e R n Euro peanRespiratory News Issue 85 Volume XXII 3-2014 Euroscienze Ed

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

eRnEuropeanRespiratoryNewsIssue 85
Volume XXII
Scientific Direction:Dario Olivieri DirectorEmilio Marangio Vice-DirectorAlfredo Chetta Vice-DirectorDepartment of Clinical andExperimental MedicineUniversity of Parma (Italy)
Editorial Board:Marina AielloElisa BonatiFrancesco LongoGiovanna PisiRoberta PisiMartina RendoElisabetta TeopompiPanagiota TzaniDina Visca
International Board:Alvar Agusti (Barcelona, S)Peter J. Barnes (London, UK)Demosthenes Bouros (Alexandroupolis, GR)Jean Bousquet (Montpellier, F)Chris Brightling (Leicester, UK)Roland Buhl (Mainz, D)Andrew Bush (London, UK)Pascal Chanez (Marseille, F)Vincent Cottin (Lyon, F)Carlos Robalo Cordeiro (Coimbra, P)Ronald Dahl (Odense, DK)Marc Decramer(Leuven, B)Richard Dekhuijzen (Nijmegen, NED)Stephen T. Holgate (Southampton, UK)Marc Humbert (Paris, F)Guy Joos (Ghent, B)Marc Miravitlles (Barcelona, S)Klaus Rabe (Grosshandorf, D)Jo/rgen Vestbo (Manchester, UK)Christian Virchow (Rostock, D)
Editorial Office:Stefano OlivieriMob. + 39 335 5422554E-mail: [email protected]
Printing and diffusion:Mattioli 1885Strada di Lodesana 649/sxLoc. Vaio - 43036 Fidenza-PRTel. 0524/530383Fax 0524/[email protected]
Pubbl. Trimestrale - Poste Italiane s.p.a. - Spedizioni in Abb. Postale D.L. 353/2003 (conv. in L. 27/02/2004 n. 46) art. 1, comma 1, DCB ParmaAut. Trib. Parma n. 26 del 27/28-10-1992 - Euro 2,58
Copyright: All the copyrights have been observed. However, for information, please contact the Editorial Office
3-2014
Euroscienze Ed
00-copertina 3-2014:copertina 2-2014 7-01-2015 8:06 Pagina 1

HELP SHAPE THE FUTURE OF RESPIRATORY SCIENCE AND MEDICINEtake part in ERS Amsterdam 2015
european respiratory societyevery breath counts
ATTEND the ERS International Congress, the largest respiratory meeting in theworld.
PRESENT your work in a learning environment of the highest level, to thewidest and most influential audience of respiratory professionals.
FORGE and RENEW working relationships with the leading specialists in thefield and update on the latest research and clinical best practice.
00-copertina 3-2014:copertina 2-2014 7-01-2015 8:06 Pagina 2
eRn
97
Contents
Europ. Respir. News XXII (85): 97, 2014
� EditorialOn Mentor and mentorshipDario Olivieri pag. 99
� Invited articlesClimate change, air pollution, extreme meteorological events andrespiratory diseasesGennaro D’Amato, Isabella Annesi-Maesano, Carolina Vitale,Maria D’Amato pag. 100Critical review of instruction checklists for proper inhaler useAndrea Melani pag. 112
� ERSHighlights of the 24th ERS International Congress, Munich:onwards and upwardsStephen T. Holgate pag. 125Driving the implementation of the ERS 2013-2018 Strategic planGiovanni Battista Migliori pag. 130
� StatisticsThe riddles of statisticsGiovanna Pisi, Alfredo Chetta pag. 138
� Research ProjectsNeonatal Physiological and Neural Correlates of Early Neurodevelopmentin Preterm ChildrenJessica Rose, Rachel Vassar, Katelyn Cahill-Rowley, Naama Barnea-Goraly,Susan R. Hintz, Kristen Yeom, David K. Stevenson pag. 141AsthmaZoè: Nanostructured Materials for the Detection of Markersof Asthma and Other Correlated Inflammatory DiseasesRossella De Marco, Giampaolo Ricci, Sergio Schinelli, Luisa De Cola,Luca Prodi, Luca Gentilucci pag. 142Passive Smoking and Vehicular Traffic Effect on Small Airway Functionand InflammationP. Paredi, A. Ruprecht, P.J. Barnes, O.S. Usmani pag. 144
01-indice e cover:01-indice e cover 7-01-2015 8:07 Pagina 97

eRn
98
About the cover
Miles Davis (1926-1991)- From “Kind of Blue” to “On the Corner”Miles Davis was an extraordinary influential musician with a wonderful giftfor original performances and innovative compositions.
Miles began playing the trumpet in the ‘40s during the bebop period up againstlegends such as Charlie Parker and Dizzy Gillespie. He quickly got away fromthat style which he did not particularly enjoy, revealing also a certain techni-cal inferiority in keeping up with the rapid beat characteristic of bebop.
He was the creator of several new styles such as cool jazz, hard bop, modaljazz and jazz fusion. The album “Birth of the Cool”, recorded in 1949, gaveits name to the cool jazz trend of the time. Hard bop was born out the “firstquintet” (1954-1958) made up of Miles on trumpet, John Coltrane on tenorsaxophone, Red Garland playing piano, Paul Chambers on bass and PhillyJoe Jones on drums.
Next, the “sextet” was made up of Coltrane and Chambers and new membersincluding Julian “Cannonball” Adderley on sax, Jimmy Cobb on drums andBill Evans and Wynton Kelly alternating on piano. “Kind of Blue”, producedin 1959, is the best expression of modal jazz, and probably also the best-sell-ing jazz album of all time.
The “second quintet” (1964-1968) was formed with George Coleman on sax,Ron Carter on bass, Tony Williams on drums and Herbie Hancock playing pi-ano. “Seven Steps to Heaven” is one of the most notable albums produced inthose years. The albums that followed such as “Miles Smiles”, “Sorcerer”,“Nefertiti”, and “Filles de Kilimanjaro”, introduced electrical instrumentsand lead into the successive fusion phase. New talents such as Dave Hollandand Chick Corea were also introduced.
Miles’ transition into fusion (blending funk and rock) came about from 1968-1975 with the albums “In a Silent way” and “Bitches Brew”. Live record-ings were made at the two Fillmores along with Steve Grossman and KeithJarret. The album “Live-Evil” and “Tribute to Jack Johnson” (1971) were al-so produced. Next followed “On the Corner” (1972) in which the influenceof modern composers such as Karlheinz Stockhausen can be felt. Critics weredivided, and many still today disparage Miles’ fusion period.
Many other musicians who later rose to prominence such as Joe Zawinul,Jack De Johnette, Tony Williams, John McLaughlin, were called up to play inensembles with Miles who was the bandleader and inspiration for every piece.
The later years from 1975-1980 were marked with silence and illness. Milesthen returned to the jazz scene and his performances received controversialreviews until his death at 65. Miles was inducted into the Rock and Roll hallof Fame in 2006.
1972, 2000 Sony Music Inc.Columbia Rec. N.Y.Columbia LegacyCover Art by Corky McCoy
01-indice e cover:01-indice e cover 7-01-2015 8:07 Pagina 98
eRn
99
Editorial
Europ. Respir. News XXII (85): 99, 2014
On Mentor and mentorship
“Don’t play what’s there, play what’s not there”.In: SPIN, December 1990, p. 30
Ulysses, before leaving for his long journey to Troy, asked one of his friends totake care of educating his son Telemachus. That friend was Mentor, who becamea surrogate father as well as an educator for Telemachus. The relationshipbetween Telemachus and Mentor has led the English language to adapt thepersonal name Mentor to mean someone who imparts wisdom to and shares knowl-edge with a less experienced colleague.
Young researchers and medical students are strongly advised “to find” themselvesa great mentor. What exactly makes for a “great mentor”, and in what does men-torship consist? Of course the literature is full of articles which try to explain theprocess, obligations, and steps characterising medical education and tutoring inits various phases.
An unusual example of mentorship is offered by the musician Miles Davis. Mileswas considered to be a wonderful performer, a visionary always striving for thenext level and ready to start all over again by questioning his creative capacityand genius. Miles was also famous for letting other musicians freely express them-selves according to how they thought best. He was always on the lookout for newtalent and novel ways to express music. The artists that worked with him wereboth honoured and intimidated to be chosen by the bandleader. Commonly, it wassaid that when musicians asked Miles how he wanted them to play, he always re-sponded to play as you want to and as you know how. In reality Miles alreadyknew what he wanted to hear from the group he formed or the individual musicianhe hired. In jazz, improvisation is important, but also the interplay between themusicians.
Many people wonder if that behaviour which works well in the arts can also betranslated into the field of medical research. Some think that a good researcher ismade by rigorous methodology and intellectual honesty (little inspiration and tonsof perspiration). Others believe that without imagination and creative liberty, theresult will always be rather flat and repetitive. Let alone renouncing any possibil-ity for the grace of serendipity. Alas, that is another story…
And you? How do you like Miles?
02-editoriale:02-editoriale 7-01-2015 8:08 Pagina 99
eRn
100
1. Introduction
The global environment is under-going profound change and manyof these changes can affect respira-tory health. Increased concentra-tions of greenhouse gases, and es-pecially CO2, in the earth’s atmos-phere have already warmed theplanet substantially, causing moresevere and prolonged heat waves,temperature variability, air pollu-tion, forest fires, droughts, andfloods, all of which put respiratoryhealth at risk (1-2). These changesin climate and air quality have aquantifiable impact, not only onthe morbidity but also on the mor-tality for respiratory diseases (3-5).The massive increase in emissionsof air pollutants due to economicand industrial growth in the lastcentury made air quality an envi-ronmental problem of first order ina large number of European andNorth American countries and it isnow an emerging problem in otherregions of the world (1-5).Global earth’s temperature hasmarkedly risen over the last 50years due to the increase in green-house gas emissions, largely fromanthropogenic sources. As stated in
the recent Working Group I Reportof the Intergovernmental Panel onClimate Change “most of the ob-served increase in globally aver-aged temperatures since the mid-20th century is very likely due tothe observed increase in anthro-pogenic greenhouse gas concentra-tions (1, 2)”. Changes are also oc-curring in the amount, intensity,frequency, and type of precipita-tion as well as the increase of ex-treme events, like heat waves,droughts, floods, thunderstormsand hurricanes and these are a realand daunting problem. A recentposition statement on climatechange and health impacts fromthe European Respiratory Society(ERS) was developed after a work-shop co-organized by the HEN-VINET Project and the AmericanThoracic Society (6). The positionstatement highlights climate relat-ed health impacts, including deathsand acute morbidity due to heatwaves; increased frequency ofacute cardio-respiratory events dueto higher concentrations of groundlevel ozone; changes in the fre-quency of respiratory diseases dueto transboundary particle pollu-tion; and altered spatial and tem-
Climate change, air pollution,extreme meteorological eventsand respiratory diseases
Invited article
Europ. Respir. News XXII (85): 100-111, 2014
Gennaro D’Amato1 (photo),Isabella Annesi-Maesano2,Carolina Vitale3, Maria D’Amato3
1 Division of Respiratory and AllergicDiseases, Department of Chest DiseasesHigh Specialty A.Cardarelli Hospital,Naples, ItalyCentro Studi Salute e Ambiente, Napoli2 EPAR, Institute Pierre Louis ofEpidemiology and Public Health, UMR-S1136 INSERM & UPMC Paris6,Sorbonnes Universités3 First Division of Pneumology, HighSpeciality Hospital “V. Monaldi” andUniversity “Federico II” Medical SchoolNaples, Italy
Correspondence to:Gennaro D’Amato, MD, FAAAAIDivision of Respiratory and Allergic Diseases,Department of Chest Diseases High SpecialityA.Cardarelli Hospital, Napoli ItalyCentro Studi Salute e Ambiente, NapoliVia Rione Sirignano,1080121 Napoli, ItalyE-mail: [email protected]
03-d'amato:d'amato 7-01-2015 8:09 Pagina 100
eRn
101
poral distribution of allergens (pol-lens, moulds and mites) and someinfectious disease vectors. Accord-ing to the report these impacts willnot only affect those with existingrespiratory disease but will likelyincrease the incidence and preva-lence of respiratory conditions (6).
2. Extreme temperature events
The effect of heat waves on mortal-ity is well documented (7). It hasbeen observed a rapid rise in thenumber of hot days and severe me-teorological events (8,9) such as the2003 and 2012 heat waves whentemperatures reached or went be-yond 35°C degrees resulting in ex-cess deaths across Europe (8,9).There is evidence of an increasednumber of deaths and acute mor-bidity especially among respiratorypatients due to heat waves. Forevery one degree Celsius rise in tem-
perature, the risk of prematuredeath among respiratory patients isup to six times higher than in therest of the population (6). The in-crease in respiratory mortality (rela-tive risk) is larger than total or car-diovascular mortality (10). Al-though the association between heatand the number of hospital admis-sions is less studied, and less evi-dent, admissions are, however, alsomore apparent for respiratory dis-ease than for cardiovascular (8).Moreover, climate scenarios for thenext century predict that thewarming will be associated withmore frequent and more intenseheat waves in wide areas of ourplanet with increased risk of wild-fires and desertification. Heat anddrought conditions contribute towildfire risks. Smoke emissions cantravel hundreds of kilometersdownwind of fire areas, exposingpeople to a complex mixture of fineparticles, ozone precursors, and
03-d'amato:d'amato 7-01-2015 8:09 Pagina 101

eRn
102
other health-harming compounds(11, 12) One recent worldwide es-timate is that 339,000 deaths an-nually may be attributable to land-scape fire smoke (12). Respiratoryand cardiovascular hospital admis-sions and emergency room visitsincrease in response to wildfiresmoke exposures, strongly associ-ated with PM levels (12, 13).Drought conditions create multiplehealth challenges: in dry condi-tions, more pollen, dust, particu-lates, and when present, wildfiresmoke which can irritate respirato-ry epithelium, exacerbate chronicrespiratory illnesses, asthma, andincrease risks for acute respiratoryinfection (14).In urban areas the effects are high-er since climate change influencesoutdoor air pollution because thegeneration and dispersion of airpollution is in strictly correlationwith local patterns of temperature,wind and precipitation (15).
3. Air Pollution
Air pollution is the environmentalfactor with the greatest impact onrespiratory health in Europe (1, 2).Particle pollution, vehicle exhaustand ground level ozone are themost important types of hazardouspollutants. Ozone is a powerful ox-idant that has been associated withpersistent structural airway andlung tissue damage, as well as con-tributing to more severe symptomsof asthma and an increase in respi-
ratory hospital admissions anddeaths in Europe and the USA(16). It is estimated that there willbe 1,500 more annual ozone asso-ciated deaths by the year 2020 inthe UK alone (16).Pollution models for climate changescenarios predict an increase inozone concentrations over large ar-eas, while the effect on particle con-centrations is less clear (17). High-er temperatures, clear skies andstagnant conditions will favorozone production. The short-termeffects of ozone on daily mortalityand respiratory disease are exten-sively studied, while there is onlylimited documentation of long-termeffects on mortality (18, 19).Positive associations have been ob-served between urban air pollutionand respiratory symptoms in chil-dren, and the literature containsmany reports of a relation betweenmotor vehicle exhausts and acuteor chronic respiratory symptoms inchildren living near traffic (18-20).Air pollution can negatively influ-ence lung development in childrenand adolescents (18-20).Most studies suggested the adverseeffects of air pollution on children’slung function and respiratorysymptoms. Particles and NO2showed more significant results,whereas effects of SO2 were notconsistent. A few studies indicatedthat O3 interacted with tempera-ture and sometimes seemed to be aprotective factor for children’s res-piratory health (21). Negative as-sociations between air pollutants
03-d'amato:d'amato 7-01-2015 8:09 Pagina 102

eRn
103
and pulmonary health were moreserious in asthmatic children thanin healthy subjects (21).Air pollution has a decremental ef-fect on lung function parametersfor up to 6 days after exposure inhealthy adults. SO2 emerged as themost significant air pollutant af-fecting short-term lung functionparameters. Deficits in lung func-tion were associated with a corre-lated set of pollutants that includednitrogen dioxide, acid vapor, fine-particulate matter (PM 2 5), andelemental carbon.Deficits in lung function duringyoung adulthood may increase therisk of respiratory conditions – forexample, episodic wheezing thatoccurs during a viral infection.However, the greatest effect of pol-lution related deficits may occurlater in life, since reduced lungfunction is a strong risk factor forcomplications and death duringadulthood (22).Prediction about the effects of cli-mate change on health-related airpollution is hampered by severallimits: future emissions depend onnumerous factors, such as popula-tion growth, economic develop-ment, energy use and production;current knowledge about weathereffects on air pollution is still un-satisfactory; there is still a need ofbetter emission inventories and ob-servational datasets; long-term ef-fects and actual enforcement of in-ternational agreements to reduceair pollution and greenhouse gases
emissions (e.g. Kyoto protocol) areunpredictable.
4. Allergens and allergicresponses
The effects of climate change onrespiratory allergy are still unclear,and studies addressing this topicare lacking. Global warming is ex-pected to affect the start, duration,and intensity of the pollen seasonon the one hand, and the rate ofasthma exacerbations due to respi-ratory infections and/or cold air in-halation on the other (23).Knowledge of a plant’s geographi-cal distribution and its floweringperiod and possible variations in-duced by climate change is of greatimportance.Plant species require a certainamount of heat to complete theirdevelopment; then air temperatureplays a key role, together with oth-er factors, such as day-length, wa-ter and nutrients availability andsoil type. An increasing amount ofevidence from all over the worldshow that the timing of life cycleevents of a large number of specieshave responded to the observed in-crease in earth’s temperature.Changes involve also plants pro-ducing allergenic pollen, with ex-pected consequences on atopicpopulation. Data provided by 30years of observations within the In-ternational Phenological Gardensnetwork showed that spring events
03-d'amato:d'amato 7-01-2015 8:09 Pagina 103

eRn
104
advanced by six days, the highestrate of phenological changes beingobserved in Western Europe andBaltic regions. Conversely, pheno-logical trends appear to be differ-ent in eastern border of Europe,sometimes showing a 1-2 weekslater start of the phases. An earli-er start of the season was con-firmed in studies focused on aller-genic plants, as birch, mugworth,grass and Japanese cedar, even ifdifferent methods and differentlength of datasets have been used.Due to the earlier onset, the pollenseasons are more often interruptedby adverse weather conditions inlate winter/early spring (23-25).Duration of the pollen season is al-so extended, especially in summerand in late flowering species.The climate changes projected dur-
ing the next century will influenceplant and fungal reproductive sys-tems and alter the timing, produc-tion, and distribution of aeroaller-gens. Increased exposure to aller-gens as a result of global warming,combined with exposure to pollu-tants that act synergistically to in-tensify the allergic response, couldpoint to increased respiratory prob-lems in the future. In fact, climatechange is likely to influence vegeta-tion, with consequent changes ingrowth and reproductive cycles andin the production of allergenicpollen (seasonal period and intensi-ty). In addition, weed species are ex-pected to proliferate. These changescan vary from one region to another,since some areas receive greateramounts of UV radiation and/orrainfall, than others (Table 1 and 2).
Table 1 - Effects of Climate Change on respiratory health
• An increased number of deaths and acute morbidity especially among respi-ratory patients due to heat waves
• An increased frequency of cardio-respiratory attacks due to higher concen-trations of ground-level ozone
• Changes in the frequency of respiratory disease due to transboundary long-range air pollution
• Altered distribution of allergens and some infectious disease vectors
Table 2 - Why Climate Change is correlated with pollen allergy?
• Increase and faster plant growth• Increase in the amount of pollen produced by each plant• Increase in the amount of allergenic proteins contained in pollen• Increase in the start time of plant growth and therefore the start of pollen
production and earlier and longer pollen seasons
03-d'amato:d'amato 7-01-2015 8:09 Pagina 104
eRn
105
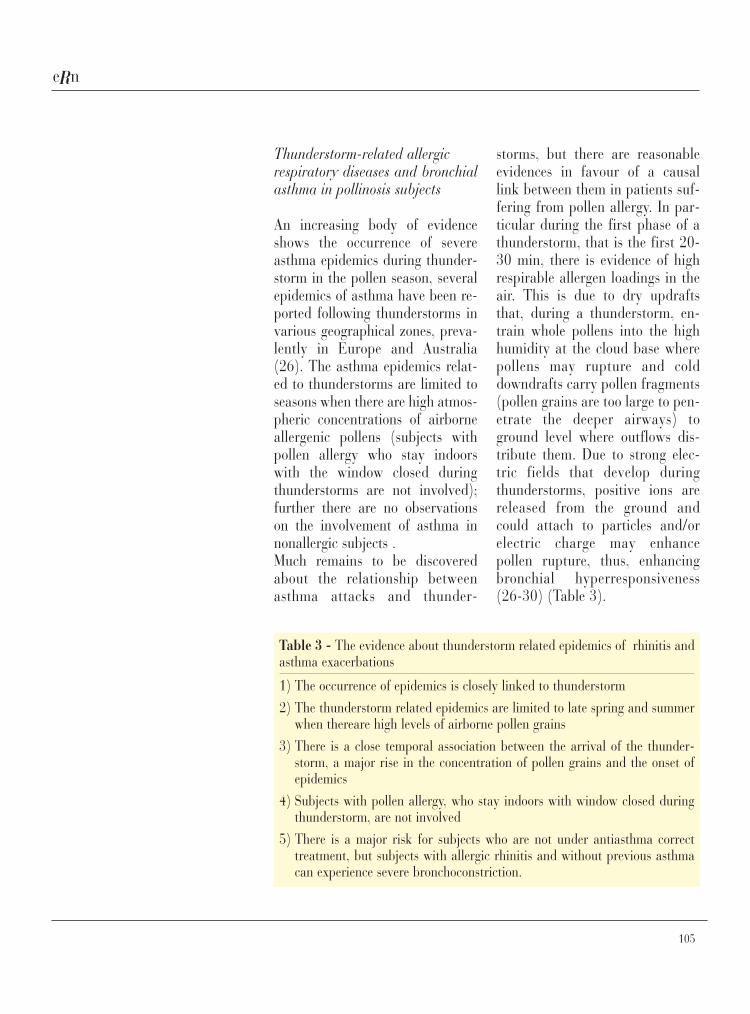
Thunderstorm-related allergicrespiratory diseases and bronchialasthma in pollinosis subjects
An increasing body of evidenceshows the occurrence of severeasthma epidemics during thunder-storm in the pollen season, severalepidemics of asthma have been re-ported following thunderstorms invarious geographical zones, preva-lently in Europe and Australia(26). The asthma epidemics relat-ed to thunderstorms are limited toseasons when there are high atmos-pheric concentrations of airborneallergenic pollens (subjects withpollen allergy who stay indoorswith the window closed duringthunderstorms are not involved);further there are no observationson the involvement of asthma innonallergic subjects .Much remains to be discoveredabout the relationship betweenasthma attacks and thunder-
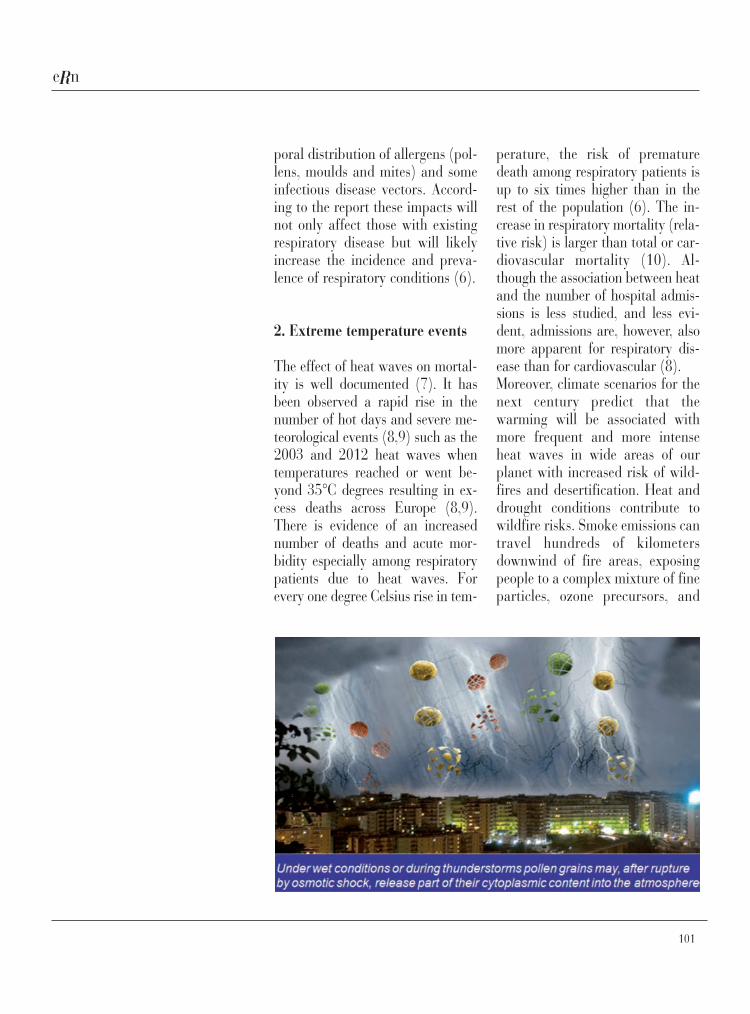
storms, but there are reasonableevidences in favour of a causallink between them in patients suf-fering from pollen allergy. In par-ticular during the first phase of athunderstorm, that is the first 20-30 min, there is evidence of highrespirable allergen loadings in theair. This is due to dry updraftsthat, during a thunderstorm, en-train whole pollens into the highhumidity at the cloud base wherepollens may rupture and colddowndrafts carry pollen fragments(pollen grains are too large to pen-etrate the deeper airways) toground level where outflows dis-tribute them. Due to strong elec-tric fields that develop duringthunderstorms, positive ions arereleased from the ground andcould attach to particles and/orelectric charge may enhancepollen rupture, thus, enhancingbronchial hyperresponsiveness(26-30) (Table 3).
Table 3 - The evidence about thunderstorm related epidemics of rhinitis andasthma exacerbations
1) The occurrence of epidemics is closely linked to thunderstorm2) The thunderstorm related epidemics are limited to late spring and summer
when thereare high levels of airborne pollen grains3) There is a close temporal association between the arrival of the thunder-
storm, a major rise in the concentration of pollen grains and the onset ofepidemics
4) Subjects with pollen allergy, who stay indoors with window closed duringthunderstorm, are not involved
5) There is a major risk for subjects who are not under antiasthma correcttreatment, but subjects with allergic rhinitis and without previous asthmacan experience severe bronchoconstriction.
03-d'amato:d'amato 7-01-2015 8:09 Pagina 105

eRn
106
Though the degree of symptoms isinfluenced by the concentration ofallergenic pollen, the relationshipbetween allergen exposure, inflam-mation of airways and clinicalsymptoms is complex, and factorsother than allergens are probablyinvolved, one of these is air pollu-tion. Air pollution may contributeto the asthmatic activity as gaseousair pollution affects airways by in-ducing inflammation and subjectsliving in urban areas tend to bemore affected by plant-derived res-piratory disorderes than those liv-ing in rural areas, and pollen aller-gens release is modified by expo-sure of pollen to enviromental pol-lution (26-30).In the light of the above, subjectsaffected by pollen allergy, not olyasthmatic patients but also subjectsaffected by seasonal rhinitis with-out asthma symptoms, should bealert to the danger of being out-doors during a thunderstorm in thepollen season, as such events maybe an important cause of severe ex-acerbations.
5. Respiratory Infections
The seasonal patterns and climaticsensitivities of many respiratorydiseases are well known; the impor-tant contemporary concern is theextent to which changes in diseasepatterns will occur under the condi-tions of global climate change (13).It is clear that infectious diseaseranges are shifting with increasing
temperatures into higher latitudesand elevation, but the impacts onhuman health are largely un-known.Pneumonia is rarely mentioned inthe context of climate change,butclear seasonal variation is notedsuggesting climate related effects.The incidence of respiratory infec-tions varies on a seasonal basis.Lower respiratory tract infectionshave a higher incidence during thewinter in temperate areas, but intropical areas, the incidence of in-fection is usually higher during theannual rainy season. A recent studyin China found that multi-day in-creases in temperature (i.e., lack ofcooling at night) were associatedwith increase emergency depart-ment utilization for respiratorytract infections. Climate changecould potentially increase the inci-dence of childhood pneumonia intropical settings through severaldifferent mechanisms. Increasedtime indoors because of heavierrainfall could increase crowdingand exposure to biomass fuelsmoke, and decrease exposure tosunlight (i.e., reduced vitamin D).Population displacement due todrought and famine could furtherincrease the rate of transmission ofinfections. Malnutrition due todrought as a result of climatechange is likely to increase pneu-monia deaths, since a substantialproportion of pneumonia deaths inchildren under 5 years are attrib-uted to this factor (13).In addition to increased rainfall in
03-d'amato:d'amato 7-01-2015 8:09 Pagina 106

eRn
107
tropical areas, climate change ispredicted to increase the intensity ofstorm events that will lead to flood-ing. Floods can also cause persistentdampness in homes that is associat-ed with microbial growth, especial-ly fungal (molds). The molds thatgrow in buildings in a post-floodenvironment can be different andthe levels much higher than what iscommon when flooding has not oc-curred. High indoor/outdoor moldratios were observed in the monthsimmediately following HurricanesKatrina and Rita, indicating the po-tential for high indoor exposures.Respiratory illness associated withmold exposure is generally non-in-fectious in immune-competent indi-viduals. Individuals who are sensi-tized to fungal allergens are at riskfor exacerbations of allergic rhinitisand asthma with high indoor expo-sures. Aero-allergenic mold levelsmay increase under climate changethrough several mechanisms: 1) el-evated carbon dioxide concentra-tions augmenting growth, indoordampness and conditions in build-ing materials that encourage toxicmold growth indoors, and risingtemperatures that support growth(13).
6. Conclusion
Health effects of climate change in-clude an increase in the prevalence
of allergic respiratory diseases, ex-acerbations of chronic lung disease,premature mortality, and declinesin lung function.Climate change, mediated bygreenhouse gases, causes adversehealth effects to the most vulnera-ble patient populations-the elderly,children, and those in distressedsocioeconomic strata.Considering these aspects govern-ments worldwide and internationalorganizations such as the WorldHealth Organization and the Euro-pean Union are facing a growingproblem of the respiratory effectsinduced by gaseous and particulatepollutants arising from motor vehi-cle emissions.In conclusion, strategies to reduceclimate changes and air pollutionare political in nature, but citizenand in particular health profession-als and societies must raise theirvoices in the decision process togive strong support for clean poli-cies on both national and interna-tional levels.Policy changes are beginning toimpact greenhousegas productionin many parts of the world.Theseefforts are crucial for reducing fu-ture impacts, but because over-allglobal emissions continue to raise,adaptation to the impacts of futureclimate variability will also be re-quired.
eRn
03-d'amato:d'amato 7-01-2015 8:09 Pagina 107
eRn
108
References
1. IPCC. Climate Change 2007: The Phys-ical Science Basis.http://ipcc-wg1.ucar.edu/wg1/docs/WG1AR4_SPM_PlenaryApproved.pdf
2. Solomon, S., D. Qin, M. Manning et al,Technical Summary. In: Climate Change2007: The Physical Science Basis. Con-tribution of Working Group I to theFourth Assessment Report of the Inter-governmental Panel on Climate ChangeSolomon, S., D. Qin, M. Manning, Z.Chen, M. Marquis, K.B. Averyt, M. Tign-or and H.L. Miller (eds.). CambridgeUniversity Press, Cambridge, UnitedKingdom and New York, NY, USA.
3. Peters A, von Klot S, Heier M, Trenti-naglia I, Hörmann A,Wichmann H,Löwel H. Exposure to traffic and theonset of myocardial infarction. N Engl JMed 2004; 351: 1721-30.
4. Schwartz J. Particulate air pollutionand daily mortality: a synthesis. PublicHealth Rev 1992; 19: 39-60.
5. Dockery DW, Stone PH. Cardiovascularrisks from fi ne particulate air pollu-tion. N Engl J Med 2007; 356: 511-3.
6. Ayres JG, Forberg B, Annesi-Maesano Iet al Climate change and respiratorydisease. European Respiratory Societyposition paper on behalf of the Envi-ronment & Human Health Committee.Eur Respir J 2009, 34: 295-302.
7. Kovats RS, Hajat S:Heat stress andpublic health: a critical review AnnuRev Public Health 2008; 29: 41-55.
8. Stafoggia M, Forastiere F, Agostini D, etal. Factors affecting in-hospital heat-re-lated mortality: a multi-city case-crossover analysis J Epi Comm Health2008; 62: 209-215.
9. Michelozzi P, Accetta G, De lario M. etal. PHEWE Collaborative Group: Hightemperature and hospitalizations forcardio-vascular and respiratory causesin 12 european cities. Am J Respir CritCare Med 2009; 179 (5): 383-389.
10. Baccini M, Biggeri A, Accetta G. et al.Heat effects on mortality in 15 Euro-
pean cities. Epidemiology 2008; 19:711-19.
11. Delfino RJ, Brummel S, Wu J, et al. Therelationship of respiratory and cardio-vascular hospital admissions to thesouthern California wildfires of 2003.Occup. Environ Med 2009; 66 (3): 189-197.
12. Dennekamp M, Abramson MJ. The ef-fects of bushfire smoke on respiratoryhealth. Respirology 2011; 16 (2); 198-209.
13. Takaro TK, Knowlton K, Balmes JR Cli-mate Change and Respiratory HealthExpert Rev Resp Med 2013; 7 (4): 349-361.
14. D’Amato G, Baena-Cagnani CE, CecchiL. Climate change, air pollution and ex-treme events leading to increasingprevalence of allergic respiratory dis-eases. Multidisciplinary RespiratoryMedicine 2013, 8:12 doi:10.1186/2049-6958-8-12.
15. Filippidou EC. Koukouliata A Ozone ef-fects on the respiratory system. ProgHealth Sci 2011; 1; 144-155.
16. Jacob DJ, Winner DA. Effect of climatechange on air quality. Atmos Environ2009; 43: 51-63.
17. Gryparis A, Forsberg B, Katsouyanni K,et al. Acute effects of ozone on mortali-ty from the “air pollution and health: aEuropean approach” project. Am JRespir Crit Care Med 2004; 170: 1080-7.
18. Jerrett M, Burnett RT, Pope CA 3rd et al:Long-term ozone exposure and mortali-ty. N Engl J Med 2009; 360: 1085-95.
19. Epton MJ, Dawson RD, Brooks WM, etal. The effect of ambient air pollutionon respiratory health of school children:a panel study. Environ Health 2008; 14:7-16.
20. Gauderman WJ, Vora H, McConnell etal. Effect of exposure to traffic on lungdevelopment from 10 to 18 years of age:a cohort study. Lancet 2007; 369: 571-7.
21. Li S, William G, Jalaudin B, Baker P.Panel studies of air pollution on chil-
dren’s lung function and respiratorysymptoms: a literature review. J Asthma2012; 49 (9): 895-910. doi: 10.3109/02770903.2012.724129. Epub 2012Sep 28.
22. Steinvil A, Fireman E, Kordova-Biezuner L, et al. Environmental airpollution has decremental effects onpulmonary function test parameters upto one week after exposure. Am J MedSci 2009; 338 (4): 273-9. doi: 10.1097/MAJ.0b013e3181adb3ed.
23. D’Amato G, Liccardi G, D’Amato M,Cazzola M. Outdoor air pollution, cli-matic changes and allergic bronchialasthma. Eur Respir J 2002; 20 (3): 763-76.
24. D’Amato G, Cecchi L, Bonini S, et al.Allergenic pollen and pollen allergy inEurope. Allergy 2007: 62: 976-990.
25. Wayne P, Foster S, Connolly J, et al.Production of allergenic pollen by rag-weed (Ambrosia artemisiifolia L.) is in-creased in CO2-enriched atmospheres.Ann Allergy Asthma Immunol 2002; 88:279-282
26. D’Amato G. Holgate S. The impact ofair pollution on respiratory health.European Society Monograph n. 22,2002.
27. D’Amato G, Liccardi G, Frenguelli G.Thunderstorm-associated asthma inpollinosis patients. Allergy 2007; 62:11-16.
28. D’Amato G, Cecchi L, Annesi-MaesanoI. A trans-disciplinary overview of casereports of thunderstorm-related asthmaoutbreaks and relapse. Eur Respir Rev2012; 21 (124): 82-7.
29. D’Amato G, Cecchi L, D’Amato M, An-nesi-Maesano I. Climate change andrespiratory diseases. Eur Respir Rev2014; 23 (132): 161-9.
30. D’Amato G. Holgate ST. Pawanker R,Annesi-Maesano I, et al. Meteorologi-cal Conditions, Climate Change, NewEmerging Factors and Bronchial Asth-ma. A Statement of the World AllergyOrganization. In press on WAO Jour-nal.
03-d'amato:d'amato 7-01-2015 8:09 Pagina 108

eRn
109
Gennaro D’Amato graduated in Medicine and Surgery summa cum laude in 1970 inthe University of Naples (Italy);Board in Respiratory Medicine and Phtisiology sum-ma cum laude University of Naples “Federico II” ,1972; Board in Allergy and Clini-cal Immunology summa cum laude ,University of Florence,1975. Director, Division ofPneumology and Allergology, Department of Chest Diseases, High Speciality Hospital“A.Cardarelli” Naples, Italy from 1985 to 2013; Consultant Professor of RespiratoryAllergy, Medical School of Specialization in Respiratory Medicine, University ofNaples “Federico II” from 1984 to present. He had periods of research stages atSt.Mary’s Hospital-Medical School in London; Hopital Universitaire Saint Margueritein Marseille, France; University of Michigan Ann Arbor, USA. At national level heserved in the directive board of Italian Society of Allergology and Clinical Immunolo-gy and in the Italian Societies of Pneumology. In particular he served as general sec-retary of Italian Society of Respiratory Diseases (SIMeR) from 2006 to 2009 and, from2011 to 2013, as chairman of clinical area in the Italian Association of Pneumology(AIPO). In AIPO he is now chairman of national group of study on “Asthma-COPD-Respiratory Allergy”. From 2013 to present he is chairman of the GARD workinggroup on “Environment and Respiratory Health” of Italian Ministry of health. Heserves in the MIUR committee of evaluation of scientific university production in Italy.He serves in the GINA Italian board. At the international level he served from 1995 to2005 as chairman of committee on “Air pollution, aerobiology and allergic respirato-ry diseases” of European Academy of Allergy and Clinical Immunology (EAACI) andfrom 2008 to 2009 he served as chairman of the joint task force EAACI-ERS to pro-duce documents on “Climate change, air pollution and respiratory diseases”. From2008 at present he is chairman of committee on “Climate change, air pollution andallergic respiratory diseases” of World Allergy Organization. Starting from 2012 heacts also as chairman of the WAO task force on “Meteorological Conditions, ClimateChange, New Emerging Factors and Bronchial Asthma.” to produce a Statement ofthe World Allergy Organization which is now in press on WAO Journal as a manus-cipt and as a book with 14 chapters and with the collaboration of 48 top leaders inthe world on this topic. He is currently member of several societies in the context ofrespiratory diseases (national:AIPO and SIMeR and international: ERS, Interasmaand ATS) and allergic diseases (national:AAITO and SIAAIC and international:AAAAI,EAACI,WAO) and he acts as invited speaker and/or chairman in several con-gresses and meetings of these societies in symposia and in plenary sessions in all theworld (Europe, USA, Canada, Asia, South America, Australia). He has been invitedas speaker and chairman also in the Congresses of World Society of internal medicine.He serves or has served in the editorial board of several medical journal ssuch as Clin-ical and Experimental Allergy; Allergy; Journal of Investigation of Allergy and Clini-cal Immunology; Respiratory Medicine; European Annals of Allergy and Clinical Im-munology; Multidisciplinary Respiratory Medicine; Journal of Allergy; MonaldiArchives for Chest Diseases; Aerobiology and others. He studies also the interrela-tionship between the use of social networks and symptoms of asthma, publishing sev-eral manuscripts on this topic. He is consultant reviewer fo the major medical scien-tific journals such as The Lancet; AJRCCM; JACI; CEA; Respiratory Medicine and oth-ers. He authored more than 300 papers (cumulative IF 650; H index 44) in peer re-view journals. He served as editor of 3 books in english, as unique author of 14 booksin italian and authored several chapters of books and monographs. He was theunique winner in southern Italy of the academic qualification as university full pro-fessor of respiratory medicine in the CINECA-MIUR evaluation of 2013.
03-d'amato:d'amato 7-01-2015 8:09 Pagina 109

eRn
110
Dr. Isabella Annesi-Maesano is Director of the Department of Epidemiology of Al-lergic and Respiratory Diseases (EPAR) (http://www.epar.fr/) at the French NIH andUniversity Pierre and Marie Curie (UPMC), Sorbonne Universités, in Paris, France,conducting research on the distribution and the aetiology of allergic and respirato-ry diseases and Professor of Environmental Epidemiology at Université Diderot,Paris. She is currently member of the Environmental & Health Committee of the Eu-ropean Respiratory Society (ERS) and Chair of the Interest Group Aerobiology andAir Pollution of the European Academy of Allergy and Clinical Immunology(EAACI). Previously she served the ERS as member of the Executive Committee andChair and Secretary of the Occupation and Epidemiology Assembly and the Inter-national Union Against Tuberculosis and Lung Diseases as Chair and ProgrammeSecretary of the Respiratory Diseases Section. She is PI of the EU-funded HEALSproject (www.heals-eu.eu). Dr Annesi-Maesano serves as Associate Editor of the ed-itorial boards of: European Respiratory Journal, European Respiratory Review;Clinical Experimental Allergy, International Journal of Tuberculosis and Lung Dis-ease, BMC Public Health, European Respiratory Review, Therapeutic Advances inRespiratory Disease, Respiratory Multidisciplinary Review and at the national lev-el of La lettre du pneumologue. Dr Annesi-Maesano has published more than 250international articles and book chapters and received Research Awards and onefrom the Medical Research Council, UK. Dr Annesi-Maesano is a respiratory epi-demiologist by training through a PhD, a DSc and a post-doc (Department of Pub-lic Health Sciences at St George’s Hospital, London) in Epidemiology and PublicHealth. She graduated in Physics (Rome) and Medicine (Paris).
Carolina Vitale was born in Caserta (Italy), 30 April 1982. Degree in Medicineand Surgery 110/110 summa at the University “Federico II”of Naples, 2007;Board in Respiratory Diseases, 70/70 summa cum laude at the University “Fed-erico II” of Naples in 2012. Since 2012 she works with a scholarship in Respira-tory Unit “Federico II” Department of Chest Diseases, High Speciality UniversityHospital “V. Monaldi”, Naples, Italy taking care both inpatients and outpatients.Dr Carolina Vitale is co-investigator and sub-investigator in numerous Nationaland international clinical trials (Fase II, Fase III a-b), in particular on pharma-cological and biological treatment of obstructive respiratory diseases. She haspublished her research findings in several manuscripts in national and interna-tional journals.
03-d'amato:d'amato 7-01-2015 8:09 Pagina 110

eRn
111
Maria D’Amato was born in Salerno (Italy), 12 October 1972. Degree in Medi-cine and Surgery 110/110 summa cum laude at the University of Naples, 1996;Board in Respiratory Diseases, 50/50 summa cum laude at the University ofNaples in 2000; PhD in Respiratory Physiopathology in Heart-Lung Department,Second University of Naples in 2003.Dr D’Amato had the opportunity to spend seven months (from January to July1999) in the King’s Hospital in London to study etiopathogenetic and therapeuticaspects of Bronchial Hyperresponsiveness.Dr Maria D’Amato served as pneumologist in the Division of Respiratory Diseasesof High Specialty Hospital “San Sebastiano” in Caserta (Italy) from 2004to 2009 and in the Pneumotisiological Division of “V.Monaldi” Hospitalin Naplesfrom 2009 to 2011.Since 2011 she works in Respiratory Unit “Federico II” De-partment of Chest Diseases, High Speciality University Hospital “V. Monaldi”,Naples, Italy taking care both inpatients and outpatients. Dr Maria D’Amato hasserved as co-investigator in several clinical and pharmacological trials conductedaccording to good clinical practice (GCP) guidelines in the field of asthma andCOPD. Dr D’Amato’s main clinical expertise is in the diagnosis, management andtreatment of asthma and COPD and in particular she studies bronchial hyperre-sponsiveness in bronchial asthma, pathophysiological mechanisms of COPD andtherapeutic (pharmacological and biological) aspects of obstructive respiratorydiseases.Maria D’Amato is Principal investigator, co-investigator and sub-investigator innumerous National and international clinical trials (Fase II, Fase III a-b), in par-ticular on pharmacological and biological treatment of obstructive respiratory dis-eases. She has published her research findings in more than 100 manuscripts innational and international journals, including the top medical journals.
03-d'amato:d'amato 7-01-2015 8:09 Pagina 111

eRn
112
The dream of inhaled medicationsfor treating bronchopulmonarydiseases existed long before mod-ern technology has turned it intoreality. Interestingly, the availabili-ty of drugs for the management oflung diseases has often precededthat of devices, providing effectivepulmonary drug delivery. Nowa-days, a range of devices are avail-able allowing safe, effective, andconvenient drug delivery to thelungs, with some of them releasingthe same drug and considered to beequally effective at equivalentdosages (1). Guidelines on asthmaand COPD do not prioritize thechoice of the device, but they high-light the importance of a proper in-halation technique. Therefore, it iscrucial to have a device in whichthe drug dose is optimally generat-ed and delivered to the lung onlywhen the inhaler is properly used.Although manufacturers are in-vesting many resources and effortsin improving the usability of de-vices, inhaler misuse is still com-mon with all devices in real life andit is associated to poor asthma andCOPD control (2). A major causeof the persistently high rate of in-haler misuse is that many users do
not know or forget how to use theirinhaler properly. Practical educa-tion by trained health care givers atfirst prescription together with aregular check of proper inhalertechnique at follow-up visits arethe most important factors to im-prove inhaler technique (3). How-ever, this education activity re-quires a standardized checklist ofsteps for proper inhaler usage ofeach device. Unfortunately, there isnot yet such an accepted instruc-tion checklist for the most com-monly used devices, even if somerelevant efforts have been done (4).Three main reasons may contributeto explain this unfavourable find-ing. Firstly, the advancements oftechnology may determine somechanges in the inhaler technique.Secondly, manufacturers mayeventually test some options of in-haler use and select the final rec-ommendations based on clinical ormarketing advantages, without ex-plaining them to customers. Lastly,as a variety of inhalers have beendeveloped and different studieshave confirmed the difficulty ofmaintaining a proper inhalationtechnique, some manufacturers au-tomatically tend to extend some
Critical review of instructionchecklists for proper inhaler use
Invited article
Europ. Respir. News XXII (85): 112-124, 2014
Andrea MelaniUniversity HospitalSanta Maria alle Scotte,Siena, Italy
Correspondence to:Andrea Melani, MDUOC Pathophysiology andRespiratory RehabilitationUniversity Hospital of SienaPoliclinico Le ScotteV.le Bracci - 53100 Siena (Italy)E-mail: [email protected]
04-melani:melani 7-01-2015 8:10 Pagina 112

eRn
113
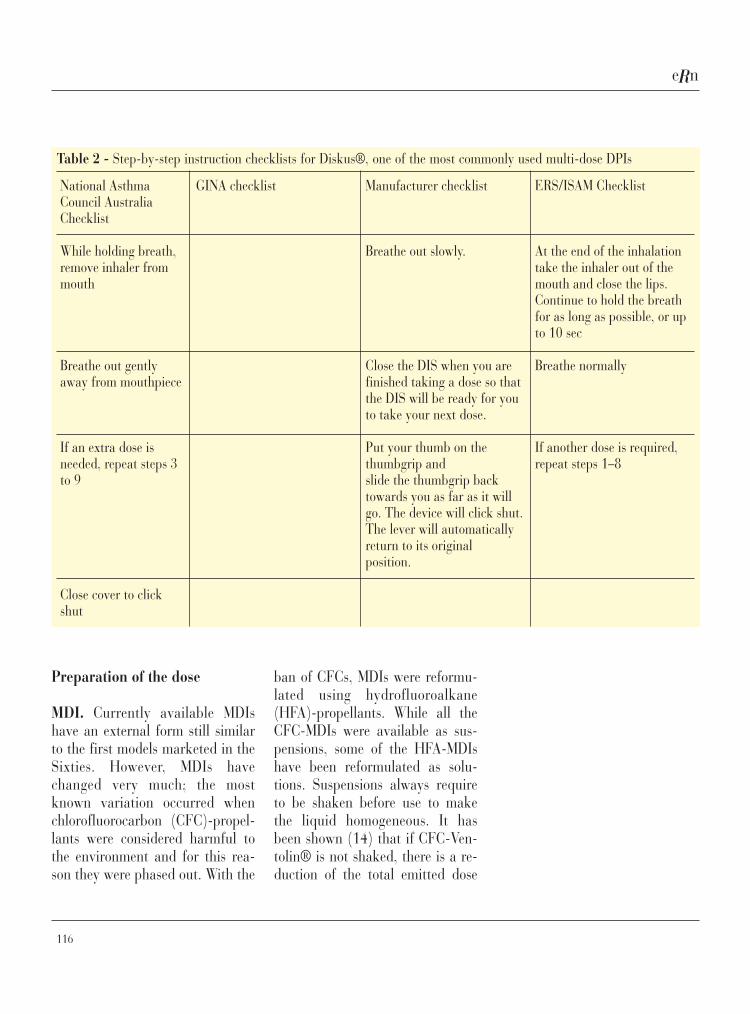
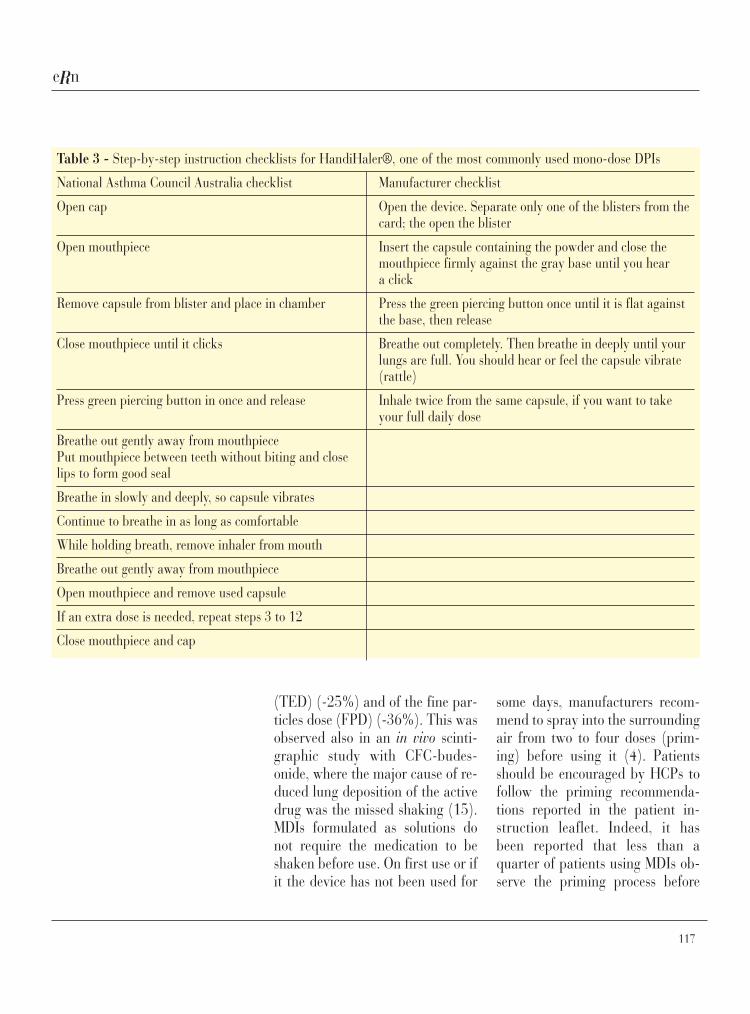
steps demonstrated with anotherdrug/device system to their owndevice with little or no evidence.Web sites, guidelines and manufac-turers’ instruction leaflets often de-scribe different steps for the in-halers without explaining theirclinical relevance, therefore caus-ing confusion among patients andhealth care givers.Four different types of devices arecurrently used for pulmonary drugdelivery: pressurized metered doseinhalers (pMDIs), dry powder in-halers (DPIs), soft mist inhalers(SMIs) and nebulizers. Inhalers(pMDIs and DPIs) are the mostpreferred and used devices becausethey are less cumbersome and moreconvenient than nebulizers. Respi-mat® is the only available SMI. Al-though it is a very interesting de-vice, it is not very common. DPIsand pMDIs are by far the mostcommonly used inhalers and theirinstruction checklists will be dis-cussed in the present review. In Ta-bles 1-3 we have displayed somestep-by-step instruction checklistsfor proper use of MDIs and somecommonly used DPIs (3-9).Typically, all instruction checklistsinclude the description of some keypoints: 1) exhalation (how muchand where) before inhaling, 2)preparation of the dose, 3) positionof the user with reference to place-ment of device mouthpiece, imme-diately before inhaling, 4) inhala-tion of the dose (how and howmuch), 5) breath-holding after in-halation and subsequent exhala-
tion, 6) maintenance and storageof device after using.
Exhalation before inhaling
MDI. Some checklists do not in-clude how much air is to be exhaledbefore inhaling, as this does notusually affect clinical outcomes.Other checklists specify “exhalingto empty the lungs” or “up to resid-ual volume” or at least “up to func-tional residual capacity”, based onthe clinical experience according towhich the patient should subse-quently develop a larger inhalation.Newman et al. (10) showed that thebronchodilator response is reducedif the inhalation starts from 80%instead of 20% of Vital Capacity(VC). These findings are in accor-dance with a scintigraphic study(11) demonstrating that the aver-age lung drug deposition is 10% ofthe delivered dose with an inhala-tion at 20% of VC, but only 7% or6% with an inhalation at 50% or80% of VC, respectively. It may beestimated that an inspiratory vol-ume of approximately 1.5 liter isenough for optimum drug lung de-livery (11). Obviously, the inhala-tion starting point is more criticalfor subjects with low lung volumes,such as children or elderly peoplewith severe airway obstruction,rather than healthy individuals. Itis well known that exhalationshould be gentle because an abruptact may cause bronchoconstrictionin some patients.
04-melani:melani 7-01-2015 8:10 Pagina 113

eRn
114
DPI. Differently from pMDIs,when using a DPI it is important toexhale away from the mouthpieceafter loading the dose. This avoidsto blow the powder away or tomake the powder moist. It has beenshown that exhalation into the de-vice may reduce the effect of thebronchodilator (12). Importantly,
this error is very common accord-ing to a review that evaluates theincorrect use of DPIs (13). Somenewer DPIs, such as Genuair® andNEXThaler®, may attenuate theexhalation through the mouth-piece, even if this is currently un-der evaluation.
Table 1 - Step-by-step instruction checklists for the pressurised MDI
Checklist of steps
GINA checklist ERS/ISAM checklist
Remove cap and shake inhaler Shake four or five times if suspension formulation
Breathe out gently Take the cap off
Put mouthpiece in mouth and at start of inspiration, Prime the inhalerwhich should be slow and deep, press canister downand continue to inhale deeply
Hold breath for 10 seconds, or as long as possible Exhale slowly, as far as comfortable to empty the lungsthen breathe out slowly
Wait for a few seconds before repeating steps 2-4 Hold the inhaler in upright position
Place the inhaler in the mouth between the teeth, with thetongue flat under the mouthpiece. Ensure that the lips haveformed a good seal with the mouthpiece
Start to inhaler slowly, through the mouth, and at the sametime press the canister to actuate a dose
Maintain a slow and deep inhalation, though the mouth,until the lungs are full of air. This should take 4-5 sec inan adult
At the end of inhalation, take the inhaler out of the mouthand close the lips
Continue to hold the breath for as long as possible, orup to 10 sec before breathing out
Breathe normally
If another dose is required, repeat steps 4-11
04-melani:melani 7-01-2015 8:10 Pagina 114

eRn
115
Table 2 - Step-by-step instruction checklists for Diskus®, one of the most commonly used multi-dose DPIs
National AsthmaCouncil AustraliaChecklist
Open using thumb grip
Holding horizontally,load dose by slidinglever until it clicks
Breathe out gentlyaway from mouthpiece
Place mouthpiece inmouth and seal lips
Breathe in steadily anddeeply
Hold breath for about10 seconds or as longas comfortable
GINA checklist
Hold the outer casing in onehand whilst pushing thethumb grip away until a clickis heard
Hold the device withmouthpiece towards you,slide lever away until itclicks. This makes the doseavailable for inhalation andmoves the dose counter on
Hold the device on level,breathe out gently away fromthe device, put mouthpiece inmouth and suck in steadilyand deeply
Remove the device frommouth and hold breath forabout 10 sec
To close, slide thumb gripback towards you as far as itwill go until it clicks
For a second dose repeatsections 1-5
Manufacturer checklist
Hold the device in one handand put the thumb of yourother hand on the thumbgrip.Push your thumb away fromyou as far as it will go untilthe mouthpiece appears andsnaps into position.
Hold the device in a level,horizontal position with themouthpiece towards you.
Slide the lever away from youas far as it will go until itclicks
Before inhaling your dose,breathe out as far as iscomfortable, holding thedevice on level and awayfrom your mouth.
Put the mouthpiece to yourlips. Breathe in quickly anddeeply through the device,not through your nose.
Remove the device from yourmouth. Hold your breath forabout 10 seconds, or for aslong as is comfortable.
ERS/ISAM Checklist
Take (or rotate) the cap off
Follow the dose preparationinstructions
Do not point the mouthpiecedownwards once a dose hasbeen prepared for inhalationbecause the dose could fallout
Exhale slowly, as far ascomfortable (to empty thelungs). Do not exhale into thedevice
Start to inhale forcefullythrough the mouth from thevery beginning. Do notgradually build up the speedof inhalation
Continue inhaling until thelungs are full
(continued)
04-melani:melani 7-01-2015 8:10 Pagina 115
eRn
116
Preparation of the dose
MDI. Currently available MDIshave an external form still similarto the first models marketed in theSixties. However, MDIs havechanged very much; the mostknown variation occurred whenchlorofluorocarbon (CFC)-propel-lants were considered harmful tothe environment and for this rea-son they were phased out. With the
ban of CFCs, MDIs were reformu-lated using hydrofluoroalkane(HFA)-propellants. While all theCFC-MDIs were available as sus-pensions, some of the HFA-MDIshave been reformulated as solu-tions. Suspensions always requireto be shaken before use to makethe liquid homogeneous. It hasbeen shown (14) that if CFC-Ven-tolin® is not shaked, there is a re-duction of the total emitted dose
Table 2 - Step-by-step instruction checklists for Diskus®, one of the most commonly used multi-dose DPIs
National AsthmaCouncil AustraliaChecklist
While holding breath,remove inhaler frommouth
Breathe out gentlyaway from mouthpiece
If an extra dose isneeded, repeat steps 3to 9
Close cover to clickshut
GINA checklist Manufacturer checklist
Breathe out slowly.
Close the DIS when you arefinished taking a dose so thatthe DIS will be ready for youto take your next dose.
Put your thumb on thethumbgrip andslide the thumbgrip backtowards you as far as it willgo. The device will click shut.The lever will automaticallyreturn to its originalposition.
ERS/ISAM Checklist
At the end of the inhalationtake the inhaler out of themouth and close the lips.Continue to hold the breathfor as long as possible, or upto 10 sec
Breathe normally
If another dose is required,repeat steps 1–8
04-melani:melani 7-01-2015 8:10 Pagina 116
eRn
117
(TED) (-25%) and of the fine par-ticles dose (FPD) (-36%). This wasobserved also in an in vivo scinti-graphic study with CFC-budes-onide, where the major cause of re-duced lung deposition of the activedrug was the missed shaking (15).MDIs formulated as solutions donot require the medication to beshaken before use. On first use or ifit the device has not been used for
some days, manufacturers recom-mend to spray into the surroundingair from two to four doses (prim-ing) before using it (4). Patientsshould be encouraged by HCPs tofollow the priming recommenda-tions reported in the patient in-struction leaflet. Indeed, it hasbeen reported that less than aquarter of patients using MDIs ob-serve the priming process before
Table 3 - Step-by-step instruction checklists for HandiHaler®, one of the most commonly used mono-dose DPIs
National Asthma Council Australia checklist Manufacturer checklist
Open cap Open the device. Separate only one of the blisters from thecard; the open the blister
Open mouthpiece Insert the capsule containing the powder and close themouthpiece firmly against the gray base until you heara click
Remove capsule from blister and place in chamber Press the green piercing button once until it is flat againstthe base, then release
Close mouthpiece until it clicks Breathe out completely. Then breathe in deeply until yourlungs are full. You should hear or feel the capsule vibrate(rattle)
Press green piercing button in once and release Inhale twice from the same capsule, if you want to takeyour full daily dose
Breathe out gently away from mouthpiecePut mouthpiece between teeth without biting and closelips to form good seal
Breathe in slowly and deeply, so capsule vibrates
Continue to breathe in as long as comfortable
While holding breath, remove inhaler from mouth
Breathe out gently away from mouthpiece
Open mouthpiece and remove used capsule
If an extra dose is needed, repeat steps 3 to 12
Close mouthpiece and cap
04-melani:melani 7-01-2015 8:10 Pagina 117

eRn
118
use of the inhaler (16). The lack ofpriming may significantly reducethe first dose of the released drug(17). It is reported that primingmay have less importance with ex-trafine HFA-MDIs (18), but moredetailed information is lacking.Many MDIs have a dose counter. Indevices without a dose counter, it isimportant to count the sprayeddoses as many MDIs allow to re-lease a greater number of actua-tions than reported on the label.Unfortunately, after this limit, ac-curacy in the drug dose is not as-sured and this phenomenon iscalled “tail-off”. Ogren et al. (16)reported that only 8% of their pa-tients counted the doses deliveredby their MDI, while, almost 80%decided to throw away the inhaleron the basis of visual or gustatoryfeelings.DPI. The loading of a dose is dif-ferent (and often largely different)according to the used DPI. Twomajor types of DPIs are available:i) multi-dose systems, where moredoses of active drug are containedin the same device; and ii) single-or mono-dose devices where dosesare separated in sealed packages(4). The way of preparing a dose isdescribed in the patient instructionleaflet. To improve inhaler usabili-ty, manufacturers have successfullyreduced the number of steps re-quired for effective loading in new-er multi-dose DPIs, such as NEX-Thaler® (19). Some DPIs may pre-sent additional difficulties concern-ing the need of maintaining the de-
vice with the greater axis arrangedvertically during loading (2). How-ever, not all the instruction check-lists fully describe if loading and/orinhalation have to be performed ina forced position (4).All multi-dose DPIs have countingsystems. Manufacturers are im-proving these counters in order topermit an easy check of the resid-ual doses, even in subjects with vi-sual impairments.
Position of the user immediatelybefore and during inhalation
It is advisable that the subject hasto stay comfortable during prepa-ration and inhalation of the drugdose. It is generally ruled out that aslight tilting to the back of the head(about 60° on the horizontal plane)can have a significant role at thetime of delivery (20). Some check-lists previously recommended it ac-cording to the hypothesis thatmaking the aerosol path as linearas possible could improve lungdrug deposition.MDI. Traditionally, it was suggest-ed that the inhaler mouthpieceshould be placed 2-4 cm in front ofthe open mouth towards the phar-ynx when the aerosol is deliveredwith MDIs. Dolovich et al. suggest-ed this step for a better evaporationof the propellant in order to reducethe aerosol particle size and conse-quently the impact in the large air-ways (21). With the availability ofsofter aerosols, the open-mouth
04-melani:melani 7-01-2015 8:10 Pagina 118

eRn
119
technique is no more advisable.Most leaflets currently support theclose-mouth technique, but not allavailable pMDIs have soft aerosols.Possibly, the open-mouth tech-nique might predispose the aerosolto false pathways. Patients also de-liver the aerosol into the nostrils,the chest or the neck, rather thaninto the mouth, as it is anecdotallyreported. Dr. House seems to havebeen a witness of this practice (22).DPI. Placing the mouthpiece be-tween teeth and lips immediatelybefore inhaling is mandatory for allDPIs. A tight seal between the lipsand the mouthpiece avoids airleakage that would otherwise re-duce the inspiratory flow rate dur-ing inhalation.
Inhalation of the dose
Inhaling through the mouth, andnot the nose, is advisable with alldevices as the nose acts as a filter.Nasal inhalation reduces the lungdrug deposition by 40-50% ormore compared to oral inspiration(23-24).MDI. Most MDIs require to activatethe aerosol by pressing the canisterdownwards into the case. The opti-mal timing of aerosol delivery is thefirst half of a slow inhalation. Poorhand-lung coordination is possiblythe most typical error with pMDIs(2) and it may reduce or abolishlung drug delivery. In a seminalscintigraphic study, it has beenshown (25) that lung drug deposi-
tion was abolished only when theaerosol delivery occurred at least 3seconds before starting the inhala-tion and after having reached TotalLung Capacity (TLC). Add-onspacers can be associated to MDIsand usefully overcome the problemof poor hand-lung coordination. Al-though misuse is also reported forMDIs with add-on spacers, it isknown that their use may reducethe risk of errors in subjects withpoor MDI technique (2). The mostuseful spacers are the Valved Hold-ing Chambers (VHCs) that haveunidirectional valves permitting therelease of an aerosol only when thepatient is inhaling. There are a va-riety of different spacers that differconsiderably in shape, size, use,maintenance and performances (4).However, the use of spacers is notcurrently increasing despite thepersistently high rate of MDI mis-use. Probably they are not well ac-cepted by physicians and patients,because they are cumbersome. Pos-sibly, novel extrafine MDI formula-tions, characterized by smalleraerosol particle size, might reducethe relevance of incorrect hand-lung coordination, compared to tra-ditional MDI products (4). The av-erage lung deposition of an ex-trafine BDP formulation was 59%of ex-actuator dose with optimaldelivering, 50% if the inhaler wasactuated later (in the second half ofa 3-sec inspiration), and 37% whenthe inhaler was actuated 0.5 sec be-fore the inhalation (26). Currentlyavailable extra-fine products in-
04-melani:melani 7-01-2015 8:10 Pagina 119

eRn
120
clude Beclomethasone Dipropionate(BDP)Ò, cicloesonide, flunisolideand the corticosteroid/Long-Actingb2-Agonist BDP/formoterol Mod-ulite® combination.Inhalation of the dose has to beslow and it should last 5-sec in anadult (4). In a seminal study, thepercentage of metered dose in thelungs was 14% with slow inhala-tion vs. 7% with fast inhalation(25). Fast inhalation is not indicat-ed with pMDIs, because it increas-es the speed of inhaled particleswith a greater chance of depositionin the upper airways. This errormight have less relevance with ex-trafine aerosols (27).It is known that once started, theinhalation should be completedwithout stopping up to total pul-monary capacity. The abrupt inter-ruption of the inhalation that oc-curs when the aerosol reaches thepharynx is named cold Freon ef-fect. This is related to the aerosolimpact force and temperature atthe patient’s throat. The greater theforce, the lower the temperature ofaerosol is and the more commonthe risk of the cold Freon effect isbelieved to be. It is reported thatthe maximum impact force and theminimum plume temperature ofHFA-BDP and an of old CFC-BDPformulation are 34 mNewtons and+4°C vs. 100 mN and -28°C, re-spectively (28). These results sug-gest that newer pMDIs with softerand warmer aerosol might reducethe risk of cold Freon effect. How-ever, HFA-propellant sprays do not
necessarily have warmer and softeraerosols. For instance, althoughboth formulations contains salbu-tamol as an active drug and are us-ing HFA-propellants, the maxi-mum impact force and the mini-mum plume temperature were re-spectively 30 mN and +8°C forProventil® and 76 mN and -36°Cfor Ventolin® (29). Again, themean minimum plume tempera-ture for fluticasone Evohaler® 250was -51°C at 20 mm from themouthpiece (30).If an extra dose is needed, an inter-val of a few tenths of a second be-tween actuations is required. Mul-tiple actuations without waitingbetween doses are possible only us-ing MDIs. More puffs deliveredduring the same inhalation reducethe percentage of fine particlesfraction (FPF) by about 16% (31).DPI. Poor hand-lung coordinationcannot occur with DPIs that arebreath-actuated. This may havesupported the false view that DPIswere necessarily easy-to-use. Un-fortunately, DPI misuse is commonin real life (2). Inhaling forcefullyis critical for all DPIs, because itensures de-aggregation of the dose.Each DPI has a minimally effectiveinhalation flow required for itsfunction. Likewise, the inhalationflow varies according to the inhalerresistance. Each DPI has a specificinhaler resistance, ranging from0.04 to 0.18 cmH2O1/2/L/min.Aerolizer®, Breezhaler®, Diskus®,Genuair®, Turbohaler® andHandiHaler® have a progressively
04-melani:melani 7-01-2015 8:10 Pagina 120

eRn
121
increasing resistance (32-33). It islargely demonstrated that failure toforcefully inhale results in partialor no delivery of the medication tothe lungs. Importantly, in real life,only a minority of subjects with in-adequate inspiratory flow througha certain DPI are unable to obtaina proper drug lung delivery afterappropriate training (34). We sus-pect that the somewhat ambiguousterms used in some instructionchecklist (“breathe in slowly anddeeply”, or “breath in deeply”, or“breath in steadily and deeply”)may have contributed to the highrates of this error in clinical prac-tice. The ERS/ISAM task force op-portunely stated the need of aforceful inspiration through the de-vice from the beginning of inhala-tion (4). There are concerns aboutthe use of DPIs, mainly for high-re-sistance devices, in pre-schoolingchildren and elderly patients withsevere respiratory diseases. Howev-er, DPIs are generally not advocat-ed for children under the age of 6years. Some portable instruments,such as the InCheck Dial®, canmeasure the peak inspiratory flowaccording to the specific resistanceof the chosen inhaler and reassurethe clinician about the choice of theDPI for a given patient. It is impor-tant to stress the need of forcefulinspiration from the beginning ofinhalation, as most of the drugdose is emitted in the first part ofthe inhalation manoeuvre (35).Some novel DPIs, such as Genu-air® and NEXThaler®, have a
breath actuated mechanism (BAM)able to overcome the problem ofinitially slow inhalation as theshutter is opened only when theminimally effective flow isachieved. Another unclear point re-garding inhalation with mono-doseDPIs is the significance of the rec-ommendation that each doseshould be inhaled twice (4). In reallife, most subjects do not inhaletwice using mono-dose DPIs (2).Likewise, it has been reported thatinhaling through the HandiHaler®only once and not with two sepa-rate inhalations determines a sig-nificant residual dose in the device(36). Because many patients can-not perceive whether they are in-haling their dose effectively, manu-facturers are adding one or moreinteresting feedback systems usefulto the patient.
Post-inspiratory breath-holdingand exhalation
MDI. Breath-holding for at least10 sec or as long as possible afterthe inhalation is included in manychecklists of MDI use. Newman etal. have shown that a post-inspira-tory breath-holding may signifi-cantly improve the bronchodilatorefficacy of CFC-terbutaline; a 10-second pause is more advantageousthan 4 seconds, while prolongingthe breath-holding to 20 secondsdoes not give additional improve-ment (11). Possibly, the value ofthe post-inspiratory pause has
04-melani:melani 7-01-2015 8:10 Pagina 121

eRn
122
greater significance when the in-halation is fast (10) and with ex-trafine aerosols.DPI. It is thought that lung deposi-tion increases with longer residencetime even with DPIs. However,there is evidence about a signifi-cant role of breath-holding withDPIs (37), and other authors (38-39) reported no advantages with a10-sec. breath-holding. Not allDPIs instruction checklists suggestbreath-holding, that is always ad-visable with MDIs.Exhaling towards the mouthpieceafter inhalation has an un-favourable effect when a same dosehas to be inhaled twice or withmulti-dose reservoir-type DPIs, iftwo doses are prescribed.
Maintenance and storage ofdevices after using
A classical advantage of inhalers isthat they do not require particularmaintenance. By contrast, add-onspacers require regular mainte-nance with differences in terms ofhow and how often they have to becleaned (4). However, each prod-uct provides proper cleaning in-structions in its patient informationleaflet.Possibly, subjects are using andstoring their device in a range ofenvironments and conditions.Manufacturers recommend that in-halers should not be stored at tem-peratures above 30 °C. Some new-er MDIs have to be discarded 12
weeks after pharmacy dispensing.Regulatory agencies require thatinhalers should be tested for phar-maceutical stability over 3 monthsat 25 °C and 60% relative humidi-ty (RH) and for 1-month stabilityat 40 °C and 75% RH. Some pre-liminary findings (18, 40) accord-ing to which extrafine MDIs areless influenced from environmentalconditions than traditional sprayformulations, needs further confir-mation. Traditionally, multi-dosereservoir-type DPIs are consideredto be prone to influence un-favourable environmental condi-tions. Conditions of high tempera-ture and humidity have beenshown in in vitro studies to nega-tively affect the efficacy of the Tur-buhaler® (41). It was also foundthat FPD was largely reduced whenthe Turbuhaler® was used at 5 °C(42). However, another studyshowed that the FPF from theDiskus® was shown to be reducedby 50% after 3 months of storageat high temperature and humidity(43).
Conclusions
Manufacturers, according to regu-latory agencies, defined standard-ized requirements in terms of thequantity, quality and variability inthe emitted doses from inhalers, toensure consistent dosing boththroughout the entire life of an in-dividual device and from differentsamples of the same device. As
04-melani:melani 7-01-2015 8:10 Pagina 122
eRn
123
proper inhaler use is one of themain challenges, it would also beimportant that manufacturers de-fine standards with exhaustive ex-planations about the instructions ofthe inhaler technique. There is the
need of matching manufacturers’instructions for a particular devicewith the knowledge of health caregivers and patients.
eRn
References
1. Dolovich MB, Ahrens RC, Hess DR, etal. Device selection and outcomes ofaerosol therapy: evidence-based guide-lines. Chest 2005; 127: 335-71.
2. Melani AS, Bonavia M, Cilenti V, et al.Inhaler mishandling remains commonin real life and is associated with re-duced disease control. Respir Med2011; 105: 930-8.
3. Sestini P, Cappiello V, Aliani M, et al,on behalf of the Associazione ItalianaPneumologi Ospedalieri (AIPO) Edu-cational Group. Prescription bias andfactors associated to improper uso ofinhaler. J Aerosol Med 2006; 19: 127-36.
4. Laube BL, Janssens HM, de Jongh FH,et al. What the pulmonary specialistshould know about the new inhalationtherapies. ERJ 2011; 37 (6): 1308-31.
5. How to use a metered-dose inhaler (GI-NA). Available at: http://www.ginasthma.org/local/uploads/content/files/inhaler_charts_2011.pdf. Last ac-cessed 12 April 2014.
6. How to use the Accuhaler/Diskus, GI-NA. Available at: http://www.ginasthma.org/local/uploads/files/accuhaler.pdf Last accessed 12 April 2014.
7. Inhaler technique in adults with asthmaor COPD. National Asthma Council ofAustralia. Available at: http://www.nationalasthma.org.au/uploads/publication/inhaler-technique-in-adults-with-asthma-or-copd.pdf. Last ac-cessed 12 April 2014.
8. Manufacturers instructions for Advair-Diskus, GSK. Available at: https://www.gsksource.com/gskprm/htdocs/do
cuments/ADVAIR-DISKUS-PI-MG.PDF. Last accessed 12 April 2014
9. How to use Spiriva. Boehringer Ingel-heim. Available at: https://www.spiriva.com/assets/pdf/SPIRIVA_HandiHaler_Instructions.pdf. Last accessed 12April 2014.
10. Newman SP, Pavia D, Clarke SW. Sim-ple instructions for using pressurizedaerosol bronchodilators. J R Soc Med1980; 73: 776-9.
11. Newman SP, Pavia D, Clarke SW. Howshould a pressurized beta-adrenergicbronchodilator be inhaled? Eur J RespirDis 1981; 62: 3-21.
12. Engel T, Scharling B, Skovsted B,Heinig JH. Effects, side effects andplasma concentrations of terbutaline inadult asthmatics after inhaling from adry powder inhaler device at differentinhalation flows and volumes. Br J ClinPharmacol 1992; 33: 439-44.
13. Lavorini F, Magnan A, Dubus JC, et al.Effect of incorrect use of dry powder in-halers on management of patients withasthma and COPD. Respir Med 2008;102(4): 593-604.
14. Everard ML, Devadason SG, SummersQA, LeSouëf PN. Factors affecting totaland respirable dose delivered by asalbutamol metered dose inhaler. Tho-rax 1995; 50: 746-9.
15. Thorsson L, Edsbäcker S. Lung deposi-tion of budesonide from a pressurizedmetered dose inhaler attached to a spac-er. Eur Respir J 1998; 12: 1340-5.
16. Ogren RA, Baldwin JL, Simon RA. Howpatients determine when to replace theirmetered-dose inhalers. Ann Allergy Asth-ma Immunol 1995;75 part 1: 485-9.
17. Cyr TD, Graham SJ, Li RKY, Lovering
EG. Low first-spray drug content in al-buterol metered-dose inhalers. PharmRes 1991; 8: 658-60.
18. Nave R, Mueller H. From inhaler tolung: clinical implications of the formu-lations of ciclesonide and other inhaledcorticosteroids. Int J Gen Med 2013; 6:99-107.
19. Voshaar T, Spinola M, Linnane P, et al.Comparing usability of NEXThaler®with other inhaled Corticosteroid/Long-Acting β2-Agonist fixed combinationDry Powder Inhalers in asthma pa-tients. J Aerosol Med Pulm Drug DelivDecember 3 2013; doi.
20. Pedersen S. Optimal use of tube spaceraerosols in asthmatic children. Clin Al-lergy 1985; 15: 473-478.
21. Dolovich M, Ruffin RE, Roberts R,Newhouse MT. Optimal delivery ofaerosols from metered dose inhalers.Chest 1981; 80: Suppl.6: 911-5.
22. Dr. House asthma inhaler. YouTube.Available at: http://www.youtube.com/watch?v=zG2DVoRP86g. Last accessed12 April 2014.
23. Everard ML, Hardy JG, Milner AD.Comparison of nebulised aerosol depo-sition in the lungs of healthy adults fol-lowing oral and nasal inhalation. Tho-rax 1993; 48: 1045-6.
24. Chua HL, Collis GG, Newbury AM, etal. The influence of age on aerosol de-position in children with cystic fibrosis.Eur Respir J 1994; 7: 2185-91.
25. Newman SP, Pavia D, Garland N,Clarke SW. Effects of various inhalationmodes on the deposition of radioactivepressurized aerosols. Eur Respir J Dis1982; 63:Suppl.119: 57-65.
26. Leach CL, Davidson PJ, Hasselquist
04-melani:melani 7-01-2015 8:10 Pagina 123

eRn
124
Andrea Melani is a pulmonologist working in the University Hospital SantaMaria alle Scotte, in Siena, Italy. His primary research interests cover aerosoltherapy, COPD, asthma, respiratory infections, tobacco-related diseases andsmoking cessation methods, sleep-respiratory disturbances.He contributes to various medical committees and is a member of the Associ-azione Italiana Pneumologi Ospedalieri (AIPO), where he has served as Secre-tary of the Educational Group from 2002 to 2004 and as responsible from2010 to 2012. He is the coordinator of the local anti-smoking center and theRespiratory Rehabilitation and Sleep disturbance Service. He served as coor-dinator of domiciliary respiratory assistance to patients with chronic respira-tory failure in the Siena district. He has published over 100 articles pertinentto pulmonology in a range of peer-reviewed medical journals and served as re-viewer in a variety of international journals
BE, Boudreau RJ. Influence of particlesize and patient dosing technique onlung deposition of HFA-beclomethasonefrom a metered dose inhaler. J AerosolMed 2005; 18: 379-85,
27. Usmani OS, Biddiscombe MF, BarnesPJ. Regional lung deposition and bron-chodilator response as a function of β2-agonist particle size. Am J Respir CritCare Med 172: 1497-504.
28. Gabrio BJ, Stein SW, Velasquez DJ. Anew method to evaluate plume charac-teristics of hydrofluoroalkane and chlo-rofluorocarbon metered dose inhalers.Int J Pharm 1999; 186: 3-12.
29. McCabe JC, Koppenhagen F, Blair J,Zeng X-M. ProAir® HFA deliverswarmer, lower-impact, longer-durationplumes containing higher fine particledose than Ventolin® HFA. J AerosolMed Pulm Drug Deliv 2012; 25(2):104-9.
30. Brambilla G, Church T, Lewis D,Meakin B. Plume temperature emittedfrom metered dose inhalers. Int J Pharm2011; 405: 9-15.
31. Barry PW, O’Callaghan C. A compara-tive analysis of the particle size outputof beclomethasone dipropionate, salme-terol xinafoate and fluticasone propi-onate metered dose inhalers used withthe Babyhaler, Volumatic and Ae-rochamber spacer devices. Br J ClinPharmacol 1999; 47: 357-60.
32. Clark AR, Hollingworth AM. The rela-tionship between powder inhaler resis-tance and peak inspiratory conditions inhealthy volunteers: implications for invitro testing. J Aerosol Med 1993; 6: 99-110.
33. Melani AS. Focus su Breezhaler per iltrattamento della BPCO. Rassegna diPatologia dell'Apparato Respiratorio2013; 28: 135-41.
34. Melani AS, Bracci LS, Rossi M. Reducedpeak inspiratory effort through theDiskus® and the Turbuhaler® due tomishandling is common in clinical prac-tice. Clin Drug Invest 2005; 25 (8):543-9.
35. Everard ML, Devadason SG, Le SouëfPN. Flow early in the inspiratory ma-noeuvre affects the aerosol particle sizedistribution from a Turbuhaler. RespirMed 1997; 91: 624-8.
36. Al-Fadhi SA, Assi KH, Clark BJ,Chrystyn H. Tiotropium dose emissionis influenced by the inhalation flow andthe recommended two inhalations foreach dose. Eur Respir J 2005; 26 (Sup-pl. 49): 125s–6.
37. Auty RM, Brown K, Neale MG, SnashallPD. Respiratory tract deposition ofsodium cromoglycate is highly depen-dent upon technique of inhalation usingthe Spinhaler. Br J Dis Chest 1987; 81:371-80.
38. Pedersen S, Steffensen G. Fenoterol
powder inhalation technique in chil-dren: influence of inspiratory flow rateand breath-holding. Eur J Respir Dis1986; 68: 207-14.
39. Pitcairn GR, Lim J, Hollingworth A,Newman SP. Scintigraphic assessmentof drug delivery for the Ultrahaler DryPowder Inhaler. J Aerosol Med 1997;10: 295-306.
40. Shemirani FM, Hoe S, Lewis D, ChurchT, Vehring R, Finlay WH. In vitro inves-tigation of the effect of ambient humid-ity on regional delivered dose with solu-tion and suspension MDIs. J AerosolMed Pulm Drug Deliv 2013; 26(4):215-22.
41. Lindsay DA, Russell NL, Thompson JE,Warnock TH, Shellshear ID,Buchananet PR. A multicentre compar-ison of the efficacy of terbutaline tur-buhaler and salbutamol pressurizedmetered dose inhaler in hot, humid re-gions. Eur Respir J 1994; 7: 342–5.
42. Meakin BJ, Cainey JM, Woodcock PM.Simulated ‘in-use’ and ‘mis-use’ aspectsof the delivery of terbutaline sulphatefrom Bricanyl Turbohaler™ dry powderinhalers. Int J Pharm 1995; 119: 103-8.
43. Borgström L. An in vivo and in vitrocomparison of two powder inhalers fol-lowing storage at hot/humid conditions.J Aerosol Med 2005; 18: 304-10.
04-melani:melani 7-01-2015 8:10 Pagina 124

eRn
125
The 24th ERS International Con-gress took place in Munich on Sep-tember 6th-10th led by Oliver Eickel-berg and Jürgen Behr as localchairs and under Peter Barnes’Presidency. This year’s Congresssaw the launch of the HealthyLungs for Life campaign, with thetheme Breathe Clean Air. Thelong-term awareness campaignaimed to focus on prevention andpublic education, to try and reducethe burden of lung disease on soci-ety and in the face of climatechange, a move to make our meet-ing “greener”. At a time when theworld is facing considerable eco-nomic and security challenges, thisyears’ event was a great successwith almost 22,000 registrants anda programme designed to cater forall the many needs of different pro-fessionals, patient and carers andindustry. As Chair of the ScientificProgramme Committee, it has beenmy responsibility to continue tostrengthen the Congress in linewith the new directions agreed bythe ERS Executive and Council ata Leadership Strategy Meeting heldin Lausanne on July 3rd-4th 2013(1). In reviewing how far we havemet these new ERS developments,
I will outline briefly how the pro-gramme for Munich has now ma-tured to a point where the ERS isconsidered to be the internationalcongress that respiratory profes-sionals must attend.In line with the ERS Strategic Plan(1), the Congress attracted thegreatest number of paid registrantsoutside Europe than any previousERS or other respiratory meeting.This was in a large part becausethe programme addressed interna-tional problems with speakers andchairpersons from all over theworld. Topics such as drug-resis-tant TB, biomass-related air pollu-tion, occupational lung disease andthe devastating consequences oftear gas to control civil unrest aswell as major sessions on COPDand asthma in different countriesprovided the clear conclusion thatthe ERS is now clearly internation-al. The successful Spanish session,which was held for the first time atlast years’ Congress in Barcelona,was repeated on the Saturday, andthis year we also had a “Chinaday” which was attended by over200 delegates. Paired presentationswere given by Chinese and Euro-pean speakers and all the Power-
Highlights of the 24th ERSInternational Congress, Munich:onwards and upwards
ERS
Europ. Respir. News XXII (85): 125-129, 2014
Stephen T. HolgateFERS, Chair, ERS Science Counciland Scientific Programme Committee
Correspondence to:Stephen T. Holgate,Clinical and Experimental SciencesLevel F, South BlockSouthampton General HospitalSouthampton, S6YD, UKE-mail: [email protected]
05-holgate:holgate 7-01-2015 8:12 Pagina 125

eRn
126
Point slides were shown both inEnglish and Chinese. I can see fur-ther attempts to cross cultural andlanguage barriers in the future. Forexample, there are early discus-sions on a possible Russia day atnext years’ Congress.The outcomes of the ERS ScientificStrategy meeting in April 2013 em-phasised the key role of science (ba-sic, translational and clinical re-search) as a major pillar of theERS. The Programme Committee,which included enormous inputfrom the 11 ERS Assembly Leader-ship, worked hard to try to embedmore science in the different sym-posia and other sessions. The ideawas to provide greater scientific un-derpinning of clinical and health-related sessions. I do believe this ex-tra effort improved the quality ofthe overall Congress enabling a rea-son for greater interactions betweenbasic and clinical scientists andhealth practitioners. As our special-ity takes on the more complex man-tles of stratified medicine, greaterunderstanding of the early life ori-gins of disease and its evolutionover the life course, then embracingthe new science offered by technol-ogy (the ‘omics), informatics anddeep phenotyping will be essentialif the emergence of greater diagnos-tic, preventative and therapeuticunderstanding is to occur as em-phasised by the recent ERS Presi-dent’s Summit in Rome (2).An equally important task is tomove new knowledge coming fromresearch into practice for patient
benefit. This means the science as-pect of the Congress working moreclosely with the Educational Coun-cil. Again, real attempts were madein Munich to explore those emerg-ing fields where getting researchinto practice is ripe. There weremany sessions where this interfaceworked especially well such as therole of psychology in asthma man-agement, how to deal with antimi-crobial resistance (in TB manage-ment and the adoption of molecu-lar diagnostics for stratifying lungcancer). The inclusion of thespirometry training programme,championship sessions, patient fo-rums, postgraduate courses, meetthe expert sessions, morning ses-sions and the increasingly populareducational skill workshops creat-ed a terrific learning environmentfor delegates to become more fa-miliar with new approaches, tech-nologies and care pathways. Oneexample of an innovative sessionwas a Patient Forum on non-inva-sive ventilation that included inputfrom both a patient and profession-al, offering an insightful user per-spective. All these sessions werevery well attended and greatly con-tributed to the unique success ofthe Congress. Once again, the Con-gress enabled the staging of a Har-monised Education in RespiratoryMedicine for European Specialists(HERMES) examination whichcontinues to prove very popular.This year we have also strength-ened the role played by our JuniorMembers. A very popular session
05-holgate:holgate 7-01-2015 8:12 Pagina 126

eRn
127
was the Fellows Get Together or-ganised by Maria Belvisi, ResearchDirector in charge of Fellowshipsand Awards in close collaborationwith the Junior Members Commit-tee (JMC) and especially its formerChair, Indre Butiene. This attract-ed a large audience of early careerresearchers (Figure 1). The objec-tive of this session aimed to bringtogether researchers who wereawarded an ERS Fellowship be-tween 1997 and 2013, as well asexperts involved in reviewing ap-plications, so that they can com-municate their experience to any-one interested in applying for theERS Fellowship programmes in thefuture. The inspirational talks werefrom those who had benefited fromprevious ERS Fellowships as wellas current Fellows in training. Aspecial focus this year was on “Ca-reers for women in science” ledby Elisabeth Bel (now ERS Presi-
dent) and “Careers for scientists inindustry” presented by Gary An-derson (University of Melbourne),both of which were outstanding.The idea of this Saturday sessionand the Young Scientists Network-ing evening on the Tuesday of theCongress is to provide a valuableplatform for early career re-searchers who wish to interact withexperienced ERS Officers and toshare their experiences with otherjunior delegates.For the first time, we also organiseda session presenting the best of the12th Estoril 2014 Lung ScienceConference (LSC) Lung inflamma-tion and immunity organised bythe LSC Director, Bruno Crestaniand his very able LSC Committee.The LSC is an annual conferencetaking place in Estoril, Portugal,which is designed to create aunique environment in a congenialsetting for young and more experi-enced researchers to interact andcollaborate (3). It cannot be em-phasised enough that investing en-ergy, time and resources in early re-searchers’ career development isamong the most important tasksany professional society can deliver.I am delighted to report on allfronts this is occurring with an in-crease in clinical and non-clinicalresearch long- and short-term fel-lowships, research seminars, clini-cal research collaborations and theLung Science Conference. In addi-tion, we have developed a new fel-lowship scheme for those wishingto pursue research training from
Figure 1 - Faculty who contributedto the early career researchers ses-sion including from left to right: GuyJoos (ERS President 2016-17),Stephen Holgate (Chair ScienceCouncil), Maria Belvisi (ERS Re-search and Fellowships Director),Elizabeth Bel (ERS President 2014-15), past recipients of ERS Fellow-ships and Gary Anderson (Mel-bourne) and Guy Brusselle (Guide-lines Director)
>
05-holgate:holgate 7-01-2015 8:12 Pagina 127

eRn
128
low and middle income countries.An important part of the ERS is torecognise those who have made sig-nificant scientific achievements.Among these is the ERS MaurizioVignola Award for Innovation inPneumology. The award is a bestpublication award on the basicmechanisms in respiratory diseases.The award is dedicated to thememory of Professor A. MaurizioVignola for his outstanding contri-bution to the field of respiratorymedicine. The 2014 award thisyear was shared by Kristin West-phalen from Munich for a paper inNature - Sessile alveolarmacrophages communicate withalveolar epithelium (4) and KlausBønnelykke from Copenhagen pub-lished in Nature Genetics - Agenome-wide association studyidentifies CDH3 as a susceptibilitylocus for early childhood asthmawith severe exacerbations (5). Con-gratulations to them both. As aclose friend and colleague of Maur-izio before his untimely passingaway, I am sure he would havebeen proud to see the increase inbasic and translational science inthis years’ Congress as his own out-standing research contributionsshowed (6). Therefore, it is verypleasing to know that at our Con-gress next year in Amsterdam, theChiesi Foundation will be awardinga Gold Medal to the “best asthmaresearcher” worldwide whose ca-reer is on an ascending trajectory.Not only has there been greater fo-
cus on our younger members, but,as described in the strategic plan(1), a new highly competitive Fel-lowship of those more senior mem-bers who have made major contri-butions to respiratory science, edu-cation and practice has been intro-duced this year; Fellows of the Eu-ropean Respiratory Society(FERS). It is intended to have ayear-on-year rolling admissionprocess to build up these experi-enced and productive individualsand engaging their help in such ac-tivities as mentorship and horizonscanning.To conclude, the ERS is continuingto evolve and our annual Congress-es reflect this. It is the ScienceCouncil’s intention to further em-bed scientific understanding intothe ERS as a society and the nextCongress, as we further progressclinical and educational activitiesthat are the bedrock of our society.As we look forward to our Amster-dam Congress in 2015, there willbe further integration of high qual-ity science into the programme,closer working with the Education-al Council to facilitate researchtranslation and uptake into patientbenefit and drawing in new tech-nologies and disease areas outsideour own respiratory field where wecan learn more e.g. regenerativemedicine, aging, nutrition, envi-ronment.See you in Amsterdam (7)!
eRn
References
1. Migliori GB, Rabe KF, Bel E, Elliott M,Gaga M, Holgate ST, Joos G, BurriezaFM, Sax B, Sculier JP, Simonds AK,Blasi F, Barnes PJ. The European Res-piratory Society plans its future: the2013-2018 strategic plan. Eur Respir J2014; 43: 927-32.
2. Barnes PJ, Ward B, Barry M. Breakingdown barriers to lung health. LancetRespir Med 2014; 2: 687-9.
3. Crestani B, Pretolani M, Hammad H.Lung inflammation and immunity: re-port from the 12th ERS Lung ScienceConference. Eur Respir Rev 2014; 23:275-7.
4. Westphalen K, Gusarova GA, IslamMN, Subramanian M, Cohen TS,Prince AS, Bhattacharya J. Sessile alve-olar macrophages communicate withalveolar epithelium to modulate immu-nity. Nature 2014; 506: 503-6.
5. Bønnelykke K, Sleiman P, Nielsen K,Kreiner-Møller E, Mercader JM, Bel-grave D, den Dekker HT, Husby A,Sevelsted A, Faura-Tellez G, MortensenLJ, Paternoster L, Flaaten R, MølgaardA, Smart DE, Thomsen PF, RasmussenMA, Bonàs-Guarch S, Holst C, NohrEA, Yadav R, March ME, Blicher T,Lackie PM, Jaddoe VW, Simpson A,Holloway JW, Duijts L, Custovic A,Davies DE, Torrents D, Gupta R, Holle-gaard MV, Hougaard DM, HakonarsonH, Bisgaard H. A genome-wide associa-tion study identifies CDHR3 as a sus-ceptibility locus for early childhoodasthma with severe exacerbations. NatGenet 2014; 46: 51-5.
6. K.F. Rabe and P.J. Sterk. In memoriamMaurizio Vignola. Eur Respir J 2005;25: 775.
7. www.erscongress.org
05-holgate:holgate 7-01-2015 8:12 Pagina 128

eRn
129
Stephen Holgate, qualified in Medicine at Charing Cross Hospital Medical Schoolin 1971 and completed his postgraduate medical studies in Internal and Respira-tory Medicine at the London Postgraduate Hospitals and the then new medicalschool at the University of Southampton. His entry into research was through hisDM thesis entitled “ -agonist resistance in normal human airways”. In 1978 hewas awarded an MRC Travel Scholarship to study the cellular and mediatormechanisms of allergy and asthma under Dr K Frank Austen at the Women andBrigham Hospital and Harvard Medical School, Boston. On returning to the UKhe teamed up with Martin Church to establish a focus on asthma mechanisms witha strong translational element. He has utilized many approaches to study this dis-ease including epidemiology, genetics, pathology, microbiology and immunology,pharmacology and experimental medicine. This research has informed guidelineson asthma management and has identified and validated novel therapeutic tar-gets. Notable research contributions include the role of mast cells and their medi-ators in asthma and allied disorders, the regulation and pharmacology of mastcells, placing inflammation at the core of asthma pathophysiology, uncovering therole of respiratory viruses, allergens and pollutants in asthma exacerbation, thediscovery of defects in innate immune responses in asthmatic airways, mechanismsof airway wall remodelling and the discovery of novel asthma susceptibility genessuch as ADAM33. His current research focuses on stratified medicine, the role ofthe epithelium in orchestrating asthma and the evolution of asthma across the life-course. His work has resulted in over 980 peer reviewed publications (H index134), 60 Book editorships, 453 Book Chapters and Reviews, 48 Editorials, 76 Of-ficial and Government Reports. He holds an MRC programme grant focused on thepathogenesis of asthma. He is a Past President of the British Society of Allergy andClinical Immunology and British Thoracic Society, was Chair of the MRC Popu-lation and Systems Medicine Board (PSMB). Stephen is Chair of Main Panel A(Medicine, Health and Life Sciences) of the UK Research Excellence Framework2014, Chairs the UK National Centre for the Replacement, Refinement and Re-duction of Animals in Research (NC3Rs), the British Lung Foundation ResearchCommittee, the Hazardous Substances Advisory Committee (HSAC), and from2014, will join the Science and Innovation Strategy Board of the Natural Envi-ronment Research Council (NERC). He is chair of the MRC Translation ResearchGroup, member of MRC Strategy Board and member of the European RespiratorySociety Science Council, and Member of the Medical Science Committee of ScienceEurope. In 2003 he cofounded of Synairgen a publically quoted respiratory drugdevelopment company with a particular focus on lung antiviral defence in asthma,COPD and severe viral infections. His contributions have been recognised by anumber of awards including The King Faisal International Prize in Medicine, theBSACI William Frankland Medal for Allergy Services, the Paul Ehrlich Award bythe EAACI, the American Thoracic Society (ATS) Recognition Award for ScientificAccomplishments and the British Thoracic Society Medal. In 2011 he was ap-pointed Commander of the Order f the British Empire (CBE) in the Queen’s NewYear’s Honours list for services to Clinical Science.
05-holgate:holgate 7-01-2015 8:12 Pagina 129

eRn
130
When Prof. Olivieri asked me to write this article, I immediately consid-ered it as a good opportunity to make a mid-term evaluation of my man-date of ERS Secretary General.Just being freshly elected, in 2012 the ERS leadership (under the guide ofKlaus Rabe and Francesco Blasi) started discussing about the need of re-defining strategic objectives and developing a new plan for our society.To say the truth, in 2006-2007 a strategic document had been already de-veloped by ERS (1). Unfortunately, a section on implementation, moni-toring and evaluation was missing, leading to a sub-optimal impact of thedecisions taken. So the perceived issue, this time, was to develop a planwith a professional approach, as to ensure its future implementation aswell as its monitoring and evaluation.At present the senior leadership of ERS has a 3 year mandate, precededby one year of “training” in the respective function.As in other circumstances of my professional life I was immediately asked,during my ‘training’ year to develop the concept and content of the Lead-ership Retreat for the development of the new 2013-2108 ERS StrategicPlan together with Klaus Rabe and Fernando Martin. Klaus was supposedto chair, Fernando with the office support, to adapt the slides and theminutes with a “real time” approach. I was asked to moderate, in order toensure via a “draconian” management of the meeting, to end the 2 daysretreat with an approved plan and a draft Editorial ready for the ERJ. Wewanted, in fact, make ERS members aware of this important step forwardof the society via the scientific journal of the society. The ERS leadershipretreat was held on July 3rd and 4th, 2013 in Lausanne (Figure 1) (2).It was agreed to start for the three ERS Pillars, then developed by PeterBarnes in a Greek temple format (Figure 2), and from the mission to bet-ter serve its members and achieve its mission objectives (Table 1). The re-cently published ERS Presidential plans were also used as an operationalguide (2-5).The preparation was accurate. The approach was to encourage partici-pants to express their opinions freely and to think “out of the box” in or-der to bring fresh ideas to the table. Whilst the focus of the exercise wasdefinitely the future, the importance of the past as the basis of all change
Driving the implementation of theERS 2013-2018 Strategic plan
ERS
Europ. Respir. News XXII (85): 130-137, 2014
Giovanni Battista MiglioriWHO Collaborating Centre for TB andlung diseases, Fondazione S. Maugeri,Care and Research Institute, Tradate(Italy); ERS Secretary General Elect
Correspondence to:Giovanni Battista MiglioriWHO Collaborating Centre for Control ofTuberculosis and Lung Diseases,Fondazione Salvatore Maugeri,Care and Research Institute,via Roncaccio 16 - 21049 Tradate (VA), ItalyTel ++39. 0331. 829404Fax ++39. 0331. 829402E-mail:[email protected]
06-migliori:migliori 7-01-2015 8:13 Pagina 130

eRn
131
was emphasized by the presence of the former Executive Director who at-tended in an observer role to recall the history of the ERS and previousdecisions.
The agenda included 8 strategic areas for decision: 1) remaining Euro-pean or going global; 2) expanding membership; 3) coordinating withother societies; 4) strengthening science; 5) improving education; 6) im-proving publications; 7) coordinating and enhancing advocacy; 8) orga-nizational changes to put in practice the decisions taken.A specific business plan for implementation of the activities was devel-oped for each strategic area under the responsibility of the President andthe Secretary General together with the ERS Executive Director / ERS Of-fice, in alignment with the ERS budget process.
For the purpose of this article, I have recalled the 8 areas and summarisedin italic the main achievements so far.
06-migliori:migliori 7-01-2015 8:13 Pagina 131
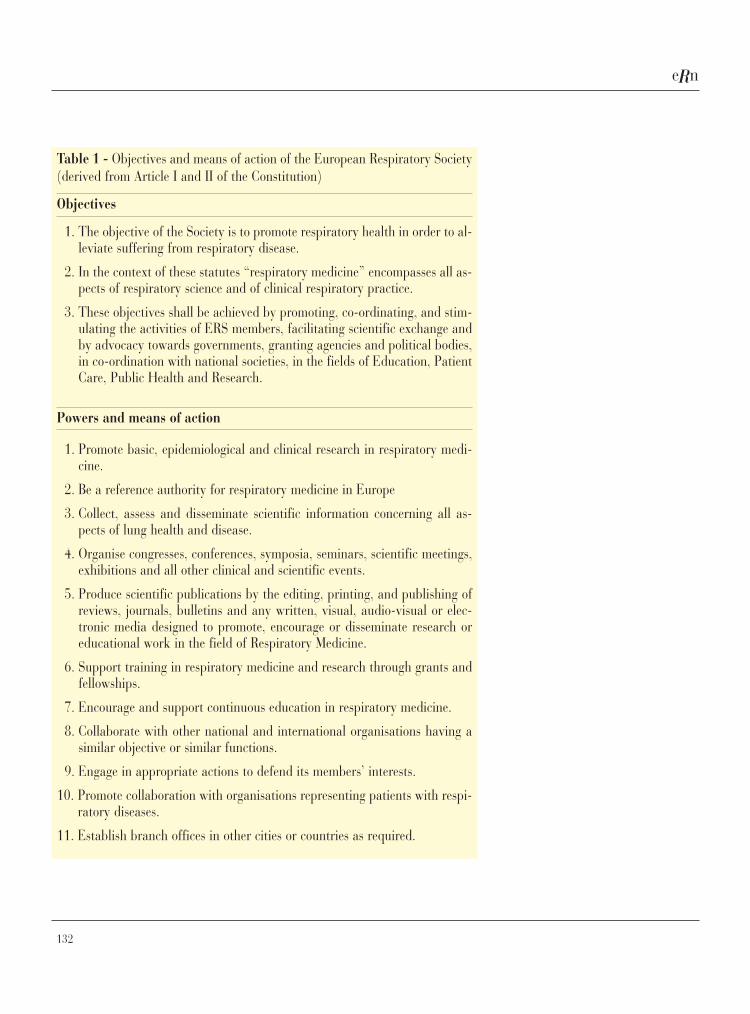
eRn
132
Table 1 - Objectives and means of action of the European Respiratory Society(derived from Article I and II of the Constitution)
Objectives
1. The objective of the Society is to promote respiratory health in order to al-leviate suffering from respiratory disease.
2. In the context of these statutes “respiratory medicine” encompasses all as-pects of respiratory science and of clinical respiratory practice.
3. These objectives shall be achieved by promoting, co-ordinating, and stim-ulating the activities of ERS members, facilitating scientific exchange andby advocacy towards governments, granting agencies and political bodies,in co-ordination with national societies, in the fields of Education, PatientCare, Public Health and Research.
Powers and means of action
1. Promote basic, epidemiological and clinical research in respiratory medi-cine.
2. Be a reference authority for respiratory medicine in Europe
3. Collect, assess and disseminate scientific information concerning all as-pects of lung health and disease.
4. Organise congresses, conferences, symposia, seminars, scientific meetings,exhibitions and all other clinical and scientific events.
5. Produce scientific publications by the editing, printing, and publishing ofreviews, journals, bulletins and any written, visual, audio-visual or elec-tronic media designed to promote, encourage or disseminate research oreducational work in the field of Respiratory Medicine.
6. Support training in respiratory medicine and research through grants andfellowships.
7. Encourage and support continuous education in respiratory medicine.
8. Collaborate with other national and international organisations having asimilar objective or similar functions.
9. Engage in appropriate actions to defend its members’ interests.
10. Promote collaboration with organisations representing patients with respi-ratory diseases.
11. Establish branch offices in other cities or countries as required.
06-migliori:migliori 7-01-2015 8:13 Pagina 132
eRn
133
Strategic Decision 1: remaining European or going global?
ERS has remained a European Society, with EU-centred activities, but isfurther developing to act as a “magnet” at the international/global level.This new approach is encouraging global participation in the ERS Con-gress because of its excellence and high level networking opportunities, aswell as the development of collaborative projects with Regional/ NationalRespiratory Societies through joint activities, which will empower them tobring the acquired knowledge to their respective countries. A new Inter-national Programme Committee was implemented to ensure proper repre-sentation of non-European speakers.
ERS is now a global organisation in view of the global relationship offi-cially established in Latin America, Asia and Africa. While expanding it-self, the architecture of the society needs to be modified to tackle the newchallenge. The name of the conference has been already modified into ERSInternational Conference. At the same time the EU activities have beenstrengthened, particularly on advocacy with several events organised atthe EU Parliament in Brussels on TB and COPD, and by creating bridgeswith the Russian speaking societies. This year in Munich we have launchedsuccessfully the China day (a full day in English and Chinese on Saturday,the day traditionally devoted to PG Courses). In Amsterdam 2015 ERS willorganise the China day, and also a full day in Spanish and Portuguese onSunday to further open to a multi-lingual and multi-cultural approach.
Strategic Decision 2: expanding membership
It was decided to initiate a new approach to all national and regional so-cieties to expand membership and lower the annual fee within the specif-ic agreements.The focus of this initiative was in generating contacts and interactionswith societies all over the world and not to generate revenues .The impactof moving from 10,000 to 100,000 members will be obvious, just consid-ering the benefits for the ERJ and the other ERS journals or the poten-tialities in terms of guidelines.Within this perspective the Fellowship of the ERS (FERS) project hasbeen launched to acknowledge outstanding contributions of ERS mem-bers to respiratory research, education and clinical practice.
ERS is in the process of signing agreement with the majority of Respirato-ry societies in and outside Europe. After signing with ALAT (the RegionalLatin American Society), the Spanish and Portuguese Society and the na-
06-migliori:migliori 7-01-2015 8:13 Pagina 133
eRn
134
tional respiratory societies in Latin America, ERS is presently discussingsimilar agreements in Asia (with APSR, the Asian Pacific Society) and inAfrica (with PATS, the Pan African Thoracic Society) while having intensecollaboration with ATS and the Canadian society. In January ERS will al-so sign the agreement with the SPLF, the respiratory society of Frenchspeaking countries which will include France, the French speaking Africa(north and west Africa) as well as Quebec and other countries in the fareast(Vietnam, Cambodia, etc). The number of members has increasedfrom the original 10,000 to about 40,000 in Munich. We expect to reachabout 70,000 members by Amsterdam.
Strategic Decision 3: coordinating with other societies
The ERS will strengthen links with other major national and internationalrespiratory societies as mentioned above. The management and governingarchitecture of the ERS will be revisited to capture the new challenges andto ensure special collaboration with the national respiratory societies.Collaboration with international organisations like the World Health Or-ganisation (WHO) and ECDC (European Centre for Diseases Control andprevention) has been valued, particularly in the area of science, educationand advocacy for respiratory health in tuberculosis and non communica-ble diseases.
ERS is presently developing a new database (achieved by merging the ex-isting databases), in collaboration with the different societies, in order tobetter serve its members. The first collaborative projects are under devel-opment in collaboration with ALAT. Two MoU (Memorandum of Under-standing) have been signed with WHO to cover the TB Consilium (5) anda special collaboration in Tuberculosis, while a second agreement is un-der discussion in the area of non-communicable diseases. A strict collab-oration is also ongoing with ECDC in the area of the European Standardsfor TB Care and Influenza. The new Assembly 10 Head, Stefano Alibertiis also coordinating with the Science Council a specific fellowship pro-gramme to be jointly organised with WHO and ECDC.
Strategic Decision 4: strengthening science
Strategic Decision 5: improving education
It was decided to support all aspects of science (basic, translational, clin-ical research) and integrate it better with educational activities.In addition a discussion started on the possibility to modify the ERS As-
06-migliori:migliori 7-01-2015 8:13 Pagina 134

eRn
135
sembly’s structure (according to a disease-specific pattern) and to launchan ERS Research Agency (which will coordinate and fund respiratory re-search across Europe)
The name and structure of the different committees has started changing.We have now the Science and the Education Council, which work in amuch more coordinated manner than in the past.The budget allocated for fellowships and grants (in particular for theCRC- Clinical Research Collaboration) has increased significantly.A special task force, guided by the Secretary General, is developing aWhite Paper for the Research Agency. The document will be discussed bythe leadership in January 2015 and by the Executive Committee in Aprilat the Spring Meeting.
Strategic Decision 6: improving publications
It was decided to further professionalise the Editorial Boards of all ERSPublications, and to consider future extensions of the Editors’ mandate,as well as the rationalization of the location of the publication services.
Several actions are under implementation. The most visible achievementis represented by the new impact factor of the ERJ (7.125), the highestever reached in the ERS history.
Strategic Decision 7: coordinating and enhancing advocacy
The current overall structure requires revision and restructuring to avoidoverlap in functions of European Lung Foundation (ELF) and ERS, withELF being clearly identified as a unit within the ERS rather than a sepa-rate organization operating independently (with its fundraising effortssometimes conflicting with ERS corporate relations).
The role of ELF has been enhanced, as testified by many initiatives andby the brilliant performances in the last Opening Cerimonies in Barcelonaand Munich. A patient is currently running ELF, to make clear that this isthe “voice of patients”:The advocacy office in Brussels has been crucial inmaking this process possible.
Strategic Decision 8: implementing strategic decisions via organisa-tional changes
The successful implementation of this strategy will involve several ERSstructures, including Human Resources; ERS Staff, ERS InformationTechnology (IT) and the ERS Communication Strategy.
06-migliori:migliori 7-01-2015 8:13 Pagina 135

eRn
136
Major changes are under implementation in the ERS Offices, starting fromLausanne. Those are centred on the need to improve IT and the service toour new members, while maintaining the leadership our conference has inscience and education.
Thanking Dario Olivieri for the opportunity to briefly revise the work Ihave been asked to coordinate in the past 2 years, I have realised oncemore that something has been achieved but much still needs to be done!Special thanks are due to the Presidential cycle, the Steering and the Ex-ecutive Committee members for making this possible.Last but not least, the visionary contribution of the ERS Executive Direc-tor, Fernando Martin was the “condicio sine qua non” to have a ERSStrategic Plan in place.
eRn
References
1. McNee W. The ERS Strategy report. Lau-sane, 2007.
2. Migliori GB, Rabe KF, Bel E, Elliott M,Gaga M, Holgate ST, Joos G, BurriezaFM, Sax B, Sculier JP, Simonds AK, BlasiF, Barnes PJ. The European RespiratorySociety plans its future: the 2013-2018
strategic plan. Eur Respir J 2014; 43 (4):927-32.
3. Blasi F, Reichman LB, Migliori GB. Pre-senting the European Forum for TB In-novation: innovative thinking in pro-gressing towards TB elimination in Eu-rope. Eur Respir J 2012; 40 (4): 806-808.
4. Blasi F, Barnes PJ, Gaga M , Migliori GB.
Future Directions for the ERS: Presiden-tial plans. ERJ 2013; 42: 875-880.
5. Blasi F, Dara M, van derWerf MJ, MiglioriGB. Supporting TB clinicians managingdifficult cases: the ERS/WHO Consilium.Eur Respir J 2013; 41 (3): 491-494.
06-migliori:migliori 7-01-2015 8:13 Pagina 136

eRn
137
Giovanni Battista Migliori is specialist in Respiratory Medicine and Medical Sta-tistics, and Auditor of Quality Systems. With more than 20 years of experience indesign, implementation and Monitoring & Evaluation of TB and TB/HIV controlprogrammes globally, he is Head of Clinical Epidemiology of Respiratory DiseasesService and Director of the World Health Organization (WHO) CollaboratingCentre for TB and Lung Diseases at Fondazione S. Maugeri, Tradate, Italy activein TB control, training and research activities at the global level. He was electeda Fellow of the Royal College of Physicians (FRCP), London in 2012 (honorarynomination, bye-law 39b) and foundation Fellow of the European Respiratory So-ciety (FERS) in 2014. He has published more than 250 peer-review papers onCOPD, Asthma, Pulmonary Rehabilitation and TB (h-index 42). He is author ofthe first European Respiratory Society TB guidelines (1999); author/coordinatorof several guidelines supporting ECDC/WHO development of EU-TB control poli-cy; author of all guidelines belonging to the Wolfheze series (EuropeanWHO/UNION/ECDC Consensus); coordinator of the ESTC (European Standardsfor Tuberculosis Care); promoter of the newly built Kosovo national TB Pro-gramme, in collaboration with USAID, and of the implementation of TB control incountries experimenting war or massive migration; coordinator of DST EQA stud-ies and drug resistance surveys in several countries (Italy, Mozambique, Burkina,Kosovo, Russia, Ukraine); pioneer of the TB under-reporting evaluation with a se-ries of important studies in different journals, which have been used by WHO toimplement better surveillance guidance; promoter of treatment outcome evaluationas a surveillance and research tool; author of the 2013 WHO educational pack-age supporting Countries to develop National Strategic Plans and to apply to theGlobal Fund for funding. He demonstrated with experimental data the adequacyof the XDR-TB definition, the impossibility to use the TDR definition and the needto stratify outcomes beyond XDR-TB. He has coordinated the USAID-funded pro-ject which developed a tool supporting countries in identifying gaps and propos-ing solutions to prevent and manage MDR- and XDR-TB. This tool has become thestandard tool used by the WHO Green Light Committee. He is the coordinator ofthe European TB Elimination movement, with conceptualisation of TB Elimina-tion, development of the first framework, of the feasibility white paper within theERS Forum initiative, of the European survey on preparedness and finalisation ofthe WHO framework resulting from the ERS/WHO event in Rome (2014). He hascreated and directed over 100 WHO Training Courses for TB and TB/HIV Con-sultants /managers, PPM Consultants/managers, Infection Control Consultants,GFATM Consultants/managers; Laboratory Consultants/managers. He is cur-rently an Associate Editor of the European Respiratory Journal and of the Inter-national Journal of Tuberculosis and Lung Disease. He is Secretary General andWHO /ECDC Liaison Officer of the European Respiratory Society.
06-migliori:migliori 7-01-2015 8:13 Pagina 137
eRn
138
Oedipus on the road to Thebessolved the riddle of the Sphinx andwas granted not only safety but akingdom and a queen as well. Theparagon may seem quite irreverent,but researchers, like in the greatGreek myth, must also answer a se-ries of complicated queries almostworthy of the Sphinx before start-ing statistical analysis so as to notraise questions about the validityof their work and credibility.The first problem to solve is thecreation of a logical and rationalstudy design, also technically re-ferred to as the research or workhypothesis. Next follows the analy-sis of the data. Unfortunately, thereverse order often prevails. Inevery case, the work hypothesismust respond to specific requisites.First of all, it must be formulatedin operative terms, in that anyonecould accept and follow the proce-dures thereby insuring the repro-ducibility of the data. The secondrequisite of the work hypothesis isrigor, which is the anticipation ofall possible results generated fromthe experiments. Finally, the hy-pothesis must always be verifiable;while some hypotheses may bebrilliant and suggestive, they are
often formulated in vague andgeneric terms and therefore notverifiable.Once the work hypothesis is cor-rectly formulated, the second rid-dle must be solved, which is thetype of statistical data or variables.Based on the data, the appropriatestatistical test may be chosen. Thevariables can be of three differenttypes: continuous, also calledquantitative or parametric such asweight and height; ordinal, such asschool and military grades; nomi-nal, or categorical or non-paramet-ric such as sex, race and hair col-or. The organization of data is fun-damental for research, especially inmedicine where there is maximumvariability in parameters as well asindividual variability, since the da-ta frequently refers to sick humans.Continuous variables may be dis-tributed normally or not, while or-dinal or nominal variables maydistribute in various ways, whilenever in a Gaussian fashion.Hence, the third enigma to solve: toverify the distribution of the vari-ables. Normal or Gaussian distrib-ution is characterized by a curvederived from a common variable,and looks like a bell which is sym-
The riddles of statistics
Statistics
Europ. Respir. News XXII (85): 138-140, 2014
Giovanna Pisi1, Alfredo Chetta21Cystic Fibrotic Unit, Dept of Pediatric2Dept Clinical and Experimental Medicine,University Hospital, Parma, Italy
Correspondence to:Alfredo ChettaDepartment of Clinical and Experimental MedicineUniversity of Parma (Italy)University Hospital G. RasoriVia G. Rasori, 10 - 43100 Parma, ItalyTel. +39 0521 903475Fax +39 0521 292615E-mail: [email protected]
Giovanna Pisi is Head of Cystic Fibro-sis Unit, Dept of Pediatrics at the Uni-versity Hospital of Parma. In 1985 shegraduated from the School of Medicineof University of Parma and in 1989 and1993 obtained the diploma in Pedi-atrics and in Respiratory Diseases, re-spectively at the University of Parma.She is member of Italian Society of Cys-tic Fibrosis. Her main fields of interestare cystic fibrosis and pediatric asthmaas well as statistics. She is author of 30scientific papers published in peer- re-view journals.
07-pisi statistics:pisi statistics 7-01-2015 8:14 Pagina 138

eRn
139
metrical relative to a point of max-imum density called the mean, andwith two equidistant tails. If dis-persion indexes such as standarddeviations are used, it is observedthat 68% of the data, normally dis-tributed, falls within one standarddeviation, while about 95% of thedata falls within two standard de-viations from the mean. A normaldistribution of the data points toparametric tests, and vice versa, tonon-parametric tests. Based on ex-perience, most biological parame-ters can be considered to be ex-tracted from ideal infinite popula-tions and normally distributed.That assumption, when leftunchecked, can lead to cataclysmicmethodological errors. In order toapply parametric tests, certain spe-cific prerequisites must be met.Firstly, the observations must beindependent, that is the single case
included in the sample must not in-fluence the choice of other cases.Secondly, the populations otherthan having normal distributions,must also in the case of paired ormultiple comparisons have thesame variance. The condition ofhomogenous variance or homosce-daticity can be verified by specificstatistical tests (Bartlett, Box, andHartley’s F-max tests). Lastly, thevariables under examination mustbe numerical in that arithmeticmay be applied to them.Since the requisites are rigid andrestrictive, especially in the med-ical field as well as in the case ofcomplex experimental designs, itbecomes at times difficult to applyparametric tests. The need tobroaden the possibility of the sta-tistical analysis to abnormal popu-lations, or to ones with unknowncharacteristics, led to the inception
Table 1 – Statistical tests based on programed experiment
Type of experiment Parametric test Non-parametric test
Two treatments with different populations t-test for independent data Mann-Whitney test,chi-square
Three or more treatments with different analysis of variance Kruskal-Wallis testpopulations chi-square
Before and after treatment with same paired t-test Wilcoxon or McNemar testspopulation
Multiple treatments on same population analysis of variance for Friedman testrepeated measures Cochrane Q-test
Association between two variables linear regression and Spearman test andPearson correlation contingency coefficient
07-pisi statistics:pisi statistics 7-01-2015 8:14 Pagina 139

eRn
140
in the 1940’s of new methodologiesof inference. The novel statisticalapproach was independent frompopulation parameters and definedas non-parametric or distributionfree. It was not by chance that thisnew methodology was born out ofthe statistical need of experimentalpsychologists who frequently dealtwith qualitative or population vari-ables with non-homogenous vari-ance. It is worthy to recall that Sid-ney Siegel, one of the fathers ofnon-parametric inference, prior todedicating himself to statistics, ob-tained his Ph.D in psychologyfrom Stanford University. Table 1
summarizes the use of the most dif-fuse statistical tests, parametricalor non, based on the experiment athand.Oedipus solved the riddle but as weknow, in the end things went ratherawry for him. And so it follows forthe researcher, forgive the paragonyet again, that the application ofadequate statistical tests do notguarantee convincing results. Whatcan data from an experiment reallysuggest will be the topic of the nextand last chapter.
eRn
Alfredo Chetta is Full Professor in Respiratory Medicine at the University of Parmaand Head of Lung Function Unit at the University Hospital of Parma. In 1978 hegraduated cum laude from the School of Medicine of Catholic University in Rome andin 1982 obtained the diploma in Respiratory Diseases at the University of Parma. Heis reviewer for several scientific journals and member of the Editorial Board of Chestand Respiration. His main fields of interest are exercise capacity, asthma and chron-ic obstructive pulmonary disease as well as history of Medicine. He is author of morethan 150 scientific papers published in peer-review journals, 120 of them available inpubmed.
07-pisi statistics:pisi statistics 7-01-2015 8:14 Pagina 140

eRn
141
This research aims to develop aneonatal prognostic index for neu-rodevelopment in very-low-birth-weight (VLBW) preterm childrenin order to guide early, more effec-tive treatment for cerebral palsy(CP) and other neurodevelopmen-tal impairments. Preterm birth af-fects 1 in 10 worldwide (March ofDimes 2012) and is recognized as aleading cause of long-term neuro-logical disability in children. Ad-vances in neonatal medicine haveimproved survival rates and out-come among preterm infants; how-ever, 40-50% of VLBW infants ex-perience neurodevelopmental im-pairments such as CP and develop-mental coordination disorder byschool age (Woodward et al. 2009).Currently, it is difficult to predictwhich preterm infants will developneurodevelopmental impairments,limiting the potential to implementearly treatment at a time of opti-mal neuroplasticity. Today, chil-dren with CP typically do not re-ceive prognosis or treatment untilafter they present with motordeficits, a time when treatmentmay not be as successful. However,early identification of infants atrisk for motor and cognitivedeficits is essential to guide early,more effective treatment that may
improve neurodevelopment andquality of life.Risk factors such as bronchopul-monary dysplasia and inflammato-ry conditions have been associatedwith worse neurodevelopmentaloutcomes, but specific criteria foridentifying these risk factors arenot well understood. Additionally,routine neuroimaging, includingultrasound and MRI performedprior to discharge from the NICU,has only been partially successfulat predicting which preterm infantsare at highest risk for future im-pairment (Rose et al. 2009),(Woodward et al. 2012). Semi-au-tomated, atlas-based diffusion ten-sor imaging (DTI) and automaticfiber tract quantification arepromising methods to assess earlyneonatal white matter microstruc-ture to augment standard clinicalMRI for improved prognosis (Roseet al. 2007, 2009, 2014), (Oishi etal. 2013), (Johnson et al. 2014).The proposed research follows acohort of 102 VLBW preterm in-fants recruited prior to routinenear-term brain MRI at 36.6±1.8weeks postmenstrual age; 66/102also had DTI. At 18-22 months ad-justed age, a total of 93/102 chil-dren returned for follow-up evalu-ation with the Bayley Scales for In-
Research Projects
Research Projects
Europ. Respir. News XXII (85): 141-144, 2014
Neonatal Physiological andNeural Correlates of EarlyNeurodevelopment inPreterm Children
Jessica Rose1,2,3, Rachel Vassar1,2,Katelyn Cahill-Rowley1-4,Naama Barnea-Goraly1,2,Susan R. Hintz5, Kristen Yeom6,David K. Stevenson5
1 Department of Orthopaedic Surgery,Stanford University School of Medicine,Stanford CA2 Neonatal Neuroimaging Lab,Stanford University School of Medicine,Stanford CA3 Motion Analysis Lab, Lucile PackardChildren’s Hospital, Stanford CA4 Department of Bioengineering, StanfordUniversity, Stanford CA5 Division of Neonatal & DevelopmentalMedicine, Stanford University School ofMedicine, Stanford CA6 Division of Pediatric Radiology,Stanford University School of Medicine,Stanford CA
Correspondence to:E-mail: [email protected]
08-research project:08-research project 7-01-2015 8:15 Pagina 141

eRn
142
A correct diagnosis of asthma isessential for drug therapy. Cur-rently, diagnosis is made throughevaluation of symptoms and pul-monary function testing. Targetedtests, designed to detect markersof chronic inflammation thatcharacterizes asthma, are veryfew. More recently, new biomark-ers have emerged by the ‘omicsapproach, but the measure of suchbiomarkers requires sophisticatedlarge-scale analytical methods toquantify gene expression (tran-scriptomics), proteins (pro-teomics), lipids (lipidomics) andmetabolites (metabolomics) in thelungs, blood or urine. As a conse-quence, it would be attractive toprovide a more simple and reliable
method of detecting markers pre-dictive of a level of asthma exacer-bation or control.In this context, the ambitiousscope of the project AsthmaZoè isto develop a method to measure aspecific biomarker of asthma withone drop of blood or body fluid.The chronic inflammation thatcharacterizes asthma is mediatedby the eosinophils. The interactionthat takes place between al-fa4beta1 integrins (α4β1, orVLA-4, a subclass of transmem-brane glycoproteins) expressed byeosinophils, and the Vascular-1Cell Adhesion Molecules (VCAM-1), small proteins expressed byendothelial cells of affected bloodvessels after appropriate stimula-
eRn
fant and Toddler Development(BSID-III) and a total of 82/102children returned for follow-upevaluation of gait temporal-spatialparameters and upper limb reach-ing. Neonatal physiological riskfactors and neuroimaging will beanalyzed in relation to BSID-III,the Toddler Gait Index of tempo-ral-spatial gait parameters, and theToddler Reaching Index based onaccelerometer metrics during up-per-limb reaching. Our goal is todevelop a prognostic index for ear-ly neurodevelopment that can beadministered prior to dischargefrom the NICU.The Specific Aims are:Aim 1: Determine neonatal physio-
logical biomarkers that best predictmotor and cognitive function at18-22 months adjusted age in chil-dren born preterm with VLBW.Aim 2: Determine structural char-acteristics of brain regions and whitematter tract microstructure at near-term age that best predict upper-limb and lower-limb motor functionat 18-22 months adjusted age inchildren born preterm with VLBW.Aim 3: Develop the Toddler GaitIndex and the Toddler ReachingIndex.Aim 4: Develop a neonatal prog-nostic index to predict motor andcognitive development in toddlersborn preterm with VLBW.
AsthmaZoè: NanostructuredMaterials for the Detectionof Markers of Asthma andOther CorrelatedInflammatory Diseases
Rossella De Marco1,Giampaolo Ricci2, Sergio Schinelli3,Luisa De Cola4, Luca Prodi1,Luca Gentilucci11 Dept. of Chemistry “G. Ciamician”,University of Bologna, Bologna, Italy2 “Gozzadini” Children’s Hospital, PoliclinicoS. Orsola-Malpighi, University of Bologna,Bologna Italy3 Dept. of Drug of Science, University ofPavia, Pavia, Italy4 Institut de science et d’ingénieriesupramoléculaire (ISIS), icFRC and CNRS,Université de Strasbourg, Strasbourg, FranceCorrespondence to:E-mail: [email protected]
08-research project:08-research project 7-01-2015 8:15 Pagina 142

eRn
143
tion by cytokines, is essential forthe realization of a firm adhesionbetween the vascular endotheliumand eosinophils, followed by themigration of the latter towards theregion of inflammation. Recentfindings revealed that followingstimulation by cytokines, theoverexpressed integrins experiencea conformational switch that pre-cedes and is necessary for highaffinity/strong interaction withVCAM-1.Starting from these assumptions,AsthmaZoè is aimed at the designof new diagnostic tools capable ofselectively quantify only the al-fa4beta1 integrin-expressingeosinophils in their active/highaffinity conformation, plausiblebiomarker of the subsequenteosinophils recruitment that trig-gers the inflammatory process.Since VCAM-1 bind the active in-tegrins by interaction of a shortpeptide portion of the exposedsurface (UniPv), AsthmaZoè willutilized small-molecule pep-tidomimetics of such native recog-nition motif (UniBo). To consent arapid detection, the pep-tidomimetics will be grafted ontoself-assembled monolayers(SAMs) of inorganic nanoparti-cles, nanostructured materialswhich demonstrated a good abili-ty to reproduce protein-protein in-teractions (UniStrasbourg). SAMs
of nanoparticles allow strong in-teractions with eosinophils, due tothe high functionalization densityand mechanical stability. Thenanoparticles can be loaded with afluorescent dye for the expedientdetection of adherent cells. Final-ly, the SAMs of peptidomimetic-coated nanoparticles can be di-mensioned to microscale and canbe easily engineered by micro-contact methods and other nan-otechnologies.The optimized microchip-devicewill be validated by clinical trial(Policlinico S. Orsola-Malpighi),through analyses of patient’s bodyfluids, sputum, urine, nasal secre-tion, blood, sampled at differentstages of the disease (mild to se-vere symptoms, and during corti-costeroids/beta2-agonist therapy).The correlation between the levelsof the biomarker and the clinicalpicture for nasal and bronchialsymptoms, using the levels of thebiomarker obtained for patientswith nasal symptoms (rhinitis) ascontrol, will confirm the aspira-tion of AsthmaZoè to improve di-agnosis, in particular of pediatricasthma, i.e. facilitate the monitor-ing of disease activity and therapy,and define disease phenotypes.
eRn
08-research project:08-research project 7-01-2015 8:15 Pagina 143

eRn
144
Objective: This study proposes tocompare the effect of outdoor envi-ronmental pollution and passivesmoking on small airway functionand inflammation, which is Objec-tive 2 of the call for scientific re-search from the 2014 Chiesi Foun-dation Onlus Call for Proposals.
Background & Aims: Passive sec-ond hand smoke (SHS) is a healthrisk to the general population. Weaim to determine the adverse effectof SHS on airway function com-pared to that of traffic pollution.Specifically, we would like to quan-tify the changes produced by SHSand traffic pollution on the small(and large) airways of the lungs inhealthy volunteers. Air pollutionalso poses a greater risk to thehealth of patients with chronic un-derlying lung disorders. We willtherefore asses the airway (largeand small) effects of SHS and traf-fic pollution in patients with asth-ma. We will also be able to com-pare results from asthmatic pa-tients to those of healthy volun-teers.
Methods: Phase 1: During the first3 months of the study, we willmonitor air pollution by measuring
particulate matter (PM) and blackcarbon (BC) in a pedestrian onlyzone in London, and in a high traf-fic road,. This will provide us withthe background pollution analysisnecessary to evaluate the effect ofdifferent weather conditions on thelevel of pollution. Phase 2: In thefollowing 6 months, we will recruithealthy volunteers, to a crossoverstudy where they walk in thepedestrian only zone at one visitand then the high traffic road onanother visit. Phase 3: During thenext 6 months of the study asth-matic subject will be invited to acrossover study where they walk inthe pedestrian only zone at one vis-it and then the high traffic road onanother visit.
Impact: The study we propose is ofinterest not only to clinicians butalso to policy makers. SHS hasknown negative adverse health ef-fects. Our study will quantify theinflammation and the resulting air-way dysfunction induced by vehic-ular pollution compared to SHS.This may prove to be instrumentalto provide guidelines for the pro-tection of the public population.
Passive Smoking andVehicular Traffic Effect onSmall Airway Function andInflammation
P. Paredi, A. Ruprecht, P.J. Barnes,O.S. UsmaniImperial College London & Royal BromptonHospital
Correspondence to:E-mail: [email protected]
eRn
08-research project:08-research project 7-01-2015 8:15 Pagina 144
HELP SHAPE THE FUTURE OF RESPIRATORY SCIENCE AND MEDICINEtake part in ERS Amsterdam 2015
european respiratory societyevery breath counts
ATTEND the ERS International Congress, the largest respiratory meeting in theworld.
PRESENT your work in a learning environment of the highest level, to thewidest and most influential audience of respiratory professionals.
FORGE and RENEW working relationships with the leading specialists in thefield and update on the latest research and clinical best practice.
00-copertina 3-2014:copertina 2-2014 7-01-2015 8:06 Pagina 2

eRnEuropeanRespiratoryNewsIssue 85
Volume XXII
Scientific Direction:Dario Olivieri DirectorEmilio Marangio Vice-DirectorAlfredo Chetta Vice-DirectorDepartment of Clinical andExperimental MedicineUniversity of Parma (Italy)
Editorial Board:Marina AielloElisa BonatiFrancesco LongoGiovanna PisiRoberta PisiMartina RendoElisabetta TeopompiPanagiota TzaniDina Visca
International Board:Alvar Agusti (Barcelona, S)Peter J. Barnes (London, UK)Demosthenes Bouros (Alexandroupolis, GR)Jean Bousquet (Montpellier, F)Chris Brightling (Leicester, UK)Roland Buhl (Mainz, D)Andrew Bush (London, UK)Pascal Chanez (Marseille, F)Vincent Cottin (Lyon, F)Carlos Robalo Cordeiro (Coimbra, P)Ronald Dahl (Odense, DK)Marc Decramer(Leuven, B)Richard Dekhuijzen (Nijmegen, NED)Stephen T. Holgate (Southampton, UK)Marc Humbert (Paris, F)Guy Joos (Ghent, B)Marc Miravitlles (Barcelona, S)Klaus Rabe (Grosshandorf, D)Jo/rgen Vestbo (Manchester, UK)Christian Virchow (Rostock, D)
Editorial Office:Stefano OlivieriMob. + 39 335 5422554E-mail: [email protected]
Printing and diffusion:Mattioli 1885Strada di Lodesana 649/sxLoc. Vaio - 43036 Fidenza-PRTel. 0524/530383Fax 0524/[email protected]
Pubbl. Trimestrale - Poste Italiane s.p.a. - Spedizioni in Abb. Postale D.L. 353/2003 (conv. in L. 27/02/2004 n. 46) art. 1, comma 1, DCB ParmaAut. Trib. Parma n. 26 del 27/28-10-1992 - Euro 2,58
Copyright: All the copyrights have been observed. However, for information, please contact the Editorial Office
3-2014
Euroscienze Ed
00-copertina 3-2014:copertina 2-2014 7-01-2015 8:06 Pagina 1
Related Documents











