Unintentional Injuries in the African Countries “Overview and Control Challenges” Injury Epidemiology Workshop PEERCORPS Trust Fund in collaboration with The IPIFA/WHO Dar Es Salaam , Tanzania July 3-5, 2009 Hesham El-Sayed Faculty of Medicine Suez Canal University, Egypt

Epidemiology of Unintentional Injuries in the African Countries ...
May 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Epidemiology of Unintentional Injuries
in the African Countries“Overview and Control
Challenges”Injury Epidemiology Workshop
PEERCORPS Trust Fund in collaboration with The IPIFA/WHO
Dar Es Salaam , TanzaniaJuly 3-5, 2009
Hesham El-SayedFaculty of Medicine
Suez Canal University, Egypt
Global Burden of Injuries
Injuries caused 5 million deaths worldwide >9% of all deaths (2000)
Injuries are the leading causes of death in children <18 years of age.
Injuries caused 875,000 deaths among children (<18 years) in the year 2000 (40/100,000).
More than 90% of injury deaths occur in low- and middle-income countries.

Global Burden of Injuries (2)
45 injuries need hospital admission and 1300 injuries requiring ambulatory care for every injury death.
Injuries represent 15-24% of all hospital admissions.
Injuries responsible for >12% of global burden of disease (DALYs).

75%
50%
25%
Africa AmericasEastern
MediterraneanEurope
South EastAsia
WesternPacific
Deaths, by Broad Cause Group & WHO Region, 2001
Communicable diseases, maternal and perinatal conditions and nutritional deficiencies
Noncommunicableconditions
Injuries
Source: WHR 2002


Global Injury Rates by Age Groups
0-4 5_14 15-44 45-69 70+0
50
100
150
200
250
300
Age Group
Per
10
0,0
00
Pop
ula
tion
WHO, 2002

Global Causes of Injury Mortality
RTI
Poisoning
Falls
Burns
Drowning
Violence
Others
Chart Title
Global Injury Mortality (WHO, 2002)

RTI Global Fatalities

1987 1988 1989 1990 1991 1992 1993 1994 1995-20
-10
0
10
20
30
40
50
60
Highly Motorised Countries Latin America & Carribean
Africa Middle East & North Africa
% c
hang
e si
nce
1987
Global Road Fatality Trends

10Source: WHO. Injury – A leading cause of the global burden of disease. . WHO, 2002
DISABILITY ADJUSTED LIFE YEARS (DALYS) LOST DUE TO ROAD TRAFFIC INJURIES, MALES, 2000

Injuries due to Unintentional Falls

Fire-related Burns

Drowning injuries
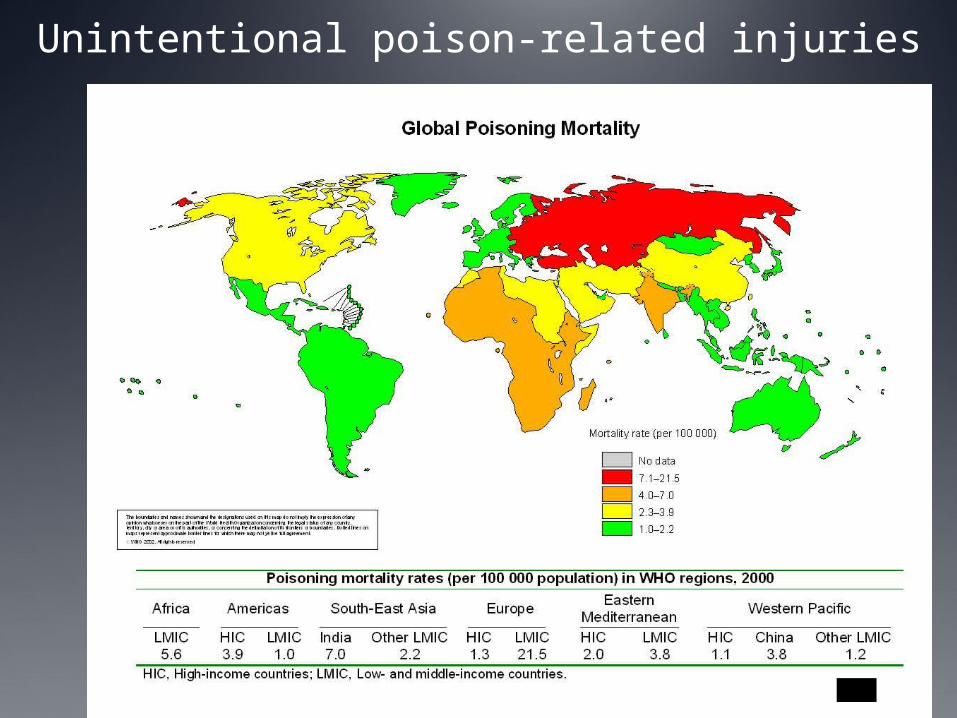
Unintentional poison-related injuries

Sources of Injury Information “National records from various sources”
Death certificates Hospital records Trauma registries Case reports (Media) Epidemiological studies Police data Industrial reports Bureau of crime records NGO’s reports

Factors Affecting the Prevalence and Pattern of
Injuries
Age.
Gender (Male/Female Ratio [2-3/1]).
Fatal vs. Nonfatal injuries.
Residence: Region, Country, Urban vs. Rural.
Socioeconomic conditions (poverty/equity).
Community vs. health facilities and vital statistics data.

Strengths & Weaknesses of Injuries Records in the African Countries
Poor recording system in most of the health facilities and even in tertiary and secondary hospitals (El-Sayed et.al., 2001).
Under-registration of RTI is 46% in vital statistics of Ministry of Health, and 57% in traffic police records (Verbal Autopsy Studies, El-Sayed et.al., 1992 & Khallaf et.al, 1996).
Newly developed injury surveillance programs that started in the some countries (Egypt).
Injury surveys conducted in some countries.
Why limited action against injuries?
Perception of injuries as “Accidents” unpredictable and inevitable.
Reluctance of health professionals to accept that injury prevention is science (work with other sectors).
Lack of ownership (multi-sectoral complexity). Media focus on key events rather than on
relentless daily loss & prefer high technology medicine.
Challenges to powerful vested interests (motor vehicle industry, firearms, big industries).

Why limited policy response to injuries?
Relative neglect, due to Limited awareness of the burden & little evidence of response.
Limited awareness of what can be done. Limited availability of data necessary for
making decisions. (cost, sequences, perception).
Limited public health capacity to highlight the problem, and media focus on key events rather than on relentless daily loss .
Limited resources. Minimal links between society organizations
(e.g., NGOs) and public health community.

Scope for the Response to Injuries
Change thinking about injuries to scientific approach as preventable health problem.
Scientific bases for injury prevention: Structural framework of time and vector, host
and environment (Haddon’s matrix).
Risk response: Health education & works with legislation.
Public Health Approach: Surveillance, risk factors, interventions &
implementation.

Steps of Developing Injury Control Program
1. Identify size of the injury problem.2. Determine specific circumstances of injury
(risk factors).3. Identify possible preventive measures.4. Based on local evidence and research.5. Taking into account existing social, political, and
economic considerations.6. Prioritize intervention programs:
(size of the problems, likelihood of success, constraints, additional benefits).
7. Implement interventions.8. Evaluate intervention effects.

Essential Features of Successful Injury Control
Program
Data collection & Analysis
Plan goals & Interventions
ImplementInterventio
ns
Monitoring &
Evaluation
Priority Setting Criteria
Overall impact of priority setting process on equity.
Answerability in an ethical way.
Likelihood of efficacy and effectiveness of interventions affected by new knowledge.
Likelihood of deliverability, affordability and sustainability.
Maximum potential of reduction of existing disease burden.* Child Health and Nutrition Research Initiative

Steps of Research Utilization
Problem Identification
Dissemination
Research Design
Implementation
Utilization
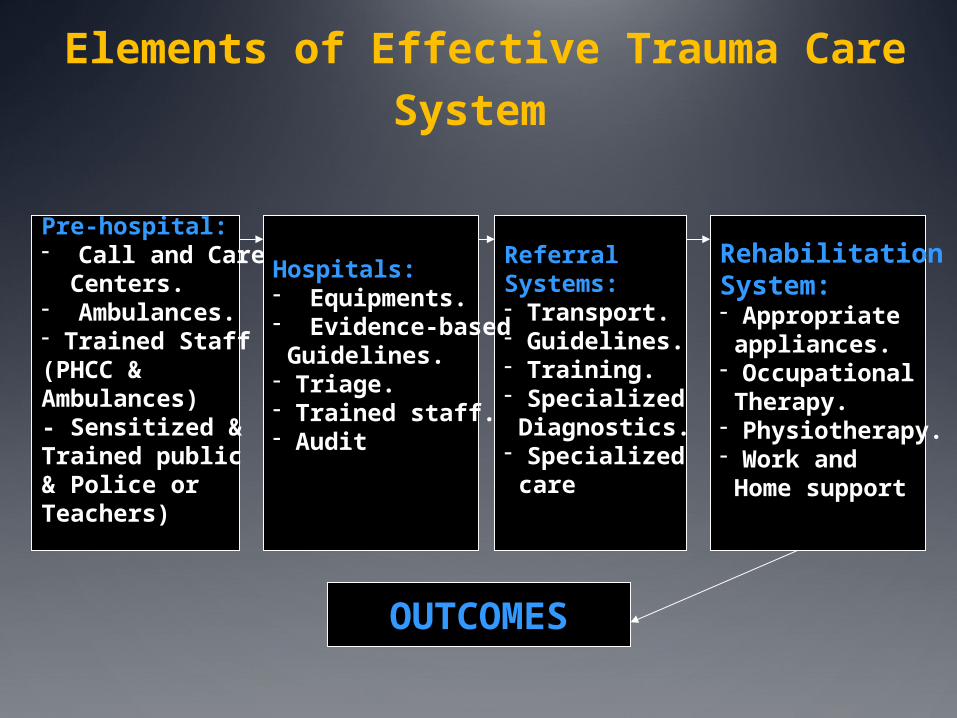
Elements of Effective Trauma Care System
Pre-hospital:- Call and Care Centers.- Ambulances.- Trained Staff(PHCC & Ambulances)- Sensitized &Trained public& Police orTeachers)
ReferralSystems:- Transport.- Guidelines.- Training.- Specialized Diagnostics.- Specialized care
RehabilitationSystem:- Appropriate appliances.- Occupational Therapy.- Physiotherapy.- Work and Home support
Hospitals:- Equipments.- Evidence-based Guidelines.- Triage.- Trained staff.- Audit
OUTCOMES
Intervention Strategies for Injury Control
Education.
Legislation, regulations and enforcement
Product modification.
Environmental modification.
Supportive home visiting.
Community-based studies.

Global Response to the Injury Problem
Increasing recognition of injuries as priority health problem, especially RTI.
Acknowledgement of injury targets in MOHP and Universities programs.
Recognition of injuries as manifestation of inequalities (political pressure).
Working with International Organizations:MOHP/WHO/EMRO RTI Health Days , Injury
Surveillance Programs, International Injury Control Meetings, IPIFA, Safe Community projects, NGOs.)
But limited action & Few additional resources.

Recommendations for Injury Control Strategies
Based on local evidence and research.
Taking into account existing social, political, and economic considerations.
Legislations that should:Convince the public.Enforcement, swiftness and severity..
Attitude of law enforcement personnel.
Recommendations (Cont.) for Injury Control
Training of medical staff and the public on injury care:Train all hospitals medical staff
including physicians, nurses, and paramedics.
Train PHC physicians, nurses, and paramedics.
Training of the public and first respondents (i.e., Policemen, teachers, drivers).

Recommendations (Cont.) for RTI control strategies
Address special factors:Urban development.Vulnerable road users:
Pedestrians especially children and older people.
Two wheelers users (bicycles, motorcycles, etc.).
Public transport.Poor communities (equity challenges).

African Activities for Injury Control


WHO/CNIS Teach Injury Epidemiology Workshop (Kampala-Uganda 2009)

Injury Control Activitiesin Egypt

Egypt Activities for Injury Control
Establishing MOHP Injury Registry Program.
Training medical professionals and health workers on registration and data management.
Training primary health care workers on Injury control and prevention programs (Golden Hour in Trauma Care, WHO/EMRO).
Universities and MOH programs and courses for Emergency and Injury care (ATLS, ACLS).
Childhood injury registry project (WHO )
Safe-Community Program in Port-Said city.

Egyptian Activities for RTI Control
New more stringent traffic law.
National campaign on RTI by MOHP (1997).
Decree for free emergency care by private and investment hospitals.
Establishing emergency medical centers along highways.
Establishing the National Council for Traffic Safety.

Efforts for Injury Control in the EMRO Region
“The Golden Hour in Trauma Care”
Injury Control Program in Ismailia Schools, Egypt

Road Traffic Injury Control Seminar Cairo, Egypt (May 18,
2007)

Related Documents











