Current Pharmaceutical Design, 2008, 14, 3768-3778 3768 1381-6128/08 $55.00+.00 © 2008 Bentham Science Publishers Ltd. Endothelial Effects of Drugs Designed to Treat Erectile Dysfunction Antonio Aversa 1, * , Massimiliano Caprio 1 , Giuseppe M.C. Rosano 2 and Giovanni Spera 2 1 Cattedra di Medicina Interna, Dipartimento Fisiopatologia Medica, Sapienza Università di Roma and 2 Cardiovascular Research Unit, Department of Medical Sciences, IRCCS San Raffaele - Rome, Italy Abstract: Erectile dysfunction (ED) and endothelial dysfunction are common in individuals with multiple cardiovascular risk factors (CRFs) and are longitudinal predictors of cardiovascular events. ED is associated with systemic endothelial cell activation/dysfunction independent from CRFs or from diffuse, unrecognized vascular damage. The pathogenesis of endothelial dysfunction and ED is intimately linked through decreased expression and activation of endothelial nitric ox- ide (NO) synthase and the subsequent physiologic actions of NO. Furthermore, reduced biologic activity of endothelium- derived NO links atherosclerosis to ED and underscores the role of altered endothelium in the pathogenesis of both condi- tions. Evidence-based data suggest that daily use of phosphodiesterase type-5 inhibitors (PDE5-i) improves endothelial and erectile functions and that this benefit is lost upon drug withdrawal. Daily PDE5-i may also improve lower tract uri- nary symptoms related to benign prostatic hyperplasia through a reduction of adrenergic overtone. The relevance for these drugs in the prevention of complications in internal medicine diseases, i.e. cardiovascular disease, clotting disorders and autoimmune disease is uncertain. Finally, endothelial dysfunction is present in testosterone deficiency syndromes and re- placement therapy is able to revert ED and to improve endothelial function. Aim of the present review is to discuss the systemic effects of drugs designed to treat ED, such as testosterone and PDE5- i, with regard to safety, unwanted effects and efficacy in improving endothelial function; finally, a goal-oriented approach to rehabilitation using daily vs. on-demand PDE5-i in difficult patients is discussed. Key Words: Endothelial dysfunction, nitric oxide, testosterone, phosphodiesterase type-5 inhibitors, benign prostatic hyperpla- sia, LUTS, rehabilitation, internal medicine. INTRODUCTION It has been demonstrated that male erectile dysfunction (ED) and coronary heart disease (CHD) share common risk factors and etiological mechanisms [1]. Vasculogenic ED results from impairment of endothelial-dependent or -inde- pendent smooth muscle relaxation (functional vascular ED, initial stages), occlusion of the cavernosal arteries by athero- sclerosis (structural vascular ED, late stages), or a combina- tion of these. Endothelial dysfunction is the key event in the pathophysiology of ED and, importantly, men with penile vascular damage have endothelial dysfunction in other vas- cular beds, as well [2]. Endothelial dysfunction is a primary step in the development of cardiovascular diseases, including hypertension, atherosclerosis, and CHD. These diseases share also the frequent occurrence of different degrees of impaired glucose metabolism and insulin resistance or overt type-2 diabetes mellitus (T2DM). All these forms of altered glucose and insulin metabolism are also associated with endothelial dysfunction. Thus, a modern approach to ED should be geared not only toward ameliorating the symptom of erectile inadequacy, but also toward modifying the burden of any concomitant medical conditions in which endothelial dys- function plays a pivotal role in worsening the course of dis- ease and thus contributing to the severity of ED [3]. *Address correspondence to this author at the Internal Medicine Unit, Medical Pathophysiology Department, “Sapienza” University of Rome, Viale del Policlinico 155, 00161, Rome, Italy; Tel: +39 06 49970721; Fax: +39 06 4461450; E-mail: [email protected] In this article, we discuss the role of therapies targeted to improve ED and their possible effects on endothelial func- tion/dysfunction. THE ENDOTHELIUM LINKS INTERNAL TO SEX- UAL MEDICINE The vascular endothelium is an active, dynamic tissue that controls many important functions on the vasculature, including regulation of vascular tone, local hemostasis, pro- liferative process, and maintenance of blood circulation, flu- idity, coagulation, and inflammatory responses. Each endo- thelial cell (EC) is analogous to a miniature adaptive input- output device, sensing changes in the extracellular compart- ment, and responding in ways that are beneficial, or at times harmful, to the host. This model provides a useful conceptual framework for understanding the role of the endothelium in health and disease. Input to the EC arises from the extracel- lular environment and may include soluble mediators, cell to cell interactions, degree of oxygenation, hemodynamic forces, temperature, and pH. Endothelial cell response (out- put) is manifested as its cellular phenotype and may include alterations in vasomotor tone, vascular permeability, haemo- static balance, inflammatory response, as well as cellular proliferation and survival. The intrinsic properties of the EC, the so-called "set point", serve to channel and filter this in- formation flow, linking input with output in ways that differ from one EC to another. Indeed, all three elements (input, output, and set point) vary according to time and location within the vascular tree. When viewed from the perspective

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Current Pharmaceutical Design, 2008, 14, 3768-3778 3768
1381-6128/08 $55.00+.00 © 2008 Bentham Science Publishers Ltd.
Endothelial Effects of Drugs Designed to Treat Erectile Dysfunction
Antonio Aversa1,*, Massimiliano Caprio
1, Giuseppe M.C. Rosano
2 and Giovanni Spera
2
1Cattedra di Medicina Interna, Dipartimento Fisiopatologia Medica, Sapienza Università di Roma and
2Cardiovascular
Research Unit, Department of Medical Sciences, IRCCS San Raffaele - Rome, Italy
Abstract: Erectile dysfunction (ED) and endothelial dysfunction are common in individuals with multiple cardiovascular
risk factors (CRFs) and are longitudinal predictors of cardiovascular events. ED is associated with systemic endothelial
cell activation/dysfunction independent from CRFs or from diffuse, unrecognized vascular damage. The pathogenesis of
endothelial dysfunction and ED is intimately linked through decreased expression and activation of endothelial nitric ox-
ide (NO) synthase and the subsequent physiologic actions of NO. Furthermore, reduced biologic activity of endothelium-
derived NO links atherosclerosis to ED and underscores the role of altered endothelium in the pathogenesis of both condi-
tions. Evidence-based data suggest that daily use of phosphodiesterase type-5 inhibitors (PDE5-i) improves endothelial
and erectile functions and that this benefit is lost upon drug withdrawal. Daily PDE5-i may also improve lower tract uri-
nary symptoms related to benign prostatic hyperplasia through a reduction of adrenergic overtone. The relevance for these
drugs in the prevention of complications in internal medicine diseases, i.e. cardiovascular disease, clotting disorders and
autoimmune disease is uncertain. Finally, endothelial dysfunction is present in testosterone deficiency syndromes and re-
placement therapy is able to revert ED and to improve endothelial function.
Aim of the present review is to discuss the systemic effects of drugs designed to treat ED, such as testosterone and PDE5-
i, with regard to safety, unwanted effects and efficacy in improving endothelial function; finally, a goal-oriented approach
to rehabilitation using daily vs. on-demand PDE5-i in difficult patients is discussed.
Key Words: Endothelial dysfunction, nitric oxide, testosterone, phosphodiesterase type-5 inhibitors, benign prostatic hyperpla-sia, LUTS, rehabilitation, internal medicine.
INTRODUCTION
It has been demonstrated that male erectile dysfunction (ED) and coronary heart disease (CHD) share common risk factors and etiological mechanisms [1]. Vasculogenic ED results from impairment of endothelial-dependent or -inde- pendent smooth muscle relaxation (functional vascular ED, initial stages), occlusion of the cavernosal arteries by athero-sclerosis (structural vascular ED, late stages), or a combina-tion of these. Endothelial dysfunction is the key event in the pathophysiology of ED and, importantly, men with penile vascular damage have endothelial dysfunction in other vas-cular beds, as well [2]. Endothelial dysfunction is a primary step in the development of cardiovascular diseases, including hypertension, atherosclerosis, and CHD. These diseases share also the frequent occurrence of different degrees of impaired glucose metabolism and insulin resistance or overt type-2 diabetes mellitus (T2DM). All these forms of altered glucose and insulin metabolism are also associated with endothelial dysfunction. Thus, a modern approach to ED should be geared not only toward ameliorating the symptom of erectile inadequacy, but also toward modifying the burden of any concomitant medical conditions in which endothelial dys-function plays a pivotal role in worsening the course of dis-ease and thus contributing to the severity of ED [3].
*Address correspondence to this author at the Internal Medicine Unit,
Medical Pathophysiology Department, “Sapienza” University of Rome,
Viale del Policlinico 155, 00161, Rome, Italy; Tel: +39 06 49970721; Fax:
+39 06 4461450; E-mail: [email protected]
In this article, we discuss the role of therapies targeted to improve ED and their possible effects on endothelial func-tion/dysfunction.
THE ENDOTHELIUM LINKS INTERNAL TO SEX-UAL MEDICINE
The vascular endothelium is an active, dynamic tissue that controls many important functions on the vasculature, including regulation of vascular tone, local hemostasis, pro-liferative process, and maintenance of blood circulation, flu-idity, coagulation, and inflammatory responses. Each endo-thelial cell (EC) is analogous to a miniature adaptive input-output device, sensing changes in the extracellular compart-ment, and responding in ways that are beneficial, or at times harmful, to the host. This model provides a useful conceptual framework for understanding the role of the endothelium in health and disease. Input to the EC arises from the extracel-lular environment and may include soluble mediators, cell to cell interactions, degree of oxygenation, hemodynamic forces, temperature, and pH. Endothelial cell response (out-put) is manifested as its cellular phenotype and may include alterations in vasomotor tone, vascular permeability, haemo-static balance, inflammatory response, as well as cellular proliferation and survival. The intrinsic properties of the EC, the so-called "set point", serve to channel and filter this in-formation flow, linking input with output in ways that differ from one EC to another. Indeed, all three elements (input, output, and set point) vary according to time and location within the vascular tree. When viewed from the perspective

ED Drugs and Endothelial Function Current Pharmaceutical Design, 2008, Vol. 14, No. 35 3769
of trillions of miniature adaptive input-output devices ar-ranged in parallel, the endothelium takes on the appearance of a complex circuit board, one that is at least partially hard-wired to meet the demands of the underlying tissue and yet highly vulnerable to "short-circuiting" as a mechanism un-derlying focal vascular disease.
The continuous damage to endothelial cells caused by exposure to risk factors is balanced, up until a certain point, by the endogenous reparative processes. Normal vascular endothelium is essential for the synthesis and release of sub-stances affecting vascular tone (Nitric Oxide; NO), cell ad-hesion (endothelins, interleukins) and the homeostasis of clotting and fibrinolysis (plasminogen inhibitors, von Wille-brand factor) thus suggesting an anti-inflammatory role in physiologic conditions [4]. Quiescent endothelial cells ex-press an anticoagulant, anti-adhesive, and vasodilatory phe-notype, whereas activated endothelial cells express proco-agulant, pro-adhesive, and vasoconstricting properties. The degeneration of endothelial integrity causes endothelial dys-function with impaired release of NO and loss of its anti-atherogenic protection. An imbalance between NO and su-peroxide anions towards reduced NO bioavailability en-hances migration of monocytes into the vessel wall and pro-liferation of smooth muscle cells. These augmented oxida-tive processes, resembling a chronic inflammatory process extending to the vessel wall, contribute to plaque architec-ture, e.g., by destabilization of fibrous caps. In particular, oxidized low-density lipoprotein cholesterol initiates a series of events that begin with cell activation, endothelial dysfunc-tion, local inflammation, and a pro-coagulant vascular sur-face. This event, nominated “endothelial activation”, results into plaque formation [5]. EC activation is not an all-or-nothing response, nor is it necessarily linked to disease. In-stead, it represents a spectrum of responses occurring under both physiological and pathophysiological conditions so that it may represent one initiating event in atherosclerosis [6]. On the other hand, EC dysfunction is not restricted anatomi-cally to the heart, nor is it limited in disease scope to athero-sclerosis. Accordingly, ECs residing in arteries, capillaries, and veins of every tissue and organ are prone to non-adaptive, dysfunctional changes [7]. Currently, the term EC dysfunction may be broadly applied to states in which the EC phenotype, whether or not it meets the definition of acti-vation, poses a net liability to the host. Examples include severe sepsis, pulmonary hypertension, pathological angio-genesis, thrombotic thrombocytopenic purpura, hepatic veno-occlusive disease, and sickle cell disease. In men with co-existing ED and CHD, ED symptoms were reported as having become clinically evident prior to cardiac symptoms by 67%. The mean time interval between the onset of ED and CHD was 3 ys [8]. Remarkably, in the age group 50 to 59 years, patients with proven cavernous arterial insuffi-ciency at penile Duplex ultrasound showed a significantly increased risk to develop CHD within 4 years [9]. In another series of patients, it was found that a considerable proportion (19%) of men with ED of vascular origin had angiographi-cally documented silent CHD [10]. Biochemical measures of EC activation were evaluated in patients with ED associated or not associated with cardiovascular risk factors (CRFs) to assess whether ED may be considered a sentinel of athero-sclerosis. Increased circulating soluble P-selectin, intercellu-
lar adhesion molecule-1 (ICAM1), vascular cell adhesion molecule-1 (VCAM1) and endothelin-1 (ET-1) concentra-tions were associated with ED independently of coexisting CRFs and overt vascular damage, suggesting that ED may be considered a sentinel of early atherosclerosis [11].
Insulin resistance (IR), another important risk factor for cardiovascular disease, is thought to promote atherosclerosis through a reciprocal relationship with endothelial dysfunc-tion [12]. A mutual relationship between IR and vascular endothelial dysfunction has recently been identified as an important factor in the development of atherosclerosis. Metabolic actions of insulin to promote glucose disposal are augmented by vascular actions of insulin in endothelium to stimulate production of the vasodilator NO. Indeed, NO-dependent increases in blood flow to skeletal muscle account for 25% to 40% of the increase in glucose uptake in response to insulin stimulation. Phosphatidylinositol 3-kinase- (PI3K) dependent insulin-signaling pathways in endothelium related to production of NO, share striking similarities with meta-bolic pathways in skeletal muscle that promote glucose up-take. Indeed, several reports have suggested that in response to a variety of stimuli, efficient NO production requires NOS (NO-synthase) phosphorylation through the PI3-K/Akt path- way [13]. PI3-K subsequently phosphorylates Akt, which in turn phosphorylates NOS, and thereby increases NO produc-tion. Other distinct non-metabolic branches of insulin-signal- ing pathways regulate secretion of the vasoconstrictor pep-tide ET-1 in endothelium [14]. Several studies suggest that in diabetes the relative ineffectiveness of insulin and the hyper-glycemia act together to reduce activity in the insulin-receptor substrates (IRS)/PI3-K/Akt pathway, resulting in impairments of both IRS/PI3-K/Akt-mediated endothelial function and NO production [15]. Metabolic insulin resis-tance is characterized by pathway-specific impairment in PI3K-dependent signaling, which in endothelium may cause imbalance between production of NO and secretion of ET-1, leading to decreased blood flow, which worsens insulin re-sistance. Deficiency of endothelial-derived NO is believed to be the primary defect that links insulin resistance and endo-thelial dysfunction. NO deficiency results from decreased synthesis and/or release, in combination with exaggerated consumption in tissues by high levels of reactive oxygen (ROS) and nitrogen (RNS) species, which are produced by cellular disturbances in glucose and lipid metabolism [16]. Endothelial dysfunction contributes to impaired insulin ac-tion, by altering the trans-capillary passage of insulin to tar-get tissues. Reduced expansion of the capillary network, with attenuation of microcirculatory blood flow to metabolically active tissues, contributes to the impairment of insulin-stimulated glucose and lipid metabolism. This establishes a reverberating negative feedback cycle in which progressive endothelial dysfunction and disturbances in glucose and lipid metabolism develop secondary to the insulin resistance [17]. Hyperglycemia and overt T2DM may accelerate endothelial dysfunction by promoting release of free oxygen radicals [18]. Vascular damage, which results from lipid deposition and oxidative stress to the vessel wall, triggers an inflamma-tory reaction, and the release of chemo attractants and cyto-kines that worsen the insulin resistance and endothelial dys-function [19]. This circuit may reverberate in other districts and may be involved in the pathogenesis of benign prostate

3770 Current Pharmaceutical Design, 2008, Vol. 14, No. 35 Aversa et al.
hyperplasia (BPH), thus suggesting the hypothesis of an in-creased sympathetic nerve activity in men with BPH [20]. Evidence show that diabetic men are at higher risk for both ED and BPH [21], being vascular damage considered as the mainstay of both [22]; hyperplasia of the stromal and glan-dular prostate compartments might be induced by stromal growth secondary to hypoxia, which in turn results from re-duced blood flow patterns at Duplex ultrasound [23]. It ap-pears clear that endothelial dysfunction and consequent adrenergic overtone can be considered as the common de-nominator linking atherosclerosis, cardiovascular disease and ED-BPH [24]. The recognition of the importance of the bal-ance between endothelial injury (incurred by exposure to risk factors) and endogenous reparative processes (which mediate endothelial repair) has led to a paradigm shift in vascular biology.
The recent discovery that circulating endothelial mi-croparticles (EMPs) are a hallmark of endothelial dysfunc-tion [25] and that circulating endothelial progenitor cells (EPCs) of bone marrow origin contribute to the regeneration of damaged endothelium has opened up exciting avenues of research [26]. EPCs play a key role in promoting endothelial repair processes after different injuries and their circulating levels are intimately correlated with the degree of vascular response to vasoconstrictor stimuli; in other words, the higher the EPCs, the better is the vasodilator arterial re-sponse to shear stress. A low number of circulating EPCs is supposed to be an independent risk factor for CHD. Recent studies demonstrated that reduced levels of circulating EPCs independently predicted the atherosclerotic process and the occurrence of cardiovascular events and death from cardio-vascular causes [27]. The finding that men with ED of any origin have reduced number of EPCs and that men with T2DM have increased levels of EMPs which are independ-ently involved in the pathogenesis of ED, opens a new sce-nario for the application of these potential novel markers in the early detection of ED [28]. However, there is still a mat-ter of debate as to whether any reliable surrogate marker of endothelial dysfunction in cardiovascular medicine may be applied [29]. A recent cross-sectional study investigating the degree of ED and its relationship to atherosclerotic biomark-ers has been carried out in 998 men and concluded that se-lected biomarkers for endothelial function (VCAM, ICAM), thrombosis (Factor VII) and dyslipidemia (total choles-terol/HDL and triglycerides) but not inflammation (Lipopro-tein-a, homocysteine, interleukin-6 and tumour-necrosis-factor receptor, C-reactive protein and fibrinogen) are asso-ciated with the degree of ED even after adjusting for age, socio-demographic and traditional CHD risk factors [30].
We can conclude that endothelial integrity has a para-mount role in preserving a man’s from cardiovascular and genital organ injuries. Penile erection is a hemodynamic event regulated by arterial and corporal smooth muscle re-laxation, which normally is the result of increase in para-sympathetic activity during sexual stimulation. Any imbal-ance between corporal smooth muscle contraction and re-laxation is a clinically relevant phenomenon leading to ED. It is our opinion that endothelial function assessment in the clinical setting is an important step leading to prevention strategies both in internal and sexual medicine, i.e. metabolic
syndrome [31], CHD, autoimmune disorders [32], hypogo-nadism, Peyronie’s disease [33].
Vascular reactivity tests represent the most widely used methods in the clinical assessment of endothelial function. Numerous methodologies have been proposed to study mi-crocirculation (resistance arteries and arterioles) and macro-circulation (conduit arteries), both in coronary and peripheral vascular districts [34]. Flow-mediated-dilatation of the bra-chial arteries under basal (shear-stress) and stimulated (NO-donor administration) conditions represents the most widely non-invasive technique to evaluate endothelium-dependent and –independent functions, respectively [35]. This tech-nique has been applied for investigational purposes to penile arteries also [36]. Even if a linear relationship between FMD and ED as detected by clinical questionnaire has been dem-onstrated [37], we believe that dynamic penile ultrasound is the unique tool for evaluating not only penile arterial tree but also the man’s capacity to attain ‘best quality erection’, which is important for regaining self-esteem and confidence [38]. The possibility to use alternative and non-invasive di-agnostic approaches to vascular ED is still under validation [39]. The presence of endothelial dysfunction does not nec-essarily means the presence of either ED or CHD, but when we approach a man with co-morbid conditions, i.e. obesity or metabolic syndrome, endothelial dysfunction severity may disclose the presence of unrevealed ED (data unpublished). In this view, we believe that performing endothelial function assessment by means of a new validated, reproducible and not operator-dependent diagnostic tools i.e. peripheral arte-rial tonometry (PAT) [40], represents a new modern ap-proach to the patient with vascular disease.
TESTOSTERONE, THE ENDOTHELIUM AND ERECTILE FUNCTION
Hypogonadism related-ED represents the link between internal medicine and sexual medicine, so far. Testosterone (T) circulating levels are determinant for correct endothelial function, and tend to a step-ward decrease with ageing and with the presence of numerous co-morbidities [41]. The in-creased incidence of cardiovascular disease in ageing men compared with premenopausal women suggests an unfavor-able effect of male sex hormone testosterone on the cardio-vascular system. However, numerous epidemiological and interventional studies reported a controversial relationship between T and cardiovascular disease. T inversely correlate with the severity of atherosclerosis and has beneficial effects upon vascular reactivity, inflammatory cytokine, adhesion molecules, insulin resistance, serum lipids, and haemostatic factors [42]. Furthermore, an increasing body of evidence indicates that it can exert acute vasorelaxing effects, via non-genomic mechanisms that are not mediated via modulation of cyclic nucleotide tissue levels [43]. These effects involve primarily the vascular smooth muscle, without requiring the presence of endothelium, although an endothelial contribu-tion is apparent in some studies [44]. To date, the mechanism behind the vasodilator action of testosterone is still under debate and might be exerted through either activation of K
(+)
channels or blockade of Ca(2+)
channels in vascular muscle cells. Interestingly, men with established CHD have reduced circulating testosterone levels [45] which are often associa-

ED Drugs and Endothelial Function Current Pharmaceutical Design, 2008, Vol. 14, No. 35 3771
ted with a certain degree of endothelial dysfunction inde-pendently of other risk factors, suggesting a protective effect of endogenous testosterone on the endothelium [46]. Moreo-ver, the recent finding that hypotestosteronemia is associated with a low number of circulating EPCs in young hypogo-nadotropic hypogonadal subjects [47] and that testosterone replacement is able to revert EPC counts through a direct stimulatory effect on the bone marrow [48] clearly suggests a new potential field of application to T replacement therapy. Pilot studies suggest that T may have a role as an anti-atherogenic therapy, by preserving endothelial and smooth muscle cell integrity; also, recent evidence demonstrated that androgen deprivation for prostate cancer may reduce insulin sensitivity, thus suggesting a key-role for testosterone in the development of insulin resistance/metabolic syndrome also [49].
Preclinical investigations reported by Traish et al. [50] provided convincing evidence that PDE5-i are ineffective in improving erectile function in androgen-deficient animals and that the re-administration of androgen facilitates PDE5-i action. As already outlined, T may directly control the ex-pression and activity of PDE5 in human corpus cavernosum [51]. Androgen deficiency or hypogonadism reduce the cav-ernosal expression of PDE5 mRNA, protein and enzyme activity, and T supplementation restores PDE5 expression and activity [52] which represents the substrate for the in-hibitory action of PDE5 inhibitors. The effects of androgens on penile tissues in experimental models demonstrated that androgen deprivation induces: 1) smooth muscle cell degen-eration (apoptosis), adipose tissue deposition with associated fibrosis of corpus cavernosum [53]; 2) reduction in the ex-pression of eNOS and nNOS and 3) decrease of arterial in-flow and increase of venous out-flow in the corpus caverno-sum; 4) enhanced response to mediators of vasoconstriction and smooth muscle contraction such as -adrenergic agents; 5) decrease of NO-mediated smooth muscle relaxation dur-ing sexual stimuli and 6) down-regulation of expression of PDE5 enzyme [54]. This latter aspect seems to be crucial in determining metabolic and structural imbalance in the corpus cavernosum, resulting in venous leakage and ED; this sug-gests a rationale for combination therapy with PDE5-i com-bined with T preparation for treating ED refractory to mono-therapy [55].
Aversa and co-workers were the very first one to investi-gate the effect of T on peripheral erectile mechanisms in a clinical setting. They reported that plasma T concentration was related to erection entity as evaluated by Duplex ultra-sound scanning of the penis; in that study, 52 men with ED and no known vascular risk factors were investigated in a double-blind correlation analysis. They noted a direct corre-lation between corporeal resistive index values and free-T, a relationship that was maintained after adjusting for age, SHBG, and estradiol. They concluded that men with ED and low free T may have an impaired relaxation of the penile smooth muscle, thus providing clinical evidence for the im-portance of androgen in regulating erectile function [56]. In a subsequent study, same researchers performed a perspective, randomized, placebo-controlled pilot study in 20 men with ED who failed sildenafil treatment (100-mg dose) on six consecutive attempts and had free T levels falling into the lower quartile of the lower range. One month after treatment
with transdermal T-patch and sildenafil on demand, we found significantly increased scores in the erectile function domain of the International Index of Erectile Function (IIEF). These clinical observations suggest a critical role for T in human erectile function. More importantly, in all pa-tients there was a strong direct correlation between resistive index values and free-T levels. Again, this relationship was maintained also when adjusted for age, SHBG, and estradiol. These results indicate that in men with ED, low free-T may correlate independently of age with the impaired relaxation of the cavernous smooth muscle cells [57].
These findings were then confirmed by other authors’ clinical studies who used a combination therapy with T-gel and sildenafil that has proven to be effective and safe in terms of overall and intercourse satisfaction for the patients, without side any effects on prostate size and PSA values in the long-term in hypogonadal patients [58]. This was con-firmed by a recent systematic review of the literature about prostate cancer risk associated with testosterone therapy for hypogonadism, in which it was suggested that testosterone therapy for hypogonadism did not increase prostate cancer risk or Gleason grade of cancer detected in treated vs. un-treated men [59]. However, the lack of clinical trial designed to investigate the safety of this combination therapy in the long-term, makes this option not recommended in at-large ED populations.
SYSTEMIC EFFECTS OF DRUGS TARGETED FOR ED
Up to 1998, yohimbine was the only world-wide oral available drug for the treatment of ED. In those years, a meta-analysis of all double-blind, randomized, placebo-controlled trials demonstrated significant benefits in patients treated with yohimbine (odds ratio 3.85, confidence interval 2.22 – 6.67%) [60]. Besides its central effect, it may act di-rectly at the level of corpora cavernosa facilitating their re-laxation by a dual mechanism: blocking -adrenergic recep-tors and releasing endothelium relaxing substances as NO. In an experimental model of hypogonadism, this latter activity is decreased, but completely restored by androgen supple-mentation. This effect was evident only in preparations in which the main source of NO was present (endothelium) or in which NO formation was not impaired by L-NAME, thus suggesting that its effects are both endothelium and andro-gen-dependent [61]. To date, no clinical trial regarding im-provements of endothelial function with the use of yo-himbine in men with ED is available.
Since PDE5-i are highly efficacious and widely used in treating male ED, it has been timely hypothesized that they may exert also important systemic effects, at the endothelial level, as well [62] (Fig. 1).
To further study this aspect, several studies had investi-gated the effects of sildenafil on blood pressure variations, mainly due to its vasodilatory effects and possible interac-tions with anti-hypertensive drugs. Sildenafil did not de-crease systemic arterial pressure because of its effect on re-nal PDE5 inactivation which elicits renin production thus counterbalancing hypotensive effects. Also, subsequent con-firmatory studies carried out in men with liver cirrhosis and ascites suggested the activation of the renin-angiotensin-

3772 Current Pharmaceutical Design, 2008, Vol. 14, No. 35 Aversa et al.
aldosterone pathway as a possible regulatory mechanism [63]. Further studies in an animal cirrhosis model clearly concluded that both acute and chronic sildenafil administra-tion has a natriuretic effect helping in preventing water reten-tion associated with liver cirrhosis [64]. The recent approval of sildenafil for the treatment of pulmonary idiopathic hyper-tension opens new applications for this class of drug, consid-ering its efficacy in such a difficult-to-treat population usu-ally refractory to conventional therapies [65]. In a rat model of chronic nitric oxide deprivation, where hypertension and aggravation of post-ischemic ventricular dysfunction are associated with loss of vascular endothelium-relaxant func-tion, sildenafil provided significant cardiovascular protec-tion, primarily by maintaining tissue cGMP levels [66]. It is important to remember that PDE5-i efficacy has been al-ready demonstrated in idiopathic refractory achalasia [67] and Raynaud’s phenomenon [68]. However, because in-creased NO production promotes upper airway congestion, muscle relaxation, and pulmonary vasodilatation, it is re-markable to remember that in patients with severe obstruc-tive sleep apnea, a single 50-mg dose of sildenafil at bedtime may worsen respiratory and desaturation events [69].
As already outlined, endothelial dysfunction plays a key-role in the pathogenesis of the atherosclerotic process and a growing interest on the effects of chronic PDE5-i in prevent-
ing atherosclerosis and the vascular endothelium is develop-ing [70]. The event that triggers endothelial dysfunction is represented by the reduction of overall antioxidant pool [71] with the consequent reduced response to oxidative stress and the activation of several pro-atherogenic processes: i. reduc-tion of NO bioavailability; ii. increased levels of circulating free fatty acids, with subsequent sub-endothelial storage of lipid depots and iii. increased smooth muscle cell prolifera-tion of the media layer of the vascular wall [72]. Pro-inflammatory and -infective processes may in turn contribute to activate and amplify the acute endothelial injury thus per-petuating such a vicious circle. In early atherogenic lesions, endothelial dysfunction causes adhesion and migration of monocytes and T-lymphocytes in the vascular inner layer in response to increased endothelial production of intercellular molecules, i.e. selectin, VCAM-1 and ICAM-1 that may quench NO [73]. This process may determine impaired arte-rial inflow to the penis, thus contributing to persistent ED. Although initiation of erection is mediated by rapid, short-term calcium-dependent release of NO from neuronal NOS-containing nerve terminals in the penis, full erection and maintenance of erection is achieved by the blood flow-induced phosphatidylinositol 3-kinase/Akt/eNOS (Ser-1177) phosphorylation cascade, resulting in reduced calcium de-pendence and sustained release of endothelial NO and con-
Fig. (1). Evidence-based (blue arrows) and putative molecular interactions between daily PDE5-i and the endothelium.
ACE= angiotensin-converting enzyme; AM=adrenomedullin; CAMs= cellular adhesion molecules; CRP=C-reactive protein; EPC=endo-
thelial progenitor cells; EMP=endothelial microparticles; ET-1=endothelin-1; ILs= Interleukins; NO= nitric oxide; RAA=renin-angiotensin-aldosterone; ROS=reactive oxigen species.
ED Drugs and Endothelial Function Current Pharmaceutical Design, 2008, Vol. 14, No. 35 3773
tinued cavernous smooth muscle relaxation [74]. Nowadays, data regarding the effects of PDE5-i on endothelial function are scarce and pilot studies in humans using chronic admini-stration of sildenafil have shown improvements both in en-dothelial [75] and cardiac functions [76]. Daily dose PDE5-i therapy and excessive cGMP accumulation may up-regulate PDE5 expression [77]. The clinical sequel of tachyphylaxis secondary to these mechanisms should include increased dosage requirements for efficacy. By contrast, a review of more than 1000 men using sildenafil for ED demonstrated low tachyphylaxis potential and dropout rates [78]; subse-quent studies on animal models have corroborated these findings [79]. Due to its most favorable pharmacokinetics, tadalafil administered on every other day produces steady state concentrations [80] that are able to enable better sexual performance and has confirmed patients’ such preference in the treatment of ED [81]. Furthermore, daily tadalafil was able to restore more than 30% of patients initially not re-sponding to on-demand treatment [82]. In another study by Porst et al., daily tadalafil at lower dosages (5 and 10 mg) was safe and effective and produced normalization of erec-tile function in up to 50% of men [83]. Moreover, the issue of daily dosing long-term safety was further investigated in a large multicenter trial in which no serious adverse event could have been demonstrated after one year of treatment with 5 mg per day, so far [84]. These benefits were con-firmed by our group in a recent study in men with ED of broad etiology. In that study, it was demonstrated that the rehabilitative effects of chronic tadalafil on vascular function occurs via improvement of surrogate markers of endothelial function, i.e. C-reactive protein, endothelin-1 and ICAM-1. This led to marked improvement of flow-mediated-vasodilatation (FMD) at the level of the cavernous arteries as well as better inflow to the penis when compared with on-demand regimes [85]. Moreover, this study was the very first one to report consistent improvements in morning erections as a possible mechanism for rehabilitative effects, which persisted even after 15 days withdrawal. We were also able to confirm same results in men without ED, in the presence of severe endothelial dysfunction associated with increased cardiovascular risk [86]. Noteworthy, we were able to dem-onstrate that such beneficial effects on endothelial function with once-a-day dosing were more pronounced in the occur-rence of severe endothelial dysfunction at study entry, as demonstrated by improvements in endothelial function after administration of tadalafil 10 mg daily for three months in a human model of Systemic Sclerosis [30]. Daily Tadalafil also significantly decreased hypoxia-induced up-regulation of TNF- and IL-1ß expression in pulmonary arteries, and improved erectile function in diabetic men representing a preferred dosing option when compared with on-demand administration [87]. The molecular mechanisms underlying this favorable systemic effects of chronic tadalafil admini-stration comes from recent animal studies and seems to be due to a complex mechanism: i. rescues the penis from apop-totic cell death; ii. increases two cell survival related kinases phosphorilation, namely Akt and ERK1/2 [88]. Preclinical data showing that long-term exposure of human cavernosal tissue to tadalafil neither resulted in up regulation of PDE5A expression nor decreased cyclic guanosine monophosphate levels [89]. Finally, also vardenafil has demonstrated effi-cacy in improving endothelial function in men with ED and
concomitant moderate penile arterial dysfunction [90]. Over-all, these data give the rationale for the chronic use of PDE5-i in men with ED and cardiovascular risk factors.
Incoming attention has been given to the effects of PDE5-i administration on steroid hormone production. In a recent study, the effects of the administration of sildenafil and tadalafil on steroid hormones were assessed for three months in patients with ED. Total- and free-testosterone raised more significantly in those subjects using tadalafil vs. sildenafil probably by activation of the hypothalamic-pituitary axis due to higher number of sex intercourses per month allowed by the long-acting drug [91]. Successive studies have demonstrated that due to its indirect action, the raising effect on testosterone is transient and is lost twelve months after continuative tadalafil assumption;
[92] testos-
terone:estradiol ratio increased due to a significant reduction of estradiol levels which may account for by tadalafil persis-tent efficacy over the time. This study suggested for the first time in humans a possible direct inhibitory effect of tadalafil on aromatase activity in humans independently from the body mass index and the quantity of adipose tissue; these data have been confirmed by preliminary in vitro results ob-tained by the authors in human adypocites (data unpub-lished) thus highlighting potential implications of chronic tadalafil treatment on prostate growth/lower urinary tract symtpoms, bone remodeling and breast cancer.
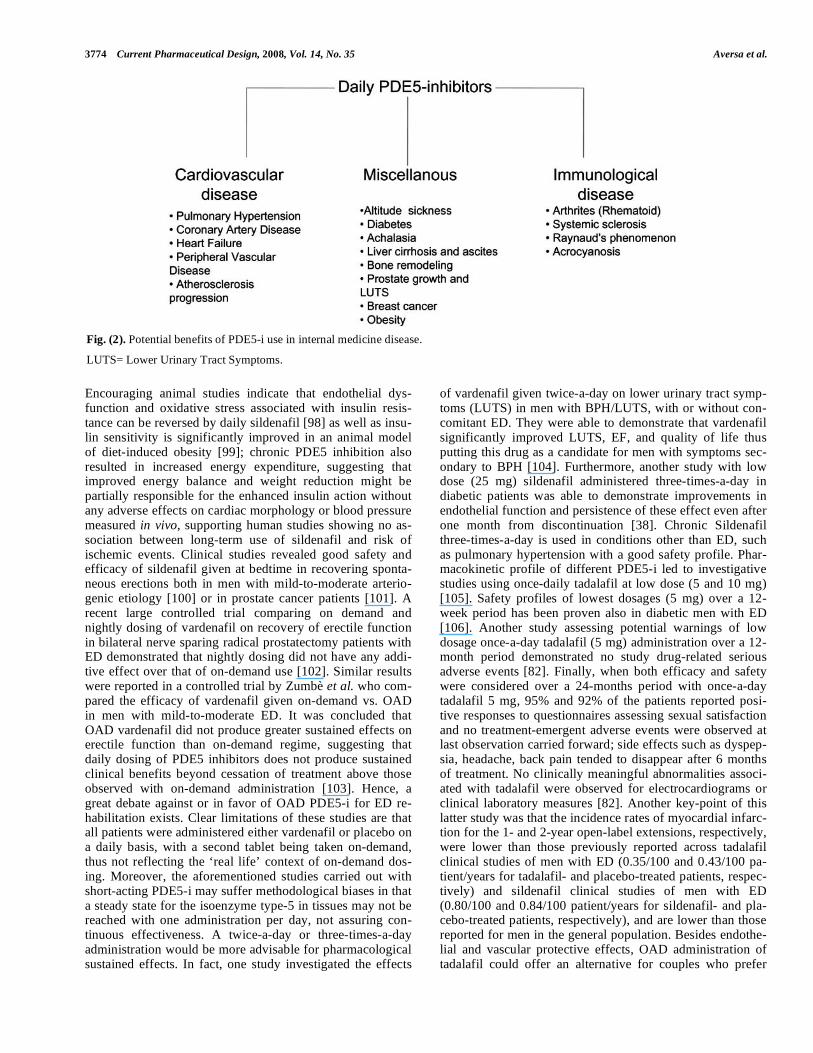
In conclusion, evidence-based medicine suggests that daily administration of PDE5-i determines better endothelial function [93] and may be of some utility in treating many non-andrological conditions [94] such as pulmonary hyper-tension, heart failure, diabetes, altitude sickness, Raynaud’s phenomenon (Fig. 2).
The future challenge seems to be the possibility of use daily dosing in special ED populations with a threefold pur-pose: 1) recovering non responders to on-demand therapy; 2) rehabilitation of erectile function which means endothelial rehabilitation and 3) modification of hormonal patterns with the possibility to possibly impact on prostate volume and bone remodeling, thus adding clinical evidence to the possi-bility of producing multiple systemic benefits [95]. On the basis of currently available evidence, it is possible to hy-pothesize that endothelial dysfunction and systemic cardio-vascular pathology may be modulated by daily PDE5 inhibi-tion, resulting in improved erectile function owing to effects upon both local and systemic targets. Unlike pulmonary hy-pertension, for which sildenafil may provide a net cost sav-ings compared with inhaled or intravenous medications [96], daily PDE5-i use may be actually limited by high costs, given the average intercourse frequency of five to six times per month. Should lower-dose daily administration confirm attractive efficacy and safety profiles compared with on-demand use, and equivalent net monthly cost approach, once-a-day PDE5-i use will become an important treatment option especially in complicated patients [97].
ON-DEMAND VS. CHRONIC PDE5-I DOSING: CRITICAL ISSUES RELATED TO EFFICACY IN
SEXUAL MEDICINE
Many concerns have been raised regarding rehabilitative effects of PDE5-i given once-a-day (OAD) in men with ED.
3774 Current Pharmaceutical Design, 2008, Vol. 14, No. 35 Aversa et al.
Encouraging animal studies indicate that endothelial dys-function and oxidative stress associated with insulin resis-tance can be reversed by daily sildenafil [98] as well as insu-lin sensitivity is significantly improved in an animal model of diet-induced obesity [99]; chronic PDE5 inhibition also resulted in increased energy expenditure,
suggesting that
improved energy balance and weight reduction might be partially responsible for the enhanced insulin action without any adverse effects on cardiac morphology or blood pressure measured in vivo, supporting human studies showing no as-sociation between long-term use of sildenafil and risk of ischemic events. Clinical studies revealed good safety and efficacy of sildenafil given at bedtime in recovering sponta-neous erections both in men with mild-to-moderate arterio-genic etiology [100] or in prostate cancer patients [101]. A recent large controlled trial comparing on demand and nightly dosing of vardenafil on recovery of erectile function in bilateral nerve sparing radical prostatectomy patients with ED demonstrated that nightly dosing did not have any addi-tive effect over that of on-demand use [102]. Similar results were reported in a controlled trial by Zumbè et al. who com-pared the efficacy of vardenafil given on-demand vs. OAD in men with mild-to-moderate ED. It was concluded that OAD vardenafil did not produce greater sustained effects on erectile function than on-demand regime, suggesting that daily dosing of PDE5 inhibitors does not produce sustained clinical benefits beyond cessation of treatment above those observed with on-demand administration [103]. Hence, a great debate against or in favor of OAD PDE5-i for ED re-habilitation exists. Clear limitations of these studies are that all patients were administered either vardenafil or placebo on a daily basis, with a second tablet being taken on-demand, thus not reflecting the ‘real life’ context of on-demand dos-ing. Moreover, the aforementioned studies carried out with short-acting PDE5-i may suffer methodological biases in that a steady state for the isoenzyme type-5 in tissues may not be reached with one administration per day, not assuring con-tinuous effectiveness. A twice-a-day or three-times-a-day administration would be more advisable for pharmacological sustained effects. In fact, one study investigated the effects
of vardenafil given twice-a-day on lower urinary tract symp-toms (LUTS) in men with BPH/LUTS, with or without con-comitant ED. They were able to demonstrate that vardenafil significantly improved LUTS, EF, and quality of life thus putting this drug as a candidate for men with symptoms sec-ondary to BPH [104]. Furthermore, another study with low dose (25 mg) sildenafil administered three-times-a-day in diabetic patients was able to demonstrate improvements in endothelial function and persistence of these effect even after one month from discontinuation [38]. Chronic Sildenafil three-times-a-day is used in conditions other than ED, such as pulmonary hypertension with a good safety profile. Phar-macokinetic profile of different PDE5-i led to investigative studies using once-daily tadalafil at low dose (5 and 10 mg) [105]. Safety profiles of lowest dosages (5 mg) over a 12-week period has been proven also in diabetic men with ED [106]. Another study assessing potential warnings of low dosage once-a-day tadalafil (5 mg) administration over a 12-month period demonstrated no study drug-related serious adverse events
[82]. Finally, when both efficacy and safety
were considered over a 24-months period with once-a-day tadalafil 5 mg, 95% and 92% of the patients reported posi-tive responses to questionnaires assessing sexual satisfaction and no treatment-emergent adverse events were observed at last observation carried forward; side effects such as dyspep-sia, headache, back pain tended to disappear after 6 months of treatment. No clinically meaningful abnormalities associ-ated with tadalafil were observed for electrocardiograms or clinical laboratory measures [82]. Another key-point of this latter study was that the incidence rates of myocardial infarc-tion for the 1- and 2-year open-label extensions, respectively, were lower than those previously reported across tadalafil clinical studies of men with ED (0.35/100 and 0.43/100 pa-tient/years for tadalafil- and placebo-treated patients, respec-tively) and sildenafil clinical studies of men with ED (0.80/100 and 0.84/100 patient/years for sildenafil- and pla-cebo-treated patients, respectively), and are lower than those reported for men in the general population. Besides endothe-lial and vascular protective effects, OAD administration of tadalafil could offer an alternative for couples who prefer
Fig. (2). Potential benefits of PDE5-i use in internal medicine disease.
LUTS= Lower Urinary Tract Symptoms.

ED Drugs and Endothelial Function Current Pharmaceutical Design, 2008, Vol. 14, No. 35 3775
spontaneous instead of scheduled sexual activities, or for those who anticipate frequent sexual activities, because dos-ing and sexual activity would no longer need to be tempo-rally linked.
There is a growing interest concerning the cross-reaction between PDE5-i and other isoenzymes like PDE11, because this is especially expressed in the prostatic gland, skeletal muscles, and the cross-reaction on this enzyme accounts for by some of the side effect of these drugs, like muscular pain and reduction of sperm quality [107]. A systematic review suggested a significant increase in sperm motility and viabil-ity both in vivo and in vitro after PDE5-i exposure, which seems to be enhanced at low doses and reduced at high con-centrations [108]. Pomara et al. have investigated the effects of a single sildenafil vs. tadalafil dose on sperm motility in a small cohort of young infertile men. Sildenafil administra-tion significantly increased sperm progressive motility; but that study lacked to investigate on the known effects of sild-enafil in stimulating a premature acrosomial reaction in vitro [109]. By contrast, tadalafil administration produced de-crease in sperm progressive motility [110]. The negative impact of tadalafil on sperm motility led to carry on a large randomized double-blind, placebo-controlled study carried out with daily tadalafil 20 mg over three spermatogenesis cycles in men over 45 yr [111]. In the opinion of the authors, the presentation of such rigorous scientific data, consistently disregarded that of Pomara’s by demonstrating a lack of un-toward effect on mean total sperm count, morphology, and motility. We can conclude that evidence-based results from multiple studies examining the effect of tadalafil on semen characteristics are among the most robust investigations of any human medicinal agent and the best studied of any PDE5-i.
CONCLUSIONS
Diagnosing endothelial dysfunction (by means of non-invasive FMD) and vascular ED (by means of dynamic penile Duplex ultrasound) is important in the clinical setting, and allows for an early detection of a systemic disease un-dermining men’s health. Furthermore, modification of re-versible causes i.e. inadequate lifestyle, cigarette smoking, alcohol or recreational drug abuse [112], hyperglycemia and hypertension, still represents the first approach to improve endothelial function and to promote general well-being and sexual health, as demonstrated by a recent study carried out on male US Veterans [113]. It is important to remember that also adequate plasmatic testosterone concentrations are cru-cial for the regulation of correct endothelial function and expression of penile PDE5 isoenzyme [114]. Daily PDE5-i administration improves endothelial function and may repre-sent a ‘salvage’ therapy especially in difficult-to-treat ED, i.e. uncompensated diabetes, bilateral nerve-sparing post-radical prostatectomy [115]. Although the safety of this class of agents has been indisputably established for the treatment of ED on an on-demand basis, there remains a paucity of data on the long-term endothelial effects and possible hor-monal side-effects of chronic use. Studies indicate main-tained treatment benefit (no tachyphylaxis) with minimal, well-tolerated side-effects; however, erectile function im-provements are not maintained after discontinuation of ther-apy, at least for the majority (approximately 75%) of the
patients [82]. Thus, FDA and EU regulatory authorities have recently approved once-a-day 5 mg tadalafil treatment for patients responding to prior PDE5 inhibitor therapy and who are exposed to high dosages due frequent use (more than 2-3 sex attempts per week). These data support the need for many patients with ED to continue therapy for successful sexual performance and endothelial rehabilitative benefits. Further well-designed, prospective randomized trials are urgently needed to assess whether once-a-day regimes will lead to restore sexual potency in patients with resistant mod-erate-to-severe ED without discontinuing the drug. Once these data will be validated in large population-based studies and endothelial penile benefits will be proven, commencing daily PDE5-i therapy combined with endothelial function enhancers in patients with refractory ED, i.e. post-radical prostatectomy, metabolic syndrome, diabetes mellitus, car-diovascular disease, chronic arthritis will represent the new frontier with the dual aim of slowing down the burden of atherosclerotic disease and curing ED.
ABBREVIATIONS
BPH = Benign Prostatic Hyperplasia
cGMP = Cyclic Guanosine MonoPhosphate
CHD = Coronary Heart Disease
CRFs = Cardiovascular Risk Factors
CRP = C-Reactive Protein
EC = Endothelial Cell
ECA = Endothelial Cell Activation
eNOS = Endothelial Nitric Oxide Synthase
nNOS = Neuronal Nitric Oxide Synthase
EMPs = Endothelial MicroParticles
EPCs = Endothelial Progenitor Cells
ERK = Extracellular signal-Regulated Kinase
ET-1 = Endothelin-1
FMD = Flow-Mediated-Dilatation
ICAM-1 = Intercellular Adhesion Molecule-1
IIEF = International Index of Erectile Function
IL-1 = Interleukin-1
IR = Insulin Resistance
IRS = Insulin-Receptor Substrates
L-NAME = Nitro-L-Arginine Methyl Ester
LUTS = Lower Urinary Tract Symptoms
NO = Nitric Oxide
OAD = Once-a-Day
PAT = Peripheral Arterial Tonometry
PI3K = Phosphatidylinositol 3-kinase
PDE5-i = Phosphodiesterase type-5 inhibitors
PSA = Prostate Specific Antigen
RAA = Renin-Angiotensin-Aldosterone
3776 Current Pharmaceutical Design, 2008, Vol. 14, No. 35 Aversa et al.
ROS = Reactive Oxigen Species
RNS = Reactive Nitrogen Species
SHBG = Sex Hormone Binding Globulin
T = Testosterone
T2DM = Type-2 Diabetes Mellitus
TNF- = Tumor Necrosis Factor alpha
VCAM-1 = Vascular Cell Adhesion Molecule-1
REFERENCES
[1] Vlachopoulos C, Rokkas K, Ioakeimidis N, Stefanadis C. Inflam-mation, metabolic syndrome, erectile dysfunction, and coronary ar-
tery disease: common links. Eur Urol 2007; 52: 1590-600. [2] Kaiser DR, Billups K, Mason C, Wetterling R, Lundberg JL, Bank
AJ. Impaired brachial artery endothelium-dependent and -indepen- dent vasodilation in men with erectile dysfunction and no other
clinical cardiovascular disease. J Am Coll Cardiol 2004; 43: 179-84. [3] Aversa A, Isidori AM, Gianfrilli D, Greco EA, Graziottin A, Zizzo
G, et al. Are subjects with erectile dysfunction aware of their con-dition? Results from a retrospective study based on an Italian free-
call information service. J Endocrinol Invest 2004; 27:548-56. [4] Gonzalez MA, Selwyn AP. Endothelial function, inflammation,
and prognosis in cardiovascular disease. Am J Med 2003; 115 (Suppl 8A): 99S-106S.
[5] Ross R. Atherosclerosis - An inflammatory disease. N Engl J Med 1999; 340: 115-26.
[6] Schwartz SM, Gajdusek CM, Reidy MA, Selden SC 3rd, Hauden-schild CC. Maintenance of integrity in aortic endothelium. Fed
Proc 1980; 39: 2618-25. [7] Haber E. Scientific American molecular cardiovascular medicine.
Scientific American Medicine: New York 1995. [8] Montorsi F, Briganti A, Salonia A, Rigatti P, Margonato A, Macchi
A, et al. Erectile dysfunction prevalence, time of onset and associa-tion with risk factors in 300 consecutive patients with acute chest
pain and angiographically documented coronary artery disease. Eur Urol 2003; 44: 360-4.
[9] Speel TG, van Langen H, Meuleman EJ. The risk of coronary heart disease in men with erectile dysfunction. Eur Urol 2003; 44: 366-
70. [10] Vlachopoulos C, Rokkas K, Ioakeimidis N, Aggeli C, Michaelides
A, Roussakis G, et al. Prevalence of asymptomatic coronary artery disease in men with vasculogenic erectile dysfunction: a prospec-
tive angiographic study. Eur Urol 2005; 48: 996-1002. [11] Bocchio M, Desideri G, Scarpelli P, Necozione S, Properzi G,
Spartera C, et al. Endothelial cell activation in men with erectile dysfunction without cardiovascular risk factor and overt vascular
damage. J Urol 2004; 171: 1601-04. [12] Kim J, Montagnani M, Koh KK, Quon MJ. Reciprocal relation-
ships between insulin resistance and endothelial dysfunction: mo-lecular and pathophysiological mechanisms. Circulation 2006; 113:
1888-904. [13] Zeng G, Nystrom FH, Ravichandran LV, Cong LN, Kirby M, Mo-
stowski, H. et al. Roles for insulin receptor, PI3-kinase, and Akt in insulin-signaling pathways related to production of nitric oxide in
human vascular endothelial cells. Circulation 2000; 101: 1539-1545.
[14] Quon MJ. Reciprocal relationships between insulin resistance and endothelial dysfunction: insights from therapeutic interventions.
Zhong Nan Da Xue Xue Bao Yi Xue Ban 2006;3:305-12. [15] Kobayashi T, Matsumoto T, Kamata K. The PI3-K/Akt pathway:
roles related to alterations in vasomotor responses in diabetic mod-els. J Smooth Muscle Res 2005; 41 6: 283-302.
[16] Hsueh WA, Quiñones MJ. Role of endothelial dysfunction in insu-lin resistance. Am J Cardiol 2003; 92: 10J-17J.
[17] Cersosimo E, DeFronzo RA. Insulin resistance and endothelial dysfunction: the road map to cardiovascular diseases. Diabetes Me-
tab Res Rev 2006; 22: 423-36. [18] Pop-Busui R, Sima A, Stevens M. Diabetic neuropathy and oxida-
tive stress. Diabetes Metab Res Rev 2006; 22: 257-73.
[19] Schwartz EA, Reaven PD. Molecular and signaling mechanisms of
atherosclerosis in insulin resistance. Endocrinol Metab Clin North Am 2006; 35: 525-49, viii.
[20] Hammarsten J, Högstedt B. Hyperinsulinaemia as a risk factor for developing benign prostatic hyperplasia. Eur Urol 2001; 39:151-8.
[21] Michel MC, Mehlburger L, Schumacher H, Bressel HU, Goepel M. Effect of diabetes on lower urinary tract symptoms in patients with
benign prostatic hyperplasia. J Urol 2000; 163: 1725-9. [22] Berger AP, Deibl M, Leonhartsberger N, Bektic J, Horninger W,
Fritsche G, et al. Vascular damage as a risk factor for benign prostatic hyperplasia and erectile dysfunction. BJU Int 2005; 96:
1073- 1078. [23] Berger AP, Horninger W, Bektic J, Pelzer A, Spranger R, Bartsch
G, et al. Vascular resistance in the prostate evaluated by colour Doppler ultrasonography: is benign prostatic hyperplasia a vascular
disease? BJU Int 2006; 98: 587-590. [24] McVary K. Lower urinary tract symptoms and sexual dysfunction:
epidemiology and pathophysiology. BJU Int 2006; 97(suppl 2):23-8.
[25] Brodsky SV, Zhang F, Nasjletti A, Goligorsky MS. Endothelium- derived microparticles impair endothelial function in vitro. Am J
Physiol Circ Heart Physiol 2004; 286: H1910-H1915. [26] Goldschmidt-Clermont PJ, Creager MA, Lorsordo DW, Lam
GKW, Wassef M, Dzau VJ. Atherosclerosis 2005: recent discover-ies and novel hypotheses. Circulation 2005; 112: 3348-53.
[27] Werner N, Wassmann S, Ahlers P, Schiegl T, Kosiol S, Link A, et al. Endothelial progenitor cells correlate with endothelial func-
tion in patients with coronary artery disease. Basic Res Cardiol 2007; 102: 565-71.
[28] Esposito K, Ciotola M, Giugliano F, Schisano B, Improta L, Im-prota MR, et al. Endothelial microparticles correlate with erectile
dysfunction in diabetic men. Int J Impot Res 2007; 19: 161-6. [29] Braunwald E. Biomarkers in heart failure. N Engl J Med 2008;
358: 2148-59. [30] Eaton CB, Liu YL, Mittleman MA, Miner M, Glasser DB, Rimm
EB. A retrospective study of the relationship between biomarkers of atherosclerosis and erectile dysfunction in 988 men. Int J Impot
Res 2007; 19: 218-25. [31] Virdis A, Ghiadoni L, Versari D, Giannarelli C, Salvetti A, Taddei
S. Endothelial function assessment in complicated hypertension. Curr Pharm Des 2008; 14: 1761-70.
[32] Proietti M, Aversa A, Letizia C, Rossi C, Menghi G, Bruzziches R, et al. Erectile dysfunction in systemic sclerosis: effects of long-
term inhibition of phosphodiesterase type-5 on erectile function and plasma endothelin-1 levels. J Rheumatol 2007; 34:1712-1717.
[33] Agrawal V, Ellins E, Donald A, Minhas S, Halcox J, Ralph DJ. Systemic Vascular Endothelial Dysfunction in Peyronie's Disease.
J Sex Med 2008 Jul 14. Epub ahead of print. [34] Deanfield J, Donald A, Ferri C, Giannattasio C, Halcox J, Halligan
S, et al. Endothelin and Endothelial Factors of the European Soci-ety of Hypertension. Endothelial function and dysfunction. Part I:
Methodological issues for assessment in the different vascular beds: A statement by the Working Group on Endothelin and Endo-
thelial Factors of the European Society of Hypertension. J Hyper-tens 2005; 23: 7-17.
[35] Patel S, Celermajer DS. Assessment of vascular disease using arterial flow mediated dilatation. Pharmacol Rep 2006; 57(Suppl):
3-7. [36] Virag R, Floresco J, Richard C. Impairment of shear-stress-
mediated vasodilation of cavernous arteries in erectile dysfunction. Int J Impot Res 2004; 16: 39-42.
[37] Kovács I, Császár A, Toth J, Siller G, Farkas A, Tarján J, et al. Correlation between flow-mediated-dilatation and erectile dysfunc-
tion. J Cardiovasc Pharmacol 2008; 51: 148-153. [38] Aversa A, Sarteschi LM. The role of penile color-Duplex ultra-
sound for the evaluation of erectile dysfunction. J Sex Med 2007; 4: 1437-47.
[39] Brunner H, Cockcroft JR, Deanfield J, Donald A, Ferrannini E, Halcox J, et al. and Working Group on Endothelin and Endothelial
Factors of the European Society of Hypertension. Endothelial func-tion and dysfunction. Part II: Association with cardiovascular risk
factors and diseases. A statement by the Working Group on Endo-thelins and Endothelial Factors of the European Society of Hyper-
tension. J Hypertens 2005; 23: 233-46. [40] Aversa A, Vitale C, Volterrani M, Fabbri A, Spera G, Fini M, et al.
Chronic administration of Sildenafil improves markers of endothe-
ED Drugs and Endothelial Function Current Pharmaceutical Design, 2008, Vol. 14, No. 35 3777
lial function in men with Type 2 diabetes. Diabet Med 2008; 25:
37-44. [41] Travison TG, Araujo AB, Kupelian V, O'Donnell AB, McKinlay
JB. The relative contributions of aging, health, and lifestyle factors to serum testosterone decline in men. J Clin Endocrinol Metab
2007; 92: 549-55. [42] Fukui M, Kitagawa Y, Ose H, Hasegawa G, Yoshikawa T, Naka-
mura N. Role of endogenous androgen against insulin resistance and atherosclerosis in men with type 2 diabetes. Curr Diabetes Rev
2007; 3: 25-31. [43] Waldkirch E, Uckert S, Schultheiss D, Geismar U, Bruns C,
Scheller F, et al. Non-genomic effects of androgens on isolated human vascular and nonvascular penile erectile tissue. BJU Int
2008; 101:71-5. [44] Yildiz O, Seyrek M. Vasodilating mechanisms of testosterone. Exp
Clin Endocrinol Diabetes 2007; 115: 1-6. [45] Rosano GM, Sheiban I, Massaro R, Pagnotta P, Marazzi G, Vitale
C, et al. Low testosterone levels are associated with coronary artery disease in male patients with angina. Int J Impot Res 2007; 19:
176-82. [46] Akishita M, Hashimoto M, Ohike Y, Ogawa S, Iijima K, Eto M,
et al. Low testosterone level is an independent determinant of en-dothelial dysfunction in men. Hypertens Res 2007; 30:1029-34.
[47] Foresta C, Caretta N, Lana A, De Toni L, Biagioli A, Ferlin A, et al. Reduced number of circulating endothelial progenitor cells in
hypogonadal men. J Clin Endocrinol Metab 2006; 91:4599-602. [48] Foresta C, Zuccarello D, De Toni L, Garolla A, Caretta N, Ferlin
A. Androgens stimulate endothelial progenitor cells through an an-drogen receptor-mediated pathway. Clin Endocrinol 2008; 68: 284-
9. [49] Smith MR, Lee H, Nathan DM. Insulin sensitivity during combined
androgen blockade for prostate cancer. J Clin Endocrinol Metab 2006 91:1305-1308.
[50] Traish AM, Park K, Dhir V, Kim NN, Moreland RB, Goldstein I. Effects of castration and androgen replacement on erectile function
in a rabbit model. Endocrinology 1999; 140: 1861-8. [51] Traish AM, Munarriz R, O’Connell L, Choi S, Kim SW, Kim NN,
et al. Effects of medical or surgical castration on erectile function in an animal model. J Androl 2003; 24: 381-7.
[52] Morelli A, Filippi S, Mancina R, Luconi M, Vignozzi L, Marini M, et al. Androgens regulate phosphodiesterase type-5 expression and
functional activity in corpora cavernosa. Endocrinology 2004; 145: 2253-63.
[53] Traish AM, Guay AT. Are androgens critical for penile erections in humans? Examining the clinical and preclinical evidence. J Sex
Med 2006; 3: 382-407. [54] Aversa A, Bruzziches R, Spera G. A rationale for the use of testos-
terone “salvage” in treatment of men with erectile dysfunction fail-ing phosphodiesterase inhibitors. Endocrinologist 2005; 15: 99-
105. [55] Shabsigh R, Rajfer J, Aversa A, Traish AM, Yassin A, Ka-
linchenko SY, et al. The evolving role of testosterone in the treat-ment of erectile dysfunction. Int J Clin Pract 2006; 60: 1087-92.
[56] Aversa A, Isidori AM, De Martino MU, Caprio M, Fabbrini E, Rocchietti-March M, et al. Androgens and penile erection: evi-
dence for a direct relationship between free testosterone and cav-ernous vasodilation in men with erectile dysfunction. Clin Endocri-
nol 2000; 53: 517-22. [57] Aversa A, Isidori AM, Spera G, Lenzi A, Fabbri A. Androgens
improve cavernous vasodilation and response to sildenafil in pa-tients with erectile dysfunction. Clin Endocrinol 2003; 58: 632-8.
[58] El-Sakka, AI, Hassoba HM, Elbakry AM, Hassan HA. Prostate Specific Antigen in patients with hypogonadism: effect of testos-
terone replacement. J Sex Med 2005; 2: 235-40. [59] Shabsigh R, Crawford ED, Nehra A, Slawin KM. Testosterone
therapy in hypogonadal men and potential prostate cancer risk: a systematic review. Int J Impot Res 2008; [Epub ahead of print].
[60] Ernst E, Pittler MH. Yohimbine for erectile dysfunction: a system-atic review and meta-analysis of randomized clinical trials. J Urol
1998; 159: 433-6. [61] Filippi S, Luconi M, Granchi S, Natali A, Tozzi P, Forti G, et al.
Endothelium-dependency of yohimbine-induced corpus caverno-sum relaxation. Int J Impot Res 2002; 14: 295-307.
[62] Reffelmann T, Kloner RA. Cardiovascular effects of phosphodi-esterase 5 inhibitors. Curr Pharm Des 2006; 12: 3485-94.
[63] Thiesson HC, Jensen BL, Jespersen B, Schaffalitzky de Muckadell
OB, Bistrup C et al. Inhibition of cGMP-specific phosphodiesterase type 5 reduces sodium excretion and arterial blood pressure in pa-
tients with NaCl retention and ascites. Am J Physiol Renal Physiol 2005; 288: F1044-52.
[64] Ghali-Ghoul R, Tahseldar-Roumieh R, Sabra R. Effect of chronic administration of sildenafil on sodium retention and on the hemo-
dynamic complications associated with liver cirrhosis in the rat. Eur J Pharmacol 2007; 572: 49-56.
[65] Galiè N, Ghofrani HA, Torbicki A, Barst RJ, Rubin LJ, Badesch D et al; Sildenafil Use in Pulmonary Arterial Hypertension (SUPER)
Study Group. Sildenafil citrate therapy for pulmonary arterial hy-pertension. N Engl J Med 2005; 353: 2148-57.
[66] Takimoto E, Champion HC, Belardi D, Ren S, Rodriguez ER, Bedja D, et al. Chronic inhibition of phosphodiesterase type 5A
prevents and reverses cardiac hypertrophy. Nat Med 2005; 11: 214-22.
[67] Bortolotti M, Mari C, Lopilato C, Porrazzo G, Miglioli M. Effects of sildenafil on esophageal motility of patients with idiopathic
achalasia. Gastroenterology 2000; 118: 253-7. [68] Levien TL. Phosphodiesterase inhibitors in Raynaud's phenome-
non. Ann Pharmacother 2006; 40:1388-93. [69] Roizenblatt S, Guilleminault C, Poyares D, Cintra F, Kauati A,
Tufik S. A double-blind, placebo-controlled, crossover study of sildenafil in obstructive sleep apnea. Arch Intern Med 2006; 166:
1763-7. [70] Aversa A, Bruzziches R, Pili M, Spera G. Phosphodiesterase 5
inhibitors in the treatment of erectile dysfunction. Curr Pharm Des 2006; 12: 3467-84.
[71] Parodi O, De Maria R, Roubina E. Redox state, oxidative stress and endothelial dysfunction in heart failure: the puzzle of nitrate-thiol
interaction. J Cardiovasc Med (Hagerstown) 2007; 8: 765-74. [72] Marks DS, Vita JA, Folts JD, Keaney JF Jr, Welch GN, Loscalzo J.
Inhibition of neointimal proliferation in rabbits after vascular injury by a single treatment with a protein adduct of nitric oxide. J Clin
Invest 1995; 96: 2630-8. [73] Basta G, Schmidt AM, De Caterina R. Advanced glycation end
products and vascular inflammation: implications for accelerated atherosclerosis in diabetes. Cardiovasc Res 2004; 63: 582-92.
[74] Hurt K J, Musicki B, Palese M A, Crone J K, Becker R E, Moriar-ity JL, et al. Akt-dependent phosphorylation of endothelial nitric-
oxide synthase mediates penile erection. Proc Natl Acad Sci USA 2002; 99: 4061-6.
[75] Desouza C, Parulkar A, Lumpkin D, Akers D, Fonseca VA. Acute and Prolonged Effects of Sildenafil on Brachial Artery Flow-
Mediated Dilatation in Type 2 Diabetes. Diabetes Care 2002; 25: 1336-1339.
[76] Gori T, Sicuro S, Dragoni S, Donati G, Forconi S, Parker JD. Sild-enafil prevents endothelial dysfunction induced by ischemia and
reperfusion via opening of adenosine triphosphate-sensitive potas-sium channels. Circulation 2005; 111:742-746.
[77] Steers WD. Tachyphylaxis and phosphodiesterase type 5 inhibitors. J Urol 2002; 168: 207.
[78] El-Galley R, Rutland H, Talic R, Keane T, Clark H. Longterm efficacy of sildenafil and tachyphylaxis effect. J Urol 2001; 166:
927-31. [79] Behr-Roussel D, Gorny D, Mevel K, Caisey S, Bernabé J, Burgess
G, et al. Chronic sildenafil improves erectile function and endothe-lium-dependent cavernosal relaxations in rats: lack of tachyphy-
laxis. Eur Urol 2005; 47: 87-91. [80] Forgue ST, Patterson BE, Bedding AW, Payne CD, Phillips DL,
Wrishko RE, et al. Tadalafil pharmacokinetics in healthy subjects. Br J Clin Pharmacol 2006; 61: 280-8.
[81] Mirone V, Imbimbo C, Rossi A, Sicuteri R, Valle D, Longo N, et al. Italian Sure Study Group. Evaluation of an alternative dosing
regimen with tadalafil, three times per week, for men with erectile dysfunction: SURE study in Italy. Asian J Androl 2007; 9: 395-
402. [82] McMahon C. Efficacy and safety of daily tadalafil in men with
erectile dysfunction previously unresponsive to on-demand tada-lafil. J Sex Med 2004; 1:292-300.
[83] Porst H, Giuliano F, Glina S, Ralph D, Casabé AR, Elion-Mboussa A, et al. Evaluation of the efficacy and safety of once-a-day dosing
of tadalafil 5 mg and 10 mg in the treatment of erectile dysfunction: results of a multicenter, randomized, double-blind, placebo-
controlled trial. Eur Urol 2006; 50: 351-9.
3778 Current Pharmaceutical Design, 2008, Vol. 14, No. 35 Aversa et al.
[84] Porst H, Rajfer J, Casabé A, Feldman R, Ralph D, Vieiralves LF,
et al. Long-term safety and efficacy of tadalafil 5 mg dosed once daily in men with erectile dysfunction. J Sex Med 2008; 5:2160-9.
[85] Aversa A, Greco E, Bruzziches R, Pili M, Rosano G, Spera G. Relationship between chronic tadalafil administration and im-
provement of endothelial function in men with erectile dysfunction: a pilot study. Int J Impot Res 2007; 19: 200-7.
[86] Rosano GM, Aversa A, Vitale C, Fabbri A, Fini M, Spera G. Chronic treatment with tadalafil improves endothelial function in
men with increased cardiovascular risk. Eur Urol 2005; 47: 214-20. [87] Buvat J, Van Ahlen H, Schmitt H, Chan M, Kuepfer C, Varanese
L. Efficacy and safety of two dosing regimens of tadalafil and pat-terns of sexual activity in men with diabetes mellitus and erectile
dysfunction: scheduled use vs. on-demand regimen evaluation (SURE) study in 14 European countries. J Sex Med 2006; 3: 512-
20. [88] Lysiak JL, Yang SK, Klausner AP, Son H, Tuttle JB, Steers WD.
Tadalafil increases Akt and extracellular signal-regulated kinase 1/2 activation, and prevents apoptotic cell death in the penis fol-
lowing denervation. J Urol 2008; 179, 779-785. [89] Vernet D, Magee T, Qian A, Nolazco G, Rajfer J, Gonzalez-
Cadavid N. Phosphodiesterase type 5 is not upregulated by tadalafil in cultures of human penile cells. J Sex Med 2006; 3: 84-94.
[90] Mazo EB, Gamidov SI, Iremashvil VV. Does the clinical efficacy of vardenafil correlate with its effect on the endothelial function of
cavernosal arteries? A pilot study. BJU Int 98 2006; 1054-58. [91] Carosa E, Martini P, Brandetti F, Di Stasi SM, Lombardo F, Lenzi
A, et al. Type 5 phosphodiesterase inhibitor treatments for erectile dysfunction increase testosterone levels. Clin Endocrinol 2004; 61:
382-6. [92] Greco EA, Pili M, Bruzziches R, Corona G, Spera G, Aversa A.
Testosterone : estradiol ratio changes associated with long-term ta-dalafil administration: a pilot study. J Sex Med 2006; 3:716-22.
[93] Sandner P, Hutter J, Tinel H, Ziegelbauer K, Bischoff E. PDE5 inhibitors beyond erectile dysfunction. Int J Impot Res 2007; 19:
533-43. [94] Bella AJ, DeYoung LX, al-Numi M, Brock GB. Daily administra-
tion of phosphodiesterase type-5 inhibitors for urological and non-urological indications. Eur Urol 2007; 52: 990-1005.
[95] Bruzziches R, Greco EA, Pili M, Francomano D, Spera G, Aversa A. Redefining the role of long-acting phosphodiesterase inhibitor
tadalafil in the treatment of diabetic erectile dysfunction. Curr Dia-betes Rev 2008; 4: 24-30.
[96] Vida VL, Gaitan G, Quezada E, Barnoya J, Castañeda AR. Low-dose oral sildenafil for patients with pulmonary hypertension: a
cost-effective solution in countries with limited resources. Cardiol Young 2007; 17: 72-7.
[97] Aversa A, Bruzziches R, Vitale C, Marazzi G, Francomano D, Barbaro G. et al. Chronic sildenafil in men with diabetes and erec-
tile dysfunction. Expert Opin Drug Metab Toxicol 2007; 3: 451-64. [98] Behr-Roussel D, Oudot A, Caisey S, Coz OL, Gorny D, Bernabé J,
et al. Daily treatment with sildenafil reverses endothelial dysfunc-tion and oxidative stress in an animal model of insulin resistance.
Eur Urol 2008; 53: 1272-80. [99] Ayala JE, Bracy DP, Julien BM, Rottman JN, Fueger PT, Wasser-
man DH. Chronic treatment with sildenafil improves energy bal-ance and insulin action in high fat-fed conscious mice. Diabetes
2007; 56: 1025-33.
[100] Sommer F, Klotz T, Engelmann U. Improved spontaneous erectile
function in men with mild-to-moderate arteriogenic erectile dys-function treated with a nightly dose of sildenafil for one year: a
randomized trial. Asian J Androl 2007; 9: 134-41. [101] Padma-Nathan H, McCullough AR, Levine LA, Lipshultz LI, Sie-
gel R, Montorsi F, et al. Randomized, double-blind, placebo-controlled study of postoperative nightly sildenafil citrate for the
prevention of erectile dysfunction after bilateral nerve-sparing radi-cal prostatectomy. Int J Impot Res 2008 Jul 24.
[102] Montorsi F, Brock G, Lee J, Shapiro J, Van Poppel H, Graefen M, et al. Effect of nightly versus on-demand vardenafil on recovery of
erectile function in men following bilateral nerve-sparing radical prostatectomy. Eur Urol 2008; 54(4): 924-31.
[103] Zumbe J, Porst H, Sommer F, Grohmann W, Beneke M, Ulbrich E. Comparable efficacy of once-daily versus on-demand vardenafil in
men with mild-to-moderate erectile dysfunction: findings of the RESTORE Study. Eur Urol 2008; 54: 204-212.
[104] Stief CG, Porst H, Neuser D, Beneke M, Ulbrich E. A randomized, placebo-controlled study to assess the efficacy of twice-daily
vardenafil in the treatment of lower urinary tract symptoms secon-dary to benign prostatic hyperplasia. Eur Urol 2008; 53:1236-44.
[105] Porst H, Giuliano F, Glina S, Ralph D, Casabé AR, Elion-Mboussa A, et al. Evaluation of the efficacy and safety of once-a-day dosing
of tadalafil 5mg and 10mg in the treatment of erectile dysfunction: results of a multicenter, randomized, double-blind, placebo-
controlled trial. Eur Urol 2006;50: 351-9. [106] Hatzichristou D, Gambla M, Rubio-Aurioles E, Buvat J, Brock GB,
Spera G, et al. Efficacy of tadalafil once daily in men with diabetes mellitus and erectile dysfunction. Diabet Med 2008; 25:138-46.
[107] Pomara G, Morelli G. Inhibition of phosphodiesterase 11 (PDE11) impacts on sperm Quality. Int J Impot Res 2005; 17: 385-386.
[108] Mostafa T. Oral phosphodiesterase-5 inhibitors and sperm func-tions. Int J Impot Res 2008; 20(6): 530-6.
[109] Glenn DRJ, McVicar CM, McClure N, Lewis SEM. Sildenafil citrate improves sperm motility but causes a premature acrosome
reaction in vitro. Fertil Steril 2007; 87: 1064-70. [110] Pomara G, Morelli G, Canale D, Turchi P, Caglieresi C, Moschini
C, et al. Alterations in sperm motility after acute oral administra-tion of sildenafil or tadalafil in young, infertile men. Fertil Steril
2007; 88: 860-5. [111] Hellstrom WJ, Gittelman M, Jarow J, Steidle C, McMurray J, Tal-
ley D, et al. An evaluation of semen characteristics in men 45 years of age or older after daily dosing with tadalafil 20mg: results of a
multicenter, randomized, double-blind, placebo-controlled, 9-month study. Eur Urol 2008; 53: 1058-65.
[112] Aversa A, Rossi F, Francomano D, Bruzziches R, Bertone C, San-tiemma V, et al. Early endothelial dysfunction as a marker of vas-
culogenic erectile dysfunction in young habitual cannabis users. Int J Impot Res 2008; in press.
[113] Khatana SA, Taveira TH, Miner MM, Eaton CB, Wu WC. Does cardiovascular risk reduction alleviate erectile dysfunction in men
with type II diabetes mellitus? Int J Impot Res 2008; 20(5): 501-6. [114] Greco EA, Spera G, Aversa A. Combining testosterone and PDE5
inhibitors in erectile dysfunction: basic rationale and clinical evi-dences. Eur Urol 2006; 50: 940-7.
[115] Montorsi F, Briganti A, Salonia A, Rigatti P, Burnett AL. Can phosphodiesterase type 5 inhibitors cure erectile dysfunction? Eur
Urol 2006; 49: 979-86.
Related Documents











