376 ActaOrthopaedica2008;79(3):376–385 Evaluation of a treatment protocol in distal radius fractures A prospective study in 581 patients using DASH as outcome Antonio Abramo, Philippe Kopylov, and Magnus Tägil Department of Orthopedics, Clinical Sciences, Lund University, Lund, Sweden Correspondence AA: [email protected] Submitted 07-10-01. Accepted 08-02-28 Copyright©Taylor&Francis2008.ISSN1745–3674.PrintedinSweden–allrightsreserved. DOI10.1080/17453670710015283 Background and purpose Distal radius fractures are most often treated nonoperatively, but sometimes they aretreatedsurgicallywhendeemedunstable.Basedon the literature, a consensus protocol for treatment has beendevelopedinsouthernSwedentoaidcliniciansin their decision making.We evaluated the results of this protocolprospectivelyusingavalidatedoutcomeinstru- ment (DASH) in a large consecutive and population- basedseriesofunselectedpatients. Methods 581 patients were treated according the protocol.Age,sex,fractureside,andtypeoftreatment wereregistered.Thesubjectiveoutcomewasmeasured byDASH.133patientswereoperated. Results75%ofthepatientsreturnedthequestion- naire.ThemedianDASHscoreat3monthswas18.3and at 12 months it was 7.5.All treatment groups had low DASHscoresatthefinalfollow-up.Reduced,nonoper- atedfractureshadaworsescore(11.6)thanundisplaced (4.2)oroperatedfractures(6.0).Agewastheonlyother predictor, with older patients having a worse score.A correlationwasfoundbetweentheshort-version11-item QuickDASHquestionnaireandthefull30-itemDASH, both at 3 months (r = 0.98) and at 1 year (r = 0.97) (p<0.001forboth). Interpretation Most patients have residual symp- tomsat3monthsafterthefracturebutarenormalized at1year.Goodfinalsubjectiveresultwasachievedwith theproposedprotocolregardlessofinitialseverityand treatmentofthefracture,asindicatedbyalowmedian DASHscoreinallgroups.Therewascorrelationbetween QuickDASHandthefullDASH,andtheformercould beusedinfuturestudies. ■ Distalradiusfractureisthemostcommontypeof fracture,accountingforone-sixthofallfracturesat anemergencyroom(Lindau2000).Severaltreat- ment options are available. Undisplaced fractures arecastedanddisplacedfracturesarereducedand casted. Unstable fractures are most often oper- atedupon,especiallyifthefractureisimpossible toreduceortoretaininareducedpositionatthe emergency ward, or when the fracture does not remainreducedatthefollow-up.Differenttypesof operativefixationcanbechosenandmanyauthors havereportedtheresultsofvarioustreatmentsfor distalradiusfractures. A particular treatment protocol for the distal radius fracture has been used at Lund Univer- sityHospitalsince1998.Thetypeoftreatmentis standardized and depends upon the radiographic appearance,reducibility,andstabilityofthefrac- tureaswellastheageanddemandsofthepatient (Figure1).Theprotocolwasdevelopedasacon- sensus document between the hospitals treating distal radius fractures in the southern Swedish region. Searching the literature, guidelines for treatment can be made for such a protocol, but (perhapssurprisingly)thereisnorobustevidence at present to suggest that any treatment method is superior to any other in the Cochrane meta- analysisreports,eitherfordifferenttypesofcon- servativetreatment(HandollandMadhok2003a) or for surgical treatment (Handoll and Madhok 2003b).Theaimofthepresentstudywasthere- fore to collect prospective outcome data for the currenttreatmentprotocolinadistalradiusfrac- Acta Orthop Downloaded from informahealthcare.com by 182.253.52.31 on 05/20/14 For personal use only.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

376 ActaOrthopaedica2008;79(3):376–385
Evaluation of a treatment protocol in distal radius fractures A prospective study in 581 patients using DASH as outcome
Antonio Abramo, Philippe Kopylov, and Magnus Tägil
Department of Orthopedics, Clinical Sciences, Lund University, Lund, SwedenCorrespondence AA: [email protected] 07-10-01. Accepted 08-02-28
Copyright©Taylor&Francis2008.ISSN1745–3674.PrintedinSweden–allrightsreserved.DOI10.1080/17453670710015283
Backgroundandpurpose Distal radius fracturesaremostoften treatednonoperatively,but sometimes theyaretreatedsurgicallywhendeemedunstable.Basedonthe literature, a consensus protocol for treatment hasbeendevelopedinsouthernSwedentoaidcliniciansintheirdecisionmaking.Weevaluatedtheresultsof thisprotocolprospectivelyusingavalidatedoutcomeinstru-ment (DASH) in a large consecutive and population-basedseriesofunselectedpatients.
Methods 581 patients were treated according theprotocol.Age,sex,fractureside,andtypeoftreatmentwereregistered.ThesubjectiveoutcomewasmeasuredbyDASH.133patientswereoperated.
Results 75%ofthepatientsreturnedthequestion-naire.ThemedianDASHscoreat3monthswas18.3andat12months itwas7.5.All treatmentgroupshad lowDASHscoresatthefinalfollow-up.Reduced,nonoper-atedfractureshadaworsescore(11.6)thanundisplaced(4.2)oroperatedfractures(6.0).Agewastheonlyotherpredictor, with older patients having a worse score.Acorrelationwasfoundbetweentheshort-version11-itemQuickDASHquestionnaireandthefull30-itemDASH,both at 3 months (r = 0.98) and at 1 year (r = 0.97)(p<0.001forboth).
Interpretation Most patients have residual symp-tomsat3monthsafterthefracturebutarenormalizedat1year.Goodfinalsubjectiveresultwasachievedwiththeproposedprotocolregardlessofinitialseverityandtreatmentofthefracture,asindicatedbyalowmedianDASHscoreinallgroups.TherewascorrelationbetweenQuickDASHandthefullDASH,andtheformercouldbeusedinfuturestudies.
■
Distalradiusfractureisthemostcommontypeoffracture,accountingforone-sixthofallfracturesatanemergencyroom(Lindau2000).Severaltreat-mentoptionsareavailable.Undisplacedfracturesarecastedanddisplacedfracturesarereducedandcasted. Unstable fractures are most often oper-atedupon,especiallyif thefractureis impossibletoreduceortoretaininareducedpositionattheemergency ward, or when the fracture does notremainreducedatthefollow-up.Differenttypesofoperativefixationcanbechosenandmanyauthorshavereportedtheresultsofvarioustreatmentsfordistalradiusfractures.
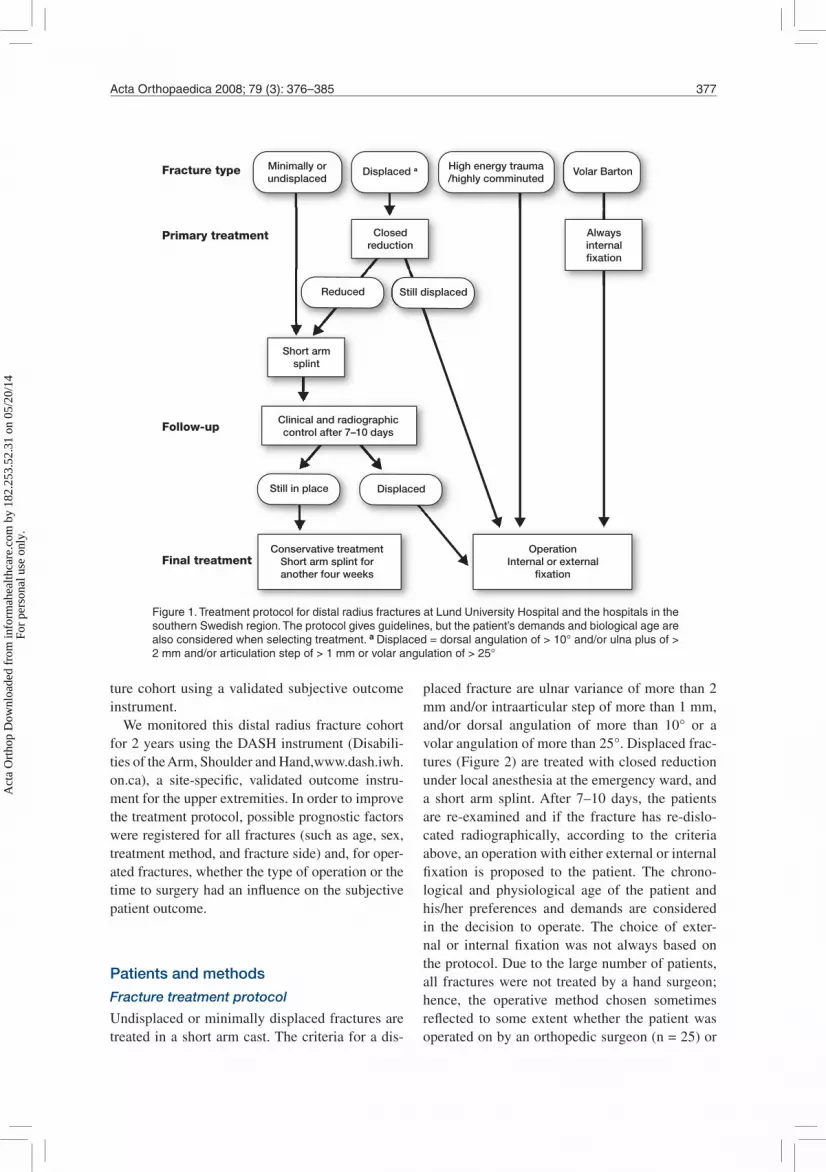
A particular treatment protocol for the distalradius fracture has been used at Lund Univer-sityHospitalsince1998.Thetypeoftreatmentisstandardizedanddependsupon the radiographicappearance,reducibility,andstabilityofthefrac-tureaswellastheageanddemandsofthepatient(Figure1).Theprotocolwasdevelopedasacon-sensus document between the hospitals treatingdistal radius fractures in the southern Swedishregion. Searching the literature, guidelines fortreatment can be made for such a protocol, but(perhapssurprisingly)thereisnorobustevidenceat present to suggest that any treatment methodis superior to any other in the Cochrane meta-analysisreports,eitherfordifferenttypesofcon-servativetreatment(HandollandMadhok2003a)or for surgical treatment (Handoll and Madhok2003b).Theaimof thepresentstudywasthere-fore to collect prospective outcome data for thecurrenttreatmentprotocolinadistalradiusfrac-
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.
ActaOrthopaedica2008;79(3):376–385 377
turecohortusingavalidatedsubjectiveoutcomeinstrument.
Wemonitored thisdistal radius fracturecohortfor2yearsusingtheDASHinstrument(Disabili-tiesoftheArm,ShoulderandHand,www.dash.iwh.on.ca), a site-specific, validated outcome instru-mentfortheupperextremities.Inordertoimprovethetreatmentprotocol,possibleprognosticfactorswereregisteredforallfractures(suchasage,sex,treatmentmethod,andfractureside)and,foroper-atedfractures,whetherthetypeofoperationorthetimetosurgeryhadaninfluenceonthesubjectivepatientoutcome.
Patients and methods
Fracture treatment protocol
Undisplacedorminimallydisplacedfracturesaretreatedinashortarmcast.Thecriteriaforadis-
placedfractureareulnarvarianceofmorethan2mmand/orintraarticularstepofmorethan1mm,and/or dorsal angulation of more than 10° or avolarangulationofmorethan25°.Displacedfrac-tures(Figure2)aretreatedwithclosedreductionunderlocalanesthesiaattheemergencyward,anda short arm splint.After 7–10 days, the patientsare re-examined and if the fracture has re-dislo-cated radiographically, according to the criteriaabove,anoperationwitheitherexternalorinternalfixation is proposed to the patient. The chrono-logical and physiological age of the patient andhis/her preferences and demands are consideredin the decision to operate. The choice of exter-nal or internal fixationwas not always based ontheprotocol.Duetothelargenumberofpatients,all fractureswerenot treatedbyahandsurgeon;hence, the operative method chosen sometimesreflected to someextentwhether thepatientwasoperatedonbyanorthopedicsurgeon(n=25)or
Fracture type
Primary treatment
Final treatment
Follow-up
Minimally orundisplaced
High energy trauma/highly comminuted
Displaced a Volar Barton
Still displacedReduced
DisplacedStill in place
Closedreduction
Alwaysinternalfixation
Short armsplint
Clinical and radiographiccontrol after 7–10 days
OperationInternal or external
fixation
Conservative treatmentShort arm splint foranother four weeks
Figure1.TreatmentprotocolfordistalradiusfracturesatLundUniversityHospitalandthehospitalsinthesouthernSwedishregion.Theprotocolgivesguidelines,butthepatient’sdemandsandbiologicalagearealsoconsideredwhenselectingtreatment.aDisplaced=dorsalangulationof>10°and/orulnaplusof>2mmand/orarticulationstepof>1mmorvolarangulationof>25°
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.
378 ActaOrthopaedica2008;79(3):376–385
ahandsurgeon(n=108).Thelattermaybemorepronetoopenreduction,butatthesametimetakescareofmorecomplexfractures.5ofthe16volarplates were done by an orthopedic surgeon.Theremaining54openreductionsweredonebyhandsurgeons.
Patientswithprimaryunstablefractures,impos-sible to either reduce or retain in an acceptablepositionaccordingtothecriteriadescribedabove,areoperated.Outof86primaryunstablefractures,70wereoperatedbyhandsurgeonsandof these,21werealsoincludedinarandomizedstudycom-paring external fixation to internal fixation. For16fractures,thedecisiontooperatewasmadebythe orthopedic surgeon on call who chose exter-nal fixation in every case. Finally, due to a highriskofsecondarydisplacement,volarlydislocatedfractureswereoperatedwithopenreductionandavolarplate.
Surgical procedures
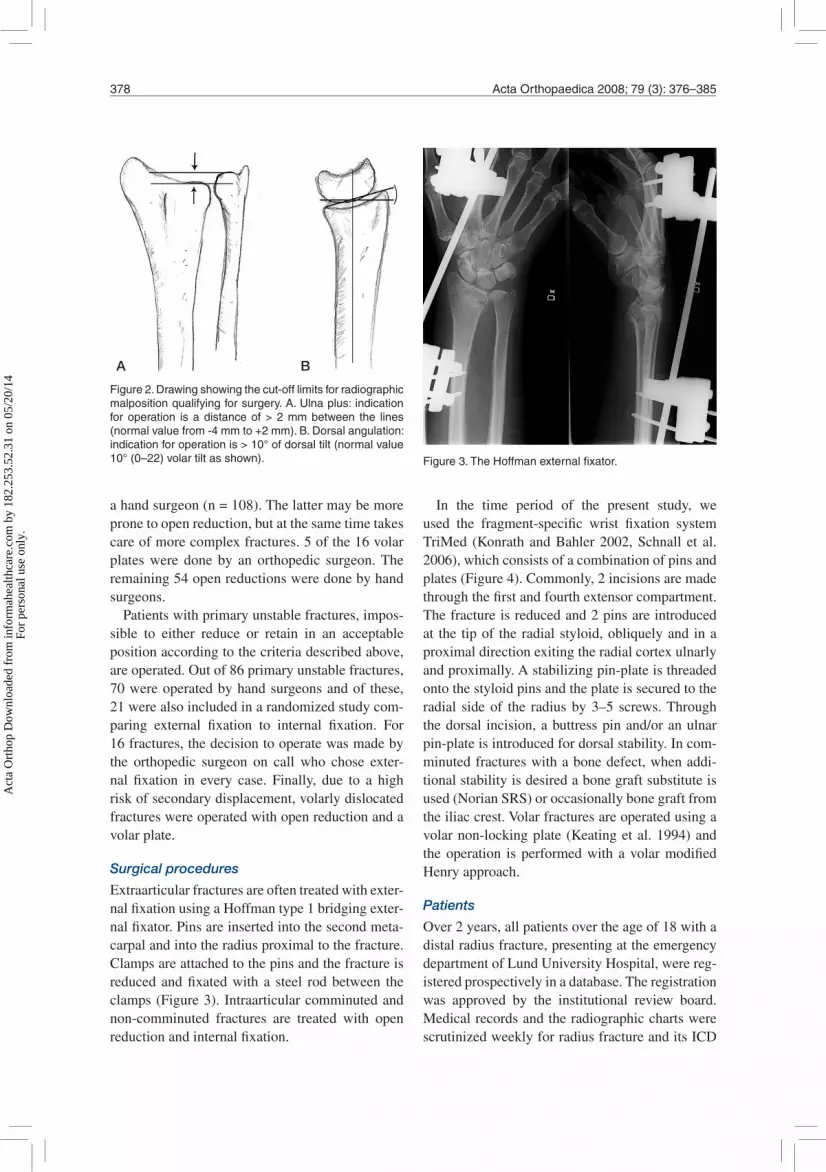
Extraarticularfracturesareoftentreatedwithexter-nalfixationusingaHoffmantype1bridgingexter-nalfixator.Pinsareinsertedintothesecondmeta-carpalandintotheradiusproximaltothefracture.Clampsareattachedtothepinsandthefractureisreducedandfixatedwith a steel rodbetween theclamps(Figure3).Intraarticularcomminutedandnon-comminuted fractures are treated with openreductionandinternalfixation.
In the time period of the present study, weused the fragment-specific wrist fixation systemTriMed (KonrathandBahler2002,Schnall et al.2006),whichconsistsofacombinationofpinsandplates(Figure4).Commonly,2incisionsaremadethroughthefirstandfourthextensorcompartment.Thefractureisreducedand2pinsareintroducedat the tipof theradialstyloid,obliquelyand inaproximaldirectionexitingtheradialcortexulnarlyandproximally.Astabilizingpin-plateisthreadedontothestyloidpinsandtheplateissecuredtotheradial sideof the radiusby3–5 screws.Throughthedorsal incision,abuttresspinand/oranulnarpin-plateisintroducedfordorsalstability.Incom-minutedfractureswithabonedefect,whenaddi-tionalstabilityisdesiredabonegraftsubstituteisused(NorianSRS)oroccasionallybonegraftfromtheiliaccrest.Volarfracturesareoperatedusingavolarnon-lockingplate (Keatingetal.1994)andtheoperation isperformedwith avolarmodifiedHenryapproach.
Patients
Over2years,allpatientsovertheageof18withadistalradiusfracture,presentingattheemergencydepartmentofLundUniversityHospital,werereg-isteredprospectivelyinadatabase.Theregistrationwas approved by the institutional review board.MedicalrecordsandtheradiographicchartswerescrutinizedweeklyforradiusfractureanditsICD
Figure2.Drawingshowingthecut-offlimitsforradiographicmalpositionqualifyingforsurgery.A.Ulnaplus:indicationforoperation isadistanceof>2mmbetween the lines(normalvaluefrom-4mmto+2mm).B.Dorsalangulation:indicationforoperationis>10°ofdorsaltilt(normalvalue10°(0–22)volartiltasshown).
A B
Figure3.TheHoffmanexternalfixator.
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.

ActaOrthopaedica2008;79(3):376–385 379
code. 581 patients with 584 fractures were iden-tifiedandgivenorsentaDASHquestionnaire tofillout.Duringthefirstweekafterinjury,patientswereaskedtoreportanypre-fractureimpairment.TheDASHquestionnairewasdistributedagainat3and12monthsafterthefracture.
63patients(47women)wereexcludedfromtheoriginal581patients. 11patientsdiedduring thefollow-uptime,7patientscouldnotspeakSwedishandcouldnotfilloutthequestionnaire.38patientssuffered from senile dementia. 7 other patientswereexcludedduetoothersimultaneousarminju-ries.Theexcludedpatientswereolder(72(18–97)years,p<0.001)buttherewasnosignificantdif-ferenceregardingtheirsex,fractureside,ortypeoftreatment.Theremaining518patientshadameanageof60(19–93)years.398werefemalewithameanageof63(19–93)years,and120weremale,withmeanage50(19–92)years.206hadfracturedtheirrightwrist,309theirleft,and3hadbilateralfractures.
Patient groups
The 518 patients were divided into 3 groupsaccording to their treatment. 220 patients hadundisplaced fractures and were casted withoutreduction. 212 patients had fractures that werereduced.Bothgroupsweretreatedinashortarmcastfor4–5weeks.86ofthepatientshadfracturesthatrequiredanoperationbecausetheywereeither
complexfractures thatwere impossible toreduceorvolarBartonfractures.
In thegroupwith reducedfractures,47of the212 fracturesshowedadislocationat the follow-upappointmentandwereoperated.Theoperationsperformedinthese133patientsweredividedinto4groups:externalfixation(63patients),internalfixa-tionwiththeTriMedsystem(51patients),internalfixationwithvolarplating(16patients),andotherprocedures(3patients:1screwfixation,and2withcombined internal and external fixation) (Figure5).As in previous studies, we arbitrarily definedmen less than60yearsofageandwomenbelowtheageof50toconstituteanon-osteoporoticagegroup, as opposed to the older osteoporotic agegroup(Kopylovetal.1993,Lindauetal.1999)
DASH questionnaire
DASH is a self-administered questionnaire thatwasdevelopedbytheAAOSandtheInstituteforWorkandHealthinCanada(Hudaketal.1996).ASwedishversionhasbeenvalidatedforuseinupperextremity disorders but not specifically for distalradiusfractures(Atroshietal.2000).Thequestion-naireconsistsof30questionsevaluatingdifferentaspectsofphysicalactivity,severityofsymptoms,andtheeffectoftheinjuryonsocialactivities.Ascoreiscalculatedandthedisabilityofthepatientis estimated on a scale from 0 to 100, with 100beingtheworstresult.Aminimumof27questions
Figure4.TheTriMedsystemwithradialpin-plate,buttresspin,andulnarpin-plate.
Figure5.Flowchartwithnumbersofpatientsinthediffer-enttreatmentgroupsandthenumberofoperations.
Patients entered581
Volar plate16
External fixation63
Internal fixation(TriMed)
51
Other3
Patients included518
Excluded63
Operated in all133
Primarily operated86
Redislocated47
Reduced212
Non-reduced220
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.

380 ActaOrthopaedica2008;79(3):376–385
mustbeansweredfortheresulttobevalidandinordertocalculatetheDASHscore.Duringthetimeofourstudyashorterform,QuickDASH,consist-ingof11questions fromtheoriginalDASHwasdevelopedandvalidated(Gummessonetal.2006).Wecorrelatedthe30-itemoriginalDASHusedinthisstudytothe11identicalquestionsintheshort-formQuickDASH.
TheDASHformwasgivenorsenttothepatientsdirectly after injury, and 3 and 12 months afterinjury.Areminder(withanewform)wassentafter2 weeks to patients who did not answer the firsttime.Ifmorethan3butlessthan6questionswereleftunanswered, thepatientswereasked tocom-pletetheformsothatascorecouldbecalculated.The patients mainly received the questionnairesbysurfacemailwithwritteninstructions,andonlyhospitalizedpatientsweregiventhequestionnairepersonally.
Reference group
Althoughthepatientswereinstructedtoreportanypre-fractureimpairment,itbecameclearearlyoninthestudythatrepliesfromthefirstenquiry,askingforpre-fracturesymptoms,provedinconsistent.Asmall number of patients reported their pre-frac-ture status as instructed but the majority insteadreportedtheirsymptomsonthefirstweekafterthefracture. To be able to present baseline data, thequestionnairewassenttoanage-andsex-matchedcontrol group of 109 individuals taken from theSwedishNationalPopulationRegistry.Theseref-erence controls came from the same catchment
areaandwerebornonthesamedayandwereofthe same sex as a randomly selected fraction oftheradiusfracturecohort(Table1).Inanaccom-panyingletter,weaskedthesepeopletofillintheDASHformandalsotostatewhethertheyhadhadapreviouswristfracture.75ofthe109(69%)indi-vidualsresponded.
Statistics
DASH data are ordinal; they showed a skeweddistributionandthereforenon-parametricanalyseswereused,andthedatawerepresentedasmedianwithinterquartilerange.Meanandstandarddevia-tionareincludedinthetablestoenablecomparisonwithpreviouslypublishedstudies.Alinearmixed-effects model was used for multivariate analysis.Age, side of fracture, type of treatment, opera-tion due to primary or secondary instability, andwhether the patient was operated by a hand sur-geonoranorthopedicsurgeonwereusedasfixedeffects and with random effect for each patient.Forgroupcomparisons,Mann-Whitneytestswereused. Correlation (Spearman) was determinedbetweenDASHandageat3and12monthsaftertheinjury,andalsobetweenstandardDASHformsandtheshorterQuickDASH.Effectsizewascalcu-latedanddefinedasmeanchangeinscoredividedbythestandarddeviationofthefirstscore.Effectsizesof0.2wereconsideredsmall,0.5moderate,and > 0.8 large (Roos et al. 1998). The statisti-cal analyses were performed with SPSS 14.0 forWindows. For calculation of power, we used PSpowerandsamplesizecalculations(http://biostat.
Table 1. Baseline data for responders and non-responders to the questionnaire and for the control group
All Responders Responders Non- Excluded Control included 3month 1year responders group (n=518) (n=357) (n=360) (n=88) (n=63) (n=75)
Age(range) 60(19–93) 61(19–93) 59(20–93) 61(19–92) 72(18–97) 63(22–91)Sex(%) Female 77 79 78 69 75 83 Male 23 21 22 31 25 17Fracturedside(%) Left 60 61 60 60 59 Right 40 39 39 39 40Primarytreatment(%) Cast 42 41 40 50 51 Reposition 41 43 43 30 14 Operation 17 17 17 20 35
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.

ActaOrthopaedica2008;79(3):376–385 381
mc.vanderbilt.edu/twiki/bin/view/Main/PowerS-ampleSize).
Results
The3-monthquestionnairewascompletedby389(75%)patientsandthe12-monthquestionnaireby389 (75%) patients of the 518 initially recorded.7%and6%hadmorethan3unansweredquestionsat7and12months,respectively.Thus,theirques-tionnairescouldnotbeusedforanalysisand357and360forms,respectively,wereusedforanalysis.Elderlypatients(osteoporoticmenover60yearsofageandosteoporoticwomenover50years)moreoftenfilledouttheformincorrectly(8%)thantheyounger group (1%).At 3 months, there was nostatisticallysignificantdifferencebetweenthenon-respondersandpatientswithinvalidatedforms(i.e.morethan3questionsunanswered)regardingage,sex,injuredside,typeoftreatment,ortypeofoper-ation.At 12 months, the patients who respondedand had valid forms were younger than the non-respondents (mean age 58 and 61 years, respec-tively). Also, the proportion of responders withfracturesrequiringanoperationwaslower.
AmultivariateanalysisrevealedaworseDASHscoreforfracturesthatwerereducedbutnotoper-ated(p=0.003),aworseDASHscorewithincreas-ingage(p<0.001),andabetterDASHscoreat12monthsthanat3months(p<0.001).
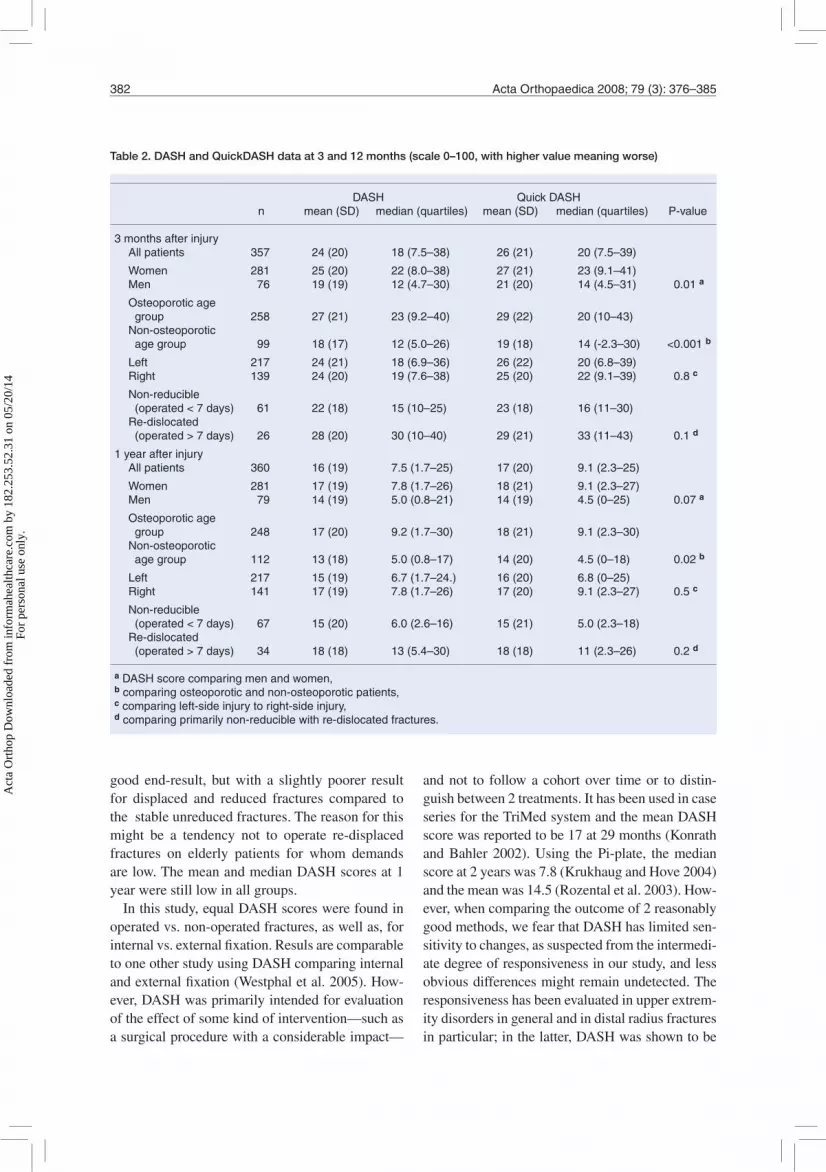
ThemedianDASHscoreforthewholegroupwas18at3monthsand7.5at12months(p<0.001).Intheolderosteoporoticagegroup,DASHscoreswere23and9.2, respectively, (p<0.001)and inthe younger age group they were 12 and 5.0 (p< 0.001). There was a correlation between ageandDASHat 3months (r=0.33, p=0.01) andat12months (r=0.28,p=0.01).TherewasnostatisticallysignificantdifferenceinDASHscoresbetween fractures of the left and the right wrist.Womenscoredworsethanmenat3months(Table2),buttheywereolder(meanage63)thanthemalegroup(meanage52).
133patientswith135fractureswereoperated.87patientsintheoperatedgroupreturnedtheformat 3 months and 103 answered at 12 months.At3months,themedianDASHscorewas17intheunoperatedgroup:14forexternalfixation,15for
volarplate, and16 for theTri-Medgroup.At12months the scores were 5.8 for the unoperatedgroup,7.0forexternalfixation,4.3forvolarplate,and7.0fortheTri-Medgroup(Figure6).Patientswithprimarilystablefractures treatedwithacasthadamedianscoreof17at3monthsand4.2at12months.Patientswithreducedfracturestreatedwithclosedreductionandcastinghadscoresof22and12,respectively,andthegroupofpatientswithoperationastheprimarytreatmenthadscoresof15and5.5at3and12months(Table3).AcorrelationbetweenDASHandQuickDASHwasfoundbothat3months (r=0.984,p<0.001)andat1yearafterinjury(r=0.974,p<0.001)(Figure7).
Reference group
The median DASH score for the age- and sex-matched reference group was 2.5 (0–9.2) for thewhole group and 0.8 and 3.7, respectively, whenconsidered as younger and older age groups.There was a significant difference between theDASHscoreof thecontrolgroupandofpatientswithadistalradiusfractureevenafter12months(p <0.001), both for the whole group and whentheyweredividedintogroupsofyoungerandolderindividuals(Table4).
Discussion
Ingeneral,patients suffering fromadistal radiusfracture, regardless of type of treatment, end upwithsomedegreeofdiscomfortandlossoffunc-tion in the first year. During the first 2 monthsafter injury, the patients have severe problemswith many daily activities but after 1 year theseproblems are minimal in the majority of cases(MacDermidetal.2003).Theotherpatientshaveresidual symptomsafter1year,andalthough thepercentageofthesepatientsmaybesmall,thehighincidenceofdistalradiusfracturemakesthisgrouplarge. Inourstudy,DASHscoresshowedasimi-lardecreasingpattern in the timeperiodbetween3and12months.TheDASHscorewashigherinthefracturepatientsafter1year(median7.5,mean17) than in the uninjured control group (median2.5, mean 8.3). The protocol, with all the weak-nessesofanon-randomizeddesign,appearstobeadequateasitbringsallfracturestoasimilarand
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.
382 ActaOrthopaedica2008;79(3):376–385
good end-result, but with a slightly poorer resultfor displaced and reduced fractures compared tothestableunreducedfractures.Thereasonforthismight be a tendency not to operate re-displacedfractures on elderly patients for whom demandsarelow.ThemeanandmedianDASHscoresat1yearwerestilllowinallgroups.
Inthisstudy,equalDASHscoreswerefoundinoperatedvs.non-operatedfractures,aswellas,forinternalvs.externalfixation.ResulsarecomparabletooneotherstudyusingDASHcomparinginternalandexternalfixation(Westphaletal.2005).How-ever,DASHwasprimarilyintendedforevaluationoftheeffectofsomekindofintervention—suchasasurgicalprocedurewithaconsiderableimpact—
andnot to followacohortover timeor todistin-guishbetween2treatments.IthasbeenusedincaseseriesfortheTriMedsystemandthemeanDASHscorewasreportedtobe17at29months(KonrathandBahler2002).Using thePi-plate, themedianscoreat2yearswas7.8(KrukhaugandHove2004)andthemeanwas14.5(Rozentaletal.2003).How-ever,whencomparingtheoutcomeof2reasonablygoodmethods,wefearthatDASHhaslimitedsen-sitivitytochanges,assuspectedfromtheintermedi-atedegreeofresponsivenessinourstudy,andlessobviousdifferencesmightremainundetected.Theresponsivenesshasbeenevaluatedinupperextrem-itydisordersingeneralandindistalradiusfracturesinparticular;inthelatter,DASHwasshowntobe
Table 2. DASH and QuickDASH data at 3 and 12 months (scale 0–100, with higher value meaning worse)
DASH QuickDASH n mean(SD) median(quartiles) mean(SD) median(quartiles) P-value
3monthsafterinjury Allpatients 357 24(20) 18(7.5–38) 26(21) 20(7.5–39)
Women 281 25(20) 22(8.0–38) 27(21) 23(9.1–41) Men 76 19(19) 12(4.7–30) 21(20) 14(4.5–31) 0.01a
Osteoporoticage group 258 27(21) 23(9.2–40) 29(22) 20(10–43) Non-osteoporotic agegroup 99 18(17) 12(5.0–26) 19(18) 14(-2.3–30) <0.001b
Left 217 24(21) 18(6.9–36) 26(22) 20(6.8–39) Right 139 24(20) 19(7.6–38) 25(20) 22(9.1–39) 0.8c
Non-reducible (operated<7days) 61 22(18) 15(10–25) 23(18) 16(11–30) Re-dislocated (operated>7days) 26 28(20) 30(10–40) 29(21) 33(11–43) 0.1d
1yearafterinjury Allpatients 360 16(19) 7.5(1.7–25) 17(20) 9.1(2.3–25)
Women 281 17(19) 7.8(1.7–26) 18(21) 9.1(2.3–27) Men 79 14(19) 5.0(0.8–21) 14(19) 4.5(0–25) 0.07a
Osteoporoticage group 248 17(20) 9.2(1.7–30) 18(21) 9.1(2.3–30) Non-osteoporotic agegroup 112 13(18) 5.0(0.8–17) 14(20) 4.5(0–18) 0.02b
Left 217 15(19) 6.7(1.7–24.) 16(20) 6.8(0–25) Right 141 17(19) 7.8(1.7–26) 17(20) 9.1(2.3–27) 0.5c
Non-reducible (operated<7days) 67 15(20) 6.0(2.6–16) 15(21) 5.0(2.3–18) Re-dislocated (operated>7days) 34 18(18) 13(5.4–30) 18(18) 11(2.3–26) 0.2d
aDASHscorecomparingmenandwomen,bcomparingosteoporoticandnon-osteoporoticpatients,ccomparingleft-sideinjurytoright-sideinjury,dcomparingprimarilynon-reduciblewithre-dislocatedfractures.
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.

ActaOrthopaedica2008;79(3):376–385 383
Figure6.DASHscoresforunoperatedpatientscomparedtoscoresforoperatedpatients.A.Unoperated.B.Operatedwithexternalfixation.C.OperatedwiththeTriMedsystem.D.Volarfracturesoperatedwithavolarplate.Theboxplotontheleftshowstheresultsat3monthsandthatontherightat12months.
DASH – 3 months100
80
60
40
20
0A
(n=270)B
(n=39)C
(n=35)D
(n=10)
DASH – 12 months100
80
60
40
20
0A
(n=259)B
(n=43)C
(n=43)D
(n=12)
Table 4. DASH data at 12 months divided into age and gender groups and compared to the reference group
Patients Referencegroup DASHvalue DASHvalue1yearafterinjury n median(quartiles) n median(quartiles) P-valuea
Allpatients 360 7.5(1.7–25) 71 2.5(0–9.2) <0.001
Women 281 7.8(1.7–26) 59 2.6(0–9.2) <0.001Men 79 5.0(0.8–21) 12 0.8(0–11) 0.4
Oldergroup 248 9.2(1.7–30) 54 3.8(0–10) 0.02Youngergroup 112 5.0(0.8–17) 17 0.8(0–2.9) 0.02
ap-valueincomparisonwiththecontrolgroup.
Table 3. DASH scores at 3 and 12 months (scale 0–100, with higher values meaning worse)
DASH n mean(95%CI) median(quartiles) P-value
3monthsafterinjury Undisplaced,casted 145 23(20–27) 17(4.4–38) Reduced,casted 157 26(23–29) 22(11–38) 0.06a Primaryoperated 55 22(16–27) 15(8.8–26) 0.8b,0.1c
1yearafterinjury Undisplaced,casted 143 15(11–18) 4.2(0.8–22) Reduced,casted 155 17(14–20) 12(2.6–28) 0.01a Primaryoperated 62 16(10–21) 6.0(2.6–18) 0.2b,0.3c
aReducedfracturescomparedtostableundisplacedfractures.bOperatedfracturescomparedtostableundisplacedfractures.cOperatedfracturescomparedtoreducedfractures.
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.

384 ActaOrthopaedica2008;79(3):376–385
sensitivewith regard tochanges from the timeofinjury to6months after injurywith ahigh effectsizeof2.3(MacDermidetal.2000).
In our study, the patients did not fully under-stand how to fill in the baseline protocol. Somepatientsreportedpre-fracturedataandotherspost-fracturedata,whichmade thebaselinedatause-less.When we instead used our normal materialas baseline data, there was a large effect size of1.12forthe3-monthresultsandamoderateeffectsize of 0.54 for the 12-month results. Perhaps amoresensitivetoolwouldbenecessaryinordertoevaluateachangeovertime,suchasimprovementbetween3and12months,withoutadrasticeventsuch as anoperationor fracture. In this study, astatistically significant subjective improvementoccurredbetween3and12months,asexpected,butthecalculatedeffectsizewasamoderate0.37.UsinganoutcomeinstrumentwiththesensitivityofDASH,eveninaratherlargegroupstudysuchas ours (with more than 100 operated patients)itwasnotpossibletodeterminetheeffectof theoperation technique or to differentiate a primaryoperationfromasecondaryone.Toourknowledge,norandomizedpublishedstudyhasbeencapableof showingadifference in theoutcomebetween2 surgical methods using DASH. If one intendstodesignarandomizedstudyoutoftheoutcomedatainthisstudywith85%poweratp=0.05,66patientsmustbeincludedineachgrouptoshowadifferenceinDASHscoreof10scalesteps,which
isconsideredtobetheminimalimportantchange(Gummessonetal.2003). Insteadof includingalargenumberofpatients,itwouldbepreferabletouseanoutcomeinstrumentthatismoresensitivetosmallerchangesorsmallerdifferencesbetweentreatment modalities. Perhaps a more sensitiveoutcome instrument should be designed beforeconductingrandomizedtrialstocomparedifferenttreatmentsincluding,forexample,differentsurgi-calmethods.
Ingeneral,DASHasauniversalfollow-upinstru-ment required substantial administrative work toensure an acceptable frequency of replies. Manypatients did not fill in all the questions, as theydid not feel that some of the questions were rel-evanttotheirsituation.If3ormorequestionswereunanswered, the reply was not considered validandhad tobedisregarded. Inacohortconsistingofmainlyelderlypatients, agedidplayapart inthefrequencyofinvalidreplies.Inthegroupover60yearsofage,8%sentininvalidformsascom-paredto1%intheyoungeragegroup.Manyoftheelderlypatientswerementallyunfit,andrelativesornursinghomestaffreportedthattherespondentwasunabletofillintheform.Areplyfrequencyof75%mustberegardedasadequateinacohortlikethis, but it could probably be improved by usingasimpleroutcome instrument.Theshort formofDASH,QuickDASH,containsonly11questions.It may improve the response rate (Figure 7) andcouldbeusedinsteadofthefullDASH.
Figure7.Correlationbetweenthefull30-itemDASHscore(y-axis)andthe11-itemQuickDASH(x-axis),at3months(leftpanel)(Spearmancorrelation0.98,p<0.001)andat1year(rightpanel)(Spearmancorrelation0.97,p<0.001).
100
80
60
40
20
00 20 40 60 80 100
QuickDASH
DASH100
80
60
40
20
00 20 40 60 80 100
QuickDASH
DASH
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.

ActaOrthopaedica2008;79(3):376–385 385
Inconclusion,itseemsthatthepatientsstillhaveresidualsymptomsat3monthsbutmostof themhavereturnedtothebaselineby1year.Ourtreat-mentprotocolmeansthatsimilar,goodsubjectiveend-results are achieved regardless of the initialseverity of the fracture. However, patients withunstable fractures, initially reduced and treatedwith a cast but later operated on, tended to havepoorer scores. This subgroup requires furtherinvestigation.
Contributions of authorsAA:settingupofproject,planning,datacollection,interpre-tationofdata,statistics,andwritingofthemanuscript.MT:setting up of project, planning, statistics, interpretation ofdata,andwritingofthemanuscript.PK:settingupofproj-ect,planning,andwritingofthemanuscript.
The authorswish to thankEwaPersson for excellent sec-retarialassistanceandstatisticianFredrikNilsson,Compe-tenceCenterforClinicalResearch,RegionSkåne(RSKC),forstatisticaladvice.TheprojectwassupportedbyRegionSkåne, Lund University Hospital, the Swedish MedicalResearch Council (project 09509), the Alfred ÖsterlundFoundation, the Greta and Johan Kock Foundation, theMaggieStephensFoundation,theFoundationforSupportofFunctionallyHinderedPatientsinSkåne,andtheFacultyofMedicine,LundUniversity.
AtroshiI,GummessonC,AnderssonB,DahlgrenE,Johans-son A. The disabilities of the arm, shoulder and hand(DASH) outcome questionnaire: reliability and validityof the Swedish version evaluated in 176 patients.ActaOrthopScand2000;71(6):613-8.
GummessonC,AtroshiI,EkdahlC.Thedisabilitiesofthearm,shoulderandhand(DASH)outcomequestionnaire:longitudinal construct validity and measuring self-ratedhealthchangeaftersurgery.BMCMusculoskeletDisord2003;4(1):11.
Gummesson C,Ward M M,Atroshi I.The shortened dis-abilities of the arm, shoulder and hand questionnaire(QuickDASH):validityandreliabilitybasedonresponseswithinthefull-lengthDASH.BMCMusculoskeletDisord2006;7:44.
Handoll H H, Madhok R. Conservative interventions fortreatingdistal radial fractures inadults.CochraneData-baseSystRev2003a;(2):CD000314.
HandollHH,MadhokR.Surgicalinterventionsfortreatingdistalradialfracturesinadults.CochraneDatabaseSystRev2003b;(3):CD003209.
HudakPL,AmadioPC,BombardierC.Developmentofanupper extremity outcome measure: the DASH (disabili-tiesofthearm,shoulderandhand)[corrected].TheUpperExtremityCollaborativeGroup(UECG).AmJIndMed1996;29(6):602-8.
Keating J F, Court-Brown C M, McQueen M M. Internalfixationofvolar-displaceddistalradialfractures.JBoneJointSurg(Br)1994;76(3):401-5.
KonrathGA,BahlerS.Openreductionandinternalfixationofunstabledistalradiusfractures:resultsusingthetrimedfixationsystem.JOrthopTrauma2002;16(8):578-85.
KopylovP,JohnellO,Redlund-JohnellI,BengnerU.Frac-turesofthedistalendoftheradiusinyoungadults:a30-yearfollow-up.JHandSurg(Br)1993;18(1):45-9.
KrukhaugY, Hove L M. Experience with theAO Pi-platefordisplacedintra-articularfracturesofthedistalradius.ScandJPlastReconstrSurgHandSurg2004;38(5):293-6.
Lindau T. Distal radial fractures and effects of associatedligamentinjuries.LundUniversityThesis2000.
LindauT,AspenbergP,ArnerM,Redlundh-JohnellI,Hag-bergL.Fracturesofthedistalforearminyoungadults.Anepidemiologic description of 341 patients.Acta OrthopScand1999;70(2):124-8.
MacDermidJC,RichardsRS,DonnerA,BellamyN,RothJH.Responsivenessoftheshortform-36,disabilityofthearm,shoulder,andhandquestionnaire,patient-ratedwristevaluation, and physical impairment measurements inevaluatingrecoveryafteradistalradiusfracture.JHandSurg(Am)2000;25(2):330-40.
MacDermidJC,RothJH,RichardsRS.Painanddisabil-ityreportedintheyearfollowingadistalradiusfracture:acohortstudy.BMCMusculoskeletDisord2003;4(1):24.
Roos E M, Roos H P, Lohmander L S, Ekdahl C, Beyn-nonBD.KneeInjuryandOsteoarthritisOutcomeScore(KOOS)—development of a self-administered outcomemeasure.JOrthopSportsPhysTher1998;28(2):88-96.
RozentalTD,BeredjiklianPK,BozentkaDJ.Functionaloutcomeandcomplicationsfollowingtwotypesofdorsalplating for unstable fractures of the distal part of theradius.JBoneJointSurg(Am)2003;85(10):1956-60.
SchnallSB,KimBJ,AbramoA,KopylovP.Fixationofdistal radius fracturesusinga fragment-specific system.ClinOrthop2006;(445):51-7.
WestphalT,PiatekS,SchubertS,WincklerS.Outcomeaftersurgeryofdistalradiusfractures:nodifferencesbetweenexternal fixation and ORIF. Arch Orthop Trauma Surg2005;125(8):507-14.
Act
a O
rtho
p D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 18
2.25
3.52
.31
on 0
5/20
/14
For
pers
onal
use
onl
y.
Related Documents











