535 Abstract: Atherosclerosis is a leading cause of vascular disease worldwide. Its major clinical manifestations include ischemic heart disease, ischemic stroke, and peripheral arterial disease. In high-income countries, there have been dramatic declines in the incidence and mortality from ischemic heart disease and ischemic stroke since the middle of the 20th century. For example, in the United Kingdom, the probability of death from vascular disease in middle-aged men (35–69 years) has decreased from 22% in 1950 to 6% in 2010. Most low- and middle-income countries have also reported declines in mortality from stroke over the last few decades, but mortality trends from ischemic heart disease have been more varied, with some countries reporting declines and others reporting increases (particularly those in Eastern Europe and Asia). Many major modifiable risk factors for atherosclerosis have been identified, and the causal relevance of several risk factors is now well established (including, but not limited to, smoking, adiposity, blood pressure, blood cholesterol, and diabetes mellitus). Widespread changes in health behaviors and use of treatments for these risk factors are responsible for some of the dramatic declines in vascular mortality in high-income countries. In order that these declines continue and are mirrored in less wealthy nations, increased efforts are needed to tackle these major risk factors, particularly smoking and the emerging obesity epidemic. (Circ Res. 2016;118:535-546. DOI: 10.1161/CIRCRESAHA.115.307611.) Key Words: atherosclerosis ■ coronary ■ epidemiology ■ peripheral ■ stroke Atherosclerosis Compendium © 2016 American Heart Association, Inc. Circulation Research is available at http://circres.ahajournals.org DOI: 10.1161/CIRCRESAHA.115.307611 Epidemiology of Atherosclerosis and the Potential to Reduce the Global Burden of Atherothrombotic Disease William Herrington,* Ben Lacey,* Paul Sherliker, Jane Armitage,† Sarah Lewington† Circulation Research Compendium on Atherosclerosis Atherosclerosis: Successes, Surprises, and Future Challenges Epidemiology of Atherosclerosis and the Potential to Reduce the Global Burden of Atherothrombotic Disease Triglyceride-Rich Lipoproteins and Atherosclerotic Cardiovascular Disease: New Insights From Epidemiology, Genetics, and Biology Genetics of Coronary Artery Disease Surprises From Genetic Analyses of Lipid Risk Factors for Atherosclerosis From Loci to Biology: Functional Genomics of Genome-Wide Association for Coronary Disease Are Genetic Tests for Atherosclerosis Ready for Routine Clinical Use? Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis Macrophages and Dendritic Cells: Partners in Atherogenesis Macrophage Phenotype and Function in Different Stages of Atherosclerosis Adaptive Response of T and B Cells in Atherosclerosis Microdomains, Inflammation, and Atherosclerosis Vascular Smooth Muscle Cells in Atherosclerosis MicroRNA Regulation of Atherosclerosis The Success Story of LDL Cholesterol Lowering From Lipids to Inflammation: New Approaches to Reducing Atherosclerotic Risk Imaging Atherosclerosis Peter Libby, Karin E. Bornfeldt, and Alan R. Tall, Editors Original received September 12, 2015; revision received November 4, 2015; accepted November 6, 2015. From the Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU), Nuffield Department of Population Health, Oxford OX3 7LF, UK. *These authors share joint contribution. †These authors share joint contribution. Correspondence to Jane Armitage, Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU), Nuffield Department of Population Health, Richard Doll Bldg, Old Rd Campus, Roosevelt Dr, Oxford OX3 7LF, UK. E-mail [email protected] by guest on November 8, 2017 http://circres.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

535
Abstract: Atherosclerosis is a leading cause of vascular disease worldwide. Its major clinical manifestations include ischemic heart disease, ischemic stroke, and peripheral arterial disease. In high-income countries, there have been dramatic declines in the incidence and mortality from ischemic heart disease and ischemic stroke since the middle of the 20th century. For example, in the United Kingdom, the probability of death from vascular disease in middle-aged men (35–69 years) has decreased from 22% in 1950 to 6% in 2010. Most low- and middle-income countries have also reported declines in mortality from stroke over the last few decades, but mortality trends from ischemic heart disease have been more varied, with some countries reporting declines and others reporting increases (particularly those in Eastern Europe and Asia). Many major modifiable risk factors for atherosclerosis have been identified, and the causal relevance of several risk factors is now well established (including, but not limited to, smoking, adiposity, blood pressure, blood cholesterol, and diabetes mellitus). Widespread changes in health behaviors and use of treatments for these risk factors are responsible for some of the dramatic declines in vascular mortality in high-income countries. In order that these declines continue and are mirrored in less wealthy nations, increased efforts are needed to tackle these major risk factors, particularly smoking and the emerging obesity epidemic. (Circ Res. 2016;118:535-546. DOI: 10.1161/CIRCRESAHA.115.307611.)
Key Words: atherosclerosis ■ coronary ■ epidemiology ■ peripheral ■ stroke
Atherosclerosis Compendium
© 2016 American Heart Association, Inc.
Circulation Research is available at http://circres.ahajournals.org DOI: 10.1161/CIRCRESAHA.115.307611
Epidemiology of Atherosclerosis and the Potential to Reduce the Global Burden of Atherothrombotic Disease
William Herrington,* Ben Lacey,* Paul Sherliker, Jane Armitage,† Sarah Lewington†
Circulation Research Compendium on Atherosclerosis
Atherosclerosis: Successes, Surprises, and Future ChallengesEpidemiology of Atherosclerosis and the Potential to Reduce the Global Burden of Atherothrombotic DiseaseTriglyceride-Rich Lipoproteins and Atherosclerotic Cardiovascular Disease: New Insights From Epidemiology, Genetics, and BiologyGenetics of Coronary Artery DiseaseSurprises From Genetic Analyses of Lipid Risk Factors for AtherosclerosisFrom Loci to Biology: Functional Genomics of Genome-Wide Association for Coronary DiseaseAre Genetic Tests for Atherosclerosis Ready for Routine Clinical Use?Endothelial Cell Dysfunction and the Pathobiology of AtherosclerosisMacrophages and Dendritic Cells: Partners in AtherogenesisMacrophage Phenotype and Function in Different Stages of AtherosclerosisAdaptive Response of T and B Cells in AtherosclerosisMicrodomains, Inflammation, and AtherosclerosisVascular Smooth Muscle Cells in AtherosclerosisMicroRNA Regulation of AtherosclerosisThe Success Story of LDL Cholesterol LoweringFrom Lipids to Inflammation: New Approaches to Reducing Atherosclerotic RiskImaging Atherosclerosis
Peter Libby, Karin E. Bornfeldt, and Alan R. Tall, Editors
Original received September 12, 2015; revision received November 4, 2015; accepted November 6, 2015.From the Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU), Nuffield Department of Population Health, Oxford OX3 7LF, UK.*These authors share joint contribution.†These authors share joint contribution.Correspondence to Jane Armitage, Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU), Nuffield Department of Population Health,
Richard Doll Bldg, Old Rd Campus, Roosevelt Dr, Oxford OX3 7LF, UK. E-mail [email protected]
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from
536 Circulation Research February 19, 2016
What Is Atherosclerosis?Atherosclerosis is a chronic arterial disease and a major cause of vascular death. Fatty streaks in arterial walls gradually de-velop into atheroma and characteristic plaques. The acute rup-ture of these atheromatous plaques causes local thrombosis, leading to partial or total occlusion of the affected artery.1 The clinical consequences of these plaques depend on their site and the degree and speed of vessel occlusion. The disease has a latency of many years and frequently coexists in >1 vascular bed. Its major clinical manifestations include ischemic heart disease (IHD), ischemic stroke, and peripheral arterial disease (PAD). The global distribution and an overview of the major determinants of these manifestations are described later.
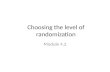
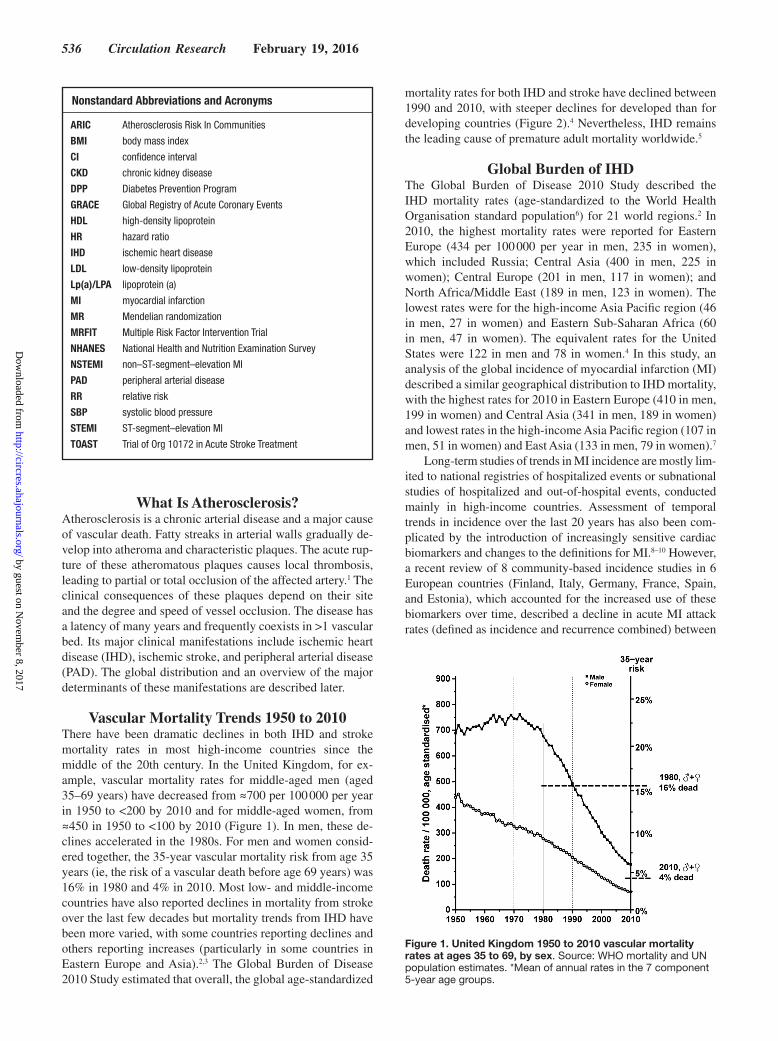
Vascular Mortality Trends 1950 to 2010There have been dramatic declines in both IHD and stroke mortality rates in most high-income countries since the middle of the 20th century. In the United Kingdom, for ex-ample, vascular mortality rates for middle-aged men (aged 35–69 years) have decreased from ≈700 per 100 000 per year in 1950 to <200 by 2010 and for middle-aged women, from ≈450 in 1950 to <100 by 2010 (Figure 1). In men, these de-clines accelerated in the 1980s. For men and women consid-ered together, the 35-year vascular mortality risk from age 35 years (ie, the risk of a vascular death before age 69 years) was 16% in 1980 and 4% in 2010. Most low- and middle-income countries have also reported declines in mortality from stroke over the last few decades but mortality trends from IHD have been more varied, with some countries reporting declines and others reporting increases (particularly in some countries in Eastern Europe and Asia).2,3 The Global Burden of Disease 2010 Study estimated that overall, the global age-standardized
mortality rates for both IHD and stroke have declined between 1990 and 2010, with steeper declines for developed than for developing countries (Figure 2).4 Nevertheless, IHD remains the leading cause of premature adult mortality worldwide.5
Global Burden of IHDThe Global Burden of Disease 2010 Study described the IHD mortality rates (age-standardized to the World Health Organisation standard population6) for 21 world regions.2 In 2010, the highest mortality rates were reported for Eastern Europe (434 per 100 000 per year in men, 235 in women), which included Russia; Central Asia (400 in men, 225 in women); Central Europe (201 in men, 117 in women); and North Africa/Middle East (189 in men, 123 in women). The lowest rates were for the high-income Asia Pacific region (46 in men, 27 in women) and Eastern Sub-Saharan Africa (60 in men, 47 in women). The equivalent rates for the United States were 122 in men and 78 in women.4 In this study, an analysis of the global incidence of myocardial infarction (MI) described a similar geographical distribution to IHD mortality, with the highest rates for 2010 in Eastern Europe (410 in men, 199 in women) and Central Asia (341 in men, 189 in women) and lowest rates in the high-income Asia Pacific region (107 in men, 51 in women) and East Asia (133 in men, 79 in women).7
Long-term studies of trends in MI incidence are mostly lim-ited to national registries of hospitalized events or subnational studies of hospitalized and out-of-hospital events, conducted mainly in high-income countries. Assessment of temporal trends in incidence over the last 20 years has also been com-plicated by the introduction of increasingly sensitive cardiac biomarkers and changes to the definitions for MI.8–10 However, a recent review of 8 community-based incidence studies in 6 European countries (Finland, Italy, Germany, France, Spain, and Estonia), which accounted for the increased use of these biomarkers over time, described a decline in acute MI attack rates (defined as incidence and recurrence combined) between
Nonstandard Abbreviations and Acronyms
ARIC Atherosclerosis Risk In Communities
BMI body mass index
CI confidence interval
CKD chronic kidney disease
DPP Diabetes Prevention Program
GRACE Global Registry of Acute Coronary Events
HDL high-density lipoprotein
HR hazard ratio
IHD ischemic heart disease
LDL low-density lipoprotein
Lp(a)/LPA lipoprotein (a)
MI myocardial infarction
MR Mendelian randomization
MRFIT Multiple Risk Factor Intervention Trial
NHANES National Health and Nutrition Examination Survey
NSTEMI non–ST-segment–elevation MI
PAD peripheral arterial disease
RR relative risk
SBP systolic blood pressure
STEMI ST-segment–elevation MI
TOAST Trial of Org 10172 in Acute Stroke Treatment
Figure 1. United Kingdom 1950 to 2010 vascular mortality rates at ages 35 to 69, by sex. Source: WHO mortality and UN population estimates. *Mean of annual rates in the 7 component 5-year age groups.
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from
Herrington et al Epidemiology of Atherosclerosis 537
1985 and 2010 in all populations.11 The annual reduction in rates over this period at age 35 to 74 years for these countries combined was 4.0% (95% confidence interval [CI] 3.7%–4.4%) for men and 4.2% (3.6%–4.8%) for women (ie, nearly a 70% reduction in MI rates over 25 years), with some regional varia-tion. These MI rate decreases are similar to those described in studies in the United States and the United Kingdom.12–14 In the United States, the 4 communities of the Atherosclerosis Risk In Communities (ARIC) Study, with a combined population of just under 400 000 adults aged 35 to 74 years, reported an average fall in incidence (first hospitalized MI or IHD death) from 1987 to 2008 of 4.3% per year in men and 3.8% per year in women; incidence was higher, and the decline in rates less steep, in African Americans compared with White Americans for both sexes.15 A nationwide study in England from 2002 to 2010 reported that rates of hospital admissions or death from acute MI decreased by 4.8% per year in men and 4.5% in wom-en.13 This study estimated that around half the decrease in IHD mortality in England over this period could be attributed to a decline in acute MI events, and just under half was attributable to a decline in the case fatality.
Over the last 2 decades, there has been a change in the type of MI presentation in high-income countries. The Global Registry of Acute Coronary Events (GRACE) Study (a large
registry of patients presenting with acute coronary syndrome to 184 hospitals in 25 mostly high-income countries) reported that for patients recruited from 2001 to 2007, 30% had ST-segment–elevation MI (STEMI; the subtype of MI with the worst short-term prognosis16), 31% had non–ST-segment–ele-vation MI (NSTEMI), 26% had unstable angina, and 12% had other cardiac or noncardiac diagnoses (ie, the ratio of MIs that were STEMI:NSTEMI was ≈50:50; median age 65 years).17 A national registry of patients presenting to hospitals in England and Wales in 2013/14 with acute coronary syndromes reported a somewhat higher proportion of MI patients with NSTEMI (61%) versus STEMI (39%).18 The proportion of patients with NSTEMI was noted to increase with age (mean age at event 69 years) and was slightly higher in women than men. A large community-based study in the United States (the Kaiser Permanente study) described similar findings to the United Kingdom: 67% of patients hospitalized for MI between 1999 and 2008 had NSTEMI and 33% had STEMI (mean age 69 years).14 Several long-term incidence studies in the West have described temporal trends in the incidence of NSTEMI and STEMI, with most reporting steep declines in the incidence of STEMI over the last 20 years and less steep declines (and oc-casionally increases)19 in the incidence of NSTEMI (perhaps the result of increased diagnostic sensitivity).14,15 Over the same period (2001–2011), and in contrast to the West, China experienced a rapid rise in hospitalization for STEMI (3.5 per 100 000 per year in 2001 to 15.4 per 100 000 in 2011).20
There is limited evidence worldwide on the incidence of an-gina,21,22 but good data on prevalence. The 2011 UK prevalence of angina estimated from primary care data varied with age from <1% at age 45 to 54 years in both men and women to 9% in men and 5% in women at age 65 to 74 years.21 In the 2009 to 2012 US National Health and Nutrition Examination Survey (NHANES), the prevalence of self-reported physician diagno-sis of angina was 2% at age 40 to 64 years in both men and women and 8% in men and 5% in women at age ≥65 years.23
Global Burden of Ischemic StrokeThe Global Burden of Disease 2010 Study also reported the mortality from ischemic stroke in different regions of the world.3 Age-standardized to the World Health Organisation standard population, the region with the highest median coun-try-specific mortality was Eastern Europe (96 per 100 000 per year), followed by the Oceanic islands (63) and Central Europe (62). The lowest mortality rates were reported for high-income North America (19), Australasia (19), and Andean Latin America (21). At a country level, the age-standardized mortality ranged from 9 per 100 000 per year in Qatar to 138 in Russia.
Like IHD, ischemic stroke incidence (fatal or not) in-creases with age. For example, the Oxford Vascular Study, a community-based study in the United Kingdom, reported that the incidence of ischemic stroke in 2002 to 2005 in-creased from 35 per 100 000 per year at age 35 to 44 years to 952 at age 75 to 84 years.24 On the whole, studies report slightly higher age-specific incidence of (and mortality from) ischemic stroke in men than women.25,26 In the United States, there is also variation in ischemic stroke incidence by
Figure 2. Developed and developing countries 1990 to 2010 ischemic heart disease and stroke mortality rates at ages 35 to 69, by sex. Source: Global Burden of Disease Study 20134; *Mean of annual rates in the 7 component 5-year age groups.
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from

538 Circulation Research February 19, 2016
ethnicity, with higher rates in African Americans compared with white Americans.27
Age-standardized to the World Health Organisation stan-dard population, the Global Burden of Disease 2010 Study estimated that the incidence of ischemic stroke in the United States for 2010 was 143 per 100 000 person-years, somewhat higher than in the United Kingdom with 85, but an 18% de-crease in incidence since 1990. Similar proportional reduc-tions were reported for other high-income countries.28 Studies of temporal trends in most low- and middle-income coun-tries have not been feasible because the use of computed tomography and magnetic resonance imaging scanners (to differentiate stroke subtypes) is not widespread.
Ischemic stroke can be divided into subtypes according to the site of the causal lesion.29–32 The Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria is commonly used and has the following categories: large vessel, small vessel, cardioembolic, stroke of other determined cause, and stroke of indeterminate cause.29 Atherosclerosis is the major underly-ing pathophysiological mechanism in large vessel disease and may also be responsible for a large proportion of ischemic strokes with indeterminate cause (eg, there is evidence that aortic atherosclerotic plaques may be a source of thrombus formation and embolism).33 In the late 1990s, the Rochester Epidemiology Project (a community-based stroke incidence study in Minnesota) reported that 16% of strokes were large vessel, 16% were small vessel, 29% were cardioembolic, 3% were other determined cause, and 36% were indeterminate cause (mean age at event 76 years).34 Broadly similar propor-tions have been reported by other studies in the United States 31,35 and Europe,36 but reliable data from low- and middle-income countries are limited.
Global Burden of PADCompared with IHD and stroke, PAD (which includes arte-rial disease of the lower extremity, renal, mesenteric, and abdominal aortic territories) is a relatively rare cause of mor-tality, accounting for only ≈1% to 2% of cardiovascular deaths globally in 2013.5 However, lower extremity PAD is a com-mon cause of morbidity, which may result in reduced mobil-ity, intermittent claudication, critical limb ischemia, and acute limb ischemia.37,38 A recent meta-analysis estimated the global prevalence of lower extremity PAD (using an ankle-brachial systolic blood pressure [SBP] index threshold of ≤0.9) from 34 population-based studies conducted between 1997 and 2011.38 In high-income countries, the average age-specific prevalence ranged from 5% at age 40 to 49 years to 13% at age 70 to 79 years (irrespective of sex). In low- and middle-income coun-tries, the age-specific prevalences were similar in women to high-income countries but were somewhat lower in men: 6% at age 40 to 49 years and 12% at age 70 to 79 years in women and 3% at age 40 to 49 years to 9% at age 70 to 79 years in men. In the 1999 to 2000 NHANES, the US prevalence of PAD (ankle-brachial SBP index <0.9) ranged from 1% at age 40 to 49 years to 15% at age ≥70 years, with no evidence of variation by sex.39 Prevalence studies of intermittent claudication have tended to find higher rates in men than women, but this difference is less apparent in studies using ankle-brachial SBP index.40
Overview of Modifiable Causes of Atherosclerosis
Many modifiable risk factors for atherosclerosis have been identified by large prospective observational studies, and the causal relevance of several risk factors is now well established. Widespread changes in health behaviors and use of treatments for these risk factors are responsible for some of the dramatic declines in vascular mortality rates in high-income countries over the last 60 years.41,42 The relevance of cigarette smoking, blood pressure, blood lipids, diabetes mellitus, chronic kidney disease (CKD), and adiposity to atherothrombotic risk is de-scribed below.
Smoking and AtherosclerosisDuring the first few decades of the 20th century, the consump-tion of manufactured cigarettes increased greatly,43 whereas the hazards of smoking remained largely unsuspected. It was only around the middle of the 20th century that several case–control studies of lung cancer were published in Western Europe44–47 and North America,48 leading to the conclusion in 1950 that smoking was a cause, and an important cause of lung cancer. This discovery led to a UK prospective obser-vational study among 35 000 British doctors, which began in 1951,49 and two US prospective studies which began in 1959 and 1982, each with over one million participants.50,51 Men born in the United Kingdom and United States were select-ed because these were the first major populations in which cigarette consumption from a young age was substantial. Consequently, these studies provided the best evidence on the relevance of smoking to many causes of deaths due both to their large size and because by the end of the 20th century, the smoking epidemic had matured so that in old age, those who still smoked had generally been regularly smoking substantial numbers of cigarettes throughout their adult life.
The 50-year follow-up of the British Doctors study con-firmed that smoking caused more deaths by other diseases than by lung cancer and that half of all smokers would eventually be killed by their habit. For example, there was a relative risk (RR) of 1.6 for IHD mortality for current smokers compared with never smokers (age-standardized mortality of 1001 per 100 000 men per year versus 619; Table 1) and 1.6 for stroke mortality (432 versus 275),52 with hazards higher among those who smoked more cigarettes. Importantly, these data also demonstrated that one-third of the absolute excess mortality among cigarette smokers was because of IHD or cerebrovas-cular disease, and even more importantly, that smoking ces-sation prevents most of this excess mortality. Quitting at age 50 halved the risk of death, and quitting by age 30 avoided almost all of it.
Only recently has it been possible to observe directly the full effects of smoking on premature mortality among women because in both the United Kingdom and the United States, the smoking epidemic in women began later, with women born around 1940 becoming the first generation in which many smoked substantial numbers of cigarettes throughout adult life. The Million Women Study of 1.3 million UK women aged 50 to 65 years recruited between 1996 and 2001 and followed for 12 years, demonstrated that
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from
Herrington et al Epidemiology of Atherosclerosis 539
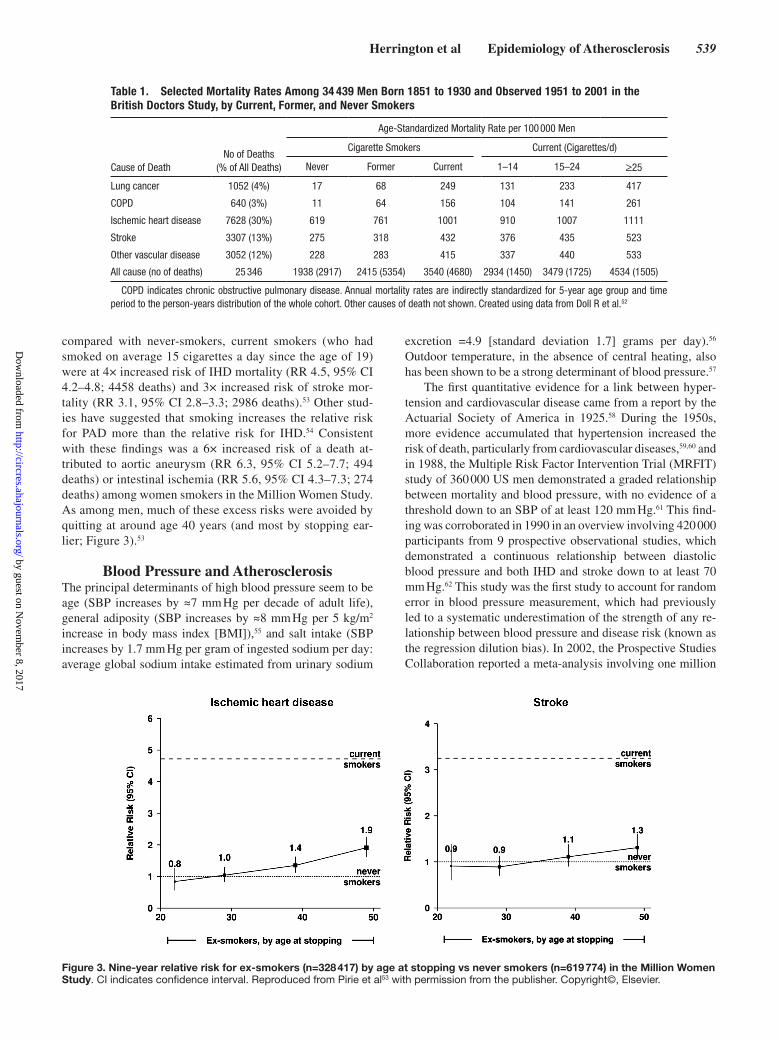
compared with never-smokers, current smokers (who had smoked on average 15 cigarettes a day since the age of 19) were at 4× increased risk of IHD mortality (RR 4.5, 95% CI 4.2–4.8; 4458 deaths) and 3× increased risk of stroke mor-tality (RR 3.1, 95% CI 2.8–3.3; 2986 deaths).53 Other stud-ies have suggested that smoking increases the relative risk for PAD more than the relative risk for IHD.54 Consistent with these findings was a 6× increased risk of a death at-tributed to aortic aneurysm (RR 6.3, 95% CI 5.2–7.7; 494 deaths) or intestinal ischemia (RR 5.6, 95% CI 4.3–7.3; 274 deaths) among women smokers in the Million Women Study. As among men, much of these excess risks were avoided by quitting at around age 40 years (and most by stopping ear-lier; Figure 3).53
Blood Pressure and AtherosclerosisThe principal determinants of high blood pressure seem to be age (SBP increases by ≈7 mm Hg per decade of adult life), general adiposity (SBP increases by ≈8 mm Hg per 5 kg/m2 increase in body mass index [BMI]),55 and salt intake (SBP increases by 1.7 mm Hg per gram of ingested sodium per day: average global sodium intake estimated from urinary sodium
excretion =4.9 [standard deviation 1.7] grams per day).56 Outdoor temperature, in the absence of central heating, also has been shown to be a strong determinant of blood pressure.57
The first quantitative evidence for a link between hyper-tension and cardiovascular disease came from a report by the Actuarial Society of America in 1925.58 During the 1950s, more evidence accumulated that hypertension increased the risk of death, particularly from cardiovascular diseases,59,60 and in 1988, the Multiple Risk Factor Intervention Trial (MRFIT) study of 360 000 US men demonstrated a graded relationship between mortality and blood pressure, with no evidence of a threshold down to an SBP of at least 120 mm Hg.61 This find-ing was corroborated in 1990 in an overview involving 420 000 participants from 9 prospective observational studies, which demonstrated a continuous relationship between diastolic blood pressure and both IHD and stroke down to at least 70 mm Hg.62 This study was the first study to account for random error in blood pressure measurement, which had previously led to a systematic underestimation of the strength of any re-lationship between blood pressure and disease risk (known as the regression dilution bias). In 2002, the Prospective Studies Collaboration reported a meta-analysis involving one million
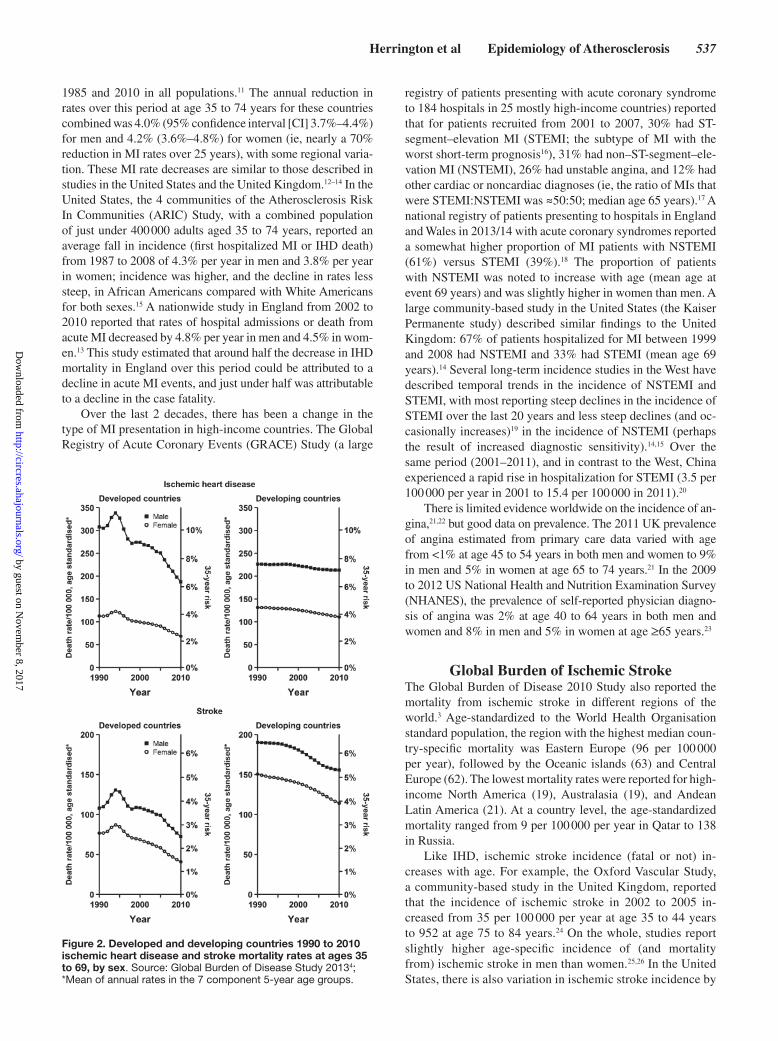
Table 1. Selected Mortality Rates Among 34 439 Men Born 1851 to 1930 and Observed 1951 to 2001 in the British Doctors Study, by Current, Former, and Never Smokers
Cause of DeathNo of Deaths
(% of All Deaths)
Age-Standardized Mortality Rate per 100 000 Men
Cigarette Smokers Current (Cigarettes/d)
Never Former Current 1–14 15–24 ≥25
Lung cancer 1052 (4%) 17 68 249 131 233 417
COPD 640 (3%) 11 64 156 104 141 261
Ischemic heart disease 7628 (30%) 619 761 1001 910 1007 1111
Stroke 3307 (13%) 275 318 432 376 435 523
Other vascular disease 3052 (12%) 228 283 415 337 440 533
All cause (no of deaths) 25 346 1938 (2917) 2415 (5354) 3540 (4680) 2934 (1450) 3479 (1725) 4534 (1505)
COPD indicates chronic obstructive pulmonary disease. Annual mortality rates are indirectly standardized for 5-year age group and time period to the person-years distribution of the whole cohort. Other causes of death not shown. Created using data from Doll R et al.52
Figure 3. Nine-year relative risk for ex-smokers (n=328 417) by age at stopping vs never smokers (n=619 774) in the Million Women Study. CI indicates confidence interval. Reproduced from Pirie et al53 with permission from the publisher. Copyright©, Elsevier.
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from
540 Circulation Research February 19, 2016
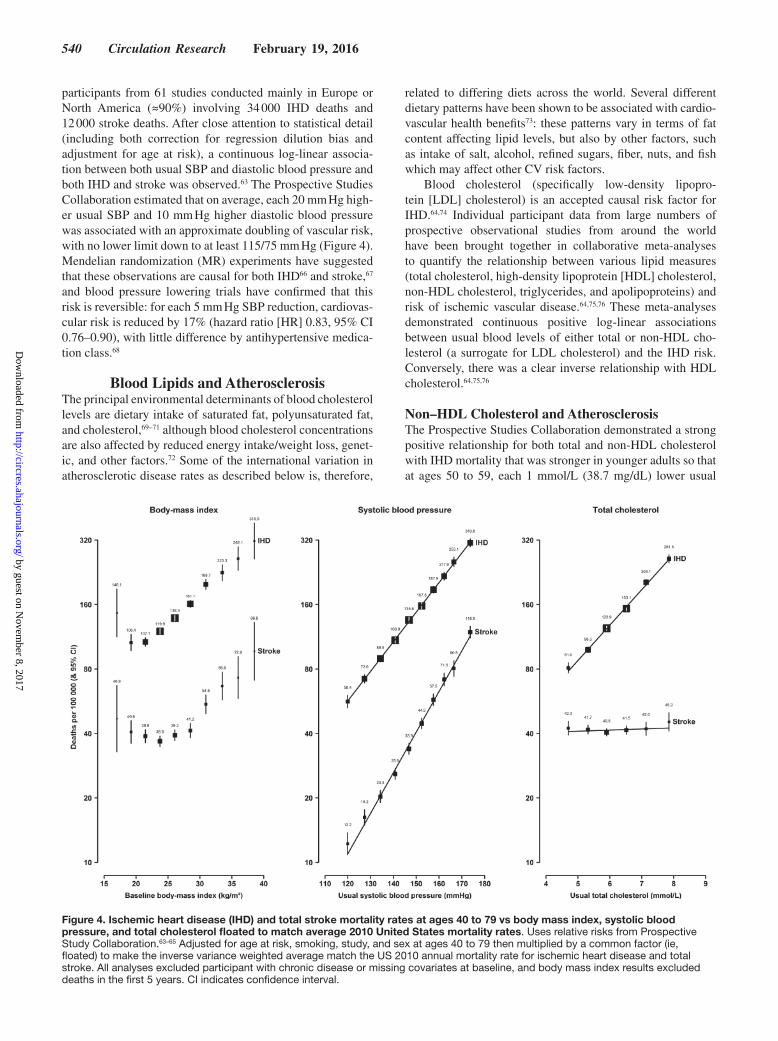
participants from 61 studies conducted mainly in Europe or North America (≈90%) involving 34 000 IHD deaths and 12 000 stroke deaths. After close attention to statistical detail (including both correction for regression dilution bias and adjustment for age at risk), a continuous log-linear associa-tion between both usual SBP and diastolic blood pressure and both IHD and stroke was observed.63 The Prospective Studies Collaboration estimated that on average, each 20 mm Hg high-er usual SBP and 10 mm Hg higher diastolic blood pressure was associated with an approximate doubling of vascular risk, with no lower limit down to at least 115/75 mm Hg (Figure 4). Mendelian randomization (MR) experiments have suggested that these observations are causal for both IHD66 and stroke,67 and blood pressure lowering trials have confirmed that this risk is reversible: for each 5 mm Hg SBP reduction, cardiovas-cular risk is reduced by 17% (hazard ratio [HR] 0.83, 95% CI 0.76–0.90), with little difference by antihypertensive medica-tion class.68
Blood Lipids and AtherosclerosisThe principal environmental determinants of blood cholesterol levels are dietary intake of saturated fat, polyunsaturated fat, and cholesterol,69–71 although blood cholesterol concentrations are also affected by reduced energy intake/weight loss, genet-ic, and other factors.72 Some of the international variation in atherosclerotic disease rates as described below is, therefore,
related to differing diets across the world. Several different dietary patterns have been shown to be associated with cardio-vascular health benefits73: these patterns vary in terms of fat content affecting lipid levels, but also by other factors, such as intake of salt, alcohol, refined sugars, fiber, nuts, and fish which may affect other CV risk factors.
Blood cholesterol (specifically low-density lipopro-tein [LDL] cholesterol) is an accepted causal risk factor for IHD.64,74 Individual participant data from large numbers of prospective observational studies from around the world have been brought together in collaborative meta-analyses to quantify the relationship between various lipid measures (total cholesterol, high-density lipoprotein [HDL] cholesterol, non-HDL cholesterol, triglycerides, and apolipoproteins) and risk of ischemic vascular disease.64,75,76 These meta-analyses demonstrated continuous positive log-linear associations between usual blood levels of either total or non-HDL cho-lesterol (a surrogate for LDL cholesterol) and the IHD risk. Conversely, there was a clear inverse relationship with HDL cholesterol.64,75,76
Non–HDL Cholesterol and AtherosclerosisThe Prospective Studies Collaboration demonstrated a strong positive relationship for both total and non-HDL cholesterol with IHD mortality that was stronger in younger adults so that at ages 50 to 59, each 1 mmol/L (38.7 mg/dL) lower usual
Figure 4. Ischemic heart disease (IHD) and total stroke mortality rates at ages 40 to 79 vs body mass index, systolic blood pressure, and total cholesterol floated to match average 2010 United States mortality rates. Uses relative risks from Prospective Study Collaboration.63–65 Adjusted for age at risk, smoking, study, and sex at ages 40 to 79 then multiplied by a common factor (ie, floated) to make the inverse variance weighted average match the US 2010 annual mortality rate for ischemic heart disease and total stroke. All analyses excluded participant with chronic disease or missing covariates at baseline, and body mass index results excluded deaths in the first 5 years. CI indicates confidence interval.
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from
Herrington et al Epidemiology of Atherosclerosis 541
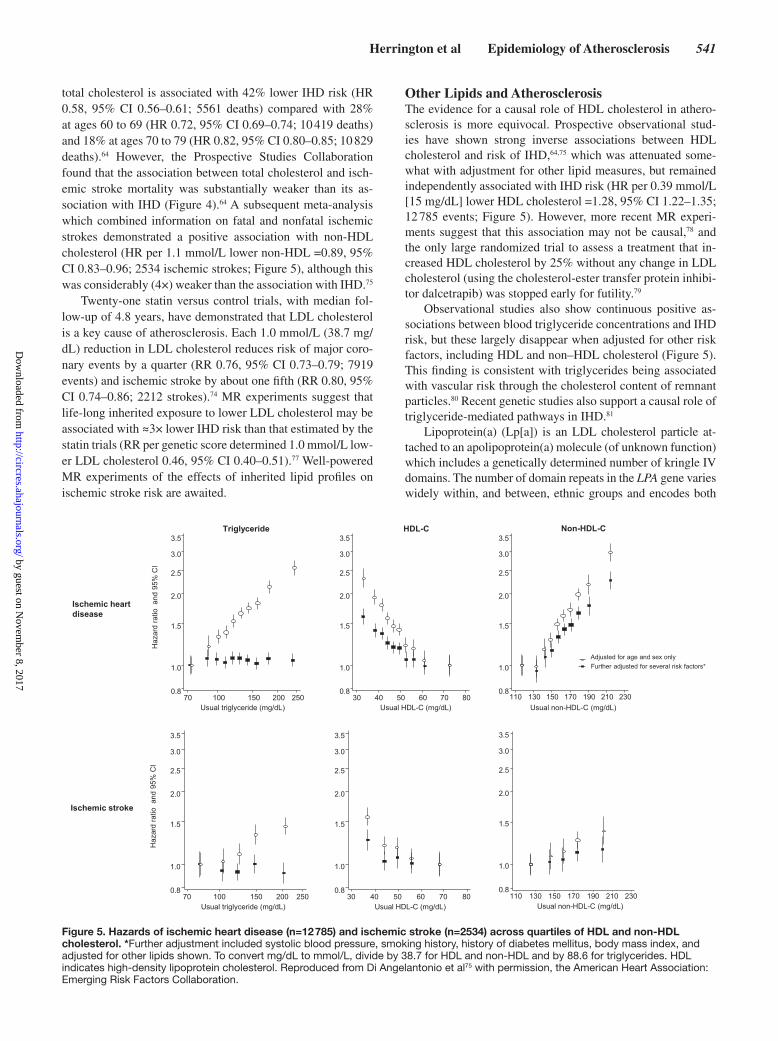
total cholesterol is associated with 42% lower IHD risk (HR 0.58, 95% CI 0.56–0.61; 5561 deaths) compared with 28% at ages 60 to 69 (HR 0.72, 95% CI 0.69–0.74; 10 419 deaths) and 18% at ages 70 to 79 (HR 0.82, 95% CI 0.80–0.85; 10 829 deaths).64 However, the Prospective Studies Collaboration found that the association between total cholesterol and isch-emic stroke mortality was substantially weaker than its as-sociation with IHD (Figure 4).64 A subsequent meta-analysis which combined information on fatal and nonfatal ischemic strokes demonstrated a positive association with non-HDL cholesterol (HR per 1.1 mmol/L lower non-HDL =0.89, 95% CI 0.83–0.96; 2534 ischemic strokes; Figure 5), although this was considerably (4×) weaker than the association with IHD.75
Twenty-one statin versus control trials, with median fol-low-up of 4.8 years, have demonstrated that LDL cholesterol is a key cause of atherosclerosis. Each 1.0 mmol/L (38.7 mg/dL) reduction in LDL cholesterol reduces risk of major coro-nary events by a quarter (RR 0.76, 95% CI 0.73–0.79; 7919 events) and ischemic stroke by about one fifth (RR 0.80, 95% CI 0.74–0.86; 2212 strokes).74 MR experiments suggest that life-long inherited exposure to lower LDL cholesterol may be associated with ≈3× lower IHD risk than that estimated by the statin trials (RR per genetic score determined 1.0 mmol/L low-er LDL cholesterol 0.46, 95% CI 0.40–0.51).77 Well-powered MR experiments of the effects of inherited lipid profiles on ischemic stroke risk are awaited.
Other Lipids and AtherosclerosisThe evidence for a causal role of HDL cholesterol in athero-sclerosis is more equivocal. Prospective observational stud-ies have shown strong inverse associations between HDL cholesterol and risk of IHD,64,75 which was attenuated some-what with adjustment for other lipid measures, but remained independently associated with IHD risk (HR per 0.39 mmol/L [15 mg/dL] lower HDL cholesterol =1.28, 95% CI 1.22–1.35; 12 785 events; Figure 5). However, more recent MR experi-ments suggest that this association may not be causal,78 and the only large randomized trial to assess a treatment that in-creased HDL cholesterol by 25% without any change in LDL cholesterol (using the cholesterol-ester transfer protein inhibi-tor dalcetrapib) was stopped early for futility.79
Observational studies also show continuous positive as-sociations between blood triglyceride concentrations and IHD risk, but these largely disappear when adjusted for other risk factors, including HDL and non–HDL cholesterol (Figure 5). This finding is consistent with triglycerides being associated with vascular risk through the cholesterol content of remnant particles.80 Recent genetic studies also support a causal role of triglyceride-mediated pathways in IHD.81
Lipoprotein(a) (Lp[a]) is an LDL cholesterol particle at-tached to an apolipoprotein(a) molecule (of unknown function) which includes a genetically determined number of kringle IV domains. The number of domain repeats in the LPA gene varies widely within, and between, ethnic groups and encodes both
70 100 150 200 2500.8
1.0
1.5
2.0
2.5
3.0
3.5
30 40 50 60 70 800.8
1.0
1.5
2.0
2.5
3.0
3.5
Usual triglyceride (mg/dL) Usual HDL-C (mg/dL)
Haz
ard
ratio
and
95%
CI
Ischemic stroke
Adjusted for age and sex only Further adjusted for several risk factors*
110 130 150 170 190 210 2300.8
1.0
1.5
2.0
2.5
3.0
3.5
Usual non-HDL-C (mg/dL)
0.8
1.0
1.5
2.0
2.5
3.0
3.5
0.8
1.0
1.5
2.0
2.5
3.0
3.5
0.8
1.0
1.5
2.0
2.5
3.0
3.5
70 100 150 200 250 30 40 50 60 70 80 110 130 150 170 190 210 230
Non-HDL-C HDL-C Triglyceride
Usual triglyceride (mg/dL) Usual HDL-C (mg/dL) Usual non-HDL-C (mg/dL)
Haz
ard
ratio
and
95%
CI
Ischemic heart disease
Figure 5. Hazards of ischemic heart disease (n=12 785) and ischemic stroke (n=2534) across quartiles of HDL and non-HDL cholesterol. *Further adjustment included systolic blood pressure, smoking history, history of diabetes mellitus, body mass index, and adjusted for other lipids shown. To convert mg/dL to mmol/L, divide by 38.7 for HDL and non-HDL and by 88.6 for triglycerides. HDL indicates high-density lipoprotein cholesterol. Reproduced from Di Angelantonio et al75 with permission, the American Heart Association: Emerging Risk Factors Collaboration.
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from

542 Circulation Research February 19, 2016
apolipoprotein(a) isoform size and Lp(a) levels (which are in-versely correlated). Lp(a) has been recognized to be a risk fac-tor for IHD for some time, but it has taken recent MR studies to support causal hypotheses.82,83 One-in-six Europeans carry LPA variants which are associated with about a 50% increased chance of developing IHD.82 The relationship between Lp(a) and stroke has been harder to elucidate, but pooling-adjusted RRs from 6 prospective studies found that high versus low Lp(a) levels were associated with an increased risk of ischemic stroke.83 There is also emerging evidence linking Lp(a) to PAD risk.84 Statins have little or no effect on Lp(a) levels, but newer lipid-modifying agents, including proprotein convertase subtil-isin/kexin type 9 and cholesterol-ester transfer protein inhibi-tors, do modestly reduce levels.85,86
Diabetes Mellitus and AtherosclerosisIn 2011, diabetes mellitus (diagnosed or not) affected ≈14% of the US adult population (including one third of those over the age of 65).87 Diabetes mellitus is a well-recognized cause of microvascular disease in the eye and kidney, but chronic raised blood glucose also promotes a combination of abnormal condi-tions, including a characteristic dyslipidemia, high blood pres-sure, vascular inflammation, and a prothrombotic tendency,88 which are all considered to be atherogenic. Large-scale meta-analysis of prospective observational studies recruited mainly from high-income countries during the second half of the 20th century quantified that diabetes mellitus increased vascular mortality rates by a factor of 2 (age- and sex-adjusted HR 2.4, 95% CI 2.2–2.6; 28 354 deaths).89 This hazard appeared similar when IHD, ischemic stroke, and PAD deaths were considered separately.90,91 The association between high blood glucose and IHD was also demonstrated to start below the threshold re-quired to diagnose diabetes mellitus: compared with lower fast-ing glucose concentrations, a glucose of ≥6.1 but <7 mmol/L was associated with 17% higher risk of IHD (HR 1.17, 95% CI 1.08–1.26; 1011 deaths).90 Although initial MR experiments associating genetic risk of type 2 diabetes mellitus to IHD risk were equivocal,92 more recent studies support causal asser-tions. Each genetically determined 1% increase in HbA1c is associated with about a 50% increased risk of IHD (odds ra-tio 1.53, 95% CI 1.14–2.05), similar in size to observational associations (although there is substantial uncertainty in both these estimates).93 Meta-analysis,94,95 and extended post-trial follow-up,96,97 of the randomized glycemic control trials also suggest that these associations are, to some extent, reversible. Aggregated results quantified that lowering HbA1c by an av-erage of 0.9%94 reduced coronary risk by about 15% (RR for IHD death 0.85, 95% CI 0.77–0.93; 2318 events), whereas the effects on ischemic stroke remain more uncertain.95
Kidney Disease and AtherosclerosisReduced glomerular filtration rate defines CKD and is identi-fied in at least 5% of the US population.98 More severe CKD (ie, lower glomerular filtration rate) is associated with increased vascular risk: compared with those with normal renal func-tion, an estimated glomerular filtration rate between 45 and 60 mL/min per 1.73 m2 is associated with at least 40% increased risk of a vascular death, and an estimated glomerular filtra-tion rate below 30 mL/min per 1.73 m2 results in at least 3×
the risk.99 CKD usually causes hypertension and is associated with an atherogenic dyslipidemia characterized by high tri-glycerides, low HDL cholesterol, and an increased proportion of LDL particles which are small and oxidized.100 CKD also causes dysregulation of calcium-phosphate metabolism (col-lectively referred to as CKD–mineral bone disease), and the high serum phosphate that results has been shown to increase vascular risk by ≈10% per 0.3 mmol/L higher phosphate (HR 1.10, 95% CI 1.06–1.13).101 Markers of CKD–mineral bone disease are associated with accelerated calcification of both the vascular intima (resulting in increased amounts of calcium in atherosclerotic plaques102) and the vascular media (leading to increased vascular stiffness),103 which helps explain why both atherosclerotic vascular risk and nonatherosclerotic vas-cular disease (eg, heart failure and arrhythmias) become more common in advanced CKD.104
Adiposity and Atherosclerotic Risk FactorsAlthough there has been success at reducing smoking rates in some parts of the world,105 globally obesity rates have been rising for the last 3 decades. Since 1980, the prevalence of obesity (currently defined as a BMI ≥30 kg/m2) among US adults has increased from 1 in 7 to 1 in 3.106 Globally, average BMI has increased by 0.5 kg/m2 each decade, slightly faster among women than men,107 and it is currently estimated that ≈600 million people (11% of adult men and 15% of adult women) are obese.108 This obesity epidemic is affecting many high- and middle-income regions and, particularly, countries in the North, Central and South Americas, the Middle East, Australasia, and Pacific Islands.106,108
Prospective observational studies, randomized trials, and MR experiments have demonstrated that adiposity increases many of the modifiable atherosclerotic risk factors described earlier, including diabetes mellitus,65,109–111 high blood pres-sure,55,65,111–113 dyslipidemia,64 and CKD114 (Table 2). Obesity may also affect levels of physical activity, in addition to being determined by them.116 Physical activity is inversely associ-ated with both stroke117–119 and IHD120–122; however, the lack of consistency in how activity has been defined and measured in different studies means there is limited evidence on the shape or strength of these relationships.122
A role for raised BMI in causing diabetes mellitus is inferred from the following observations: first, the age-adjusted US prevalence of diagnosed diabetes mellitus in adults has doubled since 1980, increasing from 3% to 6%,109 mirroring the doubling in prevalence of obesity.106 Second, prospective observational studies have demonstrated that diabetes mellitus prevalence increases across the BMI range (Table 2).65,110 Third, MR experiments have found that even relatively small genetically determined increases in BMI significantly increase the chances of developing diabetes mellitus.111,113 Fourth, randomized evidence suggests that the risk posed by adiposity is reversible: in the Diabetes Prevention Program (DPP) trial, allocation to a 6-month intensive lifestyle intervention (through calorie restriction and moderate physical activity) led to substantially great-er weight loss compared with those allocated to standard lifestyle advice and reduced the risk of developing diabetes
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from

Herrington et al Epidemiology of Atherosclerosis 543
mellitus substantially (RR per 1 kg/m2 lower BMI estimated at 0.67, 0.61–0.74; Table 2).115
In high-income countries, the causal associations between BMI and established risk factors translate into clear observa-tional associations between high BMI and mortality from IHD and ischemic stroke. A meta-analysis of prospective observa-tional studies involving 0.9 million adults has demonstrated a roughly log-linear relationship from a BMI of 25 kg/m2, with each 1 kg/m2 increase above this level associated with about an 8% increase in IHD mortality (HR per 1 kg/m2 1.08, 95% CI 1.06–1.09; 10 783 deaths) and stroke mortality (HR per 1 kg/m2 1.08, 95% CI 1.06–1.10; 3164 deaths; with similar re-sults when major stroke subtypes were considered separate-ly65,76) and a 9% increase in PAD risk (HR per 1 kg/m2 1.08, 95% CI 1.07–1.09). Applying these hazards to a uniformly age-standardized death rate for persons aged 40 to 79 years from the United States in 2010, an increase in BMI from 25 to 40 kg/m2 (ie, from ideal to 60% over ideal body weight) is estimated to increase IHD death rates by nearly 3× (from 120 to 317 per 100 000 per year), with the death rates for stroke es-timated to increase a similar amount (from 37 to 97; Figure 4).
ConclusionsAtherosclerosis is a leading cause of vascular disease world-wide. Its major clinical manifestations include IHD, ischemic stroke, and PAD. In high-income countries, there have been dramatic declines in the incidence and mortality from IHD and ischemic stroke since the middle of the 20th century. For example, in the United Kingdom, the probability of death from vascular disease in middle-aged men (35–69 years) has
decreased from 22% in 1950 to 6% in 2010. Most low- and middle-income countries have also reported declines in mortal-ity from stroke over the last few decades, but mortality trends from IHD have been more varied, with some countries report-ing declines and others reporting increases (particularly those in Eastern Europe and Asia). Many major modifiable risk fac-tors for atherosclerosis have been identified, and the causal relevance of several risk factors is now well established (in-cluding, but not limited to, smoking, adiposity, blood pressure, blood cholesterol, and diabetes mellitus). Widespread changes in health behaviors and use of treatments for these risk factors are responsible for some of the dramatic declines in vascular mortality in high-income countries. In order that these declines continue, and are mirrored in less wealthy nations, increased efforts are needed to tackle these major risk factors, particu-larly smoking and the emerging obesity epidemic.
Sources of FundingCTSU, University of Oxford receives core funding from the British Heart Foundation, Medical Research Council (UK), and Cancer Research UK.
DisclosuresNone.
References 1. Bentzon JF, Otsuka F, Virmani R, Falk E. Mechanisms of plaque for-
mation and rupture. Circ Res. 2014;114:1852–1866. doi: 10.1161/CIRCRESAHA.114.302721.
2. Moran AE, Forouzanfar MH, Roth GA, Mensah GA, Ezzati M, Murray CJ, Naghavi M. Temporal trends in ischemic heart
Table 2. Selected Studies of the Effect of Body Mass Index on Diabetes Mellitus and Blood Pressure
Study Type Study Population Exposure Result (95% confidence interval)
Diabetes mellitus
Cross-sectional observations PSC65 894 576 apparently healthy adults (57 studies)
Measured BMI Odds ratio for type 2 diabetes mellitus: 1.07 (1.07–1.08) per +1 kg/m2
Prospective observations APCSC110 154 989 adults from Asia and Pacific regions (27 studies)
Measured BMI Hazard ratio for new diabetes mellitus: 1.17 (1.14–1.20) per +1 kg/m2
Mendelian randomization Holmes et al113 4407 cases from 31 844 (7 studies)
14 SNP genetic risk score Odds ratio for type 2 diabetes mellitus: 1.27 (1.18–1.36) per +1 kg/m2
Mendelian randomization ENGAGE111 20 804 cases and 139 543 controls (28 studies)
FTO gene polymorphism Odds ratio for type 2 diabetes mellitus (ever): 1.37 (1.23–1.51) per +1 kg/m2
Randomized trial DPP115 3234 adults with glucose intolerance
Intensive lifestyle intervention versus control
Odds ratio for incident diabetes mellitus: 0.42 (0.34–0.52) per −2.2 kg/m2; 0.67 (0.61–0.74) per −1 kg/m2*
Blood pressure, mm Hg
Cross-sectional observations Kadoorie China Biobank55
512 891 Chinese adults Measured BMI SBP: +1.5 (1.4–1.5) per +1 kg/m2
Mendelian randomization Holmes et al113 SBP: 30 136 (6 studies)/ DBP: 30 137 (6 studies)
14 SNP genetic risk score SBP: +0.70 (0.24–1.16) per +1 kg/m2; DBP: +0.28 (0.03–0.52) per +1 kg/m2
Mendelian randomization ENGAGE111 SBP: 147 644 (30 studies)/ DBP: 130 380 (29 studies)
FTO gene polymorphism SBP: +0.89 (0.48–1.31) per +1 kg/m2; DBP: +0.49 (0.19–0.79) per +1 kg/m2
Randomized trial AHEAD112,113 5145 overweight or obese diabetes mellitus patients
Intensive lifestyle intervention versus control
SBP: −1.6 (−2.0 to −1.1) per −1 kg/m2; DBP: −0.1 (−0.3 to 0.2) per −1 kg/m2
AHEAD indicates Action for Health in Diabetes; APCSC, Asia-Pacific Cohort Studies Collaboration; BMI, body mass index; DBP, diastolic blood pressure; DPP, Diabetes Prevention Program; ENGAGE, European Network for Genetic and Genomic Epidemiology; FTO, fat mass- and obesity-associated; PSC, Prospective Studies Collaboration; SBP, systolic blood pressure; and SNP, single nucleotide polymorphism.
*Estimated.
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from

544 Circulation Research February 19, 2016
disease mortality in 21 world regions, 1980 to 2010: the Global Burden of Disease 2010 study. Circulation. 2014;129:1483–1492. doi: 10.1161/CIRCULATIONAHA.113.004042.
3. Bennett DA, Krishnamurthi RV, Barker-Collo S, Forouzanfar MH, Naghavi M, Connor M, Lawes CM, Moran AE, Anderson LM, Roth GA, Mensah GA, Ezzati M, Murray CJ, Feigin VL; Global Burden of Diseases, Injuries, and Risk Factors 2010 Study Stroke Expert Group. The global burden of ischemic stroke: findings of the GBD 2010 study. Glob Heart. 2014;9:107–112. doi: 10.1016/j.gheart.2014.01.001.
4. Global Burden of Disease Study 2013 (GBD 2013). Age-Sex Specific All-Cause and Cause-Specific Mortality 1990–2013. Seattle, United States: Institute for Health Metrics and Evaluation (IHME), 2014.
5. GBD 2013 Mortality and Causes of Death Collaborators. Global, region-al, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171.
6. Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. Age standardization of rates: A new WHO standard. GPE Discussion Paper Series: No. 31. Geneva, Switzerland: Wolrd Health Organisation; 2001.
7. Moran AE, Forouzanfar MH, Roth GA, Mensah GA, Ezzati M, Flaxman A, Murray CJ, Naghavi M. The global burden of ischemic heart disease in 1990 and 2010: the Global Burden of Disease 2010 study. Circulation. 2014;129:1493–1501. doi: 10.1161/CIRCULATIONAHA.113.004046.
8. Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarc-tion redefined–a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefini-tion of myocardial infarction. J Am Coll Cardiol. 2000;36:959–969.
9. Thygesen K, Alpert JS, White HD; ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Universal definition of myocardial infarction. Eur Heart J. 2007;28:2525–2538.
10. Thygesen K, Alpert JS, Jaffe AS, et al; ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal def-inition of myocardial infarction. Eur Heart J. 2012;33:2551–2567. doi: 10.1093/eurheartj/ehs184.
11. Dégano IR, Salomaa V, Veronesi G, Ferriéres J, Kirchberger I, Laks T, Havulinna AS, Ruidavets JB, Ferrario MM, Meisinger C, Elosua R, Marrugat J; Acute Myocardial Infarction Trends in Europe (AMITIE) Study Investigators. Twenty-five-year trends in myocardial infarction at-tack and mortality rates, and case-fatality, in six European populations. Heart. 2015;101:1413–1421. doi: 10.1136/heartjnl-2014-307310.
12. Gerber Y, Weston SA, Jiang R, Roger VL. The changing epidemiology of myocardial infarction in Olmsted County, Minnesota, 1995-2012. Am J Med. 2015;128:144–151. doi: 10.1016/j.amjmed.2014.09.012.
13. Smolina K, Wright FL, Rayner M, Goldacre MJ. Determinants of the de-cline in mortality from acute myocardial infarction in England between 2002 and 2010: Linked national database study. BMJ. 2012;344:d8059. doi: 10.1136/bmj.d8059.
14. Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS. Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362:2155–2165. doi: 10.1056/NEJMoa0908610.
15. Rosamond WD, Chambless LE, Heiss G, Mosley TH, Coresh J, Whitsel E, Wagenknecht L, Ni H, Folsom AR. Twenty-two-year trends in incidence of myocardial infarction, coronary heart disease mortality, and case fatal-ity in 4 US communities, 1987-2008. Circulation. 2012;125:1848–1857. doi: 10.1161/CIRCULATIONAHA.111.047480.
16. Manari A, Albiero R, De Servi S. High-risk non-ST-segment elevation myocardial infarction versus ST-segment elevation myocardial infarc-tion: same behaviour and outcome? J Cardiovasc Med (Hagerstown). 2009;10(suppl 1):S13–S16. doi: 10.2459/01.JCM.0000362039.48638.92.
17. Goodman SG, Huang W, Yan AT, Budaj A, Kennelly BM, Gore JM, Fox KA, Goldberg RJ, Anderson FA Jr; Expanded Global Registry of Acute Coronary Events (GRACE2) Investigators. The expanded Global Registry of Acute Coronary Events: baseline characteristics, management practic-es, and hospital outcomes of patients with acute coronary syndromes. Am Heart J. 2009;158:193–201.e1. doi: 10.1016/j.ahj.2009.06.003.
18. Weston C GL, Whittaker T, Van Leeven R. Myocardial Ischaemia National Audit Project (MINAP): Twelfth Public Report 2013. London: National Centre for Cardiovascular Prevention and Outcomes; 2014.
19. McManus DD, Gore J, Yarzebski J, Spencer F, Lessard D, Goldberg RJ. Recent trends in the incidence, treatment, and outcomes of patients with STEMI and NSTEMI. Am J Med. 2011;124:40–47. doi: 10.1016/j.amjmed.2010.07.023.
20. Li J, Li X, Wang Q, Hu S, Wang Y, Masoudi FA, Spertus JA, Krumholz HM, Jiang L; China PEACE Collaborative Group. ST-segment elevation
myocardial infarction in China from 2001 to 2011 (the China PEACE-Retrospective Acute Myocardial Infarction Study): a retrospective analysis of hospital data. Lancet. 2015;385:441–451. doi: 10.1016/S0140-6736(14)60921-1.
21. Townsend N, Wickramasinghe K, Bhatnagar P, Smolina K, Nichols M, Lean J, Luengo-Fernandez R, Rayner M. Coronary Heart Disease Statistics 2012 Edition. London: British Heart Foundation; 2012.
22. Hemingway H, McCallum A, Shipley M, Manderbacka K, Martikainen P, Keskimäki I. Incidence and prognostic implications of stable angina pec-toris among women and men. JAMA. 2006;295:1404–1411. doi: 10.1001/jama.295.12.1404.
23. Will JC, Yuan K, Ford E. National trends in the prevalence and medi-cal history of angina: 1988 to 2012. Circ Cardiovasc Qual Outcomes. 2014;7:407–413. doi: 10.1161/CIRCOUTCOMES.113.000779.
24. Rothwell PM, Coull AJ, Silver LE, et al; Oxford Vascular Study. Population-based study of event-rate, incidence, case fatality, and mortality for all acute vascular events in all arterial territories (Oxford Vascular Study). Lancet. 2005;366:1773–1783. doi: 10.1016/S0140-6736(05)67702-1.
25. Heuschmann PU, Di Carlo A, Bejot Y, Rastenyte D, Ryglewicz D, Sarti C, Torrent M, Wolfe CD. Incidence of stroke in europe at the beginning of the 21st century. Stroke. 2009;40:1557–1563.
26. Gibson CL. Cerebral ischemic stroke: is gender important? J Cereb Blood Flow Metab. 2013;33:1355–1361. doi: 10.1038/jcbfm.2013.102.
27. Kleindorfer DO, Khoury J, Moomaw CJ, Alwell K, Woo D, Flaherty ML, Khatri P, Adeoye O, Ferioli S, Broderick JP, Kissela BM. Stroke incidence is decreasing in whites but not in blacks: a population-based estimate of temporal trends in stroke incidence from the Greater Cincinnati/Northern Kentucky Stroke Study. Stroke. 2010;41:1326–1331. doi: 10.1161/STROKEAHA.109.575043.
28. Krishnamurthi RV, Feigin VL, Forouzanfar MH, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010: findings from the global burden of disease study 2010. Lancet Glob Health. 2013;1:e259–e281. doi: 10.1016/S2214-109X(13)70089-5.
29. Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, Gordon DL, Marsh EE III. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24:35–41.
30. Ay H, Benner T, Arsava EM, Furie KL, Singhal AB, Jensen MB, Ayata C, Towfighi A, Smith EE, Chong JY, Koroshetz WJ, Sorensen AG. A com-puterized algorithm for etiologic classification of ischemic stroke: the Causative Classification of Stroke System. Stroke. 2007;38:2979–2984. doi: 10.1161/STROKEAHA.107.490896.
31. Schneider AT, Kissela B, Woo D, Kleindorfer D, Alwell K, Miller R, Szaflarski J, Gebel J, Khoury J, Shukla R, Moomaw C, Pancioli A, Jauch E, Broderick J. Ischemic stroke subtypes: a population-based study of in-cidence rates among blacks and whites. Stroke. 2004;35:1552–1556. doi: 10.1161/01.STR.0000129335.28301.f5.
32. Bamford J, Sandercock P, Dennis M, Burn J, Warlow C. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet. 1991;337:1521–1526.
33. Kronzon I, Tunick PA. Aortic atherosclerotic disease and stroke. Circulation. 2006;114:63–75. doi: 10.1161/CIRCULATIONAHA.105.593418.
34. Petty GW, Brown RD Jr, Whisnant JP, Sicks JD, O’Fallon WM, Wiebers DO. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke. 1999;30:2513–2516.
35. White H, Boden-Albala B, Wang C, Elkind MS, Rundek T, Wright CB, Sacco RL. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111:1327–1331. doi: 10.1161/01.CIR.0000157736.19739.D0.
36. Schulz UG, Rothwell PM. Differences in vascular risk factors be-tween etiological subtypes of ischemic stroke: importance of popu-lation-based studies. Stroke. 2003;34:2050–2059. doi: 10.1161/01.STR.0000079818.08343.8C.
37. Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK. Management of patients with pe-ripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:1425–1443. doi: 10.1161/CIR.0b013e31828b82aa.
38. Fowkes FG, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, Norman PE, Sampson UK, Williams LJ, Mensah GA, Criqui MH. Comparison of global estimates of prevalence and risk factors for
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from
Herrington et al Epidemiology of Atherosclerosis 545
peripheral artery disease in 2000 and 2010: a systematic review and analy-sis. Lancet. 2013;382:1329–1340. doi: 10.1016/S0140-6736(13)61249-0.
39. Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral ar-terial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999–2000. Circulation. 2004;110:738–743. doi: 10.1161/01.CIR.0000137913.26087.F0.
40. Criqui MH, Aboyans V. Epidemiology of peripheral artery disease. Circ Res. 2015;116:1509–1526. doi: 10.1161/CIRCRESAHA.116.303849.
41. www.mortality-trends.org (accessed 25th January 2016).42. www.ctsu.ox.ac.uk/deathsfromsmoking/ (accessed 25th January 2016). 43. Doll R. Tobacco: a medical history. J Urban Health. 1999;76:289–313.
doi: 10.1007/BF02345669. 44. Doll R, Hill AB. Smoking and carcinoma of the lung; preliminary report.
Br Med J. 1950;2:739–748. 45. Doll R, Hill AB. A study of the aetiology of carcinoma of the lung. Br Med
J. 1952;2:1271–1286. 46. Muller FH. Tabakmissbrauch und lungencarcinoma. Zeitschrift
Krebsforsch 1939;49:57–85. 47. Schairer E. Lungenkrebs und tabakverbrauch. Zeitschrift Krebsforsch
1943;54:261–269. 48. Mills CA, Porter MM. Tobacco smoking habits and cancer of the mouth
and respiratory system. Cancer Res. 1950;10:539–542. 49. Doll R, Hill AB. The mortality of doctors in relation to their smoking hab-
its; a preliminary report. Br Med J. 1954;1:1451–1455. 50. Calle EE, Rodriguez C, Jacobs EJ, Almon ML, Chao A, McCullough ML,
Feigelson HS, Thun MJ. The American Cancer Society Cancer Prevention Study II Nutrition Cohort: rationale, study design, and baseline character-istics. Cancer. 2002;94:2490–2501. doi: 10.1002/cncr.101970.
51. Garfinkel L. Selection, follow-up, and analysis in the American Cancer Society prospective studies. Natl Cancer Inst Monogr. 1985;67:49–52.
52. Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328:1519. doi: 10.1136/bmj.38142.554479.AE.
53. Pirie K, Peto R, Reeves GK, Green J, Beral V; Million Women Study Collaborators. The 21st century hazards of smoking and benefits of stopping: a prospective study of one million women in the UK. Lancet. 2013;381:133–141. doi: 10.1016/S0140-6736(12)61720-6.
54. Lu L, Mackay DF, Pell JP. Meta-analysis of the association between ciga-rette smoking and peripheral arterial disease. Heart. 2014;100:414–423. doi: 10.1136/heartjnl-2013-304082.
55. Chen Z, Smith M, Du H, Guo Y, Clarke R, Bian Z, Collins R, Chen J, Qian Y, Wang X, Chen X, Tian X, Wang X, Peto R, Li L; China Kadoorie Biobank Collaborative Group. Blood pressure in relation to general and central adiposity among 500 000 adult Chinese men and women. Int J Epidemiol. 2015;44:1305–1319. doi: 10.1093/ije/dyv012.
56. O’Donnell M, Mente A, Rangarajan S, et al; PURE Investigators. Urinary sodium and potassium excretion, mortality, and cardiovascular events. N Engl J Med. 2014;371:612–623. doi: 10.1056/NEJMoa1311889.
57. Lewington S, Li L, Sherliker P, et al; China Kadoorie Biobank study collaboration. Seasonal variation in blood pressure and its relation-ship with outdoor temperature in 10 diverse regions of China: the China Kadoorie Biobank. J Hypertens. 2012;30:1383–1391. doi: 10.1097/HJH.0b013e32835465b5.
58. Society of Actuaries. Blood Pressure: Report of the Joint Committee on Mortality of the Association of Life Insurance Medical Directors and the Actuarial Society of America. New York, NY: Societies of Actuaries; 1925.
59. Society of Actuaries. Build and Blood Pressure Study, Chicago, IL: Societies of Actuaries; 1959.
60. Franklin SS, Wong ND. Hypertension and cardiovascular disease: contri-butions of the framingham heart study. Glob Heart. 2013;8:49–57. doi: 10.1016/j.gheart.2012.12.004.
61. Rutan GH, Kuller LH, Neaton JD, Wentworth DN, McDonald RH, Smith WM. Mortality associated with diastolic hypertension and isolated sys-tolic hypertension among men screened for the Multiple Risk Factor Intervention Trial. Circulation. 1988;77:504–514.
62. MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J, Abbott R, Godwin J, Dyer A, Stamler J. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet. 1990;335:765–774.
63. Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913.
64. Lewington S, Whitlock G, Clarke R, Sherliker P, Emberson J, Halsey J, Qizilbash N, Peto R, Collins R. Blood cholesterol and vascular mor-tality by age, sex, and blood pressure: A meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet. 2007;370:1829–1839.
65. Whitlock G, Lewington S, Sherliker P, Clarke R, Emberson J, Halsey J, Qizilbash N, Collins R, Peto R. Body-mass index and cause-specific mor-tality in 900 000 adults: Collaborative analyses of 57 prospective studies. Lancet. 2009;373:1083–1096.
66. Lieb W, Jansen H, Loley C, et al; CARDIoGRAM. Genetic predisposition to higher blood pressure increases coronary artery disease risk. Hypertension. 2013;61:995–1001. doi: 10.1161/HYPERTENSIONAHA.111.00275.
67. International Consortium for Blood Pressure Genome-Wide Association Study. Genetic variants in novel pathways influence blood pressure and cardiovascular disease risk. Nature. 2011;478:103–109.
68. Ninomiya T, Perkovic V, Turnbull F, Neal B, Barzi F, Cass A, Baigent C, Chalmers J, Li N, Woodward M, MacMahon S. Blood pressure lower-ing and major cardiovascular events in people with and without chronic kidney disease: Meta-analysis of randomised controlled trials. BMJ. 2013;347:f5680. doi: 10.1136/bmj.f5680.
69. Hegsted DM, Ausman LM, Johnson JA, Dallal GE. Dietary fat and serum lip-ids: an evaluation of the experimental data. Am J Clin Nutr. 1993;57:875–883.
70. Keys A, Anderson JT, Grande F. Prediction of serum-cholesterol responses of man to changes in fats in the diet. Lancet. 1957;273:959–966.
71. Clarke R, Frost C, Collins R, Appleby P, Peto R. Dietary lipids and blood cholesterol: quantitative meta-analysis of metabolic ward studies. BMJ. 1997;314:112–117.
72. Dattilo AM, Kris-Etherton PM. Effects of weight reduction on blood lipids and lipoproteins: a meta-analysis. Am J Clin Nutr. 1992;56:320–328.
73. Mozaffarian D, Appel LJ, Van Horn L. Components of a cardioprotec-tive diet: new insights. Circulation. 2011;123:2870–2891. doi: 10.1161/CIRCULATIONAHA.110.968735.
74. Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, Peto R, Barnes EH, Keech A, Simes J, Collins R. Efficacy and safety of more in-tensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681.
75. Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, Thompson A, Wood AM, Lewington S, Sattar N, Packard CJ, Collins R, Thompson SG, Danesh J. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302:1993–2000.
76. Singh GM, Danaei G, Farzadfar F, et al; Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group; Asia-Pacific Cohort Studies Collaboration (APCSC); Diabetes Epidemiology: Collaborative analysis of Diagnostic criteria in Europe (DECODE); Emerging Risk Factor Collaboration (ERFC); Prospective Studies Collaboration (PSC). The age-specific quantitative effects of metabolic risk factors on cardiovas-cular diseases and diabetes: a pooled analysis. PLoS One. 2013;8:e65174. doi: 10.1371/journal.pone.0065174.
77. Ference BA, Yoo W, Alesh I, Mahajan N, Mirowska KK, Mewada A, Kahn J, Afonso L, Williams KA Sr, Flack JM. Effect of long-term exposure to lower low-density lipoprotein cholesterol beginning early in life on the risk of coronary heart disease: a Mendelian randomization analysis. J Am Coll Cardiol. 2012;60:2631–2639. doi: 10.1016/j.jacc.2012.09.017.
78. Voight BF, Peloso GM, Orho-Melander M, et al. Plasma HDL choles-terol and risk of myocardial infarction: a mendelian randomisation study. Lancet. 2012;380:572–580. doi: 10.1016/S0140-6736(12)60312-2.
79. Schwartz GG, Olsson AG, Abt M, et al; dal-OUTCOMES Investigators. Effects of dalcetrapib in patients with a recent acute coronary syndrome. N Engl J Med. 2012;367:2089–2099. doi: 10.1056/NEJMoa1206797.
80. Nordestgaard BG, Varbo A. Triglycerides and cardiovascular disease. Lancet. 2014;384:626–635. doi: 10.1016/S0140-6736(14)61177-6.
81. Triglyceride Coronary Disease Genetics Consortium and Emerging Risk Factors Collaboration; Sarwar N, Sandhu MS, Ricketts SL, Butterworth AS, Di Angelantonio E, Boekholdt SM, Ouwehand W, Watkins H, Samani NJ, Saleheen D, Lawlor D, Reilly MP, Hingorani AD, Talmud PJ, Danesh J. Triglyceride-mediated pathways and coronary disease: Collaborative analysis of 101 studies. Lancet. 2010;375:1634–1639. doi: 10.1016/S0140-6736(10)60545-4.
82. Clarke R, Peden JF, Hopewell JC, et al; PROCARDIS Consortium. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med. 2009;361:2518–2528. doi: 10.1056/NEJMoa0902604.
83. Erqou S, Kaptoge S, Perry PL, Di Angelantonio E, Thompson A, White IR, Marcovina SM, Collins R, Thompson SG, Danesh J, Collaboration ERF. Lipoprotein(a) concentration and the risk of coronary heart disease, stroke, and nonvascular mortality. JAMA. 2009;302:412–423.
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from
546 Circulation Research February 19, 2016
84. Laschkolnig A, Kollerits B, Lamina C, Meisinger C, Rantner B, Stadler M, Peters A, Koenig W, Stöckl A, Dähnhardt D, Böger CA, Krämer BK, Fraedrich G, Strauch K, Kronenberg F. Lipoprotein (a) concentrations, apo-lipoprotein (a) phenotypes, and peripheral arterial disease in three indepen-dent cohorts. Cardiovasc Res. 2014;103:28–36. doi: 10.1093/cvr/cvu107.
85. Kassner U, Schlabs T, Rosada A, Steinhagen-Thiessen E. Lipoprotein(a)–An independent causal risk factor for cardiovascular disease and current therapeutic options. Atheroscler Suppl. 2015;18:263–267. doi: 10.1016/j.atherosclerosissup.2015.02.039.
86. Cannon CP, Shah S, Dansky HM, Davidson M, Brinton EA, Gotto AM, Stepanavage M, Liu SX, Gibbons P, Ashraf TB, Zafarino J, Mitchel Y, Barter P; Determining the Efficacy and Tolerability Investigators. Safety of anacetrapib in patients with or at high risk for coronary heart disease. N Engl J Med. 2010;363:2406–2415. doi: 10.1056/NEJMoa1009744.
87. Menke A, Casagrande S, Geiss L, Cowie CC. Prevalence of and Trends in Diabetes Among Adults in the United States, 1988–2012. JAMA. 2015;314:1021–1029. doi: 10.1001/jama.2015.10029.
88. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiol-ogy, pathophysiology, and management. JAMA. 2002;287:2570–2581.
89. Seshasai SR, Kaptoge S, Thompson A, et al. Diabetes mellitus, fasting glu-cose, and risk of cause-specific death. N Engl J Med. 2011;364:829–841.
90. Sarwar N, Gao P, Seshasai SR, et al. Diabetes mellitus, fasting blood glu-cose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375:2215–2222.
91. Joosten MM, Pai JK, Bertoia ML, Rimm EB, Spiegelman D, Mittleman MA, Mukamal KJ. Associations between conventional cardiovas-cular risk factors and risk of peripheral artery disease in men. JAMA. 2012;308:1660–1667. doi: 10.1001/jama.2012.13415.
92. Jansen H, Loley C, Lieb W, et al; CARDIoGRAM consortium. Genetic variants primarily associated with type 2 diabetes are related to coronary artery disease risk. Atherosclerosis. 2015;241:419–426. doi: 10.1016/j.atherosclerosis.2015.05.033.
93. Ross S, Gerstein HC, Eikelboom J, Anand SS, Yusuf S, Paré G. Mendelian randomization analysis supports the causal role of dysgly-caemia and diabetes in the risk of coronary artery disease. Eur Heart J. 2015;36:1454–1462. doi: 10.1093/eurheartj/ehv083.
94. Turnbull FM, Abraira C, Anderson RJ, et al. Intensive glucose con-trol and macrovascular outcomes in type 2 diabetes. Diabetologia. 2009;52:2288–2298. doi: 10.1007/s00125-009-1470-0.
95. Ray KK, Seshasai SR, Wijesuriya S, Sivakumaran R, Nethercott S, Preiss D, Erqou S, Sattar N. Effect of intensive control of glucose on cardio-vascular outcomes and death in patients with diabetes mellitus: a meta-analysis of randomised controlled trials. Lancet. 2009;373:1765–1772. doi: 10.1016/S0140-6736(09)60697-8.
96. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-Year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359:1577–1589. doi: 10.1056/NEJMoa0806470.
97. Gerstein HC, Miller ME, Ismail-Beigi F, Largay J, McDonald C, Lochnan HA, Booth GL; ACCORD Study Group. Effects of intensive glycaemic control on ischaemic heart disease: analysis of data from the randomised, controlled ACCORD trial. Lancet. 2014;384:1936–1941. doi: 10.1016/S0140-6736(14)60611-5.
98. Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012;379:165–180. doi: 10.1016/S0140-6736(11)60178-5.
99. Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J, Gansevoort RT. Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortal-ity in general population cohorts: A collaborative meta-analysis. Lancet. 2010;375:2073–2081.
100. Schiffrin EL, Lipman ML, Mann JF. Chronic kidney disease: effects on the cardiovascular system. Circulation. 2007;116:85–97. doi: 10.1161/CIRCULATIONAHA.106.678342.
101. Palmer SC, Hayen A, Macaskill P, Pellegrini F, Craig JC, Elder GJ, Strippoli GF. Serum levels of phosphorus, parathyroid hormone, and cal-cium and risks of death and cardiovascular disease in individuals with chronic kidney disease: a systematic review and meta-analysis. JAMA. 2011;305:1119–1127. doi: 10.1001/jama.2011.308.
102. Kono K, Fujii H, Nakai K, Goto S, Shite J, Hirata K, Fukagawa M, Nishi S. Composition and plaque patterns of coronary culprit lesions and clini-cal characteristics of patients with chronic kidney disease. Kidney Int. 2012;82:344–351. doi: 10.1038/ki.2012.118.
103. London GM, Guérin AP, Marchais SJ, Métivier F, Pannier B, Adda H. Arterial media calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant. 2003;18:1731–1740.
104. Wheeler DC, London GM, Parfrey PS, et al; EValuation Of Cinacalcet HCl Therapy to Lower CardioVascular Events (EVOLVE) Trial Investigators. Effects of cinacalcet on atherosclerotic and nonathero-sclerotic cardiovascular events in patients receiving hemodialysis: the EValuation Of Cinacalcet HCl Therapy to Lower CardioVascular Events (EVOLVE) trial. J Am Heart Assoc. 2014;3:e001363. doi: 10.1161/JAHA.114.001363.
105. Bilano V, Gilmour S, Moffiet T, d’Espaignet ET, Stevens GA, Commar A, Tuyl F, Hudson I, Shibuya K. Global trends and projections for to-bacco use, 1990-2025: an analysis of smoking indicators from the WHO Comprehensive Information Systems for Tobacco Control. Lancet. 2015;385:966–976. doi: 10.1016/S0140-6736(15)60264-1.
106. World Health Organization. Global database on body mass index. http://apps.who.int/bmi/. Accessed September 11, 2015.
107. Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ, Singh GM, Gutierrez HR, Lu Y, Bahalim AN, Farzadfar F, Riley LM, Ezzati M; Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Body Mass Index). National, regional, and global trends in body-mass index since 1980: systematic analysis of health ex-amination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet. 2011;377:557–567. doi: 10.1016/S0140-6736(10)62037-5.
108. World Health Organization. Global status report on noncommunicable diseases 2014. http://www.who.int/nmh/publications/ncd-status-report- 2014/en/. Accessed September 11, 2015.
109. Centre of Disease Control and Prevention. Diabetes public health re-source. http://www.cdc.gov/diabetes/home/. Accessed September 11, 2015.
110. Ni Mhurchu C, Parag V, Nakamura M, Patel A, Rodgers A, Lam TH. Body mass index and risk of diabetes mellitus in the asia-pacific region. Asia Pacific J Clin Nutr. 2006;15:127–133.
111. European Network for Genetic and Genomic Epidemiology (ENGAGE) collaboration. The role of adiposity in cardiometabolic traits: A mende-lian randomization analysis. PLoS Med. 2013;10:e1001474.
112. Wing RR, Bolin P, Brancati FL, et al; Look AHEAD Research Group. Cardiovascular effects of intensive lifestyle intervention in type 2 diabe-tes. N Engl J Med. 2013;369:145–154. doi: 10.1056/NEJMoa1212914.
113. Holmes MV, Lange LA, Palmer T, et al. Causal effects of body mass index on cardiometabolic traits and events: a Mendelian randomiza-tion analysis. Am J Hum Genet. 2014;94:198–208. doi: 10.1016/j.ajhg.2013.12.014.
114. Vivante A, Golan E, Tzur D, Leiba A, Tirosh A, Skorecki K, Calderon-Margalit R. Body mass index in 1.2 million adolescents and risk for end-stage renal disease. Arch Intern Med. 2012;172:1644–1650.
115. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, Nathan DM; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle interven-tion or metformin. N Engl J Med. 2002;346:393–403. doi: 10.1056/NEJMoa012512.
116. Wareham NJ, Brage S. Commentary: physical activity and obesity; scien-tific uncertainty and the art of public health messaging. Int J Epidemiol. 2013;42:1843–1845. doi: 10.1093/ije/dyt164.
117. Howard VJ, McDonnell MN. Physical activity in primary stroke prevention: just do it! Stroke. 2015;46:1735–1739. doi: 10.1161/STROKEAHA.115.006317.
118. Diep L, Kwagyan J, Kurantsin-Mills J, Weir R, Jayam-Trouth A. Association of physical activity level and stroke outcomes in men and women: a meta-analysis. J Womens Health (Larchmt). 2010;19:1815–1822. doi: 10.1089/jwh.2009.1708.
119. Li J, Siegrist J. Physical activity and risk of cardiovascular disease–a meta-analysis of prospective cohort studies. Int J Environ Res Public Health. 2012;9:391–407. doi: 10.3390/ijerph9020391.
120. Sofi F, Capalbo A, Cesari F, Abbate R, Gensini GF. Physical activity dur-ing leisure time and primary prevention of coronary heart disease: an updated meta-analysis of cohort studies. Eur J Cardiovasc Prev Rehabil. 2008;15:247–257. doi: 10.1097/HJR.0b013e3282f232ac.
121. Sattelmair J, Pertman J, Ding EL, Kohl HW III, Haskell W, Lee IM. Dose response between physical activity and risk of coronary heart dis-ease: a meta-analysis. Circulation. 2011;124:789–795. doi: 10.1161/CIRCULATIONAHA.110.010710.
122. Shiroma EJ, Lee IM. Physical activity and cardiovascular health: lessons learned from epidemiological studies across age, gender, and race/ethnicity. Circulation. 2010;122:743–752. doi: 10.1161/CIRCULATIONAHA.109.914721.
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from
William Herrington, Ben Lacey, Paul Sherliker, Jane Armitage and Sarah LewingtonAtherothrombotic Disease
Epidemiology of Atherosclerosis and the Potential to Reduce the Global Burden of
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 2016 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/CIRCRESAHA.115.3076112016;118:535-546Circ Res.
http://circres.ahajournals.org/content/118/4/535World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Researchin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on Novem
ber 8, 2017http://circres.ahajournals.org/
Dow
nloaded from
Related Documents