Engineering Antibodies for therapeutic applications in man Part II Lecture 5 th March 2009 by Mike Clark, PhD Department of Pathology Division of Immunology Cambridge University UK www.path.cam.ac.uk/~mrc7/

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Engineering Antibodies for therapeutic applications in man
Part II Lecture
5th March 2009 by
Mike Clark, PhDDepartment of Pathology
Division of Immunology
Cambridge University
UK
www.path.cam.ac.uk/~mrc7/

Breakdown of Protein Therapeutics Estimated Market based on the sales of the top-selling biologics drugs.*
Category 2006 (in $B)
2010 (projected) (in $B)
Monoclonal antibodies and Fc fusions 23.1 41.2 Epoetins 12.0 12.8** Insulin-related 9.0 13.0 Interferons 6.8 7.7 Antifibrinolytics 4.5 6.3 Immunostimulatory (xCSF) 4.3 5.5 Growth hormones 2.4 2.5 Other (mixed mechanisms) 3.2 4.7 Totals 65.3 93.7 * Based on published 2005 and 2006 sales, and 2010 projected sales of the top 70 biologics currently on the market, excluding vaccines (multiple sources). ** Projections were made prior to published safety concerns in mid-2007, which have depressed overall sales of epoetins.
Slide courtesy of Bill Strohl, Centocor, September 2008

Product Name (Manufacturer)
Date Indication Protein
Rituxan (Biogen/Idec)
1998 NHL IgG1, chimeric
Herceptin (Genentech)
1998 Breast cancer
IgG1, humanized
Mylotarg (Wyeth)
2000 Leukemia IgG4, humanized; conj. NP
Campath (Berlex)
2000 Leukemia IgG1, humanized
Zevalin (Biogen/Idec)
2002 NHL IgG1 murine, conjugate
Bexxar (Corixa) 2003 NHL IgG2aλ - Iodine-131, conj.
Erbitux (ImClone/BMS)
2004 Colorectal cancer
IgG1, chimeric
Avastin (Genentech)
2004 Colorectal cancer
IgG1, human
Vectibix (Amgen)
2006 Cancer IgG2; human
Examples of Therapeutic Antibody-relatedProducts on the Market
Product Name (Manufacturer)
Date Indi-cation
Protein
ReoPro (Lilly) 1994 CV Fab, chimeric
Simulect (Novartis) 1998 GVHD IgG1, chimeric
Remicade (J&J) 1998 RA IgG1, chimeric
Synagis (AZ) 1998 RSV IgG1, chimeric
Zenapax (Roche) 1998 GVHD IgG1, humanized
Enbrel (Immunex) 1998 RA TNFR-Fc fusion
Xolair (Genentech) 2003 Asthma IgG1, humanized
Raptiva (Genentech) 2003 Psoriasis IgG1, humanized
Humira (Abbott) 2003 RA IgG1, human
Orencia (BMS) 2005 RA CTLA4-Fc fusion;
Modified Fc
Tysabri (Biogen/Elan) 2005 MS IgG4; humanized
Lucentis (Genentech) 2006 AMD Fab; humanized
Soliris (Alexion) 2007 PNH IgG2/4 humanized;
Modifed Fc
Arcalyst (Regeneron) 2008 CAPS IL-1 – Fc fusion
Cimzia (UCB) 2008 RA PEGylated Fab
Nplate (Amgen) 2008 TCP Peptide-Fc fusion;
Aglycosylated Fc
Slide courtesy of Bill Strohl, Centocor, September 2008

Bioloogic Year
OKT3 1986--- ///////ReoPro® 1994--- 1995--- 1996Rituxan® 1997Zenapax® 1997Remicade® 1998Enbrel® 1998Herceptin® 1998Simulect® 1998--- 1999Mylotarg® 2000Campath® 2001Zevalin® 2002Xolair® 2003Raptiva® 2003Amevive® 2003Bexxar® 2003Humira® 2003Erbitux® 2003Avastin® 2004Tysabri® 2004Actemra® 2005Orencia® 2005Lucentis® 2006Vectibix® 2006
$0.5B $1.0B $1.5B $2.0B $2.5B $3.0B $3.5B $4.0B
2006 Sales
$271K
$3788K
$3768K$4442K
$3020K
$533K
$2020K$1069K
$2372K
$380K
$90K
$115K
*
*
*
**
**
**
* >$80M in 2006
*
$107K
Sales of Existing Commercial Monoclonal Antibodies through 2006
Slide courtesy of Bill Strohl, Centocor, September 2008

2000 2005 2008 2010
10
20
30
40
50
60
Current status as of Sept 2008; N=26
If all current BLAs are approved and result in marketed biologics
If ~50% of current Phase III candidates are approved in next 3-4 years (50% POS)
Human MAbFc fusion protein
Humanized MAbChimeric MAbMurine MAb
Year
Cu
mu
lati
ve n
um
ber
of
MA
bs
and
Fc
fusi
on p
rote
ins
app
rove
d If all (unlikely) current Phase III candidates were to be approved in next 3-4 years (100% POS)
Current and Projected Number of MarketedMonoclonal Antibodies and Fusion Proteins
10
20
30
40
50
60
1995(Current status)
75% POS (industry average) would yield approx ca. 55 marketed Mabs and Fc fusion proteins
Slide courtesy of Bill Strohl, Centocor, September 2008

MonoclonalAntibody Format
Murine
Chimeric
Humanized
Human
Monoclonal Antibody Source
Murine hybridoma
Humanized mouse hybridoma
Phage displayed human antibody library
2 4 6 8 10 12 14 16 18 20Number of Monoclonal Antibodies
33
62
1111
214
2016
1
16
8
Total Marketed Mabs = 22Total Phase III Mabs = 30
Form and Source of Existing Commercial and Phase III Monoclonal Antibodies
Slide courtesy of Bill Strohl, Centocor, September 2008

Antibody Technologies and Products
75 80 85 90 95 00 05
Products/Drugs
Hybridoma
Humanised
antibodies
Technologies
OKT3 7/86
Panorex 1/95
Chimaeric
antibodies
Remicade 8/98
ReoPro 12/94
Rituxan 11/97
Simulect 5/98
Radiolabeled Abs Immunotoxins (Pro)drug Conjugates Enzyme/Cytokine Fusions Multispecific/Multivalent Engineered Fc Cocktails
Emerging Technologies
HUMIRA 12/02
Bexxar 06/03
Mylotarg 05/00
Zevalin 02/02
Phage antibodies
Human Ab mice
Zenapax 12/97
Herceptin 9/98
Synagis 6/98
Campath 05/01
Xolair 06/03
Raptiva 10/03
Avastin 02/04
Erbitux 02/04
Tysabri 03/06

Time Required for Maturity of Technologies
Year1975 1980 1985 1990 1995 2000 2005 2010
Kohler and Milstein, 1975
Muronomab-OKT3®, 1986
11 years
Morrison etal., 1984
ReoPro®, 1994
10 years
11 years
Jones et al., 1986
Zenapax®, 1997
9 years
Capon et al., 1989;First Fc fusion
Enbrel®, 1998
12 years
McCaffertyet al., 1990
Humira®, 2002
Lonberg et al., 1994;Green et al., 1994
Vectibix®, 2004
10 years
13 years
Alegre et al., 1994;(first OKT3 ala-ala) Soliris®, 2007
Antibodies with modified,muted Fc function
Human antibodies fromtransgenic humanized mice
Human antibodies from phage display libraries
Fc fusion protein
HumanizedCDR-grafted antibodies
Chimeric antibodies
Murine hybridoma
Slide courtesy of Bill Strohl, Centocor, September 2008

Substantially Moderate High muted activity ADCC
• FcRI,II,III- silent• No comple- ment activity
• FcRI,II,III- silent• Complement activity
• FcRI,III-silent• FcRIIa-active• Little Comple- ment activity
• FcRI,II,III- active• Complement activity
• FcRI,II,III- very active• Complement activity
IgG2m4IgG2-4IgG4ala-ala
AglycosylatedIgG1
Standard IgG2 Standard IgG1EngineeredIgG1
Non-Oncology, Cytokines, OncologyNon-Infectious other soluble receptorDiseases cell targets targets; IDsurface target
Spectrum of IgG Activities
Slide courtesy of Bill Strohl, Centocor, September 2008

US Trade NamAe (generic name)
Company Approval Date (US)
Molecular target
Major Indication
Protein format
Orencia® (Abatacept)
BMS 12/23/ 05 CD80/CD86 (T-cell)
RA CTLA4-Fc fusion protein with modified IgG1 Fc
Soliris® (Ecolizumab)
Alexion Pharma
03/16/07 Complement C5
PNH(reduce hemolysis)
Humanized IgG2/4 hybrid
Nplate® (Romiplostim)
Amgen 08/22/08 TPO-R Thrombo-cytopenia
Fc-peptide fusion („peptibody“) with aglycosylated Fc
Teplizumab; HOKT31- (Ala-Ala)
Macrogenics / Eli Lilly
Phase III CD3 Diabetes Humanized Modified Fc
Otelixizumab (ChAglyCD3; TRX4)
GSK / Tolerx Phase III CD3 Type 1 Diabetes
Aglycosylated, humanized IgG
Removab® (Catumaxomab)
Fresenius / Trion
Phase II/III
EpCAM and CD3
Cancer Rat-murine hybrid
MEDI-563 (formerly BIW-8405 )
Astra-Zeneca Phase II IL-5R SLE Afucosylated IgG based on BioWa’s Potelligent technology
PRO-131921 Genentech Phase I/II CD20 (third generation)
Oncology IgG with modified Fc for increased ADCC
AME-133v (LY2469298)
Eli Lilly Phase I/II CD20 NHL IgG with modified Fc for increased ADCC
TRU-015 Wyeth Phase II CD20 RA Small modular immuno-pharmaceutical product (SMIP)
MEDI-557 Astra-Zeneca Phase I F-protein on RSV
RSV YTE mutant – longer half-life Mab
Summary: Examples of “fit-for-purpose” Mabs and Fc Fusions with Isotypes other than IgG1
Slide courtesy of Bill Strohl, Centocor, September 2008

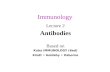
Trends in engineering Antibody fragments
From : Baker, Nature Biotechnology 2005, Figure 1. Anatomy of an optimized antibody. Red indicates sites for potential engineering. From top to bottom: the variable region, binding sites for Fc Rs and complement, and binding site for FcRn. (Source: Xencor, Monrovia, CA, USA.)
Effector Engineering
Binding site engineering
Antibody fragments and other binding
proteins
Combining antibodies

Looking beyond the initial success: remaining issues for Antibody Therapeutics
• Limited efficacy
• Safety (side effects)
• Immunogenicity
• Complex, expensive drugs
• Manufacturing (COGS)
• Delivery only possible via injection

Immunogenicity of Approved Antibody Drugs
mAb Target Molecule Immuno-suppression
Comed with immuno-suppressor
Immunogenicity
OKT3 CD3 Murine mAb, IgG2a Yes Yes 17-63%
ReoPro IIb/IIIa Chimaeric Fab No No 5.8% (1st dose)
Rituxan CD20 Chimaeric IgG1, Yes No 1-10%
Zenapax CD25 Humanized IgG1, Yes Yes 14-34%
Remicade TNF- Chimaeric IgG1, Yes Yes 10-61%*
Herceptin HER2 Humanized IgG1, No Yes/No 0-1%
Synagis RSV Humanized IgG1, No No 0.7-1.8%
Simulect CD25 Chimaeric IgG1, Yes Yes 1-20%
Mylotarg CD33 Humanized IgG4 Yes Yes 2 pts in Phase I
Campath CD52 Humanized IgG1, Yes No 1-90%
Zevalin CD20 Murine IgG1, Yes No 3.8%
HUMIRA TNF- Human IgG1, Yes Yes/No 1-12%
All antibodies administered IV; data from product inserts; *Baert et al, N. Engl. J. Medicine 2003

Engineering opportunities
• Find better binding site
• Increase affinity / potency
• Modulate on/off-rate
• Broaden epitope reactivity
• Combine binding sites
• Engineer improved effectors
• Enhance pharmacokinetics
• Diminish immunogenicity
• Increase productivity
• Improve stability
• Reduce product heterogeneity

Three Major Techniques for Making Antibodies for Therapy
I. Humanization : Immunization, hybridoma, cloning, then chimerization or humanization via CDR grafting or deimmunization
II. Mice carring Human Ab genes : Engineering the mouse, immunization, hybridoma/B-cell (Ab-gene rescue)
III. Phage Display : Creating phage display library (non-immune/immune/synthetic); selection of Ab from library
Fab IgG

Engineered antibody fragments
Holliger and Hudson, Nat. Biotechnology (Sept 2005)

Antibody fragmentsAntibody fragments: size vs half life
Holliger and Hudson, Nat. Biotechnology (Sept 2005)

University Research Programmes
• Immunosuppression
CD4, CD3, monovalent CD3, CD52 (Campath)
• Tumour Therapy
CD52 (Campath), bispecific CD3
• Organ Transplantation
CD52, CD3, CD4, synergistic CD45 pair
• Allo and auto-immunity
RhD, HPA-1a
• Chronic Inflammation
CD18, VAP-1

Declaration of interests (rights as an inventor)
• CD52 IlexOncology/Genzyme (Campath® humanisation)
• CD4 TolerRx/Genentech (for induction of tolerance)
• CD4 BTG (improved method of humanisation)
• CD3 TolerRx/GSK (immunosuppression and tolerance)
• RhD NBS / University collaboration
• HPA-1a NBS / University collaboration

Otelixizumab • Started out as a depleting monovalent rat antibody for use in
immunosuppression of graft rejection. Clark,M., Bindon,C., Dyer,M., Friend,P., Hale,G., Cobbold,S., Calne,R., & Waldmann,H.
Eur. J. Immunol. 19, 381-388 (1989) The improved lytic function and in-vivo efficacy of monovalent monoclonal CD3 antibodies.
Abbs,I.C., Clark,M., Waldmann,H., Chatenoud,L., Koffman,C.G. & Sacks,S.H. Therapeutic Immunology 1, 325-331 (1994) Sparing of the first dose effect of a monovalent anti-CD3 antibody used in allograft rejection is ssociated with diminished release of pro-inflammatory cytokines.
• Humanised as a monovalent depleting antibody. Routledge, E.G., Lloyd, I., Gorman, S., Clark, M. & Waldmann, H. Eur. J. Immunol. 21,
2717-2725 (1991) A humanized monovalent CD3 antibody which can activate homologous complement.
• Converted to a non-depleting form by modification of the Fc region.
Bolt,S., Routledge,E., Lloyd,I., Chatenoud,L., Pope,H., Gorman,S.D., Clark,M. & Waldmann,H. Eur. J. Immunol. 23, 403-411 (1993) The generation of a humanised, non-mitogenic CD3 monoclonal antibody
which retains in vitro immunosuppressive properties




The antibody isotype is important






Chimeric and humanised


Rat IgG2b is effective in therapy

Human IgG1 also effective in therapy

Antibodies (eg CD52 Campath) can be effective in killing cancer cells (BCLL)



NOVEL ANTIBODIES TO TREATFETO-MATERNAL ALLOIMMUNE
THROMBOCYTOPENIA?
Lorna M Williamson, Kathryn Armour, Mike Clark
Departments of Haematology & Pathology,
University of Cambridge/National Blood Service

Fetomaternal alloimmune thrombocytopenia
• Maternal IgG raised against fetal platelet alloantigens can
cross the placenta and cause fetal platelet destruction
• If the fetal platelet count falls dangerously low, cerebral
hemorrage or death may result
• Current therapies are intrauterine platelet transfusion and
maternal therapy with high dose IVIG

Alloantigen negativeMother
(bb)
Alloantigen positivefetal platelets
(ab)
Fetal platelet material
Feto-maternal Alloimmune Thrombocytopenia

Feto-maternal Alloimmune Thrombocytopenia
Maternal platelet antibodies
Platelet destruction by maternal HPA
alloantibodies
Anti-a

FMAIT causes neonatal purpura

FMAIT causes intracranial haemorrhage in utero

An ideal blocking antibody for FMAIT
1. HPA-1a specificity & competes with FMAIT sera
2. Inert Fc without increased immunogenicity
3. Inactive in FcR binding & FcR-mediated cell
destruction
4. Blocks destruction of cells by active antibody
5. No triggering of cell destruction in vivo
6. No effects on platelet production or function
7. Normal half-life and placental transport


2. Inert Fc without increased immunogenicity


Can a protective antibody be developed?
• 90% severe cases FMAIT are due to antibodies
against the alloantigen HPA-1a on GPIIIa
• Single B cell epitope (Leu-33) could be blocked
to prevent the binding of harmful antibodies
• Outcome depends on antibody titre
Williamson et al. Blood 1998; 92: 2280 Jaegtvik et al. Br J Obs Gynae 2000; 107: 691

Ideal properties of an antibody for FMAIT therapy
• HPA-1a specificity (B2 variable regions)
• able to cross the placenta
• inactive in FcR-mediated cell destruction
• unable to activate complement

RhDHPA-1a

Chemiluminescent response of human monocytes to sensitised RBC
-20
0
20
40
60
80
100
120
140
0 5000 10000 15000 20000 25000 30000
antibody molecules/cell
% c
hem
ilum
ines
cenc
e
G1
G1a
G1b
G1c
G1ab
G1ac
G2
G2a
G4
G4b
G4c
Fog-1 antibodies

Inhibition of chemiluminescent response due to 2 g/ml Fog-1 G1 by other Fog-1 antibodies
0
10
20
30
40
50
60
70
80
90
100
0.1 1 10 100 1000
inhibitor concentration, g/ml
% c
hem
ilum
ines
cenc
e
G1 b
G1 c
G1ab
G1ac
G2
G2a
G4b
G4c

Inhibition by Fog-1 antibodies of ADCC due to clinically relevant polyclonal anti-RhD (at 3ng/ml)
0
20
40
60
80
100
120
0.1 1 10 100 1000 10000
inhibitor antibody concentration, ng/ml
% R
BC
lysi
s
G1 ab
G2
G2a
G4
G4 b

3. No triggering of cell destruction in vivo

Red cell survival study in normal volunteers
Compare intravascular survival of RBC coated with Fog-1 G1 and Fog-1 G1nab in human volunteers.
99mTc G1
Label and coat autologous RBC
51Cr G1nabDesign allows
• simultaneous comparison in same donor• assessment of survival over several days (51Cr)• gamma camera imaging of sites of red cell
accumulation (99mTc)
Armour et al, Blood 2006;107:2619-2626

RBC incubated with antibodies at 50 g/ml,giving 75% saturation of RhD sites.
Subjects
1 2 3 4 5 6
Age / Sex 47 / F 53 / M 45 / M 41 / M 48 / M 38 / M
Predicted Rh genotype R1R2 R2R2 R1R2 R1r R1r R1r
Antibody molecules/cell:
G1 11700 ( 2700)
19900 ( 2300)
6800 ( 500)
17400 ( 3500)
13300 ( 1300)
G1Δnab 11200 ( 2100)
19900 ( 2500)
6500 ( 600)
15600 ( 2600)
13700 ( 2100)
13500 ( 3000)

Plasma counts
-1
0
1
2
3
4
5
6
7
1 10 100 1000 10000
G1nab
-1
0
1
2
3
4
5
6
7
1 10 100 1000 10000
time after injection, min
plas
ma
coun
t, %
inje
cted
dos
e
G1
subject 1 subject 2 subject 3 subject 4 subject 5

G1-coated cells
• Complete, irreversible clearance by 200 min
• Appearance of plasma radiolabel
• Accumulation in spleen and, at high coating levels, in liver
Total cell clearance and destruction
G1nab-coated cells
• Clearance incomplete and transient
• No appearance of plasma radiolabel
• Accumulation in spleen but not in liver even at high coating levels
No destruction of red cells but sequestration in the spleen

Antibody selection and design
The choice of antibody constant region is largely dictated by functional requirements of the antibody.
But what about the V-regions ?

The V-region Mythology
Chimaeric65% Human ?
Humanised95% Human ?
• This commercial marketing mythology is based on an assumption that mouse and human antibody sequences are unique.
• However a study of the Kabat database shows that there is high sequence homology for antibodies from different species.


Kabat database variability of VH sequences
Human VH Mouse VH

Are chimaeric, humanised and fully human antibodies so very different in sequence?


Possible to select alternative V genes for humanisation
Gorman,S.D., Clark,M.R., Routledge,E.G., Cobbold,S.P. & Waldmann,H. P.N.A.S. 88, 4181-4185 (1991) Reshaping a therapeutic CD4 antibody.
Routledge,E., Gorman,S., & Clark,M. in Protein engineering of antibody molecules for prophylactic and therapeutic applications in man. (Ed. Clark,M. )
Pub. Academic Titles, UK (1993) pp. 13-44 Reshaping of antibodies for therapy.
• Gorman et al recognised that homology also extended through the CDR regions not just the framework regions • Homology to Kol was increased from 69% to 89% by the humanisation process.

The same strategy can be applied to almost any V-region

Antibody comparisons FR CDR Whole V
murine versus human germline
Campath-1G (68/87) 78% (14/34) 41% (82/121) 68%
Anti-Tac (67/87) 77% (14/29) 48% (81/116) 70%
OKT3 (67/87) 77% (12/32) 38% (81/119) 68%
humanised versus human germline
Campath-1H versus germline (78/87) 90% (8/34) 24% (86/121) 71%
Anti-Tac versus germline (77/87) 89% (14/29) 48% (91/116) 78%
OKT3 versus germline (76/87) 87% (6/32) 19% (82/119) 69%
human versus human germline
Fog-1 RhD versus germline (77/87) 89% (23/37) 62% (100/124) 81%
Sequence homologies of some rodent, humanised and human sequences

Antibody Specificity V-regionHomologous
VHJH Length Matches Homology
FOG-1 RhD Human V4-34 JH6A 124 100 0.807
anti-Tac CD25 Humanised HV1F10T JH6a 116 91 0.784
anti-Tac CD25 Mouse HV1F10T JH4D 116 84 0.724
anti-TNFa TNF-alpha Mouse VI-4-IB JH3B 117 84 0.718
Campath-1H CD52 Humanised DP-71_3D197D- JH4D 121 86 0.710
Campath-1G CD52 Rat DP-34_DA-10 JH4D 121 85 0.702
OKT3 CD3 Humanised b25 JH6a 119 82 0.689
OKT3 CD3 Mouse DP-7_21-2-.. JH6a 119 81 0.681
HD37 CD19 Mouse 6M27 JH4D 124 83 0.669
anti-CD20 CD20 Mouse DP-7_21-2- JH2 121 81 0.669
Homologies for antibody heavy chain V regionscompared with human germline sequences
Sorted by homology

What of the Emperor’s new clothes?
Appropriate selection of sequences of antibody Constant and Variable regions is likely to be only one factor controlling the immunogenicity of therapeutic antibodies.
However it is the final sequence of the antibodies which matters and not the route by which they were made. For example it is possible to come up with alternative humanised sequences for the same antibody. Similar sequences can often be found for mouse, rat and human variable regions within the databases.
Even fully human antibodies may contain unusual motifs or structures as a result of the somatic recombination and junctional diversity combined with somatic hypermutation.
Related Documents