ENT Procedures Jason Fowler, MPAS, PA-C Jose C. Mercado, MMS, PA-C April 26-28, 2013 New York-Presbyterian Hospital/Weill Cornell Medical Center

ENT Procedures Jason Fowler, MPAS, PA-C Jose C. Mercado, MMS, PA-C April 26-28, 2013 New York-Presbyterian Hospital/Weill Cornell Medical Center.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ENT ProceduresJason Fowler, MPAS, PA-C
Jose C. Mercado, MMS, PA-C
April 26-28, 2013New York-Presbyterian Hospital/Weill Cornell
Medical Center
ENT Procedures Workshop
Basic instruction
Clear demonstration
Hands-on doing!
Removal Foreign Body (Nose)
Control Anterior Epistaxis
Control Posterior Epistaxis Fine Needle Aspiration
Peritonsillar Abscess Tracheostomy Care

Introduction
There are multiple methods and techniques available to successfully complete all the
topics presented in this workshop. Some are based on patient request, available
equipment or supervising physician’s preference.
The goal of this workshop is to correctly demonstrate the most common methods and give participants time for hands on
training.
ENT Procedures WorkshopLearning Objectives
• Discuss indications for and practice removal nasal foreign body.
• Discuss indications for and practice control anterior epistaxis.
• Discuss indications for and practice control posterior epistaxis.
• Discuss indications for and practice fine needle aspiration.• Discuss indications for and practice peritonsillar abscess
drainage.• Discuss indications for tracheostomy and practice
tracheostomy care.

• Purulent unilateral nasal discharge, especially in children
• Usually lodge on the floor of anterior or middle third
Figure. A: Fiberoptic nasal endoscopy shows the mass in the left anterior nasal cavity.
B: Coronal CT shows the area of attenuation in the left inferior turbinate.
C: Photograph shows the broken mass. D: Following removal of the mass, the
passageway is clear.
Removal Foreign Body (Nose)
Mercado, JC, Goldberg SG, Recurrent purulent rhinorrhea in an otherwise healthy woman Ear Nose Throat J. 2004 Jun;83(6):381-2

Removal Foreign Body (Nose)
Good visualization: headlamp & nasal speculum
Alligator forceps should be used to remove cloth, cotton, or paper
Other hard FB are more easily grasped using bayonet forceps or Kelly clamps, or they may be rolled out by getting behind it using an ear curette, single skin hook, or right angle ear hook
Practice mannequins available to practice
removal of nasal foreign bodies technique.

Control Anterior Epistaxis

Control Anterior Epistaxis
Control anterior epistaxis in office.
Apply direct manual pressure for at least 10
minutes
Mercado 2011 ©Mercado 2011 ©

Anterior vs PosteriorEpistaxis
Kiesslebach’s Plexus or Little’s Area is most common site of anterior nosebleeds.Woodruff’s Plexus is most
common site for posterior nose bleeds and may represent a lesion.
Sphenopalatine artery is generally the source of severe posterior nosebleeds.
Posterior more difficult to control will be discussed in Advanced ENT Procedures
Workshop.

Etiology of Epistaxis
Local
Trauma /Nose picking or blowing / surgery
Dry air / Irritants
Topical medications (steroids)
Foreign body
Tumor
Systemic
Bleeding disorders
Hereditary hemorrhagic telangiectasia
Drugs (anticoagulants)
Hypertension

Direct Manual Pressure
NO YESNO
Mercado 2011 ©Mercado 2011 © Mercado 2011 ©

Control Anterior Epistaxis
Spray or apply topical anesthetic with decongestant.
Reapply direct manual pressure an additional 10 minutes.
Mercado 2011 ©

Control Anterior Epistaxis
Once bleeding has subsided, identify
site of nosebleed.
Mercado 2011 ©

Control Anterior Epistaxis
Control bleeding with silver nitrate cauterization. (start from outside in)
Caution bilateral cauterization as may result in septal perforation.
Mercado 2011 ©

Control Anterior Epistaxis
Lubricate naris with Vaseline or Neosporin ointment.
Let sit for 10-15 minutes to ensure hemostasis is achieved.
Keep cotton in nares for at least 1 hour to prevent staining.
Avoid sneezing, forceful nose blowing, nose picking, etc.
Follow up 2 weeks as re-cauterization may be necessary.
Post chemical cauterization stain day 1
Mercado 2011 ©
Post chemical cauterization stain day 4
Mercado 2011 ©

Anterior Nasal Packing
Nasal packing• Absorbable gelfoam• Vasaline guaze• Nasal tampon• Anterior packing
Mercado 2011 ©

Anterior Nasal Packing
Nasal packing• Vaseline gauze – is
inserted along floor of naris to form a tight seal.

Mercado 2011 ©
Anterior Nasal Packing
Nasal packing• Nasal tampon –
expands in nasal cavity to form a tight seal.
• Do not allow packing to moisten until in position.
• Removal may cause re-bleeding.
Mercado 2011 ©

Anterior Nasal Tampon
• Insert nasal tampon horizontally.
• Lubricate with Neosporin but DO NOT moisten!
• Secure ties to cheek.
Practice mannequins available to practice anterior nasal packing
technique.
Mercado 2011 ©

Anterior Nasal Packing
Anterior nasal packing – Easy to insert and
remove due to self-lubricating hydrocolloid fabric and ultra-low profile.
– Packing quickly conforms to nasal anatomy and provides gentle and even compression to areas of epistaxis.
Mercado 2011 ©

Anterior Nasal Packing
• Soak dressing to hydrate Gel Knit hydrocolloid fabric in sterile water for 30 seconds.
• Insert Rapid Rhino horizontally.
• Inflate balloon only with air.
• Tape pilot cuff to side of face.
Mercado 2011 ©
Mercado 2011 ©

How NOT to pack a nose!!!

Control Posterior Epistaxis

Anterior vs PosteriorEpistaxis
Kiesslebach’s Plexus or Little’s Area is most common site of anterior nosebleeds.Woodruff’s Plexus is most common site for posterior nose
bleeds and may represent a lesion. Sphenopalatine artery is generally the source of severe
posterior nosebleeds.
Posterior tend to be more difficult to control and may suggest an underlying etiology.

Etiology of Epistaxis
Local
Trauma (Nose picking or blowing)
Dry air / Irritants
Topical medications (steroids)
Foreign body
Tumor / polyp
Surgery
Systemic
Hypertension
Coagulopathies
Hereditary hemorrhagic telangiectasia
Drugs (anticoagulants)
Control Posterior Epistaxis• Control Hypertension• Identify Coagulopathy –Treat with FFP,
transfusions, etc– PT, PTT, INR
• Coumadin toxicity - Vitamin K• Posterior Packing• Endoscopic Cauterization• Arterial Embolization (Interventional Radiology)

Posterior Nasal Packing
• Topical anesthetic & decongestant
• Posterior nasal packing – Foley catheter– Double balloon
device

Rapid Rhino® 900 for Posterior Epistaxis
1. Thoroughly soak in sterile water for 30 seconds.
2. Insert Rapid Rhino into the patient’s nostril parallel to the septal floor, or following along the superior aspect of the hard palate, until the blue indicator ring is inside the opening of the nostril.
3. Using a 20 cc syringe, slowly inflate the posterior (green stripe) balloon first with air only inside the patient’s nose.
1 2 3

4 5 6
4. Inflate second balloon with air.
5. Allow the patient to sit for 15-20 minutes prior to discharge. Swelling in the nasal anatomy will reduce and the balloons may need to be inflated more to avoid movement of the device. Don’t forget prophylaxis antibiotics!
6. To remove packing, deflate balloons 24-72 hours later.
Rapid Rhino® 900 for Posterior Epistaxis
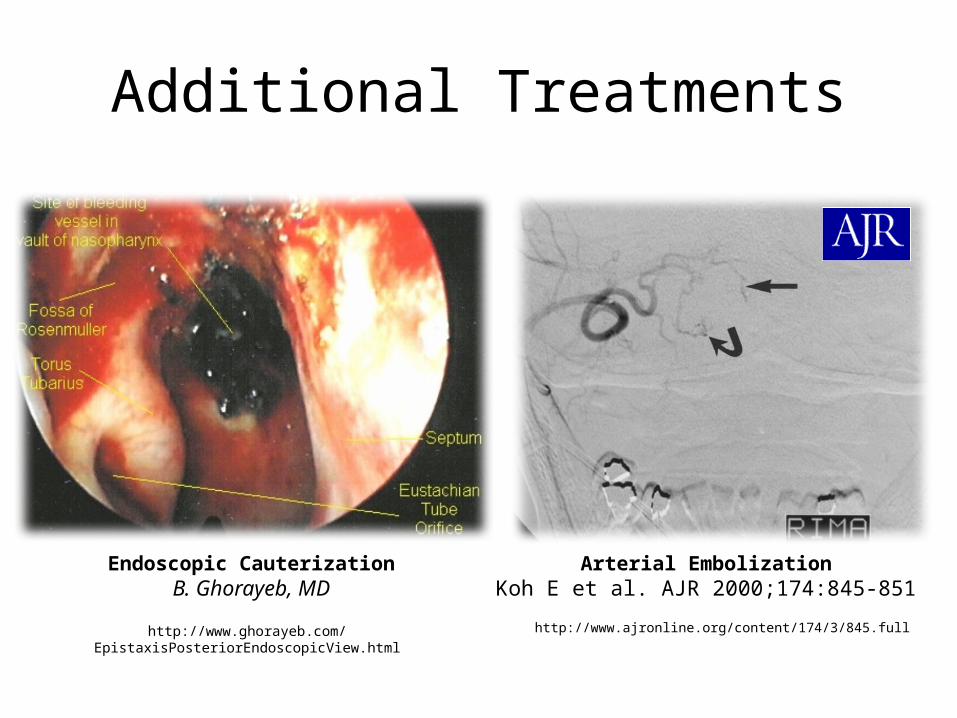
Additional Treatments
Arterial EmbolizationKoh E et al. AJR 2000;174:845-851
http://www.ajronline.org/content/174/3/845.fullhttp://www.ghorayeb.com/EpistaxisPosteriorEndoscopicView.html
Endoscopic CauterizationB. Ghorayeb, MD

Control Posterior Epistaxis
Practice mannequins available to practice
posterior nasal packing technique.
Mercado 2011 ©

Fine Needle Aspiration

Site Selection
Common sites include thyroid and parotid glands as well as lymph nodes.
Mercado 2011 © Mercado 2011 © Mercado 2011 ©

Anesthesia
• For superficial aspirates, clean technique suffices for cleansing of the skin surface.
• Local anesthetic may or may not be used. If more than two or three attempts are anticipated, this is recommended.
• However, be certain not to contaminate the lesion with a large volume of anesthetic.
• Also, make attempts not to directly interfere with the ability to palpate and localize the lesion.
• For deep aspirates, sterile technique is required for cleansing of the skin and local anesthetic is usually required.

Fine Needle Aspiration• Use a 3, 5, 10 or 20 mL syringe. Use of a “Syringe Pistol” is optional. • Needle should be at least 1 ½ inch or appropriate length and be 22 to
25 gauge. • Single end label clear glass slides (for preparation of direct smears).• Fixative to preserve fixed slides (either Cytology spray fixative,
Saccomanno fixative or 95% ethyl alcohol in coplin jar).
Mercado 2011 ©

Fine Needle AspirationPalpate and identify mass or lesion.
Clean topically with alcohol.
Stabilize the mass with non-dominant hand.
Insert needle through the skin with a quick motion.
Mercado 2011 ©Mercado 2011 ©

Fine Needle Aspiration• Advance through the subcutaneous
tissue into the mass. Aim needle toward the center of small masses but toward the periphery of larger masses as the center may be necrotic.
• A noticeable difference in the consistency of the tissue should be noted when the needle penetrates the mass.
• With the needle in the mass, the needle tip should be moved in short motions initially to loosen cells within the mass.
• Pull back on plunger to create negative pressure. Fowler 2011 ©

Fine Needle Aspiration• Without releasing pressure, withdraw
the needle within the target slightly then reinsert at a slightly different angle.
• Repeat maneuver several times before complete withdrawal. May also perform a corkscrew action before withdrawal.
• If blood or material appears in the hub of the needle, the aspiration should be stopped.
• Release negative pressure before withdrawing the needle, negative pressure must be released to prevent suction of the material into the barrel of the syringe when the needle exits the skin.
Fowler 2011 ©
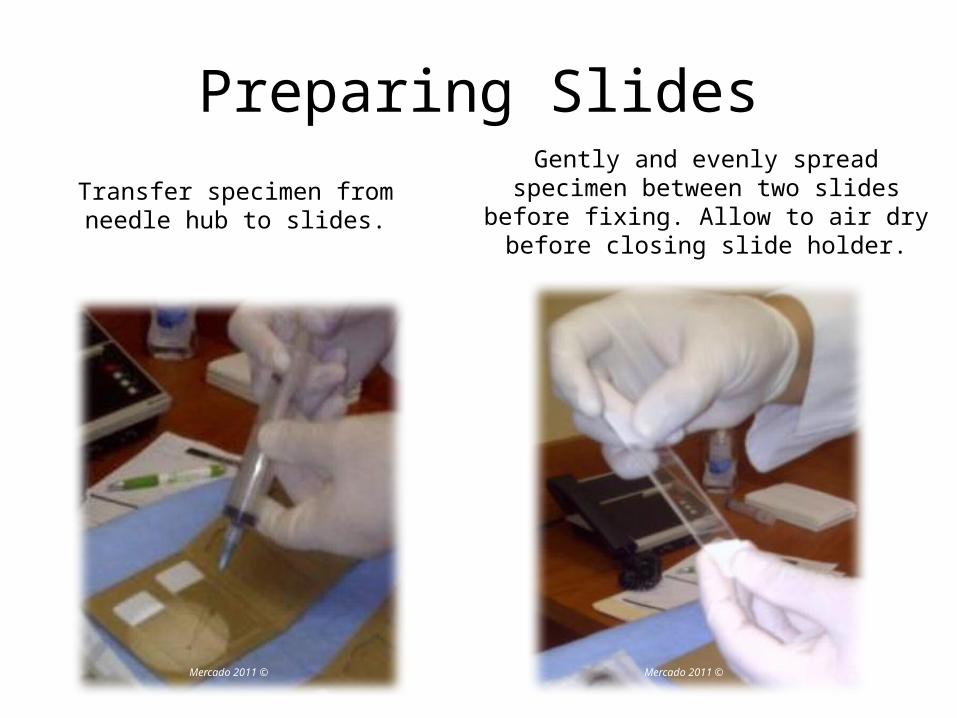
Preparing Slides
Transfer specimen from needle hub to slides.
Gently and evenly spread specimen between two slides before fixing. Allow to
air dry before closing slide holder.
Mercado 2011 © Mercado 2011 ©

Fine Needle Aspiration
Aspiration techniques vary widely based on personal preference, and specific clinical
circumstances.
Goal is to collect adequate cellular
material for cytologic evaluation.
Practice mannequins available to palpate and
practice technique.

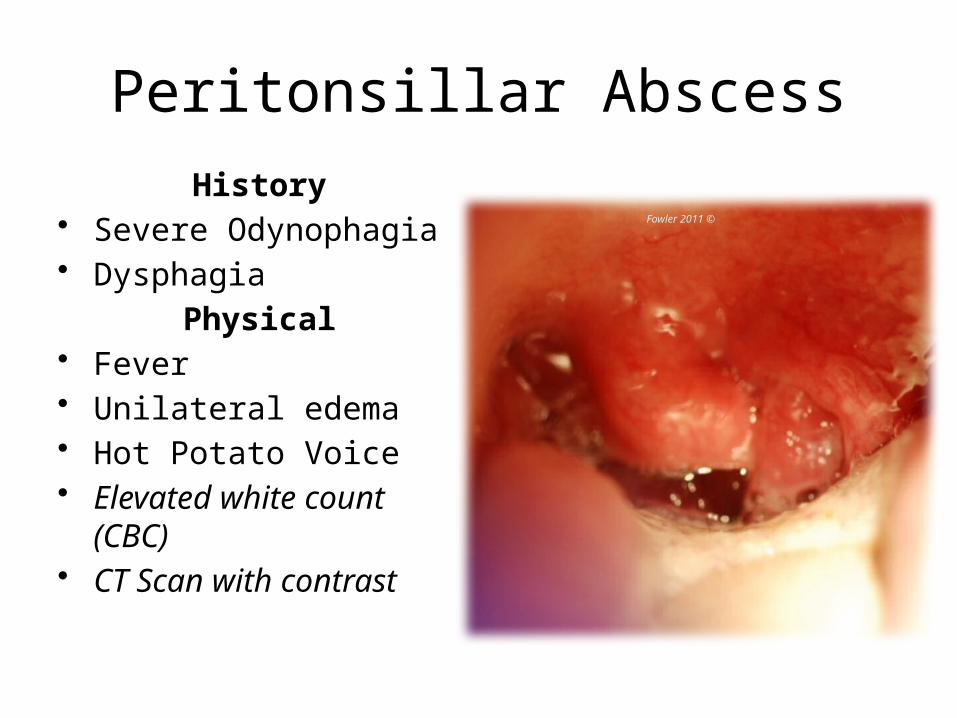
Peritonsillar Abscess
Peritonsillar Abscess
History• Severe Odynophagia• Dysphagia
Physical• Fever• Unilateral edema• Hot Potato Voice• Elevated white count
(CBC)• CT Scan with contrast
Fowler 2011 ©
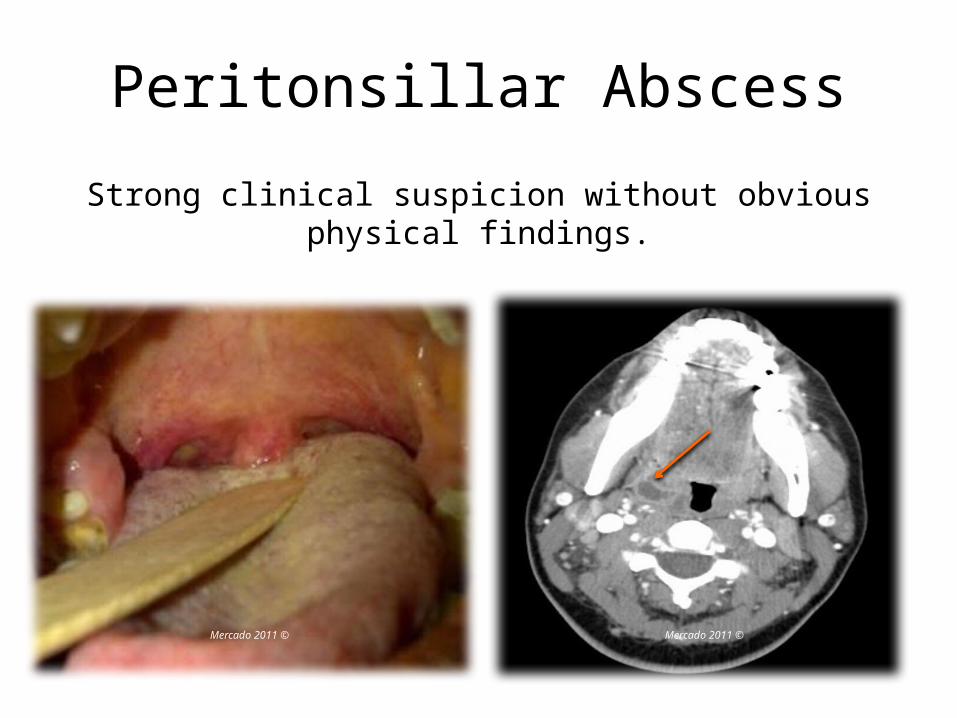
Peritonsillar Abscess
Strong clinical suspicion without obvious physical findings.
Mercado 2011 © Mercado 2011 ©

Equipment neededHurricaine sprayLidocaine w/ epi
Tongue BladeScalpel
HeadlightSuction setup
Long tonsil clampCulturette
Mercado 2011 ©

Peritonsillar Abscess• Management options
– Needle aspiration– Incision and Drainage– Quinsy tonsillectomy
• Choice will depend on site and location of abscess. Smaller, deep abscess are sometimes easier to reach with large bore needle.
• Both have similar success rates (Needle Aspiration 90-95% vs I and D 90-100%)

Peritonsillar Abscess
Peritonsillar Abscess

Needle Aspiration
Mercado 2011 © Mercado 2011 ©
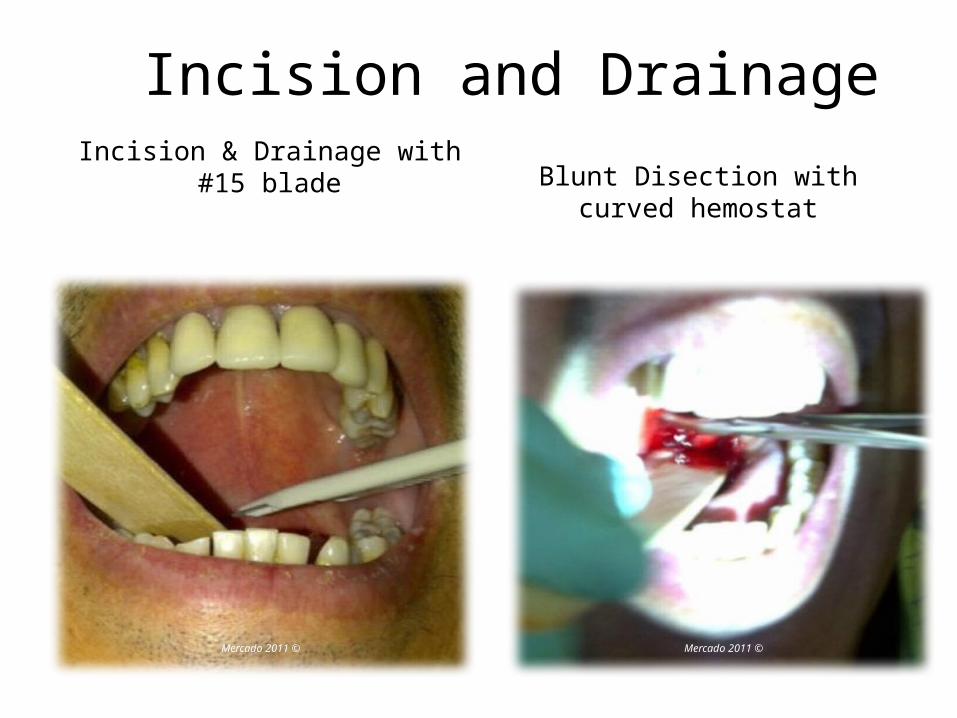
Incision & Drainage with #15 blade Blunt Disection with curved hemostat
Incision and Drainage
Mercado 2011 © Mercado 2011 ©

Peritonsillar Abscess
Discharge instruction :
Penicillin based antibiotics
Oral prednisone
In-office follow up, possible tonsillectomy
Practice mannequins available to simulate PTA and practice needle aspiration technique.
Mercado 2011 © Mercado 2011 ©

Tracheostomy Care
Clinical Consensus Statement: Tracheostomy Care
• Clinical consensus statement (CCS) Aims to improve care for pediatric and adult patient with a tracheostomy tube.
• Approaches to tracheostomy care are currently inconsistent among clinicians and between different institutions.
• The goal is to reduce variations in practice when managing patient with a tracheostomy to minimize complications.
• Variations in care and management of patient with a tracheostomy exist between hospitals, inpatient and outpatient facilities, and in the emergency room.
• Presently, the current literature does not support the development of clinical practice guidelines but favors a consensus of expertise.


Selection of Tracheostomy Tracheostomy tubes come in different sizes and different
materials. Two types of tracheostomy tubes commonly used are Polyvinyl
chloride tracheostomy tubes (Shiley) and Silicone (Bivona). Shiley tubes are slightly flexible and Bivona are the most flexible.
Both Shiley and Bivona tubes come standard with a universal adapter for ventilation. In double cannula tubes, the inner cannula is inserted and locked in place after the obturator is removed.
The inner cannula can be removed briefly for cleaning. The outer tube is secured to the paitent. Single cannula tubes are often used in children and do not have an inner cannula.

Selection of Tracheostomy
Fenestrated tracheostomy tubes facilitate speech by allowing better translaryngeal air flow. Some clinicians believe that fenestrated tubes also aid in the clearance of secretions. Other clinicians feel that these tubes promote the development of granulation tissue along the tracheal wall at the level of the fenestrations. Since there is little scientific data to support either opinion, it is up to surgeon’s preference. Cuffed tubes have a balloon at the distal end of the tube and allow for mechanical ventilation. Uncuffed tubes are generally preferred in children. Except when requiring ventilation with high pressures, requiring ventilation only at night, or with chronic translaryngeal aspiration.
Obstruction
Mercado 2011 © Mercado 2011 ©
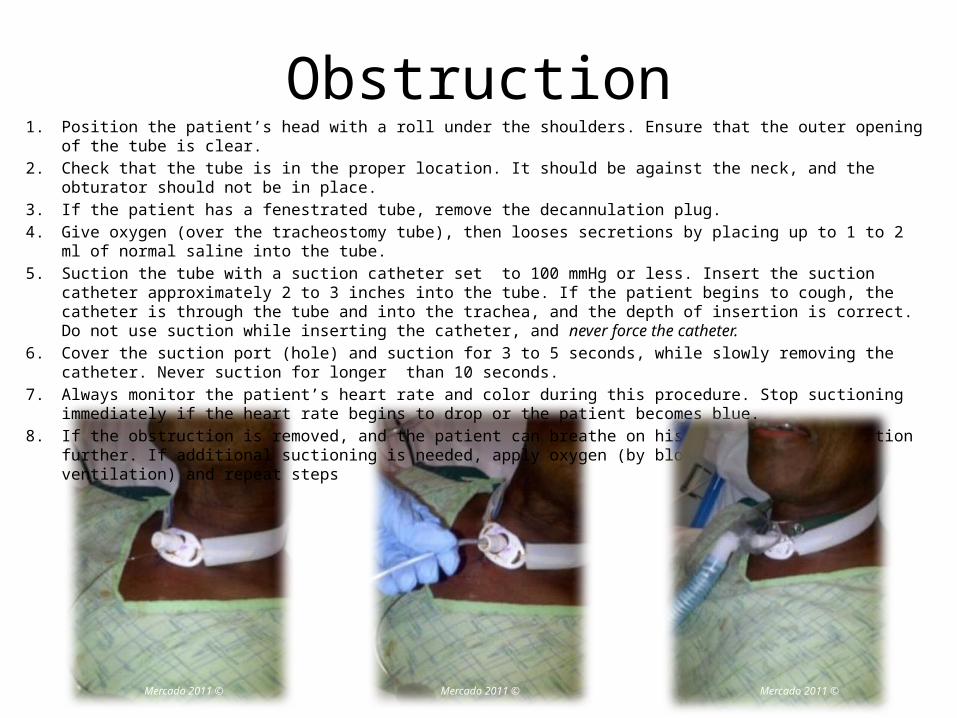
1. Position the patient’s head with a roll under the shoulders. Ensure that the outer opening of the tube is clear.
2. Check that the tube is in the proper location. It should be against the neck, and the obturator should not be in place.
3. If the patient has a fenestrated tube, remove the decannulation plug.
4. Give oxygen (over the tracheostomy tube), then looses secretions by placing up to 1 to 2 ml of normal saline into the tube.
5. Suction the tube with a suction catheter set to 100 mmHg or less. Insert the suction catheter approximately 2 to 3 inches into the tube. If the patient begins to cough, the catheter is through the tube and into the trachea, and the depth of insertion is correct. Do not use suction while inserting the catheter, and never force the catheter.
6. Cover the suction port (hole) and suction for 3 to 5 seconds, while slowly removing the catheter. Never suction for longer than 10 seconds.
7. Always monitor the patient’s heart rate and color during this procedure. Stop suctioning immediately if the heart rate begins to drop or the patient becomes blue.
8. If the obstruction is removed, and the patient can breathe on his/her own, do not suction further. If additional suctioning is needed, apply oxygen (by blow-by or direct ventilation) and repeat steps
Mercado 2011 ©

Accidental Decanulation
• Early accidental decanulation.
• Nasal speculum• Obturator• Risk of false
tract/fistula
Mercado 2011 ©

Leaks
A low-pressure, high volume cuff is preferred to avoid unnecessary injury to the tracheal mucosa such as tracheal malacia.
1. Check cuff pressure first.
2. Consider changing to a longer tracheostomy tube.
3. Monitor cuff pressure on a regular basis.
Shiley® Tube Size
Leak Test Volume
10 20cc
8 17cc
6 14cc
4 11cc

Bleeding
• Local bleeding– Granulation tissue– Superficial bleeding
from mucosa– Small vessels
• Controlled with – Pressure dressing– Gelfoam– Chemical
cauterization

Bleeding
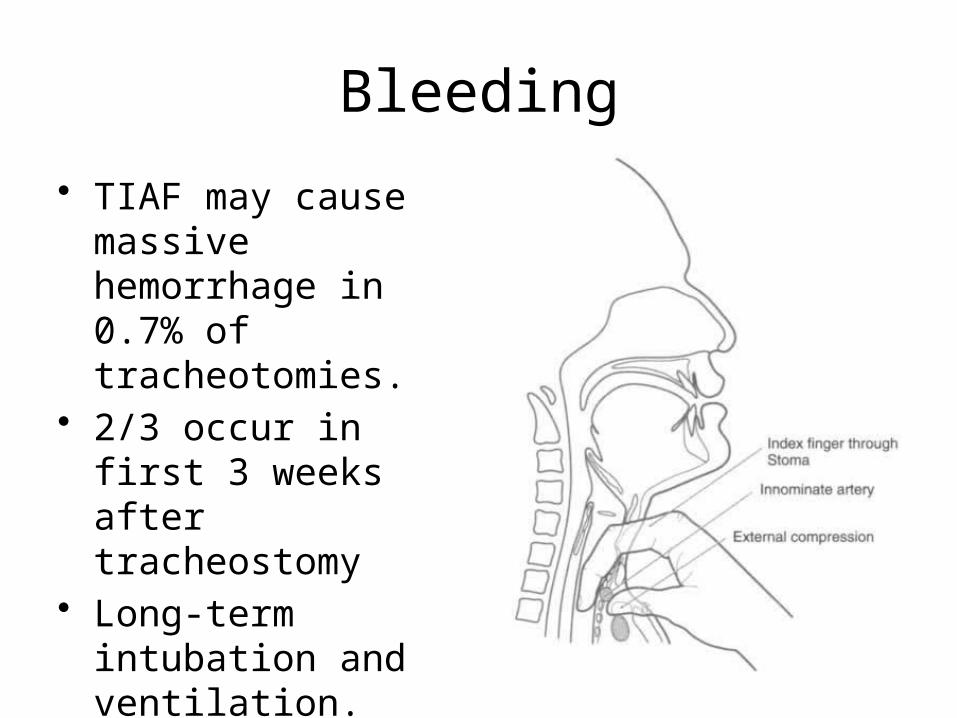
But for anything more than oozing. Must rule out tracheo-innominate artery fistula (TIAF).
Caused include;• Low
tracheostomy • High innominate
artery • Cuff overinflation • Infection
Bleeding
• TIAF may cause massive hemorrhage in 0.7% of tracheotomies.
• 2/3 occur in first 3 weeks after tracheostomy
• Long-term intubation and ventilation.
• Cuffed or uncuffed tube.

Changing Tracheostomy• In the absence of aspiration, tracheostomy tube cuffs should be
deflated when the patient no longer requires mechanical ventilation.• A patient initial tracheostomy tube should normally be replaced within
10-14 days.• The Panel agreed an experienced physician should ideally be present
for the first tube change, although there are was recognition that in some facilities, this may not be feasible and thus performed by an experienced advanced practice provider (APP) with immediate physician backup available.
• In an emergency, a dislodged, mature tracheostomy tube should be replaced with the same size or a size smaller tracheostomy tube. If those are not available for could not be inserted, then an appropriately sized endotracheal tube should be placed through the wound into the trachea. In a patient in whom a tube could not be replaced, resulting in hypoxia or concern for eventual loss of airway, they should undergo oral tracheal intubation or immediate surgical revision tracheostomy.
Decannulation When the adult patient is in the hospital and;
1. Does not require mechanical ventilation
2. Indication for tracheotomy has resolved
3. Patient tolerates breathing through the tracheotomy tube with the cuff deflated.
4. Breathing with a cuffless #6 Shiley tube is checked (smaller patients, a cuffless #4 Shiley tube is placed)
5. Patient tolerates capped tracheostomy with a red button.
6. If the patient is stable (normal oxygen and CO2) for 24 – 48 hours with the trach plugged, the tube will be removed by a qualified physician or mid-level provider, and the stoma will be allowed to close.
Downsizing, capping and decannulation

Decannulation
Downsizing, capping and decannulation

Decannulation
1. Wound margins should heal by secondary intention, with initial wound co-apting in 5 to 7 days (unless wound was created with a fenestration technique)
2. New epithelial cells grow across wound in 7 to 10 days. No leak of air from the wound at this time.
3. If wound does not heal, then wound may be closed surgically, by separating trachea from the skin, and closing the wounds in layers.
4. If scar appearance is not acceptable, wound may be closed in a transverse incision across the lower neck with a plastic closure.
When the patient succeeds at decannulation sequence,

Decannulation
Assess the patient for associated anomalies of the nervous, respiratory, cardiovascular and gastro-intestinal systems.
Re-examine the airway for associated problems: nasal obstruction, adenoid hypertrophy, tonsil hypertrophy, macroglossia, glossoptosis, micrognathia, lingual tonsil hypertrophy, laryngomalacia, glottic web, sub-glottic stenosis, tracheal stenosis or granulation
Mercado 2011 ©

Late Complications
• Bleeding • Tracheomalacia• Stenosis • Tracheoesophageal
fistula• Tracheocutaneous
fistula• Granulation• Leaks
Mercado 2011 ©
Tracheotomy- Conclusion
1. Identify source of leaking and bleeding.
2. If unable to safely change tracheostomy at bedside consider revision tracheostomy in OR.
3. Care of the tracheostomy tube and the wound require planning and communication.
4. Do only as much as you have been trained to, feel comfortable doing and is within your scope of practice. Practice mannequins
available to practice tracheostomy care
technique.
Mercado 2011 ©

Clinical Consensus Statement
• Tracheostomy tube should be changed using a clean technique. A sterile technique is not necessary and does not lead to a reduction in impaction.
• Plastic tracheostomy tube should be used among pediatric and adult patients for initial tube placement.
• Tracheostomy tube ties it should be used unless the patient recently underwent local or free flap reconstructive surgery or other major neck surgery.
• No patient should be discharged with tracheostomy tube sutured in place. Any suture securing a tracheostomy should be removed during first tube change.
• Stoma and tracheostomy tube should be suctioned when there is evidence of visual or audible secretions in the airway, suspected airway obstruction, and whether tube is changed or deflated.


Station 1Control
A/PEpistaxis
Removal FB
Station 4PTA
Station 2Control
A/PEpistaxis
Removal FB
Station 5FNA
Station 3Trach Care
Station 6FNA
ENT Procedures Practice StationsS
MR
*
Chair
*suction
Related Documents




![Ten Look Alike Rashes-1 [Read-Only] - c.ymcdn.comc.ymcdn.com/sites/ Look Alike Rashes Michelle DiBaise, MPAS, PA-C, ... firm white lesions on the ... keratotic papules, located](https://static.cupdf.com/doc/110x72/5b09f6ef7f8b9adc138b589f/ten-look-alike-rashes-1-read-only-cymcdncomcymcdncomsites-look-alike-rashes.jpg)






