CLINICAL STUDY Endovascular Treatment of Penetrating Traumatic Injuries of the Extracranial Carotid Artery Diego A. Herrera, MD, Sergio A. Vargas, MD, and Arthur B. Dublin, MD, MBA, FACR ABSTRACT Purpose: To describe the clinical and angiographic results of endovascular therapy for traumatic injuries of the extracranial carotid artery. Materials and Methods: The clinical and angiographic features of 36 traumatic injuries of the carotid artery during a 12-year period were reviewed. There were 35 male patients (97.2%) and 1 female patient (2.8%) with an average age of 28.8 years (range 13– 60 years). Of the 36 lesions of the carotid artery, 29 (80.6%) were the result of gunshot injury, and 7 (19.4%) were secondary to stab wounds. In 24 (66.7%) instances, the injury resulted in a pseudoaneurysm; in 7 (19.4%), in an arteriovenous fistula (AVF); in 4 (11.1%), in a dissection; and in 1 (2.8%), in inactive bleeding. All patients were treated with an endovascular approach using different techniques (balloon occlusion, embolization, or stent deployment). Results: Endovascular therapy resulted in documented lesion occlusion in 34 (94.4%) patients. Two patients declined any follow-up postprocedural imaging; however, they have remained asymptomatic. Clinical improvement was documented in 35 (97.2%) patients, and there was one procedure-related complication with fatal consequences. Conclusions: In this series, endovascular techniques were an effective method of treatment. It was possible to use different endovascular reconstructive techniques or parent artery occlusion depending on the degree of vessel damage, with resolution of clinical symptoms and avoidance of surgery in most cases. ABBREVIATIONS AVF arteriovenous fistula, CCA common carotid artery, ECA external carotid artery, ICA internal carotid artery, IMA internal maxillary artery, MCA middle cerebral artery The literature suggests that about 25% of cases of penetrat- ing neck trauma are accompanied by vascular injury, with the carotid the most frequently affected artery (1,2). Trau- matic lesions of the carotid artery can be classified depend- ing on the degree of vessel wall injury as dissecting, throm- botic, pseudoaneurysm, arteriovenous fistula (AVF), or transection (3). All of these lesions have a high risk of progressing to stroke or death. The clinical manifestations are variable, including cranio- cervical or thoracic pain, bleeding, dysphagia, hoarseness, hypotension, expanding or pulsatile hematoma, and neuro- logic deficit (4,5). The diagnostic work-up of stable patients usually includes computed tomography (CT) angiography; however, shotgun pellets can produce considerable image deg- radation, often requiring catheter angiography (6). Immediate surgical exploration is indicated for patients who present with signs and symptoms of shock and continuous hemorrhage from the neck wound (7,8). Different endovascular techniques have been previ- ously described for the treatment of neck vessel injuries. Closure of the pseudoaneurysm, AVF closure, or healing of the dissection with preservation of the parent artery is the main goal of treatment. Vessel sacrifice is sometimes indi- cated, however, as a last resort. The purpose of this article is to review our experience in the management of penetrat- ing traumatic injuries of the extracranial carotid artery to determine the benefits of endovascular treatment on the basis of clinical and angiographic results. MATERIALS AND METHODS The clinical records and imaging studies of patients treated for traumatic extracranial carotid artery injuries during the years 1996–2008 were retrospectively analyzed, and endo- From the Department of Radiology (D.A.H., S.A.V.), Neuroradiology Section, Universidad de Antioquia, Hospital Universitario San Vicente de Paul, and Cedi- Med, Medellin, Colombia; and Department of Radiology (A.B.D.), Neuroradiology Section, UC Davis Medical Center, Sacramento, California. Received February 17, 2010; final revision received July 29, 2010; accepted September 15, 2010. Address correspondence to D.A.H.; E-mail: [email protected] None of the authors have identified a conflict of interest. © SIR, 2011 J Vasc Interv Radiol 2011; 22:28 –33 DOI: 10.1016/j.jvir.2010.09.022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Titmibtp
chl
FUMS1A
N
©
J
D
CLINICAL STUDY
Endovascular Treatment of Penetrating Traumatic
Injuries of the Extracranial Carotid Artery
Diego A. Herrera, MD, Sergio A. Vargas, MD, andArthur B. Dublin, MD, MBA, FACR
ABSTRACT
Purpose: To describe the clinical and angiographic results of endovascular therapy for traumatic injuries of the extracranial carotid artery.
Materials and Methods: The clinical and angiographic features of 36 traumatic injuries of the carotid artery during a 12-yearperiod were reviewed. There were 35 male patients (97.2%) and 1 female patient (2.8%) with an average age of 28.8 years (range13–60 years). Of the 36 lesions of the carotid artery, 29 (80.6%) were the result of gunshot injury, and 7 (19.4%) were secondary tostab wounds. In 24 (66.7%) instances, the injury resulted in a pseudoaneurysm; in 7 (19.4%), in an arteriovenous fistula (AVF); in4 (11.1%), in a dissection; and in 1 (2.8%), in inactive bleeding. All patients were treated with an endovascular approach usingdifferent techniques (balloon occlusion, embolization, or stent deployment).
Results: Endovascular therapy resulted in documented lesion occlusion in 34 (94.4%) patients. Two patients declined any follow-uppostprocedural imaging; however, they have remained asymptomatic. Clinical improvement was documented in 35 (97.2%) patients,and there was one procedure-related complication with fatal consequences.
Conclusions: In this series, endovascular techniques were an effective method of treatment. It was possible to use differentendovascular reconstructive techniques or parent artery occlusion depending on the degree of vessel damage, with resolution ofclinical symptoms and avoidance of surgery in most cases.
ABBREVIATIONS
AVF � arteriovenous fistula, CCA � common carotid artery, ECA � external carotid artery, ICA � internal carotid artery,
IMA � internal maxillary artery, MCA � middle cerebral arteryhe literature suggests that about 25% of cases of penetrat-ng neck trauma are accompanied by vascular injury, withhe carotid the most frequently affected artery (1,2). Trau-atic lesions of the carotid artery can be classified depend-
ng on the degree of vessel wall injury as dissecting, throm-otic, pseudoaneurysm, arteriovenous fistula (AVF), orransection (3). All of these lesions have a high risk ofrogressing to stroke or death.
The clinical manifestations are variable, including cranio-ervical or thoracic pain, bleeding, dysphagia, hoarseness,ypotension, expanding or pulsatile hematoma, and neuro-ogic deficit (4,5). The diagnostic work-up of stable patients
rom the Department of Radiology (D.A.H., S.A.V.), Neuroradiology Section,niversidad de Antioquia, Hospital Universitario San Vicente de Paul, and Cedi-ed, Medellin, Colombia; and Department of Radiology (A.B.D.), Neuroradiology
ection, UC Davis Medical Center, Sacramento, California. Received February7, 2010; final revision received July 29, 2010; accepted September 15, 2010.ddress correspondence to D.A.H.; E-mail: [email protected]
one of the authors have identified a conflict of interest.
SIR, 2011
Vasc Interv Radiol 2011; 22:28–33
OI: 10.1016/j.jvir.2010.09.022
usually includes computed tomography (CT) angiography;however, shotgun pellets can produce considerable image deg-radation, often requiring catheter angiography (6). Immediatesurgical exploration is indicated for patients who present withsigns and symptoms of shock and continuous hemorrhagefrom the neck wound (7,8).
Different endovascular techniques have been previ-ously described for the treatment of neck vessel injuries.Closure of the pseudoaneurysm, AVF closure, or healing ofthe dissection with preservation of the parent artery is themain goal of treatment. Vessel sacrifice is sometimes indi-cated, however, as a last resort. The purpose of this articleis to review our experience in the management of penetrat-ing traumatic injuries of the extracranial carotid artery todetermine the benefits of endovascular treatment on thebasis of clinical and angiographic results.
MATERIALS AND METHODS
The clinical records and imaging studies of patients treatedfor traumatic extracranial carotid artery injuries during the
years 1996–2008 were retrospectively analyzed, and endo-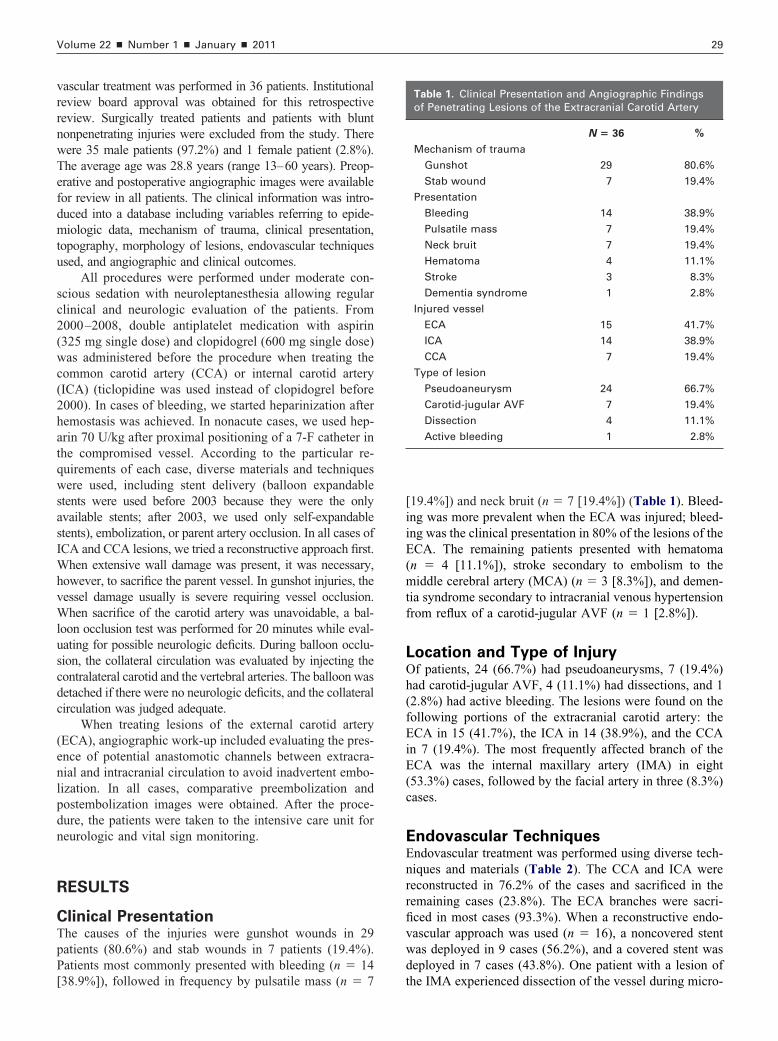
vrrnwTefdmtu
sc2(wc(2hatqwsasIWhvWluscdc
(enlpdn
R
CTpP[
Volume 22 � Number 1 � January � 2011 29
ascular treatment was performed in 36 patients. Institutionaleview board approval was obtained for this retrospectiveeview. Surgically treated patients and patients with bluntonpenetrating injuries were excluded from the study. Thereere 35 male patients (97.2%) and 1 female patient (2.8%).he average age was 28.8 years (range 13–60 years). Preop-rative and postoperative angiographic images were availableor review in all patients. The clinical information was intro-uced into a database including variables referring to epide-iologic data, mechanism of trauma, clinical presentation,
opography, morphology of lesions, endovascular techniquessed, and angiographic and clinical outcomes.
All procedures were performed under moderate con-cious sedation with neuroleptanesthesia allowing regularlinical and neurologic evaluation of the patients. From000–2008, double antiplatelet medication with aspirin325 mg single dose) and clopidogrel (600 mg single dose)as administered before the procedure when treating the
ommon carotid artery (CCA) or internal carotid arteryICA) (ticlopidine was used instead of clopidogrel before000). In cases of bleeding, we started heparinization afteremostasis was achieved. In nonacute cases, we used hep-rin 70 U/kg after proximal positioning of a 7-F catheter inhe compromised vessel. According to the particular re-uirements of each case, diverse materials and techniquesere used, including stent delivery (balloon expandable
tents were used before 2003 because they were the onlyvailable stents; after 2003, we used only self-expandabletents), embolization, or parent artery occlusion. In all cases ofCA and CCA lesions, we tried a reconstructive approach first.
hen extensive wall damage was present, it was necessary,owever, to sacrifice the parent vessel. In gunshot injuries, theessel damage usually is severe requiring vessel occlusion.hen sacrifice of the carotid artery was unavoidable, a bal-
oon occlusion test was performed for 20 minutes while eval-ating for possible neurologic deficits. During balloon occlu-ion, the collateral circulation was evaluated by injecting theontralateral carotid and the vertebral arteries. The balloon wasetached if there were no neurologic deficits, and the collateralirculation was judged adequate.
When treating lesions of the external carotid arteryECA), angiographic work-up included evaluating the pres-nce of potential anastomotic channels between extracra-ial and intracranial circulation to avoid inadvertent embo-ization. In all cases, comparative preembolization andostembolization images were obtained. After the proce-ure, the patients were taken to the intensive care unit foreurologic and vital sign monitoring.
ESULTS
linical Presentationhe causes of the injuries were gunshot wounds in 29atients (80.6%) and stab wounds in 7 patients (19.4%).atients most commonly presented with bleeding (n � 14
38.9%]), followed in frequency by pulsatile mass (n � 7[19.4%]) and neck bruit (n � 7 [19.4%]) (Table 1). Bleed-ing was more prevalent when the ECA was injured; bleed-ing was the clinical presentation in 80% of the lesions of theECA. The remaining patients presented with hematoma(n � 4 [11.1%]), stroke secondary to embolism to themiddle cerebral artery (MCA) (n � 3 [8.3%]), and demen-tia syndrome secondary to intracranial venous hypertensionfrom reflux of a carotid-jugular AVF (n � 1 [2.8%]).
Location and Type of InjuryOf patients, 24 (66.7%) had pseudoaneurysms, 7 (19.4%)had carotid-jugular AVF, 4 (11.1%) had dissections, and 1(2.8%) had active bleeding. The lesions were found on thefollowing portions of the extracranial carotid artery: theECA in 15 (41.7%), the ICA in 14 (38.9%), and the CCAin 7 (19.4%). The most frequently affected branch of theECA was the internal maxillary artery (IMA) in eight(53.3%) cases, followed by the facial artery in three (8.3%)cases.
Endovascular TechniquesEndovascular treatment was performed using diverse tech-niques and materials (Table 2). The CCA and ICA werereconstructed in 76.2% of the cases and sacrificed in theremaining cases (23.8%). The ECA branches were sacri-ficed in most cases (93.3%). When a reconstructive endo-vascular approach was used (n � 16), a noncovered stentwas deployed in 9 cases (56.2%), and a covered stent wasdeployed in 7 cases (43.8%). One patient with a lesion of
Table 1. Clinical Presentation and Angiographic Findingsof Penetrating Lesions of the Extracranial Carotid Artery
N � 36 %
Mechanism of trauma
Gunshot 29 80.6%
Stab wound 7 19.4%
Presentation
Bleeding 14 38.9%
Pulsatile mass 7 19.4%
Neck bruit 7 19.4%
Hematoma 4 11.1%
Stroke 3 8.3%
Dementia syndrome 1 2.8%
Injured vessel
ECA 15 41.7%
ICA 14 38.9%
CCA 7 19.4%
Type of lesion
Pseudoaneurysm 24 66.7%
Carotid-jugular AVF 7 19.4%
Dissection 4 11.1%
Active bleeding 1 2.8%
the IMA experienced dissection of the vessel during micro-
cd
A
aIms((r6thawhb
30 � The Treatment of Penetrating Injuries of the Extracranial Carotid Artery Herrera et al � JVIR
atheterization with consequent occlusion of a giant pseu-oaneurysm.
ngiographic Results, Complications,
nd Follow-upmmediate angiographic occlusion after endovascular treat-ent was documented in all cases treated with parent vessel
acrifice, embolization, or deployment of covered stentsn � 27 [75%]). When a noncovered stent was deployedn � 9 [25%]), there was stagnant flow in the pseudoaneu-ysm in all cases and angiographic occlusion documented at-month follow-up angiography in 77.8% patients. Two ofhe patients refused any further postprocedure imaging;owever, they have remained asymptomatic after 1-yearnd 3-year clinical follow-up. In 35 (97.2%) patients, thereas an uneventful clinical recovery. Only 1 (2.8%) patientad a procedure-related complication, with a thromboem-
Table 2. Endovascular Techniques Used for Treatment ofTraumatic Lesions of the Carotid Artery
N � 36 %
Vessel preservation and reconstruction 17 47.2%
ICA 10 27.8%
CCA 6 16.7%
ECA 1 2.8%
Vessel sacrifice 19 52.8%
ICA 4 11.1%
CCA 1 2.8%
ECA 14 38.9%
Treatment of ICA lesions 14 38.9%
Wallstent 6 16.7%
Balloon occlusion 4 11.1%
Jostent 2 5.6%
Covered Palmaz stent 1 2.8%
Velocity stent � Guglielmi
detachable coil
1 2.8%
Treatment of CCA lesions 7 19.4%
Jostent 2 5.6%
Covered Palmaz stent 2 5.6%
Noncovered Palmaz stent 1 2.8%
Wallstent 1 2.8%
Balloon occlusion 1 2.8%
Treatment of ECA lesions 15 41.7%
N-butyl 2-cyanoacrylate embolization 6 16.7%
Balloon occlusion 3 8.3%
N-butyl 2-cyanoacrylate � coil
embolization
2 5.6%
Coil embolization 1 2.8%
Polyvinyl alcohol particles
embolization
1 2.8%
Polyvinyl alcohol � coils
embolization
1 2.8%
Catheter dissection 1 2.8%
olism to the MCA after balloon occlusion of a pseudoan-
eurysm arising from the ECA. Pharmaceutical thrombolysiswith a single bolus dose of 300,000 U of intraarterialurokinase was performed with recanalization of the MCA;however, the patient presented with massive and fatal epi-staxis during the postoperative period.
Postprocedural follow-up catheter angiography was notperformed whenever the treatment consisted of parent ves-sel occlusion or ECA embolization. Of the 16 patients withlesions of the CCA and ICA who underwent stent place-ment, follow-up imaging was available in 14 cases, with anaverage follow-up time of 14.4 months (range 2–53months). Of these patients, there was one asymptomaticocclusion of the ICA, resulting from the patient’s decisionto stop antiplatelets, documented with Doppler ultrasound 3months after the procedure and a case of mild intimalhyperplasia of the ICA after 6 months. Both patients weretreated with covered stents (1 Jostent [Abbott Vascular,Redwood City, California] and 1 autologous vein-coveredPalmaz stent [Johnson and Johnson, Warren, New Jersey]).Another patient presented with an asymptomatic stent angu-lation (Palmaz noncovered) at the CCA requiring angioplastywithout complications. The remaining 11 patients (78.6%) didnot have intimal hyperplasia, stenosis, or material failure.
DISCUSSION
Several reports in the literature describe the endovasculartreatment of penetrating traumatic lesions of the neck. Dem-etriades et al (9) reported 33 patients with transcervical gun-shot injuries and concluded that 80% had a favorable initialoutcome with medical treatment, but 48% of these patients hada vascular injury that ultimately required surgery in 15% andendovascular therapy in 9%. Another author (10) reviewingtraumatic injuries of the carotid and vertebral arteries reported80% were due to gunshot injuries and 20% were due to stabwounds, in concordance with our results. The same studyreported a higher prevalence of injuries of the CCA, however,whereas we found more lesions of the ECA and ICA.
Endovascular techniques have evolved with the devel-opment of new materials. Before 1998, the Palmaz stentwas used in the treatment of carotid stenosis; currently, ithas been replaced by self-expanding stents. To our knowl-edge, Marotta et al (11) were the first to report the use of anautologous vein-covered Palmaz stent for the treatment of atraumatic pseudoaneurysm of the cervical carotid artery.Since that first report, vein-covered and polyester-coveredstents have also been used for the treatment of these lesionsby other authors (12–15). From the days of these first trials,it has been shown by several studies that it is unnecessaryalways to use covered stents for the treatment of pseudoa-neurysms of medium-caliber arteries (16–19). The use ofcovered stents could potentially cause alterations of thelocal hemodynamic factors leading to a proliferative re-sponse and subsequent intimal hyperplasia.
We have confirmed the utility of noncovered self-
expanding Wallstents (Schneider/Boston Scientific, Boston,
M(fs
F
Wp
F
wwp
Volume 22 � Number 1 � January � 2011 31
assachusetts) in the obliteration of pseudoaneurysmsFigures 1–3) by follow-up angiography in all cases exceptor two patients who rejected imaging follow-up but who
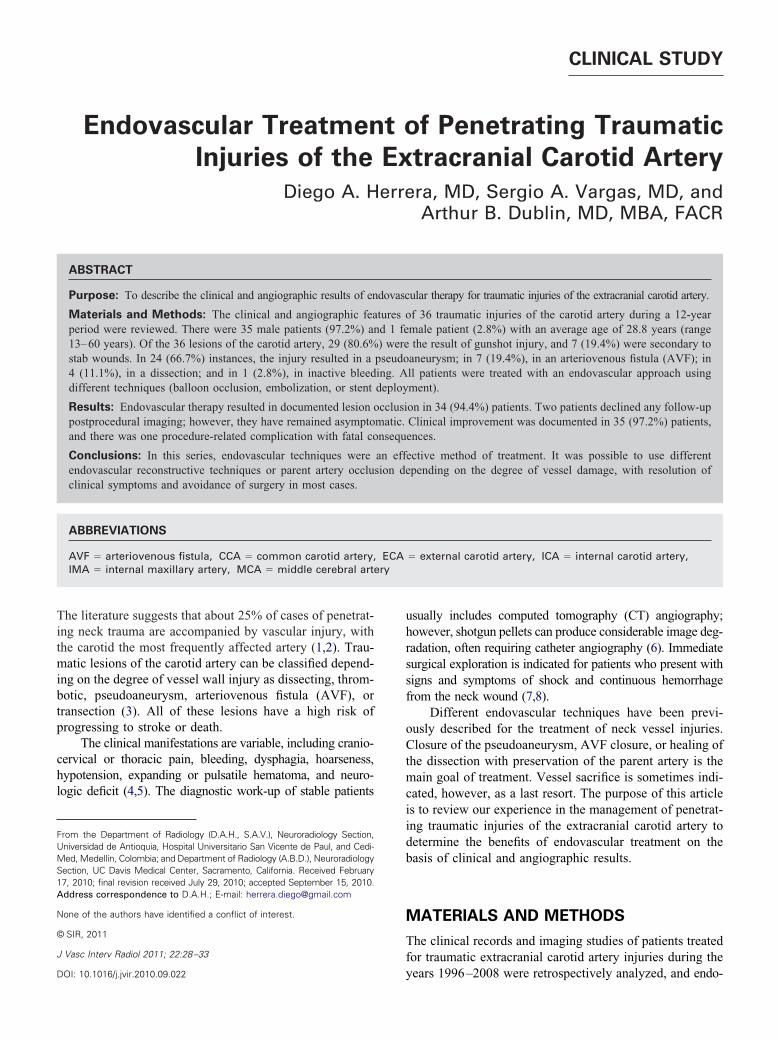
igure 1. (a) ICA pseudoaneurysm (arrow) caused by gunsallstent delivery showed reduced flow through the wall defec
seudoaneurysm.
igure 2. (a) Carotid bulb pseudoaneurysm (arrow) after stabound injury. (b) Follow-up angiogram 1 year after treatmentith Wallstent showing pseudoaneurysm exclusion with incor-oration of the stent to the vessel wall (arrowheads).
howed clinical improvement. Other authors prefer to in-
troduce coils through stent struts, especially in cases ofbroad neck pseudoaneurysm or persistent filling of sacduring follow-up (20 –22). We also used that approach inone patient with a gunshot injury of the ICA and a broadneck pseudoaneurysm treated by Guglielmi detachable coilembolization after delivery of a Velocity stent, document-ing angiographic healing of the artery after 6 months.
We treated 97.2% of the patients of this study success-fully with clinical and angiographic improvement. We re-ported a mortality of 2.8% owing to a massive epistaxis
jury. (b) Angiogram obtained immediately after noncoveredngiogram at 6-month follow-up showed complete exclusion of
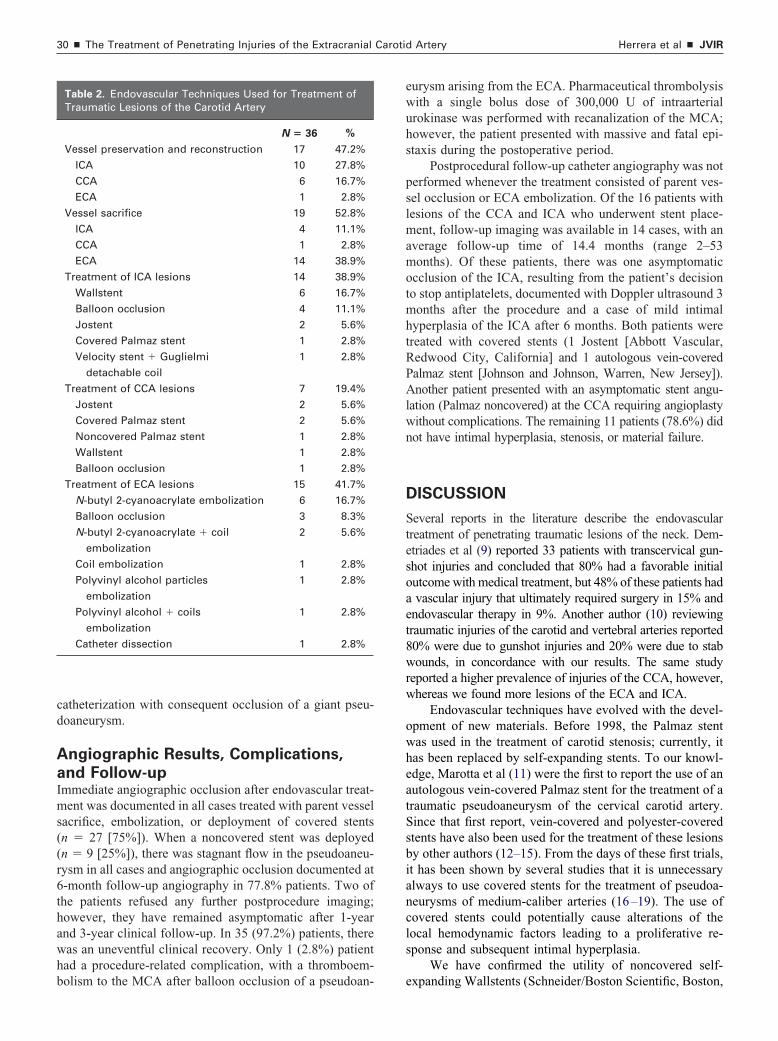
Figure 3. (a) CCA dissection (arrows) after gunshot injury. (b)
Angiogram showing resolution of dissection in the vessel wallafter Wallstent deployment.
hot int. (c) A
after thrombolysis for an embolic complication. Low mor-
berli
oEh
F
tbn
F
a(
32 � The Treatment of Penetrating Injuries of the Extracranial Carotid Artery Herrera et al � JVIR
idity and mortality rates are attained, however, when thendovascular approach is used, as described in a recenteview (23). We also found that parent artery sacrifice as aast resort can be a safe method when collateral circulations adequate (Figure 4).
ECA embolization was very effective for the treatmentf bleeding in our series. In our patients with lesions ofCA branches, epistaxis was the most frequent type of
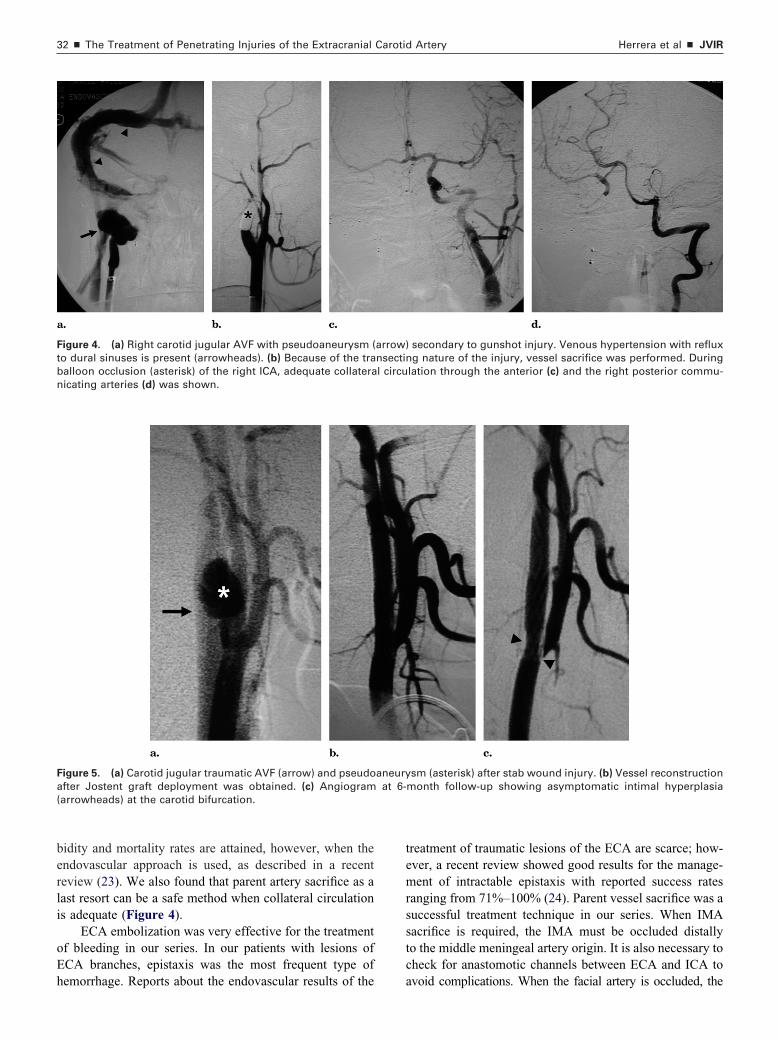
igure 4. (a) Right carotid jugular AVF with pseudoaneurysm (o dural sinuses is present (arrowheads). (b) Because of the traalloon occlusion (asterisk) of the right ICA, adequate collateraicating arteries (d) was shown.
igure 5. (a) Carotid jugular traumatic AVF (arrow) and pseudofter Jostent graft deployment was obtained. (c) Angiogramarrowheads) at the carotid bifurcation.
emorrhage. Reports about the endovascular results of the
treatment of traumatic lesions of the ECA are scarce; how-ever, a recent review showed good results for the manage-ment of intractable epistaxis with reported success ratesranging from 71%–100% (24). Parent vessel sacrifice was asuccessful treatment technique in our series. When IMAsacrifice is required, the IMA must be occluded distallyto the middle meningeal artery origin. It is also necessary tocheck for anastomotic channels between ECA and ICA to
secondary to gunshot injury. Venous hypertension with refluxg nature of the injury, vessel sacrifice was performed. During
lation through the anterior (c) and the right posterior commu-
sm (asterisk) after stab wound injury. (b) Vessel reconstructionmonth follow-up showing asymptomatic intimal hyperplasia
arrow)nsectinl circu
aneuryat 6-
avoid complications. When the facial artery is occluded, the

re1la5t
PaalcTacstleatiatwctip
ferp“vascbmmv
R
Volume 22 � Number 1 � January � 2011 33
isk of complications is small because of the extensive collat-ral circulation. We have used N-butyl 2-cyanoacrylate since996, and we still use it in our current practice because of itsow cost, high efficiency, and security profile. We dilute thegent with Lipiodol (Guerbet, Aulnay-sous-Bois, France) to0% concentrations when treating fistulas and to 25% whenreating pseudoaneurysms.
During follow-up, we observed an asymptomaticalmaz stent failure with angulation producing asymptom-tic stenosis of the CCA. We treated this patient withngioplasty without complications, and after a 4 year fol-ow-up there has not been evidence of restenosis. Thisomplication has also been reported by Roubin et al (25).he Palmaz stent is no longer used in straight mobilerteries because of the risk of deformation and externalompression, and it has been replaced by self-expandingtents, which have been shown to be safe in those condi-ions. The asymptomatic occlusion observed during fol-ow-up in a patient who stopped antiplatelets could bexpected owing to the thrombogenicity of a stent graft. Welways recommend a double antiaggregation regimen afterhe procedure with clopidogrel for 6 months and aspirinndefinitely. Finally, an additional patient presented withsymptomatic mild intimal hyperplasia (Figure 5). A Jos-ent was used in this case because self-expandable stentsere unavailable at that time. The antiplatelet medication
onsisted of aspirin 100 mg for life and ticlopidine 250 mgwice daily (clopidogrel was unavailable at that time). Dur-ng follow-up, there has not been progression of the hyper-lasia under medical treatment.
In conclusion, in this series, endovascular techniquesor occlusion of extracranial carotid artery lesions were anffective method of treatment. We recommend the use of aeconstructive approach with noncovered stents wheneverossible. Because lateral carotid wall lesions do not havehammer” effect, a noncovered stent is enough to redirectessel flow producing stasis and thrombosis of the pseudo-neurysm. Another advantage is the lower risk of resteno-is. When there is extensive damage of the vessel wall,overed stent deployment or parent artery sacrifice shoulde considered. Endovascular treatment should be theethod of choice for most extracranial carotid artery trau-atic lesions, reserving surgery only for patients with se-
ere bleeding or after failed endovascular treatment.
EFERENCES
1. Irish JC, Hekkenberg R, Gullane PJ, et al. Penetrating and blunt neck
trauma: 10-year review of a Canadian experience. Can J Surg 1997;40:33–38.2. Shatz D, Kirton O, McKinney M, Civetta J. Penetrating neck injuries.In: Shatz D, Kirton O, McKinney M, Civetta J, eds. 2000 Manual ofTrauma and Emergency Surgery. Philadelphia, PA: Saunders, 2000;34 –53.
3. Stallmeyer MJ, Morales RE, Flanders AE. Imaging of traumatic neuro-vascular injury. Radiol Clin North Am 2006; 44:13–39.
4. Demetriades D, Charalambides D, Lakhoo M. Physical examinationand selective conservative management in patients with penetratinginjuries of the neck. Br J Surg 1993; 80:1534–1536.
5. Munera F, Soto JA, Palacio D, Velez SM, Medina E. Diagnosis ofarterial injuries caused by penetrating trauma to the neck: comparison ofhelical CT angiography and conventional angiography. Radiology 2000;216:356–362.
6. Starnes BW, Arthurs ZM. Endovascular management of vasculartrauma. Perspect Vasc Surg Endovasc Ther 2006; 18:114–129.
7. Van Vugt AB. Pitfalls in penetrating trauma. Acta Chir Belg 2003;103:358–363.
8. Larsen DW. Traumatic vascular injuries and their management. Neu-roimaging Clin N Am 2002; 12:249–269.
9. Demetriades D, Salim A, Brown C, Martin M, Rhee P. Neck injuries.Curr Probl Surg 2007; 44:13–85.
10. Pearce WH, Whitchill TA. Carotid and vertebral arterial injuries. SurgClin North Am 1988; 68:705–723.
11. Marotta TR, Buller C, Taylor D, Morris C, Zwimpfer T. Autologousvein-covered stent repair of a cervical internal carotid artery pseudoan-eurysm: technical case report. Neurosurgery 1998; 42:408–412.
12. Fabian TC, Croce MA, Minard G, Bee TK, Cagiannos C, Miller PR.Current issues in trauma. Curr Probl Surg 2002; 39:1160–1164.
13. Redekop G, Marotta T, Weill A. Treatment of traumatic aneurysms andarteriovenous fistulas of the skull base by using endovascular stents.J Neurosurg 2001; 95:412–419.
14. Zwolak RM. Evolution of carotid stenting: payment issues. Semin VascSurg 2008; 21:69–72.
15. Amar AP, Teitelbaum GP, Giannotta SL, Larsen DW. Covered stent-graft repair of the brachiocephalic arteries: technical note. Neurosurgery2002; 51:247–252.
16. Wakhloo AK, Lanzino G, Lieber BB, Hopkins LN. Stents for intracranialaneurysms: the beginning of a new endovascular era. Neurosurgery1998; 43:377–379.
17. Reiter BP, Marin ML, Teodorescu VJ, Mitty HA. Endoluminal repair ofand internal carotid artery pseudoaneurysm. J Vasc Interv Radiol 1998;9:245–248.
18. Aenis M, Stancampiano AP, Wakhloo AK, Lieber BB. Modeling of flowin a straight stented and nonstented side wall aneurysm model. J Bio-mech Eng 1997; 119:206–212.
19. Lieber BB, Gounis MJ. The physics of endoluminal stenting in thetreatment of cerebrovascular aneurysms. Neurol Res 2002; 24:S33–S42.
20. Liu AY, Paulsen RD, Marcellus ML, Steinberg GK, Marks MP. Long-termoutcomes after carotid stent placement treatment of carotid artery dissec-tion. Neurosurgery 1999; 45:1368–1373.
21. Redekop G, Marotta T, Weill A. Treatment of traumatic aneurysms andarteriovenous fistulas of the skull base by using endovascular stents.J Neurosurg 2001; 95:412–419.
22. Joo JY, Ahn JY, Chung YS, et al. Therapeutic endovascular treatmentsfor traumatic carotid artery injuries. J Trauma 2005; 58:1159–1166.
23. DuBose J, Recinos G, Teixeira PG, Inaba K, Demetriades D.Endovascular stenting for the treatment of traumatic internal carotidinjuries: expanding experience. J Trauma 2008; 65:1561–1566.
24. Gandhi D, Gemmete JJ, Ansari SA, Gujar SK, Mukherji SK. Interventionalneuroradiology of the head and neck. AJNR Am J Neuroradiol 2008; 29:1806–1815.
25. Roubin GS, Yadav S, Iyer SS, Vitek J. Carotid stent-supported angio-plasty: a neurovascular intervention to prevent stroke. Am J Cardiol 1996;
78:8–12.
Related Documents











