EUROArray HLA-DQ2/DQ8 Direct Test instruction for the molecular genetic test ORDER NO. PARAMETER SUBSTRATE FORMAT MN 5321-0803 MN 5321-0505 MN 5321-1005 MN 5321-2005 EUROArray HLA-DQ2/DQ8 Direct DNA microarray 08 x 03 (024) 05 x 05 (025) 10 x 05 (050) 20 x 05 (100) Indication: The test system is exclusively designed for the molecular genetic in vitro determination of disease-associated HLA-DQA1 and HLA-DQB1 alleles coding for the alpha- and beta-subunits of the HLA-DQ2 and HLA-DQ8 molecules, respectively. For DQ2, both isoforms, HLA-DQ2.2 and HLA-DQ2.5 are detected. These genetic markers are used for the exclusion of gluten-sensitive enteropathy (coeliac disease, non-tropical sprue) in the following cases: doubtful biopsy results, ambiguous serology (especially in children under two years old), patients on a gluten-free diet with inconclusive diagnosis, clarification of the genetic predisposition of first-degree relatives, patients with Duhring’s dermatitis, type I diabetes mellitus or Down’s syndrome, and differentiation from other intestinal diseases. The test should not be used for tissue typing. Application: The EUROArray HLA-DQ2/DQ8 direct test system enables fast and easy HLA-DQ2/DQ8 detection to assess the genetic predisposition to coeliac disease and other HLA-DQ2/DQ8-associated diseases. In the direct method full blood samples can be used directly without the need of separate DNA isolation. Principles of the test: EDTA blood (direct method) or isolated genomic DNA of the patient is used as sample material. In the direct method genomic DNA of blood cells is prepared for PCR by pretreating the blood with the extraction solution provided in the test kit according to a short protocol. In the first reaction step, several sections of the HLA-DQA1 and HLA-DQB1 genes are amplified from the extract or, alternatively, from a genomic patient DNA sample by polymerase chain reaction (PCR). During their formation, the PCR products are labelled with a fluorescent dye. In the second reaction step, the PCR products are analysed using the microarray, which contains immobilised probes that are complementary to the amplified DNA. The specific binding (hybridisation) of the fluorescing PCR product to the corresponding microarray spot is detected using a special microarray scanner (EUROIMMUN). All spot signals are evaluated automatically using the EUROArrayScan software. Fluorescence signals at the different HLA-DQA1- and HLA-DQB1-specific spots indicate the presence of the respective HLA-DQA1 and HLA-DQB1 alleles in the patient DNA sample, and thus possibly also the presence of HLA-DQ2.2, HLA-DQ2.5 and/or HLA-DQ8. Contents of the test kit (e.g. MN 5321-2005-V): Description Storage location Format Symbol 1. Slide HLA-DQ2/DQ8 Direct with 5 test fields post-PCR 20 pieces SLIDE 2. PCR Mix A HLA-DQ2/DQ8 Direct (green cap), ready for use pre-PCR 1 x 1.2 ml PCR MIX A 3. PCR Mix B HLA-DQ2/DQ8 Direct (yellow cap), ready for use pre-PCR 1 x 1.2 ml PCR MIX B 4. DNA negative control 2 (brown cap), ready for use pre-PCR 1 x 1.2 ml CONTROL 5. Hybridisation buffer HB-B (red cap), ready for use post-PCR 1 x 8 ml HYB BUFFER 6. Extraction solution 1 (blue cap), ready for use pre-PCR 2 x 1.1 ml EXT SOLUT 1 7. Extraction solution 2 (violet cap), ready for use pre-PCR 2 x 1.1 ml EXT SOLUT 2 8. Test instruction - 1 booklet LOT. Lot description Storage temperature IVD. In vitro diagnostic medical device Unopened usable until MN_5321-V_A_UK_C01.doc Version: 12/09/2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EUROArray HLA-DQ2/DQ8 Direct Test instruction for the molecular genetic test
ORDER NO. PARAMETER SUBSTRATE FORMAT
MN 5321-0803 MN 5321-0505 MN 5321-1005 MN 5321-2005
EUROArray HLA-DQ2/DQ8 Direct
DNA microarray
08 x 03 (024) 05 x 05 (025) 10 x 05 (050) 20 x 05 (100)
Indication: The test system is exclusively designed for the molecular genetic in vitro determination of disease-associated HLA-DQA1 and HLA-DQB1 alleles coding for the alpha- and beta-subunits of the HLA-DQ2 and HLA-DQ8 molecules, respectively. For DQ2, both isoforms, HLA-DQ2.2 and HLA-DQ2.5 are detected. These genetic markers are used for the exclusion of gluten-sensitive enteropathy (coeliac disease, non-tropical sprue) in the following cases: doubtful biopsy results, ambiguous serology (especially in children under two years old), patients on a gluten-free diet with inconclusive diagnosis, clarification of the genetic predisposition of first-degree relatives, patients with Duhring’s dermatitis, type I diabetes mellitus or Down’s syndrome, and differentiation from other intestinal diseases. The test should not be used for tissue typing. Application: The EUROArray HLA-DQ2/DQ8 direct test system enables fast and easy HLA-DQ2/DQ8 detection to assess the genetic predisposition to coeliac disease and other HLA-DQ2/DQ8-associated diseases. In the direct method full blood samples can be used directly without the need of separate DNA isolation. Principles of the test: EDTA blood (direct method) or isolated genomic DNA of the patient is used as sample material. In the direct method genomic DNA of blood cells is prepared for PCR by pretreating the blood with the extraction solution provided in the test kit according to a short protocol. In the first reaction step, several sections of the HLA-DQA1 and HLA-DQB1 genes are amplified from the extract or, alternatively, from a genomic patient DNA sample by polymerase chain reaction (PCR). During their formation, the PCR products are labelled with a fluorescent dye. In the second reaction step, the PCR products are analysed using the microarray, which contains immobilised probes that are complementary to the amplified DNA. The specific binding (hybridisation) of the fluorescing PCR product to the corresponding microarray spot is detected using a special microarray scanner (EUROIMMUN). All spot signals are evaluated automatically using the EUROArrayScan software. Fluorescence signals at the different HLA-DQA1- and HLA-DQB1-specific spots indicate the presence of the respective HLA-DQA1 and HLA-DQB1 alleles in the patient DNA sample, and thus possibly also the presence of HLA-DQ2.2, HLA-DQ2.5 and/or HLA-DQ8. Contents of the test kit (e.g. MN 5321-2005-V): Description Storage location Format Symbol1. Slide HLA-DQ2/DQ8 Direct
with 5 test fields post-PCR 20 pieces SLIDE
2. PCR Mix A HLA-DQ2/DQ8 Direct (green cap), ready for use
pre-PCR 1 x 1.2 ml PCR MIX A
3. PCR Mix B HLA-DQ2/DQ8 Direct (yellow cap),ready for use
pre-PCR 1 x 1.2 ml PCR MIX B
4. DNA negative control 2 (brown cap), ready for use
pre-PCR 1 x 1.2 ml CONTROL
5. Hybridisation buffer HB-B (red cap), ready for use
post-PCR 1 x 8 ml HYB BUFFER
6. Extraction solution 1 (blue cap), ready for use
pre-PCR 2 x 1.1 ml EXT SOLUT 1
7. Extraction solution 2 (violet cap), ready for use
pre-PCR 2 x 1.1 ml EXT SOLUT 2
8. Test instruction - 1 booklet .LOT. Lot description Storage temperature .IVD. In vitro diagnostic medical device Unopened usable until
MN_5321-V_A_UK_C01.doc
Version: 12/09/2017

2
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Storage and stability: The HLA-DQ2/DQ8 Direct PCR mixes A and B, the DNA negative control 2 and extraction solutions 1 and 2 should be removed from the test kit immediately after delivery. PCR Mixes A and B and the DNA negative control 2 should be stored in the pre-PCR area at -18°C to -25°C and protected from light . Store extraction solutions 1 and 2 in the pre-PCR area at room temperature (+18°C to +25°C). Store the outer packaging containing the hybridisation buffer and slides in the post-PCR area away from light at a temperature of +2°C to +8°C. For further information concerning storage and handling of test components see “Preparation and stability of reagents and materials”. The stability of components when stored correctly is given on the labels. Waste disposal: Patient samples, controls and slides are to be handled as potentially infectious materials. All reagents must be disposed of in accordance with local disposal regulations. Additional required materials: Pre-PCR area: - Mini centrifuge for 0.2 ml and 1.5 ml reaction vessels, EUROIMMUN order no. YG 0612-0101
or similar - Laboratory shaker for reagent vessels (“Vortex”), EUROIMMUN order no. YG 0641-0101 or
similar - PCR cooling rack for 0.2 ml reaction vessels (“IsoFreeze Tube-Rack”) order no. ZG 0617-0101
or similar - Pre-PCR rack for 1.5 ml reaction vessels - PCR cooling rack for 1.5 ml reaction vessels (“IsoPack and IsoRack”), EUROIMMUN order no.
ZG 0618-0101 or similar - Pipettes (adjustable volume) and pipette tips with filter, 20, 200 and 1000 µl, DNA and DNase
free - Reaction vessels 0.2 ml suited for thermocycler, DNA and DNase free (recommended:
Multiply® µStripPro strips of 8 tubes with attached caps, Sarstedt, order no. 72.991.002) - Reaction vessels 1.5 ml, DNA and DNase free (recommended: Micro tube 1.5 ml SafeSeal,
Sarstedt, order no. 72.706.400) - Disposable gloves Post-PCR area: - EUROArrayScanner (incl. EUROArrayScan software), EUROIMMUN order no. YG 0602-0101
or EUROArrayScan system (EUROIMMUN Microarray Scanner incl. EUROArrayScan software), EUROIMMUN order no. YG 0601-0101
- Hybridisation station - Hybridisation station (with one incubator insert), EUROIMMUN order no. YG 0615-0101
(AccuBlock Digital Dry Bath, dual block capacity, order no. D 1200-230 V, Labnet International, Inc + Incubator insert for TITERPLANE reagent tray, EUROIMMUN order no. YG 0631-0105)
- Hybridisation station (with two incubator inserts), EUROIMMUN order no. YG 0615-0101-1 (BSH1004 Benchmark Digital Dry Bath, four positions, order no. BSH1004 (-E), Benchmark Scientific, Inc. + 2x Incubator insert for TITERPLANE reagent tray, EUROIMMUN, order no. YG 0631-0105)
- TITERPLANE reagent tray for EUROArray slides, EUROIMMUN order no. ZM 9999-0105 - Cleaning box for TITERPLANE reagent tray - Pipettes (adjustable volume) and pipette tips with filter, 100 µl, DNase free - Wash buffer 1 to 3 consisting of:
- WASH REAGENT 1, EUROIMMUN order no. ZM 0121-0050 - WASH REAGENT 2, EUROIMMUN order no. ZM 0122-0012 - Pipettes and/or measuring cylinder for measuring of the required volumes (see below)
or - Wash buffer set, EUROIMMUN order no. ZM 0123-0101
- 3 vessels or bottles for wash buffer 1 to 3, according to the batch volumes (see below) - 4 wash cuvettes (L x W x H in mm: 105 x 85 x 70) or similar

3
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
- Glass frame for EUROArray slides, compatible with wash cuvettes - Pair of tweezers - Post-PCR rack for 0.2 ml reaction vessels - Felt-tip pen, water-proof, black, Stabilo OHPen universal or similar - Canned compressed air or compressed air e.g. from VWR International GmbH order no.
291-1201 or similar - Distilled water - Laboratory tissue, lint-free - Disposable gloves Amplification area (or post-PCR area) - Thermocycler (recommendation: Applied Biosystems 2720 Thermal Cycler, Eppendorf
Mastercycler nexus SX1 (with silver block), BioRad T100™ Thermal Cycler or Applied Biosystems SimpliAmp Thermal Cycler)
Warning: In PCR, the relevant sections of the sample DNA are amplified millionfold. The smallest amounts of PCR products can lead to incorrect results, when they contaminate, e.g. via aerosols, the sample material (sample blood or DNA solution), the reagents for DNA extraction or the PCR reagents of this test kit. For this reason, the test should be performed in two separate rooms (pre-PCR and post-PCR area). Instruments, reagents and materials should be stored and used only in the area where they belong. Preferably, the thermocycler should be located in a third area (amplification area) situated between the pre- and the post-PCR area. If this is not feasible, the instrument should be set up in the post-PCR area. Use new and sterile filter pipette tips for every pipetting step. During the entire test procedure, we recommend using disposable gloves and changing them frequently. All work surfaces, devices and tools, e.g. racks, should be cleaned with DNA-degrading agents, e.g. diluted hypochlorite solution (see e.g. UK Standards for Microbiology Investigations, Q4i4.4, Dec. 2013) on a regular basis, ideally after each use. Hint: Some disinfectants, e.g. diluted ethanol, are not suited to degrade DNA. Please contact EUROIMMUN for further information on this matter.
Preparation and stability of reagents and materials Note: Unless stated otherwise, after initial opening the reagents are stable until the expiry date, when stored under the stated conditions and protected from contamination. - -Extraction solution 1 (blue cap) and 2 (violet cap): ready for use. Storage at +18°C to
+25°C in the pre-PCR range. - HLA-DQ2/DQ8 Direct PCR Mix
- PCR Mix A: green cap - PCR Mix B*: yellow cap
Ready for use. Protect from light and store in pre-PCR area at -18°C to -25°C. Before use, thaw at +2°C to +8°C for a short period (do not exceed 60 minutes).
- DNA negative control 2 (brown cap): Ready for use. Store in pre-PCR area at -18°C up to
-25°C. Before use thaw at +2°C up to +8°C. Do not leave at +2°C up to +8°C for more than 60 minutes.
- Hybridisation buffer (red cap): Ready for use. Protect from light and store in
post-PCR area at +2°C to +8°C. - Slides: Ready for use. Protect from light and store in post-PCR area at +2°C to +8°C. Open
the protective pouch only when the slide has reached room temperature (+18°C up to +25°C; condensed water can damage the substrate). Mark with the recommended felt-tip pen only. Do not touch the BIOCHIPs. After the protective pouch has been opened, the slide should be used within 30 minutes. If the protective pouch is damaged, the slide must not be used for diagnostics.

4
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
- Reagent tray: Cleaning: Remains of the incubation must be rinsed away using cold water directly after incubation. Wipe the tray thoroughly by hand (using disposable gloves!) with diluted WASH REAGENT 2 (1 part WASH REAGENT 2 + 99 parts distilled water) and store in diluted WASH REAGENT 2 for several hours (overnight). Then rinse the tray thoroughly with distilled water and air dry. Disinfection: with a suitable agent, e.g. Sekucid® concentrate (Ecolab GmbH) according to the manufacturer.
- WASH REAGENT 1**: Ready for use. Store in post-PCR area at room temperature (+18°C to
+25°C). - WASH REAGENT 2**: Ready for use. Store in post-PCR area at room temperature (+18°C to
+25°C). - Wash buffer set **: Ready for use. Store at room temperature (+18°C to +25°C) in post-PCR
area. * PCR Mix B contains GoTaq® MDx Hot Start DNA polymerase manufactured by Promega
Corporation for distribution by EUROIMMUN AG. Licensed for Promega under U.S. Patent no. 5338671 and 5587287 and corresponding related patents.
** Check for the formation of precipitates before each use of WASH REAGENT 1 and 2 and the
wash buffer set. Any precipitate must be completely dissolved by warming the bottle to around +37°C and mixing the solution thoroughly.
Preparation of wash buffer 1 to 3 if WASH REAGENT 1 and 2 (ZM 0121-0050 and ZM 0122-0012) are used: Preparation in post-PCR area. It is important to mix the individual solutions in the correct order otherwise the solution will become cloudy. - Wash buffer 1: Mix 25 ml of WASH REAGENT 1, approx. 400 ml of distilled water and 5 ml of
WASH REAGENT 2. Add distilled water to obtain a total volume of 500 ml and mix thoroughly. - Wash buffer 2: Mix 1.25 ml of WASH REAGENT 1, approx. 200 ml of distilled water and 2.5 ml
of WASH REAGENT 2. Add distilled water to obtain a total volume of 250 ml and mix thoroughly.
- Wash buffer 3: Pipette 12.5 ml of WASH REAGENT 1, then add distilled water to obtain a total
volume of 250 ml and mix thoroughly. The prepared buffers are sufficient for one wash cycle (max. 10 slides). The wash buffers can alternatively be prepared in large stock volumes. They are stable for 2 weeks at room temperature (+18°C to +25°C) as long as clean vessels are used. Buffers containing microbiological contamination must not be used. Preparation of wash buffers 1 to 3 if the wash buffer set is used (ZM 0123-0101): For the preparation of wash buffers 1 to 3 refer to the instructions in the wash buffer set. Note: Before each use, the wash buffers should be checked to ensure that they are clear and free of particles. Precipitates, which can form at low storage temperatures, must be solubilised before the buffer is used, if necessary by warming. The prepared solutions must be brought to room temperature (+18°C to +25°C) for the wash steps. Warning: Some of the reagents and controls contain sodium dodecyl sulphate (SDS), acids or bases or the agent sodium azide in a non-declarable concentration. Avoid skin contact.

5
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Sample material The sample material used is either EDTA blood (direct method) or isolated genomic DNA, which meets the specifications given below. EDTA blood (direct method): This test system was validated using EDTA blood samples (S-Monovette® Potassium EDTA, Sarstedt). For successful test performance the patient blood must be mixed thoroughly with EDTA directly after withdrawal to avoid (even partial) coagulation. The blood sample is then cooled immediately. We recommend not storing the blood sample at +2°C to +8°C for more than two weeks before DNA extraction. Freeze at -18°C to -25°C for longer storage (max. 6 months). The blood samples should only be stored and extracted in the pre-PCR area. DNA extraction should be carried out as described for the “direct method” (see below) immediately before the test performance. Isolated genomic DNA: The DNA concentration in the patient sample should be between 5 and 60 ng/µl. The DNA should be of a high level of purity (recommended OD 260:280 ratio of 1.6 to 2.0). A too high or too low DNA concentration may lead to invalid results or, in extreme cases, to false results. This test system was validated for DNA samples isolated from EDTA blood by means of the “QIAamp® DSP DNA Blood Mini Kit” (QIAGEN) according to the manufacturer’s specifications. The system is CE-labelled by the manufacturer in accordance with the IVD directive. The elution was performed using 200 µl of the elution buffer. When the isolation method above has been used, the obtained DNA solutions can be used directly and undiluted. If other isolation methods are used, the concentration of the DNA solution should be adjusted accordingly to meet the above specifications and the purity of the DNA should be checked. For successful DNA extraction the blood must be mixed thoroughly with EDTA directly after withdrawal to avoid (even partial) coagulation. Cool sample immediately (at +2°C to +8°C) or deep-freeze for longer storage. For storage and isolation of the blood sample follow the instructions of the manufacturer with respect to the used DNA isolation system. The isolated sample DNA can generally be stored at +2°C to +8°C for several days. Storage at -18°C to -25°C or below is usually also possible and increases the stability to 1 year or more. For storage and stability of isolated DNA samples follow the specifications of the manufacturer with respect to the used DNA isolation system. Storage of the blood samples, isolation of the DNA and storage of the DNA samples should only be performed in the pre-PCR area.
6
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
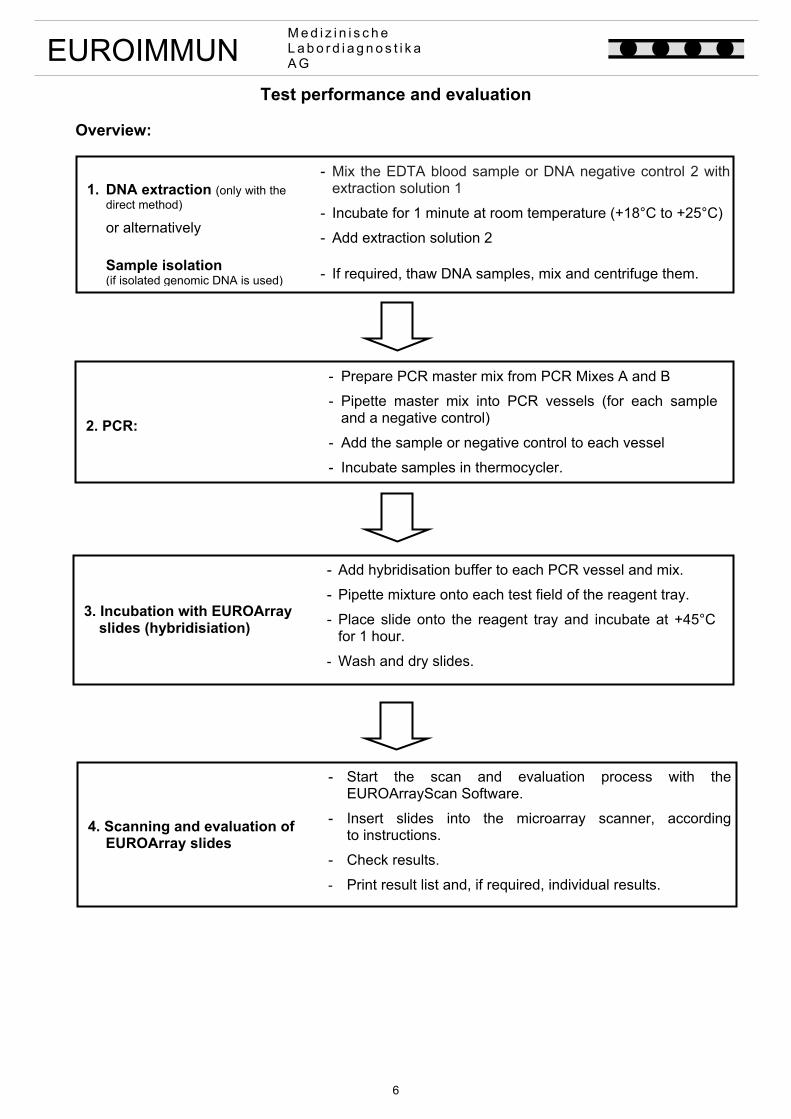
Test performance and evaluation Overview:
Fehler!
1. DNA extraction (only with the direct method)
or alternatively
- Mix the EDTA blood sample or DNA negative control 2 with extraction solution 1
- Incubate for 1 minute at room temperature (+18°C to +25°C)
- Add extraction solution 2
Sample isolation (if isolated genomic DNA is used)
- If required, thaw DNA samples, mix and centrifuge them.
4. Scanning and evaluation of EUROArray slides
- Start the scan and evaluation process with the EUROArrayScan Software.
- Insert slides into the microarray scanner, accordingto instructions.
- Check results.
- Print result list and, if required, individual results.
3. Incubation with EUROArray slides (hybridisiation)
- Add hybridisation buffer to each PCR vessel and mix.
- Pipette mixture onto each test field of the reagent tray.
- Place slide onto the reagent tray and incubate at +45°C for 1 hour.
- Wash and dry slides.
2. PCR:
- Prepare PCR master mix from PCR Mixes A and B
- Pipette master mix into PCR vessels (for each sample and a negative control)
- Add the sample or negative control to each vessel
- Incubate samples in thermocycler.
7
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Detailed work instructions: During the entire test procedure, EUROIMMUN recommends wearing disposable gloves and changing them frequently to avoid contamination. Disposable gloves worn in the post-PCR area should never be used in the pre-PCR area! DNA negative control (NC) In order to exclude contamination of the test components with amplified DNA (see warning above), a negative control should be performed as the last test in each test series, using a DNA-free solution as sample. Without a negative control the EUROArrayScan software is unable to evaluate the test run. In the direct method the negative control should already be used during DNA extraction to ensure that the extraction solutions 1 and 2 are free of amplified DNA. In the direct method the DNA negative control provided in the test kit is used as negative control instead of blood. For the investigation of isolated genomic DNA samples use a DNA-free solution (preferably elution buffer from the DNA extraction kit or alternatively DNA negative control 2) for the negative control instead of a DNA sample. EUROIMMUN recommends already using the negative control during DNA isolation with a separate isolation kit to ensure that all components of the DNA isolation kit are free of amplified DNA. Instead of blood, e.g. DNA-free water or elution buffer of the kit (do not use the DNA negative control 2 of the test kit!) should be used for isolation. Preparation: - Remove the PCR cooling rack for 0.2 ml reaction vessels from the freezer and place it on the
pre-PCR work station approx. 15 minutes before pipetting the PCRs. - Remove the PCR Mixes A and B from the freezer (-18° C to -25° C) before starting the PCR
pipetting and thaw at + 2° C to + 8° C (do not leave at +2°C to +8°C for more than 60 minutes!). - Define a protocol in the EUROArrayScan software under “New protocol” and print it out. Select
“HLA-DQ2/DQ8 Direct” as test and enter the lot number of the test kit for each slide. For the negative control (see above) define the last field of the test series as negative control (“Neg. control”). For all remaining fields select “Patient”. Further information about the definition of a new protocol can be found in the user manual of the EUROArrayScan software.
- Note: The two tests listed in the EUROArrayScan, HLA-DQ2/DQ8 and HLA-DQ2/DQ8-h Direct are different EUROArray tests which are not compatible with this test system. Danger of wrong results!
- Switch on the thermocycler and preheat the heated lid to ensure that the PCR program can start immediately after the insertion of the PCR reaction vessels.
Warning: Heated lid and incubation block of the thermocycler may reach temperatures of up to +110°C. Risk of skin burns. Please observe the operating instructions with respect to the instrument.
8
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
1. DNA extraction (direct method) or sample preparation The following steps must be performed in the pre-PCR area: DNA extraction: (only with the direct method)
- Thaw DNA negative control 2 at +2°C to +8°C. - If required, thaw EDTA blood samples. - Label reaction vessels (1.5 ml) with numbers according to
the protocol. - In each reaction vessel, pipette 20 ul extraction solution 1
(here, the same pipette tip may be used). - Of each EDTA blood sample or of the DNA negative control
2, pipette 5 µl of each into the respective reagent vessel and mix thoroughly with the extraction solution 1 directly afterwards (vortex shortly).
- Always change pipette tips ! Note: - Mix EDTA blood sample well immediately before withdrawal
of the 5 µl, e. g. by multiple inverting. - The blood must be added to extraction solution 1 within
5 minutes*. If a large number of samples is to be analysed, we recommend initially pipetting extraction solution 1 into only one part of the reaction vessels.
- After pipetting the last sample incubate at room
temperature (+18°C to +25°C) for 1 minute. - Pipette 20 µl of extraction solution 2 into each reaction
vessel and mix by pipetting up and down several times. (Change pipette tip with every step!).
- Immediately continue with pipetting the PCRs. * Note: With longer storage, it cannot be ruled out that some
alleles cannot be detected. Sample preparation: (only when isolated genomic DNA is used)
- If required, thaw the DNA samples, mix each sample by shaking it briefly and centrifuge for a short period to collect the sample at the bottom.
2. PCR The following steps must be performed in the pre-PCR area: Pipetting of PCR preparations:
- Mark the PCR reaction vessels* with numbers according to the protocol defined in EUROArrayScan and place the open vessels into the PCR cooling rack.
- After thawing at +2°C to +8°C mix the PCR Mixes A and B by shaking them briefly (do not vortex!) and centrifuge to collect the solutions at the bottom.
- Prepare PCR master mix for n individual tests (incl. NC): Add 11 µl x n PCR Mix A (green) + 11 µl x n PCR Mix B (yellow)
to a 1.5 ml reaction vessel using a clean pipette tip for each pipetting step. Mix thoroughly by pipetting up and down several times and place into a precooled PCR cooling rack. Note: Do not produce air bubbles. Immediately after use, store PCR mixes A and B at -18° C to -25° C.
- Pipette 20 µl master mixes into the PCR reaction vessels (one single pipette tip may be used).

9
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
- Add 5 µl of the corresponding DNA extract (direct method) or DNA sample (isolated genomic DNA) pipetting. Change the pipette tip with every step!
Important note when DNA extracts are used (direct method): Vortex all DNA extracts immediately before pipetting for 5 seconds at maximum speed. Sedimented particles, which might be present in the extract, should be brought in suspension and pipetted for PCR as well!
- Seal all PCR reaction vessels (Ensure that the caps are
positioned correctly!). - Centrifuge the PCR vessels briefly to collect the solutions at
the bottom.
The following steps must be performed in the amplification area (or post-PCR area, see above):
PCR: - Place all reaction vessels into the thermocycler* and start
one of the following PCR programs. Applied Biosystems 2720 Thermal Cycler: PCR program: - Direct use of EDTA blood samples (direct procedure):
temp. time +95°C 5 min +95°C 15 sec +65°C 20 sec 37 cycles +72°C 20 sec +72°C 5 min. +8°C ∞
- Direct use of isolated genomic DNA samples:
temp. time +97°C 5 Min +97°C 15 Sek +65°C 20 Sek 37 cycles +72°C 20 Sek +72°C 5 Min +8°C ∞
Further settings: PCR reaction volume: 25 µl Applied Biosystems SimpliAmp Thermal Cycler: PCR program: - Direct use of EDTA blood samples (direct procedure):
temp. time +93°C 5 min +93°C 25 sec +65°C 30 sec 37 cycles +72°C 30 sec +72°C 5 min +8°C ∞

10
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
- Direct use of isolated genomic DNA samples: temp. time +97°C 5 Min +97°C 15 Sek +65°C 20 Sek 37 cycles +72°C 20 Sek +72°C 5 Min +8°C ∞
Further settings: PCR reaction volume: 25 µl Mode: 2720 simulation Lid temperature: +103°C Eppendorf Mastercycler nexus SX1 (with silver block): PCR program: - Direct use of EDTA blood samples (direct procedure):
temp. ramp rate time +94°C 2.0°C/sec 5 min +94°C 2.0°C/sec 20 sec +65°C 2.0°C/sec 25 sec 37 cycles +72°C 2.0°C/sec 25 sec +72°C 2.0°C/sec 10 min +8°C - ∞
Further settings: Temperature mode: standard TSP heated lid: on Lid temperature: +105°C Switch off the heated lid at low temperature: on - Direct use of isolated genomic DNA samples:
temp. ramp rate time +97°C 1.5°C/sec 5 min +97°C 1.5°C/sec 15 sec +65°C 1.5°C/sec 20 sec 37 cycles +72°C 1.5°C/sec 20 sec +72°C 1.5°C/sec 5 min +8°C - ∞
Further settings: Temperature mode: safe TSP heated lid: on Lid temperature: +105°C Switch off the heated lid at low temperature: on Bio-Rad T100TM Thermal Cycler: PCR program: - Direct use of EDTA blood samples (direct procedure):
temp. ramp rate time +93°C 4.0°C/sec 5 min +93°C 4.0°C/sec 25 sec +65°C 4.0°C/sec 30 sec 37 cycles +72°C 4.0°C/sec 30 sec +72°C 4.0°C/sec 5 min +8°C - ∞

11
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
- Direct use isolated genomic DNA samples: temp. ramp rate time +97°C 4.0°C/sec 5 min +97°C 4.0°C/sec 20 sec +65°C 4.0°C/sec 25 sec 37 cycles +72°C 4.0°C/sec 25 sec +72°C 4.0°C/sec 5 min +8°C - ∞
Further settings: PCR reaction volume: 25 µl Lid temperature: +103°C - After completion of the PCR and cooling to +8°C, take the
PCR mixtures from the thermal cycler and transfer to a post-PCR rack. Continue with step 3 or store PCR products in the post-PCR area for up to 2 weeks at -20°C and protected from light .
* Note: The PCR program and settings are optimised for the thermocyclers: Applied Biosystems
2720 Thermal Cycler, Applied Biosystems SimpliAmp Thermal Cycler, Eppendorf Mastercycler nexus SX1 and Bio-Rad T100TM Thermal Cycler using above recommended PCR reaction vessels Multiply® µStripPro (Sarstedt). The use of other thermocylers and/or PCR reaction vessels can influence the amplification results and thus alter the performance data of the test, including the specificity and sensitivity. The use of other instruments or vessels should be validated and may require adjustment of the temperature program. Due to the possible device tolerances, for identical instruments we recommend testing the instrument with precharacterised samples and performing regular checks.
3. Incubation (hybridisation) with EUROArray slides All subsequent steps must be performed in the post-PCR area. The incubation technique is explained in greater detail under “TITERPLANE Technique”. Note: Do not touch the test fields containing the microarrays since this might destroy their surface. Preparation: At least 45 minutes before incubation:
- Switch on hybridisation station, set to +45°C and position the TITERPLANE reagent tray. If more than 4 slides are used, the positions of the 2nd reagent tray must be numbered serially with 5 to 8 and so on.
- Remove the required number of slides from the fridge. At least 15 minutes before incubation: - Remove slides from the packaging after they have reached
room temperature and number according to the protocol using the recommended felt-tip pen.
- Place slide onto the reagent tray on the right side of the position chosen for the incubation of the corresponding slide in the protocol (the leftmost position of the reagent tray remains free for the time being). Place the cover onto the reagent tray.
- Prepare wash buffers 1 to 3 (see above).
Pipetting of the hybridisation: - Thaw PCR products, if required. - Add 65 μl of hybridisation buffer to the first PCR product
using a clean pipette tip. Mix thoroughly by pipetting up and down three times and apply 65 μl of the solution to the corresponding reaction field (see protocol) using the same tip. Avoid air bubbles!
12
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Note: With the direct method, particles in the sample might block the pipette tip. Therefore visually check the filling volume of the tip before each transfer.
- Repeat these steps for the remaining samples. The
application of the hybridisation solution must be performed rapidly to avoid evaporation. When all samples for one slide have been pipetted onto the reagent tray, transfer the slide from the neighbouring right position to the position assigned to it according to the protocol. The microarrays come into contact with the droplets and the incubation is started. Make sure that the samples have contact with the microarrays on the slide and that the individual samples do not come into contact with each other.
- After transferring the last slide on the reagent tray to its assigned position, close the lid of the incubator insert.
Incubation: - After closing the lid, incubate at +45°C for 60 minutes. Washing: Up to 10 slides can be washed simultaneously.
- Fill each of four wash cuvettes with 200 ml of buffer (brought to room temperature: +18°C to +25°C) as follows:
- 2 wash cuvettes with wash buffer 1 - 1 wash cuvette with wash buffer 2 - 1 wash cuvette with wash buffer 3
- Place the glass frame into the second wash cuvette containing wash buffer 1.
- Carefully lift the first slide from the reagent tray without tilting it and turn it by 90° around the longitudinal axis. Hold the slide using a clean pair of tweezers and immerse completely into the first wash cuvette with wash buffer 1 for a short period. Subsequently, transfer the slide into the glass frame located in the second wash cuvette containing wash buffer 1.
- Repeat the last step for the up to 9 remaining slides until the glass frame contains the maximum amount of 10 slides.
- After transferring the last slide, incubate for one minute. - Transfer the glass frame into the wash cuvette containing
wash buffer 2 and incubate the slides for precisely 2 minutes.
- Transfer the glass frame into the wash cuvette containing wash buffer 3 and incubate the slides for at least 5 seconds.
- Remove the first slide from the glass frame in wash buffer 3 using a clean pair of tweezers and slightly tap it with its side onto a lint-free laboratory tissue. Immediately afterwards, blow away any residual liquid on the fields using compressed air (canned, if required) and wipe away any residual liquid on the rear side and the edges of the slide with lint-free tissue. Do not wipe the microarrays on the surface of the slide!
- Repeat the previous step with the remaining slides. - With more than 10 slides, repeat the entire washing
procedure with the other slides using freshly prepared wash buffers 1 to 3.
- Clean the reagent tray and disinfect, if required (see above) Note: For correct analysis results it is essential to follow the exact temperatures and times for hybridisation and washing given in this test instruction. A deviation from the hybridisation temperature of more than one degree or a wash buffer temperature outside the specified range of +18°C to +25°C may lead to invalid or, in the worst case, to false results.

13
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
4. Scanning and evaluation Scanning and evaluation are performed using the EUROArrayScanner or the EUROIMMUN Microarray Scanner and the EUROArrayScan software. Please familiarise yourself with the content of the respective manual before first use. To summarise, the following steps are performed: - Start the EUROArrayScan software and switch on the scanner*. - Select the respective protocol from the list in the EUROArrayScan program using the menu
item “Scan slides”. - Start the scanning process by clicking on the “Start” button. Follow the instructions of the
program. Place the slides into the scanner according to the instructions and scan. - Switch off the EUROIMMUN Microarray Scanner*. - Verify, under the tab “Show” using the images, that all spot signals in all arrays have been
correctly identified (there should be a white evaluation circle on each signal). If an evaluation circle is obviously falsely positioned next to the corresponding spot signal, it should be moved to the middle of the corresponding spot signal by pressing the left mouse button (the evaluation circle turns green). If an evaluation circle is obviously positioned on an artefact, e.g. lint, or if a spot signal is damaged and does not exhibit the typical spot form, the corresponding evaluation circle should be invalidated using the right mouse button (it then turns red). Further corrections are not intended and are the responsibility of the user. After the manual corrections have been entered, the software automatically determines if there is still enough data to provide a reliable evaluation of the test.
- If the entire grid is missing or is positioned incorrectly, please follow the instructions for the function “Set grid” in the user manual for the EUROArrayScan software. Manually corrected results are labelled as such in the results overview.
- Save the result evaluation by clicking on the “Save” button. - Select the tab “Results” to view the test results and print the result overview or individual
results, if desired. * Note: The EUROIMMUN Microarray Scanner is to be switched on only shortly before and
switched off directly after the scanning procedure. Do not scan more than 20 slides per hour as the fluorescence intensity is dependent on the temperature. This restriction is not valid for the EUROArrayScanner which has an active air cooling system.

14
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
TITERPLANE Technique
Pipette: 65 µl per field
Incubate: 60 min at +45°C
Wash: 1 x shortly immerse into wash buffer 1
1 x 1 min in wash buffer 1
1 x precisely 2 min in wash buffer 2
1 x 5 sec in wash buffer 3
Dry: compressed air
Scan and evaluate:
Samples are applied to the preheated reaction fields (+45°C) of a TITERPLANE reagent tray. The slides are then placed into the corresponding recesses of the reagent tray, with the BIOCHIPS facing downwards. There is only one correct position for the slides. The notch of the slide must fit into the corresponding nose of the reagent tray. Position and height of the droplets are exactly defined by the geometry of the system. The samples do not spread. The liquids are harboured in an enclosed area, an additional conventional “moisture chamber” is therefore not required.
EUROArray slide
with microarray BIOCHIPs reagent tray
hybridisation sample
microarray scanner EUROArrayScan software
15
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Test result All final and partial test results are determined and displayed automatically by the EUROArrayScan software. EUROIMMUN recommends the following evaluation of results: HLA-DQ2.2
negative: The test yielded a negative result for the HLA-DQA1 and HLA-DQB1 alleles coding for the alpha- and/or beta-subunit of HLA-DQ2.2.
positive*:
The test yielded a positive result for the HLA-DQA1 and HLA-DQB1 alleles coding for the alpha- and beta-subunit of HLA-DQ2.2 (also see section “Test characteristics”).
not valid:
A test result cannot be issued for this analysis (see below for explanation). HLA-DQ2.5
negative: The test yielded a negative result for the HLA-DQA1 and HLA-DQB1 alleles coding for the alpha- and/or beta-subunit of HLA-DQ2.5.
positive:
The test yielded a positive result for the HLA-DQA1 and HLA-DQB1 alleles coding for the alpha- and beta-subunit of HLA-DQ2.5 (also see section “Test characteristics”).
not valid:
A test result cannot be issued for this analysis (see below for explanation). HLA-DQ8
negative: The test yielded a negative result for the HLA-DQA1 and HLA-DQB1 alleles coding for the alpha- and/or beta-subunit of HLA-DQ8.
positive:
The test yielded a positive result for the HLA-DQA1 and HLA-DQB1 alleles (HLA-DQA1*03:01 and HLA-DQB1*03:02) coding for the alpha- and beta subunit of HLA-DQ8 (also see section “Test characteristics”).
positive1:
The test yielded a positive result for the HLA-DQA1 and HLA-DQB1 alleles (HLADQA1*03:02/*03:03 and HLA-DQB1*03:02) coding for the alpha- and beta-subunit of HLA-DQ8. HLA-DQA1*03:01 was not detected (see section “Test characteristics”).
not valid:
A test result cannot be issued for this analysis (see below for explanation).

16
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
β-subunit HLA-DQ2.2/DQ2.5 negative:
The test yielded a negative result for the HLA-DQB1 alleles coding for the beta-subunit HLA-DQ2.2/DQ2.5.
positive: The test yielded a positive result for the HLA-DQB1 allele coding for the beta-subunit HLA-DQ2.2/DQ2.5. From the detected HLA-DQA1 alleles, at least one codes for the HLA-DQ2.2 or -DQ2.5 alpha-subunit (also see section “Test characteristics”).
positive***: The test yielded a positive result for the HLA-DQB1 allele coding for the beta-subunit HLA-DQ2.2/DQ2.5. Of the detected HLA-DQA1 alleles, none codes for the HLA-DQ2.2 or -DQ2.5 alpha-subunit (see also section “Test characteristics”).
not valid: A test result cannot be issued for this analysis (see below for explanation).
A test result can be “not valid” for different reasons: - at least one partial result of the internal controls is not valid, and/or - at least one partial result of the investigated HLA-DQ2.2, HLA-DQ2.5 or HLA-DQ8 subunits is
not valid, and/or - more than two alleles have been identified by mistake (e.g. 2 samples have been pipetted
inadvertently into the same PCR vessel), and/or - at least one partial result of the external negative control is not valid.
The EUROArrayScan software automatically identifies all these cases. The analysis of these sample(s) should be repeated. Please contact EUROIMMUN if you wish to have further advice on this case.
The following partial results are possible for the test EUROArray HLA-DQ2/DQ8 Direct:
For DQA1*02, DQA1*03, DQA1*05, DQA1*01/*04/*06, DQA1*02/*03:01, DQA1*03:02/03, DQB1*02 and DQB1*03:02 as well as for the alpha- and beta-subunits of HLA-DQ2.2, HLA-DQ2.5 and HLA-DQ8, the results can be “positive”, “negative” or “not valid”. For the HLA-DQ8 alpha-subunit, “positive1” or “positive2” can additionally occur.
“Not valid” is given if the signal could not be clearly identified as positive or negative by the EUROArrayScan Software or if too many of the respective spots were not valid or invalid combinations were found (e.g. more than two alleles).
* In the European guidelines for coealic disease diagnostics, only the subtype HLA-DQ2.5 is specified as being disease-associated (Husby et al., J. Pediatr. Gastroenterol. Nutr. 2012 Jan;54(1):136-60). Other studies show that the subtype HLA-DQ2.2 can also be associated with coeliac disease (Mubarak et al., J. Pediatr. Gastroenterol. Nutr. 2012 Oct 18. - Status 11th March 2013).
*** The beta-subunit of DQ2 (DQB1*02) was detected, but not the alpha-subunit of DQ2 (DQA1*02 or DQA1*05). It has been described in individual cases that in coeliac disease patients only the beta-subunit of DQ2 may be present (e.g. Megiorni et al., Hum Immunol. 2009 Jan;70(1):55-9).
1 The HLA alleles DQA1*03:02 and/or DQA1*03:03 were detected in the sample together with the
beta-subunit of DQ8 (DQB1*03:02). HLA-DQA1*03:01, however, which solely represents the alpha-subunit of DQ8 according to the ESPGHAN guidelines (Husby et al., J. Pediatr. Gastroenterol. Nutr. 2012 Jan;54(1):136-60), was not detected in the sample. In many studies that investigated the connection between the presence of HLA-DQ characteristics and coeliac disease, the alleles HLA-DQA1*03:01/02/03 were not differentiated and therefore all evaluated as alpha-subunit of DQ8.

17
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
2 The HLA alleles DQA1*03:02 and/or DQA1*03:03 were detected in the sample. HLA-DQA1*03:01, however, which solely represents the alpha-subunit of DQ8 according to the ESPGHAN guidelines (Husby et al., J. Pediatr. Gastroenterol. Nutr. 2012 Jan;54(1):136-60), was not detected in the sample. In many studies that investigated the connection between the presence of HLA-DQ characteristics and coeliac disease, the alleles HLA-DQA1*03:01/02/03 were not differentiated and therefore all evaluated as alpha-subunit of DQ8.
For the controls, there are different results possible: “valid” or “not valid”. The controls are evaluated automatically by the EUROArrayScan software.
Test characteristics
Microarrays: Microarrays consist of single-stranded DNA probes of around 20 nucleotides in length, which are immobilised as spots on the BIOCHIPs located on the reaction fields of the slides. For every possible PCR product there is a corresponding probe in the form of a double spot on the microarray. Furthermore, the microarray contains control spots that hybridise with fluorescence-labelled control oligonucleotides, helping to identify faults in the test performance.
The HLA-DQ2/DQ8 Direct microarray is composed of the following spots:
HLA-DQ2/DQ8 Direct
A02: The probe hybridises with the HLA-DQA1*02 PCR product. A03: The probe hybridises with the HLA-DQA1*03 PCR product. A05: The probe hybridises with the HLA-DQA1*05 PCR product. A01/04/06: The probe hybridises with the HLA-DQA1*01/04/06 PCR product. A02/0301: The probe hybridises with the HLA-DQA1*02/03:01 PCR product. A0302/03: The probe hybridises with the HLA-DQA1*03:02/03 PCR product. B02: The probe hybridises with the HLA-DQB1*02 PCR product. B03:02: The probe hybridises with the HLA-DQB1*03:02 PCR product. CC-I and CC-II: Cross contamination control: Only one of the two probes should show a
signal. If both probes have a signal, cross contamination of adjacent slide fields has occurred.
HSC-I and -II: Hybridisation specificity control: The hybridisation buffer contains a fluorescence-labelled oligonucleotide, which is perfectly complementary to probe HSC-I and contains two variations with respect to probe HSC-II. If the signal of probe HSC-I is significantly stronger than that of probe HSC-II, sufficient stringency is confirmed for hybridisation and washing steps.
OS-I to -IV: Orientation spots: Necessary for the automatic detection of array positions using EUROArrayScan.
Unnamed spots are not used in the test. The signals at these positions are irrelevant for the result.
Sequence-specific HLA-DQA1 or HLA-DQB1 primers and probes: The primers and probes for the detection of the HLA-DQA1 and HLA-DQB1 gene segments were selected so that the relevant alleles are amplified with great sensitivity and specificity and subsequently detected by a hybridisation to specific microarray probes (see also explanations to the partial results in the following database: IMGT / HLA database; http://www.ebi.ac.uk/cgi-bin/ipd/imgt/hla/align.cgi, Release 3.25.0, October 2016).
18
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Partial result DQA1*02 (probe A02) The probe A02 detects the allele DQA1*02:01, which codes for the alpha-subunit of DQ2.2. Partial result DQA1*03 (probe A03) The probe A03 detects all DQA1*03 alleles (DQA1*03:01 and DQA1*03:02/*03:03). According to the ESPGHAN guidelines, HLA-DQA1*03:01 alone represents the alpha-subunit of DQ8 (Husby et al., J. Pediatr. Gastroenterol. Nutr. 2012 Jan;54(1):136-60). In many studies that investigated the connection between the presence of HLA-DQ characteristics and coeliac disease, the alleles HLA-DQA1*03:01/02/03 were not differentiated and therefore all evaluated as alpha-subunit of DQ8. Partial result DQA1*05 (probe A05) The probe A05 detects virtually all DQA1*05 alleles (DQA1*05:01 to DQA1*05:11). With this probe, essentially the alpha-subunit of DQ2.5 coding alleles DQA1*05:01 and DQA1*05:05 are detected, whose presence is described in European studies as average 25% (DQA1*05:01) or 18%, respectively (DQA1*05:05) (http://www.allelefrequencies.net, version: October 2016). The alleles DQA1*05:02 and DQA1*05:03 which cannot be distinguished from the alleles DQA1*05:01 and DQA1*05:05, and are therefore also classified as alpha-subunit of DQ2.5 by the test, are only found in few populations, and also in very low allele frequencies of 0.003 to 0.006. Out of the other detected alleles DQA1*05:04 and DQA1*05:06 to DQA1*05:11, none was detected in international studies (http://www.allelefrequencies.net, version: October 2016), so that their occurrence is considered to be highly unlikely. Due to mismatches in the primer or probe binding region, the alleles DQA1*05:01:02, DQA1*05:02 and DQA1*05:10 may not be detected. Except from DQA1*05:02 (see above) these alleles have not been detected in any international study (http://www.allelefrequencies.net, version: October 2016), so that their occurrence is considered to be highly unlikely. Partial result DQA1*01/*04/*06 (probe A01/04/06) Probe A01/04/06 is used to detect the alleles HLA-DQA1*01, -DQA1*04 and -DQA1*06. Owing to mismatches in the primer or probe binding region, the detection of the allele DQA1*01:10 may not take place. This allele has not been detected in any international study (http://www.allelefrequencies.net, version: October 2016), so that its occurrence is considered to be highly unlikely. Partial result DQA1*02/*03:01 (probe A02/03:01) Detection of HLA-DQA1*02:01 and HLA-DQA1*03:01 alleles is carried out via probe A02/03:01. Furthermore, the alleles HLA-DQA1*01, -DQA1*04, DQA1*05 and DQA1*06 can generate a signal at this probe. This cross-reaction which occurs, if any, is unproblematic since discrimination with the aid of the further probes is possible. Partial result DQA1*03:02/03 (probe A03:02/03) Probe A03:02/03 detects the alleles DQA1*03:02 and DQA1*03:03 together. According to the ESPGHAN guidelines, HLA-DQA1*03:01 alone represents the alpha-subunit of DQ8 (Husby et al., J. Pediatr. Gastroenterol. Nutr. 2012 Jan;54(1):136-60). In many studies that investigated the connection between the presence of HLA-DQ characteristics and coeliac disease, the alleles HLA-DQA1*03:01/02/03 were not differentiated and therefore all evaluated as alpha-subunit of DQ8. Partial result DQB1*02 (probe B02): The probe B02 detects virtually the complete family of DQB1*02 alleles (DQB1*02:01 to DQB1*02:74). This probe essentially detects the alleles coding for the beta-subunit of HLA-DQ2.2 and -DQ2.5, DQB1*02:01 and DQB1*02:02 whose presence is described in European studies with an allele frequency of approx. 15% for DQB1*02:01 and 8% for DQB1*02:02 (http://www.allelefrequencies.net, version: October 2016). Out of the other detected alleles, DQB1*02:04 to DQB1*02:74, which cannot be distinguished from DQB1*02:01 and DQB1*02:02 and are therefore also classified as beta-subunit of DQ2.2/DQ2.5 by the test, none was detected in international studies (http://www.allelefrequencies.net, version: October 2016), so that their occurrence is considered to be highly unlikely.

19
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
The allele HLA-DQB1*02:03, which occurs with an allele frequency of 0.0003 to 0.038, is not detected by the probe B02. This allele does not code for the beta-subunit of HLA-DQ2.2 or -DQ2.5 and is therefore not associated with coeliac disease. Owing to individual mismatches in the primer or probe binding region, the detection of alleles DQB1*02:01:02/07/13/15/21 and DQB1*02:14/17/18N/24/26/31/33/44/49/50/55/56/58N/68/70 in the probe B02 may not take place. None of these alleles have been detected in international studies (http://www.allelefrequencies.net, version: October 2016), so that their occurrence is considered to be highly unlikely. Partial result DQB1*03:02 (probe B03:02): The probe B03:02 detects all known DQB1*03:02 alleles. Furthermore, the alleles DQB1*03:07/08/11/18/32/37/45/62/63/64/66N/67/68/70/81/85/106/107/125, DQB1*03:146/153/ 161/174/175/178/179/184/185/189/190/199/203/204/205/210/211/213N/214/215/220/221/223/224/ 225/228/229 and DQB1*06:29/123/139 are detected. These cannot be distinguished from the DQB1*03:02 allele and are therefore classified as beta-subunit of DQ8 by the test. Out of the other detected alleles, only DQB1*03:08 with an allele frequency of 0.0001 and DQB1*03:11 with an allele frequency of 0.001, respectively, were detected in a European study. The other alleles were not detected in any international study (http://www.allelefrequencies.net, version: October 2016). Consequently, their occurrence is considered to be highly unlikely. Due to mismatches in the primer or probe binding region, the detection of the allele DQA1*03:02:14 may not take place. This allele has not been detected in any international study (http://www.allelefrequencies.net, version: October 2016), so its occurrence is considered to be highly unlikely. Partial result α-subunit HLA-DQ2.2 (HLA-DQA1*02:01): See partial result DQA1*02. Partial result α-subunit HLA-DQ2.5 (HLA-DQA1*05:01/*05:05): See partial result DQA1*05. Partial result α-subunit HLA-DQ8 (HLA-DQA1*03:01 or DQA1*03:02/*03:03): The determination is performed with 4 primer systems (spot pairs A02, A02/0301, A03 and A0302/03). To ensure a clear result in the determination of the alleles DQA1*03:01 and DQA1*03:02/*03:03, the alleles (or allele families) DQA1*02, DQA1*02/*03:01, DQA1*03 and DQA1*03:02/*03:03 are analysed. DQA1*03:01 and DQA1*03:02/*03:03 are clearly determined from the four individual results. According to the ESPGHAN guidelines, HLA-DQA1*03:01 solely represents the alpha-subunit of DQ8 (Husby et al., J. Pediatr. Gastroenterol. Nutr. 2012 Jan;54(1):136-60). In many studies that investigated the connection between the presence of HLA-DQ characteristics and coeliac disease the alleles HLA-DQA1*03:01/02/03 were not differentiated and therefore all evaluated as alpha-subunit of DQ8. Partial result β-subunit HLA-DQ2.2/DQ2.5 (HLA-DQB1*02:01/*02:02): See partial result DQB1*02. Partial result β-subunit HLA-DQ8 (HLA-DQB1*03:02): See partial result DQB1*03:02. The test EUROArray HLA-DQ2/DQ8 Direct provides the following test results: Test result HLA-DQ2.2: HLA-DQ2.2 is given as positive if the partial results “alpha-subunit HLA-DQ2.2” and “beta-subunit HLA-DQ2.2/DQ2.5” are positive. Test result HLA-DQ2.5: HLA-DQ2.5 is given as positive if the partial results “alpha-subunit HLA-DQ2.5” and “beta-subunit HLA-DQ2.2/DQ2.5” are positive.
20
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Test result HLA-DQ8: HLA-DQ8 is given as positive if the partial results “alpha-subunit HLA-DQ8” and “beta-subunit HLA-DQ8” are positive.
Test result HLA-DQ2.2/DQ2.5 β-subunit HLA-DQ2.2/DQ2.5 β-subunit is given as positive if the partial result “beta-subunit HLA-DQ2.2/DQ2.5” is positive.
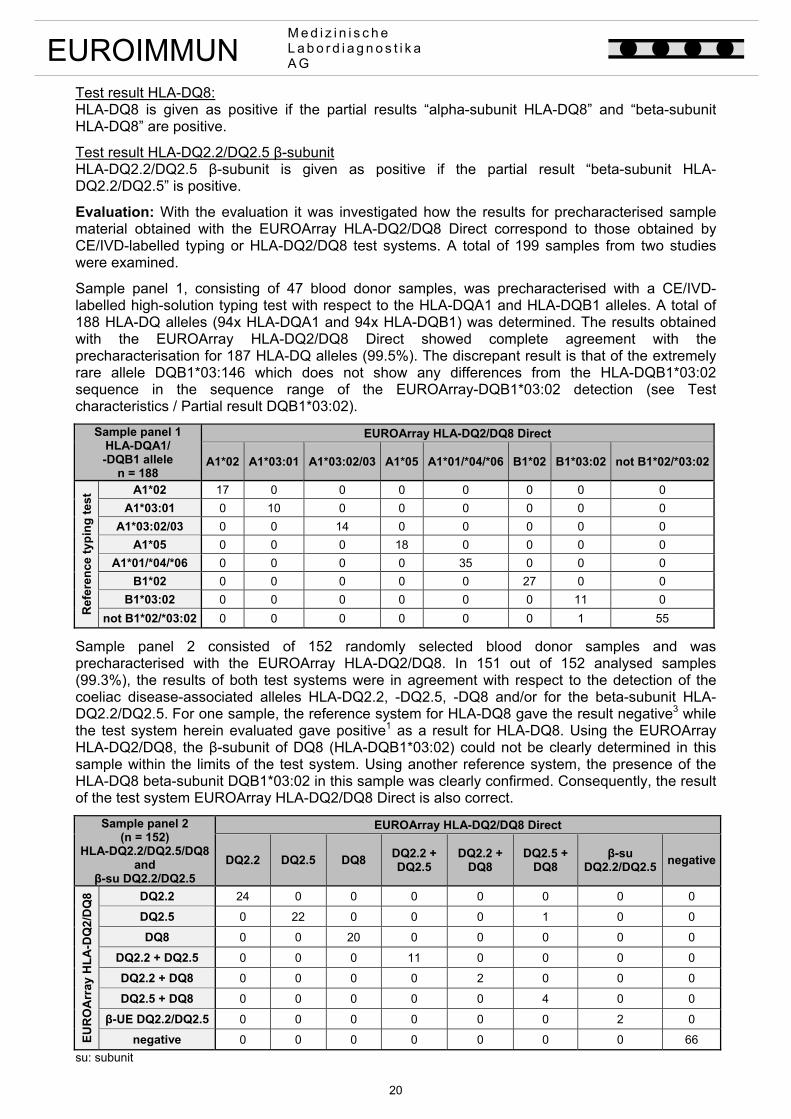
Evaluation: With the evaluation it was investigated how the results for precharacterised sample material obtained with the EUROArray HLA-DQ2/DQ8 Direct correspond to those obtained by CE/IVD-labelled typing or HLA-DQ2/DQ8 test systems. A total of 199 samples from two studies were examined.
Sample panel 1, consisting of 47 blood donor samples, was precharacterised with a CE/IVD-labelled high-solution typing test with respect to the HLA-DQA1 and HLA-DQB1 alleles. A total of 188 HLA-DQ alleles (94x HLA-DQA1 and 94x HLA-DQB1) was determined. The results obtained with the EUROArray HLA-DQ2/DQ8 Direct showed complete agreement with the precharacterisation for 187 HLA-DQ alleles (99.5%). The discrepant result is that of the extremely rare allele DQB1*03:146 which does not show any differences from the HLA-DQB1*03:02 sequence in the sequence range of the EUROArray-DQB1*03:02 detection (see Test characteristics / Partial result DQB1*03:02).
Sample panel 1 HLA-DQA1/ -DQB1 allele
n = 188
EUROArray HLA-DQ2/DQ8 Direct
A1*02 A1*03:01 A1*03:02/03 A1*05 A1*01/*04/*06 B1*02 B1*03:02 not B1*02/*03:02
Ref
eren
ce t
ypin
g t
est A1*02 17 0 0 0 0 0 0 0
A1*03:01 0 10 0 0 0 0 0 0
A1*03:02/03 0 0 14 0 0 0 0 0
A1*05 0 0 0 18 0 0 0 0
A1*01/*04/*06 0 0 0 0 35 0 0 0
B1*02 0 0 0 0 0 27 0 0
B1*03:02 0 0 0 0 0 0 11 0
not B1*02/*03:02 0 0 0 0 0 0 1 55
Sample panel 2 consisted of 152 randomly selected blood donor samples and was precharacterised with the EUROArray HLA-DQ2/DQ8. In 151 out of 152 analysed samples (99.3%), the results of both test systems were in agreement with respect to the detection of the coeliac disease-associated alleles HLA-DQ2.2, -DQ2.5, -DQ8 and/or for the beta-subunit HLA-DQ2.2/DQ2.5. For one sample, the reference system for HLA-DQ8 gave the result negative3 while the test system herein evaluated gave positive1 as a result for HLA-DQ8. Using the EUROArray HLA-DQ2/DQ8, the β-subunit of DQ8 (HLA-DQB1*03:02) could not be clearly determined in this sample within the limits of the test system. Using another reference system, the presence of the HLA-DQ8 beta-subunit DQB1*03:02 in this sample was clearly confirmed. Consequently, the result of the test system EUROArray HLA-DQ2/DQ8 Direct is also correct.
Sample panel 2 (n = 152)
HLA-DQ2.2/DQ2.5/DQ8 and
β-su DQ2.2/DQ2.5
EUROArray HLA-DQ2/DQ8 Direct
DQ2.2 DQ2.5 DQ8 DQ2.2 + DQ2.5
DQ2.2 + DQ8
DQ2.5 + DQ8
β-su DQ2.2/DQ2.5
negative
EU
RO
Arr
ay H
LA
-DQ
2/D
Q8 DQ2.2 24 0 0 0 0 0 0 0
DQ2.5 0 22 0 0 0 1 0 0
DQ8 0 0 20 0 0 0 0 0
DQ2.2 + DQ2.5 0 0 0 11 0 0 0 0
DQ2.2 + DQ8 0 0 0 0 2 0 0 0
DQ2.5 + DQ8 0 0 0 0 0 4 0 0
β-UE DQ2.2/DQ2.5 0 0 0 0 0 0 2 0
negative 0 0 0 0 0 0 0 66
su: subunit
21
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Intra-assay reproducibility: Three samples with different genetic patterns were analysed in 10 parallel runs in one test run. In all cases, the result was consistent with the precharacterisation. Inter-assay reproducibility: Three samples with different genetic patterns were analysed in duplicate on at least two different days in a total of five independent test runs. In all cases, the result was consistent with the precharacterisation.
Inter-lot reproducibility: Four samples with different genetic patterns were analysed in duplicate using three different test kit lots. In all cases, the result was consistent with the precharacterisation.
Analytical sensitivity / minimum DNA concentration*: 19 precharacterised DNA samples with a concentration of 5 ng/μl were investigated, and all determinations were successful. None of the results deviated from the precharacterisation.
Robustness: 202 samples from blood donors were investigated. All determinations were successful.
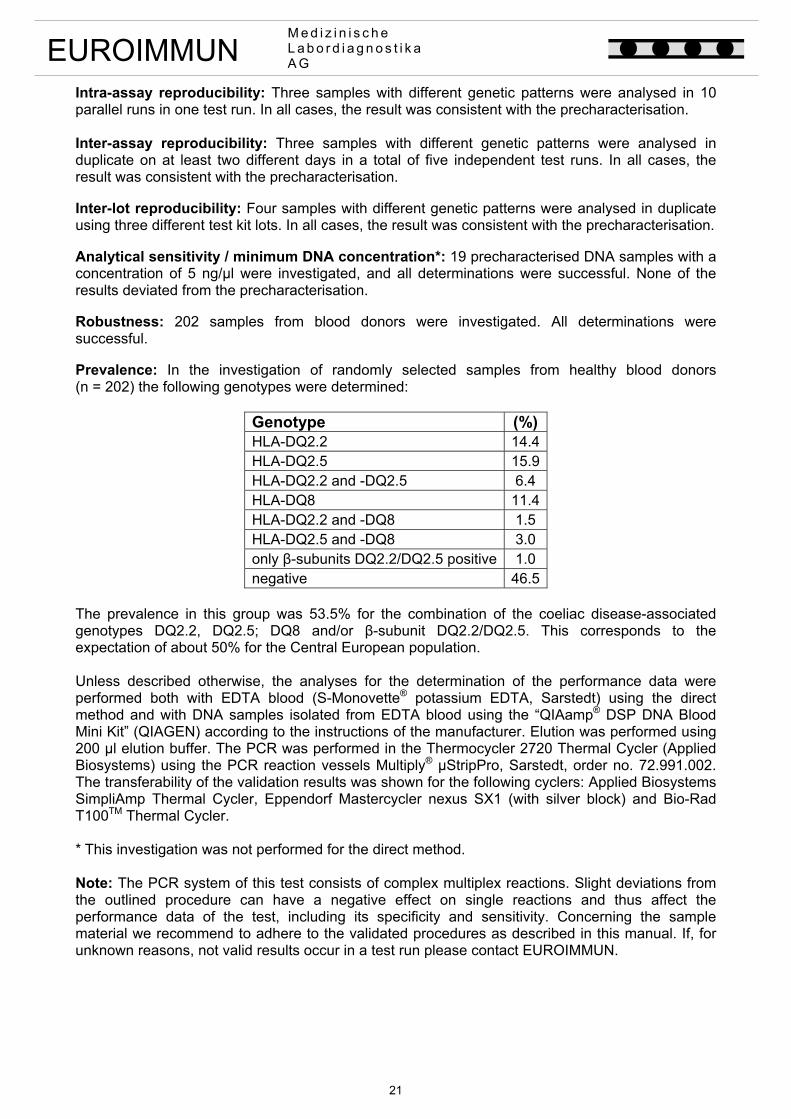
Prevalence: In the investigation of randomly selected samples from healthy blood donors (n = 202) the following genotypes were determined:
Genotype (%)HLA-DQ2.2 14.4HLA-DQ2.5 15.9HLA-DQ2.2 and -DQ2.5 6.4 HLA-DQ8 11.4HLA-DQ2.2 and -DQ8 1.5 HLA-DQ2.5 and -DQ8 3.0 only β-subunits DQ2.2/DQ2.5 positive 1.0 negative 46.5
The prevalence in this group was 53.5% for the combination of the coeliac disease-associated genotypes DQ2.2, DQ2.5; DQ8 and/or β-subunit DQ2.2/DQ2.5. This corresponds to the expectation of about 50% for the Central European population. Unless described otherwise, the analyses for the determination of the performance data were performed both with EDTA blood (S-Monovette® potassium EDTA, Sarstedt) using the direct method and with DNA samples isolated from EDTA blood using the “QIAamp® DSP DNA Blood Mini Kit” (QIAGEN) according to the instructions of the manufacturer. Elution was performed using 200 µl elution buffer. The PCR was performed in the Thermocycler 2720 Thermal Cycler (Applied Biosystems) using the PCR reaction vessels Multiply® µStripPro, Sarstedt, order no. 72.991.002. The transferability of the validation results was shown for the following cyclers: Applied Biosystems SimpliAmp Thermal Cycler, Eppendorf Mastercycler nexus SX1 (with silver block) and Bio-Rad T100TM Thermal Cycler. * This investigation was not performed for the direct method. Note: The PCR system of this test consists of complex multiplex reactions. Slight deviations from the outlined procedure can have a negative effect on single reactions and thus affect the performance data of the test, including its specificity and sensitivity. Concerning the sample material we recommend to adhere to the validated procedures as described in this manual. If, for unknown reasons, not valid results occur in a test run please contact EUROIMMUN.

22
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Limitations of the procedure 1. For diagnosis, the clinical symptoms of the patient should always be taken into account along
with the molecular genetic results. 2. In molecular biological test procedures, further very rare gene variants which are not yet
included in the sources used for specificity and sensitivity analysis of primers and probes and which may affect the test result can generally not be excluded.
3. Deviations from the specified use of the device, the test procedure, specified storage
conditions, materials, devices and/or recommended sample material may lead to deviations from the results that are obtained when all specifications are observed. The internal and external controls can help to detect errors. They may, however, not detect every possible error. Each laboratory should validate their modifications and ensure that the device specifications are met.
Clinical significance The EUROArray HLA-DQ2/DQ8 Direct is designed for the detection of the disease-associated alleles HLA-DQA1 and HLA-DQB1, which code for the human leukocyte antigens DQ2 (HLA-DQ2.2 and -DQ2.5) and DQ8. These are heterodimeric surface receptors consisting of an alpha and a beta chain. The detection is important in the diagnosis of coeliac disease (gluten-sensitive enteropathy, non-tropical sprue) since almost 100 % of coeliac disease patients are positive for HLA-DQ2 (DQ2.2/DQ2.5) and/or HLA-DQ8. Although these markers are not particularly specific (around 50 % of the healthy population is also positive for HLA-DQ2 (DQ2.2/DQ2.5) and/or -DQ8), the absence of these risk factors is an important criterion for the exclusion of coeliac disease as they possess a high negative predictive value (NPV). The NPV is at least 98%. If neither DQ2.2, DQ2.5 nor DQ8 are detected in a patient, then coeliac disease can be as good as excluded. The determination of HLA-DQ2 (DQ2.2/DQ2.5) and HLA-DQ8 is, above all, significant for the following: doubtful biopsy results, ambiguous serology (especially in children under two years old), patients on a gluten-free diet with inconclusive diagnosis, clarification of the genetic predisposition of first-degree relatives of coeliac disease patients, and differentiation from other intestinal diseases. HLA antigens play a decisive role in coeliac disease and possibly also dermatitis herpetiformis (DH), whereby there are regional differences in frequency and gene combinations. The genetic relationship becomes clear when families are analysed. The prevalence of coeliac disease in first-degree relatives is around 10 %, in identical twins 70 % and in non-identical twins only about 11 %. The determination of the homo- or heterozygous presence of the alleles coding for the human leukocyte antigens DQ2.2 and DQ2.5 is of increasing importance in risk assessment in suspected cases of coeliac disease. Individuals who are homozygous for the alleles of the complete DQ2.2 or DQ2.5 heterodimer have a five times higher risk of developing coeliac disease than heterozygous carriers. The “gene dose” effect plays a decisive role. Since carriers who present of the homozygous alleles for the HLA-DQ2 beta subunit already have an increased risk of developing coeliac disease, even if no associated alpha subunit was detected. According to Megiorini et al. (2012) the following risk categories can be defined: HLA-DQ2.5 (with double gene dose of DQA1*05 and DQB1*02) very high risk HLA-DQ2.5 and -DQ8 very high risk HLA-DQ2.5 (with double gene dose of DQB1*02) very high risk HLA-DQ8 high risk HLA-DQ2.5 (with single gene dose of DQB1*02) high risk HLA-DQ2.x (with double gene dose of DQB1*02) high risk HLA-DQ2.x (with single gene dose of DQB1*02) low risk HLA-DQX.5 very low HLA-DQX.x very low
23
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
In the guidelines for the diagnosis of coeliac disease published by the “European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN)” in 2012, only the HLA-DQ2.5 subtype is considered as associated with coeliac disease and is described as HLA-DQ2. Other studies, however, show that HLA-DQ2.2 is a further HLA-DQ2 subtype associated with coeliac disease. Furthermore, it has been described in individual studies that in rare cases coeliac disease patients may only present the beta subunit of DQ2 alone, without the corresponding HLA-DQ2.2 or HLA-DQ2.5 alpha subunit. Around 95% of individuals with coeliac disease have the HLA-DQ2.5 subtype, which is coded by the alleles HLA-DQA1*05:01 (or DQA1*05:05) and HLA-DQB1*02:01 (or DQB1*02:02). Other coeliac disease patients present HLA-DQ2.2, which is coded by the alleles HLA-DQA1*02:01 and HLA-DQB1*02:02, or HLA-DQ8, which is determined by the alleles HLA-DQA1*03:01 and HLA-DQB1*03:02 according to the ESPGHAN guidelines. Other studies investigating the relationship between the presence of HLA-DQ characteristics and coeliac disease do not differentiate between the HLA-DQA1*03:01/02/03 alleles. Accordingly, all of them are considered as alpha subunits of DQ8 and therefore, in combination with DQB1*03:02, classified as “HLA-DQ8 positive”.
Coeliac disease is an autoimmune disease which occurs in predisposed individuals as a reaction to gluten sensitivity. We know today that after resorption in the lamina propria of the intestinal mucosa, gliadin is deamidated by tissue transglutaminase (tTG). In this process, particular glutamine residues are replaced by glutamic acid residues. In individuals with a genetic predisposition, pieces (peptides) of gliadin modified in this way bind to e.g. HLA-DQ2/DQ8 molecules of the antigen-presenting cells and are presented to helper T cells. An extensive immune reaction is triggered, causing pathological tissue changes, particularly damage to the small intestine. Components of this immune reaction are antibodies against endomysium or tTG and against the deamidated gliadin generated by tTG. Antibodies against endomysium are apparently identical to antibodies against reticulin, which were discovered by Seah in 1971. These antibodies recognise tTG as their target antigen. In 2006, the frequency of diagnosed coeliac disease was around 1:300 in western Ireland, Italy, the USA, the Middle East, India and Cuba, around 1:1.000 in Germany and Austria and around 1:2.000 to 1:4.500 in other European countries.
Gluten is found in various cereals (e.g. wheat, barley, rye). It consists of a mixture of proteins, which can be divided into two groups: prolamins and glutelins, with gliadin being the most frequent prolamin. If patients with coeliac disease consume food containing gluten, this will finally lead to damage to the mucous membrane of the small intestine, which then shows a flat, mosaic-like surface without any villi structure but with deep visible crypts. This, in turn, results in functional disorders. In the Marsh classification the intestinal histopathological grade of the disease is divided into three levels:
Marsh type I: increase in intraepithelial lymphocytes (> 40 IEL/100 epithelial cells) with normal mucous membrane architecture (infiltrative phase)
Marsh type II: additional crypt hyperplasia with normal villi morphology Marsh type III: IEL increase, crypt hyperplasia, degeneration of epithelial cells and villi.
Type III is further divided into IIIA (partial villous atrophy), IIIB (subtotal villous atrophy) and IIIC (complete villous atrophy).
The clinical symptoms of coeliac disease comprise fatigue (78%), borborygmus (72%), abdominal pain (64%), diarrhoea (56%), effects of malabsorption (44%) with weight loss, anaemia and growth retardation in children, vomiting (16%), constipation (12%) and bone pains (12%). Some patients with gluten-sensitive enteropathy also suffer from dermatitis herpetiformis (10%), a chronic skin disease accompanied by the formation of blisters. In a prolonged course, mainly in adults, the risk of melanoma, particularly intestinal T-cell lymphoma, is about 10%.
If other autoimmune diseases are present in addition to coeliac disease, the risk of developing splenic hypofunction amounts to approximately 60%, independent of the duration of gluten-free diet. In severe cases of coeliac disease, the prevalence increases to 80%. A deficiency of IgM memory B lymphocytes, which play a role in the protection from bacteria, particularly encapsulated bacteria (e.g. Streptococcus pneumoniae), is held responsible for the hypofunction of the spleen accompanying coeliac disease.

24
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
In unproblematic cases of coeliac disease or without the presence of further autoimmune diseases the probability of developing a splenic hypofunction is about 20%.
Patients with gluten ataxia, a progressive cerebellar dysbasia with generalised muscular dysbalance and loss of proprioception, exhibit antibodies against gliadin both in the intestine and in the brain. This supports the assumption that gluten ataxia is immune mediated and belongs to the same group of diseases as coeliac disease and dermatitis herpetiformis.
In women with repeated foetal losses during the first trimester of pregnancy it has been shown that a subclinical form of coeliac disease is the cause in 5% of cases. Since the foetal loss can probably be avoided with a gluten-free diet, a serological screening test is particularly important in these patients, especially given that the disease is only diagnosed in 10% of affected individuals.
An important contribution to the diagnosis of gluten-sensitive enteropathy and dermatitis herpetiformis is provided by the (non-invasive) determination of antibodies (IgA and IgG), against endomysium by means of IIFT, against gliadin and tissue transglutaminase by means of ELISA and also by means of new highly specific tests, such as the Anti-Gliadin (GAF-3X) ELISA and the EUROPLUS Anti-Gliadin (GAF-3X) IIFT.
The serological investigation by IIFT and/or ELISA confirms the clinical diagnosis. It should also be performed in relatives of patients with coeliac disease to discover a predisposition. The determination of antibodies against gliadin is also suitable for use in monitoring the course of therapy and for control of a gluten-free diet or a gluten load test.
A characteristic rise or fall in titers of antibodies against gliadin can spare the patient an additional biopsy of the small intestine. The prevalence of specific antibodies in children with coeliac disease on a gluten-free diet depends on the patient’s compliance with the diet and amounts to around 15-30% according to literature. If a relapse takes place under gluten loading, the level of IgA and IgG antibodies against gliadin rises within a few days.
In most studies, IgA specific tests for the determination of antibodies against endomysium and tissue transglutaminase have been described as highly sensitive and highly specific with values of more than 95% for both parameters. They show the best results of conventional tests, both in adults and in children. Samples taken among the Italian and Belgian population show that 95% of patients with untreated coeliac disease exhibit IgA specific antibodies against endomysium. With the development of a state-of-the-art “designer antigen”, from which the immunologically reactive surface is created, the specificity of the Anti-Gliadin (GAF-3X) ELISA and the EUROPLUS Anti-Gliadin (GAF-3X) IIFT has increased to nearly 100%. It is a recombinant “gliadin-analogue fusion peptide”, which produces a positive reaction almost exclusively in patients with coeliac disease and dermatitis herpetiformis, but not in healthy persons or patients with other gastrointestinal diseases. The fusion peptide consists of two components: a deamidated epitope of gliadin consisting of nine amino acids, and an artificial gliadin-homologue octapeptide.
Up until now, natural full-length gliadin has been used as target antigen for the determination of antibodies against gliadin.
New scientific knowledge shows, however, that only a tenth of the gliadin molecule is pathophysiologically and diagnostically relevant. Antibodies against these molecular sections are formed exclusively in patients with coeliac disease and not in healthy people. The remaining 90% of gliadin is just immunological ballast for diagnostics, acting as a target for unspecific reactions. In the most up-to-date test systems this portion is left out, resulting in a huge increase in specificity. The serological determination of IgA and IgG antibodies against GAF-3X and endomysium (tissue transglutaminase) is a cost-effective and patient-friendly method for the diagnosis of coeliac disease and dermatitis herpetiformis, coeliac disease with splenic hypofunction and subclinical coeliac disease in women with repeated foetal loss during the first trimester and for the clarification of gluten ataxia.

25
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
Literature references
1. Cassinotti A, Birindelli S, Clerici M, Trabattoni D, Lazzaroni M, Ardizzone S, Colombo R, Rossi E, Bianchi Porro G. (2009). HLA and autoimmune digestive disease: A clinically orientes review for gastroenterologists. The American Journal of Gastroenterology 104 (2009) 195-217.
2. Costantini S, Rossi M, Colonna G, Facchiano AM. Modelling of HLA-DQ2 and its interaction with gluten peptides to explain molecular recognition in celiac disease. J Mol Graph Model 23 (2005) 419-431.
3. Di Sabatino A, Rosado MM, Cazzola P, Riboni R, Biagi F, Carsetti R, Corazza GR. Splenic hypofunction and the spectrum of autoimmune and malignant complications in celiac disease. Clin Gastroenterol Hepatol 4 (2006) 179-186.
4. EUROIMMUN AG. Stöcker W, Schlumberger W, Krüger C. Alle Beiträge zum Thema Autoimmundiagnostik. In: Gressner A, Arndt T (Hrsg.) Lexikon der Medizinischen Laboratoriumsdiagnostik. 2. Auflage. Springer Medizin Verlag, Heidelberg (2012).
5. Fallang LE, Bergseng E, Hotta K, Berg-Larsen A, Kim CY, Sollid LM. Differences in the risk of celiac disease associated with HLA-DQ2.5 or HLA-DQ2.2 are related to sustained gluten antigen presentation. Nat Immunol. 2009 Oct;10(10):1096-101
6. Husby S, Koletzko S, Korponay-Szabó IR, Mearin ML, Phillips A, Shamir R, Troncone R, Giersiepen K, Branski D, Catassi C, Lelgeman M, Mäki M, Ribes-Koninckx C, Ventura A, Zimmer KP; ESPGHAN Working Group on Coeliac Disease Diagnosis; ESPGHAN Gastroenterology Committee; European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr. 2012 Jan;54(1):136-60
7. Jones RB, Robins GG, Howdle PD. Advances in celiac disease. Curr Opin Gastroenterol 22 (2006) 117-123.
8. Monsuur AJ, de Bakker PI, Zhernakova A, Pinto D, Verduijn W, Romanos J, Auricchio R, Lopez A, van Heel DA, Crusius JB, Wijmenga C. Effective detection of human leukocyte antigen risk alleles in celiac disease using tag single nucleotide polymorphisms. PLoS One. 2008 May 28;3(5):e2270.
9. Murray JA, Breanndan Moore S, Van Dyke CT, Lahr BD, Dierkhising RA, Zinsmeister AR, Melton LJ, Kroning CM, El-Yousseff M, Czaja AJ. (2007). HLA DQ gene dosage and risk and severity of celiac disease. Clinical Gastroenterology and Hepatology, 5, S. 1406-1412.
10. Mubarak A, Spierings E, Wolters V, van Hoogstraten I, Kneepkens CM, Houwen R. Human leukocyte antigen DQ2.2 and celiac disease. J Pediatr Gastroenterol Nutr. 2013 Apr;56(4):428-30
11. Prause C, Probst* C, Dähnrich* C, Schlumberger* W, Stöcker* W, Richter T, Hauer AC, Stern M, Uhlig H, Laass M, Zimmer KP, Mothes T. [*EUROIMMUN AG]. Deamidated gliadin peptides are superior to native gliadin in ELISA for diagnosis of coeliac disease. In: Conrad K et al. (Hrsg.). From Etiopathogenesis to the Prediction of Autoimmune Diseases: Relevance of Autoantibodies. Pabst Science Publishers 5 (2007) 302-307.
12. Probst* C, Dähnrich* C, Schlumberger* W, Stöcker* W, Komorowski* L, Mothes T. [*EUROIMMUN AG]. Verfahren und Immunabsorbentien zur spezifischen Detektion und Absorption Zöliakie- und Dermatitis herpetiformis assoziierter Antikörper. DE 10 2007 025 291.0 (2007).
13. Rashtak S, Rashtak S, Snyder MR, Pittock SJ, Wu TT, Gandhi MJ, Murray JA. Serology of celiac disease in gluten-sensitive ataxia or neuropathy: Role of deamidated gliadin antibody. J Neuroimmunol 2010 Nov 5.
26
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G
14. Rose C, Dähnrich* C, Probst* C, Komorowski* L, Stöcker* W, Schlumberger* W, Zillikens D. [*EUROIMMUN AG]. Anti-GAF(3X) ELISA (IgG) in combination with Anti-tTG-ELISA (IgA) idenifies 100% of celiac disease patients with dermatitis herpetiformis Duhring and positive intestinal biopsy (March III). Abstract zum 6. International Congress on Autoimmunity in Porto, Portugal (2008).
15. Schirru E, Jores RD, Cicotto L, Frau F, De Virgiliis S, Rossino R, Macis MD, Lampis R, Congia M. High frequency of low risk HLA class II genotypes in latent celiac disease. Hum Immunol 2010 Nov 11.
16. Seah PP, Fry L, Rossiter MA, Hoffbrand AV, Holborow EJ. Antireticulin antibodies in childhood celiac disease. Lancet 2 (1971) 681-682.
17. Setty M, Hormaza L, Guandalini S. Celiac disease: risk assessment, diagnosis, and monitoring. Mol Diagn Ther 12 (2008) 289-298.
18. Sugai E, Vazquez H, Nachman F, Moreno ML, Mazure R, Smecuol E, Niveloni S, Cabanne A, Kogan Z, Gomez JC, Maurino E, Bai JC. Accuracy of testing for antibodies to synthetic gliadin-related peptides in celiac disease. Clin Gastroenterol Hepatol 4 (2006) 1112-1117.
19. Tollefsen S, Arentz-Hansen H, Fleckenstein B, Molberg O, Raki M, Kwok WW, Jung G, Lundin KE, Sollid LM. HLA-DQ2 and -DQ8 signatures of gluten T cell epitopes in celiac disease. J Clin Invest 116 (2006) 2226-2236.
20. Megiorni F, Mora B, Bonamico M, Barbato M, Nenna R, Maiella G, Lulli P, Mazzilli MC. HLA-DQ and risk gradient for celiac disease. Hum Immunol. 2009 Jan;70(1):55-9.
21. Megiorni F, Pizzuti A. HLA-DQA1 and HLA-DQB1 in Celiac disease predisposition: practical implications of the HLA molecular typing. J Biomed Sci. 2012 Oct 11;19:88.

27
EUROIMMUN M e d i z i n i s c h e L a b o r d i a g n o s t i k a A G

Related Documents




![DNA microarrays for SNP profi ling in thrombosis and … · 2015-07-22 · DNA microarray systems such as EUROArray [1, 2]. This microarray system pro-vides fast and efficient SNP](https://static.cupdf.com/doc/110x72/5ec9bd2b60e8c147cb596639/dna-microarrays-for-snp-proi-ling-in-thrombosis-and-2015-07-22-dna-microarray.jpg)






