Epidemiology of Epidemiology of gastric and duodenal gastric and duodenal ulcers ulcers Sarah Bowman April 2008

Epidemiology of gastric and duodenal ulcers Sarah Bowman April 2008.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Epidemiology of gastric and Epidemiology of gastric and duodenal ulcersduodenal ulcers
Sarah Bowman
April 2008

What is an ulcer?What is an ulcer?
• Acid breaks through protective substances on gut wall
• Duodenum (1st part small intestine) – most common site
• “Gastric” ulcers – in stomach
Pain, bloating, nausea, “fullness”, weight loss, tiredness
Complications: bleeding, perforation, obstruction

DiagnosisDiagnosis
• Endoscopy (>55yrs, first time). Capture all cases?• Faecal / breath tests for H. pylori• GI series (rare)
False positive tests
Missed cases? – risk of transmission / disease progression
Why are they important?Why are they important?
• HPA – “infectious disease” but main effects are from chronic burden
• Potential “medical emergency”• Chronic symptoms – health and economic costs• H. pylori also linked to:
– Functional dypepsia– Cancer (2-6x more likely, though still rare)
• Differential clinical outcome - interaction between bacterial properties (phenotypic variation), genetics and environmental / behavioural factors
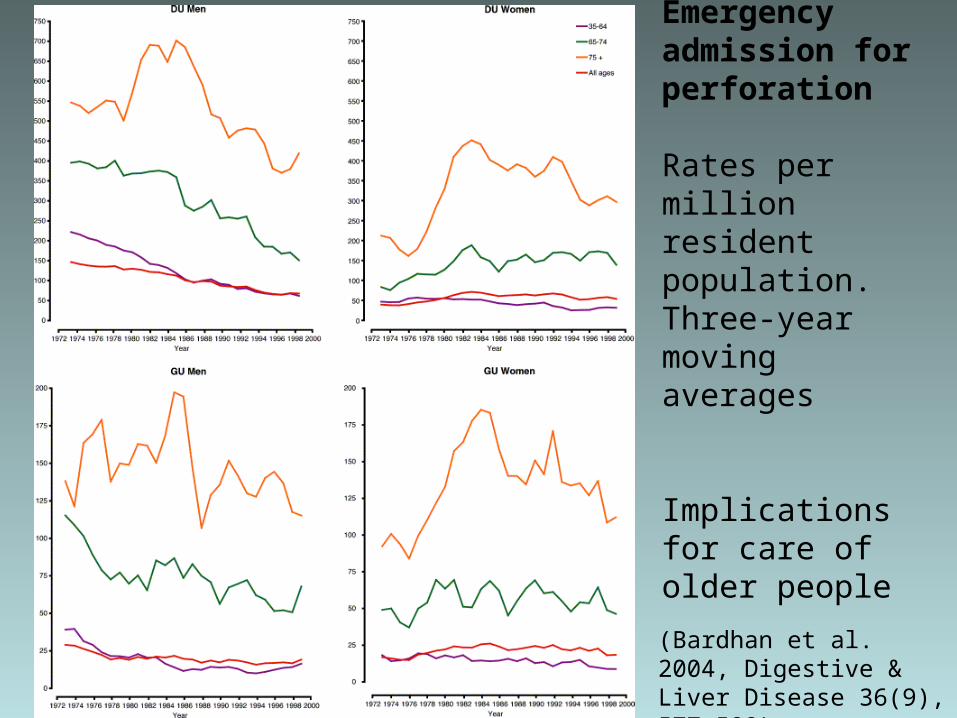
Emergency admission for perforation
Rates per million resident population. Three-year moving averages
Implications for care of older people
(Bardhan et al. 2004, Digestive & Liver Disease 36(9), 577-588)
Causes?Causes?
Ulcers are only found in white people, usually in long thin types given to worry and irritability (Robinson & Bruce 1940)
• Helicobacter pylori
– 90% duodenal ulcers
– 70-75% gastric ulcers
• NSAIDs
• Lifestyle factors increase risk – smoking, physical stress, salt (GU)
• Genetic susceptibility / protection against H. pylori infection (twin studies, mouse models)
• Rarely…Zollinger-Ellison syndrome & others
Causes & Risk FactorsCauses & Risk Factors

Treatment & Outcome (NICE)Treatment & Outcome (NICE)
• 10% cases fail treatment (HPA)• 1 course of combination therapy clears most cases (74%
duodenal ulcers)• Relapse greater for gastric ulcers (affected by lifestyle
factors). At 3-12 months:– Duodenal ulcers: 39% clear (acid suppression only);
91% (combination therapy)– Gastric ulcers: 45% clear (acid suppression only);
77% (combination therapy)

ConsequencesConsequences
• Primary care – GP consultations, drug costs (increasing resistance)
• Secondary care – complications, surgery
• Tertiary care – rarely needed
• Socio-economic cost: Standardised average annual years of life lost (up to age 75) = 2.6 (per 10,000) (Females=1.8; Males=3.5) (1999 & 2001 pooled data, ONS)

Consequences…Consequences…
• “Mass eradication of H pylori is impractical because of…generating antibiotic resistance, so we need to know how to target prophylaxis.” (Calam & Baron 2001)
• Ulcers occurring in absence of H. pylori or NSAIDs /
aspirin. Combination therapies less effective in absence of H. pylori – data needed
• Screening? Cost-effective cost/LYS < £10,000 over 80yrs. But effects of eradication on morbidity / mortality?

Time, Person, Place…Time, Person, Place…

Barron & Sonnenberg (2002)
UK Incidence & Prevalence (Time)UK Incidence & Prevalence (Time)
Increases due to:
• Increase in H.pylori?
• Different strain of H. pylori?
• Another concurrent gut infection?
But what about differing temporal changes of CU and DU and between men and women?

UK Incidence & Prevalence (Time)UK Incidence & Prevalence (Time)
Evidence of cohort effect 1970-1986: (Primatesta et al. 1994)
• Decreased hospitalized morbidity and mortality• Related more to changes in risk factors (e.g. smoking) in
different cohorts than new pharmacological treatments? - implications for public health!
OR: Genetic factors may be more important (Malaty et al. 1994)

UK Incidence & Prevalence UK Incidence & Prevalence (Person)(Person)
H. pylori infection• Incidence: 1-3% of adults p.a. (HPA)• Prevalence infection: 40% population (HPA: >50% of
50+yr olds)
Ulceration•Incidence:
–DU in 30-50yrs old; higher incidence in men –GU in >60yr olds; higher incidence in women
•Low prevalence in younger age groups•Duodenal ulcer: up to 10% of population

UK Incidence & Prevalence UK Incidence & Prevalence (Person)(Person)
Current trends:• Annual age-standardized period prevalence decreased
1994-1998, particularly deprived areas (men 3.3/1000 - 1.5/1000; women 1.8/1000 - 0.9/1000)
• Sex incidence evening out – decreasing incidence in young men; increasing in older women
• But emergency admission rates for complications unchanged in last 30yrs
• Kang et al. (2006) – increase in case fatality for DU. Due to concomitant comorbidity / increasing ulceration (NSAIDs) / H.pylori (i.e. changing natural history)?
• Future decrease in prevalence?

International prevalence (Place)International prevalence (Place)

PlacePlace
• Worldwide. Prevalence 100% in developing countries
• Potential for “re-spread” in UK through travel?
• H. pylori - oral / faeco-oral transmission associated with poverty / overcrowding in childhood
• Increased prevalence in children with history of ulcer in the mothers – due to common environmental factors?
• Variation between ethnic groups even within countries

Place – Regional variation Place – Regional variation (NCHOD)(NCHOD)
• 2004-06 pooled data from ONS• SMR
• Directly standardised age specific death rates (per 100,000 European standard population) - regional centres higher than national average
• High rates affected by lifestyle factors & e.g. aspirin in deprived areas (raised CVD risk)?
–Lowest = E. Midlands (89). Highest = London (112) –Industrial areas = 114, London suburbs = 111, London cosmopolitain = 153
E&W
NE
All Males Females
99 (97-101)
100 (97-103)
99 (96-101)
111 (102-121)
124 (110-139)
100 (88-113)

NCHOD data - critiqueNCHOD data - critique
• Based on original underlying cause of death (death certification)
• Numerator - mortality data 1993-2006 (ONS) with codes assigned using postcode of usual residence
• Changes to coding causes of death in England & Wales. Data based on new coding
• Denominator data - latest revisions of ONS mid-year population estimates, current at Oct 2007 - quite accurate
• NCHOD regularly updated

Data sourcesData sources
Data source
Valid? Reliable? Complete?
Timely?
Accessible?
Relevant?
Cochrane reviews
√ (RCTs / meta-analyses)
√ (RCTs / meta-analyses)
Treatment focus
√ √ Partial
PubMed articles
Some small studies
Some small studies
Epidemiol focus
√ √ √
NEPHO √ ONS data
√ ONS data
Regional life years lost data – London only
1999 & 2001
√ √
Other potential sources: HES, primary care records, prescribing database

Data sourcesData sources
Data source
Valid? Reliable? Complete? Timely?
Accessible?
Relevant?
NCHOD √ ONS data. Updated though based on death certification
√ ONS data. Updated though based on death certification
Age-specific rates not split by sex (small numbers)
√ Updated 2007
√ NEPHO website
√
HPA √ √ Based on reporting from primary care
Testing & trend monitoring. No routine publications
√ √ √

Data sourcesData sourcesData source
Valid? Reliable? Complete?
Timely? Accessible?
Relevant?
Patient UK
√ NICE guidance & review articles. Written by clinicians. Reviewed 18monthly
√ NICE guidance & review articles. Written by clinicians. Reviewed 18monthly
Patient info.
√ Based on recent guidance & articles
√ √
Patient Plus
√ Peer reviewed. Based on NICE guidance & review articles. Written by clinicians.
√ Peer reviewed. Based on NICE guidance & review articles. Written by clinicians.
Clinical focus – diagnosis and management
√ Based on recent guidance & articles
√ Partial

ConclusionConclusion
• Disease mechanism / transmission poorly understood• Risk factors multiple & interacting• H. pylori is main cause but has changing natural history• “Each generation has carried its own particular risk of
bearing ulcers throughout adult life” (Susser & Stein 1962)
• Current pattern = exposure to H. pylori + genetics + exposure to drugs + environmental / behavioural factors
• DU / GU likely to continue causing significant chronic disease burden and personal / societal cost. Predicting future pattern difficult

Questions?Questions?References
Bardhan, K. D., Williamson, M., Royston, C., Lyon, C. (2004) Admission rates for peptic ulcer in the Trent Region, UK, 1972-2000: Changing pattern, a changing disease? Digestive and Liver Disease, 36, 577-588
Barron & Sonnenberg, Gut (2002), 50(4), 568-570
Malaty, H., Engstrand, L., Pederson, N., Graham, D. (1994), "Helicobacter pylori infection genetic and environmental influences, a study of twins", Annals of Internal Medicine, Vol. 120 pp.982-6
Primatesta et al. (1994), Int. J. Epidemiol. 23(6), 1206-1217
Robinson, S.C., Bruce, R.M. (1940), "The body build of the ulcer patient", American Journal of Digestive Diseases, Vol. 7
Roderick P, Davies R, Raftery J, Crabbe D, Pearce R, Patel P. The cost-effectiveness of screening for Helicobacter pylori to reduce mortality and morbidity from gastric cancer and peptic ulcer disease: a discrete-event simulation model. Health Technol Assess, 2003;7(6). Available at: http://www.cinahl.com/cexpress/hta/summ/summ706.pdf

Bardhan et al. 2004Elective surgery. Rates per million resident population. Three-year moving averages.
The number of elective anti-ulcer operations has
declined, and more markedly so for DU. The greatest decline for both groups was in younger
men, 35–64 years, in whom such operations were most commonly performed (Fig. 4). The rate of decline, however, was no greater in the
era of modern medical treatment (Table 3).
Related Documents










![Role of dietary polyphenols in the management of peptic ulcer · 2017. 4. 26. · Peptic ulcer disease is a multifactorial and complex disease involving gastric and duodenal ulcers[1,2].](https://static.cupdf.com/doc/110x72/602db182f8cf5c32fc5bf263/role-of-dietary-polyphenols-in-the-management-of-peptic-ulcer-2017-4-26-peptic.jpg)
