Equity on the Path to UHC Deliberate Decisions for Fair Financing Background Report (Conference Version) Greater Equity for Better Health and Financial Protection Washington, D.C. • April 19–20, 2018

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Equity on the Path to UHCDeliberate Decisions for Fair Financing
Background Report (Conference Version)
Greater Equity for Better Health and Financial ProtectionWashington, D.C. • April 19–20, 2018

DRAFT:Notforattribution
1

DRAFT:Notforattribution
2
Thisisaforumpaper(conferenceversion)tothe“ThirdAnnualUHCFinancingForum:GreaterEquityforBetterHealthandFinancialProtection”.Thispapersetsthestageforthe
presentationsanddiscussionsattheForumandwaspreparedundertheguidanceoftheForumTechnicalWorkingGroup.Theinformationprovidedinthisdocumentdoesnotnecessarily
representtheviewsorpositionoftheorganizationsrepresentedontheTechnicalWorkingGroup

DRAFT:Notforattribution
3

DRAFT:Notforattribution
4
Section1:Introduction
In2016,theWorldBankGroupandUSAIDestablishedtheAnnualUHCFinancingForum,whichtakes
placeattheWorldBankGroup/IMPSpringMeetings.Thesemeetingsarestrategicplatformswhere
thousandsoffinanceanddevelopmentleadersfrommembercountriesdiscuss,analyzeanddebate
goalsforendingextremepovertyandboostingsharedprosperity.
TheUHCFinancingForumisembeddedintheselargerdiscussionstodivedeeplyintotheprocessesfor
acceleratingcountryprogresstowardsustainablefinancingofUniversalHealthCoverage—whichis
integraltoreachingtheSpringMeetings’largergoals.
Thisyearmarksthethirdtimeinwhichover400policymakersandotherexpertshaveconvenedto
analyzeandcriticallydiscussthehealthfinancingrealitiesthatcountriesface.Inoneoftheonlyglobal
spacesforthesenecessarydiscussions,participantsusetheforumtohelpshapeacollectiveagendafor
tacklingkeyfinancingchallengesposedbysomeofthetrickiestproblems.
TheThirdAnnualUHCFinancingForumexaminesequityforbetterhealthandfinancialprotection.It
complementsandbuildsonthetopicsandpapersofthe1stand2
ndforum,whichfocusedonhowto
generaterevenuestomeetfinancingneedsforqualityhealthservicesandfinancialprotection,andhow
touseavailableresourcesinthemostefficientway.
Eachyearourdebatesareinformedbyabackgroundreportthatexamineswhatworksanddoesn’t
work,whiletakingstockofwhatiscontroversial,innovative,ofhighimpactorinneedofclarity.
Thisyear,wetakeadifferentapproachbyaskingpolicymakerstoconsiderequitymoredeliberatelyin
theirhealthfinancingchoices.Whenpolicy-makersaimtoredressinequitiesinfinancingoutcomes,
theycandrawuponawell-establishedbodyofliteraturethatevaluatesandoffersguidanceonhowbest
toapproachpolicychoices.Butwhenpolicy-makerspursuestrategiestoaccelerateprogresstoward
UHC,theyseematalosstofullyconsidertheequityimplicationsoftheirfinancingdecisions.Oratleast
thatiswhattoday’sdeepinequitiesinhealthfinancingsuggest.Wethinkthat,perhaps,equityasa
criterionfordecision-makingisfallingthroughthecracks.
Placingtheblameonpolicymakerswouldmissthemark.ThemainproblemisthatprogresstoUHC
doesnotnecessarilyleadtoimprovementsforallandtheworse-off.This,wethink,isbecausepolicy-makersgrapplewithhowbesttoreachtheequitableendpointofUHCwhilealsoworkingonhigher
priorityobjectives,likeimprovingefficiency,overallpopulationhealth,employmentoreconomic
growth.Littleguidanceisavailabletohelpmanagedifficulttrade-offsbetweencompetingneeds.
Thispaperandthisyear’sforumaimtoclosesomeoftheinformationandguidancegaps,andfacilitate
thechangesnecessarytomoveequityconsiderationstotheforefrontofhealthfinancingpolicy
development.Weseethisasathree-prongedprocesswithafocusoni)identifyingpolicydecisionsthat
aredeemed“unacceptable”;ii)establishingwhatwecall“fairnessofprocess”indecision-making;and
iii)monitoringtheoutcomestohelpidentifywherepoliciesneedtobeadjustedforequity.
Theproposedframeworkbuildsonalargebodyofworkthathasexploredthemeaningofequityand
fairnessinhealthfinancingandfiscalpolicy.(e.g.,Wagstaff&VanDoorslaer2000;Murrayetal.2003;
Xuetal.2007;O’Donnelletal.2008;VanDoorslaer&O’Donnell2011;Bastagli,Coady&Gupta2012;
Ottersen&Norheim2014;Clements,Gaspar&Gupta2015;Mulenga&Ataguba2017;Fleurbaey&

DRAFT:Notforattribution
5
Maniquet2017;Wooetal.2017;Evanetal,2001).Morerecently,thisworkhasbeenappliedtoUHC
(WHO2014).However,noconsensushasdefinedtheboundariesandcontentoftheterms“equity”and
“fairness”andwhetherandhowtheyaredifferent.So,followingontheWHOConsultativeGroupon
MakingFairChoicesonthePathtoUHC,weusethetermsinterchangeablyinthispaper.(WHO2014).
Thescopeofourframeworkisbrokendownintothefollowingsections.
InSection2,wedescribethechallengesthatcountriesfaceastheyprogresstowardsUHCwhilealsostrugglingwithvastinequitiesinservicecoverageandfinancialprotection.
Section3mapsoutwhyhealthfinancingandtheoutcomestheyproducematter,andhowandwhy
policiesthatmakeUHCagoal—evenifit’sfarfromareality—areworthwhile.
Section4isreallythemeatofthisreport.Itidentifiesunacceptablepolicychoices,mapsout
approachestoestablishfairprocesses,anddiscussesthevalueofandneedformonitoring.
Section5outlineswhatcountriescandotofundamentallychangethewaytheyincorporateequity
concernsintotheirhealthfinancingpoliciesandstrategies.
Section2:SettingtheStageforUHC
In1978,theAlmaAtaDeclarationarticulatedanambitiousextensiontotheWorldHealthOrganization’s
constitutionbydeclaringprimaryhealthcareasabasichumanright.InwhatisnowKazakhstan,world
leaderssignedontonewoperatingprinciples,declaringthatallpeoplehadarighttopersonalhealth
andpublichealth,withaccesstotraineddoctors,nurses,midwivesandtraditionalhealers,andto
sanitation,cleanwater,essentialdrugs,immunizationsandmore.Andtheyproclaimedthatthese
servicesmustbeavailable“ascloseaspossibletowherepeopleliveandwork.”
Signatoriesgavethemselvesuntiltheyear2000—22years—andimploredactiononthepromisethat
healthforallwouldalloweveryonetoleadsociallyandeconomicallyproductivelives.
Now,40yearslater,wenotonlymissedthemark,butwemisseditbyawidemargin.Thegoodnewsis
thatthefastestprogresseverinextendinghealthservicecoverageoccurredduringtheeraofthe
MillenniumDevelopmentGoals.Thebadnewsisthat,atthecloseoftheMDGin2015,onlyabouthalf
theworld’spopulationenjoyedthebasicbenefitsenvisionedforallinAlmaAta.
ThenewtargetdateoutlinedbytheSustainableDevelopmentGoalsandtheWHOConsultativeGroupis
toreachUniversalHealthCoverage—withaccesstoservicesaccordingtoneedandwithoutfinancialhardship—by2030.Ifwearetotakethisseriously,countriesneedtobeontherightpathandstay
there.
Wehave12yearstodoalotofwork.Oneofthebiggesthurdlesisreplacingout-of-pocketpayments,
whichlimitaccessibility,withotherformsofhealthfinancing.Onlymodestprogresshasbeenmadein
reducingthesepayments,andnocleartrendshowstheiroverallburdenislightening.Tothecontrary,
everyyearapproximately100millionpeoplefallintopovertybecauseofout-of-pocketpayments.
Thetragedyisthatwehavefailed,eventhoughthemeansexisttomakehugeleapstowardUHCby
2030,andeliminatethepaymentconditionsthatknockthese100millionpeopleannuallyintopoverty.

DRAFT:Notforattribution
6
Multipleglobalestimatesshowthatthecostofapackageofessentialhealthservicesshouldrunno
morethan$90perpersonperyear.Globaldomesticpublicspendingstoodat$3.9trillionin2015,
enoughtofinancetheseessentialpackagesformorethan40billionpeople,oroversixtimestheworld’scurrentpopulation.
Theproblemiswehavevastlyinequitableinvestmentsinhealthfinancing,coverageandaccessto
services.Inthewealthiest5percentofcountrieswiththehighestpublicinvestmentsinhealth,the
averagespentonhealthperpersonis$4,600.Andforthetop10percentofcountriestheaverageis
$4,100perperson.
Butinthepoorest5percentofcountries,theaveragespentperpersononhealthisjust$4.Andforthe
bottom10percent,theaverageis$5perperson.Evenwhenadjustingforcostofliving,thedisparitiesin
healthinvestmentsarestunning.
Thebiggestchallengenowistofigureouthowtoboosthealthfinancingacrosslow-andmiddle-income
countriesinwaysthatmakehealthcoverageapriorityandareconsistentwiththegoalsofUHC.
Thisreport,andthisyear’shealth-financingforum,asksallparticipantstoseethispointintimeas
pivotal—asamomentoftruth.Ifcountriescontinueattheslowrateofprogressthatwesawinthelast
40years,wewillfailtoevencomeclosetoourgoalsby2030.
CountriesmustaccelerateprogresstowardsUHCbysystematicallytacklingfundamentalshortcomings
inhealthfinancing.Thisreportandthisyear’sforumhoneinonprovenandleadingedgeapproaches,
whichincludegivingprioritytotheworse-off(thesickestandthepoorest);reducingandultimately
eliminatinginequalitiesinhealthinvestmentsacrosscountriesandwithincountries;protectingpeople
fromfinancialruinlinkedtoOOPsbyphasingoutOOPsasameansforhealthfinancing;increasing
prepaidandpooledfinancing;andincrementallyincreasingguaranteedpackagessothatcoverageof
services,andtheirquality,improveforeveryoneovertime.
CountriesmustmakefasterprogresstowardUHC.Theinequitiesthatweseeglobally,however,exist
alsowithincountries.Ascountriesaccelerateprogress,theyruntheriskofdeepeningtheseinequities.
Figure1:Incidenceandinequalityinskilledbirtha7endance,Threshold:10%oftotalconsump6on(n=120countries)Inequali)es,
Concentra6onindex
SOURCE:HEFPI2018Database
Notes:Basedonlatestavailablesurveyyear;circlesizeispropor)onaltototalpopula)on
Popula)onincidence,%30 40 60 80 10050 70 900 10 20
0.3
0.2
0.0
-0.1
-0.2
0.1
0.4

DRAFT:Notforattribution
7
Onthebenefits,side,thenatureofthegameisthatthehigherthecoverage,thelowertheinequities.
Likewise,thehighertheaveragecoverage,thelessthevariation.Forexample,lookingatSkilledBirth
Attendance(SBA),aservicecommonlyincludedinessentialservicepackages,countrieswithservice
coverageabove80percent,haveconcentrationindiceslowerthan0.1.Incontrast,countrieswith
averageinservicecoveragebetween30and50percent,haveconcentrationsindicesbetween0.1(e.g.,
Indonesia)tocloseto0.5(e.g.,Nigeria).Theconcentrationindexmeasuresinequalitiesbysocio-
economicstatus(SES).Theindexrangesfrom-1to1,withzeromeaningnoinequalitiesincoverage
acrossincomegroupsinthiscase,andinequalitiesincreasingastheindexapproaches1.Byconvention,
pro-richinequalitieshavepositiveindices,whilepro-poorinequalitiesshownegativeindices.
Whiletheconcentrationindexisanabstractconcept,theillustrationofcoveragebyincomequintile
providesabettersenseofthedepthoftheinequalities.Forexample,theconcentrationindexof0.47
forNigeriameansthatSBAcoveragewas87.5percentinthehighestincomequintile,butonly6.7
percentforthelowestincomequintile.
Figure2:Incidenceofskilledbirtha7endance:Nigeria(2014),%
6.7
18.8
41.6
64.1
87.5
0102030405060708090
Q1 Q2 Q4Q3 Q5
SOURCE:HEFPI2018Database
Incidence,%
Figure3:Incidenceandinequalityincatastrophicpayments,Threshold:10%oftotalconsump6on(n=136countries)
SOURCE:HEFPI2018DatabaseNotes:Basedonlatestavailablesurveyyear;circlesizeispropor)onaltototalpopula)on,n
Inequali)es,Concentra6onindex
0.6
0.4
0.0
-0.2
-0.4
Popula)onincidence,%5 10 20 30 4015 25 350
0.2

DRAFT:Notforattribution
8
Source:Urquieta-SalomonandVillarreal,2016
Ontheburdenside,thepictureislessclear.Dataareonlyavailableforasmallersetofcountries.
Multiplemeasuresoffinancialprotectionexist,producingdifferentpatterns.Moreover,patternsneed
tobecarefullyinterpretedagainstinformationonservicecoverage.Forexample,adeclineinservice
coveragemayresultinreductionsofOOPexpendituressotheindicesoffinancialprotectionmightseem
toimprove.Nevertheless,weseedeepinequalitiesinmanycountries.Forthepurposeofillustration,
weusecata10consumption.Inmostcountries,inequalitiestendtobeoverwhelminglyconcentrated
amongthepoor.
Likeonthebenefitsside,theillustrationoftheincidenceoffinancialcatastrophe(inthiscasemeasured
asout-of-pockethealthexpendituresexceeding10%oftotalexpenditures,calledcata-10)byincome
quintileprovidesabetterillustrationofthedepthoftheinequalities.
Forexample,theconcentrationindexof37.39forIndiameansthattheincidenceofcata10wasin15
percenthigheramongthelowestincomequintilecomparedtothehighestquintile.
InequalitiesinUHCoutcomesoftenreflectdifferencesinthelevelofinvestmentorotherhealth
financingoutcomesandfunctions.Forexample,attheturnofthecentury,servicecoveragevariedin
Mexicosignificantlybetweenpeoplewithandwithoutsocialhealthinsurance.
Table1:Coverageofeffectiveaccesstopreventivehealthinterventions
Uninsured Insured
Skilledbirthattendance 88.91% 94.78%
Basicvaccinationschedule 71.39% 73.18%
Adultsover20withhighbloodpressure
control
47.73% 67.72%
Figure4:Incidenceandinequalityincatastrophicpayments:RepublicofKorea(2011)Threshold:10%oftotalconsump6on
37.4
17.212.8
8.25.7
0
10
20
30
40 Q1 Q2 Q4Q3 Q5
SOURCE:HEFPI2018Database
Incidence,%

DRAFT:Notforattribution
9
Whilecoverageforessentialservicessuchasmaternalandchildhealthwashighindependentof
affiliation,starkdifferencesprevailedinthecoverageofservicesfornon-communicablediseases(table
1).Effectivecoveragewithhighbloodpressurecontrolwas20percentagepointshigheramongthe
insured.
Similarly,thelikelihoodofthosewithsocialhealthinsurancetosufferfromcatastrophichealth
expenditures(frominpatientvisits)overayearwasfourtimeslower(Knauletal,2006).These
differencesinUHCoutcomescorrespondedtothelevelsofgovernmentfinancialcontributions.For
peoplewithsocialhealthinsurance,itwasfivetosixtimeshighercomparedtothecontributionsfor
governmenthealthservicesusedbytheuninsured.
Section3:TheGoal
ThedefinitionofUHCholdsthatallpeopleshouldreceivepromotive,preventive,curative,rehabilitative
andpalliativehealthservicescovered,basedonhealthneeds.Thoseservicesshouldbeofsufficient
qualitytobeeffective,whilealsoensuringthatpeopleareprotectedfromfinancialhardshipswhen
usingtheservices(WHO2010).
ThegoalofUHCexpandsontheconceptofqualityhealthcareforallasabasichumanright,asoutlined
intheWHOconstitution,theAlmaAtaDeclarationonHealthforAllandanumberofhumanright’s
treaties,addingprotectionfromfinancialhardship.
ThefirstcriticalpartofUHCisaboutbenefits,ensuringpeoplearecoveredbasedonneed.Healthy
people—thebetter-off—needlessservicesfromthesystem.Andunhealthypeople—theworse-off—
needmorefromthesystem.Thespectrumofneedshoulddeterminethebenefits,settingupservicesto
berenderedinanunequal,butequitableway.Thiswecallverticalequity;thehighertheneedthe
greaterthebenefits.Butcoverageshouldalsotreatallpeoplewiththesamehealthneedsequally,so
thateveryonewithkidneyfailureinneedofhemodialysisreceivesit(iftheywant).Thiswecall
horizontalequity;acrossanygivenneed,everyoneiscovered.
Butwithinhorizontalequityistheaddeddimensionofqualityoreffectivenessoftheavailableservices.
Theeffectivenessofthoseservicesisequallyasimportant.Thatis,servicecoverageandquality
combinedresultineffectivecoverage,orthecapacitytoachievethedesiredresults.
ThesecondpartofUHCisaboutfinancialburdens,ensuringpeopleareprotectedfromseverefinancial
hardshipwhenpayingout-of-pocketforhealthservices.Thesekindsofhardshipshavetwowidely-
accepteddefinitions:out-of-pocketpayments(OOPs)thatpushpeopleintopovertyordeeperinto
poverty,andOOPsthatarenotimpoverishingbutnonethelessprovecatastrophicforthehousehold
becausetheyleadtoexcessiveborrowingorassetdepletion,orcuttingbackonessentialneedslike
education,clothing,housingandfood.UHCisclearthatnooneshouldsufferthesekindsoffinancial
hardshipsfromOOPs.
Equity in UHC outcomes matter
UHCisimportanttoimprovinghealthandreducingpoverty.Weseethiswherepeoplelackaccessto
healthservices.Theyoftentakelongertorecoverfromanillnessorinjury,orneverrecover,leadingto
lossofincome.Incountrieswithsocialsafetynets,thiscanendupcostingmoreinservicesthanthe

DRAFT:Notforattribution
10
originaltreatmentwouldhavecost(thepenny-wise,pound-foolishproblem).Wherenosocialsafety
netsexist,healthcostsareknowntotumblefamiliesintopovertyandholdthemthere.Forexample,the
compoundingeffectsofpovertyforcefamiliestoforegothecostofeducation,eitherbecausetheyhave
nomoneyforthefeesortheyneedtheirchildrentostayhomeandhelpearnincome.Wherethesick
areexpectedtopayforhealthservices,familiesmayendupborrowing,incurringdebtthatcanget
passeddownfromgenerationtogeneration.
Werecognizethatsocialdeterminantsalsoplayanimportantroleinhealth.Thatis,peoplewithperfect
healthcoverageataffordablecostswholiveinacommunitywithgunviolencearestillsusceptibleto
beingshot.Butwherethetwomeet,iswhereUHCmakeshealthcoveragereliableandaffordable.
Peoplehavemoremoneytopayforotherthings,likebettereducation,nutritionandlivingconditions
(tomoveawayfromthegunviolence).Andthatcanimprovehealthoutcomesandhelpliftpeoplefrom
poverty,oratleastnotexacerbateit.
WeseeUHCasleadingtooutcomesthatreachbeyondthepopulation’soverallphysicalhealth,because
theyplayaroleinreducingfinancialstresses.Theexplicitpovertyaversionaspectofthisholdsthe
potentialofpositivelyripplingout.Thatis,inadditiontogroundinghealthsystemsintheidealthat
healthisahumanright—asmuchasdecentlivingconditionsare—equitablefinancingthatprotects
peoplefromeconomichardshipensuresthatthehealthsectorplaysnopartinincreasingpoverty.
Wealsoseethatreducinginequalitiesinhealthoutcomeshelpsreduceincomeinequalities.Andbetter
healthtranslatesintohigherincome.Thisistrueofhealthservicesandsocialdeterminantsofhealth.So
wehavetwostrands.Financialprotectionimprovesincomeinequality,andhealthoutcomesreduce
incomeinequalitywhenoutcomesimprovethehealthofthepoor.Weknowreducedincomeinequality
promotesgrowth,andthatincomeinequalityhasa“negativeandstatisticallysignificantimpacton
subsequentgrowth.”(Cinganro,F.,2014)
Importantlessonscanalsobelearnedfromseveralhigh-incomecountriesthattodayfacegrowing
inequitiesinhealthoutcomesandincreasingratesofpoverty,andthathavecorrespondingerosionof
socialcohesion,advancedpoliticalpolarization,andslowereconomicgrowth.(IMFFiscalMonitor,
October2017)Closingthesegapsshouldbethegoalofallcountries,andhealth-financingchoicescan
help.
Dramaticglobalhealthsecuritylessonsalsocanbelearnedfromlower-incomecountriesthathavebeen
unableorunwillingtoworkequitablytowardUHC,orotherwisestrengthentheirentirehealthsystems.
Intheseplaces,infectiousdiseasesspreadmorerapidlyinareaswithweakcorepublichealthfunctions,
sometimesindramaticwaysthatputimmensefinancialandpoliticalstressontheentireglobalhealth
system.The2014EbolaoutbreakinWestAfricaservesasoneofthemostrecentacuteexamples.We
canbegintohead-offthesekindsofoutbreaksbybringingequitytohealthfinancingsothathealth
systemsare,attheveryleast,abletodeliverbasicdiagnosticanddiseasesurveillancetoolseverywhere.
Journeying to UHC
AchievingUHCisthegoal.Butnocountryisallthewaythere,withcompletecoverageofhighquality
servicesthatareaccessibleandaffordableforall.Somewealthycountriescomeclosewithrelatively

DRAFT:Notforattribution
11
largeguaranteedcoveragepackagesthatincludeabroadrangeofhealthservicesavailableforloworno
out-of-pocketpayments.
Formanycountries,however,UHCisinthedistantfuture.Toofewcanaffordthesuiteofhealth
interventionsthatareknowntoprolongandimprovelife,whilealsoensuringfinancialprotectionforall
users.ThegoalforthemistoseeUHCasajourney,tostartwithatleastasmallerguaranteedpackage
withabaselineofessentialservicesthatareavailabletoall,ofequalqualityforallandaffordable.Then,
overtime,thesizeandscopeofthepackagesshouldexpand—allthewhilekeepingasagoal
improvementsinequitability,availabilityandaffordabilityofservices.Bystartingoutsmall,these
countriesarestrategicallyandtacticallysetuptocontinuethejourneytoUHC.
Signposts show the way
CountriesthathavesetUHCasatargetandmadetheobligationtoprogressivelystayonthejourney,
however,areunabletolooktotheUHCgoalsforguidanceonmakingpolicychoicestohelpkeepthem
oncourse.Indeed,assomecountriesmadeprogressonservicecoverageoverall,inequitieswidened.
Andduringtimesofcrisis,servicecoveragedroppedandfailedtoprotectthepoor.
SoUHCshowstheobjectiveofthejourney,nothowtogetthere.Weattempttofillsomeofthosegaps
inguidancebyofferingpolicy-makerswhatwecallsignposts.Theyaredesignedtoprovidenecessary
directionsforstayingoncourse.
Onthebenefitsside,UHCrequiresdistributionofhealthservicesaccordingtoneed.Ontheburden
side,financingsystemsthereforecannotputupfinancialbarriertoaccessthebenefits.Andthatis
wherehealthfinancingofUHCextendsbeyondfinancialprotectiontoprovidingservicesregardlessof
theabilitytopay.Sothesetwocomponentshavetobeseparated.
Wecallitdecoupling.Policy-makersforUHCmustdevelopauniversalguaranteedcoveragepackage
accordingtotheircountry’sfinancingcapacities.Whatisincludedinthepackagewillbebasedon
Inequali)es,Concentra6onindex
Figure5:Servicecoveragevs.inequality,Concentra6onindex(-1=skewtopoorto1=skewtorich)
0.3
0.2
0.1
0.0
-0.1 30 40 50 60 70
Servicecoverage,%
SOURCE:WorldBankHEFPI2017

DRAFT:Notforattribution
12
whatevercountryfinancingwillallow,startingwithacoresetofhealthservicesandexpandingitover
time.
Onaseparatetrackpolicy-makersmustraisethefinancing.Butthismustbedoneinawaythatremoves
thefinancialburdenforpeoplewhoareunabletopay.Theonlywaytodothisisthroughprepaidand
pooledfinancing.Inpractice,thismeanspublicfinancing--taxesandcontributionstosocialhealth
insurance.Tosubsidizethepoor,andthosewithlargehealthneeds,publicfundsshouldingeneralbe
raisedbasedontheabilitytopaywithsomedegreeofprogressivity,thatis,therichercontributea
highershareoftheirincome.
Socountriesestablishaguaranteedpackagewithhealthservicesthatareavailabletoallatan
affordableprice(UHC).Whoutilizestheservicesisseparatedfromwhopaysforthem.Utilizationis
basedonhealthserviceneed.Payingintoprepaidandpooledsystemsisbasedontheabilitytopaywith
OOPsminimized.
ThisprovidestwoguidepostswhendevelopingpoliciestowardUHC:healthservicesaccordingtoneed
andcontributionstoprepaidandpooledfinancingbasedonabilitytopay.Twotrackswithseparate
directionsforstayingonthepathtoUHC.
OnthejourneytoUHCcomefurtherconsiderationswithinthesetracks.Thereisbroadconsensusthat
someprioritymustbegiventotheworse-off.Onthebenefitsside,thismeansgivingprioritytothe
sickestandthosewiththelowestservicecoverage;ontheburdenside,thismeansgivingprioritytothe
poor.1Inthisway,UHCdirectspolicy-makerstopayspecialattentiontothemostdisadvantaged
segmentsoftheirpopulations,andmakedecisionsdesignedtoreachthem.
Incountrieswithlittlepotentialforraisingenoughprepaid,pooledfundstocoverabroadsuiteof
healthservices,effortshavefocusedonidentifyingpackagesofsufficientserviceswithguaranteed
accessandfinancialprotectionwithinthelimitationsofavailablepublicfinancingandservicedelivery
capacities.ThesepackagesconstitutethestartingpointfortheprogressiverealizationofUHC.Decision-
makersthenfacethechallengeofdefiningwhatis“sufficient”inabasicpackage,andwhatshouldbe
addedasthepackageexpandsovertime.
ThechallengescountriesfacestayingonthepathtoUHCaremany.Thefollowingarefourinterrelated
butdistinguishablechoicesthatmakepolicydecisionsdifficult.
First,theprinciplesofbenefitsandburdenarenotabsolute.Forinstance,withrespecttobenefits,
shouldcountriesgiveprioritytoexpandingtherangeofservicesavailabletoall,basedonneed,or
shouldtheyfocusonimprovingthequalityofexistingservices?Likewise,ontheburdenside,shouldthe
principleofabilitytopaybeinterpretedastherichpaymorethanthepoororthattherichpayahigher
proportionoftheirincomesthanthepoor?Eveniffaircontributionsareunderstoodasthelatter,i.e.
progressivecontributionswheretherichpayahigherproportionoftheirincome,policymakersmust
stilldeterminehowmuchmoretherichshouldpay.
1
Oneformalizationofthisapproachisinherentintheidealsofprogressiveuniversalism,whichdictatethatateverystageon
thepathtoUHC,topoor—whoasagroupareinthemostneedofhealthservicesandfinancialprotection—shouldbenefitat
leastasmuchastherich.

DRAFT:Notforattribution
13
Second,decisionsoftenpitbenefitsagainstburden.Often,decision-makershavetodecidebetweenthe
twocompetinginterests:expandingandimprovinghealthservicesontheonehand,andextending
financialprotectionontheother.Shouldcountriesprioritizetheexpansionofeffectiveservicesfor
thosewiththegreatesthealth-serviceneeds,ortheextensionoffinancialprotectiontothosewiththe
leastabilitytopay?Moreover,ifcountriesdecidetofocusonamixofhealthserviceexpansionand
financialprotection,howmuchweightshouldbegiventoeachcomponent?And,ofcourse,theyhaveto
figureouthowtopayforeverything—whichcirclesbacktothefirstdifficulty.
Third,prioritizingtheworse-offrequiresdata,whicharescarce.Whilemanycountriesaresettingup
systemstoidentifytheworseoff,lackofsufficientsurveydatahasmadeidentifyingthosewithgreater
healthcoverageneedsandlowestactualcoveragedifficult.Oneansweristofocusfirstonuniversal
coveragetocastawidenetthatcoversabasicsetofservicesthatreacheveryone,includingtheworse-
offandpoorestpeople.Thisensuresthatthepoorgainatleastasmuchasthebetter-offduringservice
coverageexpansions,onthewaytoUHC.
Thefourthdifficultyweseeis,perhaps,thetrickiest.Thisiswhenpolice-makersmustdecidebetween
improvingequityinhealthfinancingandreachingothersocialgoals—suchasstimulatingeconomic
growthorraisingadditionalrevenuerapidly.Thisisthefocusofthenextsection.
Section4
ChartinganequitablepathforwardinfinancingUHCincludesthreepolicyanglesthatthispaperdefines
andofferssuggestionsfor.Thefirstisidentifyingunacceptablepolicychoicesthatshouldbeavoided.Thesecondisestablishingcriteriaforfairprocessesthatwillengagethepublicandkeeppolicydecisionsoncourse.Andthethirdismonitoringimpactsbyusingavailabledatatohelpinformpolicy
choicesandleadtoequitableoutcomes—notexacerbateexistinginequitiesorleadtonewones.
UnacceptablePolicyChoicesinFinancingUHC
Decisionsthatdeepeninequitiesinhealthfinancingneedtobeidentifiedandavoidedascountries
moverclosertoUHConaggregate.Broadlyspeaking,an“unacceptablepolicychoice”isonethatcreates
orexacerbatesanexistingunfairinequalityandcannotbejustifiedbytrade-offsagainstotherpolicy
objectives.Herewearetalkingaboutincrementalpolicychoiceswithinthethreehealthfinancing
functions:revenuegeneration,poolingandpurchasing.
WearrivedattheseunacceptablepolicychoicesbybuildingonthelogicoftheWHOConsultativeGroup
onEquityandUniversalHealthCoverage,whichfocusedonfairchoicesintheprioritizationofservicesin
theprogressiverealizationofUHC.Here,welookmorebroadlyatfinancingUHC.
WhileexaminingoptionsforimprovingUHCoutcomes(everyonegetsthehealthservicestheyneed,of
goodquality,andwithfinancialprotection),weidentifiedpotentialinequalitiesamongindividualsand
groups(differingbyincome,gender,geographicregion,ethnicorigin,affiliationwithpooling
arrangements,legalstatusofresidency,andhealthordiseaserelatedproblem).Wethendrilleddown
tounderstandtheinequalitiesacrossthethreehealthfinancingfunctionsthatcontributetoinequalities
inhealthoutcomes.

DRAFT:Notforattribution
14
Fromthereweestablishedprinciplesoffairnessinthedistributionofbenefitsandburdens,basedon
thevaluesinherentinUHCandthemorewidelyacceptedprinciplesoffairnessandequity.Wethen
scrutinizedtheinequalitiesinUHCoutcomesandthoserelatedtoeachhealthfinancingfunction;
measuredthoseinequalitiesagainsttheprinciplesoffairness;determinedwhethertheywere
inequitable(i.e.inequalitiesthatareinherentlyunfair);identifiedpolicychoiceslikelytodeepen
inequities,andconcludedthatsuchchoices—unlessjustifiedbytheneedtopursueotherpolicy
objectives—are“unacceptable”.
Thepolicychoicesthatwedeem“unacceptable”inallthreefinancingfunctions,basedontheapproachdescribedabove,meettwocriteria:
1) TheydeepeninequalitiesidentifiedasunfairintheUHCprinciplesforbenefitsandburden.
2) Theycannotbejustifiedbytheneedtopursueotherpolicyobjectives.Examplesinclude
stimulatingemployment,maximizingrevenues,controllinginflation,orstimulatingeconomic
growth.
Bothcriteriainvolvevaluejudgmentsthatreasonablepeoplecandebate.Whatwefocusonispolicy
decisionsthatincreaseinequity,butthatcannotbejustifiedbyotherpolicyobjectivesthatoffer
counterbalancingtrade-offs.
TenUnacceptableChoices
Thefollowingareten“unacceptable”choices,byhealthfinancingfunction(revenuegeneration,pooling
orpurchasing)outlinedintable1ofAnnex1
Thefirstthreeunacceptablechoicesrelatetorevenuegeneration,whichisdefinedasraisingfinancialresourcesneededtodevelopandrunahealthsystem.
Broadconsensusisthatguaranteedservicesmustbefinancedlargelywithcompulsoryprepaid
resourcesandnotout-of-pocketpayments.Thisprovidesbetterfinancialprotectionandpreventsthat
tumbling-into-povertyeffectthatOOPstoooftencause.Wearguethattheequitabilityofhowthese
prepaidfundsareraisedmattersonlytotheextentthatthechoicesaffectthefairnessoftheentire
publicfinancingsystem,includingbothcontributionsandexpenditures.Soweseehealthfinancingasa
partofpublicfinancing—fromindividualtaxrevenuestofirmsthatpaydedicatedtaxesordirectlyfund
employeehealthservices.Howrevenuesareraisedandspent,onthewhole,iswhatmattersmost.
UnacceptablechoiceNo.1:Raiseadditionalrevenuesforhealththatmakecontributionstothepublic
financingsystemlessprogressivewithoutcompensatorymeasuresthatensurethatthepost-tax,post-
transferdisposableincomedistributionisnotlessequal.

DRAFT:Notforattribution
15
Atfirstglance,thePhilippines’2012decisiontoraiseamajorityofrevenuesforthenationalinsurance
programthroughtaxesontobaccoandalcoholmighthavebeenseenasanunacceptedpolicydecision
becausesintaxesareknowntoberegressive.2However,thegovernmentusedaportionofthetaxesto
payhealthinsurancepremiumsforthebottom40percentofthepopulation(Kaiseretal,2016).From
2012to2014,theprogramexpandedhealthinsurancecoverageamongthepoorto14.71million
households,upfrom4.61million—a300percentincreaseinjusttwoyears.
Datahasyettobecomeavailabletoconfirmthattheexpansioncounter-balancedtheregressivityofthe
taxmeasure.Butresultsfromothercountriesthathavemadesimilarchoicesareencouraging.For
example,Indonesiareliesheavilyonregressivetaxestoraiserevenue,butthenetfiscalincidenceis
progressivethroughmostlyin-kindtransfersforhealthandeducationforthepoor(Jellemaetal,2017).
Thecountryhassinceseenadeclineinincomeinequities,asmeasuredbyadropintheGINIcoefficient
from0.394to0.370(whichmeasureschangesonscalefrom0to1,with0indicatingperfectequality
and1beingperfectinequality.
UnacceptablechoiceNo.2:Increaseout-of-pocketpaymentsforuniversallyguaranteedpersonalhealth
serviceswithoutanexemptionsystem3orcompensatingmechanisms.
Debatesoverout-of-pocketpaymentsariseintwocategoriesofcountries:thepoorestandthosein
crisissituations.Extremelypoorcountrieswithlimitedresourcesfacethemostdifficulttrade-offs.Their
limitedoptionsforraisingfinancescanhemthemintouserfees,iftheyseenootherpathtofinancing
government-sponsoredhealthservices.Doministriesofhealthrelyonuserfeesorletservicedelivery
falter(withnomedicinespurchasedtorestockshelves,nonewhealthworkerstofillshortages,andno
capitaltorepaircrumblinghealth-relatedinfrastructure)?Withlittleevidencethatexemptionsystems
work,mostlookforalternativefinancingmechanisms.
Eveninhigher-incomeOECDcountries,whenfacedwiththe2008financialcrisis,one-thirdofthem
(includingGreeceandIreland)introducedorincreaseduserfeestoshoreuphealthfinancingshortfalls.
Greeceoffersaparticularlyvividexampleofwhatcanhappenwithoutexemptionsforthepoor.There,
userfeeswereincreasedforoutpatientcare.Buteventhoughsomevulnerablegroupswereexempted
fromthecharges,unforced4unmetneedforhealthservicesincreasedfrom7.5percentto11.7percent
forthepoorestpeople(OECD,2015andEuropeanCommission,2013).
2Tobaccotaxesareregressiveintheburdenspacesincesmokingprevalenceisconsistentlyfoundtobehigher
amongthepoor,theycontributeadisproportionallyhigherproportionoftheirincomestothesetaxesthanthe
rich.Ontheotherhand,theimpactofthesetaxesisprogressiveinthebenefitsspace–thepoorgain
disproportionallymorethantherichintermsofsubsequenthealthbenefits(Summers,2018).
3
Giventhelimitedevidence-baseinsupportofsuchpolicies,proofthatthesesystemsandmechanismsiscritical4
Unforcedunmeetreferstotheproportionofpeoplewhoreportanunmetneedforhealthcareduetothree
reasons:(i)affordability,(ii)waitinglist,and(iii)distancetohealthfacility/nomeansoftransport

DRAFT:Notforattribution
16
UnacceptablechoiceNo.3:Raiseadditionalrevenuesforuniversallyguaranteedpersonalhealthservicesthroughvoluntary,prepaidandpooledfinancingarrangementsbasedlargelyonhealthstatus,
includingpre-existingconditionsandriskfactors.
Countrieswithnoorlimitedgovernment-sponsoredservicepackagesrelyonprivatehealthinsurance,
whichhavebeenknowntosetpremiumsbasedonvariablessuchasage,genderandpre-existinghealth
conditions.Thesepremiumschedulesmakeinsuranceunaffordableforthosewhoarepoorandsick.
Peopledon’tgetcareaccordingtoneed.Yet,somecountriesencouragesuchcoveragethroughtax
exemptions.
Thenextthreeunacceptablechoicesrelatetopoolingresources,whichmeansspreadingcontributions
acrossindividualsandgroupsinawaythatreducesthefinancialriskassociatedwithmedicalexpenses.
Healthsystemstendtobehighlyfragmentedintopoolsoffundsforhealthfinancingschemes,
administrativeterritorialunits,orhealthprograms.Healthfinancingschemesarethefinancing
arrangementsthroughwhichhealthservicesarepaidforandobtainedbypeople.Examplesinclude
nationalhealthservices,socialhealthinsuranceandvoluntaryinsurance,includingcommunity-based
healthinsurance.Administrativeterritorialunitswithinhealthfinancingschemesmayconstitute
separatepools,wherelowerlevelsofgovernmentareresponsibleforservicedeliveryandreceive
transfersfromhigherlevelsofgovernmentandsometimesalsoraiselocaltaxesandotherrevenues.
Financingsystemsmaybefurtherfragmentedintoprogramsthattargetcertainpopulationsand
diseases,withring-fencedfundinginlessdevelopedcountries,oftenco-financedfromDAH,whether
passingthroughgovernmentbudgetsoradministeredseparately.
Theproblemsweseearelargelyassociatedwithallocatingpublicmoniesinawaythatmakesexisting
inequitiesintheavailabilityoffundsperpersonacrosspoolsworse,thatis,inequalitiesinthe
availabilityoffundsunlesstheyarejustifiedbydifferentneeds.Inequities,though,mayalsoarisefrom
exclusionbecausepeopleareineligibleorfaceotherbarrierstotheirparticipationinpools.
UnacceptablechoiceNo.4:Changepercapitaallocationsoftaxrevenue5ordonorfundsacrossprepaidandpooledfinancingschemesinwaysthatexacerbateinequities,unlessjustifiedbydifferencesinneed
ortheavailabilityoffundsfromothersources.
Priorto2003,Mexicohadthreemajorfinancingschemes,twoofthemsocialhealthinsuranceschemes
paidforbyemployeeandemployercontributions.Andthethird,paidforthroughgeneralgovernment
revenues,servedtheuninsured.Thetwosocialhealthinsuranceschemesspentnearlyfivetosixtimes
morepercapitaonbeneficiariesthanthegovernment-fundedprogram.(WorldBank,2012).
5
Taxrevenueexcludessocialhealthinsurancecontributions

DRAFT:Notforattribution
17
Whenthetwoemployment-relatedschemesfacedshortfalls,theyreceivedbailoutmoneywithno
increasesinallocationtothethirdscheme.So,ineffect,thetwoplansservicingwealthierpeoplewith
broaderpackagesweregivenadditionalresourcesfromthesamepotofmoneythatunderfundedand
providedfewerservicestothegeneralpopulation.Theseallocationsdeepenedinequitiesandwerenot
justifiedbyanyotherpolicyobjectives.
MexicorectifiedtheentirefundinglevelsbylaunchingtheSocialProtectionSysteminHealth(SPSS),
widelyreferredtoasSeguroPopular.Thisprogramdirectsfederalandstatecontributionstoincrease
financingforthenationalhealthscheme,sothatthepercapitaspendingisnowmoreeven.
UnacceptablechoiceNo.5:Withinfinancingschemes,changepercapitaallocationsfromhigherto
loweradministrativelevelsinwaysthatexacerbateinequities,unlessjustifiedbydifferencesinneedor
theavailabilityoffundsfromothersources.
Infederalsystems,centralgovernmentstypicallytransferblockgrantstosubnationalentities.InNigeria,
thesizeoftheseblockgrantsislargelydeterminedbywhatiscalled“principleofequality,”whichmeans
allstatesreceiveanequalshareoftherevenues(WorldBank,forthcoming).Population,size,levelof
socialdevelopment,andfiscalcapacityplayonlyminorrolesindeterminingeachstate’sshare.6This
formulaforresourceallocationalsofailstoaccountforthelargevariationsinrevenuegeneratedbythe
states.7
Undertheassumptionthatallstatesgivethesameprioritytohealth,disparitiesinavailablerevenues
leadtosignificantinequalityinpercapitaallocationsforhealth.Moreover,poorerstateswithsmaller
overallbudgetsoftentendtogivelowerprioritytohealthdespitehigherneeds,furtherexacerbating
inequalities.
Toaddressthisproblem,thegovernmentproposedtheBasicHealthCareProvisionFund(BHCPF),which
seekstorectifythedifferencesbyofferingadditionalfinancingtostatesproportionaltotheir
populations.Thefundsarechanneleddirectlytofrontlineserviceswiththeaimtoexpandcoveragewith
theBasicMinimumPackageofHealthServices.
Thenextfourunacceptablechoicesrelatetopurchasing,whichisconcernedwithdecisionsmadeon
whatandhowtopayfor,includingservicesandinputs(coveringhumanresources,equipment,supplies
andinfrastructure).
Herewemakethreeprincipledistinctions.First,wedifferbetweenpersonalhealthservices(suchas
treatment,rehabilitation,palliationaswellaspreventionandpromotionatthepersonallevel)andnon-
6
Forinstance,populationestimatesonlyaccountfor25.6%oftheformula.7
StategeneratedrevenuesrangefromNRA1000percapitainNigerstatetoNRA25000percapitainLagos

DRAFT:Notforattribution
18
personalhealthservices(suchasessentialpublichealthfunctions,includingpopulation-based
preventionandpromotionaswellassystemgovernance).
Amongpersonalhealthservices,wedistinguishbetweenentitlementsandtheservicesthataredefacto
available.Ontheentitlementside,forexample,socialhealthinsuranceservicepackagestypically
guaranteefortheformalsectorabroaderrangeofservicesthanthoseguaranteedbygovernment
fundingorinsuranceschemesdesignedspecificallyfortheinformalsectororthepoor.Onthe
availabilityside,guaranteedhealthbenefitspackagesareinprincipleavailabletoeverypoolmember,
but,inreality,contractingandpaymentsystemsmaynotmaketheseservicesavailableforeveryone.
Finally,forservicesthatareactuallyavailable,wemustlookatkeyinputs(humanresources,medicines,
othersupplies,equipmentandinfrastructure)Thedefactoavailabilityofserviceshingesontheactual
availabilityoftheseinputs,whichoftendiffersinqualityandrangeacrossurbanandruralareas.
UnacceptablechoiceNo.6:Withinschemesorpools,changeallocationsoffundsacrossdiseasesin
waysthatexacerbateinequities,unlessjustifiedbydifferencesinneedortheavailabilityoffundsfrom
othersources.
Acommonexampleiswheregovernmentsincreasefundingforparticulardiseaseprogramsthatare
alreadywell-fundedthroughexternaldonorfinancing,perhapsaspartofcounterpartfunding
requirements,leavingotherdiseasesprogramsaddressingpriorityhealthproblemswithseverefunding
shortages.
UnacceptablechoiceNo.7:Introducehigh-cost,low-benefitinterventionstoauniversallyguaranteedservicepackagebeforeachievingclosetofullcoveragewithlow-cost,high-benefitservices.
Inmanycountries,publicsectorresourcesaredirectedtowardshospitalizationbenefitsbeforefull
coverageofbasichealthserviceisachieved.Forexample,in2008,IndialaunchedtheRashtriya
SwasthyaBimaYojana(RSBY)toprovideinsurancecoveragetohouseholdslivingbelowthepovertyline.
RSBYismeanttoaddressthehighincidenceofOOPsamongthepoor.Theschemeoffershospitalization
benefitswithcompletecoverageinbothprivateandpublichospitals,whichwouldpreviouslyhavebeen
inaccessibletothepoor.Theprogramhasenrolledover36millionhouseholdslivingunderthepoverty
line(RSBY,2018).
WhileRSBYsignificantlyimprovedfinancialprotectionfromhospitalizationamongthepoorest,itdidnot
addresstheneedforlow-costinterventionslikeprimaryandpreventivecare.Toaddressthisgap,the
governmentsimultaneouslyexpandedsignificantresourcesdirectedtowardstheNationalRuralHealth
Mission(NRHM)throughConditionalCashTransfers(CCTs)andcommunityhealthvolunteers.Andin
February2018,thegovernmentalsoannouncedtherolloutoftheNationalHealthProtectionScheme

DRAFT:Notforattribution
19
(NHPS),whichwillincludeinpatientandoutpatientcare,andbuild150,000newhealthandwellness
centerstoincreaseaccesstocareinunderservedareas.
UnacceptablechoiceNo.8:Increasetheavailabilityandqualityofpersonalhealthservicesthatareuniversallyguaranteedinwaysthatexacerbateexistinginequalitiesunlessjustifiedbydifferencesin
need.
Governmentstendtoprioritizeinvestmentsinhospitalinfrastructuretoensureaminimumaccessto
life-savingservicesaswellastotraintheirfuturehealthworkers.Thesehospitalstendtobe
concentratedinurbanareas,whilepeopleinruralareasoftenlackaccesstothemostbasicservices.
UnacceptablechoiceNo.9:Increasetheavailabilityandqualityofcorepublichealthfunctionsinwaysthatexacerbateexistinginequalitiesunlessjustifiedbydifferencesinneed.
Priorto2013,Brazilhadhugedifferencesinthedensityofskilledhealthprofessionals.Thiswaslargely
becausethedecentralizedsystemthatallowedsub-nationalentitiestosettheirownsalariesfor
physicianshadinadvertentlycreateddisincentivesfordoctorstoworkinareaswheresalarieswere
lower.WealthierstatesandcitiesinBrazilthatpaidhigherwagesendedupwithahighernumberof
physicians,whileotherpartsofthecountryexperiencedsignificantshortages.
Acrossthecountrymorethan20percentofmunicipalitieshadashortageofphysiciansinpublicsector
facilities,whilemorethan10percentofmunicipalitieshadnodoctorsatall.ThepooreststatesofBrazil
hadthehighestshortageofhealthworkers,forcingpatientstorelyonnurse-associatesandcommunity
healthworkerswithrelativelylowerlevelsofhealthtraining.(Ref:MonitoringInequalitiesintheHealth
Workforce:TheCaseStudyofBrazil1991-2005,PLOS1,2012).
Then,in2013,Brazillaunchedthemaismedicosprogram,whichofferedfinancialandcareer
advancementincentivesfordoctorstoacceptpostsinunderservedlocations.Thisnewpolicyaddressed
significantdisparitiesinthedistributionofphysiciansinthecountryandmadethecountry’sallocations
forstaffacceptable.
UnacceptablechoiceNo.10:Increasetheavailabilityandqualityofcorepublichealthfunctionsinwaysthatexacerbateexistinginequalities,unlessjustifiedbydifferencesinneed.

DRAFT:Notforattribution
20
Failurestopreventtherapidspreadofthe2014Ebolaoutbreakgrewoutofseveralweaknessesin
Liberia’shealthsystem.Thecountry’slimitedsurveillancecapacitytoidentifyandreportanoutbreak
wasconcentratedinurbanareas,andalmostnon-existentinruralareas,whereEbolawasspreading
fast.ThispostponeddetectionofthediseaseuntilitwasfinallydiagnosedforthefirsttimeinMonrovia.
Skewingresourcestocitiesallowedadeadlyvirustokillpeoplebeforeitwasfinallydetected.
Sincethen,Liberiahasmadesignificantinvestmentsinstrengtheningcorepublichealthfunctions,while
addressingexistinginequalitiesincommunity-levelsurveillanceanddiseasereporting.Theresultshave
alreadybeenfelt.Duringthe2018Lassafeveroutbreakthere,CommunityBasedEventSurveillance
reportingshowedmarkedimprovementswithcompletenessandtimelinessofreporting.Healthofficials
estimatedthatnearlyallLassacaseswerereported.
Fairnessofprocessandaccountability:Aframeworkformakingdecisions
Certainprocessesmustbeestablishedtoclaimfairnessandaccountabilityinpolicymaking.Thisisas
trueinhealthpolicyasitisinanyotherareaofsocialpolicy.Werecognizethatcompleteagreementon
the“fairness”oftheoutcomesofpolicydecisionsisunachievablebecausepeople’sperceptionsofsocial
justicevary.Butwecanagreeonafairprocessformakingthosedecisionsthatthepublicseesas
legitimate.Sopublicparticipationandsomelevelofaccountabilityarenecessary,becausetheyhelp
leadtodecisionsthatcreateageneralsenseoffairnessintheprocess,eventhoughsomepeoplemay
disliketheoutcome.
Hereweteaseoutdifferentstrandsofhealth-financing-relateddecisionsastheyrelatetopublic
involvementandaccountabilityforreasonableness.
Thesefirsttworefertopublicinvolvementandpurchasingdecisions(whattobuy):
• Publicinvolvementinmakingone-offdecisionssuchaswheretolocateanewhealthcenter
oftentakestheshapeofopendiscussionsordebateinconsensusconferences,townmeetings,
orcitizenjuriesorpanels.(Rowe&Frewer2005;Abelsonetal.2008;Mittonetal.2009;WHO
2014).
• Publicinputstolonger-termdecision-makinghave,insomecountries,beenformalizedthrough
representationonbodiessuchashospitalboards,localgovernmenthealthauthorities,priority-
settingcommitteesandinstitutions,ortheboardsofhealthinsurancefunds(Sabik&Lie2008;
Glassman&Chalkidou2008;Stewartetal.2016;Byskovetal.2017;Giedion&Guzman2017;
Simonet2017).
Thesenexttworefertopublicinvolvementandallocationdecisions(howtospend):
• Furtherupstreaminfinancingfunctions,citizenshavebeeninvitedtoparticipateinformal
decisionsonhowtoallocategovernmentbudgetsacrosscompetingneeds.Thishashappened

DRAFT:Notforattribution
21
inplacesasdiverseasBrazil,Cameroon,Europe,Peru,SriLankaandNewYorkCity(WHO2014;
Kasdan&Markman2017).
• Lessdirecteffortsbycivilsocietyorganizationsinclude,forexample,theAfricanHealthBudget
Network.Thisnetworkofgroupshasinfluencedgovernmentallocationstohealththrough
advocacyandbyencouragingAfricangovernmentstoadheretotheagreementmadeinAbuja
Declarationof2001toallocate15%oftheirbudgetstohealth(AfricaHealthBudgetNetwork
2018).
Thesekindsofcitizenengagementcaninfluencedecisions,thoughtheyareonarelativelylimitedscale.
Forexample,withformaldecisions,citizeninvolvementinbudgetinghasbeengenerallylimitedtolower
levelsofgovernment–e.g.municipalities–andusuallyrestrictedtoarelativelysmallproportionofthe
budget(Shapiro&Talmon2017).Withone-offdecisions,limitedevidencesuggeststhatthingslike
townmeetingsandjuriesinfluencethepublic’ssenseofinclusion,eitherwithrespecttothequalityof
publicdebateortheresultingdecisions.Andthoseonhospitalboardsorcitizenpanelstendtobewell
educatedandmaybelimitedintheirabilitytoreflecttheviewsofthebroadercommunity(Campbell,
Craig&Escobar2017).
Thesefinalpointsrefertotheneedforaccountability(transparencywithfairprocess):
Answerabilityandenforceabilityarefundamentaltoaccountability.Sodecisionsthataffectthe
population’swellbeingmustbetransparentandjustified.Andindividualsandinstitutionsengagedin
fraudorothermisconductmustfacecensureorsanctions,perhapsbackedbythejudiciary(Schedler
1999;WHO2014,Gruskin&Daniels2008;Rumboldetal.2017;Yamin2017).
Acommonmotivationforestablishingaccountabilitycomesfromthehumanrightsframework,which
seestheStateasactingonbehalfofitscitizens(Yamin2000;Farmer2003).Informedpublicscrutiny,in
turn,requiresareliablemonitoringsystem,meaningfulpublicparticipationinprocesses,and
transparencyandaccesstoinformation(Yamin2008).
Agrowingbodyofliteraturepointstotheadvantageofinfusingdecisionswithaccountabilityand
transparency.ForemostistheAccountabilityforReasonablenessframeworkappliedtotherationalefor
purchasingservicesinpooledfunds(Daniels2000;Daniels2008;DanielsandSabin2008;Daniels2016;
WHO2014;Petricca&Bekele2017).Thisframeworkestablishesfourconditions:
1. Publicity:Detailsofdecisionsmadeneedtobereadilyavailabletothepublic,alongwiththe
justificationforthosedecisions;
2. Relevance:Theorganizationorauthoritymakingthedecisionmustprovideareasonable
explanationofthecriteriaitusestomakedecisions;
3. Revisionandappeals:Mechanismsforchallengeandappealneedtobeavailablewith
opportunitiestomodifydecisionsovertime,forexample,whennewevidencebecomes
available(whichrequiresadequatedatacollection,discussedinthenextsection);
4. Regulation:Formalrulesareneededtoensurethefirstthreeconditionsarefulfilled.

DRAFT:Notforattribution
22
Whilemostoftheseconditionsarerelativelystraightforward,therelevanceconditioncanbetricky.On
thewholeitsimplymeansthatfair-mindedpeoplecanandshouldagreeondecision-makingcriteria
thatareclearandeasytounderstand—andbeaccessibletothepublic.Thisapproachisincreasingly
usedfordecisionsonbudgetallocationsduringscarcityandforotherdifficultdecision-makingareas,
likepolicyresponsestoclimatechange.Butnoteveryonewillagreeonwhatconstitutesreasonable
criteria.Andevenwhenthecriteriaareacceptedasreasonable,decision-makersmayreasonably
disagreeonhowtoweighthedifferentcriteria.Forexample,“valueformoney”(orbangforthebuck)
asacriterionforallocatingscarceresourcesmightshortchangeequityconsiderations.Inthiscase,
additionalcriteria(cost-effectivenessversusequity)areneededtofullyinformrationingdecisions(e.g.
WHO2014;Baltussenetal.2017;Badano2018).
But,onthewhole,havingdecision-makingbodiesexplainthecriteriafortheirdecisionsfeedsintothis
greatersenseoffairnessinprocess.Box1and2offergoodexamples.
Box1:ParticipatoryBudgetinginBrazil
AprocesspioneeredinPortoAlegrein1989,called“participatorybudgeting”(WHO2014-Makingfair
choices),invitedthepublicintothedecision-makingprocessandexplicitlyprioritizedimprovinghealth
servicesinpoorercommunities.Civilsocietyorganizationshaddemandedgreaterrepresentationin
thesedecisionstobringbalancetowhattheyperceivedasacorruptpoliticalestablishment.Within10
yearsofitsimplementation,publicparticipationinthemunicipality’sbudgetprocessesforthingslike
howtousebondsforcapitalimprovementsincludedover40,000peopleeachyear.[Bhatnagar,Prof.
Deepti;Rathore,Animesh;Torres,MagüiMoreno;Kanungo,Parameeta(2003),ParticipatoryBudgeting
inBrazil(PDF),Ahmedabad;Washington,DC:IndianInstitutesofManagement;WorldBank.]Andthe
shareofthetotalbudgetdedicatedtohealthandeducationtripledto40percentby1996,upfrom13
percentin1985.(RebeccaAbers,“FromClientelismtoCooperation:LocalGovernment,Participatory
Policy,andCivicOrganizinginPortoAlegre,Brazil,”Politics&Society26(1998),pp.511–538.)
Sincethen,participatorybudgetinghasspreadtoBrazil’spublichealthsystem,calledSistemaÚnicode
Saúde(SUS).HalfofthehealthcouncilssetupinnearlyallBrazilianmunicipalitiesareregularcitizens
whoareusersofSUS(mainlypatients).Theremainderincludeshealthworkers,administrators,and
managers.Thesecouncilsareresponsibleforoversightfunctionsthatincludestrategicplanning,
approvingtheannualhealthbudget,andmonitoringthedisbursementoffunds.(MartinezMG&Kohler,
JC.Civilsocietyparticipationinthehealthsystem:thecaseofBrazil'sHealthCouncils.Globalizationand
Health2016.)Thisdrovechangeandpeople’spreferencesarenowreflected.
Absentfromthisframeworkisthequestionofoversight.
Thatis,doesanorganizationorbodyneedtobecreatedtoensurefairnessinthedecision-making
process?Forexample,theWHOConsultativeGrouparguedthatoneoptionwouldbetoestablisha
“standingnationalcommitteeonprioritysettingtohandleparticularlydifficultcases”(WHO2014).
Thesekindsofbodiescanensurepublicdebateandinvolvementwhencombinedwiththeprinciples
behindtheAccountabilityforReasonablenesscriteria.
Publicinvolvementandaccountabilityforreasonablenesscouldbeappliedtoanyofthekeyhealth
financingdecisionsaroundrevenuegeneration,poolingorpurchasing.Thiswouldincludeinvolvingthe

DRAFT:Notforattribution
23
publicindecisionmaking;makingpublicallinformationaboutthedecisionsandmotivationsbehind
them;creatingappealandreviewprocesses;andsettingclearcriteriathatlayoutwhatfactorsshould
influencedecisionoutcomes.Criteriaforreasonableness,however,woulddifferdependingonthe
question.Forexample,decisionsoncontracting(whichhealthservicesorinputsshouldbepurchased
andatwhatprice)aredrivenbyfactorssuchasefficiency,thecostsofadministrationandenforcement,
incentivesforquality,andtheriskoffraud.Theextenttowhichthepubliccouldfeasiblybeengagedin
eachtypeofdecisionwouldneedtobedeterminedonacase-by-casebasis.Butbroadpublicdebate
wouldbewarranted.
Thequestionofoveralltaxpolicy—decisionsabouthowmuchtoraise,whoshouldcontributeand
when—isevenmorecomplicatedandrequiresdeeperconsideration.Thesedecisionsareusuallymade
inparliament,byelectedrepresentativeswhotheoreticallyactonbehalfofcitizens.Changestotax
policyusuallygeneratewidepublicreaction.Anddecisionsmadeusuallyfollowwidelypublicized
debatesamongmembersofparliaments.Buttheoutcomes—thewaythevotestally—donot
necessarilyrepresentpublicsentiment.Viewsvaryonwhetherthisissufficienttoensureaccountability
andfairnessinprocesses.Forexample,addinganadditionallayerofcomplexitytore-enforceprocess
fairnessmaynotbejustifiedwhenthepurposeofaparliamentistorepresentthepeople.However,
manycountrieshaveelectedofficialswhoarerelativelywealthyandwhorepresentwealthy
constituencies.Theywilloftenhaveaconflictofinterestwhenitcomestoraisingmoretaxesormaking
ataxsystemmoreequal.Sootherwaysofinfluencingthesedecisionsneedtobefound.
Box2:SocialAccountabilityinEthiopia
Ethiopiaisnowinitsthirdphaseofalongprocessthatisbringingthepublicintogovernmentdecisions
onhealth,education,agriculture,ruralroadprojects,andwaterandsanitation.Since2011,theEthiopia
SocialAccountabilityProgramhashelpedsetupSocialAccountabilityCommittees(SACs)in223ofthe
country’s770localdistricts,calledworedas.
Thecommitteesaremadeupinequalpartsoflocallyelectedcouncilmembers,locallyappointed
administratorsandcivilsocietyorganizations.Theirmainpurposeistoensurethatlocaladministrative
unitsaretransparentandheldaccountabletocitizens.
TheseSACshelpbuildstrongsystemsforevidence-basedserviceperformancemeasures,usingfive
socialaccountabilitytools:CommunityScoreCards(CSCs)thatusefocusgroupsforself-assessments;
CitizenReportCards(CRCs)thatsurveyhouseholdstoassesthelevelofservicestheyarereceiving;
ParticipatoryPlanningandBudgeting(PPB)andGenderResponsiveBudgeting(GRB)forcitizen
engagementinbudgetplanning;andthePublicExpenditureTrackingSurvey(PETS)forassessmentof
budgetexecution.
Oneexampleofawell-functioningSACisinMalgaWoreda,insouthwesternEthiopia.TheSACthere
startedbyusinghouseholdsurveysandmeasuredaninsufficientnumberofhealthworkerstoservethe
community.Thatputpressureonthelocalgovernmenttoallocatemoreresources.And,asaresult,
healthcentersrecruitedandtrainedadditionalmidwives,healthofficers,andrecordofficers.Through
purchasing,clinicsreceivedneededmedicalequipmentandmedicines.Andinfrastructuremoneywas
allocatedtobuildroadstohealthcentersinTenkaroandHaro,andcreateanewwatersourcein
Manichotown.
TheseSACs,aswithparticipatorybudgetinginBrazil,createinclusionandbringfairnesstotheprocess,

DRAFT:Notforattribution
24
whichmakethelocalgovernmentsaccountabletothecitizenstheyrepresent.
Monitoring
TrackingProgressisaMust
Countriesmustgetmoreseriousaboutdatacollection,orthequestforequitywillbemeaningless.This,
ofcourse,requirestrackingUHCoutcomes.Butitalsorequirestrackinginequitiesinthethree
componentsofhealthfinancing(revenuegeneration,poolingandpurchasing)thatcanaffectUHC
outcomes.
Decisionmakerscannotadjusttheirpoliciesovertimeunlessknowledgeisavailableonwherehealth-
relatedoutcomesaregettingbetterand,moreimportantly,wheretheyaregettingworse.Thisrequires
trackingthosewhoarecovered,thequalityofhealthservicestheyarereceiving,andtheextentto
whichtheyareprotectedfromfinancialhardship.Withouttheseaggregateddata,policymakersare
unabletofocusonthemostdisadvantaged—whichtheymustdotoremaininkeepingwiththegoalsof
UHC.
Ataminimum,policymakersneedregularlycollecteddatadisaggregatedbygender,income(orwealth),
andgeographicallocation(forexample,ruralorurban).Countriesshouldaddonotherdeterminants
thatapplytotheiruniquepopulations,like,forexample,ethnicity,age,familystructure,typeofhealth
problem,andcapacitytodeliver.Theimportantpointhereisthatdisaggregateddatawillallowthe
healthfinancing-relatedinequitiestobemeasuredandtrackedovertime,whichissocriticalto
producingequityduringpolicyadjustments,andkeepinghealthfinancingdecisionsontrackforUHC.
Forexample,onrevenuegeneration,dataneedstobecollectedtounderstandwhoissufferingsevere
financialhardshipfromout-of-pocketpaymentsforwhichtypeofservice,andwhetheradjustmentsto
policiesarereducingtheburden.Onpooling,dataisneededtotrackhowdomesticrevenuesare
allocatedtofinancingschemestoensuretaxmoneyisusedequitablyandnottosubsidizealreadywell-
endowedpools.Andonpurchasing,inequitiesinthedistributionofhealthworkersandotherinputs
suchasessentialmedicinesneedtobemonitored,becausethisfunctiondetermineswhetherthe
servicespeopleneedareavailable,closetothem,andofgoodquality.
Tosupportfairnessofprocess,thesedatathenmustbeanalyzedaccuratelyandpresentedtopolicy
makersinaneasy-to-understandformat(seeHosseinpooretal2018).Theotherhalfofsupporting
fairnessofprocessistoalsoensurethatdataaresharedwiththepublicandotherstakeholdersinaway
theycandigest.
Thismeansmanycountrieswillhavetochangethewaytheymonitor,shareandevaluateprogressin
theirhealthsystems.Neededarerecordsofpatientattendanceandtreatmentathealthfacilities.These
canbecollectedthroughhouseholdsurveys,butareroutinelyavailableiftheyaresystematicallyand
accuratelycollectedatthetimeofserviceandquicklyaggregatedandreported.Theserecordsmaybe
supplementedbyothersources,suchascancerregistries.Buttheyvaryacrosscountriesinnumberand
qualityandgenerallyfailtoprovideinformationonqualityofservices,levelsoffinancialprotection,and
abaseline(whoneedsservices).

DRAFT:Notforattribution
25
Apushisbeingmadenowtouseelectronicmedicalrecordsandspecificallyinputsystems,which
capturecomprehensiveinformationonpatientcare,includingsymptoms,diagnoses,etiologies,
proceduresandoutcomes.(“Towardgreaterintegrationofcareandimprovedefficiency:Acritical
reviewofEHIF’spaymentsystem,WorldBank2017,page46.)
Othermethodsforundertakingtherequiredanalysisincludetrackingoutcomesofadult,maternaland
childmortality(e.g.Marmotetal1991;Mackenbacketal.1997;Gwatkin2000;Victora2003;Moseret
al.2005;Barrosetal.2010;Bendavid2014;Wagstaff,Bredenkamp&Buisman2014;Gwatkin2017).
Theyalsoincludemeasuringprogressinincreasingoverallcoverageandreducinginequalitiesin
coveragewithcorehealthinterventions,largelyfocusedontargeteddiseasesoftheMDGs(e.g.Raoet
al.2014;Alkenbracketal.2015;Restrepo-Méndezetal.2016;Hoganetal.2017;WHO&WorldBank
2017;Wongetal.2017;Victoraetal.2017).
AnumberofdifferentmethodshavebeenusedtodocumentOOPs-relatedfinancialcatastropheand
impoverishment,whichhashelpedpolicymakersunderstandwhoissufferingthemost(e.g.Xuetal.
2003&2006;Wagstaff&Lindelow2014;Bredenkamp&Buisman2016;Khan,Ahmed&Evans2017;
Wagstaffetal.2017aandb;Ghimireetal.2018).Disagreementoverwhichonesworkbesthaveledto
studiesthatincluderesultsfromtwoormoreofthesemethods(forexample,WHOandWorldBank
2017).
AshortcomingintheoverallapproachtotrackingprogresstowardsUHC,asitrelatestoservice
coverageandfinancialprotection,isthatthemethodsdevelopedfailtodrilldowndeepenoughto
unearthalltheinequalitiesassociatedwithhealth-financingfunctions(e.g.Boermaetal.2014;WHO
andWorldBank2017).Improvementsthathavebeenmaderelateto:
• examiningwhetherfiscalpolicyispro-poor,whiletakingintoaccountthenetimpactofwhat
theypayinandwhattheyreceiveincashorin-kindbenefits(e.g.Lustig2016&2017;Jellemaet
al.2017;Lustig2018).
• inequalitiesintheavailabilityofservicesandinkeyinputs,suchashealthworkers(e.g.O’Neillet
al.2013;WHO2015;Speybroecketal.2012).
Toolstohelpcountryanalystsundertakethisworkarenowbeingdeveloped.Theyaredesignedtogive
guidanceon1)estimatingtheabsenceoffinancialprotectionandinequalitiesinthehealthfinancing
functions(Wagstaffetal.2007;Wagstaff2008;Saksena,Hsu&Evans2014;Wagstaff&Eozenou2014;
WorldBank2018a),and2)analyzinginequalitiesinhealthoutcomesandhealthservicecoverage
(Hosseinpoor2016&2018;WorldBank2018).
Forcountrieswithresourcestodohouseholdexpendituresurveys,theWorldBankhasestablishedthe
ADePTResourceCenterwithsoftwarethatallowsanalyststouploadtheirsurveydataandproduce
indicatorsofinequalitiesandunsustainablehealth-relatedfinancialburdens.(WorldBank2018a).
Approachestorapidserviceavailabilityandreadiness,whichcanbeusedtotrackgeographic
inequalities,havealsobeendeveloped,includingtheServiceAvailabilityandReadinessTool(WHO
2018b).
Butforcountrieslackingtheresourcesfortheseexpensive,time-consumingandlabor-intensive
householdsurveys,theWorldBankhasdevelopedtheSwiftSurveyapproach.Thisisalowcost,rapid

DRAFT:Notforattribution
26
wayofmeasuringincomesandtrackingprogressinthereductionofpoverty(WorldBank2018b).This
approachoffershopeoflower-costandtimelywaysofobtainingthenecessarydataforUHCtracking.
Themainmessagehereisthattoolsareavailabletohelpcountries.Butwerecognizethatfindingfunds
topayformonitoringischallenging,especiallyinlow-incomecountries.Thisareaofhealthsystemsis
generallyunderfunded.MostOECDcountriesinvestlessthan4percentoftotalhealthexpendituresin
informationsystems,andlow-andmiddle-incomecountriesinvestlessthan1percent.(WHO,OECD,
WorldBank,2018)
Robustinformationsonecessarytomonitoring,whichprovidespolicymakersandthepublicwith
neededdatatohelpestablishfairprocessesandassesswhetheradecisionisunacceptable,mustbea
priority.
Section5:SeeingtheWayForward
ThisexerciseinmappingoutwhatequityinfinancingUHCmeansistoshowtheneedforafundamental
shiftinpolicymaking.Weknowthatmany,manycountrieshavecommittedtoUHC.Wearestillseeing
deepinequitiesinservicecoverageandfinancialprotectionthatareassociatedwithequityinfinancing.
Thistellsusthatsomethingisgoingwrongindecision-makingprocesses.Webelievethattakingamore
mindfulapproach—applyingthethreeprongsoutlinedinthispaper—willmakeadifference.Thereward
willbemoreequitableUHCoutcomesandgreatersocietalandeconomicbenefits.
Countriesmustchartawayforward.Whetheralreadyontherightpathortryingtoafindawaythere,
theapproachmappedoutinthisreportshouldhelp.Itisdesignedtofillsomegapsinguidanceforthose
whohavecommittedtoUHC.Andwhilemosttechnicaldetailsofwhatcanandshouldbedonehaveto
bedomesticallydetermined,weknowhealthassistanceplaysarole.Theprincipleslaidoutherealso
applytodevelopmentassistance;theyshowthatequitableoutcomesmustbetheultimategoal.
Soforcountryministriesandpolicymakers,thestartingpointistoestablishorexpandbasicguaranteed
packages,withprogressiverealization(expandingthereachovertimetoincludemoreandbetter
services).BasedonanextensionofthelogicofUHC,everycountryshouldstartwithsomelevelof
guaranteedcoveragewithsomeprioritygivetotheworse-off,financedbyprepaidandpooledsystems,
accordingtoabilitytopay.OncecommittedtothisUHCpolicy-makingpath,webelievethethree-
prongedapproachmappedoutinthisreportwillbringclaritytodifficultdecisions.
Onlycountriescanknowwhatneedstobedone,andinwhatorder—identifyingandavoiding
unacceptabledecisions,invitingincivilsocietyandestablishprocessesthatcommunitiescanagreeare
fair,orsettingupdatacollectionprocessesforbettermonitoring.
Thesethreeprongsareintrinsicallylinked.Whenthepublicparticipatesindecisionsandfeelsthat
processesarefair,alldecisionsmovingforwardcarrythatimportantquality.Decisions,ofcourse,are
bestmadebasedonevidence,whichrequiresdatacollectionandmonitoring.Butpolicy-makersneedto
moveforwardwithpublicinvolvementasameansforestablishingprocessfairness,regardlessofwhere
theyareindatacollection.Slowprogressononeshouldnotleadtoslowprogressontheother.
Likewise,countriescangothroughthisprocessandlookforward—andmaybeaddtothelistof10
unacceptableoutcomeswe’veidentifiedthusfar—regardlessofwheretheyareinsettinguppublic

DRAFT:Notforattribution
27
involvementordatacollectionandmonitoring.Theseothertwoprongswilleventuallypropupthe
abilitytoidentifyunacceptabledecisionssotheymaybecorrected,andwillhelpavoidmakingfuture
decisionsthatleadtoinequities.
Theglobalcommunityshouldhelpfacilitatethisshiftusingaparallelthree-prongedapproach.
Aswithcountrydecisions,developmentpartnersshouldsystematicallyintroduceequityconsiderations
intoallengagementsonhealthfinancingpolicies,andassesstheequityimplicationsoftheirfinancial
support.Thegoalhereisthesame:toseewhetherhealthsectorfinancialsupportisleadingcountriesto
makeunacceptablechoices.Developmentpartnersalsoshouldusetheirfinancialandtechnicalsupport
toincreasinglybuildcountrycapacitiesandinstitutionsthatproduceandsupportprocessestoteaseout
unacceptablechoices,establishfairnessinprocess,andcreatebetterdatacollectionandmonitoring.
And,finally,developmentpartnersshoulddevelopthetools,methodsandapproachesessentialto
carryingouttheseworkstreams—asglobalpublicgoods.

AN
NEX
1
Tabl
e 1:
Ineq
ualit
ies
and
Ineq
uitie
s in
UH
C O
utco
mes
and
UH
C F
inan
cing
, Inc
ludi
ng U
nacc
epta
ble
UH
C F
inan
cing
Pol
icy
Cho
ices
UHC
Outc
omes
Outc
omes
In
equa
lities
In
equi
ties
Effec
tive C
over
age w
ith
Need
ed H
ealth
Ser
vices
Diffe
renc
es ac
ross
peop
le or
grou
ps in
eff
ectiv
e cov
erag
e with
healt
h ser
vices
(p
erso
nal h
ealth
servi
ces,
publi
c hea
lth
(inclu
ding n
on-p
erso
nal h
ealth
servi
ces)
and
gove
rnan
ce fu
nctio
ns
Diffe
renc
es in
the e
ffecti
ve co
vera
ge of
he
alth s
ervic
es (in
cludin
g non
-per
sona
l he
alth s
ervic
es) a
nd go
vern
ance
func
tions
un
less j
ustifi
ed by
diffe
renc
es in
healt
h ne
eds1
No
diffe
renc
es in
effec
tive c
over
age o
f he
alth s
ervic
es w
hen t
here
are d
iffere
nces
in
healt
h nee
ds2
Cove
rage
with
Fina
ncial
Pr
otecti
on
Some
peop
le or
grou
ps ar
e pus
hed i
nto
pove
rty or
furth
er in
to po
verty
due t
o out-
of-po
cket
paym
ents
(OOP
s) for
healt
h ser
vices
Some
peop
le or
grou
ps ar
e pus
hed i
nto
pove
rty, o
r dee
per in
to po
verty
due t
o OOP
s be
caus
e of la
ck of
acce
ss or
in us
ing qu
ality
servi
ces g
uara
nteed
by co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g arra
ngem
ents
Diffe
renc
es ac
ross
peop
le or
grou
ps in
the
incide
nce o
r exte
nt of
catas
troph
ic OO
Ps fo
r he
alth s
ervic
es
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n the
inc
idenc
e or e
xtent
of ca
tastro
phic
OOPs
be
caus
e of la
ck of
acce
ss or
in us
ing qu
ality
servi
ces g
uara
nteed
by co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g arra
ngem
ents
1 Hor
izonta
l equ
ity
2 Ver
tical
equit
y

Healt
h Fi
nanc
ing
Func
tions
In
equa
lities
3 In
equi
ties4
Un
acce
ptab
le Fi
nanc
ing
Polic
y Cho
ices5
Reve
nue G
ener
atio
n
Di
ffere
nces
acro
ss pe
ople
and g
roup
s in n
et co
ntribu
tions
to th
e pub
lic fin
ance
syste
m (in
cludin
g, bu
t not
limite
d to h
ealth
) 6
Reve
nue g
ener
ation
syste
ms w
ith
differ
ence
s acro
ss pe
ople
and g
roup
s in n
et co
ntribu
tions
to th
e pub
lic fin
ance
syste
m (in
cludin
g, bu
t not
limite
d to h
ealth
) whic
h ma
ke th
e pos
t-tax
, pos
t-tra
nsfer
disp
osab
le inc
ome d
istrib
ution
less
equa
l than
the p
re-
tax di
stribu
tion
1. Ra
ise ad
dition
al re
venu
es fo
r hea
lth th
at ma
ke co
ntribu
tions
to th
e pub
lic fin
ancin
g sy
stem
less p
rogr
essiv
e with
out
comp
ensa
tory m
easu
res t
hat e
nsur
e tha
t the
post-
tax, p
ost-t
rans
fer di
spos
able
incom
e dist
ributi
on is
not le
ss eq
ual.
Di
ffere
nces
acro
ss pe
ople
and g
roup
s in t
he
incide
nce o
f OOP
s for
healt
h ser
vices
Some
peop
le or
grou
ps ar
e pus
hed i
nto
pove
rty, o
r dee
per in
to po
verty
due t
o OOP
s be
caus
e of la
ck of
acce
ss or
in us
ing qu
ality
servi
ces g
uara
nteed
by co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g arra
ngem
ents
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n the
inc
idenc
e or e
xtent
of ca
tastro
phic
OOPs
be
caus
e of la
ck o
f acc
ess o
r in us
ing qu
ality
servi
ces g
uara
nteed
by co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g arra
ngem
ents
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n the
inc
idenc
e of O
OPs t
hat d
eter t
hem
from
using
quali
ty se
rvice
s gua
rante
ed by
co
mpuls
ory p
repa
id an
d poo
led fin
ancin
g ar
rang
emen
ts
2. Inc
reas
e out-
of-po
cket
paym
ents
for
unive
rsally
guar
antee
d per
sona
l hea
lth
servi
ces w
ithou
t an e
xemp
tion s
ystem
7 or
co
mpen
satin
g mec
hanis
ms.
3 Link
ed to
UHC
outco
mes
4 Link
ed to
UHC
outco
mes
5 Una
ccep
table
as th
ey ex
acer
bate
inequ
ities i
n UHC
outco
mes
6 Net
contr
ibutio
ns ar
e gro
ss co
ntribu
tions
minu
s tra
nsfer
s rec
eived
in ca
sh or
kind
7 G
iven t
he lim
ited e
viden
ce-b
ase i
n sup
port
of su
ch po
licies
, pro
of tha
t thes
e sys
tems a
nd m
echa
nisms
is cr
itical

Healt
h Fi
nanc
ing
Func
tions
In
equa
lities
3 In
equi
ties4
Un
acce
ptab
le Fi
nanc
ing
Polic
y Cho
ices5
Di
ffere
nces
acro
ss fir
ms in
their
net
contr
ibutio
ns to
the p
ublic
finan
ce sy
stem8
Reve
nue g
ener
ation
syste
ms w
ith
differ
ence
s acro
ss fir
ms in
their
net
contr
ibutio
ns to
the p
ublic
finan
ce sy
stems
tha
t can
not b
e jus
tified
by so
me
comp
ensa
ting b
enefi
t for t
he ec
onom
y
Di
ffere
nces
acro
ss in
dividu
als or
grou
ps in
co
ntribu
tions
to vo
luntar
y pre
paid
and
poole
d fina
ncing
arra
ngem
ents
Diffe
renc
es ac
ross
indiv
idual
or gr
oups
in
contr
ibutio
ns to
volun
tary p
repa
id an
d po
oled f
inanc
ing ar
rang
emen
ts ba
sed
large
ly on
healt
h stat
us, in
cludin
g pre
-ex
isting
cond
itions
and r
isk fa
ctors
3. Ra
ise ad
dition
al re
venu
es fo
r univ
ersa
lly
guar
antee
d per
sona
l hea
lth se
rvice
s thr
ough
volun
tary,
prep
aid an
d poo
led
finan
cing a
rrang
emen
ts ba
sed l
arge
ly on
he
alth s
tatus
, inclu
ding p
re-e
xistin
g co
nditio
ns an
d risk
facto
rs.
Pool
ing
Func
tion
Ine
ligibi
lity ac
ross
peop
le an
d gro
ups t
o pa
rticipa
te in
any p
ool o
r diffe
renc
es in
eli
gibilit
y acro
ss pe
ople
and g
roup
s to
partic
ipate
in po
ols
Inelig
ibility
of pe
ople
and g
roup
s to
partic
ipate
in an
y poo
l or d
iffere
nces
in
eligib
ility a
cross
peop
le an
d gro
ups t
o pa
rticipa
te in
pools
unles
s jus
tified
by
differ
ence
s in n
eed9
,10
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n en
rolm
ent w
ith pr
ivate
healt
h ins
uran
ce
includ
ing in
sura
nce f
or se
rvice
s not
guar
antee
d by c
ompu
lsory
prep
aid an
d po
oled f
inanc
ing ar
rang
emen
ts
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n en
rolm
ent w
ith pr
ivate
healt
h ins
uran
ce
includ
ing in
sura
nce f
or se
rvice
s not
guar
antee
d by c
ompu
lsory
prep
aid an
d po
oled f
inanc
ing ar
rang
emen
ts un
less
justifi
ed by
diffe
renc
es in
need
8 For
exam
ple, ta
x holi
days
, exe
mptio
ns fr
om so
cial c
ontrib
ution
s, pr
ofit s
hiftin
g, etc
.) 9 D
iffere
nces
in ne
ed in
clude
both
healt
h and
inco
me. T
hose
with
lowe
r hea
lth ne
ed m
ore h
ealth
servi
ces,
and t
hose
that
are p
oor a
re le
ss ab
le to
pay f
or ne
eded
healt
h ser
vices
. 10
It is
acce
ptable
whe
n elig
ibility
is re
strict
ed to
the w
orse
off (
sicke
r and
poor
er),
but n
ot the
bette
r off (
healt
hier a
nd ric
her).

Healt
h Fi
nanc
ing
Func
tions
In
equa
lities
3 In
equi
ties4
Un
acce
ptab
le Fi
nanc
ing
Polic
y Cho
ices5
Diffe
renc
es in
per
capit
a allo
catio
ns (o
f do
mesti
c gen
eral
gove
rnme
nt re
venu
e or
dono
r fun
ds) t
o pre
paid
and p
ooled
healt
h fin
ancin
g sch
emes
(inclu
ding p
ublic
ly fun
ded h
ealth
servi
ces,
socia
l hea
lth
insur
ance
, volu
ntary
insur
ance
)11
Diffe
renc
es in
per c
apita
alloc
ation
s (of
dome
stic g
ener
al go
vern
ment
reve
nue o
r do
nor f
unds
) acro
ss pr
epaid
and p
ooled
sc
heme
s unit
s unle
ss ju
stifie
d by d
iffere
nces
in
need
or th
e ava
ilabil
ity of
fund
s fro
m oth
er
sour
ces
4. Ch
ange
per c
apita
alloc
ation
s of t
ax
reve
nue1
2 or
dono
r fun
ds ac
ross
prep
aid
and p
ooled
finan
cing s
chem
es in
way
s tha
t exa
cerb
ate in
equit
ies, u
nless
justi
fied
by di
ffere
nces
in ne
ed or
the a
vaila
bility
of
funds
from
othe
r sou
rces.
W
ithin
finan
cing s
chem
es, d
iffere
nces
in pe
r ca
pita a
lloca
tions
from
high
er to
lowe
r au
tonom
ous,
admi
nistra
tive u
nits
With
in fin
ancin
g sch
emes
, diffe
renc
es in
per
capit
a allo
catio
ns fr
om hi
gher
to lo
wer
auton
omou
s, ad
minis
trativ
e unit
s unle
ss
justifi
ed by
diffe
renc
es in
need
or th
e av
ailab
ility o
f fund
s fro
m oth
er so
urce
s
5. W
ithin
finan
cing s
chem
es, c
hang
e per
ca
pita a
lloca
tions
from
high
er to
lowe
r ad
minis
trativ
e lev
els in
way
s tha
t ex
acer
bate
inequ
ities,
unles
s jus
tified
by
differ
ence
s in n
eed o
r the
avail
abilit
y of
funds
from
othe
r sou
rces.
W
ithin
sche
mes o
r poo
ls, di
ffere
nces
in
alloc
ation
s of fu
nds a
cross
dise
ases
With
in sc
heme
s or p
ools,
diffe
renc
es in
all
ocati
ons o
f fund
s acro
ss di
seas
es th
at ar
e no
t justi
fied b
y diffe
renc
es in
need
or th
e av
ailab
ility o
f fund
s fro
m oth
er so
urce
s
6. W
ithin
sche
mes o
r poo
ls, ch
ange
all
ocati
ons o
f fund
s acro
ss di
seas
es in
wa
ys th
at ex
acer
bate
inequ
ities,
unles
s jus
tified
by di
ffere
nces
in ne
ed or
the
avail
abilit
y of fu
nds f
rom
other
sour
ces.
Purc
hasin
g Fu
nctio
n
Di
ffere
nces
in en
titlem
ents
of gu
aran
teed
servi
ce pa
ckag
es, im
plicit
or ex
plicit
, acro
ss
peop
le an
d gro
ups1
3
Diffe
renc
es in
entitl
emen
ts of
guar
antee
d se
rvice
pack
ages
acro
ss pe
ople
and g
roup
s un
less j
ustifi
ed by
diffe
renc
es in
need
9
7. Int
rodu
ce hi
gh-co
st, lo
w-be
nefit
inter
venti
ons t
o a un
iversa
lly gu
aran
teed
servi
ce pa
ckag
e befo
re ac
hievin
g clos
e to
full c
over
age w
ith lo
w-co
st, hi
gh-b
enefi
t se
rvice
s.
11 H
ealth
care
finan
cing s
chem
es ar
e the
main
type
s of fi
nanc
ing ar
rang
emen
ts thr
ough
whic
h hea
lth se
rvice
s are
paid
for an
d obta
ined b
y peo
ple. H
ere w
e refe
r to p
ooled
sche
mes r
ather
than
to
OOPs
, inclu
ding n
ation
al or
sub-
natio
nal h
ealth
servi
ces f
unde
d fro
m go
vern
ment
reve
nues
(som
etime
s with
dono
r fun
ds as
well
), so
cial h
ealth
insu
ranc
e, vo
luntar
y ins
uran
ce (O
ECD
2011
).
12 T
ax re
venu
e exc
ludes
socia
l hea
lth in
sura
nce c
ontrib
ution
s 13
Enti
tleme
nts re
flect
the se
rvice
s and
leve
ls of
finan
cial p
rotec
tion t
o whic
h peo
ple ar
e enti
tled
de ju
re. W
hethe
r peo
ple re
ceive
thes
e enti
tleme
nts de
facto
is a
matte
r for
purch
asing
.
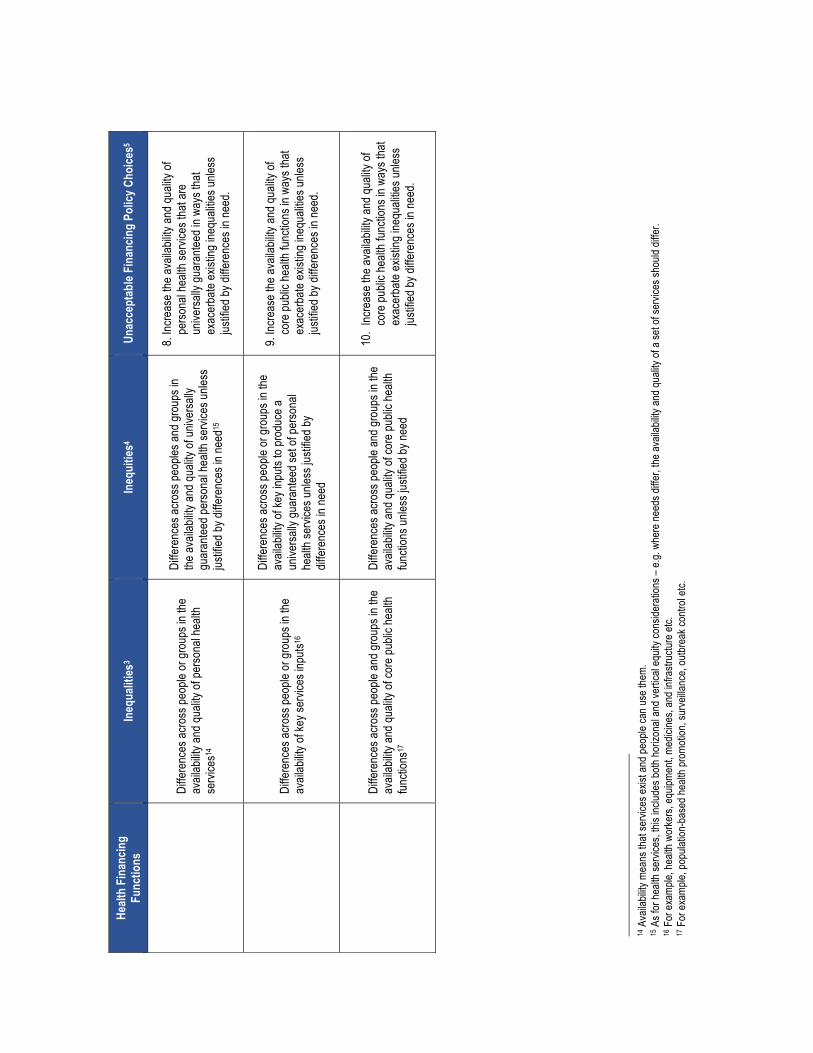
Healt
h Fi
nanc
ing
Func
tions
In
equa
lities
3 In
equi
ties4
Un
acce
ptab
le Fi
nanc
ing
Polic
y Cho
ices5
Di
ffere
nces
acro
ss pe
ople
or gr
oups
in th
e av
ailab
ility a
nd qu
ality
of pe
rsona
l hea
lth
servi
ces1
4
Diffe
renc
es ac
ross
peop
les an
d gro
ups i
n the
avail
abilit
y and
quali
ty of
unive
rsally
gu
aran
teed p
erso
nal h
ealth
servi
ces u
nless
jus
tified
by di
ffere
nces
in ne
ed15
8. Inc
reas
e the
avail
abilit
y and
quali
ty of
perso
nal h
ealth
servi
ces t
hat a
re
unive
rsally
guar
antee
d in w
ays t
hat
exac
erba
te ex
isting
ineq
ualiti
es un
less
justifi
ed by
diffe
renc
es in
need
.
Di
ffere
nces
acro
ss pe
ople
or gr
oups
in th
e av
ailab
ility o
f key
servi
ces i
nputs
16
Diffe
renc
es ac
ross
peop
le or
grou
ps in
the
avail
abilit
y of k
ey in
puts
to pr
oduc
e a
unive
rsally
guar
antee
d set
of pe
rsona
l he
alth s
ervic
es un
less j
ustifi
ed by
dif
feren
ces i
n nee
d
9. Inc
reas
e the
avail
abilit
y and
quali
ty of
core
publi
c hea
lth fu
nctio
ns in
way
s tha
t ex
acer
bate
exist
ing in
equa
lities
unles
s jus
tified
by di
ffere
nces
in ne
ed.
Di
ffere
nces
acro
ss pe
ople
and g
roup
s in t
he
avail
abilit
y and
quali
ty of
core
publi
c hea
lth
functi
ons1
7
Diffe
renc
es ac
ross
peop
le an
d gro
ups i
n the
av
ailab
ility a
nd qu
ality
of co
re pu
blic h
ealth
fun
ction
s unle
ss ju
stifie
d by n
eed
10.
Incre
ase t
he av
ailab
ility a
nd qu
ality
of co
re pu
blic h
ealth
func
tions
in w
ays t
hat
exac
erba
te ex
isting
ineq
ualiti
es un
less
justifi
ed by
diffe
renc
es in
need
.
14 A
vaila
bility
mea
ns th
at se
rvice
s exis
t and
peop
le ca
n use
them
. 15
As f
or he
alth s
ervic
es, th
is inc
ludes
both
horiz
onal
and v
ertic
al eq
uity c
onsid
erati
ons –
e.g.
wher
e nee
ds di
ffer,
the av
ailab
ility a
nd qu
ality
of a s
et of
servi
ces s
hould
diffe
r.
16 F
or ex
ample
, hea
lth w
orke
rs, eq
uipme
nt, m
edici
nes,
and i
nfras
tructu
re et
c. 17
For
exam
ple, p
opula
tion-
base
d hea
lth pr
omoti
on, s
urve
illanc
e, ou
tbrea
k con
trol e
tc.

References
Abelson,J.,Giacomini,M.,Lehoux,P.,andGauvin,F.P.2007.“Bringing‘thePublic’intoHealthTechnologyAssessmentandCoveragePolicyDecisions:FromPrinciplestoPractice.”HealthPolicy82:37-50.
AfricaHealthBudgetNetwork.2018.http://africahbn.info
AlkenbrackS,ChaitkinM,ZengW,CoutureT,SharmaS.DidequityofreproductiveandmaternalhealthservicecoverageincreaseduringtheMDGera?Ananalysisoftrendsanddeterminantsacross74low-andmiddle-incomecountries.PLoSOne2015;10:e134905.
Badano,G.,2018.”IfYou’reaRawlsian,HowComeYou’reSoClosetoUtilitarianismandIntuitionism?ACritiqueofDaniels’AccountabilityforReasonableness.”HealthCareAnalysis26(1):1-16.
Baltussen,R.,Jansen,M.P.,Bijlmakers,L.,Tromp,N.,Yamin,A.E.,andNorheim,O.F.2017.“ProgressiveRealisationofUniversalHealthCoverage:WhataretheRequiredProcessesandEvidence?”BMJGlobalHealth2(3),p.e000342.
Barros,F.C.,Victora,C.G.,Scherpbier,R.andGwatkin,D.,2010.Socioeconomicinequitiesinthehealthandnutritionofchildreninlow/middleincomecountries.RevistadeSaúdePública,44(1),pp.1-16.
Bastagli,F,Coady,D.,andGupta,M.S.2012.“IncomeInequalityandFiscalPolicy.”InternationalMonetaryFundStaffDiscussionNote12/08.
Bendavid,E.,2014.Changesinchildmortalityovertimeacrossthewealthgradientinless-developedcountries.Pediatrics,134:e1551–59.
Byskov,J.,Maluka,S.O.,Marchal,B.,Shayo,E.H.,Bukachi,S.,Zulu,J.M.,Blas,E.,Michelo,C.,Ndawi,B.,andHurtig,A.K.2017.“TheNeedforGlobalApplicationoftheAccountabilityforReasonablenessApproachtoSupportSustainableOutcomes:CommentonExpandedHTA:EnhancingFairnessandLegitimacy".InternationalJournalofHealthPolicyandManagement6(2):115.
Campbell,M.,Craig,P.,andEscobar,O.2017.“ParticipatoryBudgetingandHealthandWellbeing:ASystematicScopingReviewofEvaluationsandOutcomes.”TheLancet390:S30.
Cevik,S.andCorrea-Caro,C.2015.“Growing(Un)equal:FiscalPolicyandIncomeInequalityinChinaandBRIC.”IMFWorkingPaper15/68,Washington,DC.
Chaumont,C.,Hsi,J.,Bohne,C.,Mostaghim,S.andMoon,S.,2017.“ANewGoldenAge?ProposalforanInnovativeGlobalHealthFundingMechanismforMiddle-IncomeCountries.”GlobalChallenges1(7).
Chima,C.C.andFranzini,L.,2015.“SpilloverEffectofHIV-specificForeignAidonImmunizationServicesinNigeria.”InternationalHealth8(2):108-115.
Clements,B.,Gaspar,V.,andGupta,S.2015.“TheIMFandIncomeDistribution.”InequalityandFiscalPolicy,page21.

Daniels,N.2000.“AccountabilityforReasonableness.EstablishingaFairProcessforPrioritySettingisEasierthanAgreeingonPrinciples.”BritishMedicalJournal321:1300-1301.
Daniels,N.2008.“Justhealth:meetinghealthneedsfairly.”Cambridge:CambridgeUniversityPress.
Daniels,N.andSabin,J.E.,2008.“SettingLimitsFairly:LearningtoShareResourcesforHealth.”2ndedition.Oxford:OxfordUniversityPress.
Daniels,N.2011.“AgingandIntergenerationalEquity.”InGlobalPopulationAgeing:PerilorPromise,editedbyJ.R.Beard,S.Biggs,D.E.Bloom,L.P.Fried,P.Hogan,A.Kalache,andS.J.Olshansky.Geneva:WorldEconomicForum.
Daniels,N.2016.“AccountabilityforReasonablenessandPrioritySettinginHealth.InPrioritizationinMedicine,editedbyE.NagelandM.Lauerer.Springer,Cham.
EuropeanCommission.2013.“TheImpactoftheFinancialCrisisonUnmetneedsforHealthcare
Evans,T.,Whitehead,M.,Diderichsen,F.,Bhuiya,A.andWirthM.2001.ChallengesInequitiesinHealth:FromEthicstoAction.NewYork:TheRockefellerFoundation,NewYork:OxfordUniversityPress.
Farmer,P.2004.“PathologiesofPower:Health,HumanRights,andtheNewWaronthePoor.”Volume4.Berkeley:UniversityofCaliforniaPress.
Fleurbaey,M.andManiquet,F.2017.“OptimalIncomeTaxationTheoryandPrinciplesofFairness.”CentreforOperationalResearchandEconometricsDiscussionPaper,UniversitéCatholiquedeLouvain.https://uclouvain.be/en/research-institutes/immaq/core/discussion-papers.html
Ghimire,M.,Ayer,R.andKondo,M.,2018.Cumulativeincidence,distribution,anddeterminantsof catastrophic health expenditure in Nepal: results from the living standards survey.Internationaljournalforequityinhealth,17(1),p.23.
Giedion,U.andGuzman,J.2017.“DefiningtheRulesoftheGame:GoodGovernancePrinciplesfortheDesignandRevisionoftheHealthBenefitsPackage,”inWhat'sIn,What'sOut:DesigningBenefitsforUniversalHealthCoverage,editedbyA.Glassman,U.Giedion,andP.C.Smith.Washington,DC:BrookingsInstitutionPress.
Glassman,A.andChalkidou,K.2012.“Priority-settinginHealth:BuildingInstitutionsforSmarterPublicSpending.”Washington,DC:CenterforGlobalDevelopment.
Gruskin,S.andDaniels,N.2008.“JusticeandHumanRights:PrioritySettingandFair,DeliberativeProcess.”AmericanJournalofPublicHealth98:1573-7.
Gwatkin,D.R.,2000.Healthinequalitiesandthehealthofthepoor:Whatdoweknow?Whatcanwedo?.Bulletinoftheworldhealthorganization,78(1),pp.3-18.
Gwatkin,D.R.,2017.Trendsinhealthinequalitiesindevelopingcountries.TheLancetGlobalHealth,5(4),pp.e371-e372.

Hogan,D.R.,Stevens,G.A.,Hosseinpoor,A.R.andBoerma,T.,2017.MonitoringuniversalhealthcoveragewithintheSustainableDevelopmentGoals:developmentandbaselinedataforanindexofessentialhealthservices.TheLancetGlobalHealth.
Hosseinpoor,A.R.,Bergen,N.,Barros,A.J.,Wong,K.L.,Boerma,T.andVictora,C.G.,2016.Monitoringsubnationalregionalinequalitiesinhealth:measurementapproachesandchallenges.Internationaljournalforequityinhealth,15(1),p.18.DHS,comparemethods
Hosseinpoor,A.R.,Bergen,N.,Schlotheuber,A.andBoerma,T.,2018.Nationalhealthinequalitymonitoring:currentchallengesandopportunities.Globalhealthaction,11(sup1),p.1392216.
International MonetaryFund (IMF).2017. FiscalMonitor: Tackling Inequality.WashingtonDC.October2017
Jellema, J., Wai-Poi, M. and Afkar, R., 2017. The Distributional Impact of Fiscal Policy inIndonesia. The Distributional Impact of Taxes and Transfers, p.149. CEQ Commitment toEquity,TulaneUniversity,WorkingPaper40.
Kaiser,K.,Bredenkamp,C.,andIglesias,R.2016.SinTaxReforminthePhilippines:TransformingPublicFinance,Health,andGovernanceforMoreInclusiveDevelopment.DirectionsinDevelopment.Washington,DC:WorldBank.doi:10.1596
Kasdan, A. andMarkman, E., 2017. “Participatory Budgeting and Community-Based Research:Principles,Practices,andImplicationsforImpactValidity.”NewPoliticalScience,39(1):143-155.
Khan, J.A.,Ahmed,S.andEvans,T.G.,2017.“Catastrophichealthcareexpenditureandpovertyrelatedtoout-of-pocketpaymentsforhealthcareinBangladesh—anestimationoffinancialrisk protection of universal health coverage.”Health policy and planning. 32(8), pp.1102-1110.
Knaul,F.M.,Wong,R.,Arreola-Ornelas,H.,Méndez,O.,Bitran,R.,Campino,A.C.,FlórezNieto,C.E.,Giedion,U.,Maceira,D.,Rathe,M.,andValdivia,M.2011.“HouseholdCatastrophicHealthExpenditures:AComparativeAnalysisof12LatinAmericanandCaribbeanCountries.SaludPúblicadeMéxico53:s85-s95.
Knaul,F.M.,Arreola-Ornelas,H.,Mendez-Carniado,O.,Bryson-Cahn,C.,Barofsky,J.,Maguire,R.,Miranda,M.andSesma,S.2006.“Evidenceisgoodforyourhealthsystem:policyreformtoremedycatastrophicandimpoverishinghealthspendinginMexico.”TheLancet,368:1828-41
Kotlikoff,L.J.2018.“MeasuringIntergenerationalJustice.”IntergenerationalJusticeReview11(2).
Lu,J.F.R.,Leung,G.M.,Kwon,S.,Tin,K.Y.,vanDoorslaer,E.,andO’Donnell,O.“HorizontalEquityinHealthCareUtilization:EvidencefromThreeHigh-IncomeAsianEconomies.”EQUITAPProject:WorkingPaperNo.6.
Lustig,N.,etal.2013.“TheImpactofTaxesandSocialSpendingonInequalityandPovertyinArgentina,Bolivia,Brazil,Mexico,PeruandUruguay:AnOverview.”CEQWorkingPaperNo.13.NewOrleans:TulaneUniversity.
Lustig,N.2016.“InequalityandFiscalRedistributioninMiddleIncomeCountries:Brazil,Chile,Colombia,Indonesia,Mexico,PeruandSouthAfrica.”JournalofGlobalizationandDevelopment7(1):17-60.

Lustig,N.2017.“TheImpactofTaxesandSocialSpendingonIncomeDistributionandPovertyinLatinAmerica:AnApplicationoftheCommitmenttoEquity(CEQ)Methodology.”No.1714.NewOrleans:TulaneUniversity,DepartmentofEconomics.
Mackenbach,J.P.,Kunst,A.E.,Cavelaars,A.E.,Groenhof,F.,Geurts,J.J.andEUWorkingGrouponSocioeconomicInequalitiesinHealth,1997.SocioeconomicinequalitiesinmorbidityandmortalityinwesternEurope.Thelancet,349(9066),pp.1655-1659.
Marmot,M.G.,Stansfeld,S.,Patel,C.,North,F.,Head,J.,White,I.,Brunner,E.,Feeney,A.andSmith,G.D.,1991.HealthinequalitiesamongBritishcivilservants:theWhitehallIIstudy.TheLancet,337(8754),pp.1387-1393.
MartinsenL.etal.2017.“DoLessPopulousCountriesReceiveMoreDevelopmentAssistanceforHealthperCapita?Longitudinalevidencefor143countries,1990–2014.”BMJGlobalHealth2018,(3).doi:10.1136/bmjgh-2017-000528
Mitton,C.,Smith,N.,Peacock,S.,Evoy,B.,andAbelson,J.2009.“PublicParticipationinHealthCarePrioritySetting:AScopingReview.”HealthPolicy,91:219-28.
Moser,K.A.,Leon,D.A.andGwatkin,D.R.,2005.Howdoesprogresstowardsthechildmortalitymillenniumdevelopmentgoalaffectinequalitiesbetweenthepoorestandleastpoor?AnalysisofDemographicandHealthSurveydata.Bmj,331(7526),pp.1180-1182.
Mulenga,A.andAtaguba,J.E.O.2017.“AssessingIncomeRedistributiveEffectofHealthFinancinginZambia.”SocialScience&Medicine189:1-10.
Murray,C.J.,Xu,K.,Klavus,J.,Kawabata,K.,Hanvoravongchai,P.,Zeramdini,R.,Aguilar-Rivera,A.M.,andEvans,D.B.2003.“AssessingtheDistributionofHouseholdFinancialContributionstotheHealthSystem:ConceptsandEmpiricalApplication.”HealthSystemsPerformanceAssessment:Debates,MethodsandEmpiricism12.Geneva:WorldHealthOrganization.
O’Donnell,O.,VanDoorslaer,E.,Rannan-Eliya,R.P.,Somanathan,A.,Adhikari,S.R.,Akkazieva,B.,Harbianto,D.,Garg,C.C.,Hanvoravongchai,P.,Herrin,A.N.,andHuq,M.N.2008.“WhoPaysforHealthCareinAsia?”JournalofHealthEconomics27(2):460-475.
O'Neill,K.,Takane,M.,Sheffel,A.,Abou-Zahr,C.andBoerma,T.,2013.Monitoringservicedeliveryforuniversalhealthcoverage:theServiceAvailabilityandReadinessAssessment.BulletinoftheWorldHealthOrganization,91(12),pp.923-931.
OECD.2015.“FiscalSustainabilityofHealthSystems:BridgingHealthandFinancingPerspectives.”
Ottersen,T.andNorheim,O.F.2014.“MakingFairChoicesonthePathtoUniversalHealthCoverage.”OnbehalfoftheWorldHealthOrganizationConsultativeGrouponEquityandUniversalHealthCoverage.BulletinoftheWorldHealthOrganization2014(92):389.doi:http://dx.doi.org/10.2471/BLT.14.139139
Ottersen,T.,Moon,S.,andRøttingen,J.A.2017.“TheChallengeofMiddle-IncomeCountriestoDevelopmentAssistanceforHealth:Recipients,Funders,Both,orNeither?”HealthEconomics,PolicyandLaw12(2):265-284

Ottersen,T.,Kamath,A.,Moon,S.,Martinsen,L.,andRøttingen,J.A.2017.“DevelopmentAssistanceforHealth:WhatCriteriadoMulti-andBilateralFundersUse?”HealthEconomics,Policy,andLaw12(2):223-244.
Ottersen,T.andSchmidt,H.2017.“UniversalHealthCoverageandPublicHealth:EnsuringParityandComplementarity.”AmericanJournalofPublicHealth17(2):248-250.
Petricca,K.andBekele,A.2017.“ConceptualizationsofFairnessandLegitimacyintheContextofEthiopianHealthPrioritySetting:ReflectionsontheApplicabilityofAccountabilityforReasonableness.”DevelopingWorldBioethics00:1–8.https://doi.org/10.1111/dewb.12153
Pietschmann,E.2014.“ForgottenorUnpromising?TheElusivePhenomenonofUnder-aidedCountries,SectorsandSub-NationalRegions.”GermanDevelopmentInstitute,Studies80.http://edoc.vifapol.de/opus/volltexte/2015/5612/pdf/Studies_80.pdf
Rao,M.,Katyal,A.,Singh,P.V.,Samarth,A.,Bergkvist,S.,Kancharla,M.,Wagstaff,A.,Netuveli,G.andRenton,A.,2014.ChangesinaddressinginequalitiesinaccesstohospitalcareinAndhraPradeshandMaharashtrastatesofIndia:adifference-in-differencesstudyusingrepeatedcross-sectionalsurveys.BMJopen,4(6),p.e004471.
RashtriyaSwasthyaBimaYojana(RSBY).2018.OverviewofStateWiseenrolment.http://www.rsby.gov.in/statewise.aspx?state=4
Rechel,B.,Thomson,S.,andVanGinneken,E.2010.“HealthSystemsinTransition:TemplateforAuthors.”WHOfortheEuropeanObservatoryonHealthSystemsandPolicies,Copenhagen.
Resnik,D.B.,MacDougall,D.R.,andSmith,E.M.2018.“EthicalDilemmasinProtectingSusceptibleSubpopulationsfromEnvironmentalHealthRisks:Liberty,Utility,Fairness,andAccountabilityforReasonableness.”TheAmericanJournalofBioethics18(3):29-41.
Restrepo-Méndez,M.C.,Barros,A.J.,Wong,K.L.,Johnson,H.L.,Pariyo,G.,França,G.V.,Wehrmeister,F.C.andVictora,C.G.,2016.Inequalitiesinfullimmunizationcoverage:trendsinlow-andmiddle-incomecountries.BulletinoftheWorldHealthOrganization,94(11),p.794.
RoweG.andFrewerL.J.2005.“ATypologyofPublicEngagementMechanisms.”Science,Technology,andHumanValues30:251-90.
Rumbold,B.,Baker,R.,Ferraz,O.,Hawkes,S.,Krubiner,C.,Littlejohns,P.,Norheim,O.F.,Pegram,T.,Rid,A.,Venkatapuram,S.,andVoorhoeve,A.2017.UniversalHealthCoverage,PrioritySetting,andtheHumanRighttoHealth.TheLancet390(10095):712-714.
Sabik,L.M.andLie,R.K.2008.“PrioritySettinginHealthCare:LessonsfromtheExperiencesof
EightCountries.”InternationalJournalforEquityinHealth7:4.
Saksena,P.,Hsu,J.andEvans,D.B.,2014.Financialriskprotectionanduniversalhealthcoverage:evidenceandmeasurementchallenges.PLoSmedicine,11(9),p.e1001701.
Schedler,A.1999.“ConceptualizingAccountability.”InTheSelf-restrainingState:PowerandAccountabilityinNewDemocracies,editedbyA.Schedler,L.Diamond,andM.F.Plattner.Boulder,Co:LynneRiennerPublishers.

Shapiro,E.andTalmon,N.2017.“ACondorcet-ConsistentParticipatoryBudgetingAlgorithm.”
Simonet,D.2017.“PublicValuesandAdministrativeReformsinFrenchHealthCare.”JournalofPublicAffairs17(3).
Skirbekk,V.,Ottersen,T.,Hamavid,H.,Sadat,N.,andDieleman,J.L.2017.“VastMajorityofDevelopmentAssistanceforHealthFundsTargetThoseBelowAgeSixty.”HealthAffairs36(5):926-930.
Sousa,A.,Dal,M.andCarvalho,C.2012.“Monitoringinequalitiesinthehealthworkforce:thecasestudyofBrazil1991-2005”PLoSOne.7(3):e33399.doi:10.1371/journal.pone.0033399.
Speybroeck, N., G. Paraje, A. Prasad, P. Goovaerts, S. Ebener, D.B. Evans, 2012. "Inequalityindicators of access to human resources for health: measurement issues", GeographicalAnalysis,44(2):151-161,2012.
Steele,C.A.2017.“PublicGoodsandDonorPriorities:ThePoliticalEconomyofDevelopmentAidforInfectiousDiseaseControl.”ForeignPolicyAnalysisp.orx002.
Stewart,E.A.,Greer,S.L.,Wilson,I.,andDonnelly,P.D.2016.“PowertothePeople?AnInternationalReviewofTheDemocratizingEffectsofDirectElectionstoHealthcareOrganizations.”TheInternationalJournalofHealthPlanningandManagement31(2).
Summers,L.2018.“Taxesforhealth:Evidenceclearstheair.”CommentaryinTheLancetTaskforceonNCDsandeconomics.
UnitedNations.2018.“TheSustainableDevelopmentGoals:17GoalstoTransformOurWorld.”http://www.un.org/sustainabledevelopment/sustainable-development-goals
Urquieta-Salomon,JandVillarreal,H.2016.“EvolutionofhealthcoverageinMexico:evidenceofprogressandchallengesintheMexicanhealthsystem.”HealthPolicyandPlanning31,28-36doi10.1093/heapol/czv015
VanDoorslaer,E.andO’Donnell,O.2011.“MeasurementandExplanationofInequalityinHealthandHealthCareinLow-IncomeSettings.InHealthInequalityandDevelopment.London:PalgraveMacmillan.
VanMinh,H.,Phuong,N.T.K.,Saksena,P.,James,C.D.,andXu,K.2013.“FinancialBurdenofHouseholdOut-of-PocketHealthExpenditureinVietNam:FindingsfromtheNationalLivingStandardSurvey2002–2010.”SocialScienceandMedicine96:258-263.
Vassall,A.,Shotton,J.,Reshetnyk,O.K.,Hasanaj-Goossens,L.,Weil,O.,Vohra,J.,Timmermans,N.,Vinyals,L.,andAndre,F.2014.“TrackingAidFlowsforDevelopmentAssistanceforHealth.”GlobalHealthAction7(1):23510.
Verbist,G.andFigari,F.2014.“TheRedistributiveEffectandProgressivityofTaxesRevisited:AnInternationalComparisonAcrosstheEuropeanUnion.”FinanzArchiv:PublicFinanceAnalysis70(3):405-429.
Victora,C.G.,Wagstaff,A.,Schellenberg,J.A.,Gwatkin,D.,Claeson,M.andHabicht,J.P.,2003.Applyinganequitylenstochildhealthandmortality:moreofthesameisnotenough.TheLancet,362(9379),pp.233-241.

Victora,C.G.,Barros,A.J.,França,G.V.,daSilva,I.C.,Carvajal-Velez,L.andAmouzou,A.,2017.Thecontributionofpoorandruralpopulationstonationaltrendsinreproductive,maternal,newborn,andchildhealthcoverage:analysesofcross-sectionalsurveysfrom64countries.TheLancetGlobalHealth,5(4),pp.e402-e407.
Wagstaff,A.andVanDoorslaer,E.,2000.Equityinhealthcarefinanceanddelivery.Handbookofhealtheconomics,1,pp.1803-1862.
Wagstaff,A.,O'Donnell,O.,VanDoorslaer,E.andLindelow,M.,2007.Analyzinghealthequityusinghouseholdsurveydata:aguidetotechniquesandtheirimplementation.WorldBankPublications.
Wagstaff,A.,2008.Measuringfinancialprotectioninhealth(Vol.4554).WorldBankPublications.
Wagstaff,A.andEozenou,P.,2014.CATAmeetsIMPOV:aunifiedapproachtomeasuringfinancialprotectioninhealth[PolicyResearchWorkingPaperSeries:6861].WashingtonDC:TheWorldBank
Wagstaff,A.andLindelow,M.,2014.Arehealthshocksdifferent?EvidencefromamultishocksurveyinLaos.Healtheconomics,23(6),pp.706-718.
Wagstaff,A.,Bredenkamp,C.andBuisman,L.R.,2014.Progressonglobalhealthgoals:arethepoorbeingleftbehind?.TheWorldBankResearchObserver,29(2),pp.137-162.–healthoutcomes;coverage.
Wagstaff,A.,Flores,G.,Smitz,M.F.,Hsu,J.,Chepynoga,K.andEozenou,P.,2017a.Progressonimpoverishinghealthspendingin122countries:aretrospectiveobservationalstudy.TheLancetGlobalHealth.
Wagstaff,A.,Flores,G.,Hsu,J.,Smitz,M.F.,Chepynoga,K.,Buisman,L.R.,vanWilgenburg,K.andEozenou,P.,2017b.Progressoncatastrophichealthspendingin133countries:aretrospectiveobservationalstudy.TheLancetGlobalHealth.
WorldBank.2012.“Mexico’sSocialProtectionSysteminHealthandtheFinancialProtectionofCitizenswithoutSocialSecurity”.WashingtonDC
WorldHealthOrganization.2010.“TheWorldHealthReport2010:HealthSystemsFinancing,thePathtoUniversalCoverage.”Geneva:WHO.
WorldHealthOrganization.2014.Makingfairchoicesonthepathtouniversalhealthcoverage.FinalreportoftheWHOConsultativeGrouponEquityandUniversalHealthCoverage,WHO,Geneva.http://www.who.int/choice/documents/making_fair_choices/en/
WorldHealthOrganizationandtheInternationalBankforReconstructionandDevelopment.2017.“Trackinguniversalhealthcoverage:2017globalmonitoringreport.”TheWorldBank,WashingtonDC.
WorldBank.NigeriaHealthFinancingSystemAssessment-WorldBankDiscussionpaper(forthcoming).WorldBank:Washington,DC

Wong,K.L.,Restrepo-Méndez,M.C.,Barros,A.J.andVictora,C.G.,2017.Socioeconomicinequalitiesinskilledbirthattendanceandchildstuntinginselectedlowandmiddleincomecountries:Wealthquintilesordeciles?.PloSone,12(5),p.e0174823.
Woo,J.,Bova,E.,Kinda,T.,andZhang,Y.S.2017.“DistributionalConsequencesofFiscalAdjustments:WhatDotheDataSay?”IMFEconomicReview,pages1-35.
Xu, K., Evans, D.B., Kawabata, K., Zeramdini, R., Klavus, J. andMurray, C.J., 2003. Householdcatastrophichealthexpenditure:amulticountryanalysis.Thelancet,362(9378),pp.111-117.
Xu, K., Evans, D.B., Kawabata, K., Zeramdini, R., Klavus, J. andMurray, C.J., 2003. Householdcatastrophichealthexpenditure:amulticountryanalysis.Thelancet,362(9378),pp.111-117.
Xu,K.,Evans,D.,Carrin,G.,Aguilar-RiverA.M.,Musgrove,T.,andEvans,T.2007.“ProtectingHouseholdsfromCatastrophicHealthSpending.”HealthAffairs26(4).
Yamin,A.E.,2008.Sufferingandpowerlessness:thesignificanceofpromotingparticipationinrights-basedapproachestohealth.HealthandHumanRights,11:5-22.
Yamin,A.E.2010.“TowardTransformativeAccountability:ApplyingRights-BasedApproachtoFulfillMaternalHealthObligations.”SUR-InternationalJournalonHumanRights,12:95.
Yamin,A.E.2017.«TakingtheRighttoHealthSeriously:ImplicationsforHealthSystems,Courts,andAchievingUniversalHealthCoverage.”HumanRightsQuarterly39(2):.341-368.

#UHCfinance
For more information about theAnnual UHC Financing Forum please visit
http://worldbank.org/uhcfinancingforum
Related Documents