Estimation of the Optimal Brachytherapy Utilization Rate in the Treatment of Carcinoma of the Uterine Cervix Review of Clinical Practice Guidelines and Primary Evidence Stephen Thompson, MBBS Geoff Delaney, MBBS, MD Gabriel Sam Gabriel, MBBS, MPH Susannah Jacob, MBBS, MD, MHA Prabir Das, MBBS, MPH Michael Barton, MBBS Collaboration for Cancer Outcomes Research and Evaluation (CCORE), Liverpool Hospital, Sydney, Australia. BACKGROUND. Brachytherapy (BT) is an integral part of cervical carcinoma treat- ment. There have been no attempts to estimate the optimal proportion of new cervi- cal carcinoma cases that should be treated with BT, that is, the optimal rate of brachytherapy utilization (BTU). METHODS. Evidence-based guidelines and primary evidence were used to construct a BTU tree for carcinoma of the uterine cervix. Searches were performed of the epide- miological literature to ascertain the proportion of patients who fulfilled criteria for BT. The robustness of the model was tested by sensitivity analyses and by peer review. A patterns of care study of BT in New South Wales for 2003 was conducted, and actual BTU for cervical carcinoma determined. The differences between optimal and actual rates of BTU were assessed. RESULTS. The optimal cervical carcinoma BTU was 49% (range, 42% to 50%). In New South Wales in 2003, actual BTU was only 30% of 256 cervical carcinoma patients. The major discrepancy was for FIGO stage IB-IIA disease, where there was an under- utilization of BT, estimated to be 15% actual use compared with 47% optimal use. In Surveillence, Epidemiology, and End Results (SEER) areas, there was underutilization for stage IB-IIA (22% actual BTU versus 47% optimal BTU) and for stage IIB-IVA (54% actual BTU versus 100% optimal BTU). CONCLUSIONS. BT for cervical carcinoma is underutilized in New South Wales and in SEER areas. The authors’ model of optimal BTU can be used as a quality assurance tool to provide an evidence-based benchmark against which actual patterns of prac- tice can be measured. The model can also be used to help determine adequacy of BT resource allocation. Cancer 2006;107:2932–41. Ó 2006 American Cancer Society. KEYWORDS: cervical carcinoma, carcinoma of the uterine cervix, brachytherapy, radiotherapy, utilization rate, patterns of care studies. T he incidence of cervical carcinoma is decreasing in first world countries such as Australia. 1 Despite this, and the promise of newly developed cervical carcinoma vaccines, 2 cervical carcinoma is still the third largest cancer killer of women world-wide, causing 274,000 deaths in 2002. 3 Cervix cancer is a curable cancer, but achiev- ing the best results depends on well-organized and appropriately resourced cancer services. Previous studies have shown best results to be critically dependent on service-related factors such as dose and number of patients treated. 4–8 Brachytherapy (BT) is an integral part of the cervical carcinoma treatment armamentarium. It is a techni- cally demanding and highly specialized method of radiotherapy (RT) delivery. Depending on equipment usage, capital expenditures and staff costs may be high. However, there have been no attempts to esti- We thank the Court of Reviewers who critiqued the utilization tree: Prof David Allen, Prof Johnathan Carter, Prof Neville Hacker, Prof Roger Houghton, Prof Graeme Morgan, Prof Kailash Narayan, Prof Michael Quinn, Dr Colin Bull, Dr Catherine Clark, Dr Viet Do, and Dr Tony Proietto. Address for reprints: Stephen Thompson, MBBS, Department of Radiation Oncology, Prince of Wales Hospital, High St, Randwick, NSW 2031, Australia; Fax: (011) 61 2 9382 2550; E-mail: stephen. [email protected] Received August 23, 2006; revision received September 25, 2006; accepted September 26, 2006. ª 2006 American Cancer Society DOI 10.1002/cncr.22337 Published online 15 November 2006 in Wiley InterScience (www.interscience.wiley.com). 2932

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Estimation of the Optimal Brachytherapy Utilization Ratein the Treatment of Carcinoma of the Uterine CervixReview of Clinical Practice Guidelines and Primary Evidence
Stephen Thompson, MBBSGeoff Delaney, MBBS, MDGabriel Sam Gabriel, MBBS, MPHSusannah Jacob, MBBS, MD, MHAPrabir Das, MBBS, MPHMichael Barton, MBBS
Collaboration for Cancer Outcomes Research andEvaluation (CCORE), Liverpool Hospital, Sydney,Australia.
BACKGROUND. Brachytherapy (BT) is an integral part of cervical carcinoma treat-
ment. There have been no attempts to estimate the optimal proportion of new cervi-
cal carcinoma cases that should be treated with BT, that is, the optimal rate of
brachytherapy utilization (BTU).
METHODS. Evidence-based guidelines and primary evidence were used to construct a
BTU tree for carcinoma of the uterine cervix. Searches were performed of the epide-
miological literature to ascertain the proportion of patients who fulfilled criteria for
BT. The robustness of the model was tested by sensitivity analyses and by peer review.
A patterns of care study of BT in New South Wales for 2003 was conducted, and
actual BTU for cervical carcinoma determined. The differences between optimal and
actual rates of BTUwere assessed.
RESULTS. The optimal cervical carcinoma BTU was 49% (range, 42% to 50%). In New
South Wales in 2003, actual BTU was only 30% of 256 cervical carcinoma patients.
The major discrepancy was for FIGO stage IB-IIA disease, where there was an under-
utilization of BT, estimated to be 15% actual use compared with 47% optimal use. In
Surveillence, Epidemiology, and End Results (SEER) areas, there was underutilization
for stage IB-IIA (22% actual BTU versus 47% optimal BTU) and for stage IIB-IVA (54%
actual BTU versus 100% optimal BTU).
CONCLUSIONS. BT for cervical carcinoma is underutilized in New South Wales and in
SEER areas. The authors’ model of optimal BTU can be used as a quality assurance
tool to provide an evidence-based benchmark against which actual patterns of prac-
tice can be measured. The model can also be used to help determine adequacy of BT
resource allocation. Cancer 2006;107:2932–41.� 2006 American Cancer Society.
KEYWORDS: cervical carcinoma, carcinoma of the uterine cervix, brachytherapy,radiotherapy, utilization rate, patterns of care studies.
T he incidence of cervical carcinoma is decreasing in first world
countries such as Australia.1 Despite this, and the promise of
newly developed cervical carcinoma vaccines,2 cervical carcinoma is
still the third largest cancer killer of women world-wide, causing
274,000 deaths in 2002.3 Cervix cancer is a curable cancer, but achiev-
ing the best results depends on well-organized and appropriately
resourced cancer services. Previous studies have shown best results to
be critically dependent on service-related factors such as dose and
number of patients treated.4–8 Brachytherapy (BT) is an integral part
of the cervical carcinoma treatment armamentarium. It is a techni-
cally demanding and highly specialized method of radiotherapy (RT)
delivery. Depending on equipment usage, capital expenditures and
staff costs may be high. However, there have been no attempts to esti-
We thank the Court of Reviewers who critiqued theutilization tree: Prof David Allen, Prof JohnathanCarter, Prof Neville Hacker, Prof Roger Houghton,Prof Graeme Morgan, Prof Kailash Narayan, ProfMichael Quinn, Dr Colin Bull, Dr Catherine Clark,Dr Viet Do, and Dr Tony Proietto.
Address for reprints: Stephen Thompson, MBBS,Department of Radiation Oncology, Prince of WalesHospital, High St, Randwick, NSW 2031, Australia;Fax: (011) 61 2 9382 2550; E-mail: [email protected]
Received August 23, 2006; revision receivedSeptember 25, 2006; accepted September 26,2006.
ª 2006 American Cancer SocietyDOI 10.1002/cncr.22337Published online 15 November 2006 in Wiley InterScience (www.interscience.wiley.com).
2932
mate the optimal proportion of new cervical carci-
noma cases that should be treated with BT.
The current study had two aims: 1) The first was to
estimate the optimal brachytherapy utilization (BTU)
rate for treatment of carcinomas of the uterine cervix.
The optimal BTU was the ideal proportion, based on
the best available evidence, of those patients who
should have been treated with BT at least once during
the course of their illness. 2) The second aim was to
compare the optimal BTU with actual BTU. The actual
BTU was defined as the proportion of patients with cer-
vical carcinoma who received at least 1 course of BT
during the course of their illness.
MATERIALS AND METHODSOptimal Brachytherapy UtilizationMethods similar to those described by Tyldesley et al.9
and Delaney et al.10 in their estimates of optimal exter-
nal beam radiation therapy (EBRT) utilization rates in
the treatment of various cancers were used to develop a
model of the optimal BTU for cervical carcinoma.
Review of evidence for the efficacy of brachytherapySystematic Medline searches, manual review of biblio-
graphies, and expert advice were used to identify
English-language evidence-based clinical practice
guidelines for management of cervical carcinoma.
These were used to derive indications and contraindi-
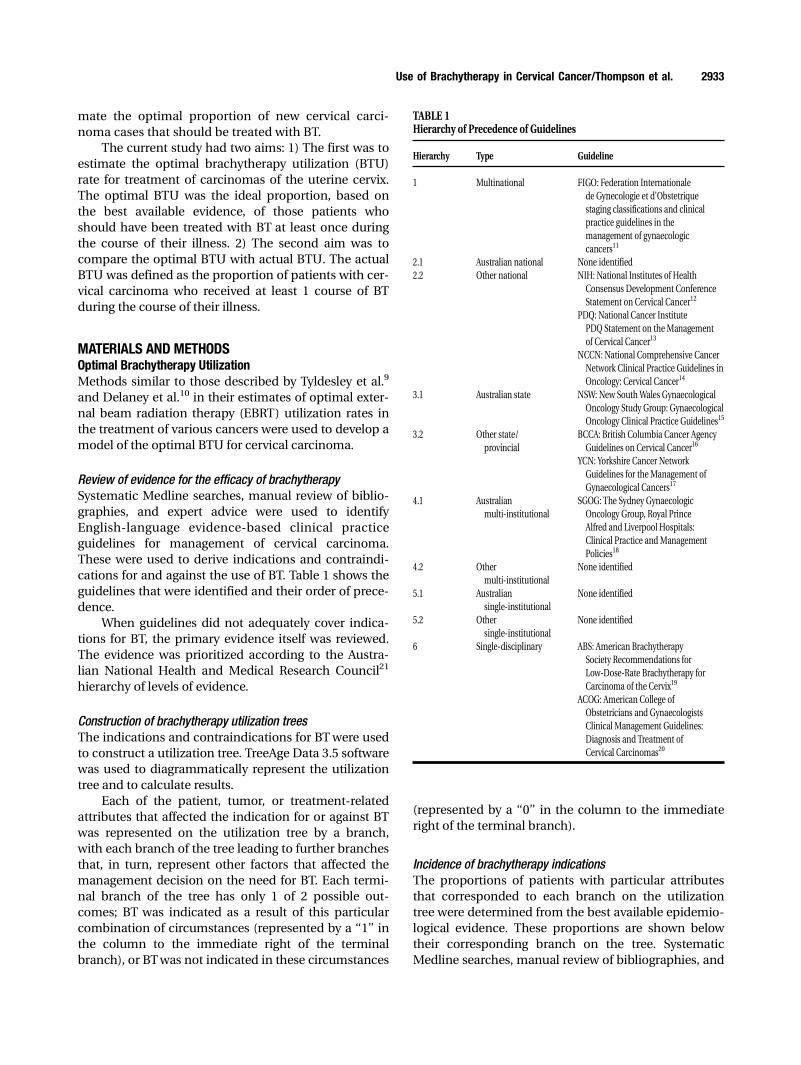
cations for and against the use of BT. Table 1 shows the
guidelines that were identified and their order of prece-
dence.
When guidelines did not adequately cover indica-
tions for BT, the primary evidence itself was reviewed.
The evidence was prioritized according to the Austra-
lian National Health and Medical Research Council21
hierarchy of levels of evidence.
Construction of brachytherapy utilization treesThe indications and contraindications for BTwere used
to construct a utilization tree. TreeAge Data 3.5 software
was used to diagrammatically represent the utilization
tree and to calculate results.
Each of the patient, tumor, or treatment-related
attributes that affected the indication for or against BT
was represented on the utilization tree by a branch,
with each branch of the tree leading to further branches
that, in turn, represent other factors that affected the
management decision on the need for BT. Each termi-
nal branch of the tree has only 1 of 2 possible out-
comes; BT was indicated as a result of this particular
combination of circumstances (represented by a ‘‘1’’ in
the column to the immediate right of the terminal
branch), or BTwas not indicated in these circumstances
(represented by a ‘‘0’’ in the column to the immediate
right of the terminal branch).
Incidence of brachytherapy indicationsThe proportions of patients with particular attributes
that corresponded to each branch on the utilization
tree were determined from the best available epidemio-
logical evidence. These proportions are shown below
their corresponding branch on the tree. Systematic
Medline searches, manual review of bibliographies, and
TABLE 1Hierarchy of Precedence of Guidelines
Hierarchy Type Guideline
1 Multinational FIGO: Federation Internationale
de Gynecologie et d’Obstetrique
staging classifications and clinical
practice guidelines in the
management of gynaecologic
cancers11
2.1 Australian national None identified
2.2 Other national NIH: National Institutes of Health
Consensus Development Conference
Statement on Cervical Cancer12
PDQ: National Cancer Institute
PDQ Statement on theManagement
of Cervical Cancer13
NCCN: National Comprehensive Cancer
Network Clinical Practice Guidelines in
Oncology: Cervical Cancer14
3.1 Australian state NSW: New SouthWales Gynaecological
Oncology Study Group: Gynaecological
Oncology Clinical Practice Guidelines15
3.2 Other state/
provincial
BCCA: British Columbia Cancer Agency
Guidelines on Cervical Cancer16
YCN: Yorkshire Cancer Network
Guidelines for theManagement of
Gynaecological Cancers17
4.1 Australian
multi-institutional
SGOG: The Sydney Gynaecologic
Oncology Group, Royal Prince
Alfred and Liverpool Hospitals:
Clinical Practice and Management
Policies18
4.2 Other
multi-institutional
None identified
5.1 Australian
single-institutional
None identified
5.2 Other
single-institutional
None identified
6 Single-disciplinary ABS: American Brachytherapy
Society Recommendations for
Low-Dose-Rate Brachytherapy for
Carcinoma of the Cervix19
ACOG: American College of
Obstetricians and Gynaecologists
Clinical Management Guidelines:
Diagnosis and Treatment of
Cervical Carcinomas20
Use of Brachytherapy in Cervical Cancer/Thompson et al. 2933

expert advice were used to identify English-language lit-
erature that provided data used to estimate the size of
these proportions. Usually more than 1 epidemiological
source of data for each branch of these utilization trees
was identified. Competing epidemiological data were
ranked by quality as shown in Table 2 by using criteria
modified by Delaney et al.10 that were previously deter-
mined by Tyldesley et al.9 Precedence was given to
higher ranking epidemiological data, as these data were
less likely to suffer from referral bias and sampling
error. Where 2 or more sources of data of equivalent
quality (based on criteria in Table 2) were found, a
weighted average of the results was calculated. If large
differences in incidences existed between similar stu-
dies, then the effect of this uncertainty on the BTU esti-
mate was estimated by sensitivity analysis.
Calculation of the optimal brachytherapy utilization rateThe proportion of patients with each indication for BT
was calculated by multiplying the proportions of
patients with each individual attribute that constituted
the BT indication. This proportion is shown in the sec-
ond column to the right of the terminal branch. The
optimal BTU was calculated by adding the proportions
of patients for all terminal branches that end with an
indication for BT.
Expert reviewTo obtain multidisciplinary input and remove potential
for investigator bias, a panel of experts in cervical can-
cer radiation oncology and gynecological oncology
from across Australia formed a Court of Reviewers for
the model. This Court of Reviewers was drawn from the
group who were asked to review the study of optimal
rates of EBRT.10 Minor changes were recommended
and incorporated.
Sensitivity analysisUncertainties in the indications for BT or in the epide-
miological data were potential sources of error in the
model. The robustness of the utilization tree and the
magnitude of the potential sources of error were mod-
eled by sensitivity analyses. TreeAge Data 3.5 software
enables 1-way sensitivity analyses to be performed,
altering a single variable (such as an indication for BTor
the proportion of patients with a particular attribute
that affects a treatment decision) to assess the effect
that this change has on the optimal BTU.
Actual Brachytherapy UtilizationThe actual BTU for cervical carcinoma was determined
as part of a Patterns of Care Study for 2003 for New
SouthWales (NSW). NSW is the largest state of Australia,
with a population of 6.6 million in 2003, 63% of whom
live in Sydney.22 Site visits were made to all 9 radiation
oncology departments in NSW that deliver BT and de-
identified data on all patients who were treated with BT
in 2003 were extracted from patient records. Information
on all NSW cervical carcinoma patients for 2003 was
obtained from the Health Outcomes Information Statisti-
cal Toolkit (HOIST) database. HOIST contains data from
the NSW Central Cancer Registry. It does not contain
data on stage of disease for cervical carcinoma. The likely
stage distribution of cervical carcinoma in NSW was
assumed to be similar to that of the United States, and,
therefore, the incidence of each stage of cervical carci-
noma in NSW was extrapolated from the Surveillance,
Epidemiology, and End Results (SEER) Database.23 SEER
data for 1997–2001 were used to estimate the distribution
of stages and substages because no other source pro-
vided this level of information. Comparison of cervical
screening rates24,25 and overall cervical carcinoma stage
distribution in US and Australia23,26 showed similar
results, suggesting that the SEER substage distributions
are likely to be representative of those in Australia. The
actual BTU was calculated by dividing the number of
NSW cervical carcinoma patients treated with BT by the
estimated stage incidence of cervical carcinoma. Ethics
approval was obtained from South Western Sydney Area
Health Service (Western Zone) Human Research Ethics
Committee.
RESULTSOptimal Brachytherapy Utilization RateThe BT utilization tree for cervical carcinoma is shown
in Fig. 1.
Table 3 lists the patient, tumor, and treatment-
related attributes for each indication for BT, Austra-
lia’s National Health and Medical Research Council
(NHMRC) level of evidence for the indication, guide-
TABLE 2Hierarchy of Epidemiological Data9,10
Quality of
source Source type
a Australian National Epidemiological data
b Australian State Cancer Registry
g Epidemiological databases from other
large international groups (eg, SEER)
d Results from reports of a random sample from a population
e Comprehensive multi-institutional database
z Comprehensive single-institutional database
u Multi-institutional reports on selected
groups (eg, multi-institutional clinical trials)
l Single-institutional reports on selected groups of cases
m Expert opinion
2934 CANCER December 15, 2006 / Volume 107 / Number 12

FIGURE 1. This is the decision tree for optimal brachytherapy utilization to treat cervical carcinoma. LVI indicates lymphatic vascular space invasion; PLND, pelviclymph node dissection; LN, lymph nodes; GOG, Gynecology Oncology Group.
Use of Brachytherapy in Cervical Cancer/Thompson et al. 2935

lines that support it, and the proportion of patients with
uterine cervical carcinoma that have that indication for
BT. Of patients with cervical carcinoma, 49% have an in-
dication for BT (the optimal BTU). The optimal BTU for
FIGO stage IA disease is 14%, for IB-IIA disease 47%, for
IIB-IVA disease 100%, and for IVB disease 0%.
Table 4 summarizes epidemiological data related to
indications for or against BT: the proportion of patients
with cervical carcinoma with the BT indication or con-
traindication, the quality of epidemiological evidence,
and sources of data.
Two issues require further explanation. There were
no data available on the proportion of patients with
nonmetastatic cancer who were unfit for surgery
(branches G, H, K, and P, Fig. 1). We used NSW commu-
nity self-reported health status,30 adjusting the results
by the known age distribution of patients with cervical
cancer1: 19% of this population reported their health to
be in the 2 worst of 5 categories (‘‘fair’’ or ‘‘poor’’). It
was assumed that these patients would not be fit for
radical surgical resection, apart from therapeutic coni-
zation in the case of stage IA1 disease. All other medi-
cally unfit patients would be referred for RT including
BT. We chose this measure because it is NSW popula-
tion-based data and because self-reported health status
is a predictor of later morbidity and death.44,45 We per-
formed sensitivity analysis to estimate the effect of
considering only the 4% of patients with ‘‘poor’’ self-
reported health as nonoperable candidates. Note that
the 19% figure is similar to that obtained by using data
from Tyldesley et al.,31 who used the Canadian National
Population Health Survey to estimate the proportion of
Canada’s population to be of poor performance status
by age category (Eastern Cooperative Oncology Group
[ECOG] scores of 2 or 3 and 4). These data were as-
sumed to be representative of the performance status
of Australian patients with nonmetastatic cervical can-
cer, and data were adjusted for the age distribution of
Australian patients with cervical cancer1 to calculate
the average percentage of Australian patients with non-
metastatic cervical cancer who had poor performance
status. This average was 16%.
The other issue is whether patients with stage IB-
IIA disease should be managed with primary surgery or
RT (branches O, Fig. 1). There has been 1 randomized
trial of surgery versus RT including BT for operable cer-
vical carcinoma.33 Although disease-free survival rates
and overall survival rates were identical in both arms of
the study, the authors suggested that morbidity of RT
(particularly in postmenopausal women) was less.
TABLE 3Cervical Carcinoma: Indications for Brachytherapy—Levels and Sources of Evidence
Outcome no. Clinical scenarioTreatmentindicated
Level ofevidence References
Percentage of
all cervixcancer patients
3 Stage IA1 (Cone biopsy); LVI negative;
Margin positive; Medically inoperable
BT IV 12, 13, 14, 16, 19 1.0
5 Stage IA1 (Cone biopsy); LVI positive;
Medically operable (Hyst and PLND);
LN negative; Local recurrence
EBRTand BT IV 12, 13, 14, 15, 18 0.1
7 Stage IA1 (Cone biopsy); LVI positive;
Medically inoperable
EBRTand BT IV 12, 13, 14, 16, 19 0.2
9 Stage IA2 (Cone biopsy); Medically
operable (Hyst and PLND); LN negative;
Local recurrence
EBRTand BT IV 12, 13, 14, 15, 18 0.3
11 Stage IA2 (Cone biopsy); Medically inoperable EBRTand BT IV 12, 13, 14, 16, 19 2.2
13 Stage IB-IIA; <4 cm; Medically operable
(Hyst and PLND); Margin negative;
LN negative; GOG score<120; Local recurrence
(nil distant metastases); Central local recurrence
EBRTand BT IV 12, 13, 14, 15, 18 0.4
17 Stage IB-IIA; <4 cm; Medically operable
(Hyst and PLND); Margin positive;
Vaginal margin positive
EBRTand BT IV 12, 13, 14, 18, 19 0.9
19 Stage IB-IIA; <4 cm; Medically inoperable EBRTand BT IV 12, 13, 15, 16, 17, 18, 19 5.6
20 Stage IB-IIA; >4 cm EBRTand BT II, III 12, 13, 16, 18, 19 13.3
21 Stage IIB-IVA EBRTand BT III 11, 12, 13, 14, 15, 16, 17, 18, 19, 20 25
Total 49
LVI indicates lymphatic vascular space invasion; Hyst, hysterectomy; PLND, pelvic lymph node dissection; LN, lymph node.
2936 CANCER December 15, 2006 / Volume 107 / Number 12

TABLE 4Cervical Carcinoma: Incidence of Attributes Used to Define Indications for Brachytherapy
Key*Population orsubpopulation of interest Attribute
Proportion of
population withthis attribute
Quality ofinformation References
A All registry cancers Gynecological cancer 0.045 a AIHW1
B All gynecological cancer Cervical carcinoma 0.194 a AIHW1
C All cervical carcinoma Stage IA 0.26 g SEER23
D Stage IA Stage IA1 0.55 g SEER23
E Stage IA1, (conization) LVI negative 0.92 e Ostor AG27
F Stage IA1, (conization);
LVI negative
Margin positive 0.60 z Jones et al.28
0.10 z Creasman et al.29
G Stage IA1, (conization);
LVI negative;
Margin positive
Medically operable (Hyst) 0.81 b NSWHealth Surveys30
0.84 g Tyldesley et al.31
H Stage IA1, (conization);
LVI positive
Medically operable
(Hyst and PLND)
0.81 b NSWHealth Surveys30
0.84 g Tyldesley et al.31
I Stage IA1, (conization);
LVI positive; Medically operable,
(Hyst and PLND
LN negative 0.97 e Ostor AG27
J Stage IA1, (conization);
LVI positive; Medically operable,
(Hyst and PLND); LN negative
Local recurrence 0.06 e Ostor AG27
K Stage IA2 Medically operable
(Hyst and PLND)
0.81 b NSWHealth Surveys30
0.84 g Tyldesley et al.31
L Stage IA2; Medically operable,
(Hyst and PLND)
LN negative 0.94 e Ostor AG27
M Stage IA2; Medically operable,
(Hyst and PLND); LN negative
Local recurrence 0.03 e Ostor AG27
N All cervical carcinoma Stage IB/IIA 0.43 g SEER23
O Stage IB/IIA ‘‘Non-bulky’’disease 0.69 z Fuller et al.32
0.67 u Landoni et al.33
P Stage IB/IIA;
‘‘Non-bulky’’disease
Medically operable
(Hyst and PLND)
0.81 b NSWHealth Surveys30
0.84 g Tyldesley et al.31
Q Stage IB/IIA; ‘‘Non-bulky’’disease;
Medically operable, (Hyst and PLND)
Margin negative 0.94 u Landoni et al.33
R Stage IB/IIA; ‘‘Non-bulky’’disease;
Medically operable; (Hyst and PLND);
Margin negative
LN negative 0.75 u Landoni et al.33
0.84 z Kim et al.34
0.86 z Kamura et al.35
S Stage IB/IIA; ‘‘Non-bulky’’disease;
Medically operable, (Hyst and PLND);
Margin negative; LN negative
‘‘Low risk’’ for recurrence
(GOG score< 120)
0.84 e Delgado et al.36
0.76 u Landoni et al.33
0.73 z Kridelka et al.37
T Stage IB/IIA; ‘‘Non-bulky’’disease;
Medically operable, (Hyst and PLND);
Margin negative; LN negative;
‘‘Low risk’’ for recurrence (GOG score< 120)
Local recurrence without
distant metastases
0.07 e Delgado et al.,36 Samlal et al.38
0.08 u Landoni et al.33
U Stage IB/IIA; ‘‘Non-bulky’’disease;
Medically operable, (Hyst and PLND);
Margin negative; LN negative;
‘‘Low risk’’ for recurrence
(GOG score< 120); Local recurrence
without distant metastases
Central local relapse 0.38 z Look et al.39
0.40 z Chung et al.40
0.42 z Wang et al.41
0.48 z Burke et al.42
V Stage IB/IIA; ‘‘Non-bulky’’disease;
Medically operable, (Hyst and PLND);
Margin positive
Vaginal margin positive 0.64 z Snidjers-Keilholz et al.43
W All cervical carcinoma Stage IIB-IVA 0.25 z SEER23
X All cervical carcinoma Stage IVB 0.06 g SEER23
LVI indicates lymphatic vascular space invasion; Hyst, hysterectomy; PLND, pelvic lymph node dissection; LN, lymph node; GOG, Gynecology Oncology Group.
* Key refers to the corresponding branch of the Utilization Tree in Figure 1.
Use of Brachytherapy in Cervical Cancer/Thompson et al. 2937

Others have contended that this trial actually showed
that morbidity of RT was greater than that of surgery
alone.46 Both FIGO11 and the available Australian
guidelines15,18 recommend surgery for patients with
nonbulky disease who are suitable surgical candidates.
In Australian practice, the vast majority of these pa-
tients are treated by surgery. The exceptions are usually
patients with poor performance status or significant
comorbidity or who refuse surgery. We have, therefore,
followed the Australian guidelines and Australian prac-
tice and calculated based on medically fit patients with
nonbulky IB-IIA disease being treated with primary
surgery and medically unfit patients receiving a defini-
tive RT including BT. Patients with bulky stage IB-IIA
disease have a high risk of locoregional recurrence after
surgery alone.33,47 For these patients, randomized trials
have shown EBRT and BT to be equal to surgery and
EBRT,33 surgery and EBRT to be superior to surgery
alone,47 and completion hysterectomy following RT to
have no benefit.48 Toxicity is increased by combined-
modality treatment.47 For this reason, and the lack of
evidence for a benefit for combined modality treatment
over RT (especially with chemotherapy) alone, guide-
lines12,13,16,18,19 recommend definitive treatment with
chemoradiation, rather than surgery and postoperative
EBRT, for patients with bulky stage IB-IIA disease.
Sensitivity analysisThere were 3 variables with considerable uncertainty in
the epidemiological data. By using reports in the litera-
ture of lowest and highest estimates for these variables,
we performed sensitivity analyses (see Fig. 2) on the
model to estimate the effect that these uncertainties
might have on the final BTU.
1. Proportion of patients with technically operable dis-
ease who were not fit for an operation (Branches G, H, K,
P, Fig. 1). As discussed above, this proportion was cal-
culated at 19%,1,30,31 with sensitivity analysis showing
that if this proportion was reduced to 4%, then the over-
all optimal BTU fell from 49% to 42%, with the rate for
stage IA disease falling from 14% to 4% and the rate for
stage IB-IIA disease falling from 47% to 37%.
2. Margin positivity rate after conization for stage IA1
(Branches F, Fig. 1). Two series have reported margin
positivity after conization for stage IA1 disease. In Jones
et al. 30 of 50 patients28 and in Creasman et al. 4 of 39
patients29 had an average margin positivity rate of 38%
(for these 89 patients). Sensitivity analysis was underta-
ken, varying margin positivity rate from 10% to 60%. As
a result, the BTU for stage IA disease varied from 12% to
16%, and the overall optimal BTU varied from 48% to
50%.
3. Proportion of patients with non-bulky stage IB-IIA
disease and negative surgical margins who also had neg-
ative lymph nodes (Branches R, Fig 1). Extrapolation
from data contained in Landoni et al.33 indicates that
between 73% and 80% of patients with negative mar-
gins also have negative lymph nodes. Varying these
values had no effect on the overall optimal BTU for cer-
vical carcinoma or the rate for stage IB-IIA disease.
Comparison with Actual PracticeA comparison of optimal BTU with actual BTU by stage
is shown in Table 5. Note that for the calculation of
BTU by stage, the denominator is the stage incidence of
cervical carcinoma in NSW, which is an extrapolation
from SEER data23 because local population-based data
FIGURE 2. A sensitivity analysis of optimal brachytherapy utilization for cervical carcinoma is presented here. LVI indicates lymphatic vascular space invasion; PLND,pelvic lymph node dissection; LN, lymph nodes; GOG, Gynecology Oncology Group.
2938 CANCER December 15, 2006 / Volume 107 / Number 12

were not available (see above). Therefore, the figures for
actual BTU by stage are estimates. In NSW in 2003, 77
(30%) of 256 cervical carcinoma patients were treated
with BT, less than two-thirds of the optimal percentage
of 49%. For all stages except stage IB-IIA, the optimal
and the actual BTU were similar. For FIGO stage IA, the
estimated actual BTU was 0%, compared with 14%
(range, 4%–16%) optimal; for stage IIB-IVA disease esti-
mated 92% actual BTU and 100% optimal BTU; and for
stage IVB disease estimated 7% actual and 0% optimal.
Themajor discrepancy was for stage IB-IIA, where there
was an underutilization of BT, estimated 15% actual
compared with 47% optimal BTU (range, 37%–47%).
Only 2 other sources of data on actual practice
were available. Prospective surveys of RT practice were
conducted in Sweden over 12 week periods in 199249
and in 2001.50 In 1992, 39% of patients with cervical car-
cinoma were treated with BT. In 2001, the actual rate
had fallen to 28%. According to the SEER database,23
the corresponding figures for 1992 and 2001 in the US
were 28% and 24%. The SEER figures are for ‘‘first
course of cancer directed treatment’’. BT for disease re-
currence would not be included but only accounts for
0.8% of all indications for BT. The discrepancy appeared
to be most marked for stage IB-IIA disease and for stage
IIB-IVA disease.
DISCUSSIONWe have constructed an evidence-based peer-reviewed
model that assesses the optimal brachytherapy utiliza-
tion rate in the treatment of cervical carcinoma. The
optimal BTU is 49%, (range, 48% to 50%).
Our model of optimal BTU can be used as a quality
assurance tool by comparing the optimal BTU with
actual practice. Compared with our model of optimal
practice, BTwas underutilized in the treatment of cervi-
cal carcinoma in NSW, Sweden, and the US. For NSW,
the underutilization was essentially restricted to FIGO
stages IB-IIA (approximately 15% actual versus 47%
optimal). This is surprising given that earlier research
has shown that the actual utilization of EBRT is close to
optimal, for all stages including early stage disease.51 In
that report, Delaney et al. hypothesized that the reason
the optimal and actual rates were similar was that per-
haps cervical carcinoma is most commonly treated by
specialist gynecological oncologists in a multidisciplin-
ary setting, as opposed to other tumor sites that may be
more commonly managed in a general setting. This
implies that patients with high-risk stage IB-IIA in
NSW are probably being inappropriately treated with
primary surgery and then require adjuvant EBRT,
rather than being treated in accordance with guide-
lines12,13,16,18,19 and evidence33,47,48 with definitive
radiotherapy including BT. The EBRT utilization will
remain optimal in either case, but, in the former case,
the BTU will be suboptimal. Disease control is likely to
be similar with either approach but with greater risk of
toxicity for the patients treated with both surgery and
EBRT.33,47
More concerning is the underuse of BT for patients
with stage IIB-IVA disease in the SEER registry data.
Earlier research showed that for this group of patients
utilization of EBRT was close to optimal.51 There are 3
possible explanations for these 2 observations. Possibly
these patients are being treated with surgery and EBRT
rather than EBRT and BT, against the recommendation
of all guidelines.11–20 Another possible explanation is
that these patients are being treated with definitive RT
using EBRTonly, against guideline recommendations11–20
and with a high likelihood of suboptimal dose, and
reduced local control and survival.4–8,52,53 The third
possibility is that SEER has not reliably recorded the
use of BT in these patients. There are no confirmatory
US BT utilization sources, but for EBRT, SEER’s figures
correlate well with those of the American College of
Surgeons.51 For Sweden, there is no explanation in the
literature of why BT is underutilized for cancer of the
uterine cervix.
This study of optimal and actual BTU for cervical
carcinoma has a number of limitations. As shown in Ta-
ble 3 above, there is a paucity of high-level evidence for
many of the BT indications and contraindications. It
may also be that the model is unable to fully account
TABLE 5Comparison Between Optimal and Actual BTU
FIGO stageOptimal BTUpercentage
Actual BTUpercentage
NSW 2003 Sweden 1992 Sweden 2001 SEER 1992 SEER 2001
IA 14 (4–16) 0 n/a n/a 2 2
IB-IIA 47 (37–47) 15 n/a n/a 28 22
IIB-IVA 100 92 n/a n/a 59 54
IVB 0 7 n/a n/a 11 18
All 49 (42–50) 30 39 28 28 24
Use of Brachytherapy in Cervical Cancer/Thompson et al. 2939

for individual patient circumstances. An example is
increasing patient age, which Delaney et al.10 found to
predict increased use of RT. Another issue, as discussed
above, is the use of the SEER database to give the stage
distribution of cervical cancer for the optimal model
and to provide an estimate of the incidence by stage of
cervical cancer in NSW to enable calculation of the
actual stage BTU in NSW in 2003.
Our model of optimal BT utilization can also be
used to assist in planning BT resource requirements.
In the report on Asia Pacific Region radiotherapy
resources, Tatsuzaki and Levin54 assumed that 50% of
cervical carcinoma patients in the first world would
require BT—similar to our evidence-based estimate of
49%. With the insertion of an appropriate stage distri-
bution into the model, it could be used to provide evi-
dence for or against another Tatsuzaki and Levin
assertion54 that 80% of cases in the developing world
would require BT.
ConclusionsThis study used an evidence-based peer-reviewed
method of calculating the optimal proportion of all
patients with carcinoma of the uterine cervix who
should be treated with BT at some time during the
course of their illness. This optimal brachytherapy utili-
zation rate was 49%. A patterns of care study of BT in
NSW in 2003 has shown that the actual rate of use of BT
is only 30%, with most of the undertreatment occurring
in patients with early stage, potentially operable dis-
ease. Comparison with the SEER database showed that
there is underuse of BT in the US, with this undertreat-
ment occurring in early and in more advanced stages of
disease.
We have used this model of optimal BTUas a quality
assurance tool, thus providing an evidence-based bench-
mark against which we have measured actual patterns of
practice. This model can also be used to determine the
adequacy of current BT resource allocation and to for-
mulate a plan for future BT resource allocation.
REFERENCES1. Australian Institute of Health and Welfare (AIHW). Cancer
incidence data: Cancer age-standardised database. (2000). At
URL: http://www.aihw.gov.au/cancer/datacubes/index.cfm
2. Lowndes CM, Gill ON. Cervical cancer, human papillomavi-
rus, and vaccination. BMJ. 2005;331:915–916.
3. Parkin DM, Bray F, Ferlay J, Pisani P. Global Cancer Statistics,
2002. CA Cancer J Clin. 2005;55:74–108.
4. Lanciano RM, Won M, Coia LR, Hanks GE. Pretreatment and
treatment factors associated with improved outcome in squa-
mous cell carcinoma of the uterine cervix: a final report of the
1973 and 1978 patterns of care studies. Int J Radiat Oncol Biol
Phys. 1991;20:667–676.
5. Hanks GE, Herring DF, Kramer S. Patterns of care outcome
studies. Results of the national practice in cancer of the cer-
vix. Cancer. 1983;51:959–967.
6. Coia L, Won M, Lanciano R, Marcial VA, Martz K, Hanks G.
The Patterns of Care Outcome Study for cancer of the uterine
cervix. Results of the Second National Practice Survey. Cancer.
1990;66:2451–2456.
7. Montana GS, Martz KL, Hanks GE. Patterns and sites of failure
in cervix cancer treated in the USA in 1978. Int J Radiat Oncol
Biol Phys. 1991;20:87–93.
8. Komaki R, Brickner TJ, Hanlon AL, Owen JB, Hanks GE. Long-
term results of treatment of cervical carcinoma in the United
States in 1973, 1978, and 1983: Patterns of Care Study (PCS).
Int J Radiat Oncol Biol Phys. 1995;31:973–982.
9. Tyldesley S, Boyd C, Shulze K, Walker H, Mackillop WJ. Esti-
mating the need for radiotherapy for lung cancer: an evi-
dence-based, epidemiologic approach. Int J Radiat Oncol Biol
Phys. 2001;49:973–985.
10. Delaney GP, Jacob S, Featherstone C & Barton MB. Radiother-
apy in cancer care: estimating optimal utilisation from a
review of evidence-based clinical guidelines. Collaboration
for Cancer Outcomes Research and Evaluation (CCORE),
Liverpool Hospital, Sydney, Australia. 2003. Available at URL:
http://www.ncci.org.au/supp/reports/genreports_2003-2005.
htm
11. Benedet JL, Bender H, Jones H 3rd, Ngan HY, Pecorelli S.
FIGO staging classifications and clinical practice guidelines
in the management of gynecologic cancers. FIGO Committee
on Gynecologic Oncology. Int J Gynecol Obstet. 2000;70:209–
262.
12. National Institutes of Health. Consensus Statement: National
Institutes of Health consensus development conference state-
ment on cervical cancer. Gynecol Oncol. 1997;66:351–361.
13. National Cancer Institute. US National Institutes of Health.
CancerNet PDQ Cancer Information Summaries: Treatment
of Cervical Cancer. 2003. Available at URL: http://cancernet.nci.
nih-gov/cancertopics/pdq/treatment/cervical/healthprofes-
sional
14. National Comprehensive Cancer Network. Clinical Practice
Guidelines in Oncology - v.1.2003 - Cervical Cancer. Available
at URL: http://www.nccn.org/professionals/physician_gls/
pdf/cervical.pdf. 2003. 2004.
15. NSW Gynaecological Oncology Study Group. Gynaecological
Oncology Clinical Practice Guidelines. 2004. Sydney: NSW
Gynaecological Oncology Study Group; 2004.
16. British Columbia Cancer Agency. Cancer Management Guide-
lines. Gynecology. Item 4, Uterine Cervix. 2001. Available at
URL: http://www.bccancer.bc.ca/HPI/CancerManagement-
Guidelines/Gynecology/UterineCervix1of2/default.htm [Ac-
cession date February 2004.]
17. Yorkshire Cancer Network. Guidelines for the Management of
Gynaecological Cancers. 2003. Available at URL: http://york-
shire-cancer-net.org.uk/html/publications/clinical_gynaecology.
htm [Accession date: June 15, 2004.]
18. Sydney Gynaecologic Oncology Group, Sydney Cancer Centre.
Clinical Practice and Management Policies. Johnathan Carter.
1–6-2004. Sydney: Johnathan Carter; 2004. Available at URL:
http://www.gynaecancer.org.au/
19. Nag S, Chao C, Erickson B, et al. The American Brachytherapy
Society recommendations for low-dose-rate brachytherapy
for carcinoma of the cervix. Int J Radiat Oncol Biol Phys. 2002;52:33–48.
20. Committee on Practice Bulletins-Gynecology. ACOG practice
bulletin. Diagnosis and treatment of cervical carcinomas,
number 35, May 2002.Obstet Gynecol. 2002;99(5 pt 1):855–867.
2940 CANCER December 15, 2006 / Volume 107 / Number 12
21. National Health and Medical Research Council. A guide to the
development, evaluation and implementation of clinical
practice guidelines. Appendix B, 56. Canberra: National
Health and Medical Research Council; 1999. Available at URL:
22. Australian Bureau of Statistics. New SouthWales. National Re-
gional Profile 1999 to 2003. Release date 24/11/2005. Available
at URL: www.abs.gov.au/
23. Surveillance, Epidemiology, and End Results (SEER) Program
(www.seer.cancer.gov) SEER*Stat 5.2.2 database. SEER Cancer
Incidence Public-Use Month 2004 Database (1973–2001),
National Cancer Institute, DCCPS, Surveillance Research Pro-
gram, Cancer Statistics Branch, released Month Year, based
on the Month Year submission.
24. NSW Department of Health. Report of The New South Wales
Chief Health Officer. 2006. Adelaide: Centre for Epidemiology
and Research, Population Health Division, NSW Department
of Health; 2006.
25. Sirovich BE, Welch HG. The frequency of Pap smear screening
in the United States. J Gen Intern Med. 2004;19:243–250.
26. South Australian Cancer Registry. 2000 Cancer Report—
Epidemiology of Cancer in South Australia 1977–1999. Ade-
laide: Department of Health, Government of South Australia;
2000.
27. Ostor AG. Pandora’s Box or Ariadne’s Thread? Definition and
prognostic significance of microinvasion in the uterine cervix.
Squamous lesions. Pathol Annu. 1995;(30 pt 2):103–136.
28. Jones WB, Mercer GO, Lewis JL Jr, Rubin SC, Hoskins WJ. Early
invasive carcinoma of the cervix. Gynecol Oncol. 1993;51:26–32.
29. Creasman WT, Fetter BF, Clarke-Pearson DL, Kaufmann L,
Parker RT. Management of stage IA carcinoma of the cervix.
Am J Obstet Gynecol. 1985;153:164–172.
30. NSW Department of Health. Electronic Report of the 1997
and 1998 NSW Health Surveys. Available at URL: www.
health.nsw.gov.au/public-health/nswhs
31. Tyldesley S, Zhang-Salomons J, Groome PA, et al. Association
between age and the utilization of radiotherapy in Ontario.
Int J Radiat Oncol Biol Phys. 2000;47:469–480.
32. Fuller AF, Elliott N, Kosloff C, Hoskins WJ, Lewis JL Jr. Deter-
minants of increased risk for recurrence in patients under-
going radical hysterectomy for stage IB and IIA carcinoma of
the cervix. Gynecol Oncol. 1989;33:34–39.
33. Landoni F, Maneo A, Colombo A, et al. Randomised study of
radical surgery versus radiotherapy for stage Ib-IIa cervical
cancer. Lancet. 1997;350:535–540.
34. Kim SM, Choi HS, Byun JS. Overall 5-year survival and
prognostic factors in patients with Stage IB and IIA cervi-
cal cancer treated by radical hysterectomy and pelvic
lymph node dissection. Int J Gynecol Cancer. 2000;10:305–
312.
35. Kamura T, Tsukamoto N, Tsuruchi N, et al. Multivariate analy-
sis of the histopathologic prognostic factors of cervical cancer
in patients undergoing radical hysterectomy. Cancer. 1992;69:
181–186.
36. Delgado G, Bundy B, Zaino R, Sevin BU, Creasman WT,
Major F. Prospective surgical-pathological study of disease-
free interval in patients with stage IB squamous cell carci-
noma of the cervix: a Gynecologic Oncology Group study.
Gynecol Oncol. 1990;38:352–357.
37. Kridelka FJ, Berg DO, Neuman M, et al. Adjuvant small field
pelvic radiation for patients with high risk, stage IB lymph
node negative cervix carcinoma after radical hysterectomy
and pelvic lymph node dissection. A pilot study. Cancer. 1999;
86:2059–2065.
38. Samlal RA, van der Velden J, Ten Kate FJ, Schilthuis MS,
Hart AA, Lammes FB. Surgical pathologic factors that pre-
dict recurrence in stage IB and IIA cervical carcinoma pa-
tients with negative pelvic lymph nodes. Cancer. 1997;80:
1234–1240.
39. Look KY, Rocereto TF. Relapse patterns in FIGO stage IB carci-
noma of the cervix. Gynecol Oncol. 1990;38:114–120.
40. Chung CK, Nahhas WA, Stryker JA, Curry SL, Abt AB, Mortel R.
Analysis of factors contributing to treatment failures in stages
IB and IIA carcinoma of the cervix. Am J Obstet Gynecol. 1980;
138:550–556.
41. Wang CJ, Lai CH, Huang HJ, et al. Recurrent cervical carci-
noma after primary radical surgery. Am J Obstet Gynecol. 1999;
181:518–524.
42. Burke TW, Hoskins WJ, Heller PB, Shen MC, Weiser EB, Park
RC. Clinical patterns of tumor recurrence after radical hyster-
ectomy in stage IB cervical carcinoma. Obstet Gynecol. 1987;
69(3 pt 1):382–385.
43. Snijders-Keilholz A, Hellebrekers BW, Zwinderman AH, van de
Vijver MJ, Trimbos JB. Adjuvant radiotherapy following radical
hysterectomy for patients with early-stage cervical cancer
(1984–1996). Radiother Oncol. 1999;51:161–7.
44. Idler EL, Benyamini Y. Self-rated health and mortality: a re-
view of twenty-seven community studies. J Health Soc Behav.
1997;38:21–37.
45. McCallum J, Shadbolt B, Wang D. Self-rated health and sur-
vival: a 7-year follow-up study of Australian elderly. Am J Pub-
lic Health. 1994;84:1100–1105.
46. Soutter P. Radical surgery or radiotherapy for stage IB-IIA cer-
vical cancer. Lancet. 1997;350:532.
47. Sedlis A, Bundy BN, Rotman MZ, Lentz SS, Muderspach LI,
Zaino RJ. A randomized trial of pelvic radiation therapy versus
no further therapy in selected patients with stage IB carci-
noma of the cervix after radical hysterectomy and pelvic
lymphadenectomy: a Gynecologic Oncology Group study.
Gynecol Oncol. 1999;73:177–183. Comment in: Gynecol Oncol.
1999;73:175–176.
48. Keys HM, Bundy BN, Stehman FB, et al. Radiation therapy
with and without extrafascial hysterectomy for bulky stage IB
cervical carcinoma: a randomized trial of the Gynecologic
Oncology Group. Gynecol Oncol. 2003;89:343–353.
49. [No authors listed]. A prospective survey of radiotherapy in
Sweden. Acta Oncol. 1996;35suppl 6:47–56.
50. Moller TR,BrorssonB,Ceberg J, et al. Aprospective surveyof radio-
therapypractice 2001 in Sweden.ActaOncol. 2003;42:387–410.
51. Delaney G, Jacob S, BartonM. Estimation of an optimal radio-
therapy utilization rate for gynecologic carcinoma: part I—
malignancies of the cervix, ovary, vagina and vulva. Cancer. 2004;
101:671–681.
52. Perez CA, Breaux S, Madoc-Jones H, et al. Radiation therapy
alone in the treatment of carcinoma of uterine cervix. I. Anal-
ysis of tumor recurrence. Cancer. 1983;51:1393–1402.
53. Lanciano RM, Martz K, Coia LR, Hanks GE. Tumor and treat-
ment factors improving outcome in stage III-B cervix cancer.
Int J Radiat Oncol Biol Phys. 1991;20:95–100.
54. Tatsuzaki H, Levin CV. Quantitative status of resources for
radiation therapy in Asia and Pacific region. Radiother Oncol.
2001;60:81–89.
Use of Brachytherapy in Cervical Cancer/Thompson et al. 2941
Related Documents











