PART IV. PSYCHOPATHOLOGY AND INDIVIDUAL DIFFERENCES ERPs and Psychopathology I. Behavioral Process Issuesa WALTON T. ROTH,b JOSEPH J. TECCE,' ADOLF PFEFFERBAUMP MARGARET ROSENBLOOMP AND ENOCH CALLAWAYd 'Psychiatry Service Veterans Administration Medical Center Palo Alto, California 94304 and Department of Psychiatry and Behavioral Sciences Stanford University Medical Center Stanford, California 94305 'Department of Psychology Boston College Chestnut Hill, Massachusetts 02167 and Department of Neurology Tufts Medical School Boston, Massachusetts 021 I I dLangley Porter Psychiatric Institute University of California San Francisco Medical Center San Francisco, California 941 43 Although ERPs have proven clinically useful in assessing the structural integrity of sensory pathways from the periphery to the cortex, they have failed to play a significant role in the psychiatric clinic, where questions must be answered about the efficiency of more complex forms of mental functioning than those that take place in the sensory system. Even at psychiatric research meetings, ERPs only grace a few posters in the wings, while center stage is occupied by biochemical studies of neurotransmitters or anatomic studies based on the CT scan, or most recently, positron-emission tomography. This is true even though the disorders being investi- gated are first and foremost manifested behaviorally, and the ERPs provide a window on the behaving brain. One can take no solace in believing that clinicians neglect ERPs because they have not heard of them or do not understand them. Useful techniques soon find their champions in the clinic. It is not that we are misunderstood, but rather that our limitations are understood only too well. We have never surmounted certain crucial methodological problems, have failed to demonstrate that ERPs can surpass other kinds of behavioral testing, and have never stimulated any therapeutic innovations. The rectification of these failures and the vindication of the utility of ERPs in clinical psychology and psychiatry is a huge task, in comparison to which, this report must inevitably be modest. We do address issues of central importance. The first "The preparation of this work was supported by the Medical Research Service of the Veterans Administrationand NIMH Special Research Center Grant MH 30854. 496

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PART IV. PSYCHOPATHOLOGY A N D INDIVIDUAL DIFFERENCES
ERPs and Psychopathology I. Behavioral Process Issuesa
WALTON T. ROTH,b JOSEPH J. TECCE,' ADOLF PFEFFERBAUMP MARGARET ROSENBLOOMP
A N D ENOCH CALLAWAYd 'Psychiatry Service
Veterans Administration Medical Center Palo Alto, California 94304
and Department of Psychiatry and Behavioral Sciences
Stanford University Medical Center Stanford, California 94305 'Department of Psychology
Boston College Chestnut Hill, Massachusetts 021 67
and Department of Neurology
Tufts Medical School Boston, Massachusetts 021 I I
dLangley Porter Psychiatric Institute University of California
San Francisco Medical Center San Francisco, California 941 43
Although ERPs have proven clinically useful in assessing the structural integrity of sensory pathways from the periphery to the cortex, they have failed to play a significant role in the psychiatric clinic, where questions must be answered about the efficiency of more complex forms of mental functioning than those that take place in the sensory system. Even at psychiatric research meetings, ERPs only grace a few posters in the wings, while center stage is occupied by biochemical studies of neurotransmitters or anatomic studies based on the C T scan, or most recently, positron-emission tomography. This is true even though the disorders being investi- gated are first and foremost manifested behaviorally, and the ERPs provide a window on the behaving brain.
One can take no solace in believing that clinicians neglect ERPs because they have not heard of them or do not understand them. Useful techniques soon find their champions in the clinic. It is not that we are misunderstood, but rather that our limitations are understood only too well. We have never surmounted certain crucial methodological problems, have failed to demonstrate that ERPs can surpass other kinds of behavioral testing, and have never stimulated any therapeutic innovations.
The rectification of these failures and the vindication of the utility of ERPs in clinical psychology and psychiatry is a huge task, in comparison to which, this report must inevitably be modest. We do address issues of central importance. The first
"The preparation of this work was supported by the Medical Research Service of the Veterans Administration and NIMH Special Research Center Grant MH 30854.
496

ROTH er al.: ERPs & PSYCHOPATHOLOGY: BEHAVIORAL PROCESS ISSUES 497
concerns general methodological problems of individual difference research. The second concerns the effect of aging, both as a methodological issue, and as a characteristic of a target clinical population. The effect of aging on ERPs must be understood before ERPs can be used to assess clinical populations that are not homogeneous for age. Furthermore, aging brings with it mental changes that we should be able to detect and characterize with our methods. We later raise more general theoretical and methodological issues.
Divided Attention, ERPs, and Aging: Methodology and Theory’
Difficulties necessarily arise from not being able to assign subjects randomly to experimental groups of patient and control. Theoretical formulations such as the distraction-arousal hypothesis or automatic versus controlled processing can guide application of ERPs to study divided attention in the elderly.
Joseph J. Tecce
Unresolved theoretical and methodological issues that beset clinical studies of event-related potentials (ERPs) can be exemplified in ERP research on aging. The purpose of this paper is to delineate some of these problems and to discuss possible solutions.
Problems
The main goals of science are to describe, explain, predict, and control phenomena. The method of choice in achieving these goals is that of the pure experiment, whereby the random assignment of subjects to two or more experimental groups achieves, in principle, comparability in the groups on all variables but those selected by the experimenter to be manipulated, that is, the independent variables. Through this type of control of extraneous sources of variation, lawful relationships are achieved between the manipulated stimulus (S) variables and resulting responses (R). The establishment of such S-R laws as stable and generalized relationships between variables operation- ally defined and quantitatively expressed is one way by which science proceeds to facilitate the prediction and control of phenomena. As one area of study within brain science, ERP research has achieved a measure of success in following this strategy. A major problem with clinical ERP research is the inability to equate groups of subjects by randomization. Instead, patient populations are determined by processes unamena- ble to experimental control, that is, the groups are self-selected.
The specific problem of self-selection in clinical ERP research insures the likelihood of confounding effects from variables other than the ones constituting the main differentiating characteristics of the groups. For example, in cross-sectional studies of aging where young and old groups are compared on ERPs such as CNV or P300, group differences on the ERP measures could be due to a number of factors other than age per se, namely, intelligence, education, medications, depression, sleep loss, and the like. (In view of the common occurrence of sleep problems among the aged,
eThis work was supported by USPHS Research Grant MH-34720 from the National Institute of Mental Health and a research grant from the Boston Mental Health Foundation. The author is grateful to Lynn Cattanach and Christopher J. Tecce for research assistance.
498 ANNALS NEW YORK ACADEMY OF SCIENCES
insomnia may be a particularly significant age-related confounding variable in clinical studies of those ERPs-such as CNV and P3oo-that are sensitive to modification by changes in attention, alertness, and distraction.) Hence, in this type of ex post fucto design (Greenwood, 1945), potential effects of confounding variables act to preclude clear-cut cause and effect statements about ERPs and aging. Thus, by their very nature ex post fucto studies of ERPs contribute only weakly to the construction of lawful age-ERP relationships. The major defect inherent in ex post fucto studies of ERPs in clinical populations is the lack of randomized assignment of subjects to experimental groups. This problem interferes with the establishment of S-R laws in a nomothetic sense and impedes as well the idiographic use of ERPs in predicting an individual patient’s behavior, such as treatment outcome in drug therapy.
In the sense that characteristics which define clinical populations can be considered responses to naturally occurring processes, reliable associations between ERPs and clinical characteristics (e.g., normal versus schizophrenic, younger versus older) contribute to the development of response-response (R-R) laws (Spence, 1944). In contrast to S-R associations, R-R laws are essentially correlational in nature; consequently, they are not likely, in and of themselves, to contribute significantly to the development of the type of cause-and-effect statements favored in science.
The problem of ex post fucto designs can be alleviated, but not entirely overcome, by a number of methodological and theoretical strategies that are discussed in the next two sections.
Methodology
The use of repeated measures designs in both cross-sectional and longitudinal studies is one way to provide within age-group comparisons in order to attenuate the impact of between-group confounding variables. For example, by measuring CNV at several points in time, information can be obtained on the aging process which does not entail a direct young-old cross-sectional comparison with its attendant age-related confounding variables. In addition, the intraindividual assessment of ERP-behavior associations (and dissociations) also offers an opportunity to study clinical populations and brain functioning with the impact of confounding variables reduced.
A case in point is the recent demonstration of dissociations between CNV and electromyographic (EMG) activity. The use of a divided-attention paradigm, which utilizes a short-term memory task, led to the unanticipated appearance of a supranor- ma1 elevation in CNV amplitude (rebound) when the memory task was unpredictably omitted (Tecce, 1979). More recently, this paradigm facilitated the demonstration of an experimentally produced double dissociation of CNV and EMG amplitudes (Tecce et ul.. this volume). While the presence of the short-term memory task produced a decrease in CNV amplitude and an increase in EMG amplitude (first dissociation), its unpredictable omission produced an opposite pattern, namely, CNV increase and EMG decrease (second dissociation). Should this double-dissociation effect be reliably demonstrated in an aged population (studies in progress suggest this to be so), the explanation of age-related disruption in ERP development solely in terms of general- ized, nonspecific variables, as suggested by Roth in this report, can be excluded from any serious consideration. That is, the enhanced EMG amplitudes during disruption in development of CNV rebound preempt any explanation of reduced rebound on the basis of age-related lowered motivation levels or physiological hyporeactivity. Further- more, the demonstration that a distraction challenge (divided attention paradigm) produces signifi’cantly larger heart rate increases in the elderly compared to the young (Tecce et al., 1980) also precludes a reductionistic interpretation that hinges solely on nonspecific processes.
ROTH et al.: ERPs 81 PSYCHOPATHOLOGY BEHAVIORAL PROCESS ISSUES 499
r - - - - - - - - I I------ --7 I I I I I I I I I I I F O C U S S E O I
D I S T R A C T I O N - - -1 I A T T E N T I O N I I F U N C T I O N S 1
I I I
I I N H I B I T O R Y I I O E - E N E R G I Z I N G I_ - -
I I I I
I --------- I I_ -------- I ; I I
Theoretical Considerations
E X C E S S I V E A R O U S A L
One of the main weaknesses in the study of ERPs and aging is the lack of definitive theoretical schemata emanating from brain science. The history of science indicates that progress toward the meaningful synthesis of diverse arrays of data is facilitated by the use of theory. Several criteria define a useful theory. One is that it should be comprehensive, that is, facilitate the explanation and understanding of the largest possible number of findings. Second, the theory should be parsimonious and contain the fewest number of explanatory constructs. Third, the theory should be empirically testable by lending itself to translation into operationally definable terms. A useful theory should also be heuristic i n that it generates new hypotheses for experimental testing.
A
k A/
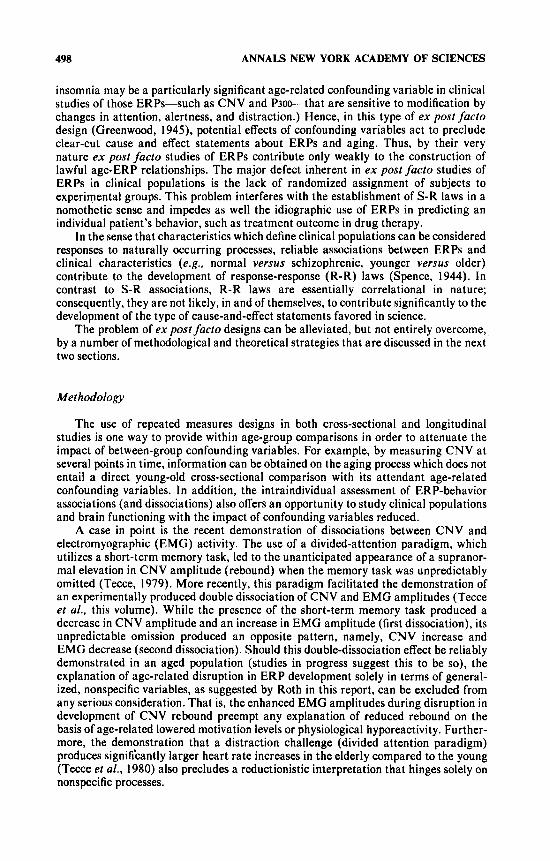
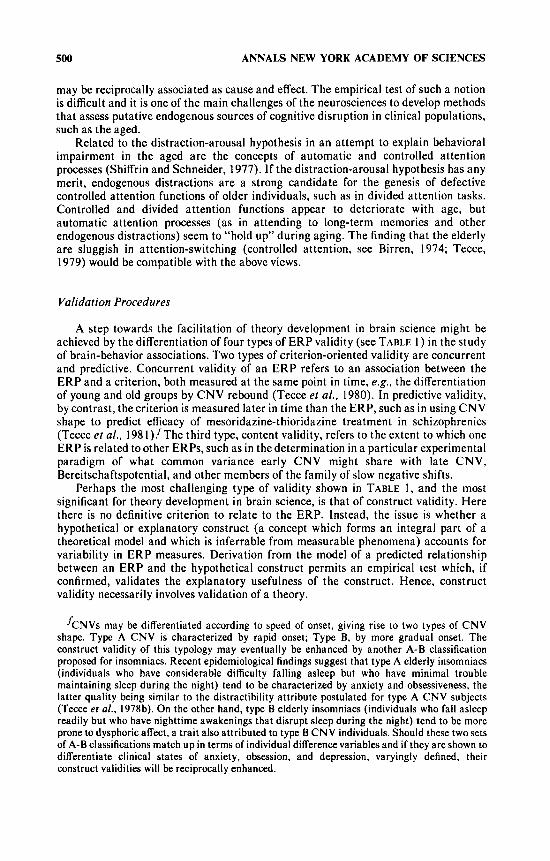
While no theories of ERPs fit these criteria perfectly, two have promise. One is the distraction-arousal hypothesis ( F I G U R E 1 ), which has been proposed to account for age-related behavioral impairment (Tecce and Cattanach, 1982). In this model, older individuals are hypothesized to be more distractible and to function at higher arousal levels than young subjects. While this view goes against what is commonly thought about the aged, i.e., that they are characteristically apathetic and excessively narrowed in attentiveness, there is sufficient empirical evidence from drug studies (Eisdorfer et al., 1970) and psychophysiological functions (Tecce and Cattanach, 1982) to indicate that the distraction-arousal hypothesis is a parsimonious explanation of age-related changes in behavior that deserves further study. One aspect of this hypothesis implies that the elderly are characterized by endogenous distractions, for example, worries and other preoccupations, and that excessively high arousal levels and distraction states
500 ANNALS NEW YORK ACADEMY OF SCIENCES
may be reciprocally associated as cause and effect. The empirical test of such a notion is difficult and it is one of the main challenges of the neurosciences to develop methods that assess putative endogenous sources of cognitive disruption in clinical populations, such as the aged.
Related to the distraction-arousal hypothesis in an attempt to explain behavioral impairment in the aged are the concepts of automatic and controlled attention processes (Shiffrin and Schneider, 1977). If the distraction-arousal hypothesis has any merit, endogenous distractions are a strong candidate for the genesis of defective controlled attention functions of older individuals, such as in divided attention tasks. Controlled and divided attention functions appear to deteriorate with age, but automatic attention processes (as in attending to long-term memories and other endogenous distractions) seem to “hold up” during aging. The finding that the elderly are sluggish in attention-switching (controlled attention, see Birren, 1974; Tecce, 1979) would be compatible with the above views.
Validation Procedures
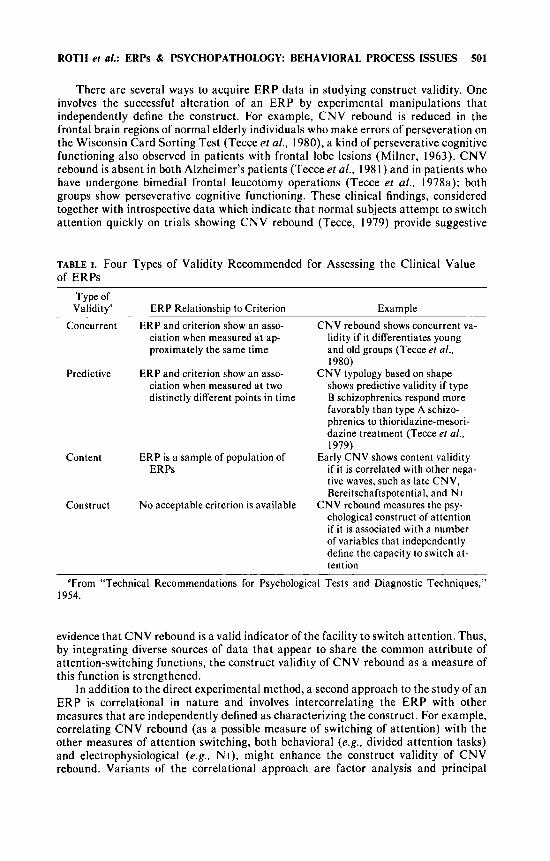
A step towards the facilitation of theory development in brain science might be achieved by the differentiation of four types of ERP validity (see TABLE 1) in the study of brain-behavior associations. Two types of criterion-oriented validity are concurrent and predictive. Concurrent validity of an ERP refers to an association between the ERP and a criterion, both measured at the same point in time, e.g. , the differentiation of young and old groups by CNV rebound (Tecce et al., 1980). In predictive validity, by contrast, the criterion is measured later in time than the ERP, such as in using CNV shape to predict efficacy of mesoridazine-thioridazine treatment in schizophrenics (Tecce et a f . , 1981)/The third type, content validity, refers to the extent to which one ERP is related to other ERPs, such as in the determination in a particular experimental paradigm of what common variance early CNV might share with late CNV, Bereitschaftspotential, and other members of the family of slow negative shifts.
Perhaps the most challenging type of validity shown in TABLE 1, and the most significant for theory development in brain science, is that of construct validity. Here there is no definitive criterion to relate to the ERP. Instead, the issue is whether a hypothetical or explanatory construct (a concept which forms an integral part of a theoretical model and which is inferrable from measurable phenomena) accounts for variability in ERP measures. Derivation from the model of a predicted relationship between an ERP and the hypothetical construct permits an empirical test which, if confirmed, validates the explanatory usefulness of the construct. Hence, construct validity necessarily involves validation of a theory.
kNVs may be differentiated according to speed of onset, giving rise to two types of CNV shape. Type A CNV is characterized by rapid onset; Type B, by more gradual onset. The construct validity of this typology may eventually be enhanced by another A-B classification proposed for insomniacs. Recent epidemiological findings suggest that type A elderly insomniacs (individuals who have considerable difficulty falling asleep but who have minimal trouble maintaining sleep during the night) tend to be characterized by anxiety and obsessiveness, the latter quality being similar to the distractibility attribute postulated for type A CNV subjects (Tecce et a/., 1978b). On the other hand, type B elderly insomniacs (individuals who fall asleep readily but who have nighttime awakenings that disrupt sleep during the night) tend to be more prone to dysphoric affect, a trait also attributed to type B CNV individuals. Should these two sets of A-B classifications match up in terms of individual difference variables and if they are shown to differentiate clinical states of anxiety, obsession, and depression, varyingly defined, their construct validities will be reciprocally enhanced.
ROTH et al.: ERPs & PSYCHOPATHOLOGY: BEHAVIORAL PROCESS ISSUES 501
There are several ways to acquire ERP data in studying construct validity. One involves the successful alteration of an ERP by experimental manipulations that independently define the construct. For example, CNV rebound is reduced in the frontal brain regions of normal elderly individuals who make errors of perseveration on the Wisconsin Card Sorting Test (Tecce et al., 1980), a kind of perseverative cognitive functioning also observed in patients with frontal lobe lesions (Milner, 1963). CNV rebound is absent in both Alzheimer’s patients (Tecceet al.. 1981) and in patients who have undergone bimedial frontal leucotomy operations (Tecce et al., 1978a); both groups show perseverative cognitive functioning. These clinical findings, considered together with introspective data which indicate that normal subjects attempt to switch attention quickly on trials showing CNV rebound (Tecce, 1979) provide suggestive
TABLE I . Four Types of Validity Recommended for Assessing the Clinical Value of ERPs
Type of Validity”
Concurrent
Predictive
Content
Construct
ERP Relationship to Criterion Example ERP and criterion show an asso-
ciation when measured at ap- proximately the same time
ERP and criterion show an asso- ciation when measured at two distinctly different points in time
ERP is a sample of population of ERPs
No acceptable criterion is available
CNV rebound shows concurrent va- lidity if it differentiates young and old groups (Tecce er a/ . , 1980)
CNV typology based on shape shows predictive validity if type B schizophrenics respond more favorably than type A schizo- phrenics to thioridazine-mesori- dazine treatment (Tecce et a/ . , 1979)
Early CNV shows content validity if it is correlated with other nega- tive waves, such as late CNV, Bereitschaftspotential, and NI
CNV rebound measures the psy- chological construct of attention if it is associated with a number of variables that independently define the capacity to switch at- tention
”From “Technical Recommendations for Psychological Tests and Diagnostic Techniques,” 1954.
evidence that CNV rebound is a valid indicator of the facility to switch attention. Thus, by integrating diverse sources of data that appear to share the common attribute of attention-switching functions, the construct validity of CNV rebound as a measure of this function is strengthened.
In addition to the direct experimental method, a second approach to the study of an ERP is correlational in nature and involves intercorrelating the ERP with other measures that are independently defined as characterizing the construct. For example, correlating CNV rebound (as a possible measure of switching of attention) with the other measures of attention switching, both behavioral (e.g., divided attention tasks) and electrophysiological (e.g.. N I ) , might enhance the construct validity of CNV rebound. Variants of the correlational approach are factor analysis and principal
502 ANNALS NEW YORK ACADEMY OF SCIENCES
component analysis (PCA). PCA, which has recently become popular among ERP investigators, is a way of organizing data that permits inferences to be made about possible psychological constructs that explain patterns of variance among ERP measures. In using correlational approaches (e.g.. factor analysis and PCA) which facilitate the development of R-R laws, the ERP investigator should exercise caution in making cause-and-effect interpretations of his data.
In summary, construct validation of ERPs involves prediction, and hopefully confirmation, of results based on an attribute (hypothetical construct) that is part of a theoretical model. Successful prediction strengthens both the ERP as a measure of the hypothetical construct and the hypothetical construct as an integral part of the model. It is highly desirable, and in most cases necessary, to integrate empirical evidence from several different sources for the development of construct validity, particularly in clinical studies of ERPs in which the hypothetical processes underlying clinical measures are very complex. Finally, despite the differentiation of four types of validity, they clearly are not discretely different from each other and are not completely orthogonal, either conceptually or operationally.
Summary
The clinical study of ERPs has an inherent defect-a self-selection of clinical populations that hampers equating of clinically defined groups on factors extraneous to the independent variables. Such ex post facto studies increase the likelihood of confounding variables in the interpretation of findings. Hence, the development of lawful relationships between clinical variables and ERPs is impeded and the fulfill- ment of description, explanation, prediction, and control in brain science is thwarted. Proper methodologies and theory development can increase the likelihood of estab- lishing these lawful relationships. One methodology of potential value in the clinical application of ERPs, particularly in studies of aging, is that of divided attention. Two promising theoretical developments in the understanding of brain functioning and aging are the distraction-arousal hypothesis and the controlled-automatic attention model. The evaluation of ERPs in the study of brain-behavior relations in clinical populations might be facilitated by the differentiation of concurrent, predictive, content, and construct validities.
Aging and the ERP
The effects of age on sensory and cognitive components of the ERP need to be documented both to establish age-norms, and to understand better the process of aging. Age-dependent changes in the peripheral sensory apparatus can be confused with changes in the central nervous system and must be controlled for when studying sensory EPs. Age-related changes in the more cognitive P300 and RT, when currently measured, reveal differences between young and old that are still poorly understood.
Adolf Pfefferbaum and Margaret Rosenbloom
Event-related potential (ERP) procedures provide a technique for investigating both sensory and cognitive processing of stimuli. The origins of several sensory evoked potential (EP) components have been inferred and these components are being used as indicators of neuroanatomical abnormality in neurology, audiology and ophthalmology
ROTH et al.: ERPs & PSYCHOPATHOLOGY: BEHAVIORAL PROCESS ISSUES 503
(Shearer and Dustman, 1980; J. E. Stockard e f al., 1979; J. J. Stockard et al., 1979). ERP components are also proving useful in the evaluation of cognitive dysfunction (Goodin et al., 1978b; Pfefferbaum et al.. 1979b.). Age-related changes in various EP and ERP components provide information about the effects of aging on sensory and cognitive processing. Clinical application also requires age normative data against which pathological deviations can be evaluated. While ERP and EP components can be characterized by both amplitude and latency, only latency, which is especially relevant to the slowing of physiologic processes that is so characteristic of old age, will be discussed in this paper.
Age Effects on Sensory EPs
An important consideration in any comparison of sensory EPs of young and old is the influence of peripheral auditory and visual decrements associated with age (Fozard et al . . 1977; Robinson and Sutton, 1979). If these measures are to provide useful information about central processes rather than those occurring at the receptor organ, then age-related changes in such things as acuity, threshold sensitivity, glare sensitivi- ty, and auditory recruitment should be addressed. One technique to control for differences in threshold is to adjust stimulus intensity to each individual’s threshold. Another technique, advocated by Allison et al., (1979) involves measuring latencies relative to a “benchmark” receptor organ component, e.g. , Wave I of the brainstem response (BSR) or the A wave of the electroretinogram (ERG). Both techniques pose problems and neither one is universally used. Many studies report some screening process to exclude subjects with gross auditory or visual deficit, but the relationship between EP variables and peripheral variables in the remaining subject pool is seldom explicitly reported. Thus, the contribution of age-related peripheral decrements to the latency of sensory EP components remains problematic, and doubtless contributes to discrepancies between data reported by different laboratories.
In the visual modality, the latencies of several components elicited by flash stimuli increase with age (Drechsler, 1978; Dustman and Beck, 1969; Kooi and Bagchi, 1964; Schenkenberg, 1970; Straumanis et al., 1965). In general, these studies do not mention controlling for differences in visual thresholds or acuity beyond reporting that subjects with visual defects were excluded. It is difficult to distinguish the relative contributions of peripheral and central factors to the latency effects observed.
More recently, pattern reversal stimuli, which are more efficient than flash stimuli at eliciting reliable, high amplitude sensory EPs with a marked PIOO (Cobb et al., 1967), have become the preferred mode for studying visual processing. Delay in the Pi00 component provides a reliable clinical indicator of optic nerve lesions associated with multiple sclerosis (MS) (Halliday et al.. 1972; J. J. Stockard et al., 1979). However, data on latency increases with age for the pattern reversal PIOO are not consistent. With pattern stimuli, visual acuity is also an important variable affecting the amplitude and latency of EP components (Harter and White, 1970). Most studies of pattern reversal EPs report that visual acuity was tested and corrected with eye glasses as necessary.
Typically, pattern reversal studies employ absolute intensities rather than intensi- ties relative to subjective thresholds. Variations in stimulus intensity and numerous other stimulus parameters make comparison between studies difficult. In young adults, latency increases of 10-12 ms for PIOO are reported for each log drop in luminance (Pastrnakova and Peregrin, 1977; Shearer and Dustman, 1980). Since receptor changes such as decline in pupillary size and increased opacity of the lens reduce the effective lumination reaching the elderly retina by up to 70% (Weale, 1961, 1965), it is
504 ANNALS NEW YORK ACADEMY OF SCIENCES
not surprising to find increased Pi00 latencies in the elderly. Most pattern stimuli normative data are from young and middle-aged adults, the age range most a t risk for MS, and relatively little is available on subjects over 60. However, the importance of age norms for the pattern reversal Pi00 component is being recognized (Shearer and Dustman, 1980, J. J. Stockard et al., 1979).
In general, fewer age effects on Pi00 latency are obtained with bright stimuli than with dim stimuli (Allison et al.. 1979; Asselman et al., 1975; Celesia and Daly, 1977; Hennerici et al., 1977; Matthews et al., 1977; Nilsson, 1978; Shaw and Cant, 1980; Shearer and Dustman, 1980; J. J. Stockard et al., 1979). Shaw and Cant (1980) explicitly studied the contribution of stimulus luminance to age effects on Pi00 latency; no age effects were seen for brighter stimuli. With the lower luminance stimuli, Pi00 latency remained stable until the 50s and only increased with age in subjects over 60. J. J. Stockard et al. (1979) also found that only over the age of 60 did mean latency increase, as did latency variability. This is a relevant factor when normative values must be established for diagnostic purposes.
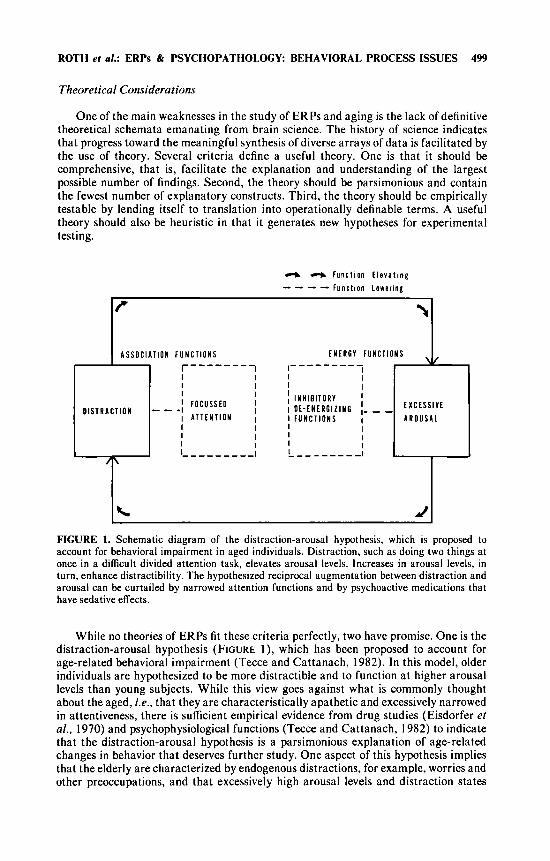
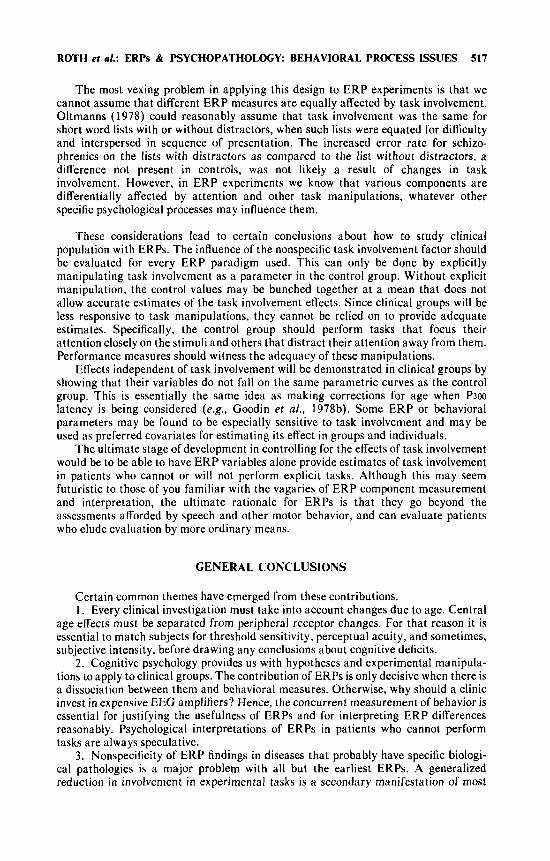
In contrast, Shearer and Dustman (1980) found a small but significant age-related increase in Pi00 over a 22 to 60 year span, with much larger changes between ages 60 and 90 years. They conclude that declining receptor sensitivities cannot account for all the latency increase seen in the population over 60. Other neuroanatomical changes such as neuronal loss and lipofuscin accumulation are probably also relevant (Ordy and Brizzee, 1979). However, the relative contribution of peripheral and central factors to this delay remains unclear. Dustman et al. (1981) recently have adopted a procedure for establishing sensory visual thresholds in ERP testing. Such a procedure should minimize the contribution of peripheral loss, which may be especially important in the subjects over age 60. Indeed, mean threshold intensity for subjects over 60 years of age was significantly higher than for subjects under 60. Patterned flashes were delivered at three intensities (1, 2, and 3 log,,, steps) over individually adjusted thresholds. A subsequent report on this study dealt with latency effects (Dustman and Snyder, 1981). However, reported analyses covered the entire age range (4-90 years); major age effects were due to the inclusion of children, and the effects of age among adults only was not considered. Visual examination of FIGURE 2 indicates a tendency towards limited latency increases by decade over age 50.
While sensory thresholds are not commonly used in visual ERP testing, they are used for establishing stimulus intensity in some auditory ERP studies. Reports of the auditory sensory components must first be sorted according to whether or not audiometric testing was done, and if so, whether or not stimuli were delivered at intensities relative to each individual subject’s sensation level (SL), some standardized hearing level (HL), or absolute sound pressure level (SPL). The ideal method is the use of stimuli individually adjusted to each subject’s threshold. This procedure should also ideally employ a signal detection paradigm for determination of threshold to minimize the effect of greater cautiousness in the elderly in making psychophysical judgements (Reese and Botwinick, 1971).
Age-related changes in auditory sensory components can be investigated as early as the brainstem level. Inferential data about the origins of BSR components enable some speculation about age-related C N S changes. Brainstem responses, increasingly used for clinical diagnosis of brainstem lesions, also call for the development of standardized age norms. However, the availability of comparable data over a range of ages remains limited.
Stimulus and recording parameters (e.g.. phase of click, intensity, rate of stimula- tion, recording location) are significant determinants of auditory BSR morphology and latency. These features are quite variable from study to study and consequently, data on the BSR in the elderly tends to inconsistency. J. E. Stockard et al. ( 1 979) have
ROTH et al.: ERPs & PSYCHOPATHOLOGY BEHAVIORAL PROCESS ISSUES 505
demonstrated that Wave I is more affected by stimulus intensity than are subsequent waves. Thus interpeak latency (IPL) depends on intensity. This fact reinforces the value of using individual S L intensities, particularly in studies examining IPL or central conduction time.
Two recent studies provide age data for BSRs elicited by SL adjusted stimuli (Patterson et al., 1981; J. E. Stockard et al., 1979). While Patterson reports only absolute peak latencies, Stockard et al. report only IPL values. Patterson et al. found that wave Ill was slowed with age across a range of intensities and repetition rates, while age effects a t waves I, I1 and IV were restricted to lower intensities and were more evident in elderly men than in elderly women. J. E. Stockard et al., (1979) found
VISUAL
N = 15
N 17 A N = 14
400 800 mmc
AUDITORY
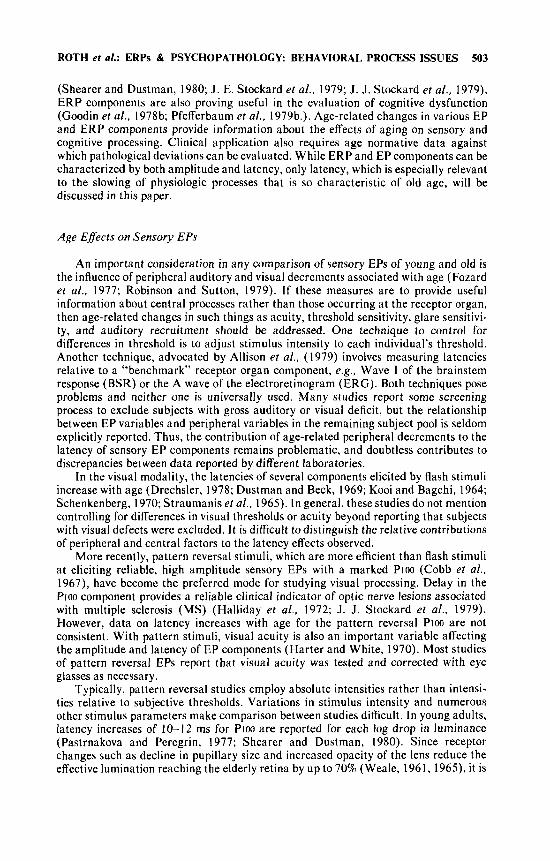
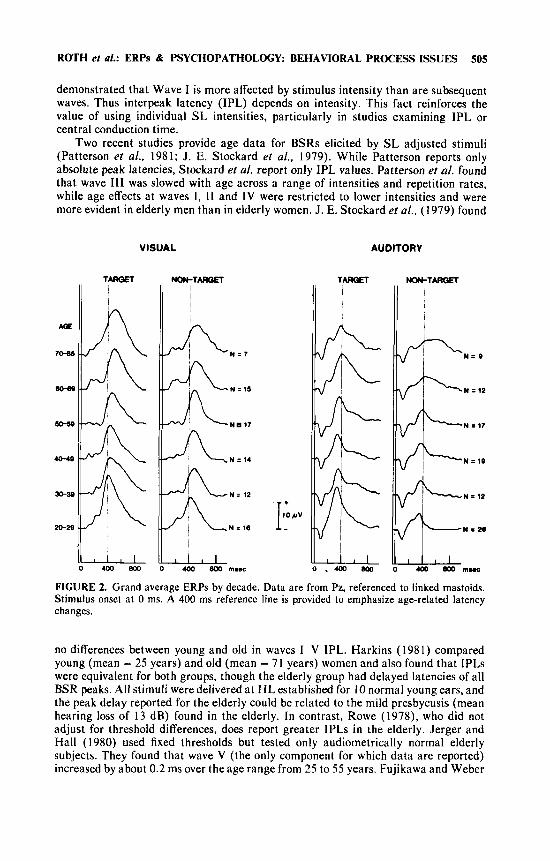
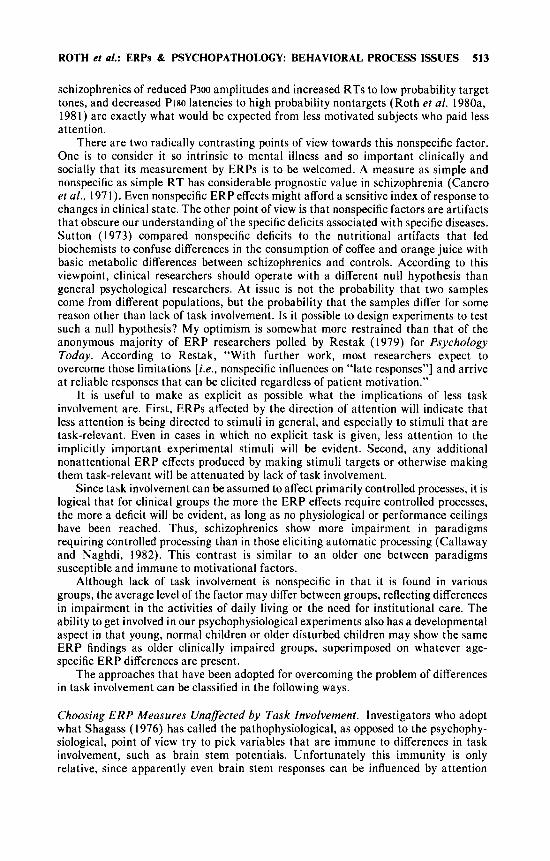
FIGURE 2. Grand average ERPs by decade. Data are from Pz, referenced to linked mastoids. Stimulus onset at 0 ms. A 400 ms reference line is provided to emphasize age-related latency changes.
no differences between young and old in waves I-V IPL. Harkins (1981) compared young (mean = 25 years) and old (mean = 71 years) women and also found that IPLs were equivalent for both groups, though the elderly group had delayed latencies of all BSR peaks. A11 stimuli were delivered at H L established for 10 normal young ears, and the peak delay reported for the elderly could be related to the mild presbycusis (mean hearing loss of 13 dB) found in the elderly. In contrast, Rowe (1978). who did not adjust for threshold differences, does report greater IPLs in the elderly. Jerger and Hall (1980) used fixed thresholds but tested only audiometrically normal elderly subjects. They found that wave V (the only component for which data are reported) increased by about 0.2 ms over the age range from 25 to 55 years. Fujikawa and Weber
506 ANNALS NEW YORK ACADEMY OF SCIENCES
(1977) demonstrated that as click rate is increased, elderly subjects show a greater latency increase in wave V than young adults. Perhaps this reflects an increasing refractoriness in the aging nervous system.
For the midlatency auditory PI and N I components, there is little evidence for age-related latency increases. Schenkenberg (1970) found none, even though he used SPL intensities. In our laboratory, work done with elderly subjects has primarily employed the auditory modality. Stimuli are delivered at intensities relative to each subject’s individual sensation level. Subjects with more than 30 dB hearing loss are excluded. Under these conditions, the P I and N I components of the auditory ERPs are not delayed with age (Pfefferbaum et al., 1979a, 1980a). Goodin et al., (1978) reported a similar finding in a comparable subject population and experimental situation. Spink et al., (1979) examined the effects of different stimulus intensities on a small sample of elderly (mean age 63) and young (mean age 22) adults. Only subjects with hearing loss less than 10 dB at 1000 Hz were included, and stimuli were presented at intensities relative to SL. Young and old subjects had essentially identical intensity functions for the latencies of PI and N I . P2 latency was shorter in old subjects than in young subjects at the 60,75 and 90 dB levels. Spink et al. hypothesize that this is due to a loss of efferent fibers in older people resulting in a reduction in inhibition at the higher intensities. Most available data, however, indicate that the auditory P2 component increases in latency with age (Goodin et al., 1978a; Pfefferbaum et al.. 1979a, 1980b; Syndulko et al., 1982). These inconsistencies remain to be resolved.
In summary, if peripheral differences are minimized, age-related differences in early and midlatency EP component latencies are small. This is particularly clear for brainstem and N I responses to auditory stimulation. With visual stimulation, the relative contributions of peripheral and central factors to PIOO latency increase with age are not yet clearly delineated. Thus it appears that the timing of sensory EPs may not provide very specific information about central neurophysiological changes asso- ciated with aging. In contrast to the early sensory EPs, the later cognitive components, especially the P300, show marked age-related latency changes.
Age Effects on the P300 Component
The latencies of sensory EP components are relevant to the study of the P300. They provide information about the sensory processing of stimuli which, because of task-induced significance, also elicit a P300 a few hundred ms later. The absence or marked delay of P300 to stimuli which elicit a normal sensory EP would indicate a different kind of deficit than absence or marked delay of P300 associated with abnormal sensory responses. While it may be assumed that receptor level or sensory processing delay would be reflected in P300 latency, there is no data available on early sensory EPs and P300 elicited by the same stimuli. This is probably because paradigms which are optimal for eliciting earlier sensory components tend not to elicit P300, and vice versa. Similarities or differences between age-related changes in early and late ERP components must be inferred from studies employing quite different testing proce- dures. In any event, paradigms used to elicit P300 in the elderly should also use stimuli with intensities adjusted to individual thresholds.
The latency of the P300 is thought to be a useful indicator of the timing of processes involved in stimulus evaluation. For example, cognitive manipulations designed to make stimulus processing more difficult increase P ~ O O latency (McCarthy and Donchin, 1981), and these task-specific changes in P300 latency are relevant to clarifying issues in information processing theory (Duncan-Johnson, 198 I ) . In addi- tion to these task-specific P300 latency changes-typically investigated in healthy
ROTH ef a/.: ERPs & PSYCHOPATHOLOGY BEHAVIORAL PROCESS ISSUES 507
young subjects-a more chronic increase in P300 latency with advancing age has been observed (Beck et al . , 1980; Ford et al.. 1979a,b, 1982a,b; Goodin et al., 1978a; Pfefferbaum et al., 1980b; Syndulko et al., 1982). This is true for P300 elicited by both auditory and visual stimuli.
FIGURE 2 illustrates grand average ERPs for each decade elicited by homologous auditory and visual paradigms. The auditory P~oo-RT paradigm consisted of a series of tone bursts, delivered a t 70 dB sensation level (SL) at one-second intervals. The series included tones at 1000 Hz, 500 Hz and 2000 Hz in a random (Bernoulli) sequence. The 1000 Hz tone occurred 72% of the time (frequent) and the 500 Hz and 2000 Hz tones each occurred 14% of the time (infrequent). Subjects were instructed to press a reaction time (RT) key when one of the two types of infrequent tones occurred. Speed and accuracy were equally emphasized in the instructions. The visual P3oo-RT paradigm paralleled the auditory paradigm. Three different shapes or symbols were presented in a random series: (i) a plus sign, the frequent stimulus, presented 72% of the time, (ii) a triangle with the apex up (14% probability), and (iii) a triangle with the apex down (14% probability). As in the auditory paradigm, one of the triangles (infrequent stimuli) was designated as the target stimulus. The other triangle represents the nontarget infrequent stimulus.
The infrequent events for both the auditory and visual paradigms produce large P300S. They are later and larger for visual than for auditory stimuli, and larger for target than for nontarget infrequent events. The reference line drawn at 400 ms poststimulation highlights the latency increase seen with advancing age.
Goodin et al. (1978a), using an auditory oddball paradigm in which subjects counted the target, obtained correlations between age and P300 latency of r = 0.83, and a linear slope of I .8 ms a year. These results are based on 40 subjects aged 15-76. Syndulko et al. (1982) tested 45 subjects aged 18-85 in a similar paradigm and obtained a correlation of 0.68 and a linear slope of 1.07 ms/year. Beck et al. (1980) used a visual stimulus sequence in which 80% were background, 10% were targets (“X” and “0” balanced across subjects) and 10% were colorful “blobs.” They studied 50 men aged 21-86 and reported that the latency of P300 elicited by the novel stimuli increased reliably with age, and that advancing age was associated with an accelera- tion of P300 slowing.
The nature and origins of the P300 are still poorly understood, and thus the extent to which chronic P300 slowing is a manifestation of a generalized “CNS slowing” resulting from a number of neurophysiological changes occurring with age is unkown (see Ordy and Brizzee, 1979). The extent to which it is an indicator of slowing of those specific cognitive operations which this component is believed to reflect in the young, is also not known. Recent studies of P300 in groups of healthy elderly and young adults indicate that this component is less closely related to the timing of behavioral response, i .e. RT, in the elderly than in the young (Ford et al.. 1982a,b; Pfefferbaum et al., 1980a,b.)
An age-related change in the temporal relationship of P300 latency and R T had been observed in both choice-RT tasks and memory-scanning tasks. In two experi- ments employing choice-RT tasks (Pfefferbaum et al.. 1980b; Ford et al., 1982a), P300 followed RT in the elderly while it preceded RT in the young. Mean RT, however, was similar in both groups. A potential problem in comparing RTs between young and old subjects is that greater variability in the elderly might render a real group difference less detectable. However, in neither of these studies was there a statistically significant difference in RT variability between young and old.
In a memory scanning task, P300 latency was less related to differences in memory load i n elderly than in young subjects (Ford et al., 1979b. 1982b; Pfefferbaum et al., 1980a). In this task, P300 latency and R T both increased linearly with increasing
508 ANNALS NEW YORK ACADEMY OF SCIENCES
memory load from one, two, three and four items in the young (Ford et al., 1979b). In the elderly, P300 latency increased when memory load increased from one to two. However, there was no further increase in P300 latency with memory loads of three and four items in spite of an increase in RT.
Elderly and young subjects showed equivalent P300 latency shifts following different stimulus sequences, even though latency “trees” of the elderly were displaced (later) approximately 50 ms (Ford et al., 1982a). The apprehension of stimulus sequence may be considered a rather “automatic” task, involving capacities which are preserved in the elderly even with overall slowing of response. Perceptual manipula- tions (physically degrading the stimulus) delayed P300 in the elderly, as in the young, and this delay was additional to the greater absolute latency of P300 in the elderly (Ford et al., 1982b).
In conclusion, the factors underlying the differential responsiveness of P300 latency to memory load, stimulus sequence, and perceptual degradation in the elderly require further investigation. P300 latency in the elderly may not have the same relation to mental chronometry, particularly in tasks involving cognitive effort, that it appears to have in young subjects. The functional significance of the age-related prolongation of P300 and reduced responsiveness to memory load remains to be determined. This determination is crucial to understanding the meaning of the reports of P300 latency prolongation in dementing diseases (Goodin et al., 1978b; Pfefferbaum et al., 1982; Syndulko et al.. 1982).
Clinical Applications of ERPs
Callaway has seen claims of ERP differences in clinical populations come and go. When replicable, these differences have seemed to reflect secondary rather than primary features of psychiatric disease. Information processing approaches give reason for some optimism that more specific psychological deficits can be uncovered in these disorders. Pharmacological manipulations might also be helpful.
Enoch Callaway
I will assert and try to defend the thesis that we have little or no reason to expect that late event-related potential (ERP) activity will have much immediate clinical utility. That is the bad news. The good news is that I believe we can now use these late potentials to develop and test hypotheses about psychiatric conditions. I think that is particularly good news because without strong hypothesis-testing designs, it is going to be increasingly hard to get funds for research.
Far-field evoked potentials (EP) provide something of an instructive contrast. Their development has been tied to hypotheses about structure and function. Effective clinical application has followed. This is not to say that the relationships between far-field EPs and underlying structures are as simple as we once thought, but at least the development and exploitation of far-field EPs has been motivated by such considerations.
Attempts to relate later waves to psychiatric conditions have had a quality that can best be described as “show and tell.” Investigator A measures a particular component derived from a particular paradigm. He then finds a correlation between this component and a particular diagnosis defined by a group with a particular bias. Meanwhile, investigator B joyfully reports an impressive F ratio for some interaction like age x sex x stimulus intensity x lead x diagnosis using another selected ERP
ROTH et al.: ERPs & PSYCHOPATHOLOGY: BEHAVIORAL PROCESS ISSUES 509
component, and different diagnostic criteria. When the results of these “show and tells” are pursued, some turn out to be unreplicable. Those few that can be replicated tend to have no relationship to any important theoretical or practical issues.
One reason why this tends to be the case is that a wide variety of central nervous system states can account for a single ERP change. Thus, we are on weak ground when we try to reason from an ERP change back to some central nervous system state. Once you have decided that pathology does not primarily involve sensory pathways, inferences from ERPs to structure and function are, by their very nature, likely to be too unreliable for clinical use.
Not only are our measurement techniques much more subtle and complex than once we thought, but so are the things we wanted to measure. Schizophrenia per se is no longer a respectable disease to study. It seems that to ask “Does ERP variability discriminate between schizophrenia and affective disorder?” is much like asking, “Does a thermometer discriminate between fever and viral influenza?” In addition, we must acknowledge that William James was probably quite mistaken when he stated, “Everyone knows what attention is.” It is now becoming increasingly clear that attention, like love, is a many splendored thing.
It was not always thus. Once upon a time schizophrenia was a respectable nosological entity, and its chief symptom was a disorder of a unitary cognitive function called “attention.” Attention was an intuitively obvious thing, but a bit hard to study. For example, introspectively it is impossible to tell much about what you are not paying attention to. Attempts to get a t that in the laboratory encountered a similar paradox. Behavioral probes of that which is excluded from attention are likely to attract attention and destroy the very phenomenon under investigation. Then ERPs came on the scene. Some, like Shagass, saw them as measures of brain activity, and adopted the so-called pathophysiological approach. In retrospect, this approach seems more defensible, if not more profitable. Others of us took the psychophysiological route. The ERP was to be a window on the mind and the ultimate tool for studying attention.
We did indeed find some strong correlations between diagnosis and ERPs. However, one of Donchin’s earliest applications of discriminant analysis (Donchin et af., 1970) showed us that one of our principal measures was simply reflecting late ERP variability in psychotics. That finding seems to be reliable. It has been replicated many times. Schizophrenics, psychotic depressives and senile psychotics all have increased variability of their late ERP components. Martineau et al. (this volume) report on increased variability in infantile autism. However, this all may be little more than an elegant way of looking at a general behavioral phenomenon. For example, if schizo- phrenics are motivated and trained so that they perform like normals (and such training is, in fact, often possible), the schizophrenics’ ERPs tend to show normal variability. We thus have begun to suspect that ERPvariability may be, like the Wrist Actograph, a clever way of measuring something that might actually be measured better and more directly by clinical observation. In any case, the ERP has certainly not proved to be a window on the mind. In the study of psychiatric conditions, it now appears more like a peep hole into a house of mirrors.
In our laboratory we find ourselves a t the tail end of an era, mopping up details. Some years ago Roy Halliday and I found some correlations between ERP measures and clinical responses of hyperactive children to methylphenidate (Halliday et al., 1976). While this seems to hold up statistically, it appears to be clinically trivial. On the other hand, we have some findings that I think will allow us to keep our ERP operation alive. Taking an information processing approach, there seem to be a number of concepts which have not been adequately explored in studies of psychopathology. In these approaches, ERPs might provide useful convergent data. One of our thoughts concerned the distinction made by Posner ( 1 978) between automatic, parallel process-
510 ANNALS NEW YORK ACADEMY OF SCIENCES
ing and voluntary, limited channel capacity processing. Another one is the sensory- evaluation/stimulus-selection distinction made by the Donchin group (Donchin, 1979). We hoped to find an N I - P ~ indication for the first and to use P3 to index the second.
We can dispense with our work on N I and P2 very briefly. These components are marvelously sensitive to many psychological factors. How much of this is due to slow negative waves and how much of it is due to actual changes in these components (or in subcomponents that add to make up these components), we have no way of telling at present. TABLE 2 illustrates the way in which various factors can move latency and amplitude independently. N I latency can be lengthened by lowering stimulus intensity or by embedding the stimulus in runs that make more demands in the subject (Roth et al.. 1976). N I amplitude may be reduced by preceding the stimulus with a similar stimulus or increased if a nontarget stimulus is similar to a demanding target stimulus. Yingling and Nethercut (1983) report on an interesting study of ERP to tone shifts. N I - P ~ amplitude was a function of content (ratio of new tone to base tone) and context (ratio of tone change to range of changes). Thus, it is both endogenous and exogenous. For now, the bottom line is that clinical application of these potentials must wait until we have a great deal more knowledge about the factors that control them.
Although P3 may be an extremely complex phenomenon in itself, the situation with regard to its clinical application seems at least a bit more encouraging. Our own data support those already reported which indicate that P3 latency reflects stimulus
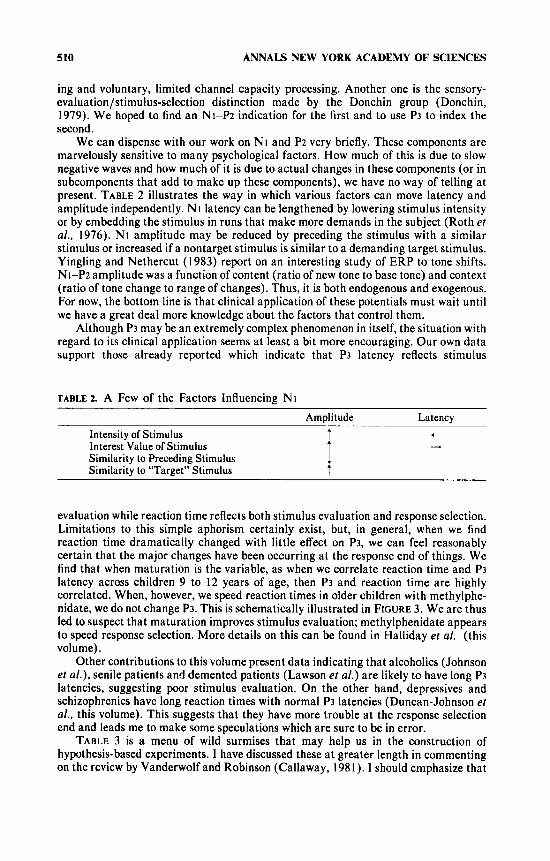
TABLE^. A Few of the Factors Influencing N I Amplitude Latency
t
--+ Intensity of Stimulus t Interest Value of Stimulus T Similarity to Preceding Stimulus 1 Similarity to “Target” Stimulus t
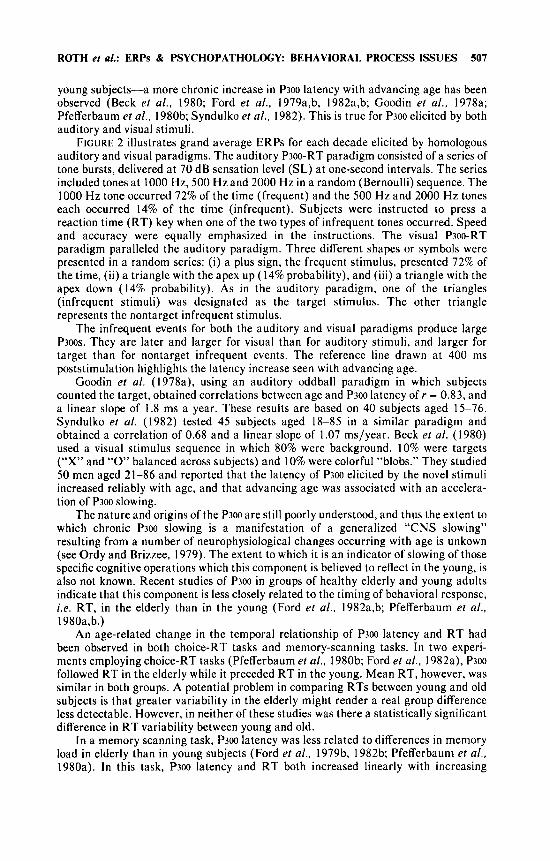
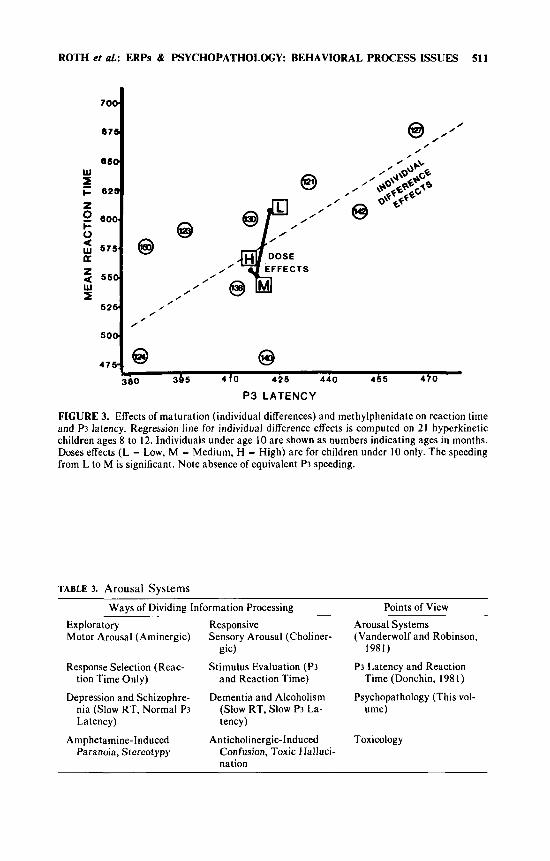
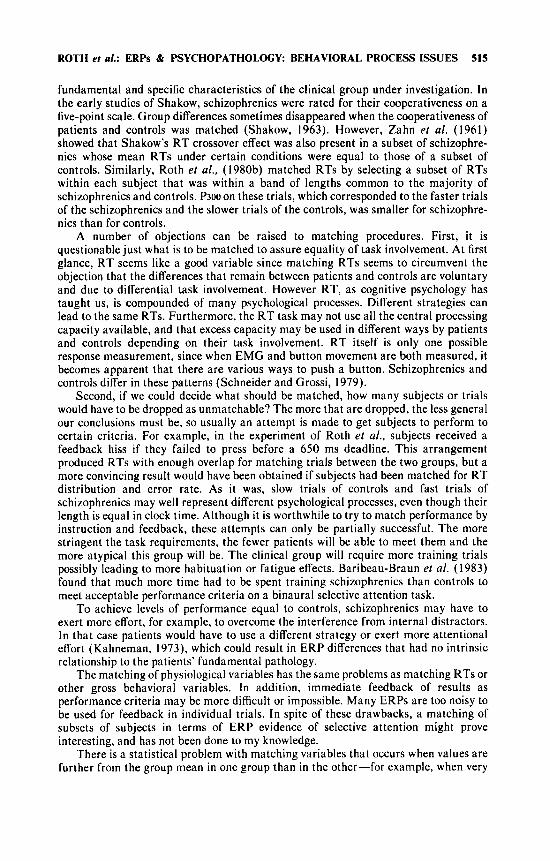
evaluation while reaction time reflects both stimulus evaluation and response selection. Limitations to this simple aphorism certainly exist, but, in general, when we find reaction time dramatically changed with little effect on P3, we can feel reasonably certain that the major changes have been occurring at the response end of things. We find that when maturation is the variable, as when we correlate reaction time and P3 latency across children 9 to 12 years of age, then P3 and reaction time are highly correlated. When, however, we speed reaction times in older children with methylphe- nidate, we do not change P3. This is schematically illustrated in FIGURE 3 . We are thus led to suspect that maturation improves stimulus evaluation; methylphenidate appears to speed response selection. More details on this can be found in Halliday et al. (this volume).
Other contributions to this volume present data indicating that alcoholics (Johnson et al .) , senile patients and demented patients (Lawson et al.) are likely to have long P3 latencies, suggesting poor stimulus evaluation. On the other hand, depressives and schizophrenics have long reaction times with normal P3 latencies (Duncan-Johnson et al., this volume). This suggests that they have more trouble a t the response selection end and leads me to make some speculations which are sure to be in error.
TABLE 3 is a menu of wild surmises that may help us in the construction of hypothesis-based experiments. I have discussed these a t greater length in commenting on the review by Vanderwolf and Robinson (Callaway, 1981). I should emphasize that
ROTH et al.: ERPs & PSYCHOPATHOLOGY: BEHAVIORAL PROCESS ISSUES 511
70e
676
6SQ w z F 625
z 0 600. k
; 575. K z a 5 5 0
525. s
5 0 0
476-
/ @ //’ , ,
@
0 , 0 ,
/
63 63 380 385 410 425 440 4 5 5 4 f 0
/
0 0
0
P3 LATENCY
FIGURE 3. Effects of maturation (individual differences) and methylphenidate on reaction time and P3 latency. Regression line for individual difference effects is computed on 21 hyperkinetic children ages 8 to 12. Individuals under age 10 are shown as numbers indicating ages in months. Doses effects ( L = Low, M = Medium, H = High) are for children under 10 only. The speeding from L to M is significant. Note absence of equivalent P3 speeding.
TABLE 3. Arousal Systems Wavs of Dividine Information Processine Points of View
Exploratory Responsive Arousal Systems Motor Arousal (Aminergic) Sensory Arousal (Choliner- (Vanderwolf and Robinson,
Response Selection (Reac- Stimulus Evaluation (P3 P3 Latency and Reaction tion Time Only) and Reaction Time) Time (Donchin, 1981)
Depression and Schizophre- Dementia and Alcoholism Psychopathology (This vol- nia (Slow RT, Normal P3 (Slow RT, Slow P3 La- Latency) tency)
Paranoia, Stereotypy Confusion, Toxic Halluci-
gic) 1981)
ume)
Amphetamine-Induced Anticholinergic-Induced Toxicology
nation
512 ANNALS NEW YORK ACADEMY OF SCIENCES
the two arousal systems are not independent. It appears that the aminergic arousal system in itself tends to turn on the cholinergic arousal system although the opposite may not be the case. This would make some intuitive sense, for when a motor exploratory arousal is in operation one would need concurrent sensory arousal. Yet a sensory (waiting) arousal might be very valuable in the absence of any motor arousal.
I have tried to relate the aminergic and cholinergic arousal systems to our findings and to the P3 findings reported here. It is also interesting that P3 latency and P3 amplitude seem to reflect different systems. While P3 latency seems to reflect early automatic aspects of stimulus evaluation, P3 amplitude seems to be a function of late, more cognitive operations. The schizophrenics with normal P3 latency have smaller P3 amplitude while aged subjects with long P3 latencies may have normal amplitudes.
In closing I will point out that we can manipulate these two systems pharmacologi- cally without great danger to our subjects. Some of these pharmacological manipula- tions have therapeutic implications. Although cholinergics and aminergics are quite different, both can improve memory. When they do so they show strong U-shaped functions. A better understanding of these arousal systems and their behavioral measurement may have more than academic interest. For example, we might use such measures to provide a more rational pharmacotherapy of cognitive disorders. However, let me again warn that TABLE 3 should be taken more as a heuristic framework than as a real theory.
Specific and Nonspecific ERP Characteristics of Clinical Groups
Nonspecific lack of task involvement may be the bate noire of clinical ERP research. All clinical groups have a tendency to show qualitatively the same findings. A number of alternatives for uncovering more specific ERP differences are available to the investigator.
Walton T. Roth
Psychologically deviant groups differ from each other and from control groups in many ways. When tested in the psychophysiology laboratory, schizophrenic, depressed, manic, mentally retarded, and demented patients are often strikingly different from normally functioning age-matched controls. For each of the clinical groups mentioned there is evidence from histopathology, genetics, or the presence of syndromes with a uniform prognosis or response to medication, that each group represents a distinct disease entity. Yet in the laboratory, some gross similarities of behavior are noticed. The most salient perhaps is that clinical groups often fail to meet the implicit and explicit task requirements of the experimenter. When recording devices are attached to normal subjects and they are sat in a quiet room where flashes or tones are presented, they quickly grasp that their reactivity to these stimuli is being measured. The stimuli assume implicit importance. Or the experimenter may assign a task that makes the stimuli explicitly important. In either case, clinical groups, through lack of motivation, failure to understand what is expected of them, preoccupa- tion with their own concerns, or restlessness, generally seem to pay less attention and perform more poorly.
The extent to which this nonspecific lack of task involvement lies behind the ERP findings reported for these clinical groups is unknown. However, many ERP differ- ences between psychotics and controls-for example, smaller ERPs after 100 ms (Shagass et af., 1978)-lend themselves to this interpretation. Our own findings in
ROTH et al.: ERPs & PSYCHOPATHOLOGY BEHAVIORAL PROCESS ISSUES 513
schizophrenics of reduced P300 amplitudes and increased RTs to low probability target tones, and decreased PI80 latencies to high probability nontargets (Roth et al. 1980a, 1981) are exactly what would be expected from less motivated subjects who paid less attention.
There are two radically contrasting points of view towards this nonspecific factor. One is to consider it so intrinsic to mental illness and so important clinically and socially that its measurement by ERPs is to be welcomed. A measure as simple and nonspecific as simple RT has considerable prognostic value in schizophrenia (Cancro et al., 1971). Even nonspecific ERP effects might afford a sensitive index of response to changes in clinical state. The other point of view is that nonspecific factors are artifacts that obscure our understanding of the specific deficits associated with specific diseases. Sutton (1973) compared nonspecific deficits to the nutritional artifacts that led biochemists to confuse differences in the consumption of coffee and orange juice with basic metabolic differences between schizophrenics and controls. According to this viewpoint, clinical researchers should operate with a different nul l hypothesis than general psychological researchers. At issue is not the probability that two samples come from different populations, but the probability that the samples differ for some reason other than lack of task involvement. Is it possible to design experiments to test such a null hypothesis? My optimism is somewhat more restrained than that of the anonymous majority of ERP researchers polled by Restak (1 979) for Psychology Today. According to Restak, “With further work, most researchers expect to overcome those limitations [i.e., nonspecific influences on “late responses”] and arrive at reliable responses that can be elicited regardless of patient motivation.”
It is useful to make as explicit as possible what the implications of less task involvement are. First, ERPs affected by the direction of attention will indicate that less attention is being directed to stimuli in general, and especially to stimuli that are task-relevant. Even in cases in which no explicit task is given, less attention to the implicitly important experimental stimuli will be evident. Second, any additional nonattentional ERP effects produced by making stimuli targets or otherwise making them task-relevant will be attenuated by lack of task involvement.
Since task involvement can be assumed to affect primarily controlled processes, it is logical that for clinical groups the more the ERP effects require controlled processes, the more a deficit will be evident, as long as no physiological or performance ceilings have been reached. Thus, schizophrenics show more impairment in paradigms requiring controlled processing than in those eliciting automatic processing (Callaway and Naghdi, 1982). This contrast is similar to an older one between paradigms susceptible and immune to motivational factors.
Although lack of task involvement is nonspecific in that it is found in various groups, the average level of the factor may differ between groups, reflecting differences in impairment in the activities of daily living or the need for institutional care. The ability to get involved i n our psychophysiological experiments also has a developmental aspect in that young, normal children or older disturbed children may show the same ERP findings as older clinically impaired groups, superimposed on whatever age- specific ERP differences are present.
The approaches that have been adopted for overcoming the problem of differences in task involvement can be classified in the following ways.
Choosing ERP Measures Unaffected by Task Involvement. Investigators who adopt what Shagass ( 1 976) has called the pathophysiological, as opposed to the psychophy- siological, point of view try to pick variables that are immune to differences in task involvement, such as brain stem potentials. Unfortunately this immunity is only relative, since apparently even brain stem responses can be influenced by attention
514 ANNALS NEW YORK ACADEMY OF SCIENCES
(Lukas, 1980). General rules, such as the earlier the peak, the less vulnerable it is to attention, are not adequate for deciding whether ERP differences in a specific experiment are due to specific or nonspecific factors. Furthermore, it is possible that for diseases characterized by behavior changes, ERPs unaffected by nonspecific psychological factors will also be insensitive to the sought-after specific psychological differences that might be reflected in specific ERP changes. On the other hand, in diseases whose neural pathology affects basic neurological functioning, psychologically insensitive measures can be clinically useful. For example, the latency of Pi00 to visual pattern reversals is more than 2.5 SDs greater than normal values in 75-97% of patients with multiple sclerosis (Halliday, 1978; Sokol, 1980). Presumably, latency differences of these magnitudes are beyond those that could be expected from attention or inattention to the pattern reversals. Similarly, if, for example, schizophrenic values on an ERP measure exceed the range of values obtained in controls by extreme maneuvers of attention and distraction, then that measure might reflect a primary characteristic of schizophrenics. However, unless otherwise demonstrated, it should be assumed that all differences in ERPs are consequences of variation in task involve- ment.
Measuring ERPs during Sleep. Ornitz and his collaborators have measured auditory N2-P2 in autistic children during stage 2 sleep to reduce the difficulties in getting the cooperation of these subjects (reviewed in Shagass et al., 1978). In another study the auditory temporal recovery of autistic children was measured during sleep (Shagass et al., 1978). No consistent differences between autistic and normal children were found. However, had such differences been found, they could not have been explained away as due to differences in task involvement. Unfortunately, this approach has one of the same drawbacks as measuring ERPs insensitive to attentional factors, namely, that specific psychophysiological differences may be missed. During sleep, autistic children may function neurophysiologically in the same way as normal children.
Finding ERP Measures That Deviate in the Direction of More Task Involve- ment. Sutton (1973) has pointed out the advantage of finding measures on which clinical groups have superior performance. He cites the example of shorter critical durations for integration of visual pulses in schizophrenics as compared to controls (see also Collins et al., 1978). Callaway and Naghdi (1982) cite psychophysiological evidence for automatic processes that are faster, more efficient, and more resistant to interference in schizophrenics. For example, schizophrenics showed more temporal auditory ERP recovery after a button press and less eye blink inhibition by a weak stimulus given before the strong stimulus eliciting the blink than did controls. However, these psychophysiological results can hardly be interpreted as the kind of superior performance that would be expected from a more involved subject. Less attention to the stimuli might have produced these effects, just as larger deep tendon reflexes can be elicited by distracting the subject.
Roth and Cannon ( 1 972) told their subjects to ignore the tones they were given, and the ERPs of the schizophrenics indicated that they paid less attention to the tones than did controls. In terms of the task instructions, schizophrenics performed superior- ly. Task involvement was paradoxically defined as task uninvolvement, in a Zen Buddhist way. Perhaps the instructions were not presented to the controls convincingly enough. It would have been interesting to know if a distracting task in another modality could have made the control ERPs look like those of schizophrenics.
Matching Task Involvement. The fundamental idea here is that if task involvement can be matched, whatever differences remain after this matching will represent more
ROTH et al.: ERPs & PSYCHOPATHOLOGY BEHAVIORAL PROCESS ISSUES 515
fundamental and specific characteristics of the clinical group under investigation. In the early studies of Shakow, schizophrenics were rated for their cooperativeness on a five-point scale. Group differences sometimes disappeared when the cooperativeness of patients and controls was matched (Shakow, 1963). However, Zahn et al. (1961) showed that Shakow’s RT crossover effect was also present in a subset of schizophre- nics whose mean RTs under certain conditions were equal to those of a subset of controls. Similarly, Roth et al.. (1980b) matched RTs by selecting a subset of RTs within each subject that was within a band of lengths common to the majority of schizophrenics and controls. P300 on these trials, which corresponded to the faster trials of the schizophrenics and the slower trials of the controls, was smaller for schizophre- nics than for controls.
A number of objections can be raised to matching procedures. First, it is questionable just what is to be matched to assure equality of task involvement. At first glance, RT seems like a good variable since matching RTs seems to circumvent the objection that the differences that remain between patients and controls are voluntary and due to differential task involvement. However RT, as cognitive psychology has taught us, is compounded of many psychological processes. Different strategies can lead to the same RTs. Furthermore, the RT task may not use all the central processing capacity available, and that excess capacity may be used in different ways by patients and controls depending on their task involvement. RT itself is only one possible response measurement, since when EMG and button movement are both measured, it becomes apparent that there are various ways to push a button. Schizophrenics and controls differ in these patterns (Schneider and Grossi, 1979).
Second, if we could decide what should be matched, how many subjects or trials would have to be dropped as unmatchable? The more that are dropped, the less general our conclusions must be, so usually an attempt is made to get subjects to perform to certain criteria. For example, in the experiment of Roth et al., subjects received a feedback hiss if they failed to press before a 650 ms deadline. This arrangement produced RTs with enough overlap for matching trials between the two groups, but a more convincing result would have been obtained if subjects had been matched for RT distribution and error rate. As it was, slow trials of controls and fast trials of schizophrenics may well represent different psychological processes, even though their length is equal in clock time. Although it is worthwhile to try to match performance by instruction and feedback, these attempts can only be partially successful. The more stringent the task requirements, the fewer patients will be able to meet them and the more atypical this group will be. The clinical group will require more training trials possibly leading to more habituation or fatigue effects. Baribeau-Braun et al. (1983) found that much more time had to be spent training schizophrenics than controls to meet acceptable performance criteria on a binaural selective attention task.
To achieve levels of performance equal to controls, schizophrenics may have to exert more effort, for example, to overcome the interference from internal distractors. In that case patients would have to use a different strategy or exert more attentional effort (Kahneman, 1973), which could result in ERP differences that had no intrinsic relationship to the patients’ fundamental pathology.
The matching of physiological variables has the same problems as matching RTs or other gross behavioral variables. In addition, immediate feedback of results as performance criteria may be more difficult or impossible. Many ERPs are too noisy to be used for feedback in individual trials. In spite of these drawbacks, a matching of subsets of subjects in terms of ERP evidence of selective attention might prove interesting, and has not been done to my knowledge.
There is a statistical problem with matching variables that occurs when values are further from the group mean in one group than in the other-for example, when very
516 ANNALS NEW YORK ACADEMY OF SCIENCES
good R T performance for schizophrenics is matched with average performance for controls. Because the correlation between underlying task involvement and any variable affected by it are subject to error, matching on extreme values of one variable is likely to result in values closer to the group mean for the second variable. In other words, there will be regression towards the mean (Neale and Oltmanns, 1980). Task involvement matched on the basis of extreme scores for schizophrenics may be less than those scores indicate. Regression towards the mean is a reason for trying to increase mean task involvement for schizophrenics rather than letting these scores simply fall where they may.
Covarying Out the Effects of Task Involvement. I f one measure such as R T is correlated with task involvement, it might be possible to adjust the scores on other measures in a way to remove the influence of task involvement. This would obviate the necessity of matching. Unfortunately the application of covariance analysis to clinical designs is full of pitfalls (Lord, 1967; Chapman and Chapman, 1973; Fleiss and Tanur, 1973; Woodward and Goldstein, 1977; Neale and Oltmanns, 1980). When the two groups to which analysis of covariance are to be applied differ on the covariate in a nonrandom way, the mathematical assumptions of the analysis are not met. The problem lies in obtaining a good estimate of the relationship between covariates and dependent measures. The estimates obtained from the two groups will differ if group effects not due to the covariate are present, and it is dangerous to accept an estimate based on the control group alone if that group does not have values that cover the range of values in the clinical group.
Finding Diflerential Deficits Inexplicable by Task Involvement. If task involvement affects two tasks equally, and if groups differ on one task but not the other, a specific deficit may be present. Chapman and Chapman (1973) have advocated this approach, which can be generalized to any number of tests, and have specified additional requirements for its validity. It is crucial that the tests have equal discriminating power, which depends on the difficulty of the tests and their reliability. Unreliable tests or tests that are too easy or too hard are poor in discriminating groups. Chapman and Chapman (1978) have given examples of how false conclusions were drawn about the ability of schizophrenics to define affect-laden words, and how these false conclusions were corrected by the use of properly constructed tests. Oltmanns and Neale (1975) and Oltmanns (1978) have used the differential deficit approach to demonstrate the specific vulnerability of schizophrenic memory performance to distraction.
It is not necessary for the scores of the tests for clinical and control groups to be equal, as with matching, but difficulty and reliability must be matched between tests. Sometimes task difficulty is matched by changing a task parameter that presumably affects only the difficulty of the task and not its nature, for example, list length or order of recall for memory tasks.
Many of the considerations that are important for demonstrating differential deficits on nonphysiological measures apply to ERPs. ERP researchers are inclined to scan the profile of their ERP results and infer differential deficits. Roth et al. (1980a) claimed that normal P300 latencies and reduced P300 amplitudes in schizophrenics signified normal stimulus evaluation speed in the face of an abnormality in one of the processes controlling P300 amplitude. However, the stimulus discrimination required in their task was so easy that a floor for P300 latency may have been reached. Furthermore, it is possible that P300 latency was measured with less reliability than amplitude and the similar latencies were the result of chance. In general, we should expect different measurements to vary in susceptibility to the noise of the background EEG. The broader and flatter a component is, the easier it is to measure its amplitude and the harder it is to measure its latency.
ROTH et al.: ERPs & PSYCHOPATHOLOGY BEHAVIORAL PROCESS ISSUES 517
The most vexing problem in applying this design to ERP experiments is that we cannot assume that different ERP measures are equally affected by task involvement. Oltmanns (1 978) could reasonably assume that task involvement was the same for short word lists with or without distractors, when such lists were equated for difficulty and interspersed in sequence of presentation. The increased error rate for schizo- phrenics on the lists with distractors as compared to the list without distractors, a difference not present in controls, was not likely a result of changes in task involvement. However, in ERP experiments we know that various components are differentially affected by attention and other task manipulations, whatever other specific psychological processes may influence them.
These considerations lead to certain conclusions about how to study clinical population with ERPs. The influence of the nonspecific task involvement factor should be evaluated for every ERP paradigm used. This can only be done by explicitly manipulating task involvement as a parameter in the control group. Without explicit manipulation, the control values may be bunched together at a mean that does not allow accurate estimates of the task involvement effects. Since clinical groups will be less responsive to task manipulations, they cannot be relied on to provide adequate estimates. Specifically, the control group should perform tasks that focus their attention closely on the stimuli and others that distract their attention away from them. Performance measures should witness the adequacy of these manipulations.
Effects independent of task involvement will be demonstrated in clinical groups by showing that their variables do not fall on the same parametric curves as the control group. This is essentially the same idea as making corrections for age when P300 latency is being considered (e.g., Goodin et al., 1978b). Some ERP or behavioral parameters may be found to be especially sensitive to task involvement and may be used as preferred covariates for estimating its effect in groups and individuals.
The ultimate stage of development in controlling for the effects of task involvement would be to be able to have ERP variables alone provide estimates of task involvement in patients who cannot or will not perform explicit tasks. Although this may seem futuristic to those of you familiar with the vagaries of ERP component measurement and interpretation, the ultimate rationale for ERPs is that they go beyond the assessments afforded by speech and other motor behavior, and can evaluate patients who elude evaluation by more ordinary means.
GENERAL CONCLUSIONS
Certain common themes have emerged from these contributions. 1 . Every clinical investigation must take into account changes due to age. Central
age effects must be separated from peripheral receptor changes. For that reason it is essential to match subjects for threshold sensitivity, perceptual acuity, and sometimes, subjective intensity, before drawing any conclusions about cognitive deficits.
2. Cognitive psychology provides us with hypotheses and experimental manipula- tions to apply to clinical groups. The contribution of ERPs is only decisive when there is a dissociation between them and behavioral measures. Otherwise, why should a clinic invest in expensive EEG amplifiers? Hence, the concurrent measurement of behavior is essential for justifying the usefulness of ERPs and for interpreting ERP differences reasonably. Psychological interpretations of ERPs in patients who cannot perform tasks are always speculative.
3. Nonspecificity of ERP findings in diseases that probably have specific biologi- cal pathologies is a major problem with all but the earliest ERPs. A generalized reduction in involvement in experimental tasks is a secondary manifestation of most
518 ANNALS NEW YORK ACADEMY OF SCIENCES
diseases characterized by behavioral abnormalities. The extent of the influence of task involvement and attention on the ERPs in each paradigm should be evaluated using attentional manipulations in control groups. When possible, performance in patients and control groups should be matched so that dissociations indicating deviant cognitive strategies or deviant brain structure can emerge.
REFERENCES
ALLISON, T., W. R. GOFF & C. C. WOOD. 1979. Auditory, somatosensory and visual evoked potentials in the diagnosis of neuropathology: Recording considerations and normative data. In Event-Related Potentials in Man: Applications and Problems. D. Lehmann & E. Callaway, Eds.: Plenum, New York. 1-16.
ASSELMAN, P., D. W. CHADWICK & C. D. MARSDEN. 1975. Visual evoked responses in the diagnosis and management of patients suspected of multiple sclerosis. Brain 9 8 261-282.
BARIBEAU-BRAUN, J., T. W. PICTON, J. Y. GOSSELIN & F. W. QUAN. 1983. Schizophrenia: A neurophysiological evaluation of abnormal information processing. Science 219 874-876.
BECK, E. C., C. SWANSON & R. E. DUSTMAN. 1980. Long latency components of the visually evoked potential in man: Effects of aging. Experimental Aging Research 6 523-545.
BIRREN. J. E. 1974. Translations in gerontology-from lab to life. Psychophysiology and speed of response. Am. Psycho]. 2 9 808-815.
CALLAWAY, E. 1981. Can the decomposition of attention clarify some clinical issues? (Commen- tary on: C. H. Vanderwolf & T. E. Robinson. Reticulo-cortical activity and behavior: A critique of the arousal theory and a new synthesis). Behav. Brain Sci. 4 477-479.
CALLAWAY, E. & S. NAGHDI. 1982. An information processing model for schizophrenia. Arch. Gen. Psychiatry 38 333-350.
CANCRO, R., S. SUITON, J. KERR & A. A. SUGERMAN. 1971. Reaction time and prognosis in acute schizophrenia. J. Nerv. Ment. Dis. 153 35 1-359.
CELESIA, G . C. & R. F. DALY. 1977. Effects of aging on visual evoked responses. Arch. Neurol. 3 4 403-407.
CHAPMAN, L. J., & J. P. CHAPMAN. 1973. Disturbed Thought in Schizophrenia. Prentice-Hall. Englewood Cliffs. N.J.
CHAPMAN, L. J . & J. P. CHAPMAN. 1978. The measurement of differential deficit. J. Psychiatr. Res. 1 4 303-3 1 I .
COBB, W. A., H. B. MORTON 8c G . ETTLINGER. 1967. Cerebral potentials evoked by pattern reversal and their suppression in visual rivalry. Nature 216 1123-1 125.
COLLINS, P. J., M. L. KIETZMAN, S. SUTTON & E. SHAPIRO. 1978. Visual temporal integration in psychiatric patients. J . Psychiatr. Res. 1 4 203-213.
DONCHIN, E. 1979. Event-related brain potentials: A tool in the study of human information processing. In Evoked Brain Potentials and Behavior. H. Begleiter, Ed.: Plenum. New York. 13-88.
DONCHIN, E. 1981. Surprise!. . . . Surprise? Psychophysiology 18 493-513. DONCHIN, E., E. CALLAWAY & R. T. JONES. 1970. Auditory evoked potential variability in
schizophrenia. 11. The application of discriminant analysis. Electroencephalogr. Clin. Neuro- physiol. 2 9 429440.
DRECHSLER, F. 1978. Quantitative analysis of neurophysiological processes of the aging CNS. J. Neurol. 218:197-2 13.
DUNCAN-JOHNSON, C. C. 1981. PSOO latency: A new metric of information processing. Psycho- physiology 18 207-2 15.
DUNCAN-JOHNSON, C. C., W. T. ROTH & B. S. KOPELL. 1984. Effects of stimulus sequence on P300 and reaction time in schizophrenics: A preliminary report. This volume.
DUSTMAN, R. E. & E. C. BECK. 1969. The effects of maturation and aging on the wave form of visually evoked potentials. Electroencephalogr. Clin. Neurophysiol. 2 6 2-1 1.
DUSTMAN, R. E., E. W. SNYDER & C. J. SCHLEHUBER. 1981. Life-span alterations in visually evoked potentials and inhibitory function. Neurobiology of Aging 2 187-192.
DUSTMAN. R. E., & E. W. SNYDER. 1981. Life span changes in visually evoked potentials at central scalp. Neurobiology of Aging 2 303-308.
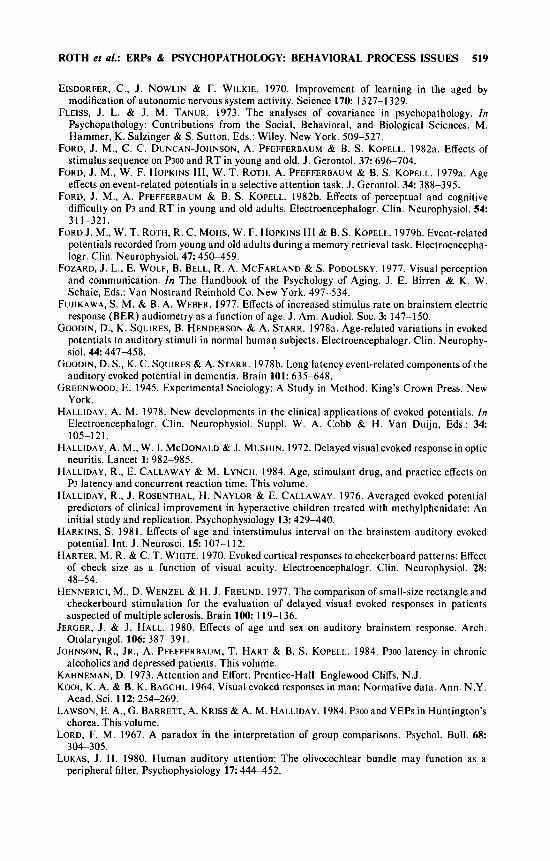
ROTH et a/.: ERPs & PSYCHOPATHOLOGY BEHAVIORAL PROCESS ISSUES 519
EISDORFER, C., J . NOWLIN & F. WILKIE. 1970. Improvement of learning in the aged by modification of autonomic nervous system activity. Science 170 1327-1 329.
FLEISS, J. L. & J. M. TANUR. 1973. The analyses of covariance in psychopathology. In Psychopathology: Contributions from the Social, Behavioral, and Biological Sciences. M. Hammer, K. Salzinger & S. Sutton, Eds.: Wiley. New York. 509-527.
FORD, J. M., C. C. DUNCAN-JOHNSON, A. PFEFFERBAUM & B. S. KOPELL. 1982a. Effects of stimulus sequence on P300 and R T in young and old. J . Gerontol. 37: 696-704.
FORD, J. M., W. F. HOPKINS 111, W. T. ROTH, A. PFEFFERBAUM & B. S. KOPELL. 1979a. Age effects on event-related potentials in a selective attention task. J. Gerontol. 34 388-395.
FORD, J. M., A. PFEFFERBAUM & B. S. KOPELL. 1982b. Effects of perceptual and cognitive difficulty on P3 and R T in young and old adults. Electroencephalogr. Clin. Neurophysiol. 54 31 1-321.
FORD J. M., W. T. ROTH, R. C. MOHS, W. F. HOPKINS 111 & B. S. K0PEt.L. 1979b. Event-related potentials recorded from young and old adults during a memory retrieval task. Electroencepha- logr. Clin. Neurophysiol. 47: 45&459.
FOZARD, J. L., E. WOLF, B. BELL, R. A. MCFARLAND & S. PODOLSKY. 1977. Visual perception and communication. In The Handbook of the Psychology of Aging. J. E. Birren & K. W. Schaie, Eds.: Van Nostrand Reinhold Co. New York. 497-534.
FUJIKAWA, S. M. & B. A. WEBER. 1977. Effects of increased stimulus rate on brainstem electric response (BER) audiometry as a function of age. J . Am. Audio]. SOC. 3: 147-150.
GOODIN, D., K. SQUIRES, B. HENDERSON & A. STARR. 1978a. Age-related variations in evoked potentials to auditory stimuli in normal human subjects. Electroencephalogr. Clin. Neurophy- siol. 44 447-458.
GOODIN, D. S., K. C. S Q U I R E S & A. STARR. I978b. Long latency event-related components of the auditory evoked potential in dementia. Brain 101: 635-648.
GREENWOOD, E. 1945. Experimental Sociology: A Study in Method. King’s Crown Press. New York.
HALLIDAY, A. M. 1978. New developments in the clinical applications of evoked potentials. In Electroencephalogr. Clin. Neurophysiol. Suppl. W. A. Cobb & H. Van Duijn, Eds.: 34 105-1 21.
HALLIDAY, A. M., W. I. MCDONALD & J. MUSHIN. 1972. Delayed visual evoked response in optic neuritis. Lancet 1: 982-985.
HALLIDAY, R., E. CALLAWAY & M. LYNCH. 1984. Age, stimulant drug, and practice effects on P3 latency and concurrent reaction time. This volume.
HALLIDAY, R., J . ROSENTHAL, H. NAYLOR & E. CALLAWAY. 1976. Averaged evoked potential predictors of clinical improvement in hyperactive children treated with methylphenidate: An initial study and replication. Psychophysiology 13: 429-440.
HARKINS, S. 198 1 . Effects of age and interstimulus interval on the brainstem auditory evoked potential. Int. J . Neurosci. 15: 107-1 12.
HARTER, M. R. & C. T. WHITE. 1970. Evoked cortical responses to checkerboard patterns: Effect of check size as a function of visual acuity. Electroencephalogr. Clin. Neurophysiol. 28:
HENNERICI, M., D. WENZEL & H. J. FREUND. 1977. The comparison of small-size rectangle and checkerboard stimulation for the evaluation of delayed visual evoked responses in patients suspected of multiple sclerosis. Brain 100 1 19-1 36.
JERGER, J. & J . HALL. 1980. Effects of age and sex on auditory brainstem response. Arch. Otolaryngol. 106 387-391.
JOHNSON, R., JR., A. PFEFFERBAUM, T. HART & B. S. KOPELL. 1984. P300 latency in chronic alcoholics and depressed patients. This volume.
KAHNEMAN, D. 1973. Attention and Effort. Prentice-Hall. Englewood Cliffs, N.J. KOOI, K. A. & B. K. BAGCHI. 1964. Visual evoked responses in man: Normativedata. Ann. N.Y.
LAWSON, E. A,, G. BARRETT, A. KRISS & A. M. HALLIDAY. 1984. P300 and VEPs in Huntington’s
LORD, F. M. 1967. A paradox in the interpretation of group comparisons. Psychol. Bull. 68:
LUKAS, J . H. 1980. Human auditory attention: The olivocochlear bundle may function as a
48-54.
Acad. Sci. 112: 254-269.
chorea. This volume.
304-305.
peripheral filter. Psychophysiology 17: 444452.
520 ANNALS NEW YORK ACADEMY OF SCIENCES
MARTINEAU, J., B. GARREAU, C. BARTHELEMY & G. LELORD. 1984. Evoked potential and P300 during sensory conditions in autistic children. This volume.
MATTHEWS, W. B., D. G. SMALL, M. SMALL & E. POUNTNEY. 1977. Pattern reversal evoked visual potential in the diagnosis of multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 4 0
MCCARTHY, G. & E. DONCHIN. 1981. A metric for thought: A comparison of PSOO latency and
MILNER, B. 1963. Effects of different brain lesions on card sorting. Arch. Neurol. 9 9&100. NEALE, J. M. & T. F. OLTMANNS. 1980. Schizophrenia. Wiley. New York. NILSSON, B. Y. 1978. Visual evoked responses in multiple sclerosis: Comparison of two methods
for pattern reversal. J. Neurol. Neurosurg. Psychiatry 41: 499-504. OLTMANNS, T. F. 1978. Selective attention in schizophrenic and manic psychoses: The effect of
distraction on information processing. J. Abnorm. Psychol. 87: 21 2-225. OLTMANNS, T. F. & J. M. NEALE. 1975. Schizophrenic performance when distractors are
present: Attentional deficit or differential task difficulty? J. Abnorm. Psychol. 84: 205-209. ORDY, J. M. & K. R. BRIZZEE. 1979. Functional and structural age differences in the visual
system of man and nonhuman primate models. I n Sensory Systems and Communication in the Elderly and Aging, Vol. 10. J. M. Ordy & K. Brizzee, Eds.: Raven. New York. 13-50.
PASTRNAKOVA, I. & J. PEREGRIN. 1977. The intensity-dependent changes of the visual evoked responses in man to patterned and blank stimulation. Pflug. Arch. 370 195-199.
PATTERSON, J. V., H. J. MlCHALEWsKl, L. W. THOMPSON & T. E. BOWMAN. 1981. Age- differences in the human auditory brainstem response. J. Gerontol. 3 6 455462.
PFEFFERBAUM, A., J. M. FORD, W. T. ROTH, W. F. HOPKINS 111 & B. S. KOPELL. 1979a. Event-related potential changes in healthy aged females. Electroencephalogr. Clin. Neurophy- siol. 4 6 81-86.
PFEFFERBAUM, A., T. B. HORVATH, W. T. ROTH & B. S. KOPELL. 1979b. Event-related potential changes in chronic alcoholics. Electroencephalogr. Clin. Neurophysiol. 47: 637-647.
PFEFFERBAUM, A., J. M. FORD, W. T. ROTH & B. S. KOPELL. 1980a. Age differences in P ~ e a c t i o n time associations. Electroencephalogr. Clin. Neurophysiol. 4 9 257-265.
PFEFFERBAUM, A., J. M. FORD, W. T. ROTH & B. S. KOPELL. 1980b. Age-related changes in auditory event-related potentials. Electroencephalogr. Clin. Neurophysiol. 4 9 266-276.
PFEFFERBAUM, A., B. WENEGRAT, B. S. KOPELL, J. M. FORD & J. R. TINKLENBERG. 1982. Electrophysiological approaches to the study of aging and dementia. I n Alzheimer’s Disease: A Review of Progress. S. Corkin, K. L. Davis, J. H. Growden, E. Usdin & R. J. Wurtman, Eds.: Raven. New York. 83-89.
1009-1014.
reaction time. Science 211: 77-80.
POSNER, M. I. 1978. Chronometric Explorations of Mind. Erlbaum. Hillsdale, N.J. REESE, J. N. & J. BOTWINICK. 1971. Detection and decision factors in auditory behavior of the
RESTAK. R. M. 1979. Brain potentials: Signaling our inner thoughts. Psychology Today 12: 42ff. ROBINSON, D. W. & G. J. SUITON. 1979. Age effects in hearing-a comparative analysis of
ROTH, W. T. & E. H. CANNON. 1972. Some features of the auditory evoked response in
ROTH, W. T., T. B. HORVATH, A. PFEFFERBAUM & B. S. KOPELL. 1980a. Event-related potentials
elderly. J. Gerontol. 2 6 133-136.
published threshold data. Audiology 1 8 320-334.
schizophrenics. Arch. Gen. Psychiatry 27: 466-47 1.
in schizophrenics. Electroencephalogr. Clin. Neurophysiol. 4 8 127-1 39.
1976. Parameters of temporal recovery of the human auditory evoked potential. Electroen- cephalogr. Clin. Neurophysiol. 4 0 623432.
ROTH, W. T., A. PFEFFERBAUM, T. B. HORVATH, P. A. BERGER & B. S. KOPELL. 1980b. P3 reduction in auditory evoked potentials of schizophrenics. Electroencephalogr. Clin. Neurophy- siol. 4 9 497-505.
ROTH, W. T., A. PFEFFERBAUM. A. F. KELLY, P. A. BERGER & B. S. KOPELL. 1981. Auditory event-related potentials in schizophrenia and depression. Psychiatry Res. 4 199-212.
ROWE, M. J. 1978. Normal variability of the brain-stem auditory evoked response in young and old adult subjects. Electroencephalogr. Clin. Neurophysiol. 4 4 459-470.
SCHENKENBERG, T. 1970. Visual, Auditory, and Somatosensory Evoked Responses of Normal Subjects from Childhood to Senescence. Ph.D. thesis. University of Utah. Salt Lake City.
SCHNEIDER, R. D., & V. GROSSI. 1979. Differences in muscle activity before, during, and after
ROTH, W. T., P. L. KRAINZ, J. M. FORD, J. R. TINKLENBERG, R. M. ROTHBART & B. S. KOPELL.
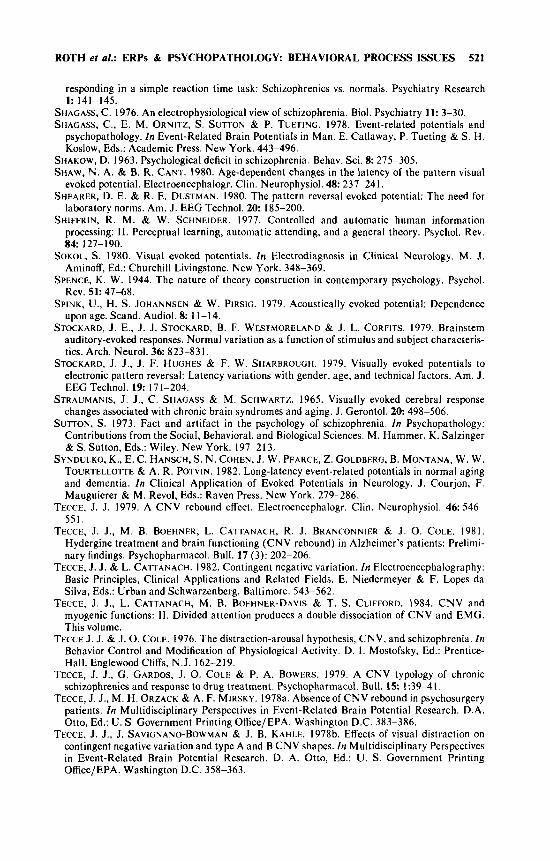
ROTH er al.: ERPs & PSYCHOPATHOLOGY: BEHAVIORAL PROCESS ISSUES 521
responding in a simple reaction time task: Schizophrenics vs. normals. Psychiatry Research 1: 141-145.
SHAGASS, C. 1976. An electrophysiological view of schizophrenia. Biol. Psychiatry 11: 3-30. SHAGASS, C., E. M. ORNITZ, S. SUTTON & P. TUETING. 1978. Event-related potentials and
psychopathology. In Event-Related Brain Potentials in Man. E. Callaway, P. Tueting & S. H. Koslow, Eds.: Academic Press. New York. 443-496.
SHAKOW, D. 1963. Psychological deficit in schizophrenia. Behav. Sci. 8: 275-305. SHAW, N. A. & B. R. CANT. 1980. Age-dependent changes in the latency of the pattern visual
evoked potential. Electroencephalogr. Clin. Neurophysiol. 48: 237-241. SHEARER, D. E. & R. E. DUSTMAN. 1980. The pattern reversal evoked potential: The need for
laboratory norms. Am. J . EEG Technol. 2 0 185-200. SHIFFRIN, R. M. & W. SCHNEIDER. 1977. Controlled and automatic human information
processing: 11. Perceptual learning, automatic attending, and a general theory. Psychol. Rev. 8 4 127-190.
SOKOL, S . 1980. Visual evoked potentials. In Electrodiagnosis in Clinical Neurology. M. J . Aminoff, Ed.: Churchill Livingstone. New York. 348-369.
SPENCE, K. W. 1944. The nature of theory construction in contemporary psychology. Psychol. Rev. 51: 47-68.
SPINK, U., H. S. JOHANNSEN & W. PIRSIG. 1979. Acoustically evoked potential: Dependence upon age. Scand. Audiol. 8: 11-14.
STOCKARD, J. E., J. J. STOCKARD, B. F. WESTMORELAND & J. L. CORFITS. 1979. Brainstem auditory-evoked responses. Normal variation as a function of stimulus and subject characteris- tics. Arch. Neurol. 3 6 823-83 1.
STOCKARD, J. J., J . F. HUGHES & F. W. SHARBROUCH. 1979. Visually evoked potentials to electronic pattern reversal: Latency variations with gender, age, and technical factors. Am. J. EEG Technol. 1 9 171-204.
STRAUMANIS, J . J., C. SHAGASS & M. SCHWARTZ. 1965. Visually evoked cerebral response changes associated with chronic brain syndromes and aging. J. Gerontol. 2 0 498-506.
SUTTON, S. 1973. Fact and artifact in the psychology of schizophrenia. In Psychopathology: Contributions from the Social, Behavioral, and Biological Sciences. M. Hammer, K. Salzinger & S. Sutton, Eds.: Wiley. New York. 197-213.
SYNDULKO, K., E. C. H A N S C H , ~ . N. COHEN, J . W. PEARCE, 2. GOLDBERG, B. MONTANA, W. W. TOURTELLOTTE & A. R. POTVIN. 1982. Long-latency event-related potentials in normal aging and dementia. In Clinical Application of Evoked Potentials in Neurology. J . Courjon, F. Mauguierer & M. Revol, Eds.: Raven Press. New York. 279-286.
TECCE, J. J. 1979. A CNV rebound effect. Electroencephalogr. Clin. Neurophysiol. 46: 546- 551.
TECCE, J. J., M. B. BOEHNER, L. CATTANACH, R. J. BRANCONNIER & J . 0. COLE. 1981. Hydergine treatment and brain functioning (CNV rebound) in Alzheimer’s patients: Prelimi- nary findings. Psychopharmacol. Bull. 17 (3): 202-206.
TECCE, J. J . & L. CATTANACH. 1982. Contingent negative variation. In Electroencephalography: Basic Principles, Clinical Applications and Related Fields. E. Niedermeyer & F. Lopes da Silva, Eds.: Urban and Schwarzenberg. Baltimore. 543-562.
TECCE, J. J., L. CATTANACH, M. B. BOEHNER-DAVIS & T. S. CLIFFORD. 1984. CNV and myogenic functions: 11. Divided attention produces a double dissociation of CNV and EMG. This volume.
TECCE J. J. & J . 0. COLE. 1976. The distraction-arousal hypothesis, CNV, and schizophrenia. In Behavior Control and Modification of Physiological Activity. D. I . Mostofsky, Ed.: Prentice- Hall. Englewood Cliffs, N.J. 162-219.
TECCE, J. J., G . GARDOS, J. 0. COLE & P. A. BOWERS. 1979. A CNV typology of chronic schizophrenics and response to drug treatment. Psychopharmacol. Bull. 15: 1:39-41.
TECCE, J . J., M. H. ORZACK & A. F. MIRSKY. 1978a. Absenceof CNV rebound in psychosurgery patients. In Multidisciplinary Perspectives in Event-Related Brain Potential Research. D.A. Otto, Ed.: U. S. Government Printing Office/EPA. Washington D.C. 383-386.
TECCE, J. J., J. SAVICNANO-BOWMAN & J. B. KAHLE. 1978b. Effects of visual distraction on contingent negative variation and type A and B CNV shapes. In Multidisciplinary Perspectives in Event-Related Brain Potential Research. D. A. Otto, Ed.: U. S. Government Printing Office/EPA. Washington D.C. 358-363.
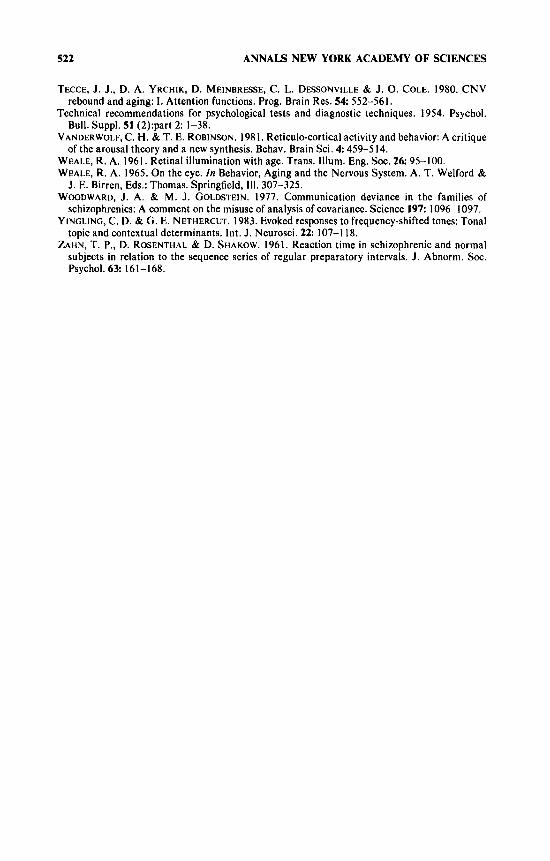
522 ANNALS NEW YORK ACADEMY OF SCIENCES
TECCE, J. J., D. A. YRCHIK, D. MEINBRESSE, C. L. DESSONVILLE & J. 0. COLE. 1980. CNV
Technical recommendations for psychological tests and diagnostic techniques. 1954. Psychol.
VANDERWOLF, C. H. & T. E. ROBINSON. 1981. Reticulo-cortical activity and behavior: A critique
WEALE, R. A. 1961. Retinal illumination with age. Trans. Mum. Eng. SOC. 26: 95-100. WEALE, R. A. 1965. On the eye. In Behavior, Aging and the Nervous System. A. T. Welford &
J. E. Birren, Eds.: Thomas. Springfield, 111. 307-325. WOODWARD, J. A. & M. J. GOLDSTEIN. 1977. Communication deviance in the families of
schizophrenics: A comment on the misuse of analysis of covariance. Science 197: 1096-1097. YINGLING, C. D. & G. E. NETHERCUT. 1983. Evoked responses to frequency-shifted tones: Tonal
topic and contextual determinants. Int. J. Neurosci. 2 2 107-1 18. ZAHN, T. P., D. ROSENTHAL & D. SHAKOW. 1961. Reaction time in schizophrenic and normal
subjects in relation to the sequence series of regular preparatory intervals. J. Abnorm. SOC.
rebound and aging: 1. Attention functions. Prog. Brain Res. 5 4 552-561.
Bull. Suppl. 51 (2):part 2: 1-38.
of the arousal theory and a new synthesis. Behav. Brain Sci. 4 459-5 14.
Psychol. 6 3 161-168.
Related Documents