Prostate Cancer Enzalutamide Antitumour Activity Against Metastatic Castration-resistant Prostate Cancer Previously Treated with Docetaxel and Abiraterone: A Multicentre Analysis Klaus Brasso a, *, Frederik B. Thomsen a , Andres J. Schrader b , Sebastian C. Schmid c , David Lorente d , Margitta Retz c , Axel S. Merseburger e , Christoph A. von Klot e , Martin Boegemann f , Johann de Bono d a Copenhagen Prostate Cancer Centre, Department of Urology, Rigshospitalet, University of Copenhagen, Denmark; b Department of Urology, Ulm University Medical Centre, Ulm, Germany; c Urologische Klinik und Poliklinik, Technische Universita ¨t Mu ¨nchen, Munich, Germany; d Royal Marsden NHS Foundation Trust and The Institute of Cancer Research, Sutton, United Kingdom; e Department of Urology and Urological Oncology, Hannover Medical School, Hannover, Germany; f Department of Urology, Muenster University Medical Centre, Muenster, Germany E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X ava ilable at www.sciencedirect.com journa l homepage: www.europea nurology.com Article info Article history: Accepted July 21, 2014 Keywords: Castration-resistant prostate cancer Enzalutamide Abiraterone Docetaxel Survival PSA Abstract Background: The degree of antitumour activity of enzalutamide following disease progression on docetaxel and abiraterone remains controversial. Objective: To examine the effect of enzalutamide in patients progressing following taxane-based chemotherapy and abiraterone. Design, setting, and participants: Metastatic castration-resistant prostate cancer patients entering one of four European compassionate use programmes of enzalutamide. Outcome measurements and statistical analysis: The primary end point was overall survival (OS). Secondary end points were association between OS and posttreatment prostate-specific antigen (PSA) kinetics, patient characteristics, and progression-free survival, respectively. Kaplan-Meier survival analysis and Cox proportional hazard analysis were performed. Results and limitations: We identified 137 patients who prior to enzalutamide had progressed following a median of eight cycles of docetaxel and seven courses of abiraterone. The median time on enzalutamide was 3.2 mo; median OS from the time patients started enzalutamide was 8.3 mo (95% confidence interval, 6.8–9.8). Only 45 (38%) and 22 (18%) patients had PSA declines (unconfirmed) >30% and 50%, respectively. Patients who had more than 30% or 50% falls in PSA had improved survival compared with patients who had no such PSA fall (11.4 mo vs 7.1 mo; p = 0.001 and 12.6 vs 7.4 mo; p = 0.007, respectively). Poor performance status and low haemoglobin was negatively associated with OS. Conclusions: Median OS on enzalutamide following disease progression on taxane- based chemotherapy and abiraterone was modest, but patients who experience a PSA decline >30% or 50%, respectively, with enzalutamide in this setting had longer survival. Patient summary: Enzalutamide produces modest prostate-specific antigen (PSA) responses in patients progressing following chemotherapy and abiraterone. Despite a modest PSA response, survival may still be improved. # 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Copenhagen Prostate Cancer Centre, Rigshospitalet, Tagensvej 20, Afsnit 7521, Copenhagen N, DK-2200, Denmark. Tel. +45 35 457 125; Fax: +45 35 452 716. E-mail address: [email protected] (K. Brasso). EURURO-5754; No. of Pages 8 Please cite this article in press as: Brasso K, et al. Enzalutamide Antitumour Activity Against Metastatic Castration-resistant Prostate Cancer Previously Treated with Docetaxel and Abiraterone: A Multicentre Analysis. Eur Urol (2014), http://dx.doi.org/ 10.1016/j.eururo.2014.07.028 http://dx.doi.org/10.1016/j.eururo.2014.07.028 0302-2838/# 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EURURO-5754; No. of Pages 8
Prostate Cancer
Enzalutamide Antitumour Activity Against Metastatic
Castration-resistant Prostate Cancer Previously Treated with
Docetaxel and Abiraterone: A Multicentre Analysis
Klaus Brasso a,*, Frederik B. Thomsen a, Andres J. Schrader b, Sebastian C. Schmid c,David Lorente d, Margitta Retz c, Axel S. Merseburger e, Christoph A. von Klot e,Martin Boegemann f, Johann de Bono d
a Copenhagen Prostate Cancer Centre, Department of Urology, Rigshospitalet, University of Copenhagen, Denmark; b Department of Urology, Ulm University
Medical Centre, Ulm, Germany; c Urologische Klinik und Poliklinik, Technische Universitat Munchen, Munich, Germany; d Royal Marsden NHS Foundation
Trust and The Institute of Cancer Research, Sutton, United Kingdom; e Department of Urology and Urological Oncology, Hannover Medical School, Hannover,
Germany; f Department of Urology, Muenster University Medical Centre, Muenster, Germany
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X
ava i lable at www.sc iencedirect .com
journa l homepage: www.europea nurology.com
Article info
Article history:Accepted July 21, 2014
Keywords:
Castration-resistant prostate
cancer
Enzalutamide
Abiraterone
Docetaxel
Survival
PSA
Abstract
Background: The degree of antitumour activity of enzalutamide following diseaseprogression on docetaxel and abiraterone remains controversial.Objective: To examine the effect of enzalutamide in patients progressing followingtaxane-based chemotherapy and abiraterone.Design, setting, and participants: Metastatic castration-resistant prostate cancer patientsentering one of four European compassionate use programmes of enzalutamide.Outcome measurements and statistical analysis: The primary end point was overallsurvival (OS). Secondary end points were association between OS and posttreatmentprostate-specific antigen (PSA) kinetics, patient characteristics, and progression-freesurvival, respectively. Kaplan-Meier survival analysis and Cox proportional hazardanalysis were performed.Results and limitations: We identified 137 patients who prior to enzalutamide hadprogressed following a median of eight cycles of docetaxel and seven courses ofabiraterone. The median time on enzalutamide was 3.2 mo; median OS from the timepatients started enzalutamide was 8.3 mo (95% confidence interval, 6.8–9.8). Only 45(38%) and 22 (18%) patients had PSA declines (unconfirmed) >30% and 50%, respectively.Patients who had more than 30% or 50% falls in PSA had improved survival comparedwith patients who had no such PSA fall (11.4 mo vs 7.1 mo; p = 0.001 and 12.6 vs 7.4 mo;p = 0.007, respectively). Poor performance status and low haemoglobin was negativelyassociated with OS.Conclusions: Median OS on enzalutamide following disease progression on taxane-based chemotherapy and abiraterone was modest, but patients who experience a PSAdecline >30% or 50%, respectively, with enzalutamide in this setting had longer survival.Patient summary: Enzalutamide produces modest prostate-specific antigen (PSA)responses in patients progressing following chemotherapy and abiraterone. Despite amodest PSA response, survival may still be improved.
soc
. Copenhagen Prostate Cancer Centre, Rigshospitalet, Tagensvej 20,n N, DK-2200, Denmark. Tel. +45 35 457 125; Fax: +45 35 452 [email protected] (K. Brasso).
# 2014 European As
* Corresponding authorAfsnit 7521, CopenhageE-mail address: klausbr
Please cite this article in press as: Brasso K, et al. EnzalutamideProstate Cancer Previously Treated with Docetaxel and Abiratero10.1016/j.eururo.2014.07.028
http://dx.doi.org/10.1016/j.eururo.2014.07.0280302-2838/# 2014 European Association of Urology. Published by Elsevier
iation of Urology. Published by Elsevier B.V. All rights reserved.
Antitumour Activity Against Metastatic Castration-resistantne: A Multicentre Analysis. Eur Urol (2014), http://dx.doi.org/
B.V. All rights reserved.

Fig. 1 – Consolidated Standards of Reporting Trials diagram of prostate-specific antigen and radiographic responses following abirateroneacetate and enzalutamide.mCRPC = metastatic castration-resistant prostate cancer;PFS = progression-free survival; PSA = prostate-specific antigen.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X2
EURURO-5754; No. of Pages 8
1. Introduction
The introduction of new treatment options for patients who
have metastatic castration-resistant prostate cancer
(mCRPC) during the past decade has provided several
effective new therapeutic strategies, including two different
taxanes, a systemic alpha particle–emitting radionuclide, as
well as two novel endocrine drugs and a vaccine [1–8].
Because docetaxel had been shown to prolong survival [1,2],
first cabazitaxel [3] and more recently two new drugs—
blocking androgen synthesis through CYP17 inhibition and
the androgen receptor (AR), respectively—have been shown
to further improve survival in mCRPC patients both before
and after chemotherapy [5–8]. Abiraterone acetate, a
selective CYP17A1 inhibitor, blocks the synthesis of andro-
genic steroids, causing effective systemic and intratumoural
suppression of androgen production [9]. Enzalutamide is a
second-generation antiandrogen that binds to and blocks the
AR with higher affinity than previously available antiandro-
gens. Enzalutamide is also reported to inhibit AR nuclear
translocation and binding of the AR complex to DNA [10].
Abiraterone and enzalutamide can prolong survival by
4.6 mo and 4.8 mo, respectively, and produce significant
prostate-specific antigen (PSA) and objective responses in
mCRPC patients progressing after docetaxel [6,11].
This increasing number of new therapies has resulted in
a multiple unresolved issues regarding optimal timing,
sequencing, possible combinations, drug-resistance mech-
anisms, and cost. Recently, PSA response and survival
have been reported both in patients managed with
abiraterone following progression on docetaxel and enzalu-
tamide [12,13] and in patients managed with enzalutamide
following docetaxel and abiraterone [14–17]. All publica-
tions involve small patient numbers and retrospective case
series, and the all demonstrate modest PSA responses and
median survival compared with the randomised, placebo-
controlled COU-AA-301 and AFFIRM trials [6,11].
In this report, we present a pooled analysis of PSA
response and survival from four independent European
compassionate access programmes that provided enzaluta-
mide as third-line treatment to patients with mCRPC
following progression after docetaxel and abiraterone
treatment.
2. Materials and methods
The US Food and Drug Administration (FDA) approved enzalutamide for
postdocetaxel mCRPC patients who experienced disease progression
following publication of the AFFIRM trial [6]. In Europe, compassionate
use programmes were initiated to bridge the time between FDA and
European Medicines Agency approval. All programmes, from which we
derived the patients presented in this study, have been described in
details elsewhere [14–17]. Patients and clinical information included is
presented in the Consolidated Standards of Reporting Trials diagram
(Fig. 1). In brief, mCRPC patients progressing following chemotherapy
and subsequent abiraterone and prednisone were treated with 160 mg
enzalutamide daily in two German [14,15], one British [16], and one
Danish [17] compassionate use programme if considered candidates for
further therapy. All patients continued castration-based therapy during
enzalutamide.
Please cite this article in press as: Brasso K, et al. EnzalutamideProstate Cancer Previously Treated with Docetaxel and Abiratero10.1016/j.eururo.2014.07.028
Follow-up consisted of regular outpatient clinic visits with biochemi-
cal and clinical evaluations. Between trials, there were minor differences in
the imaging follow-up, and evaluation of progression based on
radiographic assessment or bone scans was not mandatory. For all
patients, the following pretreatment information was recorded, if
available: Gleason score at diagnosis; time from primary endocrine
treatment to CRPC; number of docetaxel cycles; time on and PSA response
to abiraterone; Eastern Cooperative Oncology Group (ECOG) performance
score; PSA; haemoglobin; albumin; lactate dehydrogenase (LDH); and
alkaline phosphatase (ALP). The primary end point was overall survival
(OS) calculated from initiation of enzalutamide; the secondary end point
was PSA response. Radiographic response and radiographic progression-
free survival (PFS) according to the Response Evaluation Criteria in Solid
Tumors (RECIST) criteria [18] were available only in a subgroup of patients.
2.1. Statistics
Continuous variables are presented as median and range. The best PSA
response was defined as percentage of change from baseline (start of
abiraterone or enzalutamide) to nadir. The first PSA measurement was
used in patients who had an increase in PSA. Patients were dichotomised
according to their best PSA response as nonresponders (continued PSA
progression) or responders (decrease or stabilised PSA). Furthermore,
patients responding were categorised according to the best PSA fall
reported: >30% and >50% falls (unconfirmed), respectively.
Survival was calculated from the date enzalutamide was initiated
using Kaplan-Meier survival analysis and presented with a 95%
confidence interval (CI). Log-rank analysis was used to compare survival
among subgroups. We used Cox proportional hazards to estimate the
effect of clinical pre-enzalutamide parameters as well as absolute and
percentage PSA response to enzalutamide on survival. No patient was
lost to follow-up. Two-sided p value <0.05 was considered significant.
Statistical analysis was performed with R (R Development Core Team,
Vienna, Austria, www.R-project.org).
Antitumour Activity Against Metastatic Castration-resistantne: A Multicentre Analysis. Eur Urol (2014), http://dx.doi.org/

Table 1 – Patient characteristics at enzalutamide initiation
No. of patients Median IQR Range No. %
Age, yr 137 71 67–74 57–85
ECOG status 96
0 12 12.5
1 56 58.3
2 28 29.2
PSA prior to enzalutamide, ng/ml 135 348 81.9–807.6 4.7–7342
Diagnostic Gleason score 106
6 11 10.4
7 30 28.3
8 18 17.0
9 43 40.6
10 4 3.8
Time from primary endocrine treatment to CRPC, yr 58 1.8 0.7–3.8 0.2–9.8
No. of docetaxel cycles received 99 8 6–10 1–39
Time on abiraterone acetate, mo 135 7 4–10.8 1.58–53.83
Best PSA response to abiraterone acetate 93
Continued PSA progression 26 28.0
Stable or decrease in PSA 67 72.0
PSA response >30% 54* 35 64.8
PSA response >50% 54* 23 45.6
Haemoglobin, mmol/l 63 6.8 6.2–7.5 5.2–11.7
Albumin, g/l 57 36 33–42 24–48
LDH, UI/l 47 246 178–377 86–897
ALP, UI/l 63 138 78–376 29–2066
ALP = alkaline phosphatase; CRPC = castration-resistant prostate cancer; ECOG = Eastern Cooperative Oncology Group; IQR = interquartile range; LDH = lactate
dehydrogenase; PSA = prostate-specific antigen.* Exact PSA response available in only 54 of 93 patients.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 3
EURURO-5754; No. of Pages 8
3. Results
Prior to initiation of 160 mg/d of enzalutamide, the 137
patients included in this study had received a median of
eight courses of docetaxel and had subsequently received
abiraterone plus prednisone for a median of 7 mo (Table 1;
Supplemental Table 1). Of the 137 patients, information
about PSA response with prior abiraterone was available in
94 patients, of whom 32 had PSA progression and 62 were
categorised as PSA nonprogression.
Fig. 2 – Waterfall plot of best percentage change in prostate-specific antigen (Pexcluded because of unknown first PSA measurement.PSA = prostate-specific antigen.
Please cite this article in press as: Brasso K, et al. EnzalutamideProstate Cancer Previously Treated with Docetaxel and Abiratero10.1016/j.eururo.2014.07.028
The median duration of enzalutamide treatment until
clinical progression was 3.2 mo (range: 0.03–21.9). At the
time of these analyses, 14 patients were still being treated
with enzalutamide. PSA information following enzalutamide
initiation was available in 122 patients (Fig. 1). Among these
122 patients, 44 (36%) had PSA progression (nonresponders),
and the remaining 78 (64%) patients had decreased or
stabilised PSA (nonprogression, described here as responders;
Fig. 2). Forty-five (36.9%) patients had a PSA fall (uncon-
firmed) >30% and 22 (18.0%) patients >50%, respectively.
SA) from baseline. Twelve patients who had an increase in PSA were
Antitumour Activity Against Metastatic Castration-resistantne: A Multicentre Analysis. Eur Urol (2014), http://dx.doi.org/

Table 2 – Univariate Cox proportional hazard analysis between pre-enzalutamide parameters and survival
Patients who have valid information HR 95% CI p value
Age* 137 0.98 0.95–1.01 0.13
ECOG 96 0.07
0 1 (ref)
1 3.00 0.92–9.80
2 3.41 1.01–11.5
PSA** 135 1.10 0.99–1.22 0.08
Diagnostic Gleason score 104 0.77
6 1 (ref)
7 0.71 0.29–1.72
8 0.85 0.33–2.20
9 0.89 0.38–2.06
10 1.55 0.40–6.03
Time from primary endocrine treatment to CRPC* 58 0.91 0.76–1.09 0.29
No. of docetaxel series*** 99 1.02 0.98–1.07 0.36
Time on abiraterone acetatey 135 0.99 0.97–1.02 0.66
PSA response to abiraterone acetate 93
Increase in PSA 1 (ref)
Stable or decrease in PSA 0.88 0.50–1.56 0.67
Haemoglobinyy 63 1.50 1.05–2.12 0.02
Albuminyyy 57 0.74 0.38–1.43 0.37
LDHyyy 47 0.99 0.98–1.02 0.68
ALPyyy 63 1.01 1.00–1.01 0.02
ALP = alkaline phosphatase; CI = confidence interval; CRPC = castration-resistant prostate cancer; ECOG = Eastern Cooperative Oncology Group; HR = hazard
ratio; LDH = lactate dehydrogenase; PSA = prostate-specific antigen.* 1-yr increase.** A 2-fold increase.*** 1 series increase.y 1-mo increase.yy 1-mmol/l decrease.yyy 10-unit increase.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X4
EURURO-5754; No. of Pages 8
Overall, the estimated median survival was 8.3 mo (95%
CI, 6.8–9.8) for the 137 patients. On univariate analysis,
pretreatment clinical characteristics had little or no
influence on survival (Table 2). Patients who had an ECOG
score of 2 had a higher mortality than patients who had
ECOG 0 (hazard ratio [HR]: 3.41; 95% CI, 1.01–11.5), but
Fig. 3 – Kaplan-Meier survival curves for the 110 patients who had valid perceinto quartiles. Twelve patients who had an increase in PSA were excluded becaPSA = prostate-specific antigen.
Please cite this article in press as: Brasso K, et al. EnzalutamideProstate Cancer Previously Treated with Docetaxel and Abiratero10.1016/j.eururo.2014.07.028
there was no survival difference between patients with
ECOG score 1 and ECOG score 2. A 1 mmol/l decrease in
haemoglobin was associated with an increased mortality
(HR: 1.50; 95% CI, 1.05–2.12). A 10-unit increase in ALP
concentration at enzalutamide initiation had a statistically
significant association with increased mortality (HR: 1.01;
ntage prostate-specific antigen (PSA) response to enzalutamide stratifieduse of unknown first PSA measurement.
Antitumour Activity Against Metastatic Castration-resistantne: A Multicentre Analysis. Eur Urol (2014), http://dx.doi.org/
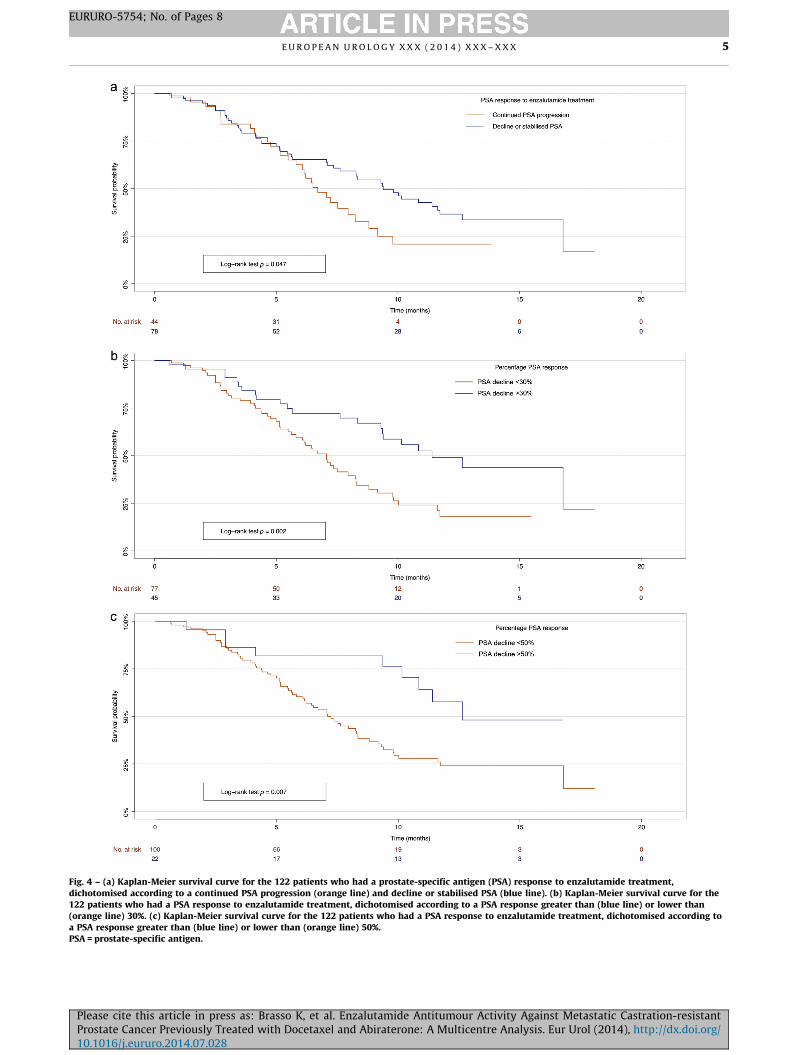
Fig. 4 – (a) Kaplan-Meier survival curve for the 122 patients who had a prostate-specific antigen (PSA) response to enzalutamide treatment,dichotomised according to a continued PSA progression (orange line) and decline or stabilised PSA (blue line). (b) Kaplan-Meier survival curve for the122 patients who had a PSA response to enzalutamide treatment, dichotomised according to a PSA response greater than (blue line) or lower than(orange line) 30%. (c) Kaplan-Meier survival curve for the 122 patients who had a PSA response to enzalutamide treatment, dichotomised according toa PSA response greater than (blue line) or lower than (orange line) 50%.PSA = prostate-specific antigen.
E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 5
EURURO-5754; No. of Pages 8
Please cite this article in press as: Brasso K, et al. Enzalutamide Antitumour Activity Against Metastatic Castration-resistantProstate Cancer Previously Treated with Docetaxel and Abiraterone: A Multicentre Analysis. Eur Urol (2014), http://dx.doi.org/10.1016/j.eururo.2014.07.028

E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X6
EURURO-5754; No. of Pages 8
95% CI, 1.00–1.01), although this finding is of limited clinical
relevance. A borderline significant association between PSA
at enzalutamide initiation and survival was found (HR:
1.10; 95% CI, 0.99–1.22), although again, the clinical
relevance of this finding is uncertain. Survival was not
associated with age ( p = 0.13), albumin ( p = 0.37); LDH
( p = 0.68) at enzalutamide initiation; Gleason score at
diagnosis ( p = 0.77); time from primary endocrine treat-
ment to CRPC ( p = 0.29); number of docetaxel courses
( p = 0.36); or time on or PSA response to abiraterone
( p = 0.66 and p = 0.67, respectively). Assessment by RECIST
criteria was not performed in all compassionate use
programmes.
Responses according to RECIST criteria were reported
in 59 patients [14,16]. Overall, only seven of these patients
had a radiographic response to enzalutamide resulting in a
partial remission according to the RECIST criteria. No
patients experienced complete remissions. The median
duration of radiographic PFS in the 34 patients who
underwent regular radiographic follow-up was 3.1 mo
(95% CI, 2.3–3.9) [15,16].
In univariate analysis, a 10% lower PSA response was
associated with an increased risk of death (HR: 1.07; 95% CI,
1.03–1.10; p < 0.001). Kaplan-Meier survival curves strat-
ified into quartiles according to the best PSA response are
depicted in Figure 3. No association between the absolute
PSA decline and survival was found in univariate analysis
(HR: 1.003; 95% CI, 0.996–1.01; p = 0.37). Patients pre-
senting with stable or declining PSA following enzaluta-
mide had a median survival of 9.4 mo (95% CI, 7.5–11.3)
compared with 6.7 mo (95% CI, 5.5–7.9) in patients who had
PSA progression ( p = 0.047; Fig. 4a). Patients who had a PSA
fall >30% had a median survival of 11.4 mo (95% CI,
8.0–14.8) compared with 7.1 mo (95% CI, 5.9–8.2) in
patients who had a PSA decline <30% ( p = 0.002; Fig. 4b).
Patients who had a �50% fall in PSA had a median survival
of 12.6 mo (undefined 95% CI) compared with 7.4 mo (95%
CI, 6.1–8.6) for patients who had a PSA response <50%
( p = 0.007; Fig. 4c). Finally, there were no major differences
in pre-enzalutamide characteristics among patients who
had a PSA response >30% compared with those patients
who had a lower response (Supplemental Table 2).
4. Discussion
Since the introduction of docetaxel, mCRPC has been
artificially divided into a prechemotherapy and a post-
chemotherapy disease state for regulatory reasons. AR
signalling remains a key driver of progression during
mCRPC, despite testosterone at castration levels in both
of these disease states [19]. New therapeutic modalities
targeting the AR have been successfully developed and are
currently being introduced for both pre- and postche-
motherapy mCRPC. With the introduction of these new
treatment options, the questions of optimal timing, patient
selection, sequencing, and the development of drug
resistance have been heavily debated.
In vitro experiments have also demonstrated impaired
antitumour activity of taxanes in cell lines resistant to
Please cite this article in press as: Brasso K, et al. EnzalutamideProstate Cancer Previously Treated with Docetaxel and Abiratero10.1016/j.eururo.2014.07.028
next-generation AR-targeting drugs [20]. This finding may
reflect the taxane mode of action, which involves the AR
pathway through the role of microtubules on AR nuclear-
cytoplasmic shuttling or may be the result of up-regulation
of other antiapoptotic mechanisms [21,22]. The response to
enzalutamide has also been reported to be affected by
glucocorticoid receptor signalling in preclinical studies,
although limited clinical data are available to support this
hypothesis to date [23]. Arora et al. indicate that exposure to
enzalutamide in a preclinical model of prostate cancer
induces glucocorticoid receptor up-regulation leading to
the development of enzalutamide resistance.
Compared with the AFFIRM trial [6], the data from the
compassionate use programmes pooled in this study
indicate more modest antitumour activity for enzalutamide
in postchemotherapy mCRPC patients previously treated
with abiraterone [14–17]. The antitumour activity of
abiraterone following both docetaxel and enzalutamide
has similarly been reported to be modest compared with
COU-AA-301 [11–13]. Mezynski et al. have also shown a
lower antitumour activity for docetaxel in patients previ-
ously managed with abiraterone [24]. Nevertheless, our
results indicate that a subset of patients previously
managed with docetaxel and abiraterone who responded
with nonincreasing or decreasing PSA following enzaluta-
mide may have improved OS. In univariate analysis, PSA
declines were associated with improved survival; further
analysis stratifying by response in patients who had no PSA
increase, a 30% decrease, and a 50% decrease in PSA
following initiation of enzalutamide, respectively, demon-
strated longer survival compared with patients who
experienced increasing PSA, <30% decrease, or a 50%
decrease, respectively. Studies applying the Prostate Cancer
Working Group 2 guidelines and implementing regular
imagining should be performed to confirm these findings.
Patients benefiting from enzalutamide may therefore be
those who have a PSA response to this agent, while patients
who have a poorer PSA response could benefit from other
treatment options. Overall, the biochemical activity of
enzalutamide after abiraterone and docetaxel may be
higher than that of abiraterone following progression on
docetaxel and enzalutamide [12,13]. Randomised clinical
trials are, however, now required to address the optimal
sequences or combinations for the administration of these
novel agents.
Lower haemoglobin and ECOG score 2 were both
associated with poorer prognosis in univariate analysis.
Patients who had a PSA >30% had significantly higher
baseline haemoglobin and a trend towards better ECOG
scores (Supplemental Table 2). These differences in baseline
parameters may partly explain the survival benefit seen in
patients who have a better PSA response. Survival following
initiation of enzalutamide was not associated with evalu-
ated pretreatment characteristics—time to CRPC, the PSA
response, and duration of prior chemotherapy and abir-
aterone or age.
This preliminary report of PSA response to enzalutamide
treatment in mCRPC patients progressing after postche-
motherapy abiraterone has obvious limitations. First, it is a
Antitumour Activity Against Metastatic Castration-resistantne: A Multicentre Analysis. Eur Urol (2014), http://dx.doi.org/

E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X 7
EURURO-5754; No. of Pages 8
retrospective study; baseline characteristics are incom-
pletely recorded, with differences among the four centres;
and the patients have not been followed systematically by
protocol. The number of patients is limited, and the study
lacks information about PSA kinetics and parameters other
than PSA to monitor the response of enzalutamide
treatment. Bone scans and radiographic evaluation was
performed only if clinically indicated; radiographic re-
sponse in accordance with the RECIST criteria was recorded
only in a subset of patients [18]. Of the patients included in
the present study, only 36.9% and 18.0% responded with a
PSA decline of 30% and 50%, respectively. However, the
combined analyses demonstrate that despite a modest PSA
response, with only a limited number of patients reaching a
PSA response �30%, a survival benefit was demonstrated in
patients who did not have a rising PSA following the
introduction of enzalutamide.
5. Conclusions
This study presents data from four European studies on
compassionate-access enzalutamide for mCRPC patients
progressing following docetaxel and abiraterone. We
demonstrate that enzalutamide, when administered as a
third-line treatment, has more modest antitumour activity
than that reported in the AFFIRM trial. Nonetheless, patients
who had a PSA decline >30% and 50% have superior survival
and may benefit from this agent. With the increasing
number of treatment options available for patients who
have mCRPC, well-conducted studies determining the
optimal treatment sequence or combination of these drugs
are urgently needed to base future treatment algorithms on
solid evidence.
Author contributions: Klaus Brasso had full access to all the data in the
study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Brasso, Thomsen, Schmid, Merseburger,
de Bono.
Acquisition of data: Brasso, Thomsen, Schrader, Schmid, Lorente, Retz,
Merseburger, von Klot, Boegemann, de Bono.
Analysis and interpretation of data: Brasso, Thomsen, Schrader, Schmid,
Lorente, Retz, Merseburger, von Klot, Boegemann, de Bono.
Drafting of the manuscript: Brasso, Thomsen.
Critical revision of the manuscript for important intellectual content:
Schrader, Schmid, Lorente, Retz, Merseburger, von Klot, Boegemann,
de Bono.
Statistical analysis: Brasso, Thomsen.
Obtaining funding: None.
Administrative, technical, or material support: None.
Supervision: Brasso.
Other (specify): None.
Financial disclosures: Klaus Brasso certifies that all conflicts of interest,
including specific financial interests and relationships and affiliations
relevant to the subject matter or materials discussed in the manuscript
(eg, employment/affiliation, grants or funding, consultancies, honoraria,
stock ownership or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: Klaus Brasso received
consulting fees from Astellas, Bayer AG, and Sanofi-Aventis as well as
lecture fees from Ferring and Sanofi-Aventis. Andres J. Schrader received
Please cite this article in press as: Brasso K, et al. EnzalutamideProstate Cancer Previously Treated with Docetaxel and Abiratero10.1016/j.eururo.2014.07.028
consulting and lecture fees from Astellas Pharma GmbH, Janssen-Cilag
GmbH, Pfizer GmbH, Bayer AG, GlaxoSmithKline, Novartis, Medac, Ipsen
Pharma, and Sanofi-Aventis. Sebastian Schmid received lecture fees from
Astellas Pharma GmbH and travel grants from GlaxoSmithKline GmbH &
Co. KG. Margitta Retz received lecture fees and honoraria from Astellas
Pharma GmbH, Janssen-Cilag GmbH, Pfizer GmbH, Bayer AG, and
GlaxoSmithKline GmbH & Co. KG. Alex Merseburger received lecture fees
and honoraria from Astellas Pharma GmbH, Janssen-Cilag GmbH, Novartis
Pharma, Pfizer GmbH, Bayer AG, and GlaxoSmithKline GmbH & Co. KG.
Martin Boegemann received lecture fees and honoraria from Astellas
Pharma GmbH, Janssen-Cilag GmbH, Pfizer GmbH, Bayer AG, Teva GmbH,
and GlaxoSmithKline GmbH & Co. KG. Johann de Bono received consulting
fees from Ortho Biotech Oncology Research and Development (a unit of
Cougar Biotechnology); consulting fees and travel support from Amgen,
Astellas, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb,
Dendreon, Enzon, Exelixis, Genentech, GlaxoSmithKline, Medivation,
Merck, Novartis, Pfizer, Roche, Sanofi-Aventis, Supergen, and Takeda;
and grant support from AstraZeneca and Genentech.
Funding/Support and role of the sponsor: None.
Appendix A. On behalf of national enzalutamide study
groups
Denmark: M.A. Røder 1, P. Rathenborg 2, M. Borre 3,
P. Iversen 1
Germany: C.H. Ohlmann 5, T.J. Schnoeller 6, L.M. Krabbe 4,
T. Hajili 7, F. Jentzmik 6, M. Stoeckle 5, M. Schrader 6,
E. Hermann 4, M.V. Cronauer 6, A. Geith 7, A. Boker 8,
R. Tauber 7, A.K. Seitz 7, M. Kuczyk 8, J.E. Gschwend 7
United Kingdom: D. Bianchini 9, A. Rodriquez-Vida 10,
A. Omlin 9, C. Pezaro 9, R. Ferraldeschi 9, A. Zivi 9, G. Attard 9,
S. Chowdhury 10
1 Copenhagen Prostate Cancer Center, Department
of Urology, Rigshospitalet, University of Copenhagen,
Copenhagen, Denmark2 Department of Urology, Herlev Hospital, Copenhagen
University Hospital, Copenhagen, Denmark3 Department of Urology, Aarhus University Hospital,
Skejby, Denmark4 Department of Urology, Muenster University Medical
Center, Muenster, Germany5 Department of Urology, Saarland University Medical
Center, Hamburg/Saar, Germany6 Department of Urology, Ulm University Medical Center,
Ulm, Germany7 Urologische Klinik und Poliklinik, Technischen Universitat
Munchen, Munich, Germany8 Department of Urology and Urological Oncology, Hann-
over Medical School, Hannover, Germany9 Royal Marsden NHS Foundation Trust and The Institute of
Cancer Research, Sutton, United Kingdom10 Guy’s and St Thomas’ NHS Foundation Trust, London,
United Kingdom
Appendix B. Supplementary data
Supplementary data associated with this article can be
found, in the online version, at http://dx.doi.org/10.1016/
j.eururo.2014.07.028.
Antitumour Activity Against Metastatic Castration-resistantne: A Multicentre Analysis. Eur Urol (2014), http://dx.doi.org/

E U R O P E A N U R O L O G Y X X X ( 2 0 1 4 ) X X X – X X X8
EURURO-5754; No. of Pages 8
References
[1] Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or
mitoxantrone plus prednisone for advanced prostate cancer. N Engl
J Med 2004;351:1502–12.
[2] Petrylak DP, Tangen CM, Hussain MHA, et al. Docetaxel and
estramustine compared with mitoxantrone and prednisone for
advanced refractory prostate cancer. N Engl J Med 2004;351:
1513–20.
[3] De Bono JS, Oudard S, Ozguroglu M, et al. Prednisone plus cabazi-
taxel or mitoxantrone for metastatic castration-resistant prostate
cancer progressing after docetaxel treatment: a randomised open-
label trial. Lancet 2010;376:1147–54.
[4] Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunother-
apy for castration-resistant prostate cancer. N Engl J Med 2010;363:
411–22.
[5] De Bono JS, Logothetis CJ, Molina A, et al. Abiraterone and increased
survival in metastatic prostate cancer. N Engl J Med 2011;364:
1995–2005.
[6] Scher HI, Fizazi K, Saad F, et al. Increased survival with enzalutamide
in prostate cancer after chemotherapy. N Engl J Med 2012;367:
1187–97.
[7] Ryan CJ, Smith MR, de Bono JS, et al. Abiraterone in metastatic
prostate cancer without previous chemotherapy. N Engl J Med
2013;368:138–48.
[8] Beer TM, Armstrong AJ, Sternberg CN, et al. Enzalutamide in men
with chemotherapy-naive metastatic prostate cancer (mCRPC):
results of phase III PREVAIL study [abstract]. J Clin Oncol 2014;32
(Suppl 4).
[9] Ang JE, Olmos D, de Bono JS. CYP17 blockade by abiraterone: further
evidence for frequent continued hormone-dependence in castration-
resistant prostate cancer. Br J Cancer 2009;100:671–5.
[10] Tran C, Ouk S, Clegg NJ, et al. Development of a second-generation
antiandrogen for treatment of advanced prostate cancer. Science
2009;324:787–90.
[11] Fizazi K, Scher HI, Molina A, et al. Abiraterone acetate for treatment
of metastatic castration-resistant prostate cancer: final overall
survival analysis of the COU-AA-301 randomised, double-blind,
placebo-controlled phase 3 study. Lancet Oncol 2012;13:983–92.
[12] Loriot Y, Bianchini D, Ileana E, et al. Antitumour activity of abirater-
one acetate against metastatic castration-resistant prostate cancer
Please cite this article in press as: Brasso K, et al. EnzalutamideProstate Cancer Previously Treated with Docetaxel and Abiratero10.1016/j.eururo.2014.07.028
progressing after docetaxel and enzalutamide (MDV3100). Ann
Oncol 2013;24:1807–12.
[13] Noonan KL, North S, Bitting RL, Armstrong AJ, Ellard SL, Chi KN.
Clinical activity of abiraterone acetate in patients with metastatic
castration-resistant prostate cancer progressing after enzaluta-
mide. Ann Oncol 2013;24:1802–7.
[14] Schrader AJ, Boegemann M, Ohlmann C-H, et al. Enzalutamide in
castration-resistant prostate cancer patients progressing after doc-
etaxel and abiraterone. Eur Urol 2014;65:30–6.
[15] Schmid SC, Geith A, Boker A, et al. Enzalutamide after docetaxel and
abiraterone therapy in metastatic castration-resistant prostate
cancer. Adv Ther 2014;31:234–41.
[16] Bianchini D, Lorente D, Rodriguez-Vida A, et al. Antitumour activity
of enzalutamide (MDV3100) in patients with metastatic castration-
resistant prostate cancer (CRPC) pre-treated with docetaxel and
abiraterone. Eur J Cancer 2014;50:78–84.
[17] Thomsen FB, Røder MA, Rathenborg P, Brasso K, Borre M, Iversen P.
Enzalutamide treatment in patients with metastatic castration-
resistant prostate cancer progressing after chemotherapy and abir-
aterone acetate. Scand J Urol 2014;48:268–75.
[18] Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evalua-
tion criteria in solid tumours: revised RECIST guideline (version
1.1). Eur J Cancer 2009;45:228–47.
[19] Schalken JA. Molecular aspects of hormone-independent prostate
cancer. BJU Int 2007;100(Suppl 2):52–5.
[20] Van Soest RJ, van Royen ME, de Morree ES, et al. Cross-resistance
between taxanes and new hormonal agents abiraterone and enza-
lutamide may affect drug sequence choices in metastatic castration-
resistant prostate cancer. Eur J Cancer 2013;49:3821–30.
[21] Zhu M-L, Horbinski CM, Garzotto M, Qian DZ, Beer TM, Kyprianou N.
Tubulin-targeting chemotherapy impairs androgen receptor activ-
ity in prostate cancer. Cancer Res 2010;70:7992–8002.
[22] Thadani-Mulero M, Nanus DM, Giannakakou P. Androgen receptor
on the move: boarding the microtubule expressway to the nucleus.
Cancer Res 2012;72:4611–5.
[23] Arora VK, Schenkein E, Murali R, et al. Glucocorticoid receptor
confers resistance to antiandrogens by bypassing androgen recep-
tor blockade. Cell 2013;155:1309–22.
[24] Mezynski J, Pezaro C, Bianchini D, et al. Antitumour activity of doc-
etaxel following treatment with the CYP17A1 inhibitor abiraterone:
clinical evidence for cross-resistance? Ann Oncol 2012;23:2943–7.
Antitumour Activity Against Metastatic Castration-resistantne: A Multicentre Analysis. Eur Urol (2014), http://dx.doi.org/
Related Documents











