European Journal of Radiology 65 (2008) 491–497 Endovascular management performed percutaneously of isolated iliac artery aneurysms Florian Wolf ∗ , Christian Loewe, Manfred Cejna, Maria Schoder, Thomas Rand, Joachim Kettenbach, Albert Dirisamer, Johannes Lammer, Martin Funovics Medical University of Vienna, Clinical Department of Cardiovascular and Interventional Radiology, Waehringer Guertel 18-20, A-1090 Vienna, Austria Received 10 October 2006; received in revised form 28 February 2007; accepted 4 April 2007 Abstract Purpose: To report about the endovascular treatment of isolated iliac artery aneurysms (IIAA) with stentgraft placement and transluminal or CT-guided embolization of the internal iliac artery or the combination of these methods. Methods and materials: Over a period of 5.6 years, 36 interventions were performed in 20 patients with 23 IIAAs. In a retrospective analysis patient records were reviewed. The CT-angiography follow-up was evaluated for the presence of re-perfusion of the IIAA and for change of aneurysm diameter. Results: Primary success was achieved in 15/23 aneurysms (65%), and secondary success in 21/23 aneurysms (91%). In 5/23 cases two interventions and in 1/23 cases three interventions were necessary to achieve secondary success. Embolization alone, as a therapy for aneurysms involving only the internal iliac artery, had a success rate of 27%. No procedure-related minor or major complications occurred. Mean decrease of aneurysm size during a mean observation period of 14.1 months was 6.9% which was not significant (p = 0.3; 95% confidence interval +7–21%). Conclusion: Endovascular therapy of isolated iliac artery aneurysms performed percutaneously has become a treatment alternative to open surgical repair. This method is feasible and safe with low procedure-related morbidity and mortality. However, on average more than one intervention has to be performed to achieve successful permanent exclusion of the aneurysm and embolization alone in isolated internal iliac artery aneurysms is not sufficient. © 2007 Elsevier Ireland Ltd. All rights reserved. Keywords: Iliac aneurysm; Therapeutic embolization; Stent; Computed tomography scanner; X-ray; Interventional radiology 1. Introduction The prevalence of isolated iliac artery aneurysms ranges from 0.03 to 0.1% according to autopsy studies from both North America and Europe [1,2]. Isolated iliac artery aneurysms, as incidental intraoperative findings in vascular surgery patients, are also rare with a reported frequency of fewer than 2% [3]. Some authors have reported that isolated iliac artery aneurysms carry a risk of spontaneous rupture [4] of up to 40% [5] with an associated mortality rate of up to 80% [6,7]. Open surgical repair of IIAAs is a major procedure, which is associated with considerable procedure-related morbidity and mortality rates. This retrospective analysis reports techni- ∗ Corresponding author. Tel.: +43 1 40400 5802; fax: +43 1 40400 5830. E-mail address: fl[email protected] (F. Wolf). cal details, clinical success rates and the mid-term results of endovascular treatment of isolated iliac artery aneurysms. 2. Methods and materials 2.1. Study group Over a period of 5.6 years in 20 patients (18 male, 2 female) endovascular treatment of 23 isolated iliac artery aneurysms (IIAA) was performed. Mean aneurysm size was 54 mm (range 20–115 mm). Three of these patients suffered from bilateral IIAAs. All the patients were considered at high operative risk, due to high age and/or high co-morbidity, and therefore endovascular treatment was favoured. Mean patient age was 69 ± 8.9 years (range 35–85 years). The majority of patients (15/20, 75%) had no symptoms and 0720-048X/$ – see front matter © 2007 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejrad.2007.04.004

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
A
PCMrdRat
iCrtn©
K
1
fAia
a[
ia
0d
European Journal of Radiology 65 (2008) 491–497
Endovascular management performed percutaneously of isolatediliac artery aneurysms
Florian Wolf ∗, Christian Loewe, Manfred Cejna, Maria Schoder, Thomas Rand,Joachim Kettenbach, Albert Dirisamer, Johannes Lammer, Martin Funovics
Medical University of Vienna, Clinical Department of Cardiovascular and Interventional Radiology,Waehringer Guertel 18-20, A-1090 Vienna, Austria
Received 10 October 2006; received in revised form 28 February 2007; accepted 4 April 2007
bstract
urpose: To report about the endovascular treatment of isolated iliac artery aneurysms (IIAA) with stentgraft placement and transluminal orT-guided embolization of the internal iliac artery or the combination of these methods.ethods and materials: Over a period of 5.6 years, 36 interventions were performed in 20 patients with 23 IIAAs. In a retrospective analysis patient
ecords were reviewed. The CT-angiography follow-up was evaluated for the presence of re-perfusion of the IIAA and for change of aneurysmiameter.esults: Primary success was achieved in 15/23 aneurysms (65%), and secondary success in 21/23 aneurysms (91%). In 5/23 cases two interventionsnd in 1/23 cases three interventions were necessary to achieve secondary success. Embolization alone, as a therapy for aneurysms involving onlyhe internal iliac artery, had a success rate of 27%. No procedure-related minor or major complications occurred.
Mean decrease of aneurysm size during a mean observation period of 14.1 months was 6.9% which was not significant (p = 0.3; 95% confidencenterval +7–21%).
onclusion: Endovascular therapy of isolated iliac artery aneurysms performed percutaneously has become a treatment alternative to open surgicalepair. This method is feasible and safe with low procedure-related morbidity and mortality. However, on average more than one intervention haso be performed to achieve successful permanent exclusion of the aneurysm and embolization alone in isolated internal iliac artery aneurysms isot sufficient.
2007 Elsevier Ireland Ltd. All rights reserved.
aphy
ce
2
2
e(
eywords: Iliac aneurysm; Therapeutic embolization; Stent; Computed tomogr
. Introduction
The prevalence of isolated iliac artery aneurysms rangesrom 0.03 to 0.1% according to autopsy studies from both Northmerica and Europe [1,2]. Isolated iliac artery aneurysms, as
ncidental intraoperative findings in vascular surgery patients,re also rare with a reported frequency of fewer than 2% [3].
Some authors have reported that isolated iliac arteryneurysms carry a risk of spontaneous rupture [4] of up to 40%5] with an associated mortality rate of up to 80% [6,7].
Open surgical repair of IIAAs is a major procedure, whichs associated with considerable procedure-related morbiditynd mortality rates. This retrospective analysis reports techni-
∗ Corresponding author. Tel.: +43 1 40400 5802; fax: +43 1 40400 5830.E-mail address: [email protected] (F. Wolf).
2I
ht
T
720-048X/$ – see front matter © 2007 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2007.04.004
scanner; X-ray; Interventional radiology
al details, clinical success rates and the mid-term results ofndovascular treatment of isolated iliac artery aneurysms.
. Methods and materials
.1. Study group
Over a period of 5.6 years in 20 patients (18 male, 2 female)ndovascular treatment of 23 isolated iliac artery aneurysmsIIAA) was performed. Mean aneurysm size was 54 mm (range0–115 mm). Three of these patients suffered from bilateralIAAs.
All the patients were considered at high operative risk, due to
igh age and/or high co-morbidity, and therefore endovascularreatment was favoured.Mean patient age was 69 ± 8.9 years (range 35–85 years).he majority of patients (15/20, 75%) had no symptoms and
492 F. Wolf et al. / European Journal of Radiology 65 (2008) 491–497
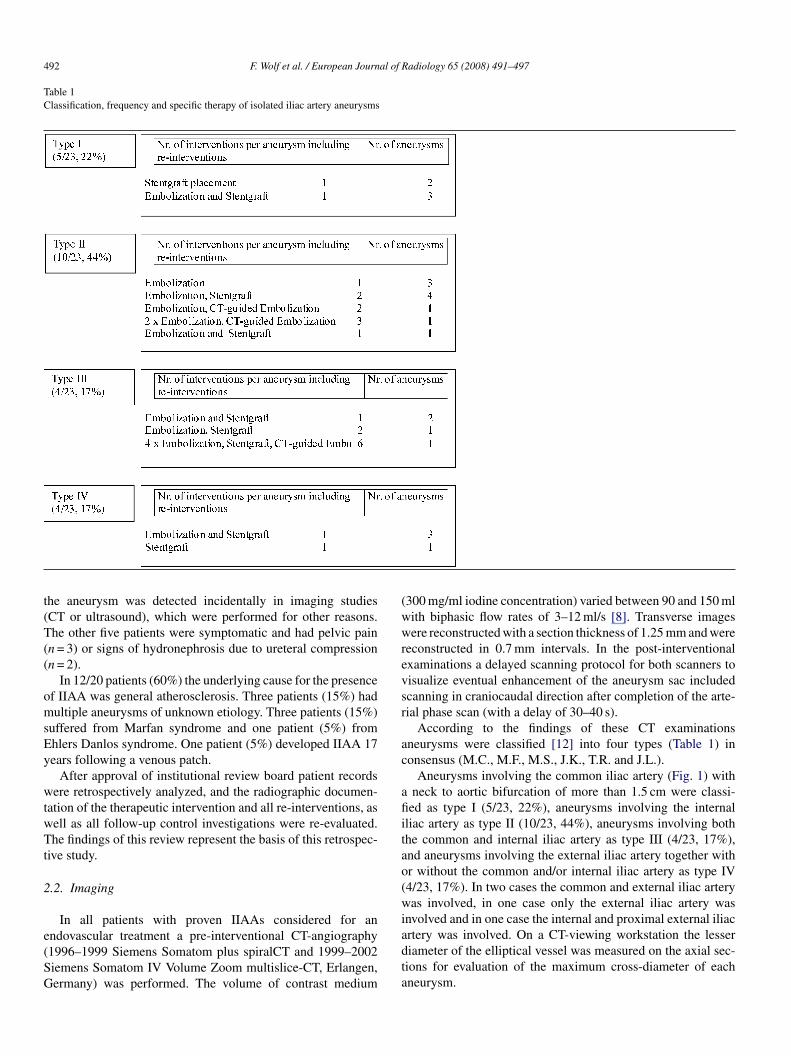
Table 1Classification, frequency and specific therapy of isolated iliac artery aneurysms
t(T((
omsEy
wtwTt
2
e(SG
(wwrevsr
ac
afiitao(wi
he aneurysm was detected incidentally in imaging studiesCT or ultrasound), which were performed for other reasons.he other five patients were symptomatic and had pelvic pain
n = 3) or signs of hydronephrosis due to ureteral compressionn = 2).
In 12/20 patients (60%) the underlying cause for the presencef IIAA was general atherosclerosis. Three patients (15%) hadultiple aneurysms of unknown etiology. Three patients (15%)
uffered from Marfan syndrome and one patient (5%) fromhlers Danlos syndrome. One patient (5%) developed IIAA 17ears following a venous patch.
After approval of institutional review board patient recordsere retrospectively analyzed, and the radiographic documen-
ation of the therapeutic intervention and all re-interventions, asell as all follow-up control investigations were re-evaluated.he findings of this review represent the basis of this retrospec-
ive study.
.2. Imaging
In all patients with proven IIAAs considered for an
ndovascular treatment a pre-interventional CT-angiography1996–1999 Siemens Somatom plus spiralCT and 1999–2002iemens Somatom IV Volume Zoom multislice-CT, Erlangen,ermany) was performed. The volume of contrast mediumadta
300 mg/ml iodine concentration) varied between 90 and 150 mlith biphasic flow rates of 3–12 ml/s [8]. Transverse imagesere reconstructed with a section thickness of 1.25 mm and were
econstructed in 0.7 mm intervals. In the post-interventionalxaminations a delayed scanning protocol for both scanners toisualize eventual enhancement of the aneurysm sac includedcanning in craniocaudal direction after completion of the arte-ial phase scan (with a delay of 30–40 s).
According to the findings of these CT examinationsneurysms were classified [12] into four types (Table 1) inonsensus (M.C., M.F., M.S., J.K., T.R. and J.L.).
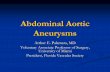
Aneurysms involving the common iliac artery (Fig. 1) withneck to aortic bifurcation of more than 1.5 cm were classi-
ed as type I (5/23, 22%), aneurysms involving the internalliac artery as type II (10/23, 44%), aneurysms involving bothhe common and internal iliac artery as type III (4/23, 17%),nd aneurysms involving the external iliac artery together withr without the common and/or internal iliac artery as type IV4/23, 17%). In two cases the common and external iliac arteryas involved, in one case only the external iliac artery was
nvolved and in one case the internal and proximal external iliac
rtery was involved. On a CT-viewing workstation the lesseriameter of the elliptical vessel was measured on the axial sec-ions for evaluation of the maximum cross-diameter of eachneurysm.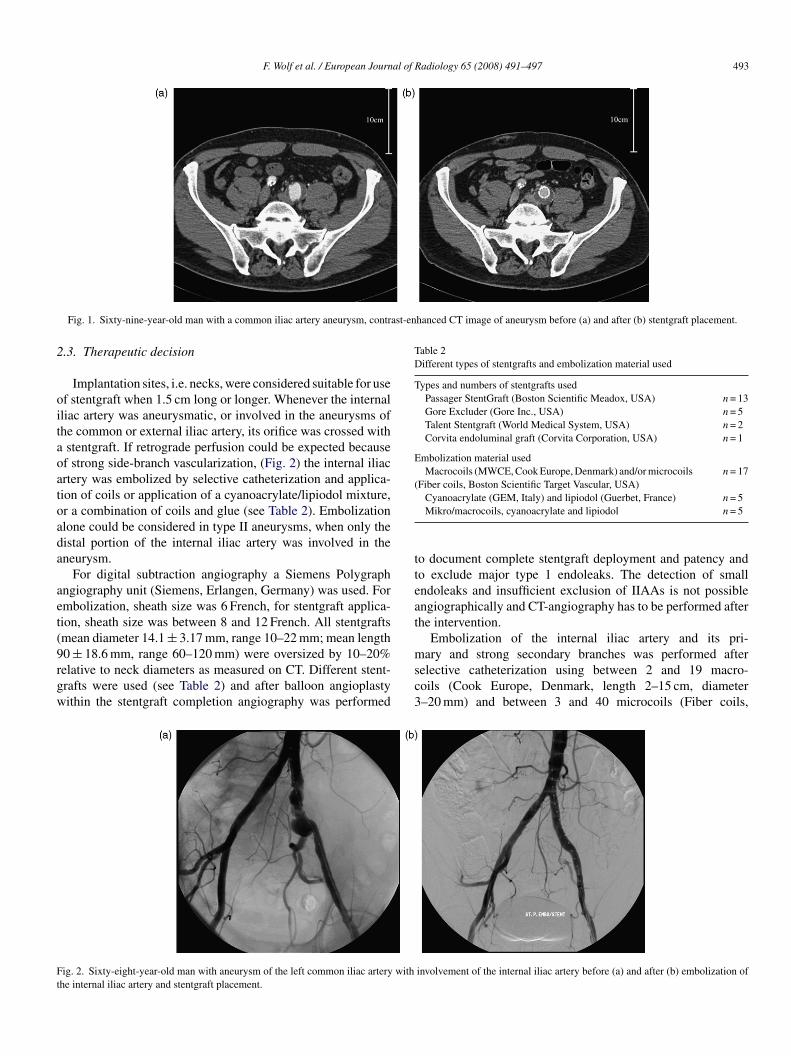
F. Wolf et al. / European Journal of Radiology 65 (2008) 491–497 493
ast-enhanced CT image of aneurysm before (a) and after (b) stentgraft placement.
2
oitaoatoada
aet(9rgw
Table 2Different types of stentgrafts and embolization material used
Types and numbers of stentgrafts usedPassager StentGraft (Boston Scientific Meadox, USA) n = 13Gore Excluder (Gore Inc., USA) n = 5Talent Stentgraft (World Medical System, USA) n = 2Corvita endoluminal graft (Corvita Corporation, USA) n = 1
Embolization material usedMacrocoils (MWCE, Cook Europe, Denmark) and/or microcoils
(Fiber coils, Boston Scientific Target Vascular, USA)n = 17
tteat
Ft
Fig. 1. Sixty-nine-year-old man with a common iliac artery aneurysm, contr
.3. Therapeutic decision
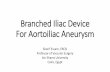
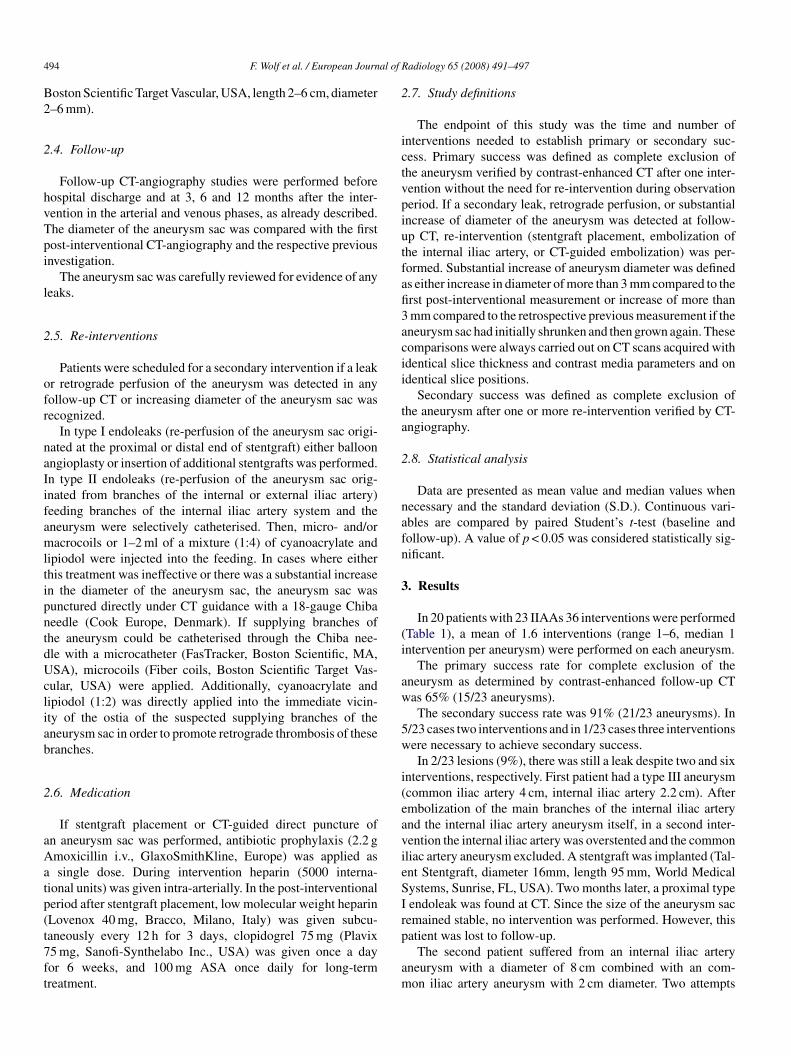
Implantation sites, i.e. necks, were considered suitable for usef stentgraft when 1.5 cm long or longer. Whenever the internalliac artery was aneurysmatic, or involved in the aneurysms ofhe common or external iliac artery, its orifice was crossed withstentgraft. If retrograde perfusion could be expected becausef strong side-branch vascularization, (Fig. 2) the internal iliacrtery was embolized by selective catheterization and applica-ion of coils or application of a cyanoacrylate/lipiodol mixture,r a combination of coils and glue (see Table 2). Embolizationlone could be considered in type II aneurysms, when only theistal portion of the internal iliac artery was involved in theneurysm.
For digital subtraction angiography a Siemens Polygraphngiography unit (Siemens, Erlangen, Germany) was used. Formbolization, sheath size was 6 French, for stentgraft applica-ion, sheath size was between 8 and 12 French. All stentgraftsmean diameter 14.1 ± 3.17 mm, range 10–22 mm; mean length
0 ± 18.6 mm, range 60–120 mm) were oversized by 10–20%elative to neck diameters as measured on CT. Different stent-rafts were used (see Table 2) and after balloon angioplastyithin the stentgraft completion angiography was performedmsc3
ig. 2. Sixty-eight-year-old man with aneurysm of the left common iliac artery withhe internal iliac artery and stentgraft placement.
Cyanoacrylate (GEM, Italy) and lipiodol (Guerbet, France) n = 5Mikro/macrocoils, cyanoacrylate and lipiodol n = 5
o document complete stentgraft deployment and patency ando exclude major type 1 endoleaks. The detection of smallndoleaks and insufficient exclusion of IIAAs is not possiblengiographically and CT-angiography has to be performed afterhe intervention.
Embolization of the internal iliac artery and its pri-
ary and strong secondary branches was performed afterelective catheterization using between 2 and 19 macro-oils (Cook Europe, Denmark, length 2–15 cm, diameter–20 mm) and between 3 and 40 microcoils (Fiber coils,
involvement of the internal iliac artery before (a) and after (b) embolization of
4 al of R
B2
2
hvTpi
l
2
ofr
naIifamltipntdUcliab
2
aAatp(t7ft
2
ictvpiutfafi3acii
ta
2
nafn
3
(i
aw
5w
i(eavieS
94 F. Wolf et al. / European Journ
oston Scientific Target Vascular, USA, length 2–6 cm, diameter–6 mm).
.4. Follow-up
Follow-up CT-angiography studies were performed beforeospital discharge and at 3, 6 and 12 months after the inter-ention in the arterial and venous phases, as already described.he diameter of the aneurysm sac was compared with the firstost-interventional CT-angiography and the respective previousnvestigation.
The aneurysm sac was carefully reviewed for evidence of anyeaks.
.5. Re-interventions
Patients were scheduled for a secondary intervention if a leakr retrograde perfusion of the aneurysm was detected in anyollow-up CT or increasing diameter of the aneurysm sac wasecognized.
In type I endoleaks (re-perfusion of the aneurysm sac origi-ated at the proximal or distal end of stentgraft) either balloonngioplasty or insertion of additional stentgrafts was performed.n type II endoleaks (re-perfusion of the aneurysm sac orig-nated from branches of the internal or external iliac artery)eeding branches of the internal iliac artery system and theneurysm were selectively catheterised. Then, micro- and/oracrocoils or 1–2 ml of a mixture (1:4) of cyanoacrylate and
ipiodol were injected into the feeding. In cases where eitherhis treatment was ineffective or there was a substantial increasen the diameter of the aneurysm sac, the aneurysm sac wasunctured directly under CT guidance with a 18-gauge Chibaeedle (Cook Europe, Denmark). If supplying branches ofhe aneurysm could be catheterised through the Chiba nee-le with a microcatheter (FasTracker, Boston Scientific, MA,SA), microcoils (Fiber coils, Boston Scientific Target Vas-
ular, USA) were applied. Additionally, cyanoacrylate andipiodol (1:2) was directly applied into the immediate vicin-ty of the ostia of the suspected supplying branches of theneurysm sac in order to promote retrograde thrombosis of theseranches.
.6. Medication
If stentgraft placement or CT-guided direct puncture ofn aneurysm sac was performed, antibiotic prophylaxis (2.2 gmoxicillin i.v., GlaxoSmithKline, Europe) was applied assingle dose. During intervention heparin (5000 interna-
ional units) was given intra-arterially. In the post-interventional
eriod after stentgraft placement, low molecular weight heparinLovenox 40 mg, Bracco, Milano, Italy) was given subcu-aneously every 12 h for 3 days, clopidogrel 75 mg (Plavix5 mg, Sanofi-Synthelabo Inc., USA) was given once a dayor 6 weeks, and 100 mg ASA once daily for long-termreatment.Irp
am
adiology 65 (2008) 491–497
.7. Study definitions
The endpoint of this study was the time and number ofnterventions needed to establish primary or secondary suc-ess. Primary success was defined as complete exclusion ofhe aneurysm verified by contrast-enhanced CT after one inter-ention without the need for re-intervention during observationeriod. If a secondary leak, retrograde perfusion, or substantialncrease of diameter of the aneurysm was detected at follow-p CT, re-intervention (stentgraft placement, embolization ofhe internal iliac artery, or CT-guided embolization) was per-ormed. Substantial increase of aneurysm diameter was defineds either increase in diameter of more than 3 mm compared to therst post-interventional measurement or increase of more thanmm compared to the retrospective previous measurement if theneurysm sac had initially shrunken and then grown again. Theseomparisons were always carried out on CT scans acquired withdentical slice thickness and contrast media parameters and ondentical slice positions.
Secondary success was defined as complete exclusion ofhe aneurysm after one or more re-intervention verified by CT-ngiography.
.8. Statistical analysis
Data are presented as mean value and median values whenecessary and the standard deviation (S.D.). Continuous vari-bles are compared by paired Student’s t-test (baseline andollow-up). A value of p < 0.05 was considered statistically sig-ificant.
. Results
In 20 patients with 23 IIAAs 36 interventions were performedTable 1), a mean of 1.6 interventions (range 1–6, median 1ntervention per aneurysm) were performed on each aneurysm.
The primary success rate for complete exclusion of theneurysm as determined by contrast-enhanced follow-up CTas 65% (15/23 aneurysms).The secondary success rate was 91% (21/23 aneurysms). In
/23 cases two interventions and in 1/23 cases three interventionsere necessary to achieve secondary success.In 2/23 lesions (9%), there was still a leak despite two and six
nterventions, respectively. First patient had a type III aneurysmcommon iliac artery 4 cm, internal iliac artery 2.2 cm). Aftermbolization of the main branches of the internal iliac arterynd the internal iliac artery aneurysm itself, in a second inter-ention the internal iliac artery was overstented and the commonliac artery aneurysm excluded. A stentgraft was implanted (Tal-nt Stentgraft, diameter 16mm, length 95 mm, World Medicalystems, Sunrise, FL, USA). Two months later, a proximal typeendoleak was found at CT. Since the size of the aneurysm sacemained stable, no intervention was performed. However, this
atient was lost to follow-up.The second patient suffered from an internal iliac arteryneurysm with a diameter of 8 cm combined with an com-on iliac artery aneurysm with 2 cm diameter. Two attempts

al of R
tmwttltaDdpattp
taashi
svttsa
d
bc
fn
(po6
4
tafi3rcoawa
lwaaTpfgf
mpwcaItEIlctoa
aPiitg(neteiasb
oaicsn
dain
F. Wolf et al. / European Journ
o embolize the main branches of the internal iliac artery withicro- and macrocoils and the proximal internal iliac arteryith macrocoils the failed to prevent retrograde perfusion of
he aneurysm sac. As the aneurysm grew to 11 cm in diame-er two stentgrafts (Talent Stentgraft, diameters 18 and 22 mm,engths 110 and 105 mm) were implanted from the commono the external iliac artery with exclusion of the common iliacrtery aneurysm across the ostium of the internal iliac artery.ue to persistent perfusion from branches taking of from theeep femoral artery, three additional embolization attempts wereerformed—two trans-catheter and the other under CT-guidancend direct puncture as previously described without success. Athe 15-month CT follow-up, following the initial intervention,he aneurysm remains stabled at 11 cm diameter with a persistenterfusion.
Regarding aneurysm type, the success rates were as follows:herapy of type I (n = 5) and type IV (n = 4) aneurysms had
primary success rate of 100%. Therapy of type II (n = 10)neurysms had a primary success rate of 40% and a secondaryuccess rate of 100%, and therapy of type III (n = 4) aneurysmsad a primary and secondary success rate of 50%. For detailednformation about therapy of each aneurysm type see Table 1.
Stentgraft deployment (n = 3) and the combination oftentgraft deployment and embolization (n = 9) as primary inter-entions had a primary success of 100%. Embolization alone ashe primary intervention had a primary success of 27% (3/11). Inhe other eight cases, secondary embolization (n = 2), secondarytentgraft placement (n = 5), or both (n = 1) had to be performedfter primary embolization.
All 36 interventions were completed without clinically evi-ent minor or major complications.
In 20/23 patients embolization of internal iliac arteryranches was performed. 4/20 patients (20%) developed mildlaudication of the buttocks after the intervention.
After 7/36 interventions (20%) a leak was detected in theollow-up CT examination although the procedure was termi-ated successful. Re-interventions were required.
Pre-treatment aneurysm size ranged from 20 to 115 mmmean 54 ± 29). In 12 cases measurement of aneurysm size wasossible after a mean follow-up time of 14.1 months. The changef aneurysm size was not significant with a mean decrease of.9% (p = 0.3; 95% confidence interval +7 to −21%).
. Discussion
Because of their pelvic localization, IIAAs produce symp-oms typically late when they have reached an advanced sizend are often incidental findings on imaging studies per-ormed for other indications. Elective surgical treatment isndicated in the majority of patients for aneurysms larger thancm in diameter [6]. Surgical reconstruction with aneurysm
esection and graft interposition is a relatively complex pro-edure with the possibility of severe complications like injury
f adjacent veins during surgical procedure [9]. Perioper-tive mortality for elective operations is 7–13% [10–12],hereas mortality approaches 30% in cases of ruptured iliacneurysms [10,13].
padh
adiology 65 (2008) 491–497 495
In this series, primary therapeutic success of endovascu-ar therapy for type I (n = 7) and type IV (n = 4) aneurysmsas 100%. Primary therapeutic success for type II (n = 10)
neurysms was 40%, with 100% secondary success. In type IIIneurysms (n = 4), primary and secondary success rate was 50%.herapy of type II and type III aneurysms seems to be more com-licated than therapy of type I and IV aneurysms. The reasonor that is the involvement of the internal iliac artery. Retro-rade perfusion by side branches of the internal iliac artery is arequent cause of a secondary leak.
Embolization alone without stentgraft placement as the pri-ary therapeutic approach was performed in 11 cases with a
rimary success in only 3 cases (27%). These three aneurysmsere type II aneurysms and showed a proximal neck to the
ommon iliac artery of more than 1.5 cm. The other eightneurysms were either type II aneurysms (n = 6) as well, or typeII aneurysms (n = 2) and required more than one emboliza-ion (n = 2) or the additional placement of a stentgraft (n = 6).mbolization alone was unsuccessfully attempted in two type
II aneurysms (small aneurysm of the common iliac artery andarge aneurysm of the internal iliac artery) and should not beonsidered as a viable treatment option. The primary therapeu-ic approach for type III aneurysms should be the combinationf stentgraft placement and embolization of the internal iliacrtery.
Stentgraft placement alone was performed in type Ineurysms in four cases and in type IV aneurysms in one case.rimary success rate was 100%. In both cases the neck to the
nternal iliac artery was more than 1.5 cm. These results are sim-lar to the results of Scheinert et al. [14], when the successfulreatment of common or external iliac artery aneurysms by stent-raft placement was described with a technical success of 97.9%47 of 48 cases). If embolization of the internal iliac artery wasecessary, these patients were excluded from their study. Schein-rt concluded that the critical selection of patients with regardo the suitability for an endovascular aneurysm repair withoutmbolization is very important. There must be a sufficient prox-mal and distal neck of greater than 1.5 cm and the internal iliacrtery should not be involved. If the proximal neck to the aorta ismaller than 1.5 cm, application of a bifurcated stentgraft woulde therapy of choice [15].
Stentgraft placement and embolization is the primary methodf choice for type II aneurysms, if it is obvious that embolizationlone will not be sufficient because the aneurysmatic internalliac artery reaches the common iliac artery. In this series theombined approach was successful in nine cases with a primaryuccess of 100% (types I and IV: n = 3; type III: n = 2; type II:= 1).
CT-guided puncture of the aneurysm sac with a Chiba nee-le and following embolization was successful in two of threeneurysms. In all three cases, the internal iliac artery wasnvolved and one or more endoluminal embolizations of all inter-al iliac artery branches had been performed previously. For
uncture of the aneurysm sac, at our institution steel needlesre generally preferred to 4F or 5F sheaths due to their smalleriameter (in order to minimize bleeding complications in case ofigh pressure in the sac), and due to their high stiffness and better
4 al of R
gicnlkaCtits
fswaIp
ihesapciaesoti
a−snSit
aeeA1
5
ltm
l
aa
denp
R
[
[
[
[
[
[
[
[
[
[
[
96 F. Wolf et al. / European Journ
uidance. The risk of cutting the microcatheter during retractions controlled by simultaneously retracting needle and micro-atheter, thereby avoiding kinking of the microcatheter near theeedle tip. Reports about this kind of therapy are very rare in theiterature [16,17] and embolization is performed with differentinds of tissue adhesive (mixture of thrombin, fibrinogen, andprotinin, and a combination of thrombin and cyanoacrylate).T-guided percutaneous embolization should be considered as
herapeutic option for repair of internal iliac artery aneurysmf there are no other therapeutic options left, and if emboliza-ion of all internal iliac artery branches was done before withoutuccessful exclusion of the aneurysm.
After 7/36 interventions (20%) a leak was detected in theollow-up examinations although the procedure was terminateduccessful. Re-interventions were required. Procedural successith absence of a leak in the control angiography immediately
fter the intervention does not exclude a small re-perfusion (typeI) endoleak. For that reason, a contrast-enhanced CT should beerformed after the intervention.
Procedure-related complications such as death, major bleed-ng, distal embolization, and transient bowel ischemia, whichave been reported in single cases by Marin et al. [18], Cardont al. [19], and Sanchez et al. [20] were not observed in thistudy. In this study in 20/23 aneurysms (87%) the internal iliacrtery was embolized alone or in combination with stentgraftlacement. Nevertheless, in the follow-up period in only 4/20ases (20%) mild claudication of the buttocks was found. Sim-lar results were found by Cormier et al. [21]. Although someuthors [22,23] found high complication rates of 26–41% aftermbolizing the internal iliac artery and there are some discus-ions [24] about the accurate use of this method, embolizationf the internal iliac artery is crucial in the majority of cases ifhe aneurysm involves the internal iliac artery or if the internalliac artery is overstented with a stentgraft.
In this study, there was a mean decrease of the maximumneurysm diameter of 6.9% (p = 0.3, 95% confidence interval21 to +7 %) in the 12 cases with follow-up. These results are
imilar to the results of Scheinert et al. [14], who also foundo significant decrease of aneurysm diameter in 48 aneurysms.ahgal et al. [25] conclude in their study about diameter changes
n IIAAs 1–6 years after endovascular graft repair that properlyreated aneurysms decrease in size 0.5 ± −0.1 cm/year.
The major limitation of this study is that it is a retrospectivenalysis with a heterogenous patient group with very differ-nt types of aneurysms. However, randomized trials comparingndovascular versus open repair by now cannot be justified.nother limitation is the relative short follow-period of mean4.1 months with a large range from 3 to 56 months.
. Conclusion
In this study it was shown that endovascular therapy of iso-ated iliac artery aneurysms has become a treatment alternative
o open surgical repair, especially for patients with severe co-orbid conditions.The methods applied are technically feasible and safe with
ow procedure-related morbidity.
[
adiology 65 (2008) 491–497
In the majority of cases, embolization of the internal iliacrtery is inevitable in order to obtain complete exclusion of theneurysm.
The absence of a re-perfusion leak on angiography imme-iately after the intervention is not a predictor of successfulxclusion of the aneurysm. For that reason, follow-up exami-ations with CT (in particularly during arterial and late venoushase) are necessary to discover possible leaks.
eferences
[1] Brunkwall J, Hauksson H, Bengtsson H, Bergqvist D, Takolander R,Bergentz SE. Solitary aneurysms of the iliac arterial system: an estimateof their frequency and occurrence. J Vasc Surg 1989;10:381–4.
[2] Lucke B, Rea MH. Studies on aneurysms. JAMA 1921;77:935–40.[3] McCready RA, Pairolero PC, Gilmore JC, Kazmier FJ, Cherry Jr
KJ, Hollier LH. Isolated iliac artery aneurysms. Surgery 1983;93:688–93.
[4] Parry DJ, Kessel D, Scott DJ. Simplifying the internal iliac artery aneurysm.Ann R Coll Surg Engl 2001;83:302–8.
[5] Dix FP, Titi M, Al-Khaffaf H. The isolated iliac artery aneurysm—a review.Eur J Vasc Endovasc Surg 2005;30:119–29.
[6] Richardson JW, Greenfield LJ. Natural history and management of iliacaneurysms. J Vasc Surg 1988;8:165–71.
[7] Bolin T, Lund K, Skau T. Isolated aneurysms of the iliac artery: what arethe chances of rupture? Eur J Vasc Surg 1988;2:213–5.
[8] Fleischmann D, Rubin GD, Bankier AA, Hittmair K. Improved unifor-mity of aortic enhancement with customized contrast medium injectionprotocols at CT angiography. Radiology 2000;214:363–71.
[9] Matsumoto K, Matsubara K, Watada S, et al. Surgical and endovascularprocedures for treating isolated iliac artery aneurysms: ten-year experience.World J Surg 2004;28:797–800.
10] Young R, Ostertag H. Incidence, etiology and risk of rupture of aorticaneurysm. An autopsy study. Dtsch Med Wochenschr 1987;112:1253–6.
11] Schroeder RA, Flanagan TL, Kron I, Tribble CG. A safe approach to thetreatment of iliac artery aneurysms: aortobifemoral bypass grafting withexclusion of the aneurysm. Am J Surg 1991;57:624–6.
12] Reber PU, Brunner K, Hakki H, Stirnemann P, Kniemayer HW. Frequency,classification and treatment of isolated iliac artery aneurysms. Chirurg2001;72:419–24.
13] Nachbuhr BH, Inderbitzi RGC, Bar W. Isolated iliac aneurysms. Eur J VascSurg 1991;5:375–81.
14] Scheinert D, Schroder M, Steinkamp H, Ludwig J, Biamino G. Treatmentof iliac artery aneurysms by percutaneous implantation of stent grafts.Circulation 2000;102:253–8.
15] Fahrni M, Lachat MM, Wildermuth S, Pfammatter T. Endovascular ther-apeutic options for isolated iliac aneurysms with a working classification.Cardivasc Intervent Radiol 2003;26:443–7.
16] Owen RJ, Jackson R, Loose HW, Lees TA, Dunlop P, Rose JDG. Per-cutaneous ablation of an internal iliac aneurysm using tissue adhesive.Cardiovasc Intervent Radiol 2000;23:389–91.
17] Rogoff PA, Stock JR. Percoutaneous transabdominal embolization of aniliac artery aneurysm. AJR 1985;145:1258–60.
18] Marin ML, Veith FJ, Lyon RT, Cynamon J, Sanchez LA. Transfemoralendovascular repair of iliac artery aneurysms. Am J Surg 1995;170:172–82.
19] Cardon JM, Cardon A, Joyeux A, Vidal V, Noblet D. Endovascular repair ofiliac artery aneurysm with endopro system. I. A multicentric French study.J Cardivasc Surg (Torino) 1996;37:45–50.
20] Sanchez LA, Patel AV, Ohki T, et al. Midterm experience with the endovas-
cular treatment of isolated iliac aneurysms. J Vasc Surg 1999;30:907–14.21] Cormier F, Al Ayoubi A, Laridon D, Melki JP, FIchelle JM, Cormier JM.Endovascular treatment of iliac artery aneurysms with covered stents. AnnVasc Surg 2000;14:561–6.

al of R
[
[
[24] Soulen CS, Fairman RM, Baum RA. Embolization of the internal iliac
F. Wolf et al. / European Journ
22] Razavi MK, DeGroot M, Olcott III C, et al. Internal iliac artery embolization
in the stent-graft treatment of aortoiliac aneurysms: analysis of outcomesand complications. JVIR 2000;11:561–6.23] Lee CW, Kaufman JA, Fan CM, et al. Clinical outcome of internal arteryocclusions during endovascular treatment of aorto-iliac aneurysmal dis-eases. JVIR 2000;11:567–71.
[
adiology 65 (2008) 491–497 497
artery: still more to learn. JVIR 2000;11:543–5.25] Sahgal A, Veith FJ, Lipsitz E, et al. Diameter changes in isolated iliac
artery aneurysms 1 to 6 years after endovascular graft repair. J Vasc Surg2001;33:289–95.
Related Documents