EPIDEMIOLOGY OF TUBERCULOSIS Presented by :Dr Saundarya Guided by :Dr Hemant Kumar Department of Community Medicine AJIMS &RC Mangalore ,Karnataka

Epidemiology of tuberculosis
Aug 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EPIDEMIOLOGY OF TUBERCULOSIS
Presented by :Dr SaundaryaGuided by :Dr Hemant Kumar
Department of Community Medicine AJIMS &RC Mangalore ,Karnataka
04/18/2023 2A Tribute of Robert Koch
04/18/2023 3
INTRODUCTION Tuberculosis (TB) -
Infectious bacterial disease caused by Mycobacterium tuberculosis - most commonly affects the lungs.
Transmitted from person to person via droplets from the throat & lungs of people with the active respiratory disease.
04/18/2023 4
HISTORYConsumption, phthisis, scrofula, Pott's
disease, and the White Plague are all terms used to refer to tuberculosis throughout history.
It is generally accepted that the microorganism originated from other, more primitive organisms of the same genus Mycobacterium
Researchers theorize that humans first acquired it in Africa about 5,000 years ago
04/18/2023 5
HISTORY
Hippocrates, in Book 1 of his Of the Epidemics, describes the characteristics of the disease: fever, colorless urine, cough resulting in a thick sputa, and loss of thirst and appetite
He notes that most of the sufferers became delirious before they succumbed to the disease
Hippocrates and many other at the time believed phthisis to be hereditary in nature
Aristotle disagreed, believing the disease was contagious.
04/18/2023 6
CONT.
1865- Jean-Antoine Villemin proved TB is contagious
1882- Robert Koch discovers M.tuberculosis
1884- First TB sanatorium established in U.S
1943- Streptomycin- a drug to treat TB was discovered
1943-1952- Two more drugs discovered to treat TB – INH & PAS
Mid 1970s- most TB sanatoriums in U.S closed

04/18/2023 7
FATHER OF MODERN TB EPIDEMIOLOGY
Karel Styblo, MD, (1921 – 13 March 1998) was born in Czechoslovakia.
Internationally renowned for his work with tuberculosis (TB) - medical advisor to the Royal Netherlands Tuberculosis Association - director of the International Union Against Tuberculosis and Lung Disease (IUATLD) in Paris from 1979
Known as the “Father of modern TB epidemiology" and the "father of modern TB control"

04/18/2023 8
BURDEN
GLOBALLY
In 2013, mortality of TB including HIV was 16 per lakh cases
Mortality of TB excluding HIV was 5 per lakh cases
Prevalence of TB was 159 per lakh
Incidence of TB was 80 per lakh
904/18/2023
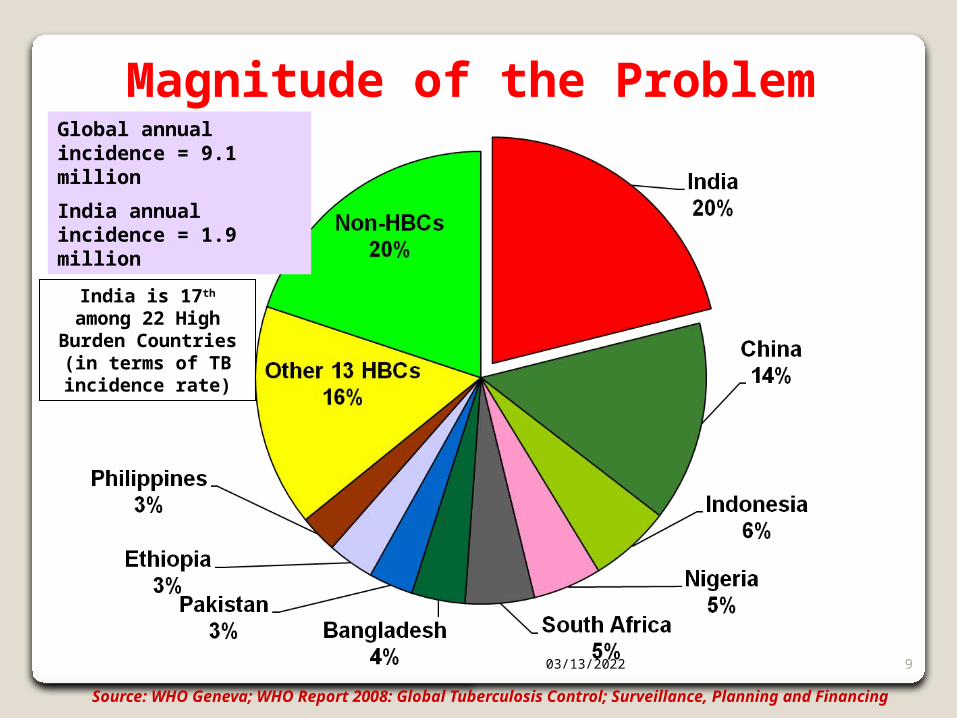
Magnitude of the Problem
Source: WHO Geneva; WHO Report 2008: Global Tuberculosis Control; Surveillance, Planning and Financing
Global annual incidence = 9.1 million
India annual incidence = 1.9 million
India is 17th among 22 High Burden
Countries (in terms of TB incidence rate)
04/18/2023 10
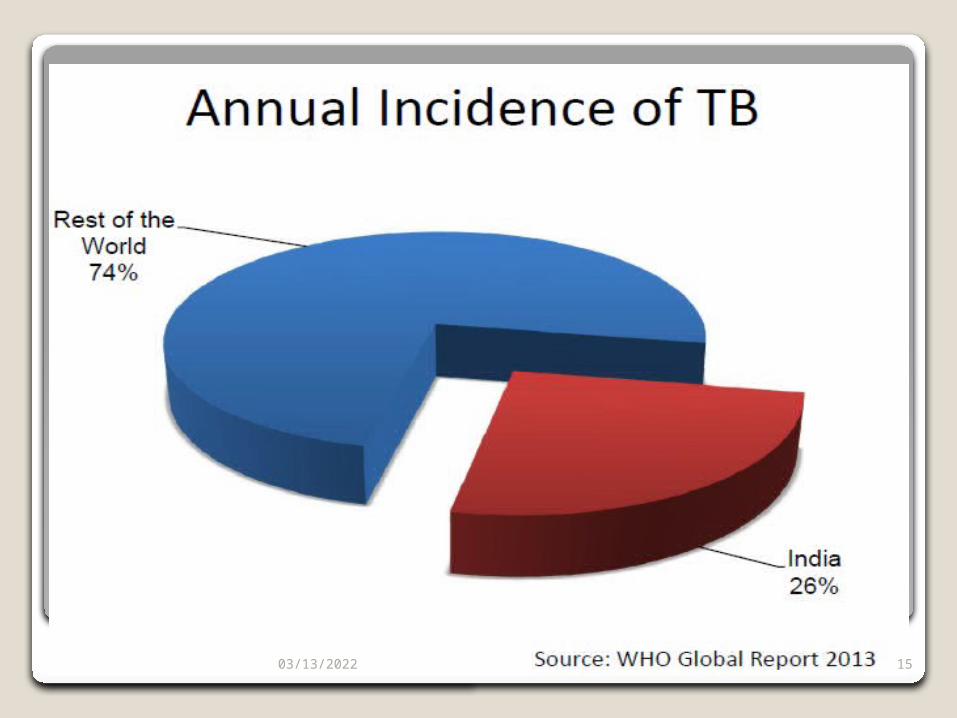
INDIAIndia is the highest TB burden country in the world & accounts for nearly 1/5th (20 per cent) of global burden of tuberculosis, 2/3rd of cases in SEAR.
04/18/2023 11
Contd… Estimated incidence
◦1.96 million new cases annually◦0.8 million new smear positive cases annually◦75 new smear positive PTB cases/1lakh
population per year Estimated prevalence of TB disease
◦3.8 million bacillary cases in 2000 ◦1.7 million new smear positive cases in 2000
Estimated mortality◦330,000 deaths due to TB each year◦Over 1000 deaths a day◦2 deaths every 3 minutes
Prevalence of TB infection ◦40% (~400m) infected with M. tuberculosis
(with a 10% lifetime risk of TB disease in the absence of HIV)
Estimated Multi-drug resistant TB◦< 3% in new cases◦12% in re-treatment cases
TB-HIV◦~2.31 million people living with HIV (PLWHA)◦10-15% annual risk (60% lifetime risk) of
developing active TB disease in PLWHA◦Estimated ~ 5% of TB patients are HIV infected
04/18/2023 12
04/18/2023 13

04/18/2023 14
1504/18/2023
04/18/2023 16
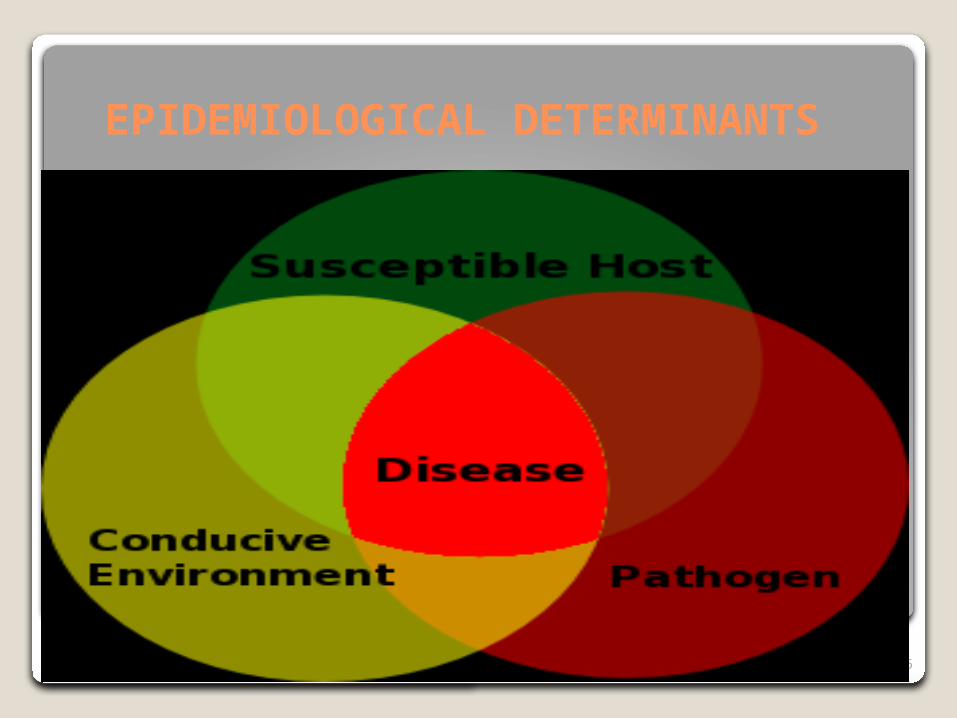
EPIDEMIOLOGICAL DETERMINANTS
04/18/2023 17
Goal 6: “Combat HIV/AIDS, malaria and other diseases”◦Target 8: “By 2015, to have halted and begun
to reverse the incidence of malaria and other major diseases…” Indicator 23: between 1990 and 2015 to halve
prevalence of TB disease and deaths due to TB Indicator 24: to detect 70% of new infectious
cases and to successfully treat 85% of detected sputum positive patients
Millennium Development Goals
04/18/2023 18
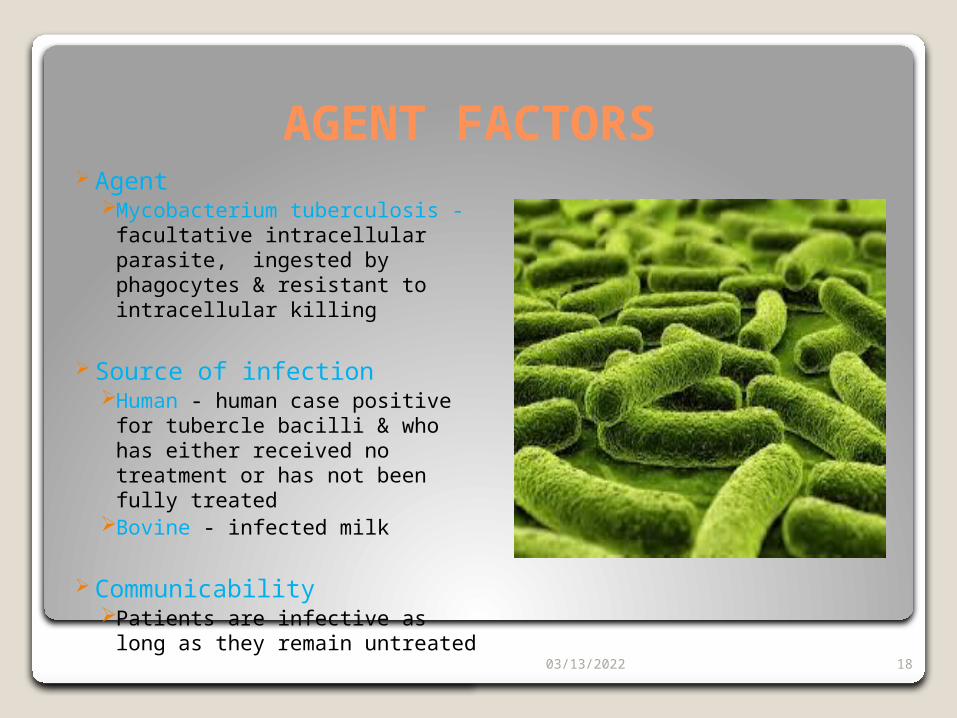
AGENT FACTORS Agent
Mycobacterium tuberculosis - facultative intracellular parasite, ingested by phagocytes & resistant to intracellular killing
Source of infectionHuman - human case positive
for tubercle bacilli & who has either received no treatment or has not been fully treated
Bovine - infected milk
CommunicabilityPatients are infective as long as
they remain untreated
04/18/2023 19
HOST FACTORS Age, Affects all ages
In India, 0-14 age group – 2% 15-24 age group - 20%
Sex,More prevalent in males
Nutrition,Malnutrition – predisposes to TB
Immunity,Man has no inherited immunity against TB
04/18/2023 20
Social factorsTB is a social disease with medical aspects, also
known as barometer of social welfare
Social factors include poor quality of life, poor housing, overcrowding, population explosion, undernutrition, lack of education, large families, & lack of awareness of causes of illness
All these factors are interrelated & contribute to the occurrence & spread of TB

04/18/2023 21
MODE OF TRANSMISSIONTransmitted mainly by
droplet infection and droplet nuclei – by sputum-positive patients with pulmonary TB
Coughing generates the largest number of droplets of all sizes
Frequency & vigour of cough & the ventilation of the enviroment influence transmission of infection
04/18/2023 22
Incubation periodTime from receipt of infection to the
development of a positive tuberculin test ranges from 3 to 6 weeks
Development of disease depends upon the closeness of contact, extent of disease & sputum positivity of the source
Incubation period may be weeks, months or years
04/18/2023 23
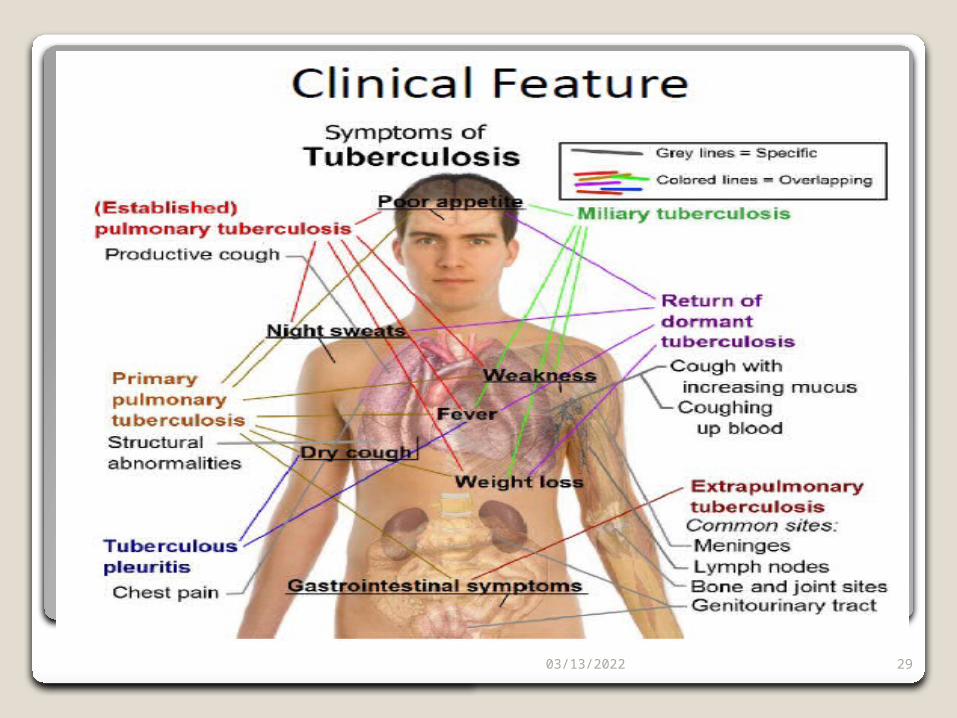
TYPES OF TB Pulmonary,
In active cases – most commonly involves the lungs (90% cases)
Symptoms – Chest pain & a prolonged cough producing sputum
About 25% of people - asymptomatic Extra pulmonary,
In 15–20% of active cases, the infection spreads outside the lungs, causing other kinds of TB
More commonly in immunosuppressed persons and young children
04/18/2023 24
CONT.
Extrapulmonary tuberculosis,
Common sites areMeninges Lymph nodesBones & joints Intestine Genitourinary tract
04/18/2023 25
CONT.
A potentially more serious, widespread form of TB - "disseminated" TB - commonly known as Miliary Tuberculosis.
Miliary TB -10% of extrapulmonary cases
04/18/2023 26
PATHOGENESIS
04/18/2023 27
04/18/2023 28
04/18/2023 29

04/18/2023 30
CLINICAL FEATURES
•Coughing that lasts two or more weeks•Coughing up blood•Chest pain, or pain with breathing or coughing•Unexplained weight loss•Fatigue•Fever•Night sweats•Chills•Loss of appetite
Signs and
symptoms of active
Tuberculosis
04/18/2023 31
CHILDHOOD TUBERCULOSIS WHO estimates(2013) – Upto 80,000 children die from
TB each year & children account for over half a million new cases annually.
Estimated deaths only include – HIV-negative children
Actual burden of TB in children is likely higher, especially given the challenge in diagnosing childhood TB
04/18/2023 32
CONT.Children with TB,
Poor familiesLack of knowledge about the diseaseLive in communities with limited access to health
services
04/18/2023 33
HIV & TBPeople living with HIV – 26 to 31 times more likely
to develop TB than persons without HIV
TB - Most common presenting illness Among people living with HIVAmong those taking antiretroviral treatmentIt is the major cause of HIV-related death.
Sub-Saharan Africa – dual epidemic, accounting for approximately 78% of the estimated burden in 2013

04/18/2023 34
COLLABORATIVE TB/HIV ACTIVITIES
To address HIV-related TB, WHO recommends a 12 point package of collaborative TB/HIV activities.
Objectives,Reducing burden of TB among people living with HIVReducing burden of HIV among TB patients.
Implementation of these activities from 2005 to 2011 – Saved 1.3 million lives
Universal access to these life-saving measures must be achieved & eliminate HIV-associated TB deaths
04/18/2023 35
MDR-TB Multi-drug-resistant tuberculosis (MDR-TB) is defined
as – tuberculosis that is resistant to at least isoniazid (INH) and rifampicin (RMP),the two most powerful first-line treatment anti-TB drugs
When the course of antibiotics is interrupted – levels of drug in the body are insufficient to kill 100% of bacteria
Spread from person to person as readily as drug-sensitive TB and in the same manner
04/18/2023 36
CONT.
Most commonly develops in the course of TB treatment,
Inappropriate treatmentMissing doses or Failing to complete their treatment
Multidrug-resistant strain can transmit TB if pathogens are alive & patient coughing
TB strains –often less fit & less transmissible & outbreaks occur more readily in people with weakened immune systems (HIV)
04/18/2023 37
PREVENTION OF DRUG RESISTANCE TB
Rapid diagnosis & treatment of TB:
• One of the greatest risk factors, especially in developing countries• If TB is identified & treated soon, drug resistance can be avoided.
Completion of treatment:
• Previous treatment of TB is an indicator of MDR TB. • Incomplete antibiotic treatment, or improper prescription of antibiotic regimen – resistance can develop. • Drugs that are of poor quality or less in quantity, especially in developing countries contribute to MDR TB
04/18/2023 38
Patients with HIV/AIDS should be identified & diagnosed as soon as possible. They lack the immunity to fight the TB infection & are at great risk of developing drug resistance.
Identify contacts who could have contracted TB: i.e. family members, people in close contact, etc.
Much research and funding is needed in the diagnosis, prevention and treatment of TB and MDR TB
PREVENTION OF DRUG RESISTANCE TB
04/18/2023 39
EXTENSIVELY DRUG RESISTANT
XDR-TB is defined as TB that has developed resistance to at least rifampicin and isoniazid , as well as to any member of the quinolone family and at least one of the following second-line anti-TB injectable drugs:
KanamycinCapreomycinAmikacin
04/18/2023 40
CONT. If TB bacteria are found in the sputum – diagnosis of TB can be made in a
day or two, but can’t distinguish bet. drug-susceptible & drug-resistant TB.
To evaluate drug susceptibility, bacteria need to be cultivated & tested in a suitable laboratory. Final diagnosis in this way for TB, & especially for XDR-TB, may take from 6 to 16 weeks
The original method used to test for MDR-TB & XDR-TB – Drug Susceptibility Testing (DST).
DST is capable of determining how well four primary ATT drugs inhibit the growth of Mycobacterium Tuberculosis
04/18/2023 41
PREVENTION & CONTROL OF TUBERCULOSIS
04/18/2023 42
Prevention & controlPrimary prevention- health education &
specific protection ◦Population strategy & high risk strategy
Secondary prevention- early diagnosis & specific treatment
Tertiary prevention- rehabilitation & disability limitation
04/18/2023 43
PREVENTION & CONTROL OF TB
Early diagnosis and treatment, particularly of sputum smear positive cases – cornerstone of tuberculosis control
The Revised National Tuberculosis Control Programme (RNTCP) has focused on achieving high cure rates
The protective efficacy of BCG has ranged between 0 to 80% in different studies
04/18/2023 44
BCG-VACCINEThe first human was vaccinated by the
intradermal technique in 1927BCG is the only widely used live bacterial
vaccine. It consists of living bacteria derived from an attenuated bovine strain of tubercle bacilli
The WHO has recommended the "Danish 1331" strain for the production of BCG vaccine
Since January 1967, the BCG Laboratory at Guindy, Chennai, has been using the "Danish 1331" strain for the production of BCG vaccine
04/18/2023 45
CONT..
There are two types of BCG vaccine - the liquid (fresh) vaccine and the freeze dried vaccine.
For vaccination. the usual strength is 0.1 mg 0.1 ml volume. The dose to newborn aged below 4 weeks is 0.05 ml.
04/18/2023 46
RNTCPNeed for a Revised Strategy India has had an on-going National TB Program, NTP
since 1962. Program reviews showed that only 30% of estimated tuberculosis patients were diagnosed & treated successfully.
Based on the findings & recommendations of the review in 1992, the GOI evolved a revised strategy and launched the Revised National TB Control Programme (RNTCP) in the country.
04/18/2023 47
COMPONENTS OF RNTCP
The directly observed treatment, short-course DOTS strategy along with the other ingredients of the Stop TB Partnership are implemented as a comprehensive package for TB control.
04/18/2023 48
FIVE PRINCIPAL COMPONENTS OF DOTS
Political and administrative commitment
Case detection by sputum smear microscopy
Uninterrupted supply of high-quality anti-TB drugs
Standardized treatment regimens with directly observed treatment for at least the first two months
Systematic monitoring and accountability
04/18/2023 49
MANTOUX TEST The Mantoux test OR Mendel-Mantoux test OR the Mantoux
screening test OR tuberculin sensitivity test OR Pirquet test OR PPD test for purified protein derivative-screening tool for TB
Tuberculin is a glycerol extract of the tubercle bacillus. PPD tuberculin -precipitate of species-nonspecific molecules obtained from filtrates of sterilized, concentrated cultures
A standard dose is 5 tuberculin units (TU - 0.1 ml) is injected intradermally (between the layers of dermis) and read 48 to 72 hours later
04/18/2023 50
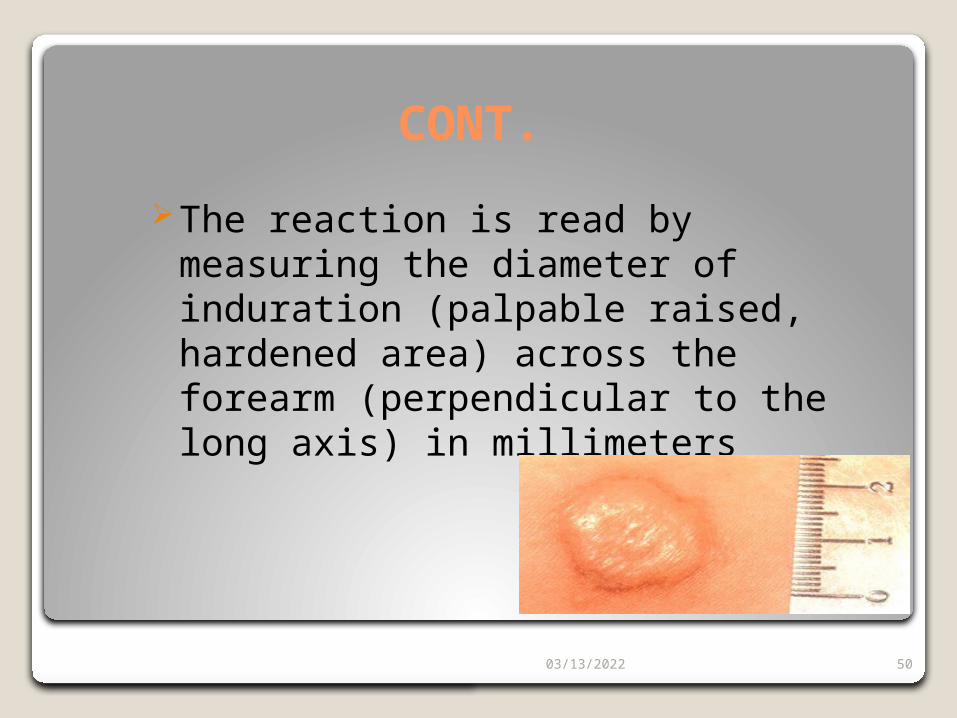
CONT.
The reaction is read by measuring the diameter of induration (palpable raised, hardened area) across the forearm (perpendicular to the long axis) in millimeters
04/18/2023 51
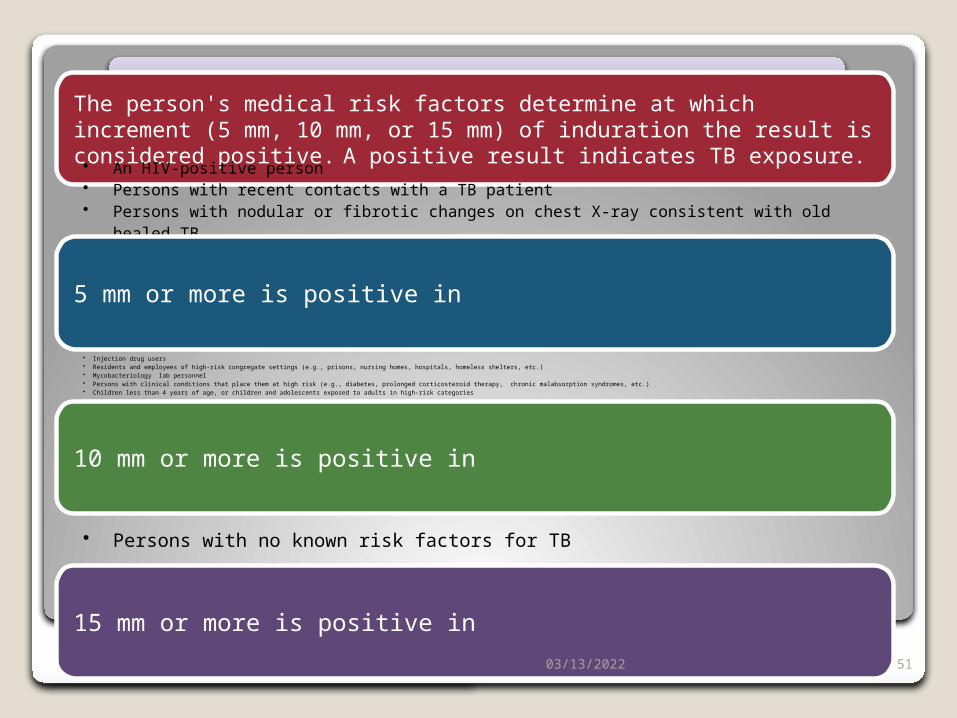
CLASSIFICATION OF TUBERCULIN REACTIONThe person's medical risk factors determine at which increment (5 mm, 10 mm, or 15 mm) of induration the result is considered positive. A positive result indicates TB exposure.• An HIV-positive person• Persons with recent contacts with a TB patient• Persons with nodular or fibrotic changes on chest X-ray consistent with old healed TB• Patients with organ transplants, and other immunosuppressed patients
5 mm or more is positive in
• Injection drug users• Residents and employees of high-risk congregate settings (e.g., prisons, nursing homes, hospitals, homeless shelters, etc.)• Mycobacteriology lab personnel• Persons with clinical conditions that place them at high risk (e.g., diabetes, prolonged corticosteroid therapy, chronic malabsorption syndromes, etc.)• Children less than 4 years of age, or children and adolescents exposed to adults in high-risk categories
10 mm or more is positive in
• Persons with no known risk factors for TB
15 mm or more is positive in
04/18/2023 52
STOP TB STRATEGY
• DOTS expansion & enhancement • Addressing TB/HIV, MDR - TB &
other challenges• Contributing to health system
strengthening• Engaging all care providers • Empowering patients & communities• Enabling & promoting research
STOP TB STRATE
GY6 Major compone
nts
04/18/2023 53
SUMMARYDespite all these national programmes &
efforts from govt of India , TB still continues to be a major socio-economic burden of the country
Still there is need to create awareness among health care professionals, and the community

04/18/2023 54
Related Documents