Circulation Journal Vol.76, March 2012 Circulation Journal Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp n increased number of circulating endothelial progeni- tor cells (EPC) has been associated with better out- comes in patients with coronary artery disease. 1–7 Microparticles are small plasma membrane structures derived from many cells, including apoptotic or activated endothelial cells and platelets. Recent evidence has suggested a key role of the endothelial microparticles (EMP) and platelet micropar- ticles (PMP) in vascular homeostasis. 8–10 In addition, a recent study has shown that their levels were predictors of cardiovas- cular events in patients with stable coronary disease. 11 Although the use of high doses of statins in acute coronary disease has been associated with increased EPC and micropar- ticles, some of these results seem to have been influenced by the infarct size or the extension of vascular injury following coronary angioplasty. 12–14 Furthermore, atorvastatin and clopi- dogrel are drugs commonly prescribed for acute coronary syn- drome and both are partially metabolized via cytochrome P450 3A4, raising concerns about pharmacokinetic interactions. 15 Clopidogrel therapy was reported to change the number of EMP, 16 but the literature is scarce on its effects on PMP or EPC, particularly when combined with high-dose statins. In the present study we therefore examined possible interac- tions between atorvastatin and clopidogrel and their effects alone or combined on platelet function, circulating micropar- ticles and EPC among patients with stable coronary disease. A Received October 11, 2011; revised manuscript received November 17, 2011; accepted November 21, 2011; released online December 28, 2011 Time for primary review: 13 days Department of Medicine, Federal University of São Paulo, São Paulo (C.N.F., L.F.M.P., M.C.O.I., M.K.C.B., R.S., H.T.B., S.H.K., S.P.B., F.A.H.F.); National Institute of Complex Fluids, São Paulo (M.C.O.I., F.A.H.F.); and Department of Pharmacology, State University of Campinas, Campinas, São Paulo (G.d.N.), Brazil Mailing address: Francisco Antonio Helfenstein Fonseca, MD, PhD, Department of Medicine, Federal University of São Paulo, Rua Pedro de Toledo, 276, São Paulo, SP 04039030, Brazil. E-mail: [email protected] ISSN-1346-9843 doi:10.1253/circj.CJ-11-1145 All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected] Endothelial Progenitor Cell Mobilization and Platelet Microparticle Release Are Influenced by Clopidogrel Plasma Levels in Stable Coronary Artery Disease Carolina N. França, PhD; Luiz F.M. Pinheiro, MD, PhD; Maria C.O. Izar, MD, PhD; Milena K.C. Brunialti, PhD; Reinaldo Salomão, MD, PhD; Henrique T. Bianco, MD; Soraia H. Kasmas, BSc; Simone P. Barbosa, BSc; Gilberto de Nucci, MD, PhD; Francisco A.H. Fonseca, MD, PhD Background: Increased numbers of endothelial (EMP) and platelet (PMP) microparticles have been related to car- diovascular risk factors and coronary artery disease. Little is known about the early effects of statins and clopidogrel on these new biomarkers of vascular homeostasis. The aim of the present study was to evaluate pharmacokinetic interactions between atorvastatin and clopidogrel and their effects, alone or combined, on EMP, PMP, and endothelial progenitor cells (EPC). Methods and Results: A prospective open-label study enrolled subjects with stable coronary disease (n=26). Drugs were given daily for 3 weeks (atorvastatin 80 mg, visits 1–3; clopidogrel 75 mg, visits 2–4). Counts of EPC (CD34+/CD133+/KDR+), EMP (CD51+) and PMP (CD42+/CD31+), and pharmacokinetic parameters over 24 h were assessed at each visit. Atorvastatin plasma concentrations were increased by concomitant therapy with clopidogrel (maximum serum concentration [Cmax], P=0.002; area under the clopidogrel or atorvastatin plasma concentration vs. time curve from 0 to the last detectable concentration [AUClast], P=0.03). After atorvastatin withdrawal there was an increase in clopidogrel plasma concentrations (Cmax, P=0.009; AUClast, P=0.039). PMP were inversely correlated with clopidogrel Cmax on visit 3 (rho=–0.57, P=0.006) and on visit 4 (rho=–0.54, P=0.01), and with clopidogrel AUClast on visit 3 (rho=–0.44, P=0.04), and on visit 4 (rho=–0.57, P=0.005). In addition, clopidogrel Cmax was correlated with EPC (CD133+/KDR+) on visit 4 (rho=0.48, P=0.025). No correlations of atorvastatin and MP or EPC were found. Conclusions: The balance between platelet MP release and EPC mobilization seems influenced by clopidogrel plasma levels, suggesting a protective mechanism on coronary artery disease. (Circ J 2012; 76: 729 – 736) Key Words: Clopidogrel; Endothelial progenitor cells; Platelets; Pharmacokinetics; Statin ORIGINAL ARTICLE Ischemic Heart Disease

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Circulation Journal Vol.76, March 2012
Circulation JournalOfficial Journal of the Japanese Circulation Societyhttp://www.j-circ.or.jp
n increased number of circulating endothelial progeni-tor cells (EPC) has been associated with better out-comes in patients with coronary artery disease.1–7
Microparticles are small plasma membrane structures derived from many cells, including apoptotic or activated endothelial cells and platelets. Recent evidence has suggested a key role of the endothelial microparticles (EMP) and platelet micropar-ticles (PMP) in vascular homeostasis.8–10 In addition, a recent study has shown that their levels were predictors of cardiovas-cular events in patients with stable coronary disease.11
Although the use of high doses of statins in acute coronary disease has been associated with increased EPC and micropar-ticles, some of these results seem to have been influenced by
the infarct size or the extension of vascular injury following coronary angioplasty.12–14 Furthermore, atorvastatin and clopi-dogrel are drugs commonly prescribed for acute coronary syn-drome and both are partially metabolized via cytochrome P450 3A4, raising concerns about pharmacokinetic interactions.15
Clopidogrel therapy was reported to change the number of EMP,16 but the literature is scarce on its effects on PMP or EPC, particularly when combined with high-dose statins.
In the present study we therefore examined possible interac-tions between atorvastatin and clopidogrel and their effects alone or combined on platelet function, circulating micropar-ticles and EPC among patients with stable coronary disease.
A
Received October 11, 2011; revised manuscript received November 17, 2011; accepted November 21, 2011; released online December 28, 2011 Time for primary review: 13 days
Department of Medicine, Federal University of São Paulo, São Paulo (C.N.F., L.F.M.P., M.C.O.I., M.K.C.B., R.S., H.T.B., S.H.K., S.P.B., F.A.H.F.); National Institute of Complex Fluids, São Paulo (M.C.O.I., F.A.H.F.); and Department of Pharmacology, State University of Campinas, Campinas, São Paulo (G.d.N.), Brazil
Mailing address: Francisco Antonio Helfenstein Fonseca, MD, PhD, Department of Medicine, Federal University of São Paulo, Rua Pedro de Toledo, 276, São Paulo, SP 04039030, Brazil. E-mail: [email protected]
ISSN-1346-9843 doi: 10.1253/circj.CJ-11-1145All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Endothelial Progenitor Cell Mobilization and Platelet Microparticle Release Are Influenced by Clopidogrel
Plasma Levels in Stable Coronary Artery DiseaseCarolina N. França, PhD; Luiz F.M. Pinheiro, MD, PhD; Maria C.O. Izar, MD, PhD;
Milena K.C. Brunialti, PhD; Reinaldo Salomão, MD, PhD; Henrique T. Bianco, MD; Soraia H. Kasmas, BSc; Simone P. Barbosa, BSc;
Gilberto de Nucci, MD, PhD; Francisco A.H. Fonseca, MD, PhD
Background: Increased numbers of endothelial (EMP) and platelet (PMP) microparticles have been related to car-diovascular risk factors and coronary artery disease. Little is known about the early effects of statins and clopidogrel on these new biomarkers of vascular homeostasis. The aim of the present study was to evaluate pharmacokinetic interactions between atorvastatin and clopidogrel and their effects, alone or combined, on EMP, PMP, and endothelial progenitor cells (EPC).
Methods and Results: A prospective open-label study enrolled subjects with stable coronary disease (n=26). Drugs were given daily for 3 weeks (atorvastatin 80 mg, visits 1–3; clopidogrel 75 mg, visits 2–4). Counts of EPC (CD34+/CD133+/KDR+), EMP (CD51+) and PMP (CD42+/CD31+), and pharmacokinetic parameters over 24 h were assessed at each visit. Atorvastatin plasma concentrations were increased by concomitant therapy with clopidogrel (maximum serum concentration [Cmax], P=0.002; area under the clopidogrel or atorvastatin plasma concentration vs. time curve from 0 to the last detectable concentration [AUClast], P=0.03). After atorvastatin withdrawal there was an increase in clopidogrel plasma concentrations (Cmax, P=0.009; AUClast, P=0.039). PMP were inversely correlated with clopidogrel Cmax on visit 3 (rho=–0.57, P=0.006) and on visit 4 (rho=–0.54, P=0.01), and with clopidogrel AUClast on visit 3 (rho=–0.44, P=0.04), and on visit 4 (rho=–0.57, P=0.005). In addition, clopidogrel Cmax was correlated with EPC (CD133+/KDR+) on visit 4 (rho=0.48, P=0.025). No correlations of atorvastatin and MP or EPC were found.
Conclusions: The balance between platelet MP release and EPC mobilization seems influenced by clopidogrel plasma levels, suggesting a protective mechanism on coronary artery disease. (Circ J 2012; 76: 729 – 736)
Key Words: Clopidogrel; Endothelial progenitor cells; Platelets; Pharmacokinetics; Statin
ORIGINAL ARTICLEIschemic Heart Disease

Circulation Journal Vol.76, March 2012
730 FRANÇA CN et al.
MethodsPatientsThis is a prospective study with participants consecutively selected from the outpatient clinic of the cardiology division of Federal University of São Paulo. The trial protocol was con-ducted in accordance with the ethics standards of the institution on human experimentation, and approval was obtained from the local ethics committee. Patients were included after having signed written informed consent.
We included patients of both genders (n=26), aged 49–77 years, with diagnosed stable coronary artery disease,17 under stable statin therapy for at least 3 months. Patients with planned revascularization were excluded. Subjects with liver (alanine aminotransferase [ALT] >2.5-fold upper limit of normal) or renal disease (creatinine >2.0 mg/dl), those with uncontrolled comorbidities, such as diabetes (glycated hemoglobin [HbA1c] >7.5%), thyroid dysfunction (thyroid-stimulating hormone >8 μU/ml), body mass index >35 kg/m2, triglycerides >400 mg/dl, genetic dyslipidemias, heart failure class III/IV (according to the New York Heart Association),18 HIV, and those with any known intolerance to the study drugs, were also excluded from the protocol.
Study DesignPatients were selected to attend a clinical visit, at which time demographic data and laboratory samples were obtained for biochemistry. Eligible patients had prior statin use discontin-ued for 1 week, and they were then scheduled to 4 visits, to receive therapy with atorvastatin, clopidogrel alone and com-bined (Figure 1).
The study drugs were atorvastatin (Lipitor®; Pfizer Pharma-ceutical, São Paulo, Brazil), and clopidogrel (Plavix®; Sanofi
Winthrop Industrie, Ambarés & la-Grave, Bordeaux, France). In all visits, patients received study medication at the same time in the morning after a 12-h fasting period. Returned tab-lets were counted at each visit.
Blood Sample Collection and AssaysBiochemistry was analyzed in samples obtained after a 12-h fasting period in a central laboratory at Federal University of São Paulo using automated techniques.
Lipids and BiochemistrySerum cholesterol, high-density lipoprotein cholesterol, and triglycerides were measured using automated methods (Advia 2400; Siemens Healthcare Diagnostics, Tokyo, Japan). Low-density lipoprotein cholesterol (LDL-C) was calculated using the Friedewald equation.19 ALT, creatinine and creatine kinase, were assayed using automated techniques (Advia 2400; Siemens Healthcare Diagnostics).
Determination of EPC, EMP and PMPMeasurements of EPC were performed as previously reported.20 Briefly, blood mononuclear cells were separated on Ficoll density gradient centrifugation. The cells were incubated for 30 min with the following mouse antibodies: CD34 FITC (BD Biosciences, Franklin Lakes, NJ, USA); CD133 APC (Miltenyi Biotec, Auburn, CA, USA) and KDR PE (R&D Systems, Minneapolis, MN, USA). As controls, we used mouse anti-body isotypes: a minimum of 500,000 events was acquired for flow cytometry (FACSCalibur; BD Biosciences, San Jose, CA, USA). EPC counts are expressed as percentage (%) of total progenitor cells in the lymphocyte gate. For EMP and PMP quantification, blood sample was collected in citrated tubes and centrifuged to obtain the platelet-rich plasma (PRP).
Figure 1. Study design. Visit 1: after a 7-day washout of the previous statin therapy, atorvastatin 80 mg daily was started. Visit 2: 1 week after visit 1, clopidogrel 75 mg daily was added to atorvastatin 80 mg. Visit 3: 2 weeks after visit 2, atorvastatin was discon-tinued. Visit 4: 1 week after visit 3, patients receive clopidogrel 75 mg alone. At all these visits, biochemistry and flow cytometry for quantification of endothelial progenitor cells, endothelial microparticles, and platelet microparticles were performed. Platelet func-tion was assessed at visits 3 and 4.

Circulation Journal Vol.76, March 2012
731Clopidogrel, Microparticles and Progenitor Cells
The PRP was then centrifuged to obtain the platelet-poor plasma (PPP). The PPP was then incubated for 20 min with the mouse antibodies CD42 FITC and CD31 PE (BD Biosciences), for PMP identification and with CD51-FITC (BD Biosciences), to detect EMP. Isotypes were used as controls. We used dis-posable containers (TruCOUNT Tubes; BD Biosciences) to determine microparticle number per microliter of PPP.
PharmacokineticsDrug Analysis Blood samples from a suitable antecubital
vein were collected at 0, 0.5, 1, 1.5, 2, 2.5, 3, 4, 6, 8, 10; 12; 16; and 24 h after dosing of the compound of reference. Plasma levels of atorvastatin21 were measured on validated liquid chromatography with mass spectrometry (LC-MS/MS) using an API 4000 system (Applied Biosystems, Canada). For clop-idogrel, we used a fast, sensitive and specific LC-MS/MS bioanalytical method validated for determination of unchanged clopidogrel in human plasma.22
Platelet Function TestsPlatelet adhesion and aggregation were tested in anti-coagu-lated whole blood collected using citrate buffer tubes. We used the IMPACT-RTM test (Matis Medical, Beersel, Belgium), which is a device for testing platelet function under close to physiological arterial flow conditions (1,800/s for 2 min).23,24 Briefly, laminar flow over the polystyrene surface of the well is achieved following the cone and plate principle. Upon application of a blood sample (130 μl) into the polystyrene well, plasma proteins immediately adhere to the well surface and become attractive for platelets, resulting in platelet adhe-sion and aggregation on the well surface under flow condi-tions. Following washing of excess blood and staining of the adhered platelets, results are quantified by an image analyzer. Results are expressed as the percentage of the well surface covered by platelet aggregates (representing platelet adhe-sion), and the average size of the aggregates (in μm2; repre-senting platelet aggregation). To test for clopidogrel efficacy, platelet activation was stimulated by adenosine diphosphate (ADP). Clopidogrel irreversibly blocks the ADP receptor P2Y12 on platelet cell membranes. This receptor plays an important role in platelet aggregation, specifically in the cross-
linking of platelets by fibrin. The blockade of this receptor inhibits platelet aggregation by blocking activation of the glycoprotein IIb/IIIa pathway.
Statistical AnalysisCategorical variables are presented as number (%); numerical data are expressed as mean ± SD or median (interquartile range).
Table 1. Baseline Patient Characteristics (Visit 1), n=26
Data
Age (years) 63 (40–77)
Male 18 (69)
Waist circumference (cm) 93±10
Body mass index (kg/m2) 27.1±3 Hypertension 26 (100)
Diabetes mellitus 9 (35)
Smoking 0 (0) Previous myocardial infarction 10 (38) Previous unstable angina 3 (11)
Previous stable angina 23 (88) Systolic blood pressure (mmHg) 127±3 Diastolic blood pressure (mmHg) 80±2 Aspirin 26 (100)
Previous statin 26 (100)
ACE inhibitor 18 (69) Angiotensin receptor blocker 5 (19)
β-blocker 8 (31)
Calcium channel blocker 12 (46) Sulphonylureas 3 (11)
Metformin 9 (34)
Insulin 7 (27)
Glucose (mg/dl) 116±46 ALT (IU/L) 24±10
Creatinine (mg/dl) 1.04±0.20
CK (IU/L) 141±102
Data given as median (interquartile range), mean ± SD or n (%).ACE, angiotensin-converting enzyme; ALT, alanine aminotrans-ferase; CK, creatine kinase.
Table 2. Lipid Level, Microparticle and EPC Changes
Parameter Visit 1 [baseline]
Visit 2 [ATV]
Visit 3 [ATV/CLO]
Visit 4 [CLO] P value
Lipids
Total cholesterol 152±36 139±20 155±31 182±36 0.0001
LDL-C 83±25 79±20 95±31 104±31 0.001 HDL-C 45±10 37±5 41±10 45±10 0.008 Triglycerides 120±61 116±56 97±50 166±76 0.002 Endothelial progenitor cells
CD34+/KDR+ 0.41±0.96 0.13±0.05 0.06±0.05 0.08±0.05 0.22 CD34+/CD133+ 0.01±0.00 0.02±0.00 0.01±0.00 0.01±0.00 0.47 KDR+/CD133+ 0.03±0.05 0.05±0.00 0.07±0.05 0.03±0.05 0.29 Microparticles†
Endothelial 1,019±1,468 1,259±1,790 1,242±1,652 529±1,168 0.35 Platelet 35,596±6,476 29,102±5,629 38,875±7,914 36,487±7,363 0.95
Data given as mean ± SD.EPC, endothelial progenitor cell; ATV, atorvastatin (80 mg daily); CLO, clopidogrel (75 mg daily); LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.Statins were discontinued 1 week before baseline visit. Total cholesterol on visit 1, visit 2 and visit 3 <visit 4; LDL-C on visit 1 and visit 2 <visit 4; HDL-C on visit 2 <visit 1 and visit 4; triglyceride levels on visit 2 and visit 3 <visit 4.ANOVA-Tukey. †Friedman test.

Circulation Journal Vol.76, March 2012
732 FRANÇA CN et al.
Continuous variables were tested for distribution of normality using the Kolmogorov-Smirnov test. Variables were compared between time points using ANOVA-repeated measures or Friedman test. Correlations were examined using the Spearman test. The first-order terminal elimination rate constant (ke) was estimated by linear regression from the points describing the elimination phase in a log-linear plot. Half-life (t1/2) was derived from this rate constant (t1/2 = ln(2)/ke). The maximum serum concentration of clopidogrel (Cmax) and the time taken to achieve this concentration (Tmax) were obtained directly from the curves. The areas under the clopidogrel and atorvastatin plasma concen-tration vs. time curves from 0 to the last detectable concentra-tion (AUClast) were calculated by applying the linear trapezoid rule. Extrapolation of these areas to infinity (AUC0-inf) was done by adding the Clast/ke to the calculated AUClast (where Clast = the last detectable concentration). Tests were 2-tailed and statistical significance was set at P<0.05. All analyses were done SPSS 18.0 for Windows (SPSS, Chicago, IL, USA).
ResultsPatientsAll patients completed the study protocol with full adherence to atorvastatin and clopidogrel. Participants were predomi-nantly middle-aged overweight men, and all subjects had stable coronary disease. All patients had diagnosis of hypertension, and one-third of participants had diabetes mellitus. Major baseline subject characteristics (visit 1) are given in Table 1.
Lipids, EPC and microparticlesTreatment with atorvastatin was effective to maintain LDL-C levels <100 mg/dl. It was noted, however, that 1-week discon-tinuation of this lipid-lowering agent was followed by increase in all measured lipid parameters (Table 2).
The numbers of EMP and PMP per μl of PPP, as well as the percentages of the 3 subpopulations of EPC were unchanged throughout the study (Table 2). An inverse correlation, how-
Figure 2. Correlations between the maximum concentration (Cmax) and area under the curve (AUClast) of clopidogrel and platelet microparticles (PMP) on visit 3 (atorvastatin+clopidogrel) and visit 4 (clopidogrel alone). (A,B) Correlations between Cmax of clopidogrel and PMP at visits 3 and 4, respectively; (C,D) correlations between AUClast of clopidogrel and PMP at visits 3 and 4, respectively.
Circulation Journal Vol.76, March 2012
733Clopidogrel, Microparticles and Progenitor Cells
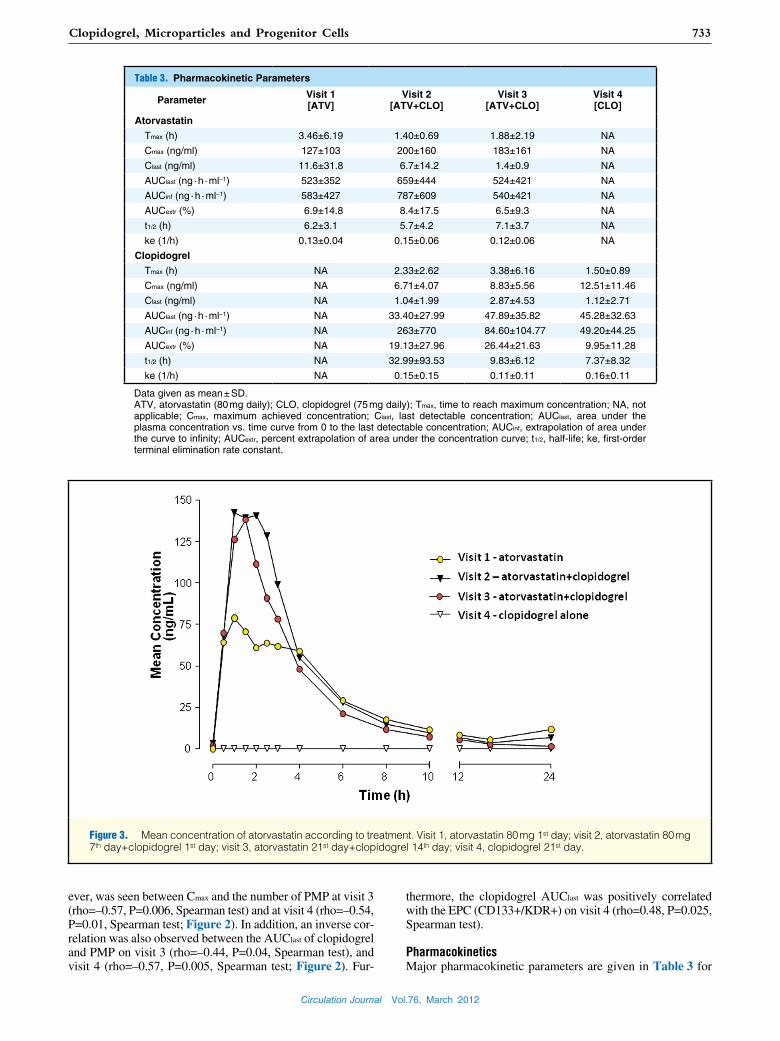
ever, was seen between Cmax and the number of PMP at visit 3 (rho=–0.57, P=0.006, Spearman test) and at visit 4 (rho=–0.54, P=0.01, Spearman test; Figure 2). In addition, an inverse cor-relation was also observed between the AUClast of clopidogrel and PMP on visit 3 (rho=–0.44, P=0.04, Spearman test), and visit 4 (rho=–0.57, P=0.005, Spearman test; Figure 2). Fur-
thermore, the clopidogrel AUClast was positively correlated with the EPC (CD133+/KDR+) on visit 4 (rho=0.48, P=0.025, Spearman test).
PharmacokineticsMajor pharmacokinetic parameters are given in Table 3 for
Figure 3. Mean concentration of atorvastatin according to treatment. Visit 1, atorvastatin 80 mg 1st day; visit 2, atorvastatin 80 mg 7th day+clopidogrel 1st day; visit 3, atorvastatin 21st day+clopidogrel 14th day; visit 4, clopidogrel 21st day.
Table 3. Pharmacokinetic Parameters
Parameter Visit 1 [ATV]
Visit 2 [ATV+CLO]
Visit 3 [ATV+CLO]
Visit 4 [CLO]
Atorvastatin
Tmax (h) 3.46±6.19 1.40±0.69 1.88±2.19 NA
Cmax (ng/ml) 127±103 200±160 183±161 NA
Clast (ng/ml) 11.6±31.8 6.7±14.2 1.4±0.9 NA
AUClast (ng · h · ml–1) 523±352 659±444 524±421 NA
AUCinf (ng · h · ml–1) 583±427 787±609 540±421 NA
AUCextr (%) 6.9±14.8 8.4±17.5 6.5±9.3 NA
t1/2 (h) 6.2±3.1 5.7±4.2 7.1±3.7 NA
ke (1/h) 0.13±0.04 0.15±0.06 0.12±0.06 NA
Clopidogrel
Tmax (h) NA 2.33±2.62 3.38±6.16 1.50±0.89
Cmax (ng/ml) NA 6.71±4.07 8.83±5.56 12.51±11.46
Clast (ng/ml) NA 1.04±1.99 2.87±4.53 1.12±2.71
AUClast (ng · h · ml–1) NA 33.40±27.99 47.89±35.82 45.28±32.63
AUCinf (ng · h · ml–1) NA 263±770 84.60±104.77 49.20±44.25
AUCextr (%) NA 19.13±27.96 26.44±21.63 9.95±11.28
t1/2 (h) NA 32.99±93.53 9.83±6.12 7.37±8.32
ke (1/h) NA 0.15±0.15 0.11±0.11 0.16±0.11
Data given as mean ± SD.ATV, atorvastatin (80 mg daily); CLO, clopidogrel (75 mg daily); Tmax, time to reach maximum concentration; NA, not applicable; Cmax, maximum achieved concentration; Clast, last detectable concentration; AUClast, area under the plasma concentration vs. time curve from 0 to the last detectable concentration; AUCinf, extrapolation of area under the curve to infinity; AUCextr, percent extrapolation of area under the concentration curve; t1/2, half-life; ke, first-order terminal elimination rate constant.

Circulation Journal Vol.76, March 2012
734 FRANÇA CN et al.
atorvastatin and clopidogrel. We found lower Cmax and AUClast of atorvastatin on visit 1 than on visits 2 and 3, when clopido-grel was added (Figure 3; P=0.0022, ANOVA for repeated measures). Conversely, atorvastatin had little influence on clopidogrel serum levels (Figure 4; P=0.034, ANOVA for repeated measures, without differences between treatments according to the Tukey-Kramer test).
Platelet Function TestsTable 4 lists the results for platelet adhesion and aggregation under steady-state conditions, for atorvastatin plus clopidogrel and clopidogrel alone. We found that neither adhesion nor aggregation were significantly modified when atorvastatin was discontinued.
DiscussionRecently, Ryu and Kim reported that clopidogrel therapy was associated with decreased EMP in vitro.25 The present study found an inverse relationship between clopidogrel serum levels and the amount of PMP. We investigated the effects of clopi-dogrel in patients who were not receiving aspirin or any anti-thrombotic agent, alone or combined with a potent statin.
Regarding microparticles, EMP are the most studied and their increase has been associated with uncontrolled cardiovas-
cular risk factors, triggering mechanisms of endothelial apop-tosis.26,27 In some circumstances, their release appears to have a protective role on endothelium integrity.28 In contrast, the significance of PMP count is less understood, but pronounced increase seems related to thrombosis.29,30 These microparticles can also stimulate the development of collateral vessels, acting as messengers of ischemic conditions.31 Taking these data together, the lower presence of EMP and PMP in patients with coronary artery disease seems to indicate a greater vascular stability, suggesting low rates of apoptosis of endothelial cells, and decreased platelet consumption.
Contrary to our expectations, we were unable to demon-strate changes in the amount of microparticles with use of high-dose atorvastatin. The highest atorvastatin dose is the most used dose in randomized clinical trials. This is in agree-ment with a recent meta-analysis showing the highest benefit among patients who had the highest LDL-C reduction,32 which is usually correlated with the highest statin dose. We found pharmacokinetic interactions between atorvastatin and clopi-dogrel, with increases in the plasma concentration of atorvas-tatin. Because atorvastatin is not a prodrug, this interaction probably had little effect on its lipid-lowering effectiveness, as well as on the anti-platelet actions of clopidogrel, as sug-gested by previous studies.33–35 Controversial results in the literature, however, may reflect a lower dose of statins or lack of an appropriate study design, because drug introduction and withdrawal were not assessed.36,37
Clopidogrel, but not atorvastatin, plasma levels were cor-related with the CD133+/KDR+ subpopulation of EPC, which is considered an immature lineage of EPC, and a marker of disease severity.38 This effect of clopidogrel, not seen with atorvastatin, may have been related to chronic and effective use of statins in the present subjects. We selected patients with relatively low levels of cholesterol, which may have attenu-ated the effects of the homing of EPC, thus decreasing EPC
Figure 4. Mean concentration of clopidogrel according to treatment. Visit 2, atorvastatin 80 mg 7th day+clopidogrel 1st day; visit 3, atorvastatin 21st day+clopidogrel 14th day; visit 4, clopidogrel 21st day.
Table 4. Platelet Function vs. Treatment
Parameter ATV+CLO CLO P value
Adhesion (%) 2.34±2.73 1.06±1.00 0.058
Aggregation (mm2) 29.65±9.49 31.58±8.07 0.178
Data given as mean ± SD.ATV, atorvastatin (80 mg daily); CLO, clopidogrel (75 mg daily).Comparisons made using Friedman test.
Circulation Journal Vol.76, March 2012
735Clopidogrel, Microparticles and Progenitor Cells
mobilization.39 But, even with significant changes to lipid profile, either by use of high-dose or by abrupt withdrawal of atorvastatin, no changes in the amount of circulating EPC or microparticles were observed.
Study LimitationsThe present study had a relatively small sample size, but we were able to demonstrate changes in surrogate endpoints. We tested patients under the highest atorvastatin dose that is the most used dose in randomized clinical trials, but without a loading dose of clopidogrel, therefore the present results can-not be extrapolated to other drug regimens.
In summary, the present study has demonstrated a pharma-cokinetic interaction between atorvastatin and clopidogrel, an inverse correlation between clopidogrel plasma concentration and the release of PMP, and a positive correlation with mobi-lization of EPC, thus suggesting a new potential benefit for protection in coronary artery disease.
A definitive clinical statin-clopidogrel interaction has yet to be demonstrated in a large-scale randomized clinical trial.
AcknowledgmentsThis study was supported by a research grant from FAPESP (São Paulo State Research Foundation) and in part from a grant from the Complex Fluid Institute of the National Council of Research Foundation (CNPq-INCT-FCx). Dr França was supported by a research grant from FAPESP (São Paulo State Research Foundation).
References 1. Wojakowski W, Kucia M, Kaźmierski M, Ratajczak MZ, Tendera
M. Circulating progenitor cells in stable coronary heart disease and acute coronary syndromes: Relevant reparatory mechanism? Heart 2008; 94: 27 – 33.
2. Fadini GP, Maruyama S, Ozaki T, Taguchi A, Meigs J, Dimmeler S, et al. Circulating progenitor cell count for cardiovascular risk strati-fication: A pooled analysis. PLoS One 2010; 5: e11488.
3. Werner N, Kosiol S, Schiegl T, Ahlers P, Walenta K, Link A, et al. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med 2005; 353: 999 – 1007.
4. Fadini GP, Agostini C, Sartore S, Avogaro A. Endothelial progenitor cells in the natural history of atherosclerosis. Atherosclerosis 2007; 194: 46 – 54.
5. Schwartzenberg S, Afek A, Charach G, Rubinstein A, Ben-Shoshan Y, Kissil S, et al. Comparative analysis of the predictive power of different endothelial progenitor cell phenotypes on cardiovascular outcome. World J Cardiol 2010; 2: 299 – 304.
6. Lee LC, Chen CS, Choong PF, Low A, Tan HC, Poh KK. Time-dependent dynamic mobilization of circulating progenitor cells during percutaneous coronary intervention in diabetics. Int J Cardiol 2010; 142: 199 – 201.
7. Park JA, Kwon YG. Could circulating progenitor cell count be a barometer for coronary artery disease progression? Circ J 2010; 74: 1804 – 1805.
8. Tushuizen ME, Diamant M, Sturk A, Nieuwland R. Cell-derived microparticles in the pathogenesis of cardiovascular disease: Friend or foe? Arterioscler Thromb Vasc Biol 2011; 31: 4 – 9.
9. Morel O, Jesel L, Freyssinet JM, Toti F. Cellular mechanisms under-lying the formation of circulating microparticles. Arterioscler Thromb Vasc Biol 2011; 31: 15 – 26.
10. Dignat-George F, Boulanger CH. The many faces of endothelial microparticles. Arterioscler Thromb Vasc Biol 2011; 31: 27 – 33.
11. Sinning JM, Losch J, Walenta K, Böhm M, Nickenig G, Werner N. Circulating CD31+/Annexin V+ microparticles correlate with cardio-vascular outcomes. Eur Heart J 2010; 32: 2034 – 2041.
12. Leone AM, Rutella S, Giannico MB, Perfetti M, Zaccone V, Brugaletta S, et al. Effect of intensive vs standard statin therapy on endothelial progenitor cells and left ventricular function in patients with acute myocardial infarction: Statins for regeneration after acute myocardial infarction and PCI (STRAP) trial. Int J Cardiol 2008; 130: 457 – 462.
13. Schwartzenberg S, Deutsch V, Maysel-Auslender S, Kissil S, Keren G, George J. Circulating apoptotic progenitor cells: A novel biomarker in patients with acute coronary syndromes. Arterioscler Thromb Vasc
Biol 2007; 27: e27 – e31.14. Wojakowski W, Tendera M. Mobilization of bone marrow-derived
progenitor cells in acute coronary syndromes. Folia Histochem Cytobiol 2005; 43: 229 – 232.
15. Lau, WC, Waskell LA, Watkins PB, Neer CJ, Horowitz K, Hopp AS, et al. Atorvastatin reduces the ability of clopidogrel to inhibit platelet aggregation: A new drug-drug interaction. Circulation 2003; 107: 32 – 37.
16. Hamilos M, Muller O, Ntalianis A, Trana C, Bartunek J, Sarno G, et al. Relationship between peripheral arterial reactive hyperemia and residual platelet reactivity after 600 mg clopidogrel. J Thromb Throm-bolysis 2011; 32: 64 – 71.
17. Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas JS, et al. ACC/AHA 2002 guideline update for the management of patients with chronic stable angina--summary article: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Chronic Stable Angina). Circulation 2003; 107: 149 – 158.
18. Hunt SA. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001. Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol 2005; 46: e1 – e82.
19. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concen-tration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 1972; 18: 499 – 502.
20. da Silva EF, Fonseca FA, França CN, Ferreira PR, Izar MC, Salomão R, et al. Imbalance between endothelial progenitor cells and mic-roparticles in HIV-infected patients naïve for antiretroviral therapy. AIDS 2011; 25: 1595 – 1601.
21. Robinson A, Hillis J, Neal C, Leary AC. The validation of a bioana-lytical method for the determination of clopidogrel in human plasma. J Chromatogr B Analyt Technol Biomed Life Sci 2007; 848: 344 – 354.
22. He BX, Shi L, Qiu J, Zeng XH, Tao L, Li R, et al. Quantitative deter-mination of atorvastatin and ortho-hydroxy atorvastatin in human plasma by liquid chromatography tandem mass spectrometry and pharmacokinetic evaluation. Methods Find Exp Clin Pharmacol 2010; 32: 481 – 487.
23. Sibbing D, Braun S, Morath T, Mehilli J, Vogt W, Schömig A, et al. Platelet reactivity after clopidogrel treatment assessed with point-of-care analysis and early drug-stent thrombosis. J Am Coll Cardiol 2009; 53: 849 – 856.
24. Morrison A, Hornsey VS, Prowse CV, Macgregor IR. Use of the DiaMed Impact R to test platelet function in stored platelet concen-trates. Vox Sang 2007; 93: 166 – 172.
25. Ryu JH, Kim SJ. Clopidogrel effectively suppresses endothelial mic-roparticle generation induced by indoxyl sulfate via inhibition of the p38 mitogen-activated protein kinase pathway. Blood Purif 2011; 32: 186 – 194.
26. Chironi GN, Boulanger CM, Simon A, Dignat-George F, Freyssinet JM, Tedgui A. Endothelial microparticles in diseases. Cell Tissue Res 2009; 335: 143 – 151.
27. Nozaki T, Sugiyama S, Koga H, Sugamura K, Ohba K, Matsuzawa Y, et al. Significance of a multiple biomarkers strategy including endo-thelial dysfunction to improve risk stratification for cardiovascular events in patients at high risk for coronary heart disease. J Am Coll Cardiol 2009; 54: 601 – 608.
28. Rautou PE, Vion AC, Amabile N, Chironi G, Simon A, Tedgui A, et al. Microparticles, vascular function, and atherothrombosis. Circ Res 2011; 109: 593 – 606.
29. Siljander P, Carpen O, Lassila R. Platelet-derived microparticles associate with fibrin during thrombosis. Blood 1996; 87: 4651 – 4663.
30. Ramacciotti E, Hawley AE, Farris DM, Ballard NE, Wrobleski SK, Myers DD Jr, et al. Leukocyte- and platelet-derived microparticles correlate with thrombus weight and tissue factor activity in an exper-imental mouse model of venous thrombosis. Thromb Haemost 2009; 101: 748 – 754.
31. Martinez MC, Andriantsitohaina R. Microparticles in angiogenesis: Therapeutic potential. Circ Res 2011; 109: 110 – 119.
32. Cholesterol Treatment Trialists’ (CTT) Collaboration; Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, et al. Effi-cacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010; 376: 1670 – 1681.
33. Lotfi A, Schweiger MJ, Giugliano GR, Murphy SA, Cannon CP; TIMI 22 Investigators. High-dose atorvastatin does not negatively influence clinical outcomes among clopidogrel treated acute coronary

Circulation Journal Vol.76, March 2012
736 FRANÇA CN et al.
syndrome patients--a Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 (PROVE IT-TIMI 22). Am Heart J 2008; 155: 954 – 958.
34. Serebruany VL, Midei MG, Malinin AI, Oshrine BR, Lowry DR, Sane DC, et al. Absence of interaction between atorvastatin or other statins and clopidogrel: Results from the interaction study. Arch Intern Med 2004; 164: 2051 – 2057.
35. Wenaweser P, Windecker S, Billinger M, Cook S, Togni M, Meier B, et al. Effect of atorvastatin and pravastatin on platelet inhibition by aspirin and clopidogrel treatment in patients with coronary stent thrombosis. Am J Cardiol 2007; 99: 353 – 356.
36. Farid NA, Small DS, Payne CD, Jakubowski JA, Brandt JT, Li YG, et al. Effect of atorvastatin on the pharmacokinetics and pharmaco-
dynamics of prasugrel and clopidogrel in healthy subjects. Pharma-cotherapy 2008; 28: 1483 – 1494.
37. Malmström RE, Östergren J, Jorgensen L, Hjemdahl P; CASTOR investigators. Influence of statin treatment on platelet inhibition by clopidogrel: A randomized comparison of rosuvastatin, atorvastatin and simvastatin co-treatment. J Intern Med 2009; 266: 457 – 466.
38. Turan RG, Turan CH, Bozdag-Turan I, Ortak J, Akin I, Kische S, et al. Impaired mobilization of CD133+ bone marrow-derived circulat-ing progenitor cells with an increased number of diseased coronary arteries in ischemic heart disease patients with diabetes. Circ J 2011; 75: 2635 – 2641.
39. Zhou Q, Liao JK. Pleiotropic effects of statins: Basic research and clinical perspectives. Circ J 2010; 74: 818 – 826.
Related Documents











