Epilepsy Epilepsy Presented by : Mohammad Ihmeidan

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EpilepsyEpilepsy
Presented by :Mohammad Ihmeidan
DEFINITIONDEFINITION
A seizure is an abnormal and excessive discharging of the neuroglial network .
Epilepsy is a chronic neurological condition characterized by recurrent, unprovoked seizures.

Seizure Etiology Seizure Etiology
Virtually any insult to the cerebral cortex can cause a seizure.
Most seizures are self-limited, and once the inciting process resolves, the seizures cease.
Synaptic TransmissionSynaptic Transmission
Neuron to neuron communication is mediated by neurotransmitters (NTs) and resultant EPSPs and IPSPs
Excitatory NTs– Glutamate– Aspartate
Inhibitory– GABA– Glycine


Epilepsy etiologyEpilepsy etiology
An epidemiologic study in Rochester, Minnesota reported that :1- the largest percentage of individuals (children and adults) with epilepsy fell into the idiopathic /cryptogenic category (i.e. presumed genetic or unknown etiologies)2- followed in order by vascular, traumatic, developmental ,infectious, neoplastic, and degenerative causes

3-In the under-14-year age group, a developmental etiology was most common (i.e. conditions manifested by mental retardation and/or cerebral palsy presumed to be present from birth )

EpidemiologyEpidemiology
The age-adjusted prevalence of epilepsy in developed countries is 5 per 1,000 population
Epilepsy ClassificationEpilepsy Classification
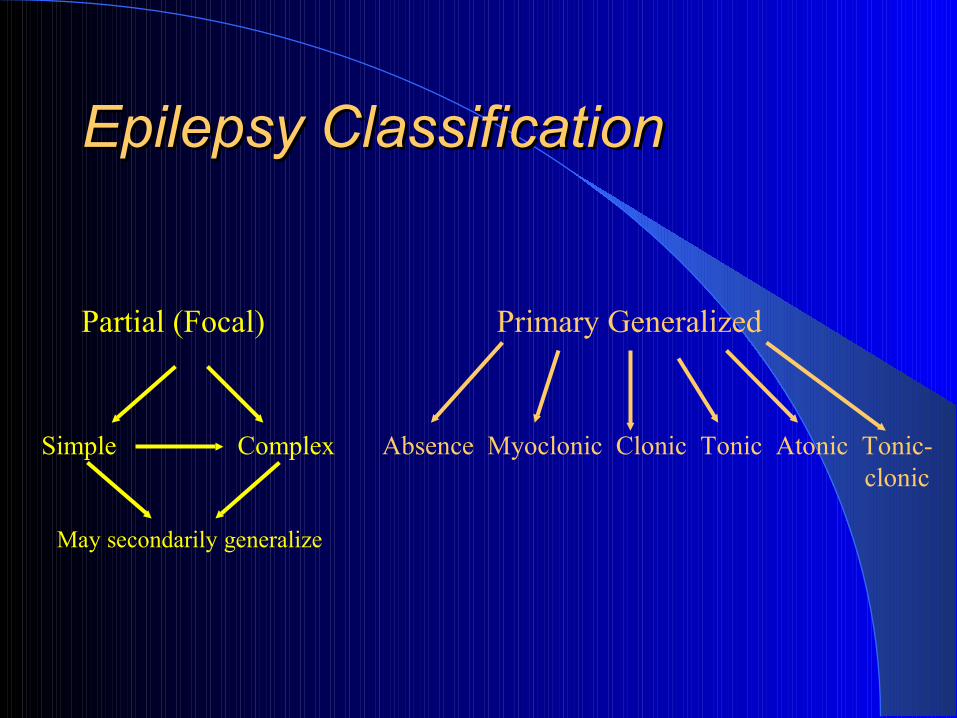
Partial (Focal) Primary Generalized
Simple Complex Absence Myoclonic Clonic Tonic Atonic Tonic- clonic
May secondarily generalize

PARTIAL SEIZUREPARTIAL SEIZURE
Partial SeizurePartial Seizure
originate within networks limited to one hemisphere
Partial or focal seizures constitute 40% to 60% of the classifiable epilepsies of childhood.

Simple PartialSimple Partial
Simple partial seizures arise from a specific anatomic focus.
Clinical symptoms include motor, sensory, psychic, or autonomic abnormalities
consciousness is preserved.
Partial seizures that manifest only with psychic or autonomic symptoms can be difficult to recognize.
Uncinate seizures arising from the medial temporal lobe manifest with an olfactory hallucination of an extremely unpleasant odor (burning rubber).
Limbic temporal lobe discharges result in dreamlike states (déjà vu and bizarre psychic abnormalities).

Video
Complex PartialComplex Partial
Complex partial seizures are similar to simple partial , but in addition, consciousness is impaired

Complex Partial SeizureComplex Partial Seizure
Video

GENERALIZED SEIZUREGENERALIZED SEIZURE
AbsenceAbsence
Brief staring episodes with unresponsiveness Sudden onset with an arrest of activity May have associated eye flutter or simple
automatisms Generalized 3 per second spike and wave usually begin between 4 and 6 years of age 80% will have resolution with age 20% also have convulsive seizures.
absence epilepsy Vs partial complexabsence epilepsy Vs partial complex Differentiating absence epilepsy from partial complex
staring seizures can be difficult. Both seizure types are characterized by cessation of
activity, staring, and alteration of consciousness and may include automatisms.
Partial complex seizures are often followed by postictal confusion; absence seizures are not.
Absence seizures are provoked by hyperventilation and usually last a few seconds; partial complex seizures occur spontaneously and usually last several minutes.
Children may have dozens of absence seizures per day; children rarely have more than one or two partial complex seizures in a day.
The distinction is important because the choice of anticonvulsant treatment is different.

AbsenceAbsence
Video

Generalized Motor (Convulsive)Generalized Motor (Convulsive)
Tonic, clonic, tonic-clonic No warning; abrupt onsetBowel and bladder incontinence are
commonPostictal unresponsiveness or confusionDuring an attack, the EEG shows repetitive
synchronous bursts of spike activity followed by periodic paroxysmal discharges
compose 10% to 15% of childhood epilepsies.
These seizures frequently are associated with underlying structural brain disease and are difficult to treat and classify.
They often occur in combination with each other and with generalized tonic-clonic seizures.
Myoclonic, tonic, atonic, and Myoclonic, tonic, atonic, and atypical absence seizures atypical absence seizures

MyoclonicMyoclonic
Myoclonus is a sudden jerk of all or part of the body; not all myoclonus is epileptic in nature.
Nonepileptic myoclonus may originate in the basal ganglia, brainstem, or spinal cord. It may be benign, as in sleep myoclonus, or indicate serious disease.

Myoclonic epilepsy usually is associated with multiple seizure types.
Myoclonic absence refers to the body jerks that commonly accompany absence seizures and atypical absence seizures.

Myoclonic SeizureMyoclonic Seizure
Video

AtonicAtonic
No warning; abrupt onsetLoss of muscular tone results in sudden fallBrief durationInjuries commonVery difficult to treat

AtonicAtonic
Video

Evaluation of EpilepsyEvaluation of Epilepsy
EEG & Epilepsy– Awake only (≅ 30-40% abnormal)– Awake and asleep (≅ 60-70% abnormal)– Photic stimulation
may induce generalized spike and wave or occipital spikes
– Hyperventilation may induce 3/sec. spike and wave (absence)
Evaluation of EpilepsyEvaluation of Epilepsy
Neuroimaging– Indicated with:
Abnormal neurological exam Focal onset seizures Uncertain if focal or primary generalized onset Onset of seizures after adolescence
– MRI is the gold standard (not CT)– CT is helpful in the acute setting
i.e. persistent alteration of consciousness or abnormal neurologic exam

General Guidelines for General Guidelines for Therapy: Therapy:
Correct classification of seizures leads to correct AED selection
Treat when the benefit of therapy outweighs the risk
Avoid polypharmacyMonotherapy usually results in better
seizure control and less side effects

General Guidelines for General Guidelines for Therapy:Therapy:
Maximize one medication before changing to the second
Treat the patient, not the EEG or the AED level
Use rational polypharmacy when indicated


Alternative Therapy for Alternative Therapy for EpilepsyEpilepsy
Ketogenic diet
Vagus nerve stimulator
Epilepsy surgery
First described by Wilder, Mayo Clinic Bulletin, 1921
Mark 9:29 “This kind can come forth by nothing, but by prayer and fasting.”
Typically reserved for children with severe, debilitating and intractable seizures
4:1 (Fat: Protein + Carbohydrates)– 75-90% of caloric intake as fat
Urinary ketosis 80- 160 millimolar
Ketogenic DietKetogenic Diet

Ketogenic Diet: EfficacyKetogenic Diet: Efficacy
150 children prospectively evaluatedAge range: 4 months - 16 yearsAverage of 410 seizures per monthResults after 1 year:
– 55% remained on the diet– 1/2 had > 50% reduction in seizures– 1/4 had > 90% decrease in seizures
Freeman, Vining, et.al. Pediatrics, December, 1998

Vagus Nerve Stimulator:Vagus Nerve Stimulator:Rule of ThirdsRule of Thirds
1/3 - marked improvement 1/3 - some improvement 1/3 – little/no improvement Potential benefits
– fewer seizures, less severe seizures, shorter recovery period, decreased meds and side effects, less fear and anxiety, more control

Epilepsy Surgery:Epilepsy Surgery:Criteria for ConsiderationCriteria for Consideration
Seizures must be medically intractable
Seizures must be debilitating
There should be no chance for spontaneous resolution

Epilepsy Epilepsy SurgerySurgery Temporal lobectomy
– 75-90% seizure free
Extratemporal lesional resection – 50-75% seizure free
Extratemporal non-lesional resection – < 50% seizure free
Functional hemispherectomy
Corpus callosotomy– Especially for atonic and
brief tonic seizures

Children with EpilepsyChildren with EpilepsySchool IssuesSchool Issues
Children with poor seizure control are more likely to have trouble making friends.
Taking medication at school may be associated with a significant decrease in social and peer relationships. Even in children with self reported good seizure control.

ا ا جزاكم جزاكمخيراخيرا
Related Documents











