YERVOY- ipilimumab injection E.R. Squibb & Sons, L.L.C. ---------- HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use YERVOY safely and effectively. See full prescribing information for YERVOY. YERVOY (ipilimumab) injection, for intravenous use Initial U.S. Approval: 2011 RECENT MAJOR CHANGES Boxed Warning, Removed 6/2020 Indications and Usage (1) 5/2021 Dosage and Administration (2) 5/2021 Warnings and Precautions (5) 5/2021 INDICATIONS AND USAGE YERVOY is a human cytotoxic T-lymphocyte antigen 4 (CTLA-4)-blocking antibody indicated for: Melanoma • • • Renal Cell Carcinoma (RCC) • Colorectal Cancer • Hepatocellular Carcinoma • Non-Small Cell Lung Cancer (NSCLC) • • • DOSAGE AND ADMINISTRATION ® Treatment of unresectable or metastatic melanoma in adults and pediatric patients 12 years and older. (1.1) Treatment of adult patients with unresectable or metastatic melanoma, in combination with nivolumab. (1.1) Adjuvant treatment of patients with cutaneous melanoma with pathologic involvement of regional lymph nodes of more than 1 mm who have undergone complete resection, including total lymphadenectomy. (1.2) Treatment of patients with intermediate or poor risk advanced renal cell carcinoma, as first-line treatment in combination with nivolumab. (1.3) Treatment of adult and pediatric patients 12 years and older with microsatellite instability-high (MSI- H) or mismatch repair deficient (dMMR) metastatic colorectal cancer that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan, in combination with nivolumab. This indication is approved under accelerated approval based on overall response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. (1.4) Treatment of patients with hepatocellular carcinoma who have been previously treated with sorafenib, in combination with nivolumab. This indication is approved under accelerated approval based on overall response rate and duration of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. (1.5) Treatment of adult patients with metastatic non-small cell lung cancer expressing PD-L1 (≥1%) as determined by an FDA-approved test, with no EGFR or ALK genomic tumor aberrations, as first-line treatment in combination with nivolumab. (1.6) Treatment of adult patients with metastatic or recurrent non-small cell lung cancer with no EGFR or ALK genomic tumor aberrations as first-line treatment, in combination with nivolumab and 2 cycles of platinum-doublet chemotherapy. (1.6) Malignant Pleural Mesothelioma Treatment of adult patients with unresectable malignant pleural mesothelioma, as first-line treatment in combination with nivolumab. (1.7)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
YERVOY- ipilimumab injection E.R. Squibb & Sons, L.L.C.----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use YERVOY safely andeffectively. See full prescribing information for YERVOY.
YERVOY (ipilimumab) injection, for intravenous useInitial U.S. Approval: 2011
RECENT MAJOR CHANGESBoxed Warning, Removed 6/2020Indications and Usage (1) 5/2021Dosage and Administration (2) 5/2021Warnings and Precautions (5) 5/2021
INDICATIONS AND USAGEYERVOY is a human cytotoxic T-lymphocyte antigen 4 (CTLA-4)-blocking antibody indicated for:Melanoma
•
•
•
Renal Cell Carcinoma (RCC)
•
Colorectal Cancer
•
Hepatocellular Carcinoma
•
Non-Small Cell Lung Cancer (NSCLC)
•
•
•
DOSAGE AND ADMINISTRATION
®
Treatment of unresectable or metastatic melanoma in adults and pediatric patients 12 years andolder. (1.1)Treatment of adult patients with unresectable or metastatic melanoma, in combination withnivolumab. (1.1)Adjuvant treatment of patients with cutaneous melanoma with pathologic involvement of regionallymph nodes of more than 1 mm who have undergone complete resection, including totallymphadenectomy. (1.2)
Treatment of patients with intermediate or poor risk advanced renal cell carcinoma, as first-linetreatment in combination with nivolumab. (1.3)
Treatment of adult and pediatric patients 12 years and older with microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) metastatic colorectal cancer that has progressed followingtreatment with a fluoropyrimidine, oxaliplatin, and irinotecan, in combination with nivolumab. Thisindication is approved under accelerated approval based on overall response rate and duration ofresponse. Continued approval for this indication may be contingent upon verification and descriptionof clinical benefit in confirmatory trials. (1.4)
Treatment of patients with hepatocellular carcinoma who have been previously treated with sorafenib,in combination with nivolumab. This indication is approved under accelerated approval based onoverall response rate and duration of response. Continued approval for this indication may becontingent upon verification and description of clinical benefit in confirmatory trials. (1.5)
Treatment of adult patients with metastatic non-small cell lung cancer expressing PD-L1 (≥1%) asdetermined by an FDA-approved test, with no EGFR or ALK genomic tumor aberrations, as first-linetreatment in combination with nivolumab. (1.6)Treatment of adult patients with metastatic or recurrent non-small cell lung cancer with no EGFR orALK genomic tumor aberrations as first-line treatment, in combination with nivolumab and 2 cycles ofplatinum-doublet chemotherapy. (1.6)Malignant Pleural MesotheliomaTreatment of adult patients with unresectable malignant pleural mesothelioma, as first-line treatmentin combination with nivolumab. (1.7)
••
•
•
•
•
•
•
DOSAGE FORMS AND STRENGTHS
•
CONTRAINDICATIONS
•
WARNINGS AND PRECAUTIONS
•
•
•
•
ADVERSE REACTIONSMost common adverse reactions (≥5%) with YERVOY as a single agent are fatigue, diarrhea, pruritus, rash,and colitis. Additional common adverse reactions at the 10 mg/kg dose (≥5%) include nausea, vomiting,headache, weight loss, pyrexia, decreased appetite, and insomnia. (6.1)Most common adverse reactions (≥20%) with YERVOY in combination with nivolumab are fatigue, rash,pruritus, diarrhea, musculoskeletal pain, cough, pyrexia, decreased appetite, nausea, abdominal pain,
Administer by intravenous infusion based upon recommended infusion rate for each indication. (2)Unresectable or Metastatic Melanoma:
∘∘
YERVOY 3 mg/kg every 3 weeks for a maximum of 4 doses. (2.2)YERVOY 3 mg/kg immediately following nivolumab 1 mg/kg on the same day, every 3 weeks for 4doses. After completing 4 doses of the combination, administer nivolumab as a single agent asrecommended in the Full Prescribing Information for nivolumab. (2.2)
Adjuvant Treatment of Melanoma: YERVOY 10 mg/kg every 3 weeks for 4 doses, followed by 10 mg/kgevery 12 weeks for up to 3 years. (2.2)Advanced Renal Cell Carcinoma: YERVOY 1 mg/kg immediately following nivolumab 3 mg/kg on thesame day, every 3 weeks for 4 doses. After completing 4 doses of the combination, administernivolumab as a single agent as recommended in Full Prescribing Information for nivolumab. (2.2)Microsatellite Instability-High (MSI-H) or Mismatch Repair Deficient (dMMR) Metastatic ColorectalCancer: YERVOY 1 mg/kg intravenously over 30 minutes immediately following nivolumab 3 mg/kgintravenously over 30 minutes on the same day, every 3 weeks for 4 doses. After completing 4 dosesof the combination, administer nivolumab as a single agent as recommended in Full PrescribingInformation for nivolumab. (2.2)Hepatocellular Carcinoma: YERVOY 3 mg/kg intravenously over 30 minutes immediately followingnivolumab 1 mg/kg intravenously over 30 minutes on the same day, every 3 weeks for 4 doses. Aftercompletion 4 doses of the combination, administer nivolumab as a single agent as recommended inFull Prescribing Information for nivolumab. (2.2)Metastatic non-small cell lung cancer:
∘∘
YERVOY 1 mg/kg every 6 weeks with nivolumab 3 mg/kg every 2 weeks. (2.2)YERVOY 1 mg/kg every 6 weeks with nivolumab 360 mg every 3 weeks and 2 cycles of platinum-doublet chemotherapy. (2.2)
Malignant pleural mesothelioma: YERVOY 1 mg/kg every 6 weeks with nivolumab 360 mg every 3weeks. (2.2)
Injection: 50 mg/10 mL (5 mg/mL) and 200 mg/40 mL (5 mg/mL) in a single-dose vial. (3)
None. (4)
Severe and Fatal Immune-Mediated Adverse Reactions: Immune-mediated adverse reactions (IMAR)can occur in any organ system or tissue, including the following: immune-mediated colitis, immune-mediated hepatitis, immune-mediated dermatologic adverse reactions, immune-mediatedendocrinopathies, immune-mediated pneumonitis, and immune-mediated nephritis with renaldysfunction, and can occur at any time during treatment or after discontinuation. Monitor forsymptoms and signs that may be clinical manifestations of IMAR. Evaluate clinical chemistriesincluding liver enzymes, creatinine, adrenocorticotropic hormone level and thyroid function at baselineand before each dose. In general, withhold YERVOY for severe (grade 3) and permanently discontinuefor life-threatening (grade 4) immune-mediated adverse reactions. See Full Prescribing Informationfor additional dosage modifications. (2.3, 5.1)Infusion-Related Reactions: Discontinue for severe and life-threatening infusion-related reactions.Interrupt or slow the rate of infusion in patients with mild or moderate infusion-related reactions. (2.3,5.2)Complications of allogeneic HSCT: Fatal and other serious complications can occur in patients whoreceive allogeneic HSCT before or after being treated with YERVOY. (5.3)Embryo-Fetal Toxicity: Can cause fetal harm. Advise of potential risk to a fetus and use of effectivecontraception. (5.4, 8.1, 8.3)
pruritus, diarrhea, musculoskeletal pain, cough, pyrexia, decreased appetite, nausea, abdominal pain,arthralgia, headache, vomiting, dyspnea, dizziness, hypothyroidism, and decreased weight. (6.1)Most common adverse reactions (≥20%) with YERVOY in combination with nivolumab and platinum-doublet chemotherapy are fatigue, musculoskeletal pain, nausea, diarrhea, rash, decreased appetite,constipation, and pruritus. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Bristol-Myers Squibb at 1-800-721-5072or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
USE IN SPECIFIC POPULATIONS
•
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.Revised: 5/2021
FULL PRESCRIBING INFORMATION: CONTENTS*1 INDICATIONS AND USAGE
1.1 Unresectable or Metastatic Melanoma1.2 Adjuvant Treatment of Melanoma1.3 Advanced Renal Cell Carcinoma1.4 Microsatellite Instability-High or Mismatch Repair Deficient Metastatic ColorectalCancer1.5 Hepatocellular Carcinoma1.6 Metastatic Non-Small Cell Lung Cancer1.7 Malignant Pleural Mesothelioma
2 DOSAGE AND ADMINISTRATION2.1 Patient Selection2.2 Recommended Dosage2.3 Recommended Dosage Modifications for Adverse Reactions2.4 Preparation and Administration
3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS
5.1 Severe and Fatal Immune-Mediated Adverse Reactions5.2 Infusion-Related Reactions5.3 Complications of Allogeneic Hematopoietic Stem Cell Transplant after YERVOY5.4 Embryo-Fetal Toxicity5.5 Risks Associated When Administered in Combination with Nivolumab
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.2 Lactation8.3 Females and Males of Reproductive Potential8.4 Pediatric Use8.5 Geriatric Use
11 DESCRIPTION12 CLINICAL PHARMACOLOGY
Lactation: Advise not to breastfeed. (8.2)

12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
14 CLINICAL STUDIES14.1 Unresectable or Metastatic Melanoma14.2 Adjuvant Treatment of Melanoma14.3 Advanced Renal Cell Carcinoma14.4 Microsatellite Instability-High or Mismatch Repair Deficient Metastatic ColorectalCancer14.5 Hepatocellular Carcinoma14.6 Metastatic Non-Small Cell Lung Cancer14.7 Malignant Pleural Mesothelioma
16 HOW SUPPLIED/STORAGE AND HANDLING17 PATIENT COUNSELING INFORMATION*
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGE
1.1 Unresectable or Metastatic MelanomaYERVOY is indicated for the treatment of unresectable or metastatic melanoma in adultsand pediatric patients 12 years and older.YERVOY, in combination with nivolumab, is indicated for the treatment of unresectableor metastatic melanoma in adult patients.
1.2 Adjuvant Treatment of MelanomaYERVOY is indicated for the adjuvant treatment of patients with cutaneous melanomawith pathologic involvement of regional lymph nodes of more than 1 mm who haveundergone complete resection, including total lymphadenectomy.
1.3 Advanced Renal Cell CarcinomaYERVOY, in combination with nivolumab, is indicated for the first-line treatment ofpatients with intermediate or poor risk advanced renal cell carcinoma (RCC).
1.4 Microsatellite Instability-High or Mismatch Repair Deficient MetastaticColorectal CancerYERVOY, in combination with nivolumab, is indicated for the treatment of adult andpediatric patients 12 years and older with microsatellite instability-high (MSI-H) ormismatch repair deficient (dMMR) metastatic colorectal cancer (mCRC) that hasprogressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan.This indication is approved under accelerated approval based on overall response rate
Sections or subsections omitted from the full prescribing information are not listed.

and duration of response [see Clinical Studies (14.4)]. Continued approval for thisindication may be contingent upon verification and description of clinical benefit inconfirmatory trials.
1.5 Hepatocellular CarcinomaYERVOY, in combination with nivolumab, is indicated for the treatment of patients withhepatocellular carcinoma (HCC) who have been previously treated with sorafenib. Thisindication is approved under accelerated approval based on overall response rate andduration of response [see Clinical Studies (14.5)]. Continued approval for this indicationmay be contingent upon verification and description of clinical benefit in the confirmatorytrials.
1.6 Metastatic Non-Small Cell Lung CancerYERVOY, in combination with nivolumab, is indicated for the first-line treatment of adultpatients with metastatic non-small cell lung cancer (NSCLC) whose tumors express PD-L1 (≥1%) as determined by an FDA-approved test [see Dosage and Administration(2.1)], with no EGFR or ALK genomic tumor aberrations.YERVOY, in combination with nivolumab and 2 cycles of platinum-doublet chemotherapy,is indicated for the first-line treatment of adult patients with metastatic or recurrentNSCLC, with no EGFR or ALK genomic tumor aberrations.
1.7 Malignant Pleural MesotheliomaYERVOY, in combination with nivolumab, is indicated for the first-line treatment of adultpatients with unresectable malignant pleural mesothelioma.
2 DOSAGE AND ADMINISTRATION
2.1 Patient SelectionSelect patients with metastatic NSCLC for treatment with YERVOY in combination withnivolumab based on PD-L1 expression [see Clinical Studies (14.6)].Information on FDA-approved tests for the determination of PD-L1 expression in NSCLCis available at: http://www.fda.gov/CompanionDiagnostics.
2.2 Recommended DosageThe recommended dosages of YERVOY as a single agent are presented in Table 1.
Table 1: Recommended Dosages for YERVOY as a Single Agent
Indication Recommended YERVOYDosage Duration of Therapy
Unresectable or metastaticmelanoma
3 mg/kg every 3 weeks(90-minute intravenous
infusion)Maximum of 4 doses
Adjuvant treatment of10 mg/kg every 3 weeks
followed by 10 mg/kg every 12 Every 3 weeks up to amaximum of 4 doses

Adjuvant treatment ofmelanoma weeks
(90-minute intravenousinfusion)
maximum of 4 dosesEvery 12 weeks for up to
3 years
The recommended dosages of YERVOY in combination with other therapeutic agents arepresented in Table 2. Refer to the respective Prescribing Information for eachtherapeutic agent administered in combination with YERVOY for recommended dosageinformation, as appropriate.
Table 2: Recommended Dosages of YERVOY in Combination with OtherTherapeutic Agents*
Indication Recommended YERVOY Dosage Duration of Therapy
Unresectable ormetastaticmelanoma
3 mg/kg every 3 weeks(90-minute intravenous infusion)
with nivolumab 1 mg/kg(30-minute intravenous infusion on the
same day)
In combination withnivolumab for a maximum
of 4 doses or untilunacceptable toxicity,
whichever occurs earlier.After completing 4 dosesof combination therapy,
administer nivolumab as asingle agent until disease
progression orunacceptable toxicity.
Advanced renal cellcarcinoma
1 mg/kg every 3 weekswith nivolumab 3 mg/kg
(30-minute intravenous infusion on thesame day)
In combination withnivolumab
for a maximum of 4doses.
After completing 4 dosesof combination therapy,administer nivolumab assingle agent until disease
progression orunacceptable toxicity.
Microsatelliteinstability-high(MSI‑H) or mismatchrepair deficient(dMMR) metastaticcolorectal cancer
1 mg/kg every 3 weekswith nivolumab 3 mg/kg
(30-minute intravenous infusion on thesame day)
After completing 4 dosesof combination therapy,administer nivolumab assingle agent until disease
progression orunacceptable toxicity.
Hepatocellularcarcinoma
3 mg/kg every 3 weekswith nivolumab 1 mg/kg
(30-minute intravenous infusion on thesame day)
In combination withnivolumab
for 4 doses.After completing 4 dosesof combination therapy,administer nivolumab assingle agent until disease
progression orunacceptable toxicity.
†
†
†
†

* Refer to the Prescribing Information for the agents administered in combination withYERVOY for recommended dosing information, as appropriate.† Refer to the Prescribing Information for nivolumab for dosage information aftercompleting use in combination with YERVOY.
Metastatic non-smallcell lung cancerexpressing PD‑L1
1 mg/kg every 6 weekswith nivolumab 3 mg/kg every 2 weeks
(30-minute intravenous infusion)
In combination withnivolumab until disease
progression,unacceptable toxicity, orup to 2 years in patients
without diseaseprogression.
Metastatic orrecurrent non-smallcell lung cancer
1 mg/kg every 6 weekswith nivolumab 360 mg every 3 weeks
(30-minute intravenous infusion)and histology-based platinum‑doublet
chemotherapy every 3 weeks
In combination withnivolumab until disease
progression,unacceptable toxicity, orup to 2 years in patients
without diseaseprogression.
2 cycles of histology-based platinum-doublet
chemotherapy
Malignant pleuralmesothelioma
1 mg/kg every 6 weekswith nivolumab 360 mg every 3 weeks
(30-minute intravenous infusion)
In combination withnivolumab until disease
progression,unacceptable toxicity, orup to 2 years in patients
without diseaseprogression.
2.3 Recommended Dosage Modifications for Adverse ReactionsNo dose reduction for YERVOY is recommended. In general, withhold YERVOY for severe(Grade 3) immune-mediated adverse reactions. Permanently discontinue YERVOY forlife-threatening (Grade 4) immune-mediated adverse reactions, recurrent severe (Grade3) immune-mediated reactions that require systemic immunosuppressive treatment,persistent moderate (Grade 2) or severe (Grade 3) reactions lasting 12 weeks or longerafter last YERVOY dose (excluding endocrinopathy), or an inability to reducecorticosteroid dose to 10 mg or less of prednisone or equivalent per day within 12weeks of initiating steroids. Dosage modifications for YERVOY or YERVOY in combinationwith nivolumab for adverse reactions that require management different from thesegeneral guidelines are summarized in Table 3.When YERVOY is administered in combination with nivolumab, withhold or permanentlydiscontinue both YERVOY and nivolumab for toxicity.
Table 3: Recommended Dosage Modifications for Adverse ReactionsAdverse Reaction Severity* Dosage ModificationsImmune-Mediated Adverse Reactions [See Warnings and Precautions (5.1)]
Grade 2 Withhold
†
†
†
a

Colitis Grade 2 WithholdGrade 3 or 4 Permanently discontinue
Hepatitis with no tumor involvementof the liverorHepatitis with tumor involvement ofthe liver/non-HCC
AST or ALT increases tomore than 3 times andup to 5 times the ULNorTotal bilirubin increasesto more than 1.5 timesand up to 3 times theULN
Withhold
AST or ALT more than 5times the ULNorTotal bilirubin more than3 times the ULN
Permanently discontinue
Hepatitis with tumor involvement ofthe liver /HCC
Baseline AST/ALT is morethan 1 and up to 3 timesULN and increases tomore than 5 and up to10 times ULNorBaseline AST/ALT is morethan 3 and up to 5 timesULN and increases tomore than 8 and up to10 times ULN.
Withhold
AST/ALT increases tomore than 10 times ULNorTotal bilirubin increasesto more than 3 timesULN.
Permanently discontinue
Exfoliative Dermatologic ConditionsSuspected SJS, TEN, orDRESS WithholdConfirmed SJS, TEN, orDRESS Permanently discontinue
Endocrinopathies Grades 3 or 4Withhold until clinicallystable or permanentlydiscontinue depending onseverity
Pneumonitis Grade 2 WithholdGrade 3 or 4 Permanently discontinue
Nephritis with Renal DysfunctionGrade 2 or 3 increasedblood creatinine WithholdGrade 4 increased bloodcreatinine Permanently discontinue
Neurological Toxicities Grade 2 WithholdGrade 3 or 4 Permanently discontinue
Myocarditis Grade 2, 3 or 4 Permanently discontinue
a
a
b c
a
d
a
a
a

ALT = alanine aminotransferase, AST = aspartate aminotransferase, DRESS = DrugRash with Eosinophilia and Systemic Symptoms, SJS = Stevens Johnson Syndrome, TEN= toxic epidermal necrolysis, ULN = upper limit of normal* Based on Common Terminology Criteria for Adverse Events (CTCAE), Version 4.03. Resume in patients with complete or partial resolution (Grade 0 or 1) after
corticosteroid taper. Permanently discontinue if no complete or partial resolution within12 weeks of last dose or inability to reduce prednisone to 10 mg per day (or equivalent)or less within 12 weeks of initiating steroids. If AST/ALT are less than or equal to ULN at baseline, withhold or permanently
discontinue YERVOY based on recommendations for hepatitis with no liver involvement. This guidance is only applicable to HCC patients who are being treated with YERVOY in
combination with nivolumab. Depending on clinical severity, consider withholding for Grade 2 endocrinopathy until
symptom improvement with hormone replacement. Resume once acute symptomshave resolved.
Ophthalmologic
Grade 2, 3, or 4 thatdoes not improve toGrade 1 within 2 weekswhile receiving topicaltherapy or that requiressystemic treatment
Permanently discontinue
Other Adverse ReactionsInfusion-Related Reactions [seeWarnings and Precautions (5.2)]
Grade 1 or 2 Interrupt or slow the rateof infusion
Grade 3 or 4 Permanently discontinue
2.4 Preparation and Administration
••
Preparation of Solution
•
••
•
•
Administration
•
a
b
c
d
Do not shake product.Visually inspect for particulate matter and discoloration prior to administration.Discard vial if solution is cloudy, there is pronounced discoloration (solution mayhave pale-yellow color), or there is foreign particulate matter other thantranslucent-to-white, amorphous particles.
Allow the vial(s) to stand at room temperature for approximately 5 minutes prior topreparation of infusion.Withdraw the required volume of YERVOY and transfer into an intravenous bag.Dilute with 0.9% Sodium Chloride Injection, USP or 5% Dextrose Injection, USP to afinal concentration ranging from 1 mg/mL to 2 mg/mL. Mix diluted solution bygentle inversion.After preparation, store the diluted solution either refrigerated at 2°C to 8°C (36°Fto 46°F) or at room temperature of 20°C to 25°C (68°F to 77°F) for no more than24 hours from the time of preparation to the time of infusion.Discard partially used or empty vials of YERVOY.
Do not co-administer other drugs through the same intravenous line.

••
•
•
3 DOSAGE FORMS AND STRENGTHSInjection: 50 mg/10 mL (5 mg/mL) or 200 mg/40 mL (5 mg/mL) as a clear to slightlyopalescent, colorless to pale-yellow solution in a single-dose vial.
4 CONTRAINDICATIONSNone.
5 WARNINGS AND PRECAUTIONS
5.1 Severe and Fatal Immune-Mediated Adverse ReactionsYERVOY is a fully human monoclonal antibody that blocks T-cell inhibitory signals inducedby the CTLA-4 pathway, thereby removing inhibition of the immune response with thepotential for induction of immune-mediated adverse reactions. Immune-mediatedadverse reactions listed herein may not be inclusive of all possible severe and fatalimmune-mediated reactions.Immune-mediated adverse reactions, which may be severe or fatal, can occur in anyorgan system or tissue. Immune-mediated adverse reactions can occur at any timeafter starting YERVOY. While immune-mediated adverse reactions usually manifestduring treatment, immune-mediated adverse reactions can also manifest afterdiscontinuation of YERVOY.Early identification and management are essential to ensure safe use of YERVOY.Monitor for signs and symptoms that may be clinical manifestations of underlyingimmune-mediated adverse reactions. Evaluate clinical chemistries including liverenzymes, creatinine, adrenocorticotropic hormone (ACTH) level, and thyroid function atbaseline and before each dose. Institute medical management promptly, includingspecialty consultation as appropriate.Withhold or permanently discontinue YERVOY depending on severity [see Dosage andAdministration (2.3)]. In general, if YERVOY requires interruption or discontinuation,administer systemic corticosteroid therapy (1 to 2 mg/kg/day prednisone or equivalent)until improvement to Grade 1 or less. Upon improvement to Grade 1 or less, initiatecorticosteroid taper and continue to taper over at least 1 month. Consideradministration of other systemic immunosuppressants in patients whose immune-mediated adverse reactions are not controlled with corticosteroid therapy.
Do not co-administer other drugs through the same intravenous line.Flush the intravenous line with 0.9% Sodium Chloride Injection, USP or 5% DextroseInjection, USP after each dose.Administer diluted solution through an intravenous line containing a sterile, non-pyrogenic, low-protein-binding in-line filter.When administered in combination with nivolumab, infuse nivolumab first followedby YERVOY on the same day. When administered with nivolumab and platinum-doublet chemotherapy, infuse nivolumab first followed by YERVOY and thenplatinum-doublet chemotherapy on the same day. Use separate infusion bags andfilters for each infusion.

Immune-Mediated ColitisYERVOY can cause immune-mediated colitis, which may be fatal. Cytomegalovirus (CMV)infection/reactivation has been reported in patients with corticosteroid-refractoryimmune-mediated colitis. In cases of corticosteroid-refractory colitis, consider repeatinginfectious workup to exclude alternative etiologies.YERVOY 3 mg/kg as a Single Agent
Immune-mediated colitis occurred in 12% (62/511) of patients who received YERVOY 3mg/kg as a single agent, including Grade 3-5 (7%) and Grade 2 (5%). Colitis led topermanent discontinuation of YERVOY in 4.3% and withholding of at least one dose ofYERVOY in 0.2% of patients.Systemic corticosteroids were required in 74% (46/62) of patients with immune-mediated colitis. Five patients required coadministration of another immunosuppressantwith corticosteroids. Colitis resolved in 76% of the 62 patients. One patient was withheldone or more doses of YERVOY for colitis, and no patient received additional treatmentafter symptom improvement.YERVOY 10 mg/kg as a Single Agent
Immune-mediated colitis occurred in 31% (144/471) of patients who received YERVOY10 mg/kg as a single agent, including fatal (0.2%), Grade 4 (1.5%), Grade 3 (14%), andGrade 2 (14%). Colitis led to permanent discontinuation of YERVOY in 61% of patientsand 3.8% of patients missed at least one dose of YERVOY due to colitis.Systemic corticosteroids were required in 85% (123/144) of patients with immune-mediated colitis. Approximately 26% of the 144 patients required coadministration ofanother immunosuppressant with corticosteroids. Colitis resolved in 90% of the 144patients. Of the 18 patients who missed one or more doses of YERVOY for colitis, 17received additional treatment after symptom improvement; of these, 14 had recurrenceof colitis.YERVOY 1 mg/kg with 3 mg/kg Nivolumab
Immune-mediated colitis occurred in 9% (60/666) of patients who received YERVOY 1mg/kg with nivolumab for the treatment of RCC or mCRC, including Grade 3 (4.4%), andGrade 2 (3.7%). Colitis led to permanent discontinuation of YERVOY and nivolumab in3.2% and withholding of YERVOY and nivolumab in 2.7% of patients.In patients who received YERVOY 1 mg/kg with nivolumab, use of systemiccorticosteroids was one of the diagnostic criteria required to identify immune-mediatedcolitis. Systemic corticosteroids were therefore required in 100% (60/60) of patientswith immune-mediated colitis. Approximately 23% of patients required coadministrationof another immunosuppressant with corticosteroids. Colitis resolved in 95% of the 60patients. Of the 18 patients in whom YERVOY or nivolumab was withheld for colitis, 16received additional treatment after symptom improvement; of these, 10 had recurrenceof colitis.YERVOY 3 mg/kg with 1 mg/kg Nivolumab
Immune-mediated colitis occurred in 25% (115/456) of patients with melanoma or HCCreceiving YERVOY 3 mg/kg with nivolumab 1 mg/kg every 3 weeks, including Grade 4(0.4%), Grade 3 (14%), and Grade 2 (8%) adverse reactions. Colitis led to permanent

discontinuation of YERVOY with nivolumab in 14% and withholding of treatment in 4.4%of patients.Systemic corticosteroids were required in 100% (115/115) of patients with colitis.Approximately 23% of patients required addition of infliximab to high-dosecorticosteroids. Colitis resolved in 93% of 115 patients. Of the 20 patients in whomYERVOY with nivolumab was withheld for colitis, 16 reinitiated treatment after symptomimprovement, and 9 had recurrence of colitis.Immune-Mediated HepatitisYERVOY 3 mg/kg as a Single Agent
Immune-mediated hepatitis occurred in 4.1% (21/511) of patients who received YERVOY3 mg/kg as a single agent, including Grade 3-5 (1.6%) and Grade 2 (2.5%). Hepatitis ledto permanent discontinuation of YERVOY in 0.4% of patients and withholding of at leastone dose of YERVOY in none of the patients.Systemic corticosteroids were required in 29% (6/21) of patients with immune-mediatedhepatitis. No patients required the coadministration of another immunosuppressant withcorticosteroids. Hepatitis resolved in 86% of the 21 patients.YERVOY 10 mg/kg as a Single Agent
Immune-mediated hepatitis occurred in 15% (73/471) of patients who received YERVOY10 mg/kg as a single agent, including Grade 4 (2.8%), Grade 3 (8%), and Grade 2 (5%).Hepatitis led to permanent discontinuation of YERVOY in 56% of patients and 1.1% ofpatients missed at least one dose of YERVOY due to hepatitis.Systemic corticosteroids were required in 85% (62/73) of patients with immune-mediated hepatitis. Approximately 15% of the 73 patients required the coadministrationof another immunosuppressant with corticosteroids. Hepatitis resolved in 93% of 73patients. Of the 5 patients who missed one or more doses of YERVOY for hepatitis, 5received additional treatment after symptom improvement; of these, 1 had recurrenceof hepatitis.YERVOY 3 mg/kg with Vemurafenib
The safety and effectiveness of YERVOY in combination with vemurafenib have not beenestablished [see Indications and Usage (1)]. In a dose-finding trial, Grade 3 increases intransaminases with or without concomitant increases in total bilirubin occurred in 6 of10 patients who received concurrent YERVOY (3 mg/kg) and vemurafenib (960 mg or720 mg twice daily).YERVOY 1 mg/kg with 3 mg/kg Nivolumab
Immune-mediated hepatitis occurred in 7% (48/666) of patients who received YERVOY 1mg/kg with nivolumab for the treatment of RCC or mCRC, including Grade 4 (1.2%),Grade 3 (4.9%), and Grade 2 (0.4%). Hepatitis led to permanent discontinuation ofYERVOY and nivolumab in 3.6% and withholding of YERVOY and nivolumab in 2.6% ofpatients.In patients who received YERVOY 1 mg/kg with nivolumab, use of systemiccorticosteroids was one of the diagnostic criteria required to identify immune-mediatedhepatitis. Systemic corticosteroids were therefore required in 100% (48/48) of patientswith immune-mediated hepatitis. Approximately 19% of patients required
coadministration of another immunosuppressant with corticosteroids. Hepatitis resolvedin 88% of the 48 patients. Of the 17 patients in whom YERVOY or nivolumab waswithheld for hepatitis, 14 received additional treatment after symptom improvement; ofthese, 10 had recurrence of hepatitis.YERVOY 3 mg/kg with 1 mg/kg Nivolumab
Immune-mediated hepatitis occurred in 15% (70/456) of patients with melanoma or HCCreceiving YERVOY 3 mg/kg with nivolumab 1 mg/kg every 3 weeks, including Grade 4(2.4%), Grade 3 (11%), and Grade 2 (1.8%) adverse reactions. Immune-mediatedhepatitis led to permanent discontinuation of YERVOY with nivolumab in 8% andwithholding of treatment in 3.5% of patients.Systemic corticosteroids were required in 100% (70/70) of patients with hepatitis.Approximately 9% of patients with immune-mediated hepatitis required addition ofmycophenolic acid to high-dose corticosteroids. Hepatitis resolved in 91% of the 70patients. Of the 16 patients in whom YERVOY with nivolumab was withheld for hepatitis,14 reinitiated treatment after symptom improvement, and 8 had recurrence of hepatitis.Immune-Mediated Dermatologic Adverse ReactionsYERVOY can cause immune-mediated rash or dermatitis, including bullous and exfoliativedermatitis, Stevens Johnson Syndrome, toxic epidermal necrolysis (TEN), and DRESS(Drug Rash with Eosinophilia and Systemic Symptoms). Topical emollients and/or topicalcorticosteroids may be adequate to treat mild to moderate non-bullous/exfoliativerashes. Withhold or permanently discontinue YERVOY depending on severity [seeDosage and Administration (2.3)].YERVOY 3 mg/kg as a Single Agent
Immune-mediated rash occurred in 15% (76/511) of patients who received YERVOY 3mg/kg as a single agent, including Grade 3-5 (2.5%) and Grade 2 (12%). Rash led topermanent discontinuation of YERVOY in 0.2% and withholding of at least one dose ofYERVOY in 1.4% of patients.Systemic corticosteroids were required in 43% (33/76) of patients with immune-mediated rash. Rash resolved in 71% of the 76 patients. Of the 7 patients in whomYERVOY was withheld for rash, 3 received additional treatment after symptomimprovement; of these, 1 had recurrence of rash.YERVOY 10 mg/kg as a Single Agent
Immune-mediated rash occurred in 25% (118/471) of patients who received YERVOY 10mg/kg as a single agent, including Grade 3 (4%) and Grade 2 (21%). Rash led topermanent discontinuation in 8% of patients and 1.5% of patients missed at least onedose of YERVOY due to rash.Systemic corticosteroids were required in 70% (83/118) of patients with immune-mediated rash. Rash resolved in 81% of 118 patients. Of the 7 patients who missed oneor more doses of YERVOY for rash, 5 received additional treatment after symptomimprovement; of these, 3 had recurrence of rash.YERVOY 1 mg/kg with 3 mg/kg Nivolumab
Immune-mediated rash occurred in 16% (108/666) of patients who received YERVOY 1mg/kg with nivolumab for the treatment of RCC or mCRC, including Grade 3 (3.5%) and

Grade 2 (4.2%). Rash led to permanent discontinuation of YERVOY and nivolumab in0.5% of patients and withholding of YERVOY and nivolumab in 2.0% of patients.In patients who received YERVOY 1 mg/kg with nivolumab, use of systemiccorticosteroids was one of the diagnostic criteria required to identify immune-mediatedrash. Systemic corticosteroids were therefore required in 100% (108/108) of patients.Rash resolved in 75% of 108 patients. Of the 13 patients in whom YERVOY or nivolumabwas withheld for rash, 11 received additional treatment after symptom improvement; ofthese, 5 had recurrence of rash.YERVOY 3 mg/kg with 1 mg/kg Nivolumab
Immune-mediated rash occurred in 28% (127/456) of patients with melanoma or HCCreceiving YERVOY 3 mg/kg with nivolumab 1 mg/kg every 3 weeks, including Grade 3(4.8%) and Grade 2 (10%) adverse reactions. Immune-mediated rash led to permanentdiscontinuation of YERVOY with nivolumab in 0.4% and withholding of treatment in 3.9%of patients.Systemic corticosteroids were required in 100% (127/127) of patients with immune-mediated rash. Rash resolved in 84% of the 127 of patients. Of the 18 patients in whomYERVOY with nivolumab was withheld for rash, 15 reinitiated treatment after symptomimprovement, and 8 had recurrence of rash.Immune-Mediated EndocrinopathiesYERVOY 3 mg/kg as a Single Agent
Grade 2-5 immune-mediated endocrinopathies occurred in 4% (21/511) of patients whoreceived YERVOY 3 mg/kg as a single agent.Severe to life-threatening (Grade 3-4) endocrinopathies occurred in 9 patients (1.8%). All9 of these patients had hypopituitarism with some patients having additionalconcomitant endocrinopathies, such as adrenal insufficiency, hypogonadism, andhypothyroidism. Six of the 9 patients were hospitalized for severe endocrinopathies.Moderate (Grade 2) endocrinopathy occurred in 12 patients (2.3%), includinghypothyroidism, adrenal insufficiency, hypopituitarism, hyperthyroidism and Cushing’ssyndrome.Of the 21 patients with moderate to life-threatening endocrinopathy, 17 required long-term hormone replacement therapy, including adrenal hormones (n=10) and thyroidhormones (n=13).YERVOY 10 mg/kg as a Single Agent
Immune-mediated endocrinopathies occurred in 28% of patients (132/471), includingGrade 4 (0.6%), Grade 3 (8%) and Grade 2 (20%).Of the 39 patients with Grade 3 to 4 endocrinopathies, 35 patients had hypopituitarism(associated with one or more secondary endocrinopathies, e.g., adrenal insufficiency,hypogonadism, and hypothyroidism), 3 patients had hyperthyroidism, and 1 hadprimary hypothyroidism. Twenty-seven of the 39 patients (69%) were hospitalized forendocrinopathies. Of the 39 patients, 10% were reported to have resolution.Of the 93 patients with Grade 2 endocrinopathy, 74 had primary hypopituitarismassociated with one or more secondary endocrinopathy, e.g., adrenal insufficiency,hypogonadism, and hypothyroidism, 9 had primary hypothyroidism, 3 had

hyperthyroidism, 3 had thyroiditis with hypo- or hyperthyroidism, 2 had hypogonadism,1 had both hyperthyroidism and hypopituitarism, and 1 subject developed Graves’ophthalmopathy. Of the 93 patients, 20% were reported to have resolution.One hundred twenty-four patients received systemic corticosteroids asimmunosuppression and/or adrenal hormone replacement for Grade 2 to 4endocrinopathy. Of these, 42 (34%) were able to discontinue corticosteroids. Seventy-three patients received thyroid hormones for treatment of Grade 2 to 4 hypothyroidism.Of these, 14 patients (19%) were able to discontinue thyroid replacement therapy.YERVOY 1 mg/kg with 3 mg/kg Nivolumab
Hypophysitis:
YERVOY can cause immune-mediated hypophysitis. Hypophysitis can present with acutesymptoms associated with mass effect such as headache, photophobia, or visual fieldcuts. Hypophysitis can cause hypopituitarism. Initiate hormone replacement as clinicallyindicated. Withhold or permanently discontinue YERVOY depending on severity [seeDosage and Administration (2.3)].Hypophysitis occurred in 4.4% (29/666) of patients who received YERVOY 1 mg/kg withnivolumab for the treatment of RCC or mCRC, including Grade 4 (0.3%), Grade 3 (2.4%),and Grade 2 (0.9%). Hypophysitis led to permanent discontinuation of YERVOY andnivolumab in 1.2% and withholding of YERVOY with nivolumab in 2.1% of patients.Approximately 72% of patients with hypophysitis received hormone replacementtherapy. Systemic corticosteroids were required in 72% (21/29) of patients withimmune-mediated hypophysitis. Hypophysitis resolved in 59% of the 29 patients. Of the14 patients in whom YERVOY or nivolumab was withheld for hypophysitis, 11 receivedadditional treatment after symptom improvement; of these, 2 had recurrence ofhypophysitis.Adrenal Insufficiency:
Adrenal insufficiency occurred in 7% (48/666) of patients who received YERVOY 1 mg/kgwith nivolumab for the treatment of RCC or mCRC, including Grade 4 (0.3%), Grade 3(2.5%), and Grade 2 (4.1%). Adrenal insufficiency led to permanent discontinuation ofYERVOY with nivolumab in 1.2% and withholding of YERVOY with nivolumab in 2.1% ofpatients. Approximately 94% of patients with adrenal insufficiency received hormonereplacement therapy. Systemic corticosteroids were required in 94% (45/48) of patientswith adrenal insufficiency. Adrenal insufficiency resolved in 29% of the 48 patients. Ofthe 14 patients in whom YERVOY or nivolumab was withheld for adrenal insufficiency, 11received additional treatment after symptom improvement; of these, 2 had recurrenceof adrenal insufficiency.Hyperthyroidism:
Hyperthyroidism occurred in 12% (80/666) of patients who received YERVOY 1 mg/kgwith nivolumab for the treatment of RCC or mCRC, including Grade 3 (0.6%) and Grade2 (4.5%). No patients discontinued YERVOY for hyperthyroidism. Hyperthyroidism led towithholding of YERVOY with nivolumab in 2.3% of patients. Approximately 19% receiveda thyroid synthesis inhibitor. Systemic corticosteroids were required in 20% (16/80) ofpatients with hyperthyroidism. Hyperthyroidism resolved in 85% of the 80 patients. Ofthe 15 patients in whom YERVOY or nivolumab was withheld for hyperthyroidism, 11received additional treatment after symptom improvement; of these, 3 had recurrence
of hyperthyroidism.Hypothyroidism:
Hypothyroidism occurred in 18% (122/666) of patients who received YERVOY 1 mg/kgwith nivolumab for the treatment of RCC or mCRC, including Grade 3 (0.6%) and Grade2 (11%). Hypothyroidism led to permanent discontinuation of YERVOY with nivolumab in0.2% and withholding of YERVOY with nivolumab in 1.4% of patients. Approximately 82%received thyroid hormone replacement. Systemic corticosteroids were required in 7%(9/122) of patients with hypothyroidism. Hypothyroidism resolved in 27% of the 122patients. Of the 9 patients in whom YERVOY or nivolumab was withheld forhypothyroidism, 5 received additional treatment after symptom improvement; of these,one patient had recurrence of hypothyroidism.Thyroiditis:
Thyroiditis occurred in 2.7% (22/666) of patients who received YERVOY 1 mg/kg withnivolumab for the treatment of RCC or mCRC, including Grade 3 (4.5%) and Grade 2(2.2%). Thyroiditis led to permanent discontinuation of YERVOY with nivolumab in 0.2%and withholding of YERVOY with nivolumab in 0.8% of patients. Systemic corticosteroidswere required in 18% (4/22) of patients with thyroiditis. Thyroiditis resolved in 64% ofthe 22 patients. Of the 5 patients in whom YERVOY or nivolumab was withheld forthyroiditis, 5 received additional treatment after symptom improvement; of these, nopatients had recurrence of thyroiditis.Type 1 Diabetes Mellitus:
Diabetes occurred in 2.7% (15/666) of patients who received YERVOY 1 mg/kg withnivolumab for the treatment of RCC or mCRC, including Grade 4 (0.6%), Grade 3 (0.3%),and Grade 2 (0.9%). Diabetes led to the permanent discontinuation of YERVOY withnivolumab in 0.5% and withholding of YERVOY with nivolumab in 0.5% of patients.Systemic corticosteroids were required in 7% (1/15) of patients with diabetes. Diabetesresolved in 27% of the 15 patients. Of the 3 patients in whom YERVOY or nivolumab waswithheld for diabetes, 2 received additional treatment after symptom improvement; ofthese, none had recurrence of diabetes.YERVOY 3 mg/kg with 1 mg/kg Nivolumab
Hypophysitis:
Hypophysitis occurred in 9% (42/456) of patients with melanoma or HCC receivingYERVOY 3 mg/kg with nivolumab 1 mg/kg every 3 weeks, including Grade 3 (2.4%) andGrade 2 (6%) adverse reactions. Hypophysitis led to permanent discontinuation ofYERVOY with nivolumab in 0.9% and withholding of treatment in 4.2% of patients.Approximately 86% of patients with hypophysitis received hormone replacementtherapy. Systemic corticosteroids were required in 88% (37/42) of patients withhypophysitis. Hypophysitis resolved in 38% of the 42 patients. Of the 19 patients inwhom YERVOY with nivolumab was withheld for hypophysitis, 9 reinitiated treatmentafter symptom improvement, and 1 had recurrence of hypophysitis.Adrenal Insufficiency:
Adrenal insufficiency occurred in 8% (35/456) of patients with melanoma or HCCreceiving YERVOY 3 mg/kg with nivolumab 1 mg/kg every 3 weeks, including Grade 4(0.2%), Grade 3 (2.4%), and Grade 2 (4.2%) adverse reactions. Adrenal insufficiency led
to permanent discontinuation of YERVOY with nivolumab in 0.4% of patients andwithholding of treatment in 2.0% of patients.Approximately 71% (25/35) of patients with adrenal insufficiency received hormonereplacement therapy, including systemic corticosteroids. Adrenal insufficiency resolvedin 37% of the 35 patients. Of the 9 patients in whom YERVOY with nivolumab waswithheld for adrenal insufficiency, 7 reinitiated treatment after symptom improvement,and all required hormone replacement therapy for their ongoing adrenal insufficiency.Hypothyroidism:
Hypothyroidism occurred in 20% (91/456) of patients with melanoma or HCC receivingYERVOY 3 mg/kg with nivolumab 1 mg/kg every 3 weeks, including Grade 3 (0.4%) andGrade 2 (11%) adverse reactions. Hypothyroidism led to permanent discontinuation ofYERVOY with nivolumab in 0.9% of patients and withholding of treatment in 0.9% ofpatients.Approximately 89% of patients with hypothyroidism received levothyroxine. Systemiccorticosteroids were required in 2.2% (2/91) of patients with hypothyroidism.Hypothyroidism resolved in 41% of the 91 patients. Of the 4 patients in whom YERVOYwith nivolumab was withheld for hypothyroidism, 2 reinitiated treatment after symptomimprovement, and none had recurrence of hypothyroidism.Hyperthyroidism:
Hyperthyroidism occurred in 9% (42/456) of patients with melanoma or HCC receivingYERVOY 3 mg/kg with nivolumab 1 mg/kg every 3 weeks, including Grade 3 (0.9%) andGrade 2 (4.2%) adverse reactions. Hyperthyroidism led to permanent discontinuation ofYERVOY with nivolumab in no patients and withholding of treatment in 2.4% of patients.Approximately 26% of patients with hyperthyroidism received methimazole and 21%received carbimazole. Systemic corticosteroids were required in 17% (7/42) of patients.Hyperthyroidism resolved in 91% of the 42 patients. Of the 11 patients in whomYERVOY with nivolumab was withheld for hyperthyroidism, 8 reinitiated treatment aftersymptom improvement, and 1 had recurrence of hyperthyroidism.Immune-Mediated PneumonitisYERVOY 1 mg/kg with 3 mg/kg Nivolumab
Immune-mediated pneumonitis occurred in 3.9% (26/666) of patients who receivedYERVOY 1 mg/kg with nivolumab for the treatment of RCC or mCRC, including Grade 3(1.4%) and Grade 2 (2.6%). Pneumonitis led to permanent discontinuation of YERVOYand nivolumab in 1.8% and withholding of YERVOY and nivolumab in 1.5% of patients.In patients who received YERVOY 1 mg/kg with nivolumab, use of systemiccorticosteroids was one of the diagnostic criteria required to identify immune-mediatedpneumonitis. Systemic corticosteroids were therefore required in 100% (26/26) ofpatients with immune-mediated pneumonitis. Approximately 8% requiredcoadministration of another immunosuppressant with corticosteroids. Pneumonitisresolved in 92% of the 26 patients. Of the 10 patients in whom YERVOY or nivolumabwas withheld for pneumonitis, 10 received additional treatment after symptomimprovement; of these, 4 had recurrence of pneumonitis.In NSCLC, immune-mediated pneumonitis occurred in 9% (50/576) of patients receivingYERVOY 1 mg/kg every 6 weeks with nivolumab 3 mg/kg every 2 weeks, including Grade

4 (0.5%), Grade 3 (3.5%), and Grade 2 (4.0%) immune-mediated pneumonitis. Fourpatients (0.7%) died due to pneumonitis. The median duration was 1.5 months (range: 5days to 25+ months). Immune-mediated pneumonitis led to permanent discontinuationof YERVOY with nivolumab in 5% of patients and withholding of YERVOY with nivolumabin 3.6% of patients.Systemic corticosteroids were required in 100% of patients with pneumonitis followed bya corticosteroid taper. Pneumonitis resolved in 72% of the patients. Approximately 13%(2/16) of patients had recurrence of pneumonitis after re-initiation of YERVOY withnivolumab.YERVOY 3 mg/kg with 1 mg/kg Nivolumab
Immune-mediated pneumonitis occurred in 7% (31/456) of patients who receivedYERVOY 3 mg/kg with nivolumab for the treatment of HCC or melanoma, including Grade4 (0.2%), Grade 3 (2.0%), and Grade 2 (4.4%). Immune-mediated pneumonitis led topermanent discontinuation or withholding of treatment in 2.9% and 3.9% of patients,respectively.Systemic corticosteroids were required in 100% of patients with pneumonitis.Pneumonitis resolved in 94% of the patients. Of the 13 patients in whom YERVOY ornivolumab was withheld for pneumonitis, 13 received additional treatment aftersymptom improvement, and 4 had recurrence of pneumonitis.Immune-Mediated Nephritis with Renal DysfunctionYERVOY 1 mg/kg with 3 mg/kg Nivolumab
Immune-mediated nephritis with renal dysfunction occurred in 4.1% (27/666) of patientswho received YERVOY 1 mg/kg with nivolumab for the treatment of RCC or mCRC,including Grade 4 (0.6%), Grade 3 (1.1%), and Grade 2 (2.2%). Nephritis with renaldysfunction led to permanent discontinuation of YERVOY and nivolumab in 1.2% andwithholding of nivolumab and YERVOY in 1.8% of patients.In patients who received YERVOY 1 mg/kg with nivolumab, use of systemiccorticosteroids was one of the diagnostic criteria required to identify immune-mediatednephritis with renal dysfunction. Systemic corticosteroids were therefore required in100% (27/27) of patients with immune-mediated nephritis with renal dysfunction.Nephritis with renal dysfunction resolved in 67% of the 27 patients. Of the 12 patients inwhom YERVOY or nivolumab was withheld for nephritis, 10 received additional treatmentafter symptom improvement; of these, 4 had recurrence of nephritis.Other Immune-Mediated Adverse ReactionsAcross clinical trials of YERVOY administered as a single agent or in combination withnivolumab, the following clinically significant immune-mediated adverse reactions, somewith fatal outcome, occurred in <1% of patients unless otherwise specified, as shownbelow:Nervous System: Autoimmune neuropathy (2%), meningitis, encephalitis, myelitis anddemyelination, myasthenic syndrome/myasthenia gravis, Guillain-Barré syndrome, nerveparesis, motor dysfunctionCardiovascular: Angiopathy, myocarditis, pericarditis, temporal arteritis, vasculitisOcular: Blepharitis, episcleritis, iritis, orbital myositis, scleritis, uveitis. Some cases can be

associated with retinal detachment. If uveitis occurs in combination with other immune-mediated adverse reactions, consider a Vogt-Koyanagi-Harada-like syndrome, which hasbeen observed in patients receiving YERVOY and may require treatment with systemiccorticosteroids to reduce the risk of permanent vision loss.Gastrointestinal: Duodenitis, gastritis, pancreatitis (1.3%)Musculoskeletal and Connective Tissue: Arthritis, myositis, polymyalgia rheumatica,polymyositis, rhabdomyolysisOther (hematologic/immune): Aplastic anemia, conjunctivitis, cytopenias (2.5%),eosinophilia (2.1%), erythema multiforme, histiocytic necrotizing lymphadenitis (Kikuchilymphadenitis), hypersensitivity vasculitis, meningitis, neurosensory hypoacusis,psoriasis, sarcoidosis, systemic inflammatory response syndrome, and solid organtransplant rejection.
5.2 Infusion-Related ReactionsSevere infusion-related reactions can occur with YERVOY. Discontinue YERVOY inpatients with severe or life-threatening infusion reactions. Interrupt or slow the rate ofinfusion in patients with mild or moderate infusion reactions [see Dosage andAdministration (2.3)]. Infusion-related reactions occurred in 2.9% (28/982) of patientswho received single-agent YERVOY 3 mg/kg or 10 mg/kg for the treatment ofmelanoma. Infusion-related reactions occurred in 5% (33/666) of patients who receivedYERVOY 1 mg/kg with nivolumab for the treatment of RCC or CRC. Infusion-relatedreactions occurred in 8% (4/49) of patients who received YERVOY 3 mg/kg withnivolumab for the treatment of HCC. Infusion-related reactions occurred in 12%(37/300) of patients with malignant pleural mesothelioma who received YERVOY 1 mg/kgevery 6 weeks with nivolumab 3 mg/kg every 2 weeks.
5.3 Complications of Allogeneic Hematopoietic Stem Cell Transplant afterYERVOYFatal or serious graft-versus-host disease (GVHD) can occur in patients who receiveYERVOY either before or after allogeneic hematopoietic stem cell transplantation (HSCT).These complications may occur despite intervening therapy between CTLA-4 receptorblocking antibody and allogeneic HSCT.Follow patients closely for evidence of GVHD and intervene promptly [see AdverseReactions (6.3)]. Consider the benefit versus risks of treatment with YERVOY afterallogeneic HSCT.
5.4 Embryo-Fetal ToxicityBased on its mechanism of action and findings from animal studies, YERVOY can causefetal harm when administered to a pregnant woman. In animal reproduction studies,administration of ipilimumab to cynomolgus monkeys from the onset of organogenesisthrough delivery resulted in higher incidences of abortion, stillbirth, premature delivery(with corresponding lower birth weight) and higher incidences of infant mortality in adose-related manner. The effects of ipilimumab are likely to be greater during the secondand third trimesters of pregnancy. Advise pregnant women of the potential risk to afetus. Advise females of reproductive potential to use effective contraception duringtreatment with YERVOY and for 3 months after the last dose [see Use in Specific
Populations (8.1, 8.3)].
5.5 Risks Associated When Administered in Combination with NivolumabYERVOY is indicated for use in combination with nivolumab for patients with advancedRCC, MSI-H or dMMR mCRC, HCC, and NSCLC. Refer to the nivolumab Full PrescribingInformation for additional risk information that applies to the combination use treatment.
6 ADVERSE REACTIONSThe following clinically significant adverse reactions are described elsewhere in thelabeling:
•
•
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reactionrates observed in the clinical trials of a drug cannot be directly compared with rates inthe clinical trials of another drug and may not reflect the rates observed in clinicalpractice.The data described in the Warnings and Precautions section reflect exposure to YERVOY3 mg/kg as a single agent (or in combination with an investigational gp100 peptidevaccine) in 511 patients in Study MDX010-20; YERVOY 10 mg/kg as a single agent in 471patients in Study CA184-029; YERVOY 1 mg/kg administered with nivolumab 3 mg/kg in1,362 patients in CHECKMATE-214, CHECKMATE-142, CHECKMATE-227, andCHECKMATE-743; YERVOY 3 mg/kg administered with nivolumab 1 mg/kg in 456 patientsenrolled in CHECKMATE-067, CHECKMATE-040, and another randomized trial; and toYERVOY 1 mg/kg, administered in combination with nivolumab and platinum-doubletchemotherapy in CHECKMATE-9LA.
Unresectable or Metastatic MelanomaThe safety of YERVOY was evaluated in 643 previously treated patients withunresectable or metastatic melanoma in Study MDX010-20 [see Clinical Studies (14.1)].Study MDX010-20 excluded patients with active autoimmune disease or those receivingsystemic immunosuppression for organ transplantation. Patients received YERVOY 3mg/kg by intravenous infusion for 4 doses as a single agent (n=131), YERVOY with aninvestigational gp100 peptide vaccine (n=380), or gp100 peptide vaccine as a singleagent (n=132). Patients in the trial received a median of 4 doses (range: 1 to 4 doses).The trial population characteristics were: median age 57 years (range: 19 to 90), 59%male, 94% White, and baseline ECOG performance status 0 (56%).YERVOY was discontinued for adverse reactions in 10% of patients. Table 4 presentsadverse reactions from Study MDX010-20.
Table 4: Selected Adverse Reactions (≥5%) in Patients Receiving YERVOYwith a Difference Between Arms of >5% for All Grades and >1% for Grades
Severe and fatal immune-mediated adverse reactions [see Warnings andPrecautions (5.1)].Infusion-related reactions [see Warnings and Precautions (5.2)].

3 to 5 Compared to gp100 Peptide Vaccine in Study MDX010-20Adverse Reactions
YERVOY 3mg/kgn=131
YERVOY 3mg/kg and
gp100n=380
gp100n=132
AllGrades
(%)
Grade3 to 5(%)
AllGrades
(%)
Grade3 to 5(%)
AllGrades
(%)
Grade3 to 5(%)
General and Administration-Site Conditions Fatigue 41 7 34 5 31 3Gastrointestinal Diarrhea 32 5 37 4 20 1 Colitis 8 5 5 3 2 0Dermatologic Pruritus 31 0 21 <1 11 0 Rash 29 2 25 2 8 0
Unresectable or Metastatic Melanoma: In Combination with NivolumabThe safety of YERVOY, administered with nivolumab or as a single agent, was evaluatedin CHECKMATE-067, a randomized (1:1:1), double-blind trial in 937 patients withpreviously untreated, unresectable or metastatic melanoma [see Clinical Studies (14.1)].The trial excluded patients with autoimmune disease, a medical condition requiringsystemic treatment with corticosteroids (more than 10 mg daily prednisone equivalent)or other immunosuppressive medication within 14 days of the start of study therapy, apositive test result for hepatitis B or C, or a history of HIV.Patients were randomized to receive:
•
•
•
The median duration of exposure to nivolumab was 2.8 months (range: 1 day to 36.4months) for the YERVOY and nivolumab arm. In the YERVOY and nivolumab arm, 39%were exposed to nivolumab for ≥6 months and 30% exposed for >1 year.Serious adverse reactions (74%), adverse reactions leading to permanentdiscontinuation (47%) or to dosing delays (58%), and Grade 3 or 4 adverse reactions(72%) occurred in patients treated with YERVOY and nivolumab.The most frequent (≥10%) serious adverse reactions in the YERVOY and nivolumab armwere diarrhea (13%), colitis (10%), and pyrexia (10%). The most frequent adversereactions leading to discontinuation of both drugs in the YERVOY and nivolumab armwere colitis (10%), diarrhea (8%), increased ALT (4.8%), increased AST (4.5%), and
YERVOY 3 mg/kg by intravenous infusion over 90 minutes with nivolumab 1 mg/kgby intravenous infusion every 3 weeks for 4 doses followed by nivolumab as asingle agent at a dose of 3 mg/kg by intravenous infusion every 2 weeks (YERVOYand nivolumab arm; n=313), orNivolumab 3 mg/kg by intravenous infusion every 2 weeks (nivolumab arm;n=313), orYERVOY 3 mg/kg by intravenous infusion over 90 minutes every 3 weeks for up to4 doses (YERVOY arm; n=311).
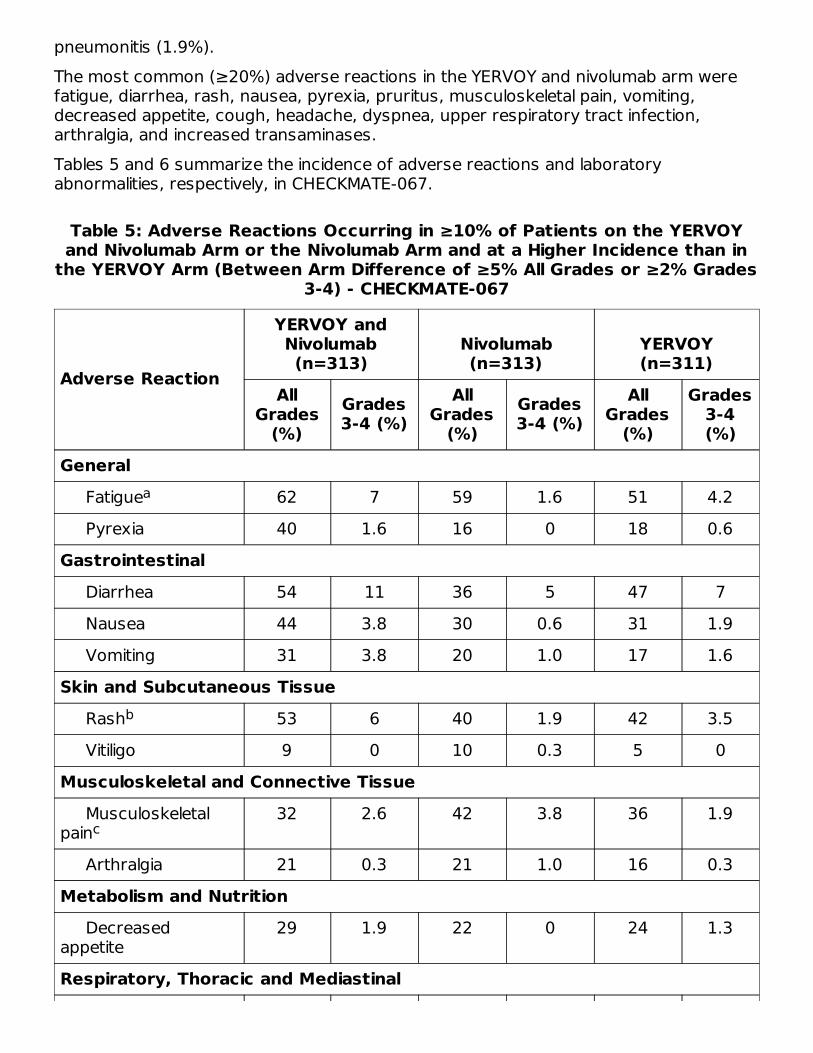
pneumonitis (1.9%).The most common (≥20%) adverse reactions in the YERVOY and nivolumab arm werefatigue, diarrhea, rash, nausea, pyrexia, pruritus, musculoskeletal pain, vomiting,decreased appetite, cough, headache, dyspnea, upper respiratory tract infection,arthralgia, and increased transaminases.Tables 5 and 6 summarize the incidence of adverse reactions and laboratoryabnormalities, respectively, in CHECKMATE-067.
Table 5: Adverse Reactions Occurring in ≥10% of Patients on the YERVOYand Nivolumab Arm or the Nivolumab Arm and at a Higher Incidence than in
the YERVOY Arm (Between Arm Difference of ≥5% All Grades or ≥2% Grades3-4) - CHECKMATE-067
Adverse Reaction
YERVOY andNivolumab(n=313)
Nivolumab(n=313)
YERVOY(n=311)
AllGrades
(%)Grades3-4 (%)
AllGrades
(%)Grades3-4 (%)
AllGrades
(%)
Grades3-4(%)
General Fatigue 62 7 59 1.6 51 4.2 Pyrexia 40 1.6 16 0 18 0.6Gastrointestinal Diarrhea 54 11 36 5 47 7 Nausea 44 3.8 30 0.6 31 1.9 Vomiting 31 3.8 20 1.0 17 1.6Skin and Subcutaneous Tissue Rash 53 6 40 1.9 42 3.5 Vitiligo 9 0 10 0.3 5 0Musculoskeletal and Connective Tissue Musculoskeletalpain
32 2.6 42 3.8 36 1.9
Arthralgia 21 0.3 21 1.0 16 0.3Metabolism and Nutrition Decreasedappetite
29 1.9 22 0 24 1.3
Respiratory, Thoracic and Mediastinal
a
b
c
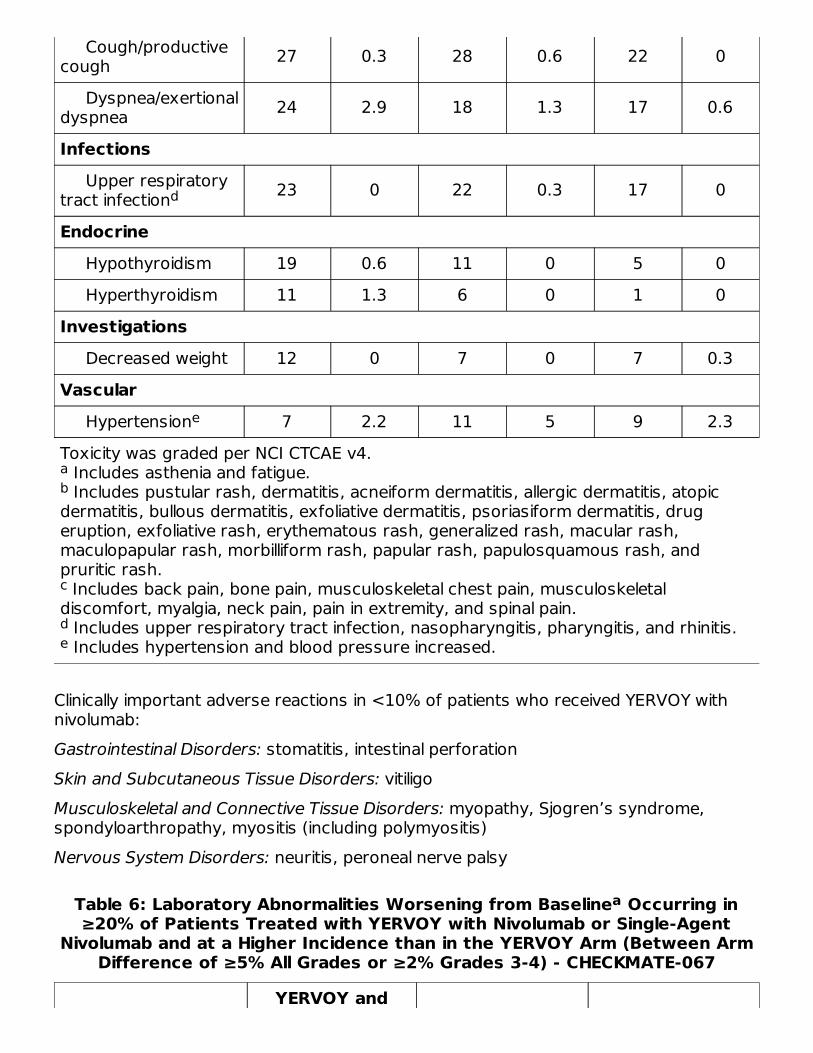
Toxicity was graded per NCI CTCAE v4. Includes asthenia and fatigue. Includes pustular rash, dermatitis, acneiform dermatitis, allergic dermatitis, atopic
dermatitis, bullous dermatitis, exfoliative dermatitis, psoriasiform dermatitis, drugeruption, exfoliative rash, erythematous rash, generalized rash, macular rash,maculopapular rash, morbilliform rash, papular rash, papulosquamous rash, andpruritic rash. Includes back pain, bone pain, musculoskeletal chest pain, musculoskeletal
discomfort, myalgia, neck pain, pain in extremity, and spinal pain. Includes upper respiratory tract infection, nasopharyngitis, pharyngitis, and rhinitis. Includes hypertension and blood pressure increased.
Cough/productivecough 27 0.3 28 0.6 22 0
Dyspnea/exertionaldyspnea 24 2.9 18 1.3 17 0.6
Infections Upper respiratorytract infection 23 0 22 0.3 17 0
Endocrine Hypothyroidism 19 0.6 11 0 5 0 Hyperthyroidism 11 1.3 6 0 1 0Investigations Decreased weight 12 0 7 0 7 0.3Vascular Hypertension 7 2.2 11 5 9 2.3
Clinically important adverse reactions in <10% of patients who received YERVOY withnivolumab:Gastrointestinal Disorders: stomatitis, intestinal perforationSkin and Subcutaneous Tissue Disorders: vitiligoMusculoskeletal and Connective Tissue Disorders: myopathy, Sjogren’s syndrome,spondyloarthropathy, myositis (including polymyositis)Nervous System Disorders: neuritis, peroneal nerve palsy
Table 6: Laboratory Abnormalities Worsening from Baseline Occurring in≥20% of Patients Treated with YERVOY with Nivolumab or Single-Agent
Nivolumab and at a Higher Incidence than in the YERVOY Arm (Between ArmDifference of ≥5% All Grades or ≥2% Grades 3-4) - CHECKMATE-067
YERVOY and
ab
c
de
d
e
a
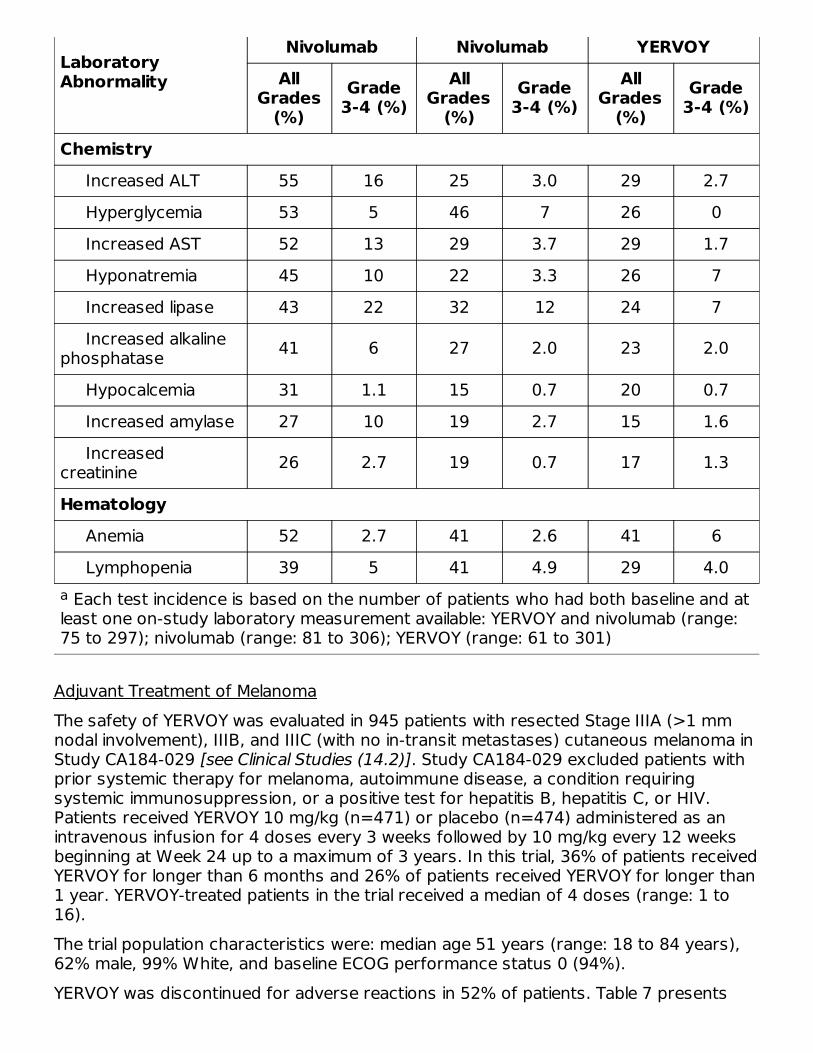
Each test incidence is based on the number of patients who had both baseline and atleast one on-study laboratory measurement available: YERVOY and nivolumab (range:75 to 297); nivolumab (range: 81 to 306); YERVOY (range: 61 to 301)
LaboratoryAbnormality
Nivolumab Nivolumab YERVOYAll
Grades(%)
Grade3-4 (%)
AllGrades
(%)Grade
3-4 (%)All
Grades(%)
Grade3-4 (%)
Chemistry Increased ALT 55 16 25 3.0 29 2.7 Hyperglycemia 53 5 46 7 26 0 Increased AST 52 13 29 3.7 29 1.7 Hyponatremia 45 10 22 3.3 26 7 Increased lipase 43 22 32 12 24 7 Increased alkalinephosphatase 41 6 27 2.0 23 2.0
Hypocalcemia 31 1.1 15 0.7 20 0.7 Increased amylase 27 10 19 2.7 15 1.6 Increasedcreatinine 26 2.7 19 0.7 17 1.3
Hematology Anemia 52 2.7 41 2.6 41 6 Lymphopenia 39 5 41 4.9 29 4.0
Adjuvant Treatment of MelanomaThe safety of YERVOY was evaluated in 945 patients with resected Stage IIIA (>1 mmnodal involvement), IIIB, and IIIC (with no in-transit metastases) cutaneous melanoma inStudy CA184-029 [see Clinical Studies (14.2)]. Study CA184-029 excluded patients withprior systemic therapy for melanoma, autoimmune disease, a condition requiringsystemic immunosuppression, or a positive test for hepatitis B, hepatitis C, or HIV.Patients received YERVOY 10 mg/kg (n=471) or placebo (n=474) administered as anintravenous infusion for 4 doses every 3 weeks followed by 10 mg/kg every 12 weeksbeginning at Week 24 up to a maximum of 3 years. In this trial, 36% of patients receivedYERVOY for longer than 6 months and 26% of patients received YERVOY for longer than1 year. YERVOY-treated patients in the trial received a median of 4 doses (range: 1 to16).The trial population characteristics were: median age 51 years (range: 18 to 84 years),62% male, 99% White, and baseline ECOG performance status 0 (94%).YERVOY was discontinued for adverse reactions in 52% of patients. Table 7 presents
a

selected adverse reactions from Study CA184-029.
Table 7: Adverse Reactions (≥5%) in Patients Receiving YERVOY with aDifference Between Arms >5% Compared to Placebo in Study CA184-029
Adverse Reaction YERVOY 10 mg/kgn=471
Placebo n=474
All Grades(%)
Grade 3 to5 (%)
All Grades(%)
Grade 3 to5 (%)
Dermatologic Rash 50 2.1 20 0 Pruritus 45 2.3 15 0Gastrointestinal Diarrhea 49 10 30 2.1 Nausea 25 0.2 18 0 Colitis 16 8 1.5 0.4 Vomiting 13 0.4 6 0.2General and Administration-Site Conditions Fatigue 46 2.3 38 1.5 Weight Decreased 32 0.2 9 0.4 Pyrexia 18 1.1 4.9 0.2Nervous System Headache 33 0.8 18 0.2Metabolism and Nutrition Decreased Appetite 14 0.2 3.4 0.2Psychiatric Insomnia 10 0 4.4 0
Table 8 presents selected laboratory abnormalities from Study CA184-029.
Table 8: Laboratory Abnormalities (>5%) Worsening from Baseline in PatientsReceiving YERVOY with a Difference Between Arms of >5% Compared to
Placebo in CA184-029
Laboratory Abnormality YERVOY 10 mg/kg PlaceboAll
Grades(%)
Grade 3to 4(%)
AllGrades
(%)
Grade 3to 4(%)
Chemistry Increased ALT 46 10 16 0 Increased AST 38 9 14 0.2 Increased lipase 26 9 17 4.5 Increased amylase 17 2.0 7 0.6 Increased alkaline phosphatase 17 0.6 6 0.2
a
a a
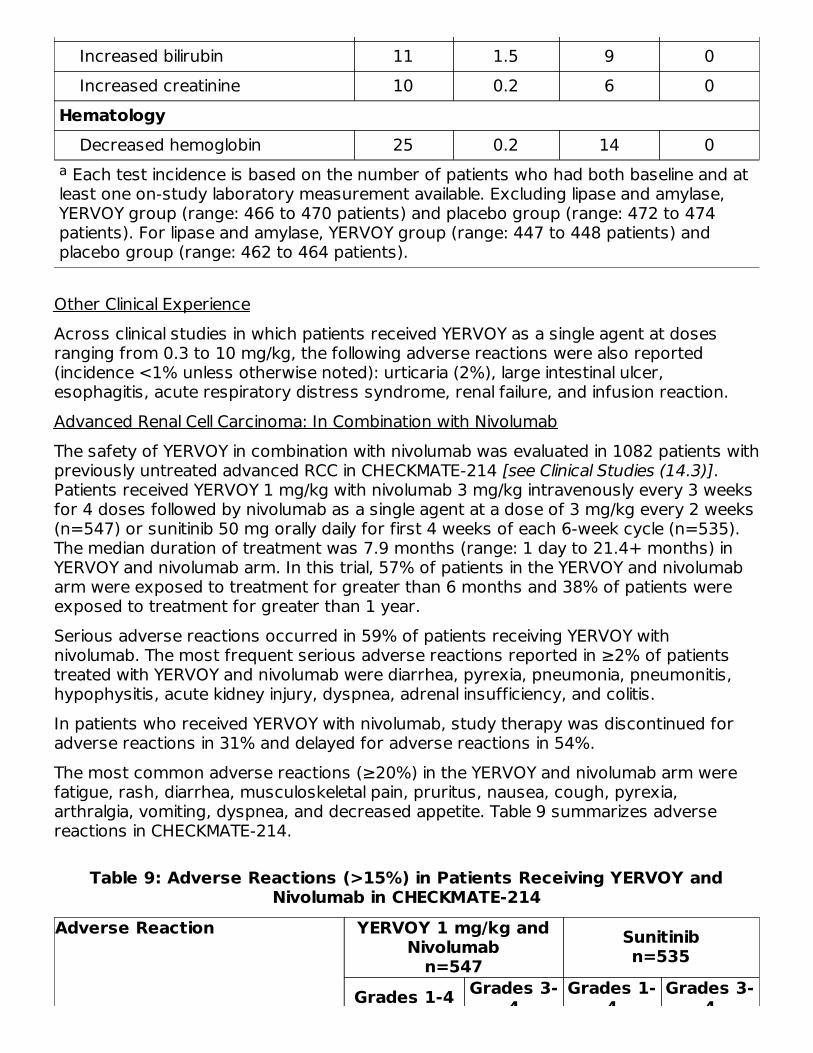
Each test incidence is based on the number of patients who had both baseline and atleast one on-study laboratory measurement available. Excluding lipase and amylase,YERVOY group (range: 466 to 470 patients) and placebo group (range: 472 to 474patients). For lipase and amylase, YERVOY group (range: 447 to 448 patients) andplacebo group (range: 462 to 464 patients).
Increased bilirubin 11 1.5 9 0 Increased creatinine 10 0.2 6 0Hematology Decreased hemoglobin 25 0.2 14 0
Other Clinical ExperienceAcross clinical studies in which patients received YERVOY as a single agent at dosesranging from 0.3 to 10 mg/kg, the following adverse reactions were also reported(incidence <1% unless otherwise noted): urticaria (2%), large intestinal ulcer,esophagitis, acute respiratory distress syndrome, renal failure, and infusion reaction.Advanced Renal Cell Carcinoma: In Combination with NivolumabThe safety of YERVOY in combination with nivolumab was evaluated in 1082 patients withpreviously untreated advanced RCC in CHECKMATE-214 [see Clinical Studies (14.3)].Patients received YERVOY 1 mg/kg with nivolumab 3 mg/kg intravenously every 3 weeksfor 4 doses followed by nivolumab as a single agent at a dose of 3 mg/kg every 2 weeks(n=547) or sunitinib 50 mg orally daily for first 4 weeks of each 6-week cycle (n=535).The median duration of treatment was 7.9 months (range: 1 day to 21.4+ months) inYERVOY and nivolumab arm. In this trial, 57% of patients in the YERVOY and nivolumabarm were exposed to treatment for greater than 6 months and 38% of patients wereexposed to treatment for greater than 1 year.Serious adverse reactions occurred in 59% of patients receiving YERVOY withnivolumab. The most frequent serious adverse reactions reported in ≥2% of patientstreated with YERVOY and nivolumab were diarrhea, pyrexia, pneumonia, pneumonitis,hypophysitis, acute kidney injury, dyspnea, adrenal insufficiency, and colitis.In patients who received YERVOY with nivolumab, study therapy was discontinued foradverse reactions in 31% and delayed for adverse reactions in 54%.The most common adverse reactions (≥20%) in the YERVOY and nivolumab arm werefatigue, rash, diarrhea, musculoskeletal pain, pruritus, nausea, cough, pyrexia,arthralgia, vomiting, dyspnea, and decreased appetite. Table 9 summarizes adversereactions in CHECKMATE-214.
Table 9: Adverse Reactions (>15%) in Patients Receiving YERVOY andNivolumab in CHECKMATE-214
Adverse Reaction YERVOY 1 mg/kg andNivolumab
n=547Sunitinibn=535
Grades 1-4 Grades 3-4
Grades 1-4
Grades 3-4
a
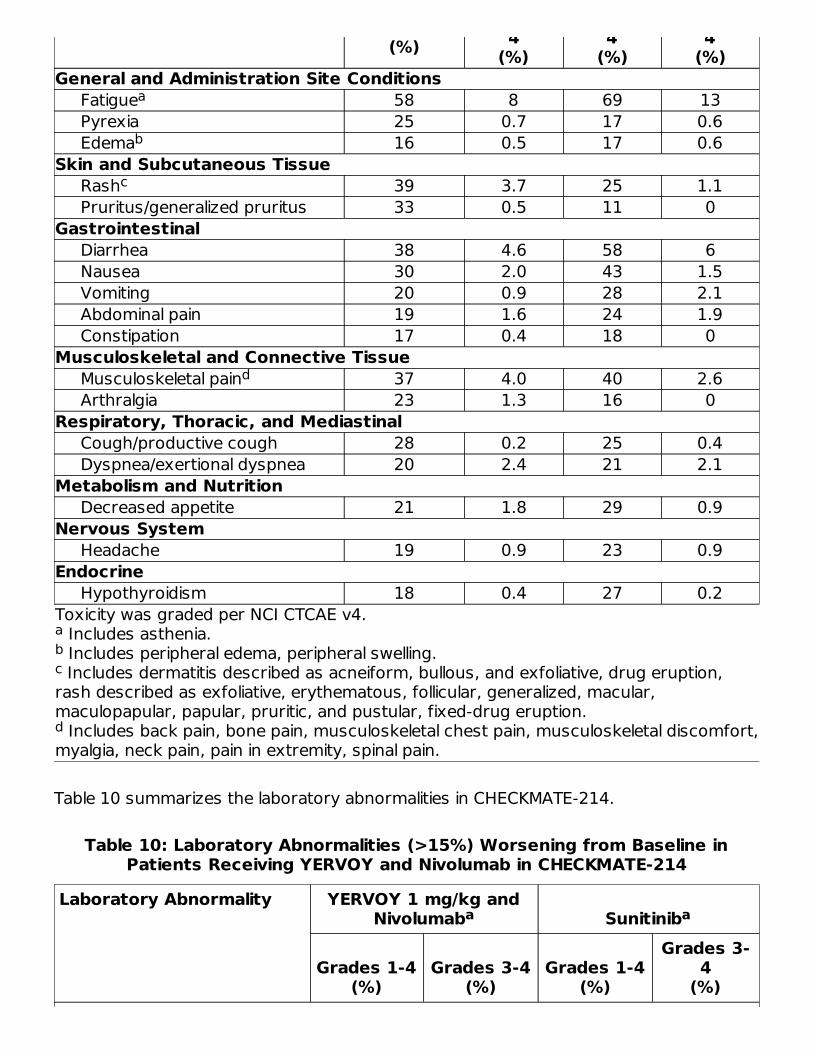
Toxicity was graded per NCI CTCAE v4. Includes asthenia. Includes peripheral edema, peripheral swelling. Includes dermatitis described as acneiform, bullous, and exfoliative, drug eruption,
rash described as exfoliative, erythematous, follicular, generalized, macular,maculopapular, papular, pruritic, and pustular, fixed-drug eruption. Includes back pain, bone pain, musculoskeletal chest pain, musculoskeletal discomfort,
myalgia, neck pain, pain in extremity, spinal pain.
(%) 4(%)
4(%)
4(%)
General and Administration Site Conditions Fatigue 58 8 69 13 Pyrexia 25 0.7 17 0.6 Edema 16 0.5 17 0.6Skin and Subcutaneous Tissue Rash 39 3.7 25 1.1 Pruritus/generalized pruritus 33 0.5 11 0Gastrointestinal Diarrhea 38 4.6 58 6 Nausea 30 2.0 43 1.5 Vomiting 20 0.9 28 2.1 Abdominal pain 19 1.6 24 1.9 Constipation 17 0.4 18 0Musculoskeletal and Connective Tissue Musculoskeletal pain 37 4.0 40 2.6 Arthralgia 23 1.3 16 0Respiratory, Thoracic, and Mediastinal Cough/productive cough 28 0.2 25 0.4 Dyspnea/exertional dyspnea 20 2.4 21 2.1Metabolism and Nutrition Decreased appetite 21 1.8 29 0.9Nervous System Headache 19 0.9 23 0.9Endocrine Hypothyroidism 18 0.4 27 0.2
Table 10 summarizes the laboratory abnormalities in CHECKMATE-214.
Table 10: Laboratory Abnormalities (>15%) Worsening from Baseline inPatients Receiving YERVOY and Nivolumab in CHECKMATE-214
Laboratory Abnormality YERVOY 1 mg/kg andNivolumab Sunitinib
Grades 1-4(%)
Grades 3-4(%)
Grades 1-4(%)
Grades 3-4
(%)
abc
d
a
b
c
d
a a
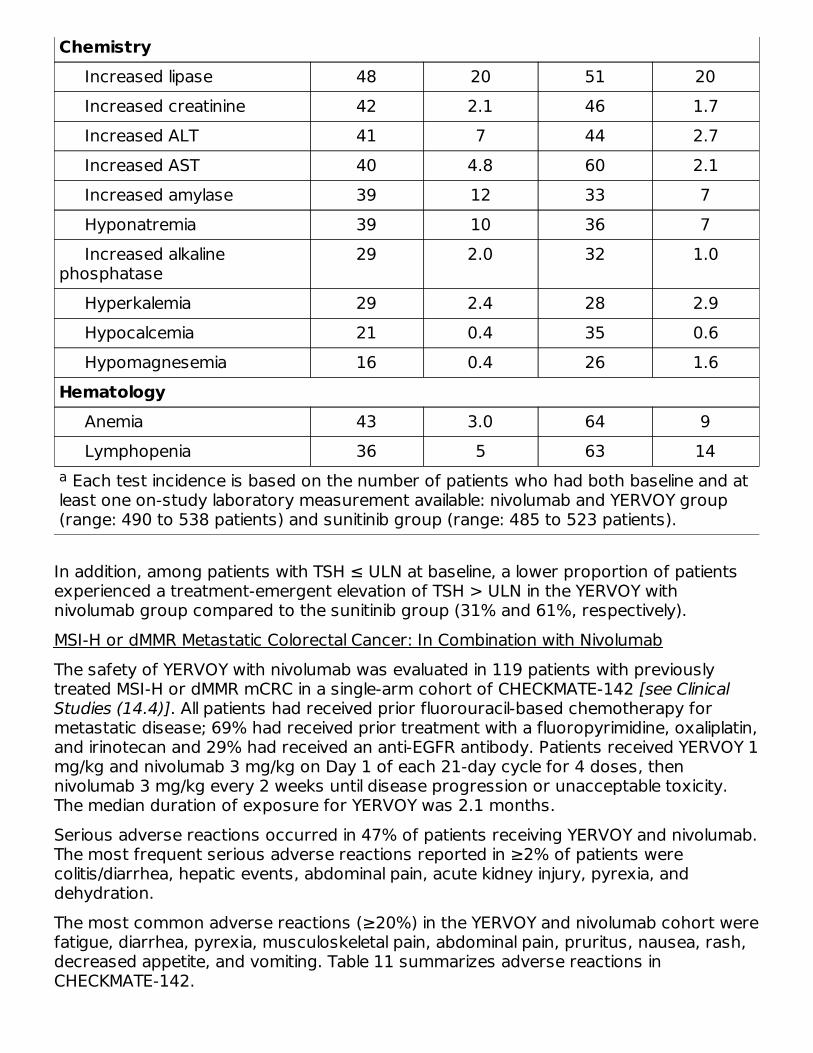
Each test incidence is based on the number of patients who had both baseline and atleast one on-study laboratory measurement available: nivolumab and YERVOY group(range: 490 to 538 patients) and sunitinib group (range: 485 to 523 patients).
Chemistry Increased lipase 48 20 51 20 Increased creatinine 42 2.1 46 1.7 Increased ALT 41 7 44 2.7 Increased AST 40 4.8 60 2.1 Increased amylase 39 12 33 7 Hyponatremia 39 10 36 7 Increased alkalinephosphatase
29 2.0 32 1.0
Hyperkalemia 29 2.4 28 2.9 Hypocalcemia 21 0.4 35 0.6 Hypomagnesemia 16 0.4 26 1.6Hematology Anemia 43 3.0 64 9 Lymphopenia 36 5 63 14
In addition, among patients with TSH ≤ ULN at baseline, a lower proportion of patientsexperienced a treatment-emergent elevation of TSH > ULN in the YERVOY withnivolumab group compared to the sunitinib group (31% and 61%, respectively).MSI-H or dMMR Metastatic Colorectal Cancer: In Combination with NivolumabThe safety of YERVOY with nivolumab was evaluated in 119 patients with previouslytreated MSI-H or dMMR mCRC in a single-arm cohort of CHECKMATE-142 [see ClinicalStudies (14.4)]. All patients had received prior fluorouracil-based chemotherapy formetastatic disease; 69% had received prior treatment with a fluoropyrimidine, oxaliplatin,and irinotecan and 29% had received an anti-EGFR antibody. Patients received YERVOY 1mg/kg and nivolumab 3 mg/kg on Day 1 of each 21-day cycle for 4 doses, thennivolumab 3 mg/kg every 2 weeks until disease progression or unacceptable toxicity.The median duration of exposure for YERVOY was 2.1 months.Serious adverse reactions occurred in 47% of patients receiving YERVOY and nivolumab.The most frequent serious adverse reactions reported in ≥2% of patients werecolitis/diarrhea, hepatic events, abdominal pain, acute kidney injury, pyrexia, anddehydration.The most common adverse reactions (≥20%) in the YERVOY and nivolumab cohort werefatigue, diarrhea, pyrexia, musculoskeletal pain, abdominal pain, pruritus, nausea, rash,decreased appetite, and vomiting. Table 11 summarizes adverse reactions inCHECKMATE-142.
a
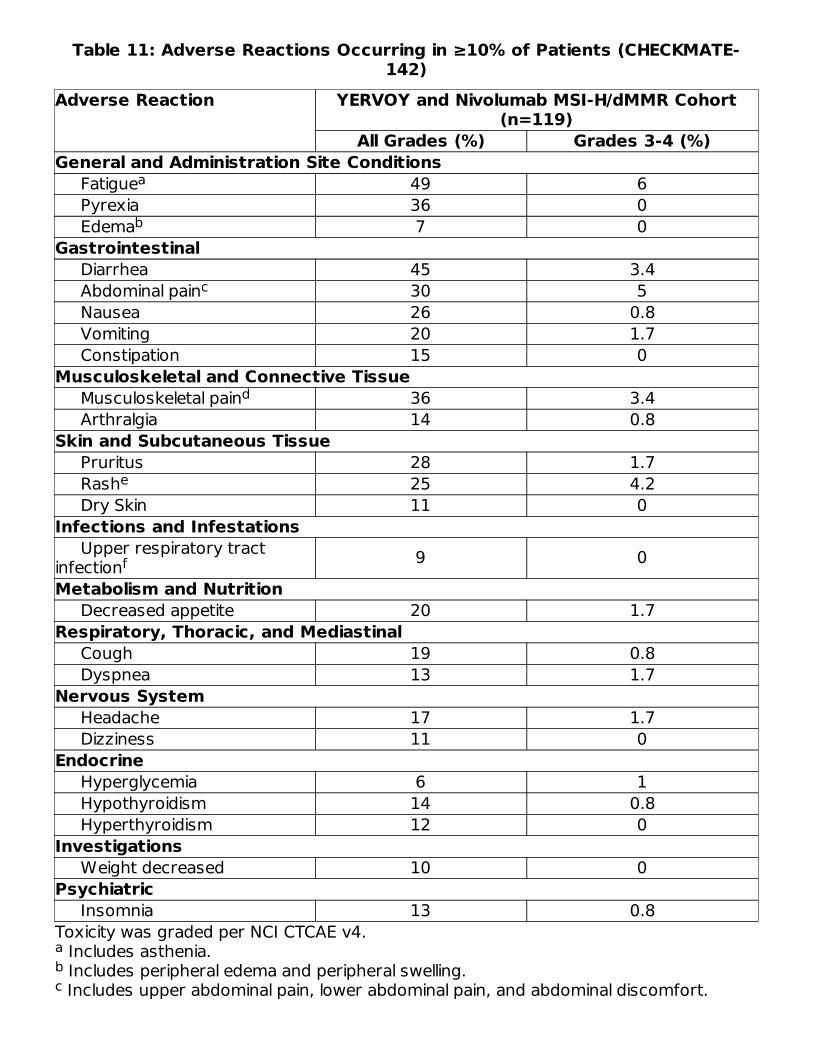
Table 11: Adverse Reactions Occurring in ≥10% of Patients (CHECKMATE-142)
Toxicity was graded per NCI CTCAE v4. Includes asthenia. Includes peripheral edema and peripheral swelling. Includes upper abdominal pain, lower abdominal pain, and abdominal discomfort.
Adverse Reaction YERVOY and Nivolumab MSI-H/dMMR Cohort(n=119)
All Grades (%) Grades 3-4 (%)General and Administration Site Conditions Fatigue 49 6 Pyrexia 36 0 Edema 7 0Gastrointestinal Diarrhea 45 3.4 Abdominal pain 30 5 Nausea 26 0.8 Vomiting 20 1.7 Constipation 15 0Musculoskeletal and Connective Tissue Musculoskeletal pain 36 3.4 Arthralgia 14 0.8Skin and Subcutaneous Tissue Pruritus 28 1.7 Rash 25 4.2 Dry Skin 11 0Infections and Infestations Upper respiratory tractinfection 9 0Metabolism and Nutrition Decreased appetite 20 1.7Respiratory, Thoracic, and Mediastinal Cough 19 0.8 Dyspnea 13 1.7Nervous System Headache 17 1.7 Dizziness 11 0Endocrine Hyperglycemia 6 1 Hypothyroidism 14 0.8 Hyperthyroidism 12 0Investigations Weight decreased 10 0Psychiatric Insomnia 13 0.8
abcd
a
b
c
d
e
f
Includes back pain, pain in extremity, myalgia, neck pain, and bone pain. Includes dermatitis, dermatitis acneiform, and rash described as maculo-papular,
erythematous, and generalized. Includes nasopharyngitis and rhinitis.
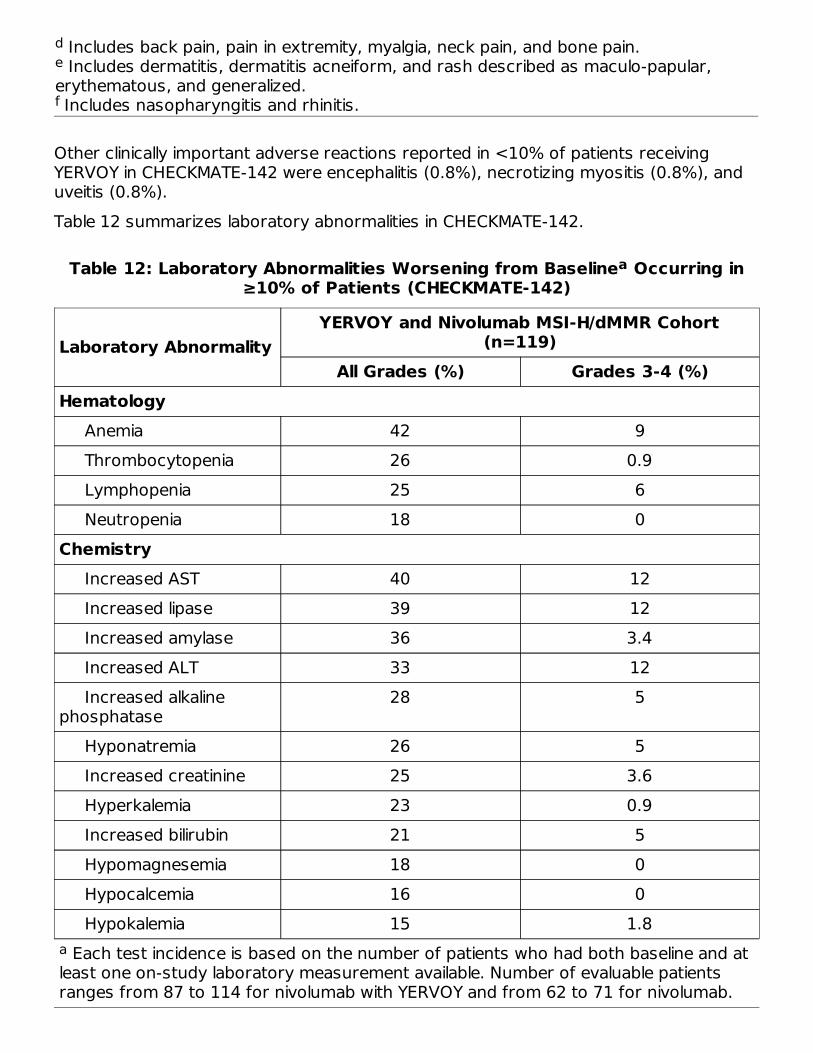
Other clinically important adverse reactions reported in <10% of patients receivingYERVOY in CHECKMATE-142 were encephalitis (0.8%), necrotizing myositis (0.8%), anduveitis (0.8%).Table 12 summarizes laboratory abnormalities in CHECKMATE-142.
Table 12: Laboratory Abnormalities Worsening from Baseline Occurring in≥10% of Patients (CHECKMATE-142)
Each test incidence is based on the number of patients who had both baseline and atleast one on-study laboratory measurement available. Number of evaluable patientsranges from 87 to 114 for nivolumab with YERVOY and from 62 to 71 for nivolumab.
Laboratory AbnormalityYERVOY and Nivolumab MSI-H/dMMR Cohort
(n=119)All Grades (%) Grades 3-4 (%)
Hematology Anemia 42 9 Thrombocytopenia 26 0.9 Lymphopenia 25 6 Neutropenia 18 0Chemistry Increased AST 40 12 Increased lipase 39 12 Increased amylase 36 3.4 Increased ALT 33 12 Increased alkalinephosphatase
28 5
Hyponatremia 26 5 Increased creatinine 25 3.6 Hyperkalemia 23 0.9 Increased bilirubin 21 5 Hypomagnesemia 18 0 Hypocalcemia 16 0 Hypokalemia 15 1.8
de
f
a
a
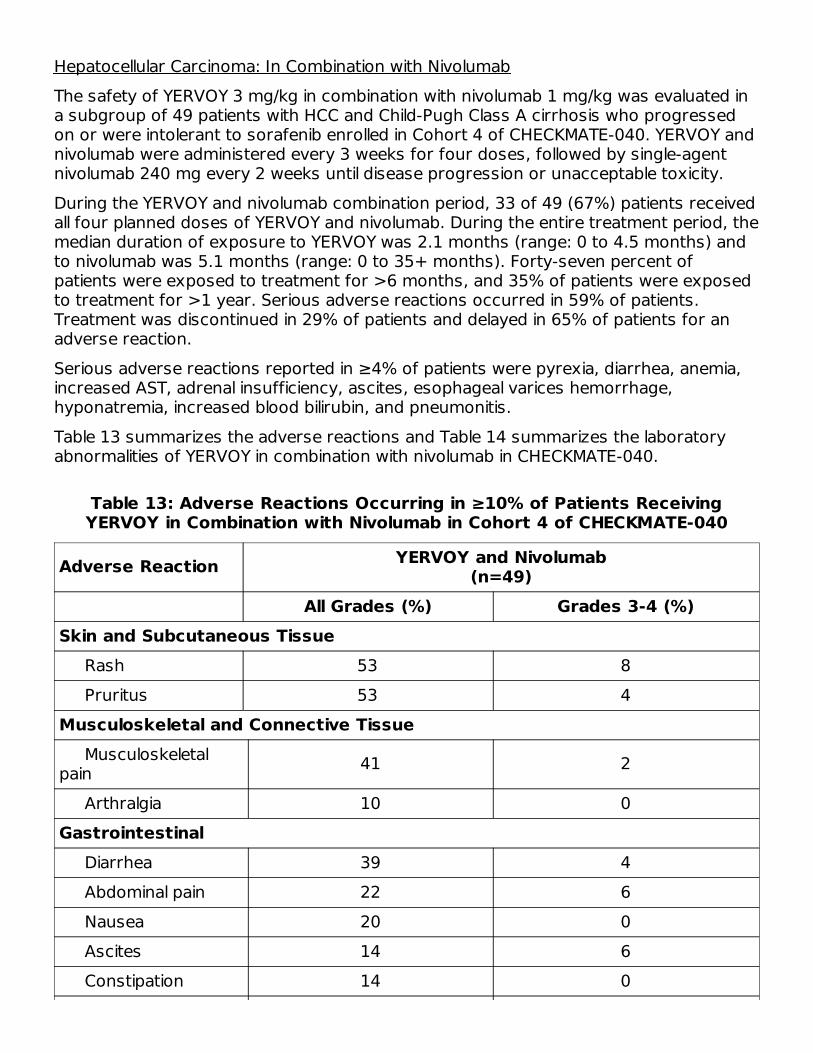
Hepatocellular Carcinoma: In Combination with NivolumabThe safety of YERVOY 3 mg/kg in combination with nivolumab 1 mg/kg was evaluated ina subgroup of 49 patients with HCC and Child-Pugh Class A cirrhosis who progressedon or were intolerant to sorafenib enrolled in Cohort 4 of CHECKMATE-040. YERVOY andnivolumab were administered every 3 weeks for four doses, followed by single-agentnivolumab 240 mg every 2 weeks until disease progression or unacceptable toxicity.During the YERVOY and nivolumab combination period, 33 of 49 (67%) patients receivedall four planned doses of YERVOY and nivolumab. During the entire treatment period, themedian duration of exposure to YERVOY was 2.1 months (range: 0 to 4.5 months) andto nivolumab was 5.1 months (range: 0 to 35+ months). Forty-seven percent ofpatients were exposed to treatment for >6 months, and 35% of patients were exposedto treatment for >1 year. Serious adverse reactions occurred in 59% of patients.Treatment was discontinued in 29% of patients and delayed in 65% of patients for anadverse reaction.Serious adverse reactions reported in ≥4% of patients were pyrexia, diarrhea, anemia,increased AST, adrenal insufficiency, ascites, esophageal varices hemorrhage,hyponatremia, increased blood bilirubin, and pneumonitis.Table 13 summarizes the adverse reactions and Table 14 summarizes the laboratoryabnormalities of YERVOY in combination with nivolumab in CHECKMATE-040.
Table 13: Adverse Reactions Occurring in ≥10% of Patients ReceivingYERVOY in Combination with Nivolumab in Cohort 4 of CHECKMATE-040
Adverse Reaction YERVOY and Nivolumab(n=49)
All Grades (%) Grades 3-4 (%)Skin and Subcutaneous Tissue Rash 53 8 Pruritus 53 4Musculoskeletal and Connective Tissue Musculoskeletalpain 41 2
Arthralgia 10 0Gastrointestinal Diarrhea 39 4 Abdominal pain 22 6 Nausea 20 0 Ascites 14 6 Constipation 14 0

Dry mouth 12 0 Dyspepsia 12 2 Vomiting 12 2 Stomatitis 10 0Respiratory, Thoracic and Mediastinal Cough 37 0 Dyspnea 14 0 Pneumonitis 10 2Metabolism and Nutrition Decreased appetite 35 2General Fatigue 27 2 Pyrexia 27 0 Malaise 18 2 Edema 16 2 Influenza-like illness 14 0 Chills 10 0Nervous System Headache 22 0 Dizziness 20 0Endocrine Hypothyroidism 20 0 Adrenalinsufficiency 18 4
Investigations Weight decreased 20 0Psychiatric Insomnia 18 0Blood and Lymphatic System Anemia 10 4Infections Influenza 10 2Vascular

Hypotension 10 0
Clinically important adverse reactions reported in <10% of patients receiving YERVOYwith nivolumab were hyperglycemia (8%), colitis (4%), and increased blood creatinephosphokinase (2%).
Table 14: Select Laboratory Abnormalities (≥10%) Worsening from Baseline inPatients Receiving YERVOY in Combination with Nivolumab in Cohort 4 of
CHECKMATE-040
LaboratoryAbnormality
YERVOY and Nivolumab(n=47)
All Grades (%) Grades 3-4 (%)Hematology Lymphopenia 53 13 Anemia 43 4.3 Neutropenia 43 9 Leukopenia 40 2.1 Thrombocytopenia 34 4.3Chemistry Increased AST 66 40 Increased ALT 66 21 Increased bilirubin 55 11 Increased lipase 51 26 Hyponatremia 49 32 Hypocalcemia 47 0 Increased alkalinephosphatase 40 4.3
Increased amylase 38 15 Hypokalemia 26 2.1 Hyperkalemia 23 4.3 Increasedcreatinine 21 0
Hypomagnesemia 11 0
In patients who received YERVOY with nivolumab, virologic breakthrough occurred in 4of 28 (14%) patients and 2 of 4 (50%) patients with active HBV or HCV at baseline,respectively. HBV virologic breakthrough was defined as at least a 1 log increase in HBV
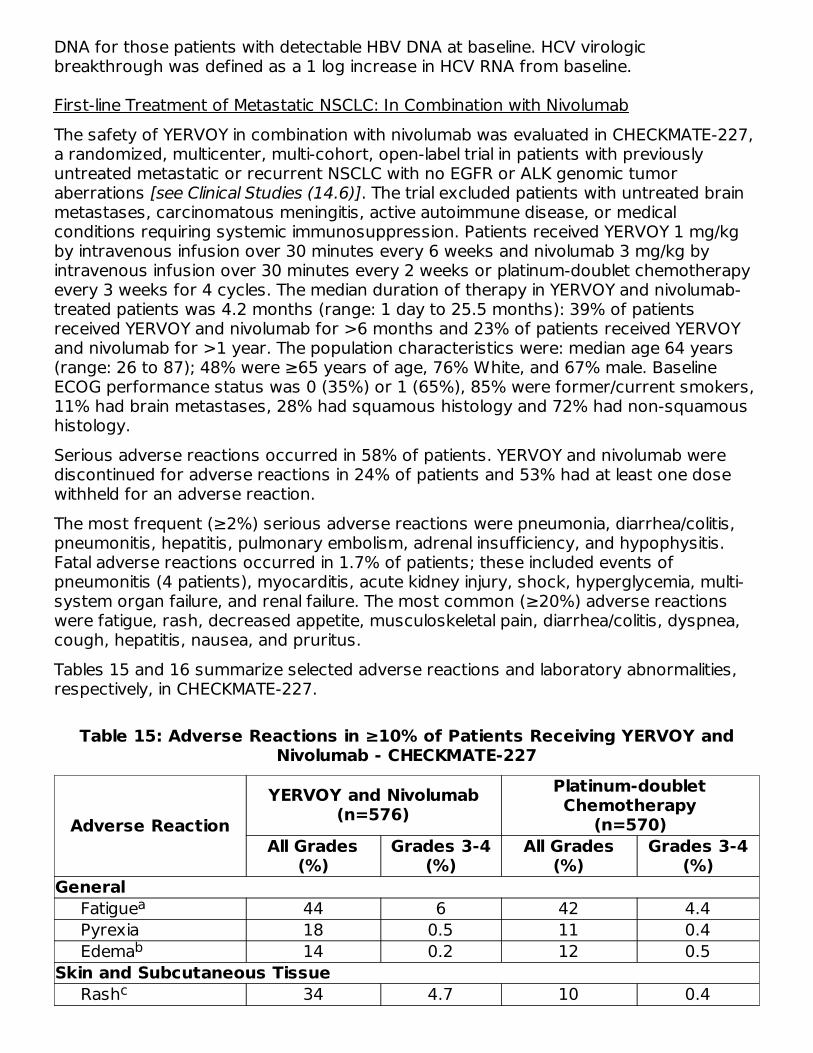
DNA for those patients with detectable HBV DNA at baseline. HCV virologicbreakthrough was defined as a 1 log increase in HCV RNA from baseline.
First-line Treatment of Metastatic NSCLC: In Combination with NivolumabThe safety of YERVOY in combination with nivolumab was evaluated in CHECKMATE-227,a randomized, multicenter, multi-cohort, open-label trial in patients with previouslyuntreated metastatic or recurrent NSCLC with no EGFR or ALK genomic tumoraberrations [see Clinical Studies (14.6)]. The trial excluded patients with untreated brainmetastases, carcinomatous meningitis, active autoimmune disease, or medicalconditions requiring systemic immunosuppression. Patients received YERVOY 1 mg/kgby intravenous infusion over 30 minutes every 6 weeks and nivolumab 3 mg/kg byintravenous infusion over 30 minutes every 2 weeks or platinum-doublet chemotherapyevery 3 weeks for 4 cycles. The median duration of therapy in YERVOY and nivolumab-treated patients was 4.2 months (range: 1 day to 25.5 months): 39% of patientsreceived YERVOY and nivolumab for >6 months and 23% of patients received YERVOYand nivolumab for >1 year. The population characteristics were: median age 64 years(range: 26 to 87); 48% were ≥65 years of age, 76% White, and 67% male. BaselineECOG performance status was 0 (35%) or 1 (65%), 85% were former/current smokers,11% had brain metastases, 28% had squamous histology and 72% had non-squamoushistology.Serious adverse reactions occurred in 58% of patients. YERVOY and nivolumab werediscontinued for adverse reactions in 24% of patients and 53% had at least one dosewithheld for an adverse reaction.The most frequent (≥2%) serious adverse reactions were pneumonia, diarrhea/colitis,pneumonitis, hepatitis, pulmonary embolism, adrenal insufficiency, and hypophysitis.Fatal adverse reactions occurred in 1.7% of patients; these included events ofpneumonitis (4 patients), myocarditis, acute kidney injury, shock, hyperglycemia, multi-system organ failure, and renal failure. The most common (≥20%) adverse reactionswere fatigue, rash, decreased appetite, musculoskeletal pain, diarrhea/colitis, dyspnea,cough, hepatitis, nausea, and pruritus.Tables 15 and 16 summarize selected adverse reactions and laboratory abnormalities,respectively, in CHECKMATE-227.
Table 15: Adverse Reactions in ≥10% of Patients Receiving YERVOY andNivolumab - CHECKMATE-227
Adverse ReactionYERVOY and Nivolumab
(n=576)Platinum-doubletChemotherapy
(n=570)All Grades
(%)Grades 3-4
(%)All Grades
(%)Grades 3-4
(%)General Fatigue 44 6 42 4.4 Pyrexia 18 0.5 11 0.4 Edema 14 0.2 12 0.5Skin and Subcutaneous Tissue Rash 34 4.7 10 0.4
a
b
cd

Includes fatigue and asthenia. Includes eyelid edema, face edema, generalized edema, localized edema, edema,
edema peripheral, and periorbital edema. Includes autoimmune dermatitis, dermatitis, dermatitis acneiform, dermatitis allergic,
dermatitis atopic, dermatitis bullous, dermatitis contact, dermatitis exfoliative, dermatitispsoriasiform, granulomatous dermatitis, rash generalized, drug eruption, dyshidroticeczema, eczema, exfoliative rash, nodular rash, rash, rash erythematous, rashgeneralized, rash macular, rash maculo-papular, rash papular, rash pruritic, rashpustular, toxic skin eruption. Includes pruritus and pruritus generalized. Includes back pain, bone pain, musculoskeletal chest pain, musculoskeletal discomfort,
musculoskeletal pain, myalgia, and pain in extremity. Includes colitis, colitis microscopic, colitis ulcerative, diarrhea, enteritis infectious,enterocolitis, enterocolitis infectious, and enterocolitis viral. Includes abdominal discomfort, abdominal pain, abdominal pain lower, abdominal pain
upper, and abdominal tenderness. Includes dyspnea and dyspnea exertional. Includes cough and productive cough. Includes alanine aminotransferase increased, aspartate aminotransferase increased,autoimmune hepatitis, blood bilirubin increased, hepatic enzyme increased, hepaticfailure, hepatic function abnormal, hepatitis, hepatitis E, hepatocellular injury,hepatotoxicity, hyperbilirubinemia, immune-mediated hepatitis, liver function testabnormal, liver function test increased, transaminases increased.
Pruritus 21 0.5 3.3 0Metabolism and Nutrition Decreased appetite 31 2.3 26 1.4Musculoskeletal and Connective Tissue Musculoskeletalpain 27 1.9 16 0.7 Arthralgia 13 0.9 2.5 0.2Gastrointestinal Diarrhea/colitis 26 3.6 16 0.9 Nausea 21 1.0 42 2.5 Constipation 18 0.3 27 0.5 Vomiting 13 1.0 18 2.3 Abdominal pain 10 0.2 9 0.7Respiratory, Thoracic, and Mediastinal Dyspnea 26 4.3 16 2.1 Cough 23 0.2 13 0Hepatobiliary Hepatitis 21 9 10 1.2Endocrine Hypothyroidism 16 0.5 1.2 0 Hyperthyroidism 10 0 0.5 0Infections and Infestations Pneumonia 13 7 8 4.0Nervous System Headache 11 0.5 6 0ab
c
de
f
g
hij
d
e
f
g
hi
j
kl
m
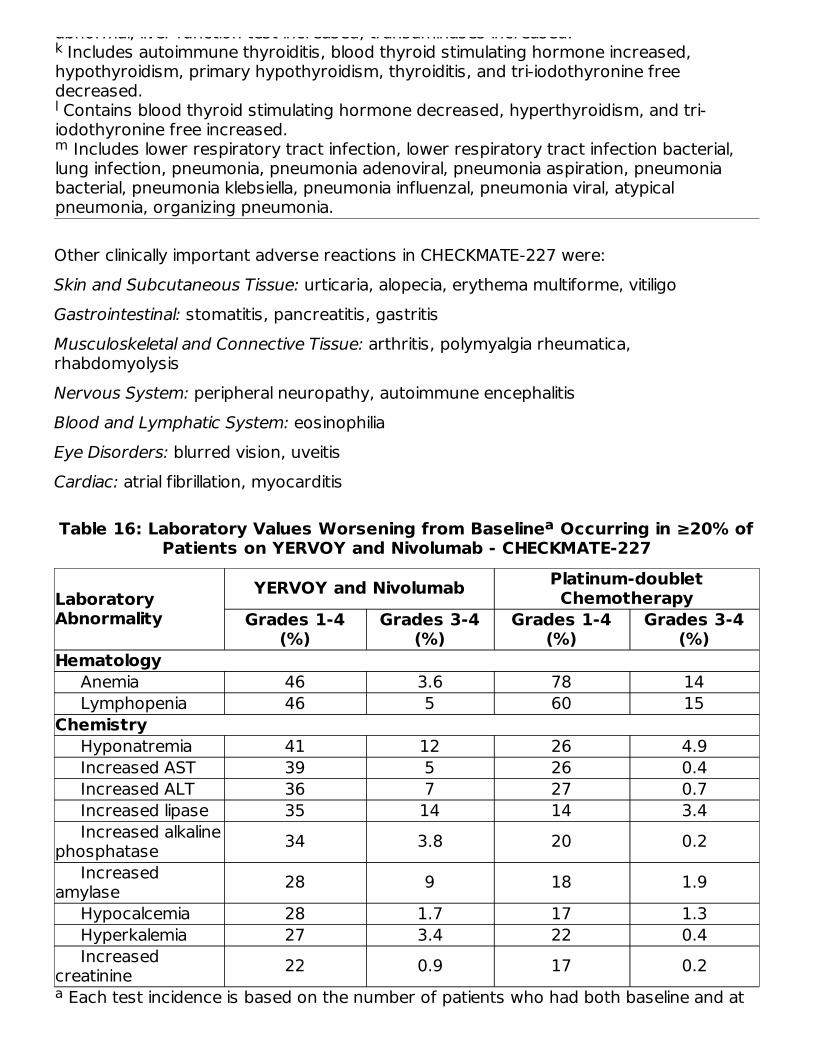
abnormal, liver function test increased, transaminases increased. Includes autoimmune thyroiditis, blood thyroid stimulating hormone increased,
hypothyroidism, primary hypothyroidism, thyroiditis, and tri-iodothyronine freedecreased. Contains blood thyroid stimulating hormone decreased, hyperthyroidism, and tri-iodothyronine free increased.
Includes lower respiratory tract infection, lower respiratory tract infection bacterial,lung infection, pneumonia, pneumonia adenoviral, pneumonia aspiration, pneumoniabacterial, pneumonia klebsiella, pneumonia influenzal, pneumonia viral, atypicalpneumonia, organizing pneumonia.
Other clinically important adverse reactions in CHECKMATE-227 were:Skin and Subcutaneous Tissue: urticaria, alopecia, erythema multiforme, vitiligoGastrointestinal: stomatitis, pancreatitis, gastritisMusculoskeletal and Connective Tissue: arthritis, polymyalgia rheumatica,rhabdomyolysisNervous System: peripheral neuropathy, autoimmune encephalitisBlood and Lymphatic System: eosinophiliaEye Disorders: blurred vision, uveitisCardiac: atrial fibrillation, myocarditis
Table 16: Laboratory Values Worsening from Baseline Occurring in ≥20% ofPatients on YERVOY and Nivolumab - CHECKMATE-227
Each test incidence is based on the number of patients who had both baseline and at
LaboratoryAbnormality
YERVOY and Nivolumab Platinum-doubletChemotherapy
Grades 1-4(%)
Grades 3-4(%)
Grades 1-4(%)
Grades 3-4(%)
Hematology Anemia 46 3.6 78 14 Lymphopenia 46 5 60 15Chemistry Hyponatremia 41 12 26 4.9 Increased AST 39 5 26 0.4 Increased ALT 36 7 27 0.7 Increased lipase 35 14 14 3.4 Increased alkalinephosphatase 34 3.8 20 0.2 Increasedamylase 28 9 18 1.9 Hypocalcemia 28 1.7 17 1.3 Hyperkalemia 27 3.4 22 0.4 Increasedcreatinine 22 0.9 17 0.2
k
l
m
a
a
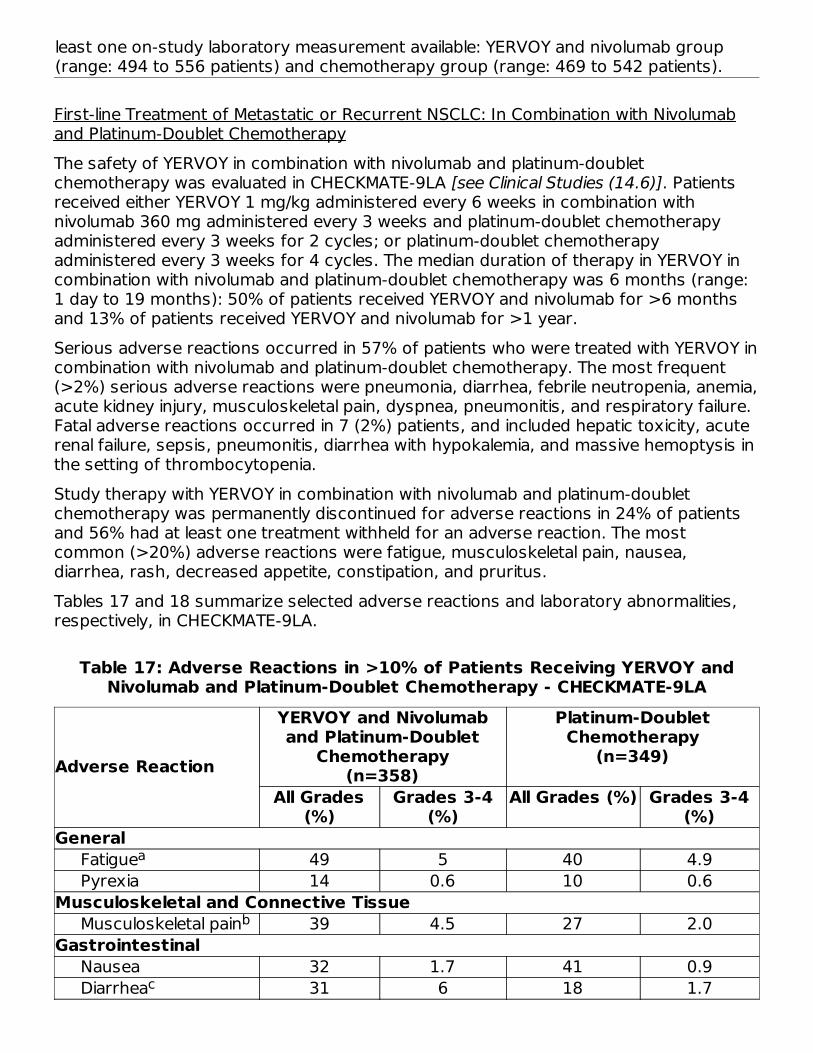
least one on-study laboratory measurement available: YERVOY and nivolumab group(range: 494 to 556 patients) and chemotherapy group (range: 469 to 542 patients).
First-line Treatment of Metastatic or Recurrent NSCLC: In Combination with Nivolumaband Platinum-Doublet ChemotherapyThe safety of YERVOY in combination with nivolumab and platinum-doubletchemotherapy was evaluated in CHECKMATE-9LA [see Clinical Studies (14.6)]. Patientsreceived either YERVOY 1 mg/kg administered every 6 weeks in combination withnivolumab 360 mg administered every 3 weeks and platinum-doublet chemotherapyadministered every 3 weeks for 2 cycles; or platinum-doublet chemotherapyadministered every 3 weeks for 4 cycles. The median duration of therapy in YERVOY incombination with nivolumab and platinum-doublet chemotherapy was 6 months (range:1 day to 19 months): 50% of patients received YERVOY and nivolumab for >6 monthsand 13% of patients received YERVOY and nivolumab for >1 year.Serious adverse reactions occurred in 57% of patients who were treated with YERVOY incombination with nivolumab and platinum-doublet chemotherapy. The most frequent(>2%) serious adverse reactions were pneumonia, diarrhea, febrile neutropenia, anemia,acute kidney injury, musculoskeletal pain, dyspnea, pneumonitis, and respiratory failure.Fatal adverse reactions occurred in 7 (2%) patients, and included hepatic toxicity, acuterenal failure, sepsis, pneumonitis, diarrhea with hypokalemia, and massive hemoptysis inthe setting of thrombocytopenia.Study therapy with YERVOY in combination with nivolumab and platinum-doubletchemotherapy was permanently discontinued for adverse reactions in 24% of patientsand 56% had at least one treatment withheld for an adverse reaction. The mostcommon (>20%) adverse reactions were fatigue, musculoskeletal pain, nausea,diarrhea, rash, decreased appetite, constipation, and pruritus.Tables 17 and 18 summarize selected adverse reactions and laboratory abnormalities,respectively, in CHECKMATE-9LA.
Table 17: Adverse Reactions in >10% of Patients Receiving YERVOY andNivolumab and Platinum-Doublet Chemotherapy - CHECKMATE-9LA
Adverse Reaction
YERVOY and Nivolumaband Platinum-Doublet
Chemotherapy(n=358)
Platinum-DoubletChemotherapy
(n=349)
All Grades(%)
Grades 3-4(%)
All Grades (%) Grades 3-4(%)
General Fatigue 49 5 40 4.9 Pyrexia 14 0.6 10 0.6Musculoskeletal and Connective Tissue Musculoskeletal pain 39 4.5 27 2.0Gastrointestinal Nausea 32 1.7 41 0.9 Diarrhea 31 6 18 1.7
a
b
c

Toxicity was graded per NCI CTCAE v4. Includes fatigue and asthenia Includes myalgia, back pain, pain in extremity, musculoskeletal pain, bone pain, flank
pain, muscle spasms, musculoskeletal chest pain, musculoskeletal disorder, osteitis,musculoskeletal stiffness, non-cardiac chest pain, arthralgia, arthritis, arthropathy, jointeffusion, psoriatic arthropathy, synovitis Includes colitis, ulcerative colitis, diarrhea, and enterocolitis Includes abdominal discomfort, abdominal pain, lower abdominal pain, upper
abdominal pain, and gastrointestinal pain Includes acne, dermatitis, acneiform dermatitis, allergic dermatitis, atopic dermatitis,
bullous dermatitis, generalized exfoliative dermatitis, eczema, keratodermablenorrhagica, palmar-plantar erythrodysaesthesia syndrome, rash, erythematous rash,generalized rash, macular rash, maculo-papular rash, morbilliform rash, papular rash,pruritic rash, skin exfoliation, skin reaction, skin toxicity, Stevens-Johnson syndrome,urticaria Includes pruritus and generalized pruritus Includes cough, productive cough, and upper-airway cough syndrome Includes dyspnea, dyspnea at rest, and exertional dyspnea Includes autoimmune thyroiditis, increased blood thyroid stimulating hormone,hypothyroidism, thyroiditis, and decreased free tri-iodothyronine Includes dizziness, vertigo and positional vertigo
Constipation 21 0.6 23 0.6 Vomiting 18 2.0 17 1.4 Abdominal pain 12 0.6 11 0.9Skin and Subcutaneous Tissue Rash 30 4.7 10 0.3 Pruritus 21 0.8 2.9 0 Alopecia 11 0.8 10 0.6Metabolism and Nutrition Decreased appetite 28 2.0 22 1.7Respiratory, Thoracic and Mediastinal Cough 19 0.6 15 0.9 Dyspnea 18 4.7 14 3.2Endocrine Hypothyroidism 19 0.3 3.4 0Nervous System Headache 11 0.6 7 0 Dizziness 11 0.6 6 0
Table 18: Laboratory Values Worsening from Baseline Occurring in >20% ofPatients on YERVOY and Nivolumab and Platinum-Doublet Chemotherapy -
CHECKMATE-9LA
Laboratory Abnormality
YERVOY and Nivolumaband Platinum-Doublet
Chemotherapy
Platinum-DoubletChemotherapy
Grades 1-4(%)
Grades 3-4(%)
Grades 1-4(%)
Grades 3-4(%)
ab
cd
e
fghi
j
d
ef
gh
i
j
a
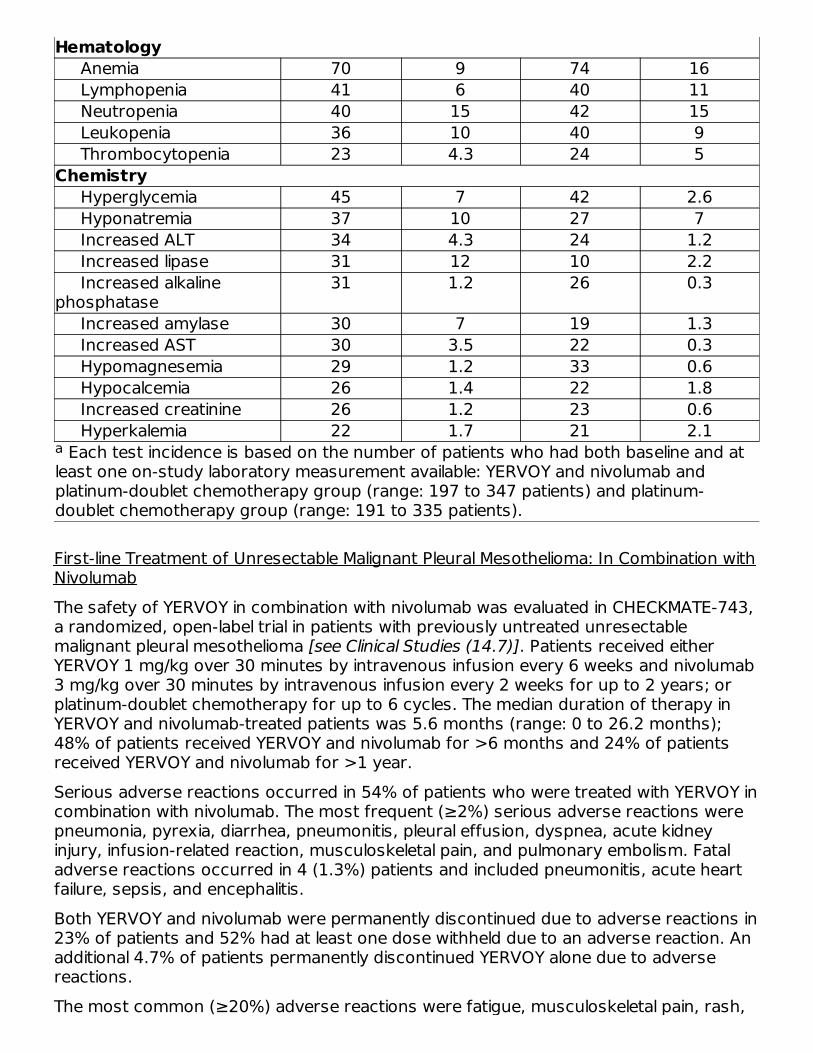
Each test incidence is based on the number of patients who had both baseline and atleast one on-study laboratory measurement available: YERVOY and nivolumab andplatinum-doublet chemotherapy group (range: 197 to 347 patients) and platinum-doublet chemotherapy group (range: 191 to 335 patients).
Hematology Anemia 70 9 74 16 Lymphopenia 41 6 40 11 Neutropenia 40 15 42 15 Leukopenia 36 10 40 9 Thrombocytopenia 23 4.3 24 5Chemistry Hyperglycemia 45 7 42 2.6 Hyponatremia 37 10 27 7 Increased ALT 34 4.3 24 1.2 Increased lipase 31 12 10 2.2 Increased alkalinephosphatase
31 1.2 26 0.3
Increased amylase 30 7 19 1.3 Increased AST 30 3.5 22 0.3 Hypomagnesemia 29 1.2 33 0.6 Hypocalcemia 26 1.4 22 1.8 Increased creatinine 26 1.2 23 0.6 Hyperkalemia 22 1.7 21 2.1
First-line Treatment of Unresectable Malignant Pleural Mesothelioma: In Combination withNivolumabThe safety of YERVOY in combination with nivolumab was evaluated in CHECKMATE-743,a randomized, open-label trial in patients with previously untreated unresectablemalignant pleural mesothelioma [see Clinical Studies (14.7)]. Patients received eitherYERVOY 1 mg/kg over 30 minutes by intravenous infusion every 6 weeks and nivolumab3 mg/kg over 30 minutes by intravenous infusion every 2 weeks for up to 2 years; orplatinum-doublet chemotherapy for up to 6 cycles. The median duration of therapy inYERVOY and nivolumab-treated patients was 5.6 months (range: 0 to 26.2 months);48% of patients received YERVOY and nivolumab for >6 months and 24% of patientsreceived YERVOY and nivolumab for >1 year.Serious adverse reactions occurred in 54% of patients who were treated with YERVOY incombination with nivolumab. The most frequent (≥2%) serious adverse reactions werepneumonia, pyrexia, diarrhea, pneumonitis, pleural effusion, dyspnea, acute kidneyinjury, infusion-related reaction, musculoskeletal pain, and pulmonary embolism. Fataladverse reactions occurred in 4 (1.3%) patients and included pneumonitis, acute heartfailure, sepsis, and encephalitis.Both YERVOY and nivolumab were permanently discontinued due to adverse reactions in23% of patients and 52% had at least one dose withheld due to an adverse reaction. Anadditional 4.7% of patients permanently discontinued YERVOY alone due to adversereactions.The most common (≥20%) adverse reactions were fatigue, musculoskeletal pain, rash,
a

diarrhea, dyspnea, nausea, decreased appetite, cough, and pruritus.Tables 19 and 20 summarize adverse reactions and laboratory abnormalities,respectively, in CHECKMATE-743.
Table 19: Adverse Reactions in ≥10% of Patients Receiving YERVOY andNivolumab - CHECKMATE-743
Includes fatigue and asthenia. Includes pyrexia and tumor-associated fever. Includes edema, generalized edema, peripheral edema, and peripheral swelling. Includes musculoskeletal pain, back pain, bone pain, flank pain, involuntary muscle
contractions, muscle spasms, muscle twitching, musculoskeletal chest pain,musculoskeletal stiffness, myalgia, neck pain, non-cardiac chest pain, pain in extremity,polymyalgia rheumatica, and spinal pain. Includes rash, acne, acneiform dermatitis, allergic dermatitis, atopic dermatitis,
autoimmune dermatitis, bullous dermatitis, contact dermatitis, dermatitis, drug eruption,
Adverse ReactionYERVOY and Nivolumab
(n=300)Chemotherapy
(n=284)All Grades
(%)Grades 3-4
(%)All Grades
(%)Grades 3-4
(%)General Fatigue 43 4.3 45 6 Pyrexia 18 1.3 4.6 0.7 Edema 17 0 8 0Musculoskeletal and Connective Tissue Musculoskeletal pain 38 3.3 17 1.1 Arthralgia 13 1.0 1.1 0Skin and Subcutaneous Tissue Rash 34 2.7 11 0.4 Pruritus 21 1.0 1.4 0Gastrointestinal Diarrhea 32 6 12 1.1 Nausea 24 0.7 43 2.5 Constipation 19 0.3 30 0.7 Abdominal pain 15 1 10 0.7 Vomiting 14 0 18 2.1Respiratory, Thoracic, and Mediastinal Dyspnea 27 2.3 16 3.2 Cough 23 0.7 9 0Metabolism and Nutrition Decreased appetite 24 1.0 25 1.4Endocrine Hypothyroidism 15 0 1.4 0Infections and Infestations Upper respiratory tractinfection 12 0.3 7 0 Pneumonia 10 4.0 4.2 2.1abcd
e
abc
d
ef
g
h
ij
k
lm
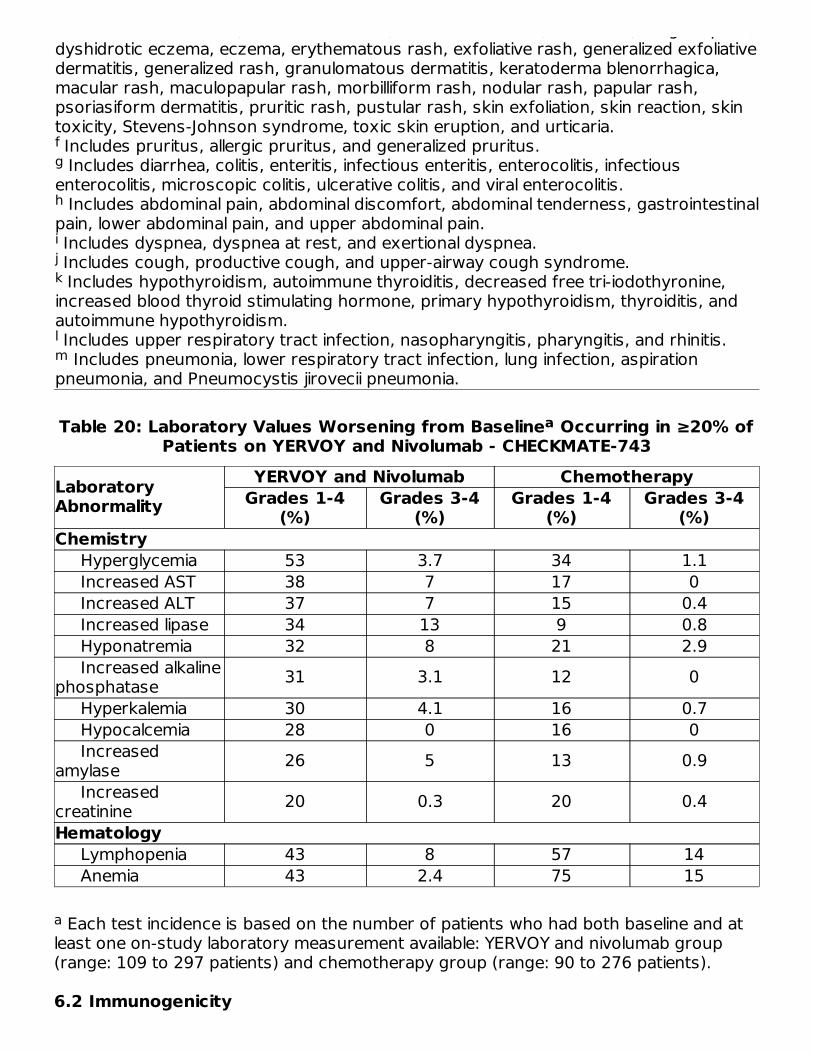
autoimmune dermatitis, bullous dermatitis, contact dermatitis, dermatitis, drug eruption,dyshidrotic eczema, eczema, erythematous rash, exfoliative rash, generalized exfoliativedermatitis, generalized rash, granulomatous dermatitis, keratoderma blenorrhagica,macular rash, maculopapular rash, morbilliform rash, nodular rash, papular rash,psoriasiform dermatitis, pruritic rash, pustular rash, skin exfoliation, skin reaction, skintoxicity, Stevens-Johnson syndrome, toxic skin eruption, and urticaria. Includes pruritus, allergic pruritus, and generalized pruritus. Includes diarrhea, colitis, enteritis, infectious enteritis, enterocolitis, infectious
enterocolitis, microscopic colitis, ulcerative colitis, and viral enterocolitis. Includes abdominal pain, abdominal discomfort, abdominal tenderness, gastrointestinal
pain, lower abdominal pain, and upper abdominal pain. Includes dyspnea, dyspnea at rest, and exertional dyspnea. Includes cough, productive cough, and upper-airway cough syndrome. Includes hypothyroidism, autoimmune thyroiditis, decreased free tri-iodothyronine,
increased blood thyroid stimulating hormone, primary hypothyroidism, thyroiditis, andautoimmune hypothyroidism. Includes upper respiratory tract infection, nasopharyngitis, pharyngitis, and rhinitis. Includes pneumonia, lower respiratory tract infection, lung infection, aspiration
pneumonia, and Pneumocystis jirovecii pneumonia.
Table 20: Laboratory Values Worsening from Baseline Occurring in ≥20% ofPatients on YERVOY and Nivolumab - CHECKMATE-743
LaboratoryAbnormality
YERVOY and Nivolumab ChemotherapyGrades 1-4
(%)Grades 3-4
(%)Grades 1-4
(%)Grades 3-4
(%)Chemistry Hyperglycemia 53 3.7 34 1.1 Increased AST 38 7 17 0 Increased ALT 37 7 15 0.4 Increased lipase 34 13 9 0.8 Hyponatremia 32 8 21 2.9 Increased alkalinephosphatase 31 3.1 12 0 Hyperkalemia 30 4.1 16 0.7 Hypocalcemia 28 0 16 0 Increasedamylase 26 5 13 0.9 Increasedcreatinine 20 0.3 20 0.4Hematology Lymphopenia 43 8 57 14 Anemia 43 2.4 75 15
Each test incidence is based on the number of patients who had both baseline and atleast one on-study laboratory measurement available: YERVOY and nivolumab group(range: 109 to 297 patients) and chemotherapy group (range: 90 to 276 patients).
6.2 Immunogenicity
fg
h
ijk
lm
a
a

As with all therapeutic proteins, there is a potential for immunogenicity. The detection ofantibody formation is highly dependent on the sensitivity and specificity of the assay.Additionally, the observed incidence of antibody (including neutralizing antibody)positivity in an assay may be influenced by several factors including assay methodology,sample handling, timing of sample collection, concomitant medications, and underlyingdisease. For these reasons, comparison of the incidence of antibodies in the studiesdescribed below with the incidences of antibodies to other studies or to other productsmay be misleading.Eleven (1.1%) of 1024 evaluable patients with unresectable or metastatic melanomatested positive for treatment-emergent binding antibodies against ipilimumab in anelectrochemiluminescent (ECL) based assay. This assay had substantial limitations indetecting anti-ipilimumab antibodies in the presence of ipilimumab. Seven (4.9%) of 144patients receiving ipilimumab developed anti-ipilimumab antibodies and 7 (4.5%) of 156patients receiving placebo for the adjuvant treatment of melanoma tested positive foranti-ipilimumab antibodies using an ECL assay with improved drug tolerance. No patientstested positive for neutralizing antibodies. No infusion-related reactions occurred inpatients who tested positive for anti-ipilimumab antibodies.Of the 499 patients evaluable for anti-ipilimumab antibodies in CHECKMATE-214 andCHECKMATE-142, 27 (5.4%) were positive for anti-ipilimumab antibodies; there were nopatients with neutralizing antibodies against ipilimumab. There was no evidence ofincreased incidence of infusion reactions to YERVOY in patients with anti-ipilimumabantibodies.Of 483 patients evaluable for anti-ipilimumab antibodies in CHECKMATE-227 Part 1, 8.5%were positive for treatment-emergent anti-ipilimumab antibodies. No patients hadneutralizing antibodies against ipilimumab. In Part 1 of the same study, of 491 patientsevaluable for anti-nivolumab antibodies, 36.7% were positive for anti-nivolumabantibodies and 1.4% had neutralizing antibodies against nivolumab.Of 305 patients evaluable for anti-ipilimumab antibodies in CHECKMATE-9LA, 8% werepositive for anti-ipilimumab antibodies and 1.6% were positive for anti-ipilimumabneutralizing antibodies. There was no evidence of increased incidence of infusionreactions to YERVOY in patients with anti-ipilimumab antibodies. Of 308 patientsevaluable for anti-nivolumab antibodies in CHECKMATE-9LA, 34% were positive for anti-nivolumab antibodies and 2.6% had neutralizing antibodies against nivolumab.Of 271 patients evaluable for anti-ipilimumab antibodies in CHECKMATE-743, 13.7% werepositive for anti-ipilimumab antibodies and 0.4% were positive for anti-ipilimumabneutralizing antibodies. Of 269 patients evaluable for anti-nivolumab antibodies inCHECKMATE-743, 25.7% were positive for anti-nivolumab antibodies and 0.7% hadneutralizing antibodies against nivolumab.
6.3 Postmarketing ExperienceThe following adverse reactions have been identified during postapproval use ofYERVOY. Because these reactions are reported voluntarily from a population ofuncertain size, it is not always possible to reliably estimate their frequency or establish acausal relationship to drug exposure.Blood and lymphatic system disorders: hemophagocytic lymphohistiocytosis (HLH)Immune System: graft-versus-host disease, solid organ transplant rejection
Immune System: graft-versus-host disease, solid organ transplant rejectionSkin and Subcutaneous Tissue: Drug reaction with eosinophilia and systemic symptoms(DRESS syndrome)
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Risk SummaryBased on findings from animal studies and its mechanism of action [see ClinicalPharmacology (12.1)], YERVOY can cause fetal harm when administered to a pregnantwoman. There is insufficient human data for YERVOY exposure in pregnant women. Inanimal reproduction studies, administration of ipilimumab to cynomolgus monkeys fromthe onset of organogenesis through delivery resulted in higher incidences of abortion,stillbirth, premature delivery (with corresponding lower birth weight), and higherincidences of infant mortality in a dose-related manner (see Data). The effects ofipilimumab are likely to be greater during the second and third trimesters of pregnancy.Human IgG1 is known to cross the placental barrier and ipilimumab is an IgG1;therefore, ipilimumab has the potential to be transmitted from the mother to thedeveloping fetus. Advise pregnant women of the potential risk to a fetus. Reportpregnancies to Bristol-Myers Squibb at 1-844-593-7869.In the U.S. general population, the estimated background risk of major birth defects andmiscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%,respectively.
Data
Animal Data
In a combined study of embryo-fetal and peri-postnatal development, pregnantcynomolgus monkeys received ipilimumab every 3 weeks from the onset oforganogenesis in the first trimester through parturition. No treatment-related adverseeffects on reproduction were detected during the first two trimesters of pregnancy.Beginning in the third trimester, administration of ipilimumab at doses resulting inexposures approximately 2.6 to 7.2 times the human exposure at a dose of 3 mg/kgresulted in dose-related increases in abortion, stillbirth, premature delivery (withcorresponding lower birth weight), and an increased incidence of infant mortality. Inaddition, developmental abnormalities were identified in the urogenital system of 2 infantmonkeys exposed in utero to 30 mg/kg of ipilimumab (7.2 times the humans exposurebased on area under the curve at a dose of 3 mg/kg). One female infant monkey hadunilateral renal agenesis of the left kidney and ureter, and 1 male infant monkey had animperforate urethra with associated urinary obstruction and subcutaneous scrotaledema.Genetically engineered mice heterozygous for CTLA-4 (CTLA-4+/−), the target foripilimumab, appeared healthy and gave birth to healthy CTLA-4+/− heterozygousoffspring. Mated CTLA-4+/− heterozygous mice also produced offspring deficient inCTLA-4 (homozygous negative, CTLA-4−/−). The CTLA-4−/− homozygous negativeoffspring appeared healthy at birth, exhibited signs of multiorgan lymphoproliferative
disease by 2 weeks of age, and all died by 3 to 4 weeks of age with massivelymphoproliferation and multiorgan tissue destruction.
8.2 Lactation
Risk SummaryThere are no data on the presence of YERVOY in human milk or its effects on thebreastfed child or milk production. In monkeys, ipilimumab was present in milk (seeData). Because of the potential for serious adverse reactions in breastfed children,advise women not to breastfeed during treatment with YERVOY and for 3 monthsfollowing the last dose.
DataIn monkeys treated at dose levels resulting in exposures 2.6 and 7.2 times higher thanthose in humans at a 3 mg/kg dose, ipilimumab was present in milk at concentrations of0.1 mcg/mL and 0.4 mcg/mL, representing a ratio of up to 0.3% of the steady-stateserum concentration of the drug.
8.3 Females and Males of Reproductive Potential
Pregnancy TestingVerify pregnancy status in females of reproductive potential prior to initiating YERVOY[see Use in Specific Populations (8.1)].
ContraceptionYERVOY can cause fetal harm when administered to a pregnant woman [see Use inSpecific Populations (8.1)]. Advise females of reproductive potential to use effectivecontraception during treatment with YERVOY and for 3 months following the last dose.
8.4 Pediatric UseThe safety and effectiveness of YERVOY have been established in pediatric patients 12years and older for the treatment of unresectable or metastatic melanoma or for thetreatment of MSI-H or dMMR mCRC that has progressed following treatment with afluoropyrimidine, oxaliplatin, and irinotecan. Use of YERVOY in this age group issupported by evidence from adequate and well-controlled studies of YERVOY in adultsand population pharmacokinetic data demonstrating that the exposure at doses of 3mg/kg and 1 mg/kg in the pediatric and adult populations are comparable. In addition,the tumor biology and course of advanced melanoma and MSI-H or dMMR mCRC aresufficiently similar in adults and pediatric patients 12 years and older to allowextrapolation of data from adults to pediatric patients.The safety and effectiveness for pediatric patients 12 years and older have not beenestablished for the adjuvant treatment of melanoma or for the treatment of renal cellcarcinoma. In addition, the safety and effectiveness have not been established withYERVOY for any indication in pediatric patients less than 12 years of age.YERVOY was evaluated in a total of 45 pediatric patients across two clinical trials. In adose-finding trial (NCT01445379), 33 pediatric patients with relapsed or refractory solid
tumors were evaluated. The median age was 13 years (range 2 to 21 years) and 20patients were ≥12 years old. YERVOY was also evaluated in an open-label, single-armtrial (NCT01696045) in 12 pediatric patients ≥12 years old (range 12 to 16 years) withpreviously treated or untreated, unresectable Stage 3 or 4 malignant melanoma.Of the 17 patients ≥12 years of age with melanoma treated with YERVOY across bothstudies, 2 patients experienced objective responses including one partial response thatwas sustained for 16 months. There were no responses in patients with non-melanomasolid tumors. No new safety signals were observed in pediatric patients in these twostudies.
8.5 Geriatric UseOf the 511 patients treated with YERVOY in Study MDX010-20 (unresectable ormetastatic melanoma), 28% were 65 years and over. No overall differences in safety oreffectiveness were observed between these patients and younger patients.Of the 314 patients randomized to YERVOY administered with nivolumab in CHECKMATE-067, 41% were 65 years or older and 11% were 75 years or older. No overalldifferences in safety or effectiveness were reported between elderly patients andyounger patients.Study CA184-029 (adjuvant treatment of melanoma) and CHECKMATE-142 (metastaticcolorectal cancer) did not include sufficient numbers of patients aged 65 years and olderto determine whether they respond differently from younger patients.Of the 550 patients randomized to YERVOY 1 mg/kg with nivolumab in CHECKMATE-214(renal cell carcinoma), 38% were 65 years or older and 8% were 75 years or older. Nooverall difference in safety was observed between these patients and younger patients.In geriatric patients with intermediate or poor risk, no overall difference in effectivenesswas observed.Of the 49 patients who received YERVOY 3 mg/kg with nivolumab in Cohort 4 ofCHECKMATE-040 (hepatocellular carcinoma), 29% were between 65 years and 74 yearsof age and 8% were 75 years or older. Clinical studies of YERVOY in combination withnivolumab did not include sufficient numbers of patients with hepatocellular carcinomaaged 65 and over to determine whether they respond differently from younger patients.Of the 576 patients randomized to YERVOY 1 mg/kg every 6 weeks with nivolumab 3mg/kg every 2 weeks in CHECKMATE-227 (NSCLC), 48% were 65 years or older and10% were 75 years or older. No overall difference in safety was reported between olderpatients and younger patients; however, there was a higher discontinuation rate due toadverse reactions in patients aged 75 years or older (29%) relative to all patients whoreceived YERVOY with nivolumab (18%). Of the 396 patients in the primary efficacypopulation (PD-L1 ≥1%) randomized to YERVOY 1 mg/kg every 6 weeks with nivolumab3 mg/kg every 2 weeks with in CHECKMATE-227, the hazard ratio for overall survival was0.70 (95% CI: 0.55, 0.89) in the 199 patients younger than 65 years compared to 0.91(95% CI: 0.72, 1.15) in the 197 patients 65 years or older [see Clinical Studies (14.6)].Of the 361 patients randomized to YERVOY 1 mg/kg every 6 weeks in combination withnivolumab 360 mg every 3 weeks and platinum-doublet chemotherapy every 3 weeks(for 2 cycles) in CHECKMATE-9LA (NSCLC), 51% were 65 years or older and 10% were75 years or older. No overall difference in safety was reported between older patientsand younger patients; however, there was a higher discontinuation rate due to adverse
reactions in patients aged 75 years or older (43%) relative to all patients who receivedYERVOY with nivolumab and chemotherapy (24%). For patients aged 75 years or olderwho received chemotherapy only, the discontinuation rate due to adverse reactions was16% relative to all patients who had a discontinuation rate of 13%. Based on an updatedanalysis for overall survival, of the 361 patients randomized to YERVOY in combinationwith nivolumab and platinum-doublet chemotherapy in CHECKMATE-9LA, the hazardratio for overall survival was 0.61 (95% CI: 0.47, 0.80) in the 176 patients younger than65 years compared to 0.73 (95% CI: 0.56, 0.95) in the 185 patients 65 years or older.Of the 303 patients randomized to YERVOY 1 mg/kg every 6 weeks in combination withnivolumab 3 mg/kg every 2 weeks in CHECKMATE-743 (malignant pleural mesothelioma),77% were 65 years old or older and 26% were 75 years or older. No overall difference insafety was reported between older patients and younger patients; however, there werehigher rates of serious adverse reactions and discontinuation rate due to adversereactions in patients aged 75 years or older (68% and 35%, respectively) relative to allpatients who received YERVOY with nivolumab (54% and 28%, respectively). For patientsaged 75 years or older who received chemotherapy, the rate of serious adversereactions was 34% and discontinuation due to adverse reactions was 26% relative to28% and 19% respectively for all patients. The hazard ratio for overall survival was 0.76(95% CI: 0.52, 1.11) in the 71 patients younger than 65 years compared to 0.74 (95%CI: 0.59, 0.93) in the 232 patients 65 years or older randomized to YERVOY incombination with nivolumab.
11 DESCRIPTIONIpilimumab is a human cytotoxic T-lymphocyte antigen 4 (CTLA-4)-blocking antibody.Ipilimumab is a recombinant IgG1 kappa immunoglobulin with an approximate molecularweight of 148 kDa. Ipilimumab is produced in mammalian (Chinese hamster ovary) cellculture.YERVOY (ipilimumab) injection, for intravenous use is a sterile, preservative-free, clear toslightly opalescent, colorless to pale-yellow solution, which may contain a small amountof visible translucent-to-white, amorphous ipilimumab particulates. It is supplied in single-dose vials of 50 mg/10 mL or 200 mg/40 mL. Each milliliter contains 5 mg of ipilimumaband the following inactive ingredients: diethylene triamine pentaacetic acid (DTPA) (0.04mg), mannitol (10 mg), polysorbate 80 (vegetable origin) (0.1 mg), sodium chloride (5.85mg), tris hydrochloride (3.15 mg), and Water for Injection, USP at a pH of 7.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of ActionCTLA-4 is a negative regulator of T-cell activity. Ipilimumab is a monoclonal antibody thatbinds to CTLA-4 and blocks the interaction of CTLA-4 with its ligands, CD80/CD86.Blockade of CTLA-4 has been shown to augment T-cell activation and proliferation,including the activation and proliferation of tumor infiltrating T-effector cells. Inhibition ofCTLA-4 signaling can also reduce T-regulatory cell function, which may contribute to ageneral increase in T cell responsiveness, including the anti-tumor immune response.
12.3 Pharmacokinetics
The pharmacokinetics (PK) of ipilimumab was studied in 785 patients with unresectableor metastatic melanoma who received doses of 0.3, 3, or 10 mg/kg once every 3 weeksfor 4 doses. The PK of ipilimumab is linear in the dose range of 0.3 mg/kg to 10 mg/kg.Following administration of YERVOY every 3 weeks, the systemic accumulation was 1.5-fold or less. Steady-state concentrations of ipilimumab were reached by the third dose;the mean minimum concentration (C ) at steady state was 19.4 mcg/mL at 3 mg/kgand 58.1 mcg/mL at 10 mg/kg every 3 weeks.EliminationThe mean (percent coefficient of variation) terminal half-life (t ) was 15.4 days (34%)and then mean (percent coefficient of variation) clearance (CL) was 16.8 mL/h (38%).The CL of ipilimumab was unchanged in presence of anti-ipilimumab antibodies.Specific PopulationsThe CL of ipilimumab increased with increasing body weight supporting therecommended body weight (mg/kg) based dosing. The following factors had no clinicallyimportant effect on the CL of ipilimumab: age (range: 23 to 88 years), sex, performancestatus, renal impairment (glomerular filtration rate ≥15 mL/min/1.73 m ), mild hepaticimpairment (total bilirubin [TB] >1 to 1.5 times the upper limit of normal [ULN] or AST >ULN), previous cancer therapy, and baseline lactate dehydrogenase (LDH) levels. Theeffect of race was not examined due to limited data available in non-White racial groups.YERVOY has not been studied in patients with moderate (TB > 1.5 to 3 times ULN andany AST) or severe (TB >3 times ULN and any AST) hepatic impairment.Pediatric Patients: Based on a population PK analysis using available pooled data from565 patients from four adult studies (n=521) and two pediatric studies (n=44), bodyweight normalized clearance of ipilimumab is comparable between adult and pediatricpatients. In pediatric patients with a dosing regimen of 3 mg/kg every 3 weeks, themodel simulated geometric mean (CV%) steady-state serum peak and troughconcentrations of ipilimumab were 65.8 (17.6%) and 20.7 (33.1%) mcg/mL (for 2 to 6years old), 70.1 (19.6%) and 19.6 (42.9%) mcg/mL (for 6 to <12 years old), and 73.3(20.6%) and 17.8 (50.8%) mcg/mL (for 12 years and older), which are comparable tothose in adult patients.Drug Interaction StudiesIpilimumab with Nivolumab
When YERVOY 1 mg/kg was administered with nivolumab 3 mg/kg every 3 weeks, the CLof ipilimumab was unchanged compared to when YERVOY was administered alone.When YERVOY 3 mg/kg every 3 weeks was administered in combination with nivolumab1 mg/kg every 3 weeks, the CL of ipilimumab was unchanged compared to ipilimumabadministered alone and the CL of nivolumab was increased by 29% compared tonivolumab administered alone.When YERVOY 1 mg/kg every 6 weeks was administered in combination with nivolumab3 mg/kg every 2 weeks, the CL of ipilimumab increased by 30% compared to YERVOYadministered alone and the CL of nivolumab was unchanged compared to nivolumabadministered alone.When YERVOY 1 mg/kg every 6 weeks was administered in combination with nivolumab360 mg every 3 weeks and chemotherapy, the CL of ipilimumab increased by 22%
min
1/2
2
compared to YERVOY administered alone and the CL of nivolumab was unchangedcompared to nivolumab administered alone.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityThe carcinogenic potential of ipilimumab has not been evaluated in long-term animalstudies, and the genotoxic potential of ipilimumab has not been evaluated.Fertility studies have not been performed with ipilimumab.
14 CLINICAL STUDIES
14.1 Unresectable or Metastatic MelanomaThe efficacy of YERVOY were investigated in a Study MDX010-20, a randomized (3:1:1),double-blind, double-dummy trial (NCT00094653) that included patients withunresectable or metastatic melanoma previously treated with one or more of thefollowing: aldesleukin, dacarbazine, temozolomide, fotemustine, or carboplatin. The trialenrolled only patients with HLA-A2*0201 genotype; this HLA genotype facilitates theimmune presentation of the investigational peptide vaccine. The trial excluded patientswith active autoimmune disease or those receiving systemic immunosuppression fororgan transplantation. Patients were randomized to YERVOY administered at a dose of 3mg/kg as an intravenous infusion every 3 weeks for 4 doses with an investigationalpeptide vaccine with incomplete Freund’s adjuvant - gp100 administered at a dose of 2mg peptide by deep subcutaneous injection every 3 weeks for 4 doses; gp100administered at a dose of 2 mg by deep subcutaneous injection every 3 weeks for 4doses as a single agent with a placebo; or YERVOY administered at a dose of 3 mg/kg byintravenous infusion every 3 weeks for 4 doses with a placebo. The major efficacyoutcome measure was overall survival (OS) in the YERVOY and gp100 arm compared tothat in the single-agent gp100 arm. Secondary efficacy outcome measures were OS inthe YERVOY and gp100 arm compared to the YERVOY arm, OS in the YERVOY armcompared to the gp100 arm, best overall response rate (BORR) as assessed by theinvestigator at week 24 between each of the trial arms, and duration of response.Assessment of tumor response was conducted at weeks 12 and 24, and every 3months thereafter. Patients with evidence of objective tumor response at 12 or 24weeks had assessment for confirmation of durability of response at 16 or 28 weeks,respectively.A total of 676 patients were randomized, 403 to YERVOY and gp100 arm, 137 toYERVOY single agent arm and 136 to gp100 single agent arm. Of the randomizedpatients, 61%, 59%, and 54% in the YERVOY and gp100, YERVOY, and gp100 arms,respectively, were male. Twenty-nine percent were ≥65 years of age, the median agewas 57 years, 71% had M1c stage, 12% had a history of previously treated brainmetastasis, 98% had ECOG performance status of 0 and 1, 23% had receivedaldesleukin, and 38% had elevated LDH level. Sixty-one percent of patients randomizedto either YERVOY-containing arm received all 4 planned doses. The median duration offollow-up was 8.9 months.The efficacy results are shown in Table 21 and Figure 1.
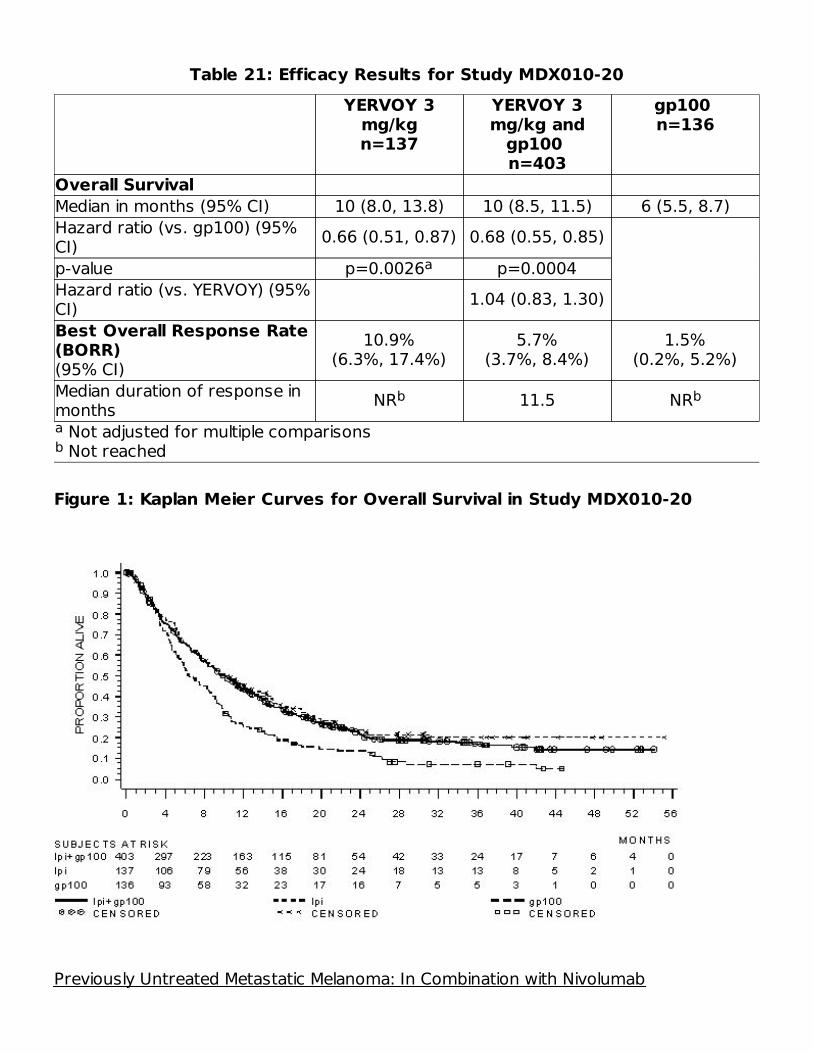
Table 21: Efficacy Results for Study MDX010-20
Not adjusted for multiple comparisons Not reached
YERVOY 3mg/kgn=137
YERVOY 3mg/kg and
gp100 n=403
gp100 n=136
Overall SurvivalMedian in months (95% CI) 10 (8.0, 13.8) 10 (8.5, 11.5) 6 (5.5, 8.7)Hazard ratio (vs. gp100) (95%CI) 0.66 (0.51, 0.87) 0.68 (0.55, 0.85)p-value p=0.0026 p=0.0004Hazard ratio (vs. YERVOY) (95%CI) 1.04 (0.83, 1.30)Best Overall Response Rate(BORR)(95% CI)
10.9%(6.3%, 17.4%)
5.7%(3.7%, 8.4%)
1.5%(0.2%, 5.2%)
Median duration of response inmonths NR 11.5 NR
Figure 1: Kaplan Meier Curves for Overall Survival in Study MDX010-20
Previously Untreated Metastatic Melanoma: In Combination with Nivolumab
ab
a
b b

CHECKMATE-067 (NCT01844505) was a multicenter, randomized (1:1:1), double-blindtrial in which 945 patients with previously untreated, unresectable or metastaticmelanoma were randomized to one of the following arms: YERVOY and nivolumab,nivolumab, or YERVOY. Patients were required to have completed adjuvant orneoadjuvant treatment at least 6 weeks prior to randomization and have no priortreatment with anti-CTLA-4 antibody and no evidence of active brain metastasis, ocularmelanoma, autoimmune disease, or medical conditions requiring systemicimmunosuppression.Patients were randomized to receive:
•
••
Randomization was stratified by PD-L1 expression (≥5% vs. <5% tumor cell membraneexpression) as determined by a clinical trial assay, BRAF V600 mutation status, and Mstage per the AJCC staging system (M0, M1a, M1b vs. M1c). Tumor assessments wereconducted 12 weeks after randomization then every 6 weeks for the first year, andevery 12 weeks thereafter. The major efficacy outcome measures were investigator-assessed PFS per RECIST v1.1 and OS. Additional efficacy outcome measures wereconfirmed ORR and duration of response.The trial population characteristics were: median age 61 years (range: 18 to 90); 65%male; 97% White; ECOG performance score 0 (73%) or 1 (27%). Disease characteristicswere: AJCC Stage IV disease (93%); M1c disease (58%); elevated LDH (36%); history ofbrain metastases (4%); BRAF V600 mutation-positive melanoma (32%); PD-L1 ≥5%tumor cell membrane expression as determined by the clinical trials assay (46%); andprior adjuvant therapy (22%).CHECKMATE-067 demonstrated statistically significant improvements in OS and PFS forpatients randomized to either nivolumab-containing arm as compared with the YERVOYarm. The trial was not designed to assess whether adding YERVOY to nivolumabimproves PFS or OS compared to nivolumab as a single agent. Efficacy results areshown in Table 22 and Figure 2.
Table 22: Efficacy Results - CHECKMATE-067YERVOY andNivolumab
(n=314)Nivolumab
(n=316)YERVOY(n=315)
Overall Survival Deaths (%) 128 (41) 142 (45) 197 (63) Hazard ratio (vs. YERVOY) (95% CI)
0.55(0.44, 0.69)
0.63(0.50, 0.78)
p-value <0.0001 <0.0001Progression-free Survival Disease progression or 151 (48%) 174 (55%) 234 (74%)
YERVOY 3 mg/kg with nivolumab 1 mg/kg intravenously every 3 weeks for 4 doses,followed by nivolumab as a single agent at a dose of 3 mg/kg by intravenousinfusion every 2 weeks (YERVOY and nivolumab arm),Nivolumab 3 mg/kg by intravenous infusion every 2 weeks (nivolumab arm), orYERVOY 3 mg/kg intravenously every 3 weeks for 4 doses followed by placeboevery 2 weeks (YERVOY arm)
a
b
c,da

OS results are based on final OS analysis with 28 months of minimum follow-up; PFS(co-primary endpoint) and ORR (secondary endpoint) results were based on primaryanalysis with 9 months of minimum follow-up. Based on a stratified proportional hazards model. Based on stratified log-rank test. If the maximum of the two OS p-values is less than 0.04 (a significance level assigned
by the Hochberg procedure), then both p-values are considered significant. p-value is compared with .005 of the allocated alpha for final PFS treatment
comparisons. Based on the stratified Cochran-Mantel-Haenszel test.+ Censored observation
death 151 (48%) 174 (55%) 234 (74%) Median (months) (95% CI)
11.5(8.9, 16.7)
6.9 (4.3, 9.5)
2.9 (2.8, 3.4)
Hazard ratio (vs. YERVOY) (95% CI)
0.42(0.34, 0.51)
0.57(0.47, 0.69)
p-value <0.0001 <0.0001Confirmed OverallResponse Rate 50% 40% 14% (95% CI) (44, 55) (34, 46) (10, 18) p-value <0.0001 <0.0001 Complete response 8.9% 8.5% 1.9% Partial response 41% 31% 12%Duration of Response Proportion ≥6 months induration 76% 74% 63% Range (months) 1.2+ to 15.8+ 1.3+ to 14.6+ 1.0+ to 13.8+
Figure 2: Overall Survival - CHECKMATE-067
a
bcd
e
f
b
c,e
a
f
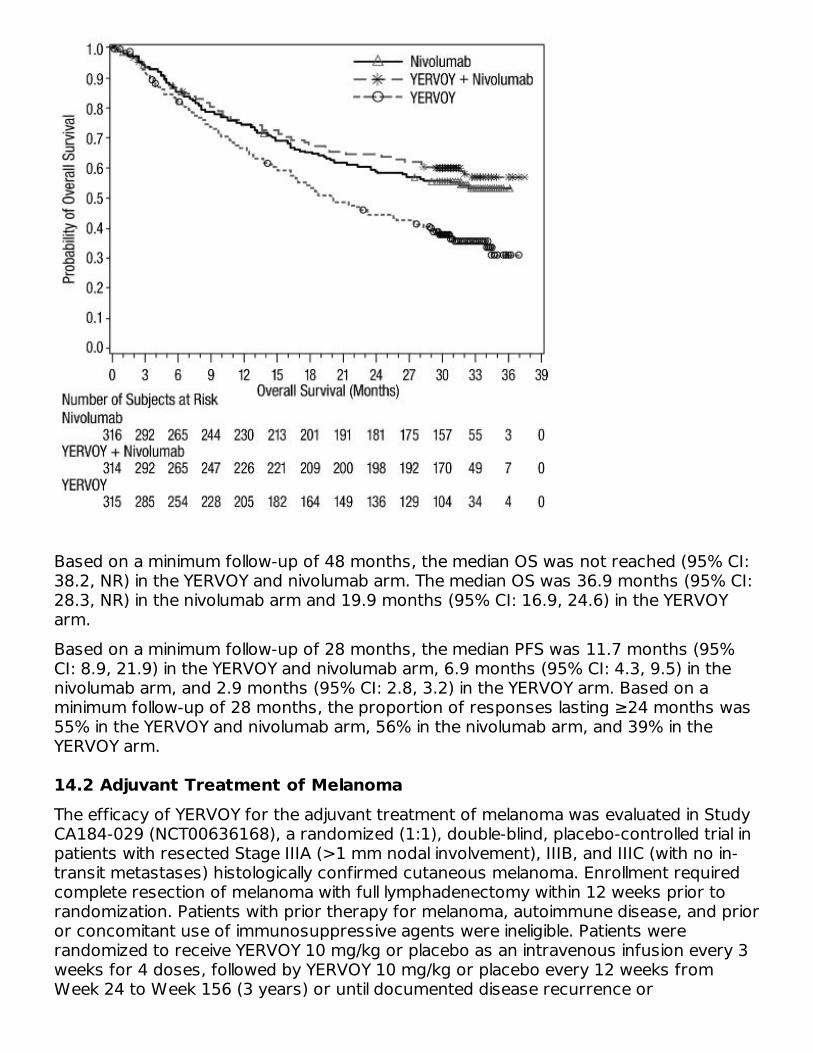
Based on a minimum follow-up of 48 months, the median OS was not reached (95% CI:38.2, NR) in the YERVOY and nivolumab arm. The median OS was 36.9 months (95% CI:28.3, NR) in the nivolumab arm and 19.9 months (95% CI: 16.9, 24.6) in the YERVOYarm.Based on a minimum follow-up of 28 months, the median PFS was 11.7 months (95%CI: 8.9, 21.9) in the YERVOY and nivolumab arm, 6.9 months (95% CI: 4.3, 9.5) in thenivolumab arm, and 2.9 months (95% CI: 2.8, 3.2) in the YERVOY arm. Based on aminimum follow-up of 28 months, the proportion of responses lasting ≥24 months was55% in the YERVOY and nivolumab arm, 56% in the nivolumab arm, and 39% in theYERVOY arm.
14.2 Adjuvant Treatment of MelanomaThe efficacy of YERVOY for the adjuvant treatment of melanoma was evaluated in StudyCA184-029 (NCT00636168), a randomized (1:1), double-blind, placebo-controlled trial inpatients with resected Stage IIIA (>1 mm nodal involvement), IIIB, and IIIC (with no in-transit metastases) histologically confirmed cutaneous melanoma. Enrollment requiredcomplete resection of melanoma with full lymphadenectomy within 12 weeks prior torandomization. Patients with prior therapy for melanoma, autoimmune disease, and prioror concomitant use of immunosuppressive agents were ineligible. Patients wererandomized to receive YERVOY 10 mg/kg or placebo as an intravenous infusion every 3weeks for 4 doses, followed by YERVOY 10 mg/kg or placebo every 12 weeks fromWeek 24 to Week 156 (3 years) or until documented disease recurrence or

unacceptable toxicity. Randomization was stratified by stage according to American JointCommittee on Cancer (AJCC) 2002 classification (Stage IIIA >1 mm nodal involvement,Stage IIIB, Stage IIIC with 1 to 3 involved lymph nodes, and Stage IIIC with ≥4 involvedlymph nodes) and by region (North America, Europe, and Australia). The major efficacyoutcome measures were independent review committee (IRC)-assessed recurrence-freesurvival (RFS), defined as the time between the date of randomization and the earliestdate of first recurrence (local, regional, or distant metastasis) or death, and overallsurvival. Tumor assessment was conducted every 12 weeks for the first 3 years thenevery 24 weeks until distant recurrence.Among 951 patients enrolled, 475 were randomized to receive YERVOY and 476 toplacebo. Median age was 51 years (range: 18 to 84), 62% were male, 99% were White,94% had ECOG performance status of 0. With regard to disease stage, 20% had StageIIIA with lymph nodes >1 mm, 44% had Stage IIIB, and 36% had Stage IIIC (with no in-transit metastases). Other disease characteristics of the trial population were: clinicallypalpable lymph nodes (58%), 2 or more positive lymph nodes (54%), and ulceratedprimary lesions (42%).The efficacy results are in Table 23 and Figure 3.
Table 23: Efficacy Results for Study CA184-029
Stratified by disease stage.
YERVOY 10 mg/kgn=475
Placebo n=476
Recurrence-Free SurvivalNumber of events 234 (49%) 294 (62%) Recurrence 220 289 Death 14 5Median in months (95% CI) 26 (19, 39) 17 (13, 22)Hazard ratio (95% CI) 0.75 (0.64, 0.90)p-value (stratified log-rank ) p<0.002Overall SurvivalNumber of deaths 162 (34%) 214 (45%)Hazard ratio (95% CI) 0.72 (0.58, 0.88)p-value (stratified log-rank ) p<0.002
Figure 3: Kaplan-Meier Curves for Overall Survival in Study CA184-029
a
a
a
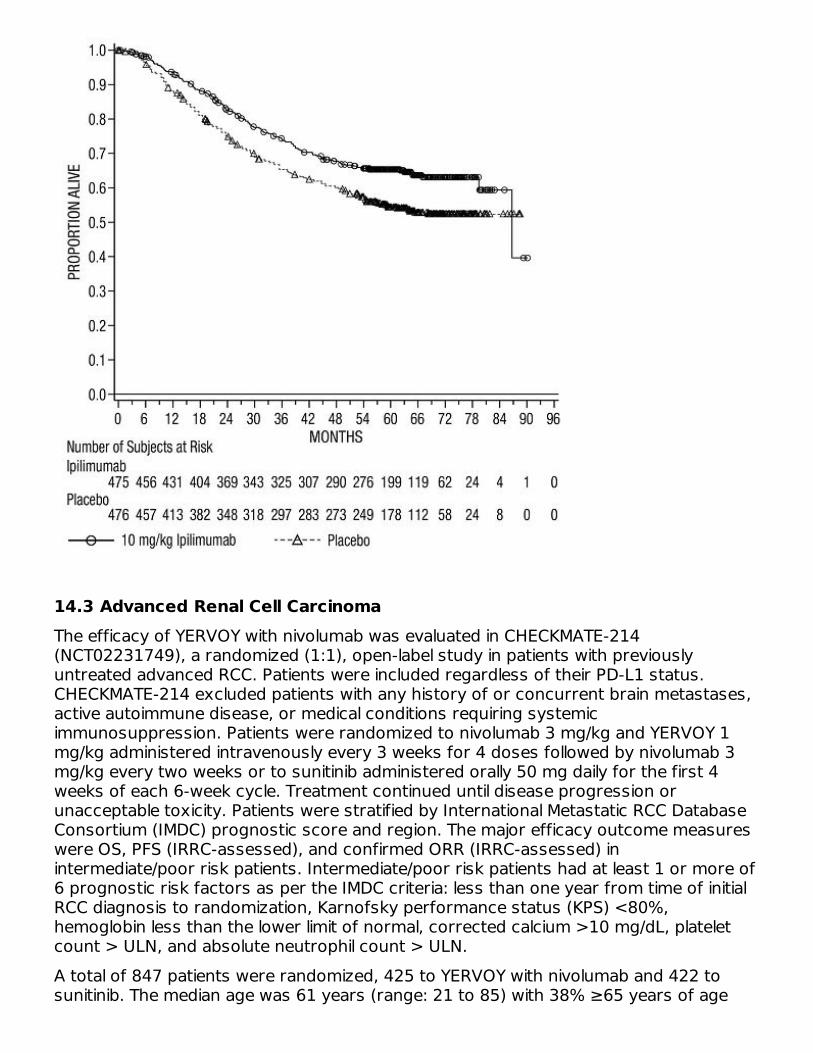
14.3 Advanced Renal Cell CarcinomaThe efficacy of YERVOY with nivolumab was evaluated in CHECKMATE-214(NCT02231749), a randomized (1:1), open-label study in patients with previouslyuntreated advanced RCC. Patients were included regardless of their PD-L1 status.CHECKMATE-214 excluded patients with any history of or concurrent brain metastases,active autoimmune disease, or medical conditions requiring systemicimmunosuppression. Patients were randomized to nivolumab 3 mg/kg and YERVOY 1mg/kg administered intravenously every 3 weeks for 4 doses followed by nivolumab 3mg/kg every two weeks or to sunitinib administered orally 50 mg daily for the first 4weeks of each 6-week cycle. Treatment continued until disease progression orunacceptable toxicity. Patients were stratified by International Metastatic RCC DatabaseConsortium (IMDC) prognostic score and region. The major efficacy outcome measureswere OS, PFS (IRRC-assessed), and confirmed ORR (IRRC-assessed) inintermediate/poor risk patients. Intermediate/poor risk patients had at least 1 or more of6 prognostic risk factors as per the IMDC criteria: less than one year from time of initialRCC diagnosis to randomization, Karnofsky performance status (KPS) <80%,hemoglobin less than the lower limit of normal, corrected calcium >10 mg/dL, plateletcount > ULN, and absolute neutrophil count > ULN.A total of 847 patients were randomized, 425 to YERVOY with nivolumab and 422 tosunitinib. The median age was 61 years (range: 21 to 85) with 38% ≥65 years of age

and 8% ≥75 years of age. The majority of patients were male (73%) and White (87%)and 26% and 74% of patients had a baseline KPS of 70% to 80% and 90% to 100%,respectively.Efficacy results from CHECKMATE-214 are presented in Table 24 and Figure 4. Inintermediate/poor risk patients, the trial demonstrated statistically significantimprovement in OS and ORR for patients randomized to YERVOY and nivolumab arm ascompared with sunitinib arm. OS benefit was observed regardless of PD-L1 expressionlevel. The trial did not demonstrate a statistically significant improvement in PFS.
Table 24: Efficacy Results for CHECKMATE-214
Based on a stratified proportional hazards model. Based on a stratified log-rank test. p-value is compared to alpha 0.002 in order to achieve statistical significance. Based on the stratified DerSimonian-Laird test. p-value is compared to alpha 0.001 in order to achieve statistical significance. Not Significant at alpha level of 0.009
Efficacy Parameter Intermediate/Poor-RiskYERVOY 1 mg/kgand Nivolumab
n=425Sunitinibn=422
Overall Survival Number of deaths 140 (32.9%) 188 (44.5%) Median in months NE 25.9 Hazard ratio (99.8% CI) 0.63 (0.44, 0.89) p-value <0.0001Confirmed Objective Response Rate(95% CI)
41.6% (36.9%, 46.5%) 26.5% (22.4%, 31.0%)
Complete Response 40 (9.4%) 5 (1.2%) Partial Response 137 (32.2%) 107 (25.4%) Median duration of response inmonths (95% CI)
NE (21.8, NE) 18.2 (14.8, NE)
p-value <0.0001Progression-free Survival Number of events (progression ordeath)
228 (53.6%) 228 (54.0%)
Median in months 11.6 8.4 Hazard ratio (99.1% CI) 0.82 (0.64, 1.05) p-value NS
Figure 4: Kaplan-Meier Curves for Overall Survival (Intermediate/Poor RiskPopulation) in CHECKMATE-214
abcdef
ab,c
d,e
ab f

CHECKMATE-214 also randomized 249 favorable risk patients as per IMDC criteria tonivolumab and YERVOY (n=125) or to sunitinib (n=124). These patients were notevaluated as part of the efficacy analysis population. OS in favorable risk patientsreceiving nivolumab and YERVOY compared to sunitinib has a hazard ratio of 1.45 (95%CI: 0.75, 2.81). The efficacy of nivolumab and YERVOY in previously untreated renal cellcarcinoma with favorable risk disease has not been established.
14.4 Microsatellite Instability-High or Mismatch Repair Deficient MetastaticColorectal CancerThe efficacy of YERVOY with nivolumab was evaluated in CHECKMATE-142(NCT02060188), a multicenter, non-randomized, multiple parallel-cohort, open-labelstudy conducted in patients with locally determined dMMR or MSI-H mCRC who haddisease progression during or after prior treatment with fluoropyrimidine-, oxaliplatin-,or irinotecan-based chemotherapy. Key eligibility criteria were at least one prior line oftreatment for metastatic disease, ECOG PS 0 or 1, and absence of the following: activebrain metastases, active autoimmune disease, or medical conditions requiring systemicimmunosuppression. Patients enrolled in the YERVOY and nivolumab MSI-H or dMMRmCRC cohort received YERVOY 1 mg/kg and nivolumab 3 mg/kg intravenously every 3weeks for 4 doses, followed by nivolumab 3 mg/kg intravenously as a single agent every2 weeks. Efficacy outcome measures were overall response rate (ORR) as assessed byBlinded Independent Central Review (BICR) using Response Evaluation Criteria in SolidTumors (RECIST v1.1) and duration of response (DOR). Tumor assessments wereconducted every 6 weeks for the first 24 weeks and every 12 weeks thereafter.A total of 119 patients were enrolled in the YERVOY and nivolumab cohort. The medianage was 58 years (range: 21 to 88), with 32% ≥65 years of age and 9% ≥75 years ofage; 59% were male and 92% were white. Baseline ECOG PS was 0 (45%) or 1 (55%),
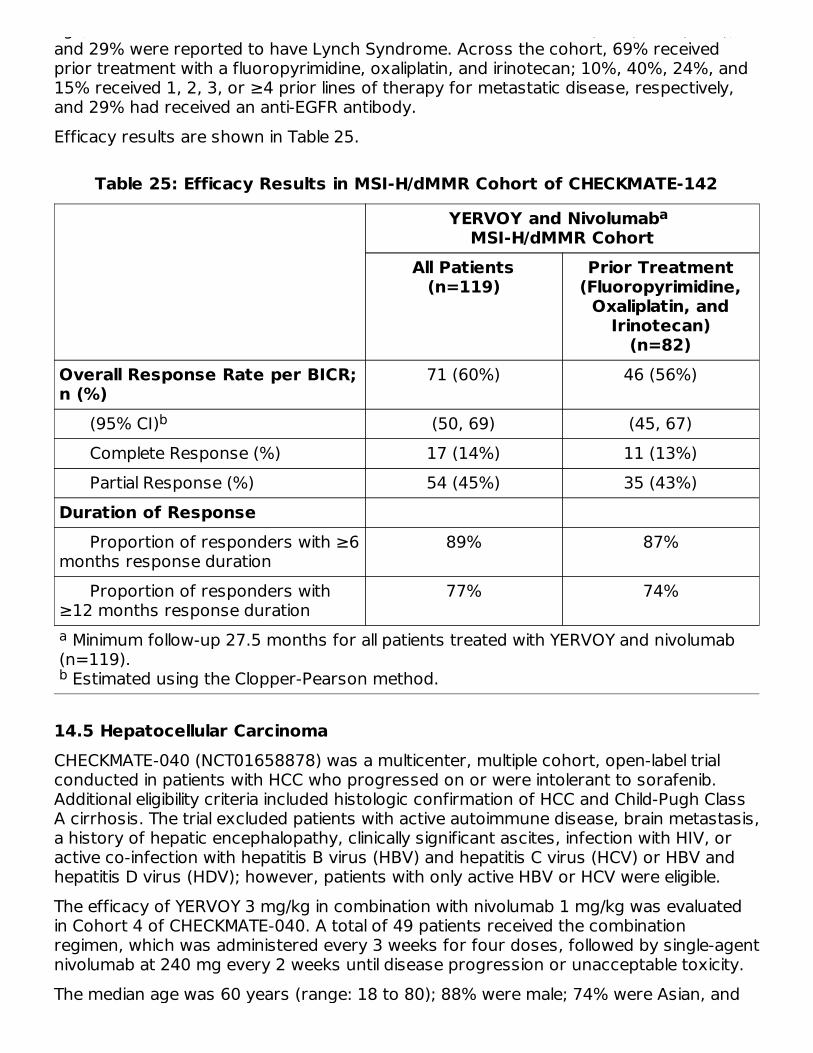
age; 59% were male and 92% were white. Baseline ECOG PS was 0 (45%) or 1 (55%),and 29% were reported to have Lynch Syndrome. Across the cohort, 69% receivedprior treatment with a fluoropyrimidine, oxaliplatin, and irinotecan; 10%, 40%, 24%, and15% received 1, 2, 3, or ≥4 prior lines of therapy for metastatic disease, respectively,and 29% had received an anti-EGFR antibody.Efficacy results are shown in Table 25.
Table 25: Efficacy Results in MSI-H/dMMR Cohort of CHECKMATE-142
Minimum follow-up 27.5 months for all patients treated with YERVOY and nivolumab(n=119). Estimated using the Clopper-Pearson method.
YERVOY and Nivolumab MSI-H/dMMR Cohort
All Patients(n=119)
Prior Treatment(Fluoropyrimidine,
Oxaliplatin, andIrinotecan)
(n=82)Overall Response Rate per BICR;n (%)
71 (60%) 46 (56%)
(95% CI) (50, 69) (45, 67) Complete Response (%) 17 (14%) 11 (13%) Partial Response (%) 54 (45%) 35 (43%)Duration of Response Proportion of responders with ≥6months response duration
89% 87%
Proportion of responders with≥12 months response duration
77% 74%
14.5 Hepatocellular CarcinomaCHECKMATE-040 (NCT01658878) was a multicenter, multiple cohort, open-label trialconducted in patients with HCC who progressed on or were intolerant to sorafenib.Additional eligibility criteria included histologic confirmation of HCC and Child-Pugh ClassA cirrhosis. The trial excluded patients with active autoimmune disease, brain metastasis,a history of hepatic encephalopathy, clinically significant ascites, infection with HIV, oractive co-infection with hepatitis B virus (HBV) and hepatitis C virus (HCV) or HBV andhepatitis D virus (HDV); however, patients with only active HBV or HCV were eligible.The efficacy of YERVOY 3 mg/kg in combination with nivolumab 1 mg/kg was evaluatedin Cohort 4 of CHECKMATE-040. A total of 49 patients received the combinationregimen, which was administered every 3 weeks for four doses, followed by single-agentnivolumab at 240 mg every 2 weeks until disease progression or unacceptable toxicity.The median age was 60 years (range: 18 to 80); 88% were male; 74% were Asian, and
a
b
a
b

25% were White. Baseline ECOG performance status was 0 (61%) or 1 (39%). Fifty-seven percent (57%) of patients had active HBV infection, 8% had active HCV infection,and 35% had no evidence of active HBV or HCV. The etiology for HCC was alcoholic liverdisease in 16% and non-alcoholic liver disease in 6% of patients. Child-Pugh class andscore was A5 for 82% and A6 for 18%; 80% of patients had extrahepatic spread; 35%had vascular invasion; and 51% had alfa-fetoprotein (AFP) levels ≥400 µg/L. Priortreatment history included surgery (74%), radiotherapy (29%), or local treatment (59%).All patients had received prior sorafenib, of whom 10% were unable to toleratesorafenib; 29% of patients had received 2 or more prior systemic therapies.Efficacy results are shown in Table 26.
Table 26: Efficacy Results - Cohort 4 of CHECKMATE-040
Confirmed by BICR. Confidence interval is based on the Clopper and Pearson method.
YERVOY and Nivolumab(Cohort 4)
(n=49)Overall Response Rate per BICR, n (%),RECIST v1.1 16 (33%)
(95% CI) (20, 48) Complete response 4 (8%) Partial response 12 (24%)Duration of Response per BICR, RECISTv1.1 n=16
Range (months) 4.6, 30.5+ Percent with duration ≥6 months 88% Percent with duration ≥12 months 56% Percent with duration ≥24 months 31%Overall Response Rate per BICR, n (%),mRECIST 17 (35%)
(95% CI) (22, 50) Complete response 6 (12%) Partial response 11 (22%)
14.6 Metastatic Non-Small Cell Lung Cancer
First-line Treatment of Metastatic Non-Small Cell Lung Cancer (NSCLC) Expressing PD-L1(≥1%): In Combination with NivolumabCHECKMATE-227 (NCT02477826) was a randomized, open-label, multi-part trial inpatients with metastatic or recurrent NSCLC. The study included patients (18 years of
ab
a
b
a
a
b

age or older) with histologically confirmed Stage IV or recurrent NSCLC (per the 7thInternational Association for the Study of Lung Cancer [ASLC] classification), ECOGperformance status 0 or 1, and no prior anticancer therapy. Patients were enrolledregardless of their tumor PD-L1 status. Patients with known EGFR mutations or ALKtranslocations sensitive to available targeted inhibitor therapy, untreated brainmetastases, carcinomatous meningitis, active autoimmune disease, or medicalconditions requiring systemic immunosuppression were excluded from the study.Patients with treated brain metastases were eligible if neurologically returned to baselineat least 2 weeks prior to enrolment, and either off corticosteroids, or on a stable ordecreasing dose of <10 mg daily prednisone equivalents.Primary efficacy results were based on Part 1a of the study, which was limited topatients with PD-L1 tumor expression ≥1%. Tumor specimens were evaluatedprospectively using the PD-L1 IHC 28-8 pharmDx assay at a central laboratory.Randomization was stratified by tumor histology (non-squamous versus squamous).The evaluation of efficacy relied on the comparison between:
•
•
Chemotherapy regimens consisted of pemetrexed (500 mg/m ) and cisplatin (75mg/m ) or pemetrexed (500 mg/m ) and carboplatin (AUC 5 or 6) for non-squamousNSCLC or gemcitabine (1000 or 1250 mg/m ) and cisplatin (75 mg/m ) or gemcitabine(1000 mg/m ) and carboplatin (AUC 5) (gemcitabine was administered on Days 1 and 8of each cycle) for squamous NSCLC.Study treatment continued until disease progression, unacceptable toxicity, or for up to24 months. Treatment continued beyond disease progression if a patient was clinicallystable and was considered to be deriving clinical benefit by the investigator. Patients whodiscontinued combination therapy because of an adverse event attributed to YERVOYwere permitted to continue nivolumab as a single agent. Tumor assessments wereperformed every 6 weeks from the first dose of study treatment for the first 12months, then every 12 weeks until disease progression or study treatment wasdiscontinued. The primary efficacy outcome measure was OS. Additional efficacyoutcome measures included PFS, ORR, and duration of response as assessed by BICR.In Part 1a, a total of 793 patients were randomized to receive either YERVOY incombination with nivolumab (n=396) or platinum-doublet chemotherapy (n=397). Themedian age was 64 years (range: 26 to 87) with 49% of patients ≥65 years and 10% ofpatients ≥75 years, 76% White, and 65% male. Baseline ECOG performance status was0 (34%) or 1 (65%), 50% with PD-L1 ≥50%, 29% with squamous and 71% with non-squamous histology, 10% had brain metastases, and 85% were former/currentsmokers.The study demonstrated a statistically significant improvement in OS for PD-L1 ≥1%patients randomized to the YERVOY and nivolumab arm compared to platinum-doubletchemotherapy arm. The OS results are presented in Table 27 and Figure 5.
Table 27: Efficacy Results (PD-L1 ≥1%) - CHECKMATE-227 Part 1a
YERVOY 1 mg/kg administered intravenously over 30 minutes every 6 weeks incombination with nivolumab 3 mg/kg administered intravenously over 30 minutesevery 2 weeks; orPlatinum-doublet chemotherapy
22 2
2 22

Kaplan-Meier estimate. Based on a stratified Cox proportional hazard model.
YERVOY and Nivolumab(n=396)
Platinum-DoubletChemotherapy
(n=397)Overall Survival Events (%) 258 (65%) 298 (75%) Median (months) (95% CI)
17.1(15, 20.1)
14.9(12.7, 16.7)
Hazard ratio (95% CI) 0.79 (0.67, 0.94) Stratified log-rank p-value 0.0066
Figure 5: Overall Survival (PD-L1 ≥1%) - CHECKMATE-227
BICR-assessed PFS showed a HR of 0.82 (95% CI: 0.69, 0.97), with a median PFS of 5.1months (95% CI: 4.1, 6.3) in the YERVOY and nivolumab arm and 5.6 months (95% CI:4.6, 5.8) in the platinum-doublet chemotherapy arm. The BICR-assessed confirmed ORRwas 36% (95% CI: 31, 41) in the YERVOY and nivolumab arm and 30% (95% CI: 26, 35)in the platinum-doublet chemotherapy arm. Median duration of response observed in the
ab
a
b
YERVOY and nivolumab arm was 23.2 months and 6.2 months in the platinum-doubletchemotherapy arm.
First-line Treatment of Metastatic or Recurrent NSCLC: In Combination with Nivolumaband Platinum-Doublet ChemotherapyCHECKMATE-9LA (NCT03215706) was a randomized, open-label trial in patients withmetastatic or recurrent NSCLC. The trial included patients (18 years of age or older) withhistologically confirmed Stage IV or recurrent NSCLC (per the 7th InternationalAssociation for the Study of Lung Cancer classification [IASLC]), ECOG performancestatus 0 or 1, and no prior anticancer therapy (including EGFR and ALK inhibitors) formetastatic disease. Patients were enrolled regardless of their tumor PD-L1 status.Patients with known EGFR mutations or ALK translocations sensitive to available targetedinhibitor therapy, untreated brain metastases, carcinomatous meningitis, activeautoimmune disease, or medical conditions requiring systemic immunosuppression wereexcluded from the study. Patients with stable brain metastases were eligible forenrollment.Patients were randomized 1:1 to receive either:
•
•
Platinum-doublet chemotherapy consisted of either carboplatin (AUC 5 or 6) andpemetrexed 500 mg/m , or cisplatin 75 mg/m and pemetrexed 500 mg/m for non-squamous NSCLC; or carboplatin (AUC 6) and paclitaxel 200 mg/m for squamousNSCLC. Patients with non-squamous NSCLC in the control arm could receive optionalpemetrexed maintenance therapy. Stratification factors for randomization were tumorPD-L1 expression level (≥1% versus <1% or non‑quantifiable), histology (squamousversus non-squamous), and sex (male versus female). Study treatment continued untildisease progression, unacceptable toxicity, or for up to 2 years. Treatment couldcontinue beyond disease progression if a patient was clinically stable and wasconsidered to be deriving clinical benefit by the investigator. Patients who discontinuedcombination therapy because of an adverse reaction attributed to YERVOY werepermitted to continue nivolumab as a single agent as part of the study. Tumorassessments were performed every 6 weeks from the first dose of study treatment forthe first 12 months, then every 12 weeks until disease progression or study treatmentwas discontinued. The primary efficacy outcome measure was OS. Additional efficacyoutcome measures included PFS, ORR, and duration of response as assessed by BICR.A total of 719 patients were randomized to receive either YERVOY in combination withnivolumab and platinum-doublet chemotherapy (n=361) or platinum-doubletchemotherapy (n=358). The median age was 65 years (range: 26 to 86) with 51% ofpatients ≥65 years and 10% of patients ≥75 years. The majority of patients were White(89%) and male (70%). Baseline ECOG performance status was 0 (31%) or 1 (68%),57% had tumors with PD-L1 expression ≥1% and 37% had tumors with PD-L1expression that was <1%, 32% had tumors with squamous histology and 68% hadtumors with non-squamous histology, 17% had CNS metastases, and 86% were formeror current smokers.
YERVOY 1 mg/kg administered intravenously over 30 minutes every 6 weeks,nivolumab 360 mg administered intravenously over 30 minutes every 3 weeks, andplatinum-doublet chemotherapy administered intravenously every 3 weeks for 2cycles, orplatinum-doublet chemotherapy administered every 3 weeks for 4 cycles.
2 2 22

The study demonstrated a statistically significant benefit in OS, PFS, and ORR. Efficacyresults from the prespecified interim analysis when 351 events were observed (87% ofthe planned number of events for final analysis) are presented in Table 28.
Table 28: Efficacy Results - CHECKMATE-9LA
Based on a stratified Cox proportional hazard model. p-value is compared with the allocated alpha of 0.033 for this interim analysis. p-value is compared with the allocated alpha of 0.0252 for this interim analysis. Kaplan-Meier estimate. Confidence interval based on the Clopper and Pearson Method. p-value is compared with the allocated alpha of 0.025 for this interim analysis.
YERVOY and Nivolumaband Platinum-Doublet
Chemotherapy(n=361)
Platinum-DoubletChemotherapy
(n=358)Overall Survival Events (%) 156 (43.2) 195 (54.5) Median (months) (95% CI)
14.1(13.2, 16.2)
10.7(9.5, 12.5)
Hazard ratio (96.71% CI) 0.69 (0.55, 0.87) Stratified log-rank p-value 0.0006Progression-free Survival per BICR Events (%) 232 (64.3) 249 (69.6) Hazard ratio (97.48% CI) 0.70 (0.57, 0.86) Stratified log-rank p-value 0.0001 Median (months) (95% CI)
6.8(5.6, 7.7)
5.0(4.3, 5.6)
Overall Response Rate perBICR (%) 38 25 (95% CI) (33, 43) (21, 30) Stratified CMH test p-value 0.0003Duration of Response per BICR Median (months) (95% CI)
10.0(8.2, 13.0)
5.1(4.3, 7.0)
With an additional 4.6 months of follow-up the hazard ratio for overall survival was 0.66(95% CI: 0.55, 0.80) and median survival was 15.6 months (95% CI: 13.9, 20.0) and10.9 months (95% CI: 9.5, 12.5) for patients receiving YERVOY and nivolumab andplatinum-doublet chemotherapy or platinum-doublet chemotherapy, respectively (Figure6).Figure 6: Overall Survival - CHECKMATE-9LA
abcdef
ab
ac
d
ef
d
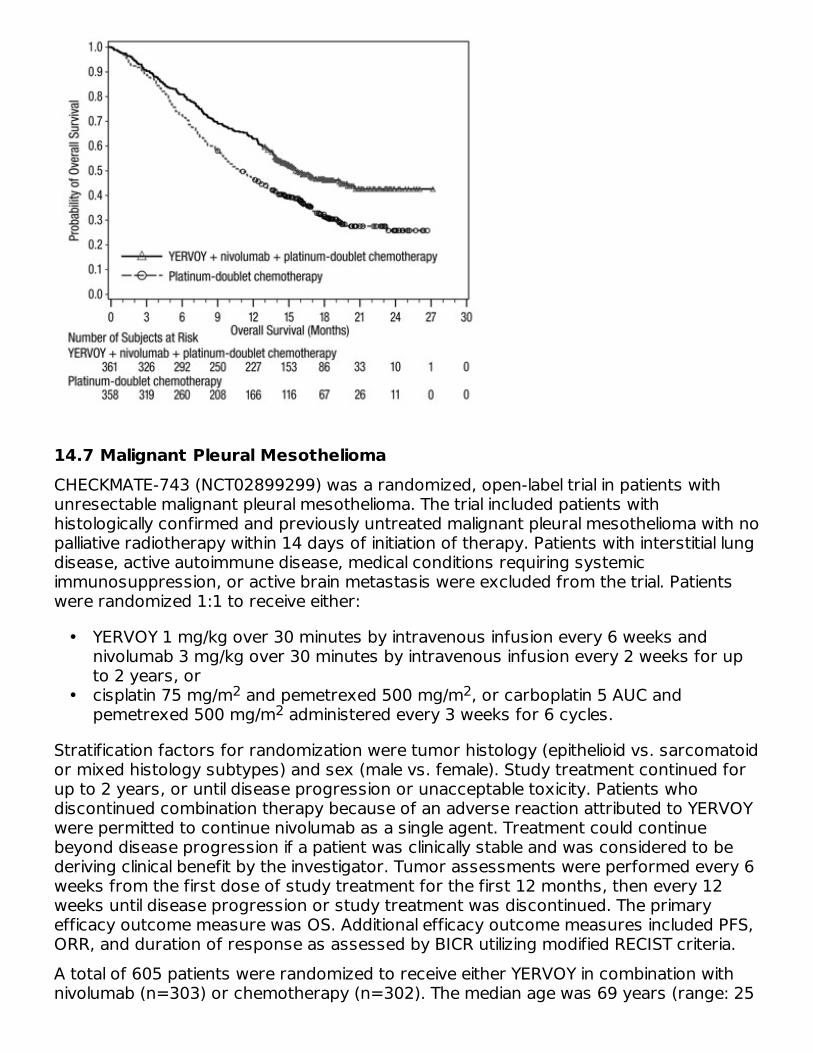
14.7 Malignant Pleural MesotheliomaCHECKMATE-743 (NCT02899299) was a randomized, open-label trial in patients withunresectable malignant pleural mesothelioma. The trial included patients withhistologically confirmed and previously untreated malignant pleural mesothelioma with nopalliative radiotherapy within 14 days of initiation of therapy. Patients with interstitial lungdisease, active autoimmune disease, medical conditions requiring systemicimmunosuppression, or active brain metastasis were excluded from the trial. Patientswere randomized 1:1 to receive either:
•
•
Stratification factors for randomization were tumor histology (epithelioid vs. sarcomatoidor mixed histology subtypes) and sex (male vs. female). Study treatment continued forup to 2 years, or until disease progression or unacceptable toxicity. Patients whodiscontinued combination therapy because of an adverse reaction attributed to YERVOYwere permitted to continue nivolumab as a single agent. Treatment could continuebeyond disease progression if a patient was clinically stable and was considered to bederiving clinical benefit by the investigator. Tumor assessments were performed every 6weeks from the first dose of study treatment for the first 12 months, then every 12weeks until disease progression or study treatment was discontinued. The primaryefficacy outcome measure was OS. Additional efficacy outcome measures included PFS,ORR, and duration of response as assessed by BICR utilizing modified RECIST criteria.A total of 605 patients were randomized to receive either YERVOY in combination withnivolumab (n=303) or chemotherapy (n=302). The median age was 69 years (range: 25
YERVOY 1 mg/kg over 30 minutes by intravenous infusion every 6 weeks andnivolumab 3 mg/kg over 30 minutes by intravenous infusion every 2 weeks for upto 2 years, orcisplatin 75 mg/m and pemetrexed 500 mg/m , or carboplatin 5 AUC andpemetrexed 500 mg/m administered every 3 weeks for 6 cycles.
2 22
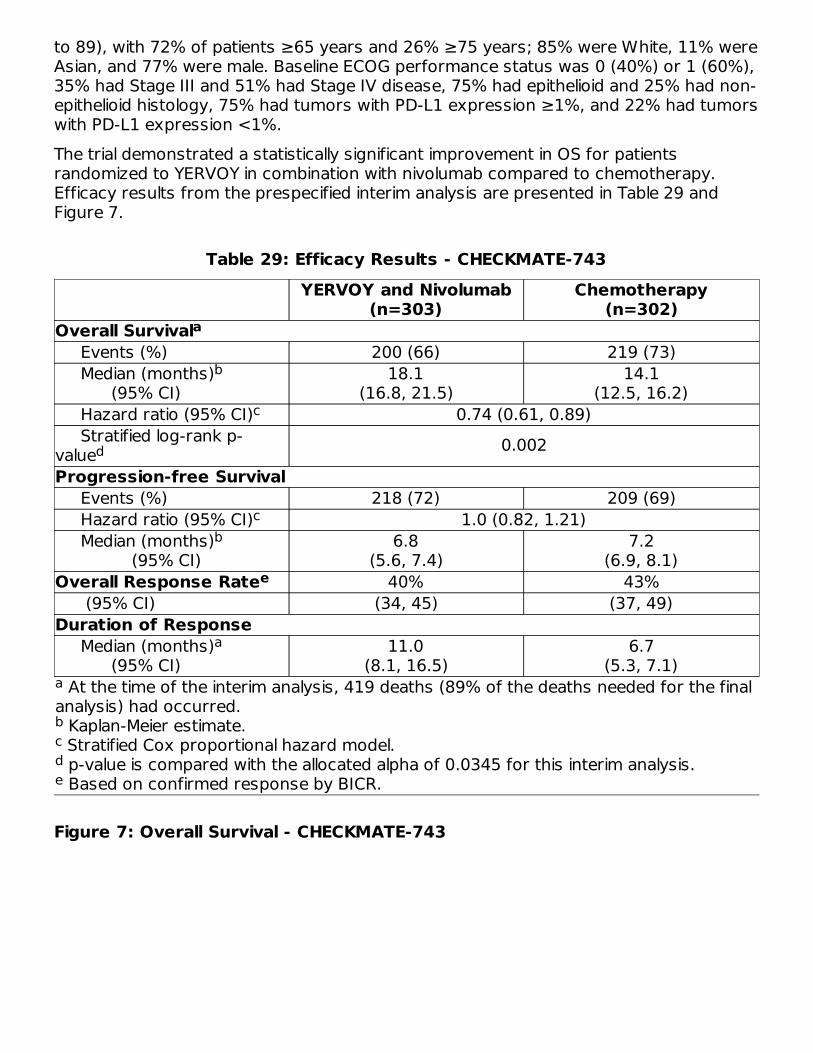
to 89), with 72% of patients ≥65 years and 26% ≥75 years; 85% were White, 11% wereAsian, and 77% were male. Baseline ECOG performance status was 0 (40%) or 1 (60%),35% had Stage III and 51% had Stage IV disease, 75% had epithelioid and 25% had non-epithelioid histology, 75% had tumors with PD-L1 expression ≥1%, and 22% had tumorswith PD-L1 expression <1%.The trial demonstrated a statistically significant improvement in OS for patientsrandomized to YERVOY in combination with nivolumab compared to chemotherapy.Efficacy results from the prespecified interim analysis are presented in Table 29 andFigure 7.
Table 29: Efficacy Results - CHECKMATE-743
At the time of the interim analysis, 419 deaths (89% of the deaths needed for the finalanalysis) had occurred. Kaplan-Meier estimate. Stratified Cox proportional hazard model. p-value is compared with the allocated alpha of 0.0345 for this interim analysis. Based on confirmed response by BICR.
YERVOY and Nivolumab(n=303)
Chemotherapy(n=302)
Overall Survival Events (%) 200 (66) 219 (73) Median (months) (95% CI)
18.1(16.8, 21.5)
14.1(12.5, 16.2)
Hazard ratio (95% CI) 0.74 (0.61, 0.89) Stratified log-rank p-value 0.002Progression-free Survival Events (%) 218 (72) 209 (69) Hazard ratio (95% CI) 1.0 (0.82, 1.21) Median (months) (95% CI)
6.8(5.6, 7.4)
7.2(6.9, 8.1)
Overall Response Rate 40% 43% (95% CI) (34, 45) (37, 49)Duration of Response Median (months) (95% CI)
11.0(8.1, 16.5)
6.7(5.3, 7.1)
Figure 7: Overall Survival - CHECKMATE-743
a
bcde
a
b
c
d
cb
e
a
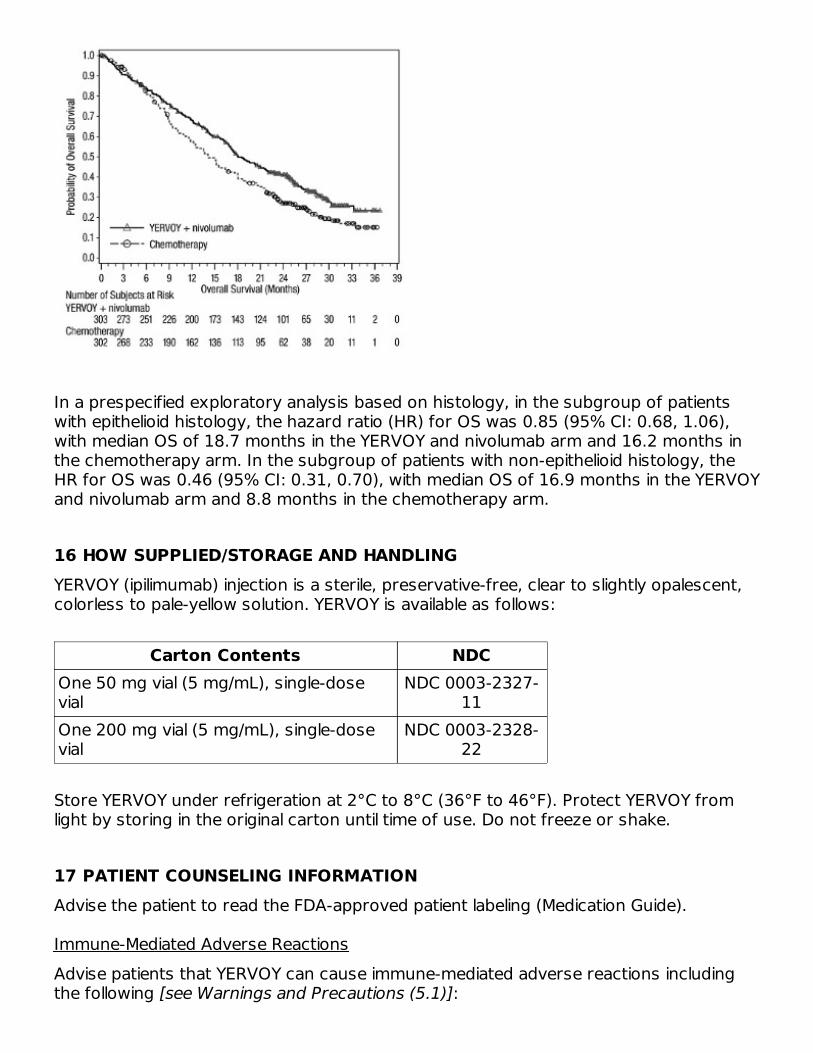
In a prespecified exploratory analysis based on histology, in the subgroup of patientswith epithelioid histology, the hazard ratio (HR) for OS was 0.85 (95% CI: 0.68, 1.06),with median OS of 18.7 months in the YERVOY and nivolumab arm and 16.2 months inthe chemotherapy arm. In the subgroup of patients with non-epithelioid histology, theHR for OS was 0.46 (95% CI: 0.31, 0.70), with median OS of 16.9 months in the YERVOYand nivolumab arm and 8.8 months in the chemotherapy arm.
16 HOW SUPPLIED/STORAGE AND HANDLINGYERVOY (ipilimumab) injection is a sterile, preservative-free, clear to slightly opalescent,colorless to pale-yellow solution. YERVOY is available as follows:
Carton Contents NDCOne 50 mg vial (5 mg/mL), single-dosevial
NDC 0003-2327-11
One 200 mg vial (5 mg/mL), single-dosevial
NDC 0003-2328-22
Store YERVOY under refrigeration at 2°C to 8°C (36°F to 46°F). Protect YERVOY fromlight by storing in the original carton until time of use. Do not freeze or shake.
17 PATIENT COUNSELING INFORMATIONAdvise the patient to read the FDA-approved patient labeling (Medication Guide).
Immune-Mediated Adverse ReactionsAdvise patients that YERVOY can cause immune-mediated adverse reactions includingthe following [see Warnings and Precautions (5.1)]:

•
•
•
•
•
•
Infusion-Related Reactions
•
Embryo-Fetal Toxicity
•
•
•
Lactation
•
Manufactured by: Bristol-Myers Squibb CompanyPrinceton, NJ 08543 USAU.S. License No. 1713[print code]
MEDICATION GUIDEYERVOY (yur-voi)
(ipilimumab) injection
Read this Medication Guide before you start receiving YERVOY and before each infusion.There may be new information. If your healthcare provider prescribes YERVOY incombination with nivolumab (OPDIVO ), also read the Medication Guide that comes withnivolumab. This Medication Guide does not take the place of talking with your healthcare
Immune-Mediated Diarrhea or Colitis: Advise patients to contact their healthcareprovider immediately for signs or symptoms of diarrhea or colitis.Immune-Mediated Hepatitis: Advise patients to contact their healthcare providerimmediately for signs or symptoms of hepatitis.Immune-Mediated Dermatologic Adverse Reactions: Advise patients to contact theirhealthcare provider immediately if they develop a new rash.Immune-Mediated Endocrinopathies: Advise patients to contact their healthcareprovider immediately for signs or symptoms of hypophysitis, adrenal insufficiency,hypothyroidism, hyperthyroidism, and diabetes mellitusImmune-Mediated Pneumonitis: Advise patients to contact their healthcare providerimmediately for any new or worsening symptoms of pneumonitis.Immune-Mediated Nephritis with Renal Dysfunction: Advise patients to contact theirhealthcare provider immediately for signs or symptoms of nephritis.
Advise patients who are receiving YERVOY of the potential risk of an infusion-relatedreaction [see Warnings and Precautions (5.2)].
Advise pregnant women of the potential risk to a fetus. Advise females ofreproductive potential to inform their healthcare provider of a known or suspectedpregnancy [see Warnings and Precautions (5.4), Use in Specific Populations (8.3)].Advise females of reproductive potential to use effective contraception duringtreatment with YERVOY and for 3 months after the last dose [see Use in SpecificPopulations (8.3)].Advise patients who may have been exposed to YERVOY during pregnancy tocontact Bristol-Myers Squibb at 1-844-593-7869 [see Use in Specific Populations(8.1)].
Advise women not to breastfeed during treatment with YERVOY and for 3 monthsafter the last dose [see Use in Specific Populations (8.2)].
®
®

nivolumab. This Medication Guide does not take the place of talking with your healthcareprovider about your medical condition or your treatment.What is the most important information I should know about YERVOY?YERVOY is a medicine that may treat certain cancers by working with your immunesystem. YERVOY can cause your immune system to attack normal organs and tissues inany area of your body and can affect the way they work. These problems cansometimes become severe or life-threatening and can lead to death. You may havemore than one of these problems at the same time. These problems may happenanytime during treatment or even after your treatment has ended. Some of theseproblems may happen more often when YERVOY is used in combination with nivolumab.Call or see your healthcare provider right away if you develop any new orworse signs or symptoms, including:Intestinal problems.
•••
Liver problems.
•
••
••
Skin problems.
••
••
Hormone gland problems.
•
•••••••
•••••••
Lung problems.
• • •
Kidney problems.
••
••
diarrhea (loose stools) or more frequent bowel movements than usualstools that are black, tarry, sticky, or have blood or mucussevere stomach-area (abdominal) pain or tenderness
yellowing of your skin or the whites ofyour eyessevere nausea or vomitingpain on the right side of your stomach-area (abdomen)
dark urine (tea colored)bleeding or bruising more easilythan normal
rashitching
skin blistering or peelingpainful sores in mouth or nose, throat,or genital area
headache that will not go away or unusualheadacheseye sensitivity to lighteye problemsrapid heartbeatincreased sweatingextreme tirednessweight gain or weight lossfeeling more hungry or thirsty than usual
urinating more often than usualhair lossfeeling coldconstipationyour voice gets deeperdizziness or faintingchanges in mood or behavior, suchas decreased sex drive, irritability,or forgetfulness
new or worsening cough shortness of breath chest pain
decrease in your amount of urineblood in your urine
swelling of your anklesloss of appetite

Eye problems.
• •
Problems can also happen in other organs and tissues. These are not all ofthe signs and symptoms of immune system problems that can happen withYERVOY. Call or see your healthcare provider right away for any new orworsening signs or symptoms.
••
•••
Getting medical treatment right away may help keep these problems frombecoming more serious. Your healthcare provider will check you for these problemsduring your treatment with YERVOY. Your healthcare provider may treat you withcorticosteroid or hormone replacement medicines. Your healthcare provider may alsoneed to delay or completely stop treatment with YERVOY if you have severe side effects.What is YERVOY?YERVOY is a prescription medicine used:
•
•
•
•
blurry vision, double vision, or othervision problems
eye pain or redness
Chest pain, irregular heartbeat, shortness of breath or swelling of anklesConfusion, sleepiness, memory problems, changes in mood or behavior, stiff neck,balance problems, tingling or numbness of the arms or legsDouble vision, blurry vision, sensitivity to light, eye pain, changes in eye sightPersistent or severe muscle pain or weakness, muscle crampsLow red blood cells, bruising
to treat a kind of skin cancer called melanoma.
o
o
YERVOY may be used alone in adults and children 12 years of age and older orin combination with nivolumab in adults when melanoma has spread or cannotbe removed by surgery.YERVOY may be used alone to help prevent melanoma from coming back afterit and lymph nodes that contain cancer have been removed by surgery.
in people with kidney cancer (renal cell carcinoma). YERVOY may be used incombination with nivolumab in certain people when their cancer has spread.in adults and children 12 years of age and older, with a type of colon orrectal cancer (colorectal cancer).
o YERVOY in combination with nivolumab may be used when your colon or rectalcancer:
▪▪
▪
has spread to other parts of the body (metastatic),is microsatellite instability-high (MSI-H) or mismatch repair deficient(dMMR), andyou have tried treatment with a fluoropyrimidine, oxaliplatin, andirinotecan, and it did not work or is no longer working.
in people with liver cancer (hepatocellular carcinoma).
o YERVOY may be used in combination with nivolumab if you have previouslyreceived treatment with sorafenib.

•
•
It is not known if YERVOY is safe and effective in children younger than 12 years of age.Before you receive YERVOY, tell your healthcare provider about all yourmedical conditions, including if you:
•••
•
•
received treatment with sorafenib.
in adults with a type of lung cancer called non-small cell lung cancer(NSCLC).
o
o
YERVOY may be used in combination with nivolumab as your first treatmentfor NSCLC:
▪
▪
when your lung cancer has spread to other parts of your body(metastatic), andyour tumors are positive for PD-L1, but do not have an abnormal EGFRor ALK gene.
YERVOY may be used in combination with nivolumab and 2 cycles ofchemotherapy that contains platinum and another chemotherapy medicine, asthe first treatment of your NSCLC when your lung cancer:
▪▪
has spread or grown, or comes back, andyour tumor does not have an abnormal EGFR or ALK gene.
in adults with a type of cancer that affects the lining of the lungs andchest wall called malignant pleural mesothelioma.
o YERVOY may be used in combination with nivolumab as your first treatmentfor malignant pleural mesothelioma that cannot be removed by surgery.
have immune system problems such as ulcerative colitis, Crohn’s disease, or lupushave received an organ transplanthave received or plan to receive a stem cell transplant that uses donor stem cells(allogeneic)have a condition that affects your nervous system, such as myasthenia gravis orGuillain-Barré syndromeare pregnant or plan to become pregnant. YERVOY can harm your unborn baby.Females who are able to become pregnant:Your healthcare provider will give you a pregnancy test before you start treatmentwith YERVOY.
o
o
o
o
You should use an effective method of birth control during your treatment andfor 3 months after the last dose of YERVOY. Talk to your healthcare providerabout birth control methods that you can use during this time.Tell your healthcare provider right away if you become pregnant or think youmay be pregnant during treatment with YERVOY. You or your healthcareprovider should contact Bristol-Myers Squibb at 1-844-593-7869 as soon asyou become aware of a pregnancy.are breastfeeding or plan to breastfeed. It is not known if YERVOY passes intoyour breast milk.Do not breastfeed during treatment with YERVOY and for 3 months after thelast dose of YERVOY.

Tell your healthcare provider about all the medicines you take, includingprescription and over-the-counter medicines, vitamins, and herbal supplements.How will I receive YERVOY?
•
•
•
•
••
•
What are the possible side effects of YERVOY?YERVOY can cause serious side effects, including:
•
•
oooo
oooo
•
YERVOY alone is given to you into your vein through an intravenous (IV) line over90 minutes.When YERVOY is used in combination with nivolumab (except for treatingunresectable or metastatic melanoma), nivolumab is given to you into your veinthrough an IV line over 30 minutes. Then YERVOY is also given through an IV over30 minutes on the same day.For unresectable or metastatic melanoma, when YERVOY is used in combinationwith nivolumab, nivolumab is given to you into your vein through an IV line over 30minutes. Then YERVOY is also given through an IV over 90 minutes on the sameday.YERVOY in combination with nivolumab is usually given every 3 weeks for 4 doses.After that, nivolumab alone is usually given every 2 or 4 weeks.
o
o
For NSCLC that has spread to other parts of your body, YERVOY is givenevery 6 weeks and nivolumab is given either every 2 or 3 weeks for up to 2years. Your healthcare provider will determine if you will also need to receivechemotherapy every 3 weeks for 2 cycles.For malignant pleural mesothelioma that cannot be removed by surgery,YERVOY is given every 6 weeks and nivolumab is given every 3 weeks for upto 2 years.
Your healthcare provider will decide how many treatments you will need.Your healthcare provider will do blood tests before starting and during treatmentwith YERVOY.If you miss any appointments, call your healthcare provider as soon as possible toreschedule your appointment.
See “What is the most important information I should know aboutYERVOY?”Severe infusion-related reactions. Tell your healthcare provider or nurse rightaway if you get these symptoms during an infusion of YERVOY:
chills or shakingitching or rashflushingshortness of breath orwheezing
dizzinessfeel like passing outfeverback or neck pain
Complications, including graft-versus-host disease (GVHD), in peoplewho have received a bone marrow (stem cell) transplant that usesdonor stem cells (allogeneic). These complications can be severe and can leadto death. These complications may happen if you underwent transplantation either
The most common side effects of YERVOY when used alone include:
••••••
•••••
The most common side effects of YERVOY when used in combination with nivolumabinclude:
•••••••••
••••••
••
The most common side effects of YERVOY when used in combination with nivolumaband chemotherapy include:
••••
••••
These are not all of the possible side effects of YERVOY.Call your doctor for medical advice about side effects. You may report side effects toFDA at 1-800-FDA-1088.General information about the safe and effective use of YERVOY.Medicines are sometimes prescribed for purposes other than those listed in aMedication Guide. If you would like more information about YERVOY, talk with yourhealthcare provider. You can ask your healthcare provider or pharmacist for informationabout YERVOY that is written for healthcare professionals.What are the ingredients of YERVOY?Active ingredient: ipilimumabInactive ingredients: diethylene triamine pentaacetic acid (DTPA), mannitol,polysorbate 80, sodium chloride, tris hydrochloride, and Water for InjectionManufactured by: Bristol-Myers Squibb Company, Princeton, NJ 08543 USAFor more information, call 1-800-321-1335U.S. License No. 1713[print code]YERVOY and OPDIVO are trademarks of Bristol-Myers Squibb Company. All other
before or after being treated with YERVOY. Your healthcare provider will monitoryou for these complications.
feeling tireddiarrheanauseaitchingrashvomiting
headacheweight lossfeverdecreased appetitedifficulty falling or staying asleep
feeling tireddiarrhearashitchingnauseapain in muscles, bones, and jointsfevercoughdecreased appetite
vomitingstomach-area (abdominal) painshortness of breathupper respiratory tract infectionheadachelow thyroid hormone levels(hypothyroidism)decreased weightdizziness
feeling tiredpain in muscles, bones, and jointsnauseadiarrhea
rashdecreased appetiteconstipationitching
® ®
trademarks are the property of their respective owners.
This Medication Guide has been approved by the U.S. Food and Drug Administration.Revised: May 2021
YERVOY 50 mg/10 mL Representative PackagingSee How Supplied section for a complete list of available packages of YERVOY.NDC 0003-2327-11Rx onlyYERVOY (ipilimumab)Injection50 mg/10 mL(5 mg/mL)For Intravenous Infusion OnlySingle-use vial; Discard unused portionDISPENSE ENCLOSED MEDICATION GUIDE TO EACH PATIENTBristol-Myers Squibb
YERVOY 200 mg/40 mL Representative Packaging
®
NDC 0003-2328-22Rx onlyYERVOY (ipilimumab)Injection200 mg/40 mL(5 mg/mL)For Intravenous Infusion OnlySingle-use vial; Discard unused portion DISPENSE ENCLOSED MEDICATION GUIDE TO EACH PATIENTBristol-Myers Squibb
YERVOY ipilimumab injection
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0003-2327
Route of Administration INTRAVENOUS
Active Ingredient/Active Moiety
®

Ingredient Name Basis of Strength StrengthIPILIMUMAB (UNII: 6T8C155666) (IPILIMUMAB - UNII:6T8C155666) IPILIMUMAB 5 mg in 1 mL
Inactive IngredientsIngredient Name Strength
TROMETHAMINE HYDROCHLORIDE (UNII: 383V75M34E) 3.15 mg in 1 mLSODIUM CHLORIDE (UNII: 451W47IQ8X) 5.85 mg in 1 mLMANNITOL (UNII: 3OWL53L36A) 10 mg in 1 mLPENTETIC ACID (UNII: 7A314HQM0I) 0.04 mg in 1 mLPOLYSORBATE 80 (UNII: 6OZP39ZG8H) 0.1 mg in 1 mLWATER (UNII: 059QF0KO0R)
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:0003-
2327-11 1 in 1 CARTON 03/25/2011
1 10 mL in 1 VIAL, SINGLE-USE; Type 0: Not aCombination Product
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
BLA BLA125377 03/25/2011
YERVOY ipilimumab injection
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:0003-2328
Route of Administration INTRAVENOUS
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
IPILIMUMAB (UNII: 6T8C155666) (IPILIMUMAB - UNII:6T8C155666) IPILIMUMAB 5 mg in 1 mL
Inactive IngredientsIngredient Name Strength
TROMETHAMINE HYDROCHLORIDE (UNII: 383V75M34E) 3.15 mg in 1 mLSODIUM CHLORIDE (UNII: 451W47IQ8X) 5.85 mg in 1 mLMANNITOL (UNII: 3OWL53L36A) 10 mg in 1 mL

E.R. Squibb & Sons, L.L.C.
PENTETIC ACID (UNII: 7A314HQM0I) 0.04 mg in 1 mLPOLYSORBATE 80 (UNII: 6OZP39ZG8H) 0.1 mg in 1 mLWATER (UNII: 059QF0KO0R)
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:0003-
2328-22 1 in 1 CARTON 03/25/2011
1 40 mL in 1 VIAL, SINGLE-USE; Type 0: Not aCombination Product
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
BLA BLA125377 03/25/2011
Labeler - E.R. Squibb & Sons, L.L.C. (011550092)
Revised: 5/2021
Related Documents











