibody.After washing away any unbound substances, an enzyme-linked polyclonal antibody specific for sFas was added to the
wells. After been washed again to remove any unbound anti-body-enzyme reagent, a substrate solution was added to thewells, and colour developed in proportion to the amount ofsFas bound in the initial step. The colour development is
stopped and the colour intensity was measured.
3.2. Data statistics
Statistical analysis was performed using the SPSS statisticalprogram which includes Spearman’s rank order correlationcoefficient, U-test from Mann–Whitney and Wilcoxon.
p< 0.05 was considered to be statistically significant.We used Kruskal–Wallis’ test in comparing more than two
groups, and when there was a significant difference we
compared them in pairs by using the Tukey and Kramermethod.
6 = endometriosis (n= 7).
Figure 2 Correlation of sFas concentration between the serum
and follicular fluid. A positive correlation was found between the
sFas levels in the serum and those in the FF (p= 0.01, r = 0.91).
4. Results
The age of these patients ranges from 26 to 41 with a mean ageof 35.56 ± 6.5 years. The median concentration of sFas in theserum was 5168 ± 1636.45 and 4938 ± 1447.9 pg/ml in follic-
ular fluid. However, the median concentration of the level ofE2 in the serum was 1548 ± 349.6. There was no statisticallysignificant correlation between age and sFas levels in serum
(p = 0.84, r = �0.35) or follicular fluid (p = 0.75, r= �0.36).It was observed that the levels of sFas in serum and FF var-
ies with different patients’ diagnosis. There was a statistically
significant increase in sFas levels in both serum (p = 0.023,r= 0.08) and FF (p = 0.014, r= 0.01) in patients with possi-ble uterine causes of infertility (subseptate uterus and previous
myomectomy) compared with those having other causes ofinfertility. sFas were detected in low concentration in serumand FF in patients with male factor and idiopathic causes ofinfertility (Fig. 1).
A positive correlation was found between the sFas levels inthe serum and those in the FF (p = 0.01, r = 0.91) (Fig. 2).However, no correlation was found between the levels of sFas
and the levels of estradiol in the serum (p = 0.427, r= �0.03).There was a significant correlation between the number of fer-tilized oocytes and the level of sFas in the serum (p= 0.013,
r= �0.42) (Fig. 3).There was no correlation between the number of fertilized
oocytes and the level of sFas in FF (p= 0.168, r= �0.40).However, a significant correlation between the levels of sFasin the serum of pregnant (n = 11) and non-pregnant women(n = 44) was observed (p = 0.045, r = 0.90) (Fig. 4).
There was a statistically significant increase in sFas levels in
serum (p= 0.023, r = 0.08) in patients with uterine causes ofinfertility compared with those having other causes ofinfertility.
There was a significant correlation between the number of
fertilized oocytes and the level of sFas in the serum(p = 0.013, r = �0.42).
A significant correlation between the levels of sFas in the
serum of pregnant (n = 11) and non-pregnant women(n = 44) was observed (p = 0.045, r= 0.90).
5. Discussion
The Fas–FasL interaction is one of the fundamental measuresfor the induction of apoptosis; however, the exact role for the
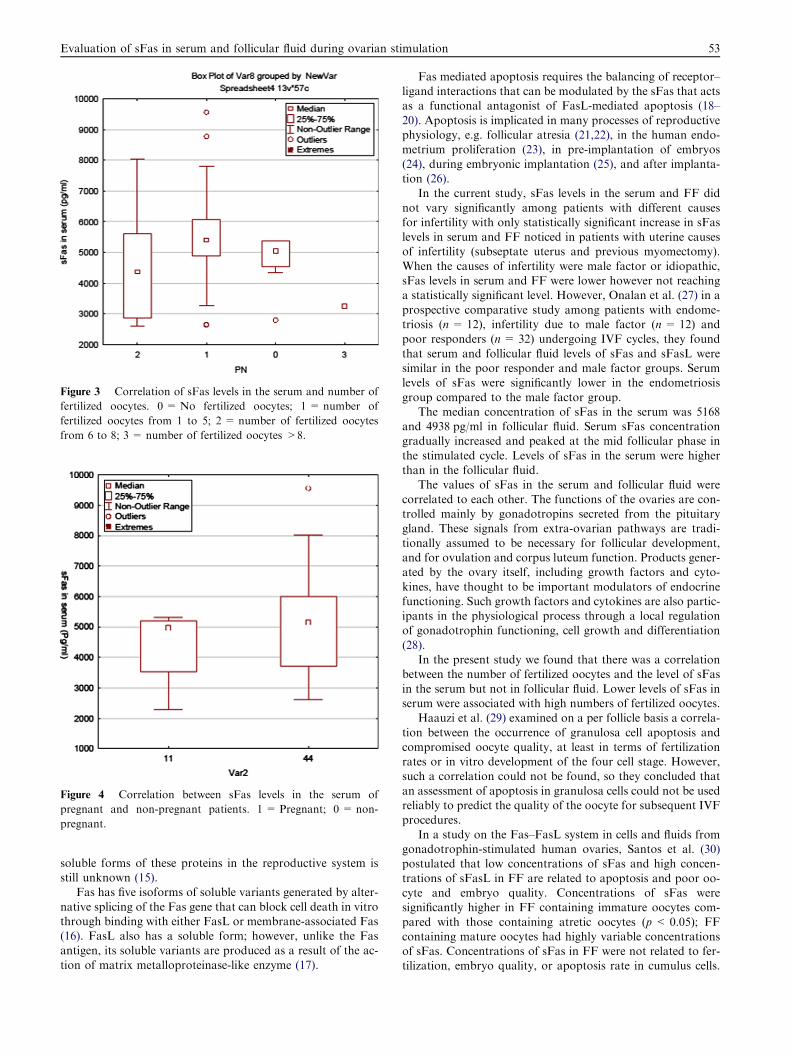
Figure 3 Correlation of sFas levels in the serum and number of
fertilized oocytes. 0 = No fertilized oocytes; 1 = number of
fertilized oocytes from 1 to 5; 2 = number of fertilized oocytes
from 6 to 8; 3 = number of fertilized oocytes >8.
Figure 4 Correlation between sFas levels in the serum of
pregnant and non-pregnant patients. 1 = Pregnant; 0 = non-
pregnant.
Evaluation of sFas in serum and follicular fluid during ovarian stimulation 53
soluble forms of these proteins in the reproductive system isstill unknown (15).
Fas has five isoforms of soluble variants generated by alter-
native splicing of the Fas gene that can block cell death in vitrothrough binding with either FasL or membrane-associated Fas(16). FasL also has a soluble form; however, unlike the Fasantigen, its soluble variants are produced as a result of the ac-
tion of matrix metalloproteinase-like enzyme (17).
Fas mediated apoptosis requires the balancing of receptor–ligand interactions that can be modulated by the sFas that actsas a functional antagonist of FasL-mediated apoptosis (18–
20). Apoptosis is implicated in many processes of reproductivephysiology, e.g. follicular atresia (21,22), in the human endo-metrium proliferation (23), in pre-implantation of embryos
(24), during embryonic implantation (25), and after implanta-tion (26).
In the current study, sFas levels in the serum and FF did
not vary significantly among patients with different causesfor infertility with only statistically significant increase in sFaslevels in serum and FF noticed in patients with uterine causesof infertility (subseptate uterus and previous myomectomy).
When the causes of infertility were male factor or idiopathic,sFas levels in serum and FF were lower however not reachinga statistically significant level. However, Onalan et al. (27) in a
prospective comparative study among patients with endome-triosis (n= 12), infertility due to male factor (n = 12) andpoor responders (n= 32) undergoing IVF cycles, they found
that serum and follicular fluid levels of sFas and sFasL weresimilar in the poor responder and male factor groups. Serumlevels of sFas were significantly lower in the endometriosis
group compared to the male factor group.The median concentration of sFas in the serum was 5168
and 4938 pg/ml in follicular fluid. Serum sFas concentrationgradually increased and peaked at the mid follicular phase in
the stimulated cycle. Levels of sFas in the serum were higherthan in the follicular fluid.
The values of sFas in the serum and follicular fluid were
correlated to each other. The functions of the ovaries are con-trolled mainly by gonadotropins secreted from the pituitarygland. These signals from extra-ovarian pathways are tradi-
tionally assumed to be necessary for follicular development,and for ovulation and corpus luteum function. Products gener-ated by the ovary itself, including growth factors and cyto-
kines, have thought to be important modulators of endocrinefunctioning. Such growth factors and cytokines are also partic-ipants in the physiological process through a local regulationof gonadotrophin functioning, cell growth and differentiation
(28).In the present study we found that there was a correlation
between the number of fertilized oocytes and the level of sFas
in the serum but not in follicular fluid. Lower levels of sFas inserum were associated with high numbers of fertilized oocytes.
Haauzi et al. (29) examined on a per follicle basis a correla-
tion between the occurrence of granulosa cell apoptosis andcompromised oocyte quality, at least in terms of fertilizationrates or in vitro development of the four cell stage. However,such a correlation could not be found, so they concluded that
an assessment of apoptosis in granulosa cells could not be usedreliably to predict the quality of the oocyte for subsequent IVFprocedures.
In a study on the Fas–FasL system in cells and fluids fromgonadotrophin-stimulated human ovaries, Santos et al. (30)postulated that low concentrations of sFas and high concen-
trations of sFasL in FF are related to apoptosis and poor oo-cyte and embryo quality. Concentrations of sFas weresignificantly higher in FF containing immature oocytes com-
pared with those containing atretic oocytes (p < 0.05); FFcontaining mature oocytes had highly variable concentrationsof sFas. Concentrations of sFas in FF were not related to fer-tilization, embryo quality, or apoptosis rate in cumulus cells.

54 A.N. Abdelmeged et al.
Soluble forms of Fas were present in FF from gonadotrophin-stimulated human ovaries, suggesting this system may playrole in preventing oocyte atresia during folliculogenesis, while
it might not be important for apoptotic events in cumulus cellsand oocytes after fertilization failure. Lastly, they reportedthat lower FF sFas does not impact negatively on the fertiliza-
tion of mature oocytes or on embryo quality.In this study it was observed that lower levels of sFas in ser-
um resulted in higher pregnancy rates. This fact attributed to
the presence of good fertilized oocytes. The above phenomenamay suggest that low levels of sFas in serum may be beneficialfor the implantation of fertilized oocytes or indeed preventdamage to the embryo. Lower levels of sFas seem to support
embryo implantation. Apoptosis regulators, including sFas,are considered to be critical in pregnancy. They affect blasto-cyst attachment, trophoblast outgrowth and the implantation
and proliferation of placenta cells. During embryonic implan-tation, apoptosis occurs during decidualization and invasion.
Our results are in contradiction with those of Onalan et al.
(27) who found similar levels of sFas and sFasL in both serumand follicular fluid among patients undergoing IVF with orwithout clinical pregnancy demonstrating that that these solu-
ble apoptotic factors may not be predictive for successful out-come of IVF. So, they concluded that they may not have anyimpact on fertilization of mature oocytes, embryo quality orpregnancy rates.
It is known that, in rodents the endometrial epithelial cellsin direct contact with the blastocyst undergo apoptosis (31).This provides a mechanism by which the blastocyst crosses
the epithelial barrier and obtains access to the maternal bloodsupply (32). Some in vitro models show that uterine epithelialcells are detached by the trophoblast and demonstrate apopto-
tic morphology during blastocyst outgrowth (33).After implantation, apoptosis also plays a role in the main-
tenance of pregnancy. The abundant expression of FasL on
trophoblast cells within the maternal decidua may provide adefense mechanism against attack from activated maternal leu-kocytes. The placental trophoblast induces a transient and spe-cific tolerance by apoptosis, mediated by the Fas /FasL system
(34).In conclusion, a lower level of sFas in serum was associated
with a higher pregnancy rates. This may be attributed to the
presence of good fertilized oocytes. The above phenomenamay suggest that low levels of sFas in serum may be associatedwith improvement in implantation of fertilized oocytes or may
prevent damage to the embryo. Lower levels of sFas seem tosupport embryo implantation.
References
(1) Hirshfield AN. Development of follicles in mammalian ovaries.
Int Rev Cytol 1991;124:93–101.
(2) Tilly JL, Kowalski KI, Johnson AL, Hsueh AJ. Involvement of
apoptosis in ovarian follicular atresia and postovulatory regres-
sion. Endocrinology 1991;5:2799–801.
(3) Itoh N, Yonehara S, Ishhii A, Yonehara M, Mizushima SI,
Sameshima M, et al. The polypeptide encoded by the cDNA for
human cell surface antigen Fas can mediate apoptosis. Cell
1991;66:233–43.
(4) Suda T, Takahashi T, Golstein P, Nagata S. Molecular cloning
and expression of the Fas ligand; a novel member of the tumour
necrosis factor family. Cell 1993;75:1169–78.
(5) Nozawa K, Kayagaki N, Tokano YH, Okumura K, Hasimoto H.
Soluble Fas and soluble Fas ligand in rheumatic diseases.
Arthritis Rheum 1997;40:1126–9.
(6) Hsu SY, Lai RJ, Finegold M, Hsuch AJ. Targeted over
expression of Bcl-2 in ovaries of transgenic mice leads to
decreased follicle apoptosis, enhanced folliculogenesis, and
increased germ cells tumorigenesis. Endocrinology
1996;137:4837–43.
(7) Byskov AG, Whitten WK, Beamer WG. The morphology of fetal
gonads of spontaneous mouse hermaphrodites. J Embryol Exp
Morphol 1978;52:63–78.
(8) Bagavandoss P, Midglley AK. Developmental changes in the
ovarian follicular basal lamina detected by immunofluorescence
and electron microscopy. Histochem Cytochem 1983;31:633–40.
(9) Greenwald GS, Moor RM. Isolation and preliminary character-
ization of pig primordial follicles. J Reprod Fert 1989;87:561–71.
(10) Carson RS, Richards JS, Kahn LG. Functional and morpholog-
ical differentiation of the theca and granulose cells during
pregnancy in the rat depend on increase basal luteinizing hormone
activation. Endocrinology 1981;109:1433–41.
(11) Boone E, Vandevoorde V, De Wild G, Haegeman G. Activation
of P42/P44 mitogen activated protein kinases and 38 MAPK by
the tumor necrosis factor (TNF) is mediated through the cell
death domain of the 55-kDa TNF receptor. FEBS Lett.
1998;441:275–80.
(12) Hakuno N, Koji T, Yano T, Kobayashi N, Tsutsumi O, Taketani
Y, et al. Fas/APO-1/CD95 system as a mediator of granulose cell
apoptosis in ovarian follicle atresia. Endocrinology
1996;5:1938–48.
(13) Tilly KL, Tilly JL. Inhibitors of oxidative stress mimic the ability
of follicle stimulating hormone to suppress apoptosis in cultured
ovarian follicles. Endocrinology 1995;136:242–52.
(14) Lambert-Messerlian G, Taylor A, leykin L, Isaacson K, Toth T,
Chang Y, et al. Characterization of intrafollicular steroid hor-
mones, inhibin, and follistatin in women with and without
polycystic ovarian syndrome following gonadotropin hyperstim-
ulation. Biol Reprod 1997;57:1211–6.
(15) Cataldo NA, Dumesic DA, Goldsmith PC, Jaffe RB. Immuno-
localization of Fas and Fas ligand in the ovaries of women with
polycystic ovary syndrome: relationship to apoptosis. Hum
Reprod 2000;15:1889–97.
(16) Cascino I, Fiucci G, Papoff G, Ruberti G. Three functional
soluble forms of the human apoptosis-inducing Fas molecule are
produced by alternative splicing. J Immunol 1995;145:2706–13.
(17) Kajagaki N, Kawasaki A, Ebata T, Ohmoto H, Ikeda S, Inoue S,
et al. Metalloproteinase-mediated release of human Fas ligand. J
Exp Med 1995;192:1777–83.
(18) Owen-Schaub LB, Angelo LS, Radinsk R, Ware CF, Gesner TG,
Bartos DP. Soluble Fas in tumour cells: a potential regulator of
apoptosis. Cancer Lett 1995;94:1–8.
(19) Kondo H, Maruo T, Peng X, Mochizuki M. Immunological
evidence for the expression of the Fas antigen in the infant and
adult human ovary during follicular regression and atresia. J Clin
Endocrinol Metab 1996;81:2702–10.
(20) Quirk SM, Harman RM, Cowan RG. Regulation of Fas antigen
(Fas, CD95)-mediated apoptosis of bovine granulosa cells by
serum and growth factors. Biol Reprod 2000;63:1278–84.
(21) Piquette GN, Tilly JL, Prichard LE. Detection of apoptosis in
human and rat ovarian follicles. J Soc Gynecol Invest
1994;1:297–301.
(22) Tao XJ, Sayegh RA, Tilly JL, Isaacson KB. Elevated expression
of pro apoptotic Bcl-2 member Bak, in the human endometrium
coincident with apoptosis during the secretory phase of the cycle.
Fertil Steril 1998;70:338–43.
(23) Zelzznik AJ, Ihrig LL, Bassett SG. Developmental expression of
Ca, Mg dependent endonuclease activity in rat granulosa and
luteal cells. Endocrinology 1989;125:2218–20.

Evaluation of sFas in serum and follicular fluid during ovarian stimulation 55
(24) Exley GE, Tang C, McElhinny AS. Expression of caspase and
Bcl-2 apoptotic family members in mouse preimplantation
embryos. Biol Reprod 1999;61:231–9.
(25) Parr EL, Tung HN, Parr MB. Apoptosis as the mode of uterine
epithelial cell death during embryo implantation in mice and rats.
Biol Reprod 1987;36:211–25.
(26) Hummer A, Blaschitz A, Daxbock C. Fas and Fas ligand are
expressed in the uteroplacental unit of first trimester pregnancy.
Am J Reprod Immunol 1999;1:558–66.
(27) Onalan G, Selam B, Onalan R, Geyhan T, Cincik M, Pabuccu R.
Serum and follicular fluid levels of soluble Fas and soluble Fas
ligand in IVF cycles. Eur J Obstet Gynecol Reprod Biol
2006;125:85–91.
(28) Adashi EY, Resnick CE, Hurwitz A. Insulin-like growth factors;
the ovarian connection. Hum Reprod 1991;6:1213–9.
(29) Haauzi D, De Vos J, Loup V, Assou S, Grasca S, Reyftmann C,
et al. Granulosa cells apoptosis and oocyte quality. Gynecol
Obstet Fertil 2008;78:730–42.
(30) Santos M, Anderson DJ, Racowski C. Presence of Fas–Fas ligand
system and bcl-2 gene products in cells and fluids from gonadot-
opin-stimulated human ovaries. Biol Reprod 2000;63:1811–6.
(31) Kamijo T, Rajabi MR, Mizunuma H. Biochemical evidence for
autocrine/paracrine regulation of apoptosis in cultured uterine
epithelial cells during mouse embryo implantation in vitro. Mol
Hum Reprod 1998;4:990–8.
(32) Pampfer S, Donnay I. Apoptosis at the time of embryo
implantation in mouse and rat. Cell Death Differ 1999;6:533–45.
(33) Hsu WL, Chen YH, Chao KC. Anti-Fas activating antibodies
enhances trophoblast outgrowth on endometrial epithelial cells by
induction of mediated apoptosis. Placenta 2008;29:338–46.
(34) Kauma SW, Huff TF, Hayes N, Nikaeo A. Placental Fas ligand
expression is a mechanism for maternal immune tolerance to the
fetus. J Clin Endocinol Metab 1999;84:2188–94.
Related Documents










![Role of herbals in the management of polycystic ovarian ...PCOS by acting directly on ovarian androgen secretion andabnormal follicular development [5] and the use of insulin-sensitizing](https://static.cupdf.com/doc/110x72/5ed75feda5b1445fe467ce70/role-of-herbals-in-the-management-of-polycystic-ovarian-pcos-by-acting-directly.jpg)
