Dr. Ramy Mostafa Abdelkader,Msc Clinical fellow in Emergency medicine Case presentation 8/11/2016 Not just back pain

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr. Ramy Mostafa Abdelkader,Msc
Clinical fellow in Emergency medicine
Case presentation
8/11/2016 Not just back pain

Not just back pain

Disclosures
I have no conflict of interest or
disclosure in relation to this
presentation

Learning Objectives
i. Case based discussion about LBP presentations and differential diagnosis
ii. Role of proper imaging in diagnosis
iii. Current Updates In Emergency Medicine management


68 years old female
Known HTN, 30yrs h/o intermittent LBP, 2wks ago
exacerbation of LBP admitted abroad, given NSAIDs, had
MRI LSS showing L3/4 L4/5 disc bulges and discharged,
from 3ds her pain became worse and now she is unable
to move .
What questions would you like to ask
regarding her history?
Patient Presentation to ER



lower limb weakness, loss of sensation plus
urinary retention and burning sensation of 3
days duration.
Till the last week the patient was mobile and
admitted to hospital in her country due to back
pain and got NSAIDs and steroids on regular
basis then discharged .
fell down at home due to Lower Limb loss of
power followed by fever and urinary retention
with drippling.
History continued

Vitals & Measurements T: 36.8 °C (Oral) HR: 72 (Monitored) RR:
19 BP: 130/58 SpO2: 98% WT: 90 kg

Past History
Hypertension
Chronic dermatitis
Chronic low back pain
Family History
Positive in her parents for hypertension
Procedure/Surgical History
Never
Medications
bisoprolol, 5.0 mg, Oral, Daily
celecoxib, 200.0 mg, Oral, BID
valsartan, 160.0 mg, Oral, Daily
Prednisolone 5 mg, Oral , Daily
Allergies
No Known Allergies
Social History
Tobacco
Details: Never smoker

Review of Systems Constitutional: History of fever, No chills.
Respiratory: shortness of breath, No cough, No wheezing.
Cardiovascular: No chest pain, No palpitations.
Gastrointestinal: no nausea, no vomiting, diarrhea, No
heartburn.
Genitourinary: dysuria and urinary urgency. Then developed
anuria
Musculoskeletal: low back pain, no joint pain, muscle pain.
Neurologic: Alert Generalized weakness

Physical Exam General: the patient looks tired and in pain but fully
conscious afebrile and vitally stable
HEENT: No pharyngeal erythema.
Respiratory: Lungs are clear to auscultation.
Cardiovascular: Normal rate, No murmur, Good pulses equal in all extremities.
No pedal edema
Abdomen: Soft, Non-tender .
Back exam: lumbosacral spinal tenderness
P/R exam: normal anal tone
Neurological: sensation lost up to umblicus
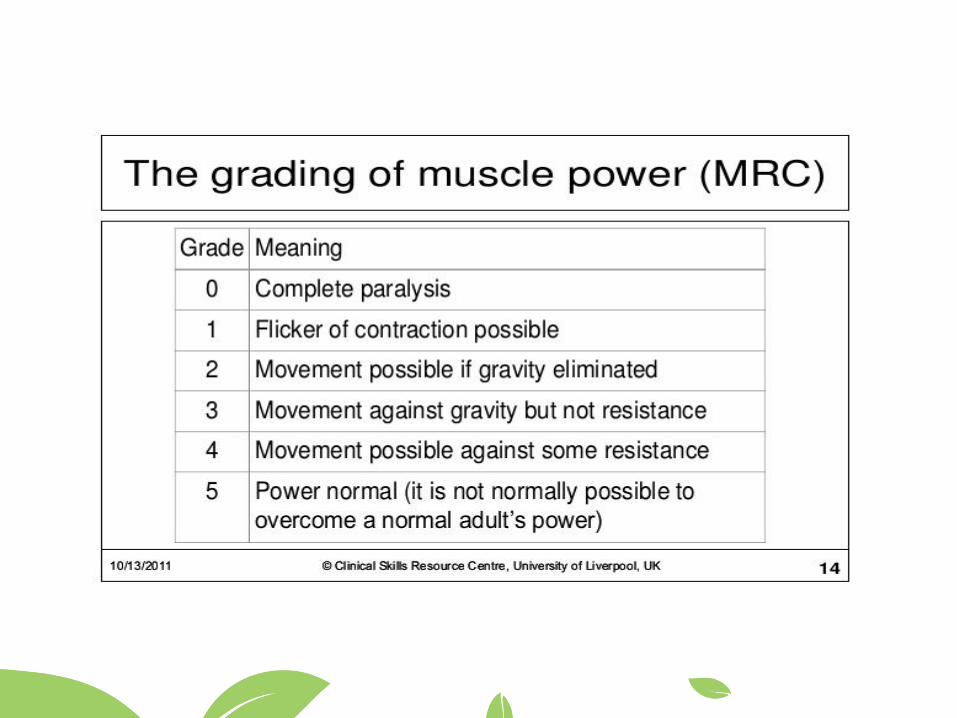
motor power 1/5 in both lower limbs
reflexes -ve
Gait couldn’t be assessed

• POCUS: full bladder and bilateral mild
Hydronephrosis
• Urinary Catheter Insertion
• Urine Microscopy/reflex culture
• Complete blood count
• Complete metabolic panel
• Coagulation profile
• Inflammatory markers
• Septic work up including blood C/S
and CXR
• MRI thoraco-lumbar
spine(with/without contrast?)
• Neurosurgeon consultation
• Start IV antibiotic and adequate
analgesia

Lab Results :
Cr932, Ur51.20, K+6.2, Na130, WBCs16.4,
ESR77, CRP198, bicarbonate 15.6,lactate 2.1
At that time ECG was requested
POC Urine analysis:
+3 RBCs
+3 wbcs
Nitrite +ve


What is your

Working diagnosis
Cauda equine
AKI + hyperkalemia
UTI

What will you do first?
• Patient shifted to Bay 1 (monitoring
for Hyperkalemia?!)/Dialysis line.
• Neurosurgeon want MRI once
patient is stable .
• Nephrologist wants to do
Hemodialysis & official Ultrasound
(ATN from NSAIDS given for pain or
post obstructive Uropathy due
to Urinary retention).

• Hemodialysis was done first (and
once)
• Patient is Delayed disposition as Bay 1
specialist and consultant refused to
admit the patient to AMU as
requested by the nephrologist (in his
notes) Until MRI is done.
• Patient developed fever (38.1 C during
her stay in ED)
• MRI done after 18 hours in ED



MRI reportImpression of the radiologist:
Extensive precontrast T1 hyperintense (subacute blood versus proteinaceous
material like pus) thoracolumbar spinal canal extramedullay collection with distal
spinal cord compression and cord signal change and crowding of cauda equina.
MRI Spine whole
There is T1 hyperintense extramedullary intraspinal collection surrounding the spinal cord which is seen
predominantly anteriorly from C6 to T11 levels and posteriorly from T5 to S2 level. There are also small
posterior loculated areas at T1-T3 on the right side and anterior collections from L4 - S2.
The posterior epidural fat is visualized in many areas where the collection is present and this feature suggest
that the collection is likely subdural in location, but exact differentiation between epidural and subdural is not
really possible in this noncontrast study. Contrast was not given due to severely elevated creatinine and
extremely low GFR
There is spinal cord compression which is most prominent at T11 and T2 levels extending superiorly to T10
and inferiorly to L1 levels. The lower spinal cord shows T2 hyperintensity.
Within the lumbar canal, there is crowding and mild compression of the nerve roots of the cauda equine due to
mass effect from the collection. Cervical spine shows mild degenerative changes most prominent at C5-6 and
C6-7 levels with mild disc bulges and right-sided uncovertebral DJD at C5-6. Mild disc bulges are also seen at
L2-3, L3-4 and L4-5 with slight ventral canal indentation, but not significant.
Multiple incidental hemangiomas are seen most prominent at T4, T7, T8, L3 and S1 levels. No evidence of
vertebral marrow or disc injury or infection.
Impression:
Extensive precontrast T1 hyperintense (subacute blood versus proteinaceous material like pus) thoracolumbar
spinal canal extramedullay collection with distal spinal cord compression and cord signal change and crowding
of cauda equina.

Spinal Epidural abscess
for Urgent intra-operative drainage
• MRI was done but without contrast and showed
long segment spinal epidural collection ( ?abscess)
with a compression mainly anteriorly above D 10
and posteriorly from the level of the 11 and below.
MRI also shows abnormal cord signal (ischemia) at
same levels.
Spinal Epidural AbscessSpinal epidural abscess (SEA) is a collection of pus or inflammatory
granulation between the dura mater and the vertebral column.[1] Currently the
annual incidence rate of SEAs is estimated to be 2.5-3 per 10,000 hospital
admissions. Incidence of SEA is on the rise, due to factors such as an aging
population, increase in use of invasive spinal instrumentation, growing number
of patients with risk factors such as diabetes and intravenous drug use.[1] SEAs
are more common in posterior than anterior areas,[2] and the most common
location is the thoracolumbar area, where epidural space is larger and contains
more fat tissue.[3] SEAs are more common in males, and can occur in all ages,
although highest prevalence is during the fifth and seventh decades of life.[1]

Spinal Epidural Abscess.
Why Care?
Irreversible paralysis in up to 22% of
patients, not because of bacterial
virulence but due to delayed diagnosis.4
50% of patients are initially
misdiagnosed.5 Paralysis lasting greater
than 24 hours is irreversible
Spinal epidural abscess: Intracranial epidural abscess
prevalence is 9:1

Predisposing factors
Trauma,
• prior surgery, or spinal procedures.
• Immunocompromised states
Pregnancy
• Diabetes mellitus (Type I or II)
• Bacteremia: (endocarditis, lung or
abdominal abscess, or previous septic
episodes)
Osteomyelitis
Acupuncture
IV drug use
Alcoholism
Chronic renal failure (Hemodialysis)

• The leading bacterial pathogen causing spinal epidural abscess
(SEA) is S. aureus, which accounts for about two-thirds of cases
caused by pyogenic bacteria
• Various other bacteria can also produce the infection.
• Mycobacterium tuberculosis is a more frequent cause of epidural
abscesses in parts of the developing world 1,2,4,5
Causative Organisms

As the pyogenic inflammation progresses and the
abscess extends longitudinally in the epidural space,
damage to the spinal cord can be caused by one or
more of the following mechanisms 6
●Direct compression
●Thrombosis and thrombophlebitis of nearby veins
●Interruption of the arterial blood supply
●Bacterial toxins and mediators of inflammation
Pathogenesis

DiagnosisThinking of spinal epidural abscess (SEA) is the key to diagnosis.
Is by Classic Triad
• Fever
• Spine pain (local spinal tenderness)
• Neurologic deficit

Differential Diagnosis
• Spinal Radiculopathy /
polyradiculopathy
• Bacterial meningitis.
• Osteomyelitis
• Spinal tumor / spinal hematoma.
• Multiple Sclerosis
• Spinal cord infraction (radiating pain
along involved nerve roots similar to the
pain seen with a spinal abscess.

LABORATORY FINDINGS
— Routine laboratory studies are seldom
helpful in the diagnosis of spinal epidural
abscess (SEA).
ESR is usually elevated in both SEA (90%)
and vertebral osteomyelitis,
the leukocyte count may be elevated or
normal 7

Approach to diagnosis• Magnetic resonance imaging (MRI)
the preferred test is MRI with Contrast because it is often
positive early in the course of the infection
• Computed tomography (CT) scanning with intravenous
contrast is an acceptable alternative to MRI if MRI is not
immediately available9

MANAGEMENTCombination of aspiration, drainage, and antibiotic
therapy
Early consulting the neurosurgeon is
mandated once SEA is suspected.
Appropriate empiric parenteral regimens include:
●Vancomycin for empiric coverage of MRSAPLUS●Either cefotaxime or ceftriaxone

The indications and timing for operative management of spinal epidural abscess: literature
review and treatment algorithm. Neurosurg Focus 37(2):E8:1-8, 2014

Quick Hits on Spinal Epidural Abscesses:
– bacteria can gain access to epidural space via
hematogones spread or direct inoculation into spinal canal
(e.g. during spinal or epidural procedures/surgery)
– risk factors include epidural catheters, diabetes mellitus,
alcoholism, HIV, bacteremia, IVDU
– Staph aureus is responsible for two-thirds of cases
caused by pyogenic bacteria
– MRI is the imaging test of choice for diagnosis; a less
sensitive/specific alternative is CT w/ contrast
– clear indications for urgent surgical interventions include
acute/progressive neurological deficits, spinal instability, or
disease progression despite antibiotics

Any Questions
REFERENCES1. Danner RL, Hartman BJ. Update on spinal epidural abscess: 35 cases and review of the literature. Rev Infect Dis 1987; 9:265.
2. Nussbaum ES, Rigamonti D, Standiford H, et al. Spinal epidural abscess: a report of 40 cases and review. Surg Neurol 1992;
38:225.
3. Pradilla G, Ardila GP, Hsu W, Rigamonti D. Epidural abscesses of the CNS. Lancet Neurol 2009; 8:292.
4. Pfister H-W, Klein M, Tunkel AR, Scheld WM. Epidural abscess. In: Infections of the Central Nervous System, Fourth Edition,
Scheld WM, Whitley RJ, Marra CM. (Eds), Wolters Kluwer Health, Philadelphia 2014. p.550.
5. Darouiche RO, Hamill RJ, Greenberg SB, et al. Bacterial spinal epidural abscess. Review of 43 cases and literature survey.
Medicine (Baltimore) 1992; 71:369.
6. Akalan N, Ozgen T. Infection as a cause of spinal cord compression: a review of 36 spinal epidural abscess cases. Acta Neurochir
(Wien) 2000; 142:17.
7. Kapeller P, Fazekas F, Krametter D, et al. Pyogenic infectious spondylitis: clinical, laboratory and MRI features. Eur Neurol 1997;
38:94.
8. Torda AJ, Gottlieb T, Bradbury R. Pyogenic vertebral osteomyelitis: analysis of 20 cases and review. Clin Infect Dis 1995; 20:320.
9. Gellin BG, Weingarten K, Gamache FW Jr, et al. Epidural Abscess. In: Infections of the Central Nervous System, 2nd Ed, Scheld
WM, Whitley RJ, Durack DT (Eds), Lippincott-Raven Publishers, Philadelphia 1997. p.507.
10. Ju KL, Kim SD, Melikian R, et al. Predicting patients with concurrent noncontiguous spinal epidural abscess lesions. Spine J 2015;
15:95.
11. Sørensen P. Spinal epidural abscesses: conservative treatment for selected subgroups of patients. Br J Neurosurg 2003; 17:513.
12. Ptaszynski AE, Hooten WM, Huntoon MA. The incidence of spontaneous epidural abscess in Olmsted County from 1990 through
2000: a rare cause of spinal pain. Pain Med 2007; 8:338.
13. Park KH, Cho OH, Jung M, et al. Clinical characteristics and outcomes of hematogenous vertebral osteomyelitis caused by gram-
negative bacteria. J Infect 2014; 69:42.
14. Cook TM, Counsell D, Wildsmith JA, Royal College of Anaesthetists Third National Audit Project. Major complications of central
neuraxial block: report on the Third National Audit Project of the Royal College of Anaesthetists. Br J Anaesth 2009; 102:179.
15. Sethna NF, Clendenin D, Athiraman U, et al. Incidence of epidural catheter-associated infections after continuous epidural
analgesia in children. Anesthesiology 2010; 113:224.
16. Pöpping DM, Zahn PK, Van Aken HK, et al. Effectiveness and safety of postoperative pain management: a survey of 18 925
consecutive patients between 1998 and 2006 (2nd revision): a database analysis of prospectively raised data. Br J Anaesth 2008; 101:832.
17. Reynolds F. Neurological infections after neuraxial anesthesia. Anesthesiol Clin 2008; 26:23.
18. Gosavi C, Bland D, Poddar R, Horst C. Epidural abscess complicating insertion of epidural catheters. Br J Anaesth 2004; 92:294;
author reply 294.
19. Centers for Disease Control and Prevention. Injection Safety. http://www.cdc.gov/injectionsafety/ (Accessed on June 24, 2014).

Thank you
Please remember to fill in your evaluation form
Presented by
Dr. Ramy Mostafa Abdelkader, MSc
Clinical fellow in Emergency medicine
Related Documents











