of the Cardiac Patient for Non-cardiac Surgery Vincent Conte, MD Attending Anesthesiologist and Director of Anesthesia Services at Baptist Children’s Hospital (Ret.) Assistant Clinical Professor FIU School of Nursing

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Evaluation of the Cardiac Patient for Non-cardiac Surgery
Vincent Conte, MDAttending Anesthesiologist and
Director of Anesthesia Services at Baptist Children’s Hospital (Ret.)
Assistant Clinical ProfessorFIU School of Nursing

Introduction Patients with co-existing Cardiac disease will be
coming for surgery very frequently for NON-cardiac procedures
Familiarity with the AHA/ACC Guidelines is very important to be able to adequately assess the status of these patients.

Topics of Discussion Familiarize yourselves with the AHA/ACC
Guidelines Learn to identify which patients present a
significant risk of having a cardiac event intraoperatively
Learn what steps in the evaluation process are important to be done preoperatively to further identify which patients are at risk

Prevalence of Cardiovascular Disease
Estimated 22,000,000 US Adults have significant Coronary Artery Disease; 17 per 1000 (2004 AHA)
Of these, 6,400,000 have active or unstable angina
Another 50,000,000 have Hypertension (16%); 217 per 1000
There are 4,600,000 Strokes each year in the US and 4,800,000 new cases of CHF

That brings the total number of Americans who have some type of Cardiovascular disease to 77,000,000 or 26% of the total population
The more alarming statistic is that approx. 14% of patients with Hypertension and a normal resting EKG have undiagnosed SIGNIFICANT Coronary Artery disease
Prevalence of Cardiovascular Disease

Cardiac Predictors
All of the flow charts and models are based on factors that are called “Cardiac Predictors”
They are graded as Minor, Intermediate, and Major
The preop evaluation all depends on which predictors are present and how many as well

Minor Cardiac Predictors

Intermediate Cardiac Predictors

Major Cardiac Predictors

Flow Charts Based on Predictors
The following are the flow charts created by the AHA/ACC based on which and how many predictors are present preoperatively
Also keep in mind that your clinical judgment has a lot to do with what level you place the patient at within the flow charts
If you think the patient is sicker than they look on paper, do not hesitate to place them in a higher risk category to start with

MET Scale Also used to place patients at their appropriate
positions in the flow charts is the MET Scale This is based on a measure called a “Metabolic
Unit” A unit is proportional to a certain amount of
physical exertion Based on how many MET’s a person is
functioning at, an approximation of their cardiac status can be made
IT IS VERY SUBJECTIVE, but can still act as a quick screening scale to rapidly assess overall cardiac status and health

MET Scale


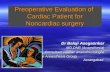
Intermediate Predictors




Cardiac Assessment
You can see that for the most part, the charts are easy to follow and do a good job of delineating who and where a patient should be placed in the sequence
However, a grey area exists with respect to newly diagnosed Valvular Heart Disease that is deemed mild by the Cardiologist
Some feel that this should be a MAJOR indicator while others feel that it should be an INTERMEDIATE indicator

Cardiac Risk Assessment Other factors may help you determine what category to put
such patients. Co-existing Hypertension or DM may bump them up to
MAJOR while a lack of symptoms and no other co-existing disease may keep them in INTERMEDIATE
Regardless, a quick phone consultation should be made with the Cardiologist and his recommendations should be noted in the chart as well as documenting that you DID contact the Cardiologist in this matter
Then you would just proceed along the recommended Anesthesia Treatment guidelines for whichever Valvular lesion the patient might have

Common Intraoperative Cardiac Conditions
The most common Cardiac complications you may encounter in the OR are:
1) ST Segment changes (Intraop Ischemia)2) Myocardial Infarction3) Sinus Bradycardia4) Non-lethal Ventricular Arrhythmias5) Pulmonary Edema

ST Segment Changes This event can manifest as either elevation or depression of
the ST Segment The etiology can vary:1) Inadequate coronary perfusion vs. demand (AS)2) Acute Myocardial Ischemia or Infarction3) Myocardial contusion (Trauma)4) Electrolyte abnormalities (hypo/hyperkalemia,
hypercalcemia)5) Head injury with raised ICP and elevated systemic blood
pressure6) Hypothermia7) Post-Defibrillation injury

ST Segment Changes Typically, this is seen in:1) Patients with pre-existing CAD2) Any changes causing either an increase in
myocardial O2 demand or decreased supply (Tachycardia, hypertension/hypotension, hypoxemia, hemodilution, or Coronary spasm)
3) After head or chest trauma4) During vaginal delivery or C-section

ST Segment Changes PREVENTION:1) Carefully evaluate and prepare patients with CAD
preoperatively2) Carefully manage hemodynamics and hematocrit
to optimize myocardial O2 Balance3) Identify and evaluate pre-existing ST segment
abnormalities preoperatively

ST Segment Changes Manifestations:1) In an awake patient, they may describe Chest
pain radiating into the arms and throat2) Dyspnea3) Nausea and vomiting4) Altered level of consciousness or cognitive
function

ST Segment Changes EKG/Systemic Manifestations:1) Depression or elevation of the ST segment from
the isoelectric level2) Development of Q waves3) Arrhythmias (PVC’s, ventricular tachycardia,
Ventricular fibrillation4) Hypotension5) Elevated ventricular filling pressures (stiff ventricle)6) V wave on pulmonary artery wedge tracing

ST Segment Changes Management:1) Verify ST segment changes (check lead placement,
compare to previous EKG’s)2) Ensure adequate oxygenation and ventilation (check
pulse oximeter, capnograph, send an ABG)3) Treat tachycardia and/or hypertension (B-Blockade with
Esmolol, Labetolol, incr. depth of anesthesia)4) NTG IV Infusion, 0.25-2micrograms/kg/min; (titrate to
desired effect)5) Calcium Channel Blockade (Verapamil IV 2.5 mg,
Diltiazem IV 2.5 mg

ST Segment Changes Management:6) Treat hypotension and/or bradycardia7) Optimize circulating fluid volume8) Support myocardial contractility as needed using inotropic
agents (Ephedrine, Dopamine, Dobutamine, Epinephrine)9) AVOID NTG/CA Blockers until hypotension or bradycardia
are resolved10) Inform the surgeon; if possible terminate procedure early11) Send blood chemistries (ABG, H/H, Electrolytes, Glucose,
CK-MB, Troponin)12) Treat underlying causes of ST Segment changes if other
than Myocardial Ischemia

ST Segment Changes COMPLICATIONS:1) Myocardial Infarction2) Arrhythmias3) Cardiac Arrest4) Complications from placement of PA catheter5) Complications from placement of TEE

Myocardial Infarction Defined as myocardial cell death due to
inadequate cellular perfusion. Transmural (Q wave) infarctions involve the entire
thickness of the myocardial wall Subendocardial (non-Q wave) infarctions involve
only the subendocardial portion of the myocardial wall

Myocardial Infarction Etiology:1) Acute occlusion of a coronary artery (thrombus,
plaque)2) Inadequate coronary perfusion for a given
myocardial O2 demand3) Acute dissection of the aorta

Myocardial Infarction Typical Situations:1) In patients with pre-existing CAD/Angina Pectoris2) In older patients (>70 years old)3) Patients with peripheral vascular disease4) Patients with DM (silent myocardial ischemia)5) During any acute change in myocardial O2 demand or
delivery (Tachycardia, hypertension, hypotension, hypoxemia, hemodilution, or Coronary spasm)
6) Patients with Aortic or Mitral STENOSIS7) Patients with recent CABG surgery8) Acute Carbon Monoxide poisoning

Myocardial Infarction Prevention:1) Carefully evaluate and prepare patients with
CAD preoperatively (evaluate myocardial function and reserve; is patient optimized?)
2) Avoid elective anesthesia and surgery in patients with Unstable Angina or with a h/o MI in the previous 6 months
3) Optimize hemodynamics and hematocrit during anesthesia

Myocardial Infarction Manifestations:1) Differentiated from Ischemia by persistence and
progression of ST segment and T wave changes2) Elevated cardiac isoenzymes3) Awake patient with chest pain, dyspnea, nausea
and vomiting4) EKG abnormalities (ST depressions/elevations;
hyperacute, prominent T waves; development of Q waves)
5) Arrhythmias (PVC’s, V Tach, V Fib, AV Block, Bundle branch block)
6) Hypotension, Tachycardia/Bradycardia7) Elevated Ventricular filling pressures

Myocardial Infarction Management:1) VERIFY manifestations of ongoing myocardial
ischenia (if patient is awake assess clinical signs and symptoms, check lead placement and check multiple leads, obtain a 12-lead EKG ASAP, evaluate hemodynamic status)
2) INFORM the surgeon and terminate surgery ASAP
3) Request ICU bed ASAP4) If present, treat Ventricular Arrhythmias (Lido IV
1-1.5mg/kg bolus, then 1-4mg/min; Procainamide IV 500mg over 10-20 minutes, then 2-6mg/min)

Myocardial Infarction Management:5) Place an arterial line and monitor blood pressure
VERY carefully6) Treat tachycardia (MOST important!!) and/or
hypertension (increase depth of anesthesia, B-Blockade w/ Esmolol, Labetolol and/or Cardene for hypertension)
7) NTG IV @ 0.25-2 microgms/min (titrate PRN)8) CA Channel Blockers (Verapamil IV 2.5 mg and
repeat as needed, or Diltiazem IV 2.5 mg, also repeat as needed)
9) If hypotension develops, maintain BP with Neosynephrine and volume (cardiac perfusion takes precedence over afterload reduction)

Myocardial Infarction Management:10) Consider placing an SG cath to guide with fluid
management (go by LVEDP to avoid overload)11) Support myocardial contractility as needed with Inotropes
such as Dopamine, Dobutamine, Epi (use with EXTREME caution as these will also increase myocardial O2 demand)
12) Avoid NTG and CA Channel Blockers until hypotension or bradycardia are resolved
13) Treat pain and anxiety if patient is awake14) Send Labs (ABG’s, H/H, electrolytes, CK, CK-MB,
Troponins)15) If hypotension persists consider placement of an IABP to
decrease workload of myocardium and allow to rest and recooperate

Myocardial Infarction
Complications:1) CHF2) Arrhythmias3) Cardiac Arrest4) Thrombus formation and complications from their
migration5) Papillary muscle dysfunction or rupture6) Rupture of Interventricular septum or ventricular
wall

Sinus Bradycardia Definition: A heart rate less than 60 bpm in an
adult, in which the impulse formation begins in the sinus node
Etiology:1) Increased vagal tone (vaso-vagal, valsalva)2) Drug induced3) Hypoxemia4) Cardiac Ischemia5) Hypothermia6) Hypothyroidism7) Brain injury with herniation8) Physiologic (congenital; physical conditioning)

Sinus Bradycardia Typical Situations:1) An isolated finding during preop evaluation2) Following administration of drugs (Narcotics,
Halothane, B-Blockers, CA Channel blockers, Anticholinesterases, A2-agonists – Clonidine)
3) During Vagal stimulation (Traction on eye or peritoneum, Laryngoscopy and Intubation, Bladder catheterization)
4) During hypertensive episodes (Baroreceptor reflex)
5) During spinal/epidural anesthesia w/ high level6) ECT

Sinus Bradycardia
Prevention:1) Premedicate patients at risk with anticholinergics
(Atropine IM 0.4 mg, Robinul IM 0.2 mg)2) Treat bradycardia early during high
spinal/epidurals (Atropine IV 0.4-0.8mg, Robinul IV 0.2-0.4mg)
3) Avoid excess traction on peritoneum or extraoccular muscles
4) Avoid excess manipulation of the carotid sinus

Sinus Bradycardia Manifestations:1) Slow heart rate on EKG, Pulse Oximeter, A-Line,
NIBP Monitor, palpation of peripheral pulses2) Hypotension3) Symptoms in a conscious patient: Nausea,
Vomiting, Change in mental status4) Junctional or Idioventricular escape beats

Sinus Bradycardia Management:1) Verify bradycardia and assess its hemodynamic
significance (Check MULTIPLE monitors to confirm or palpate a peripheral pulse)
2) Ensure adequate oxygenation and ventilation (bradycardia is common with hypoxic conditions esp. in pediatric patients)
3) Call for help if significant hemodynamic changes are associated with the bradycardia

Sinus Bradycardia Management:4) If bradycardia IS associated with SEVERE
hypotension, loss of consciousness or seizures, Rx with Epi IV, 10microgram bolus (1cc) and repeat as needed until desired effect is achieved
5) If Bradycardia fails to resolve with Epi, consider Transcutaneous pacing and Isoproterenol infusion at 1-3 micrograms/min.
6) Begin CPR if necessary

Sinus Bradycardia Management:7) If bradycardia is associated with only mild to
moderate hypotension (10-15% drop from pre-brady rate), RX with Ephedrine IV in 5-10 mg increments and/or Atropine IV 0.4mg and/or Robinul IV 0.2mg; Repeat above as necessary until desired effects obtained
8) Scan surgical field once brady is treated for possible physical causes; if none are present, observe patient closely both intra and post-op

Sinus Bradycardia Complications:1) Escape arrhythmias (Junctional/Idioventricular)2) Cardiac Arrest3) Complications with pacer operation or placement4) Tachyarrhythmias and hypertension secondary to
drug treatment (overtreatment will result in “chasing your own tail”)

Non-Lethal Ventricular Arrhythmias
Definition:Nonlethal ventricular (wide QRS complex)
arrhythmias NOT requiring ACLS although they may eventually lead to ventricular fibrillation

Non-Lethal Ventricular Arrhythmias
Etiology:1) PVC’s2) Abnormal automaticity of ventricular
myocardium3) Re-entry phenomena4) Drug Toxicity5) R on T phenomenon

Non-Lethal Ventricular Arrhythmias
Typical Situations:1) PVC’s provoked by tea, coffee, alcohol, tobacco,
or emotional excitement2) Patients with Myocardial Ischemia or infarction3) Hypoxemia and/or hypercarbia4) Potassium and/or Acid Base disturbances5) Patients with Mitral Valve Prolapse6) Excessive depth of anesthesia

Non-Lethal Ventricular Arrhythmias
Typical Situations:7) Direct Mechanical stimulation of the heart8) Acute hypertension and/or tachycardia9) Acute HYPOtension and/or bradycardia10) Drugs (Halothane, Dig, Tricyclics, Aminophylline,
antihistamines11) Hypothermia

Non-Lethal Ventricular Arrhythmias
Manifestations:1) Wide QRS complex on EKG NOT preceeded by
a P wave2) PVC’s3) Ventricular tachycardia4) Torsade de pointes (paroxysms of V-tach in
which the QRS axis changes direction continuously)

Non-Lethal Ventricular Arrhythmias
Management:1) Ensure adequate oxygenation and ventilation2) Check if the arrhythmia is hemodynamically
significant3) If it is: Lidocaine IV 1-1.5 mg bolus; consider
synchronized countershock if change is severe4) Diagnose the arrhythmia5) If V-tach is present repeat Lido q/15 min and
start infusion at 1-4 mg/min; consider synched countershock

Non-Lethal Ventricular Arrhythmias
Management:6) If Torsade de pointes is present give MgSO4, 1-2
g bolus followed by infusion at 1 mg/min7) If PVC’s ONLY are present with Tachycardia and
Hypertension deepen anesthesia with IV/inhalational agents
8) Evaluate for possible myocardial ischemia

Summary
Cardiac disease is becoming more and more prevalent every year, so the fraction of your patients who will have significant Cardiac Disease will also be on the rise
Careful Preop evaluation and testing WILL reduce the morbidity and mortality associated with any patient who has pre-existing Cardiac disease

Summary Unfortunately, due to time pressures and Surgeon
pressures, you may be tempted to just “Go for it” and hope for the best BUT
DON’T• It will ultimately be your ass hung out to dry and
the surgeon will be saying that “Anesthesia never really told me how sick the patient was”
Stick to your guns and make sure that the PATIENT and their safety comes FIRST!!!!!!!
Related Documents