Endometrial Endometrial Cancer Cancer Presented by Presented by Dr/ Ahmed Walid Anwar Dr/ Ahmed Walid Anwar Assistant professor of Obs & Gyn Assistant professor of Obs & Gyn Benha Faculty of Medicine Benha Faculty of Medicine

Endometrial Cancer; Evidence Based Approach
Jul 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Endometrial Endometrial CancerCancerPresented byPresented by
Dr/ Ahmed Walid AnwarDr/ Ahmed Walid AnwarAssistant professor of Obs & Gyn Assistant professor of Obs & Gyn
Benha Faculty of MedicineBenha Faculty of Medicine
Endometrial cancer
– The most common ♀ pelvic genital cancer .
– The life time risk of developing endometrial Ca is 2.4% in white women & 1.3% in black (In USA).
– Age: Peak incidence in the 6th & 7th decade of life (disease of
postmenopausal women). Only 2-5% occur before 40 years.
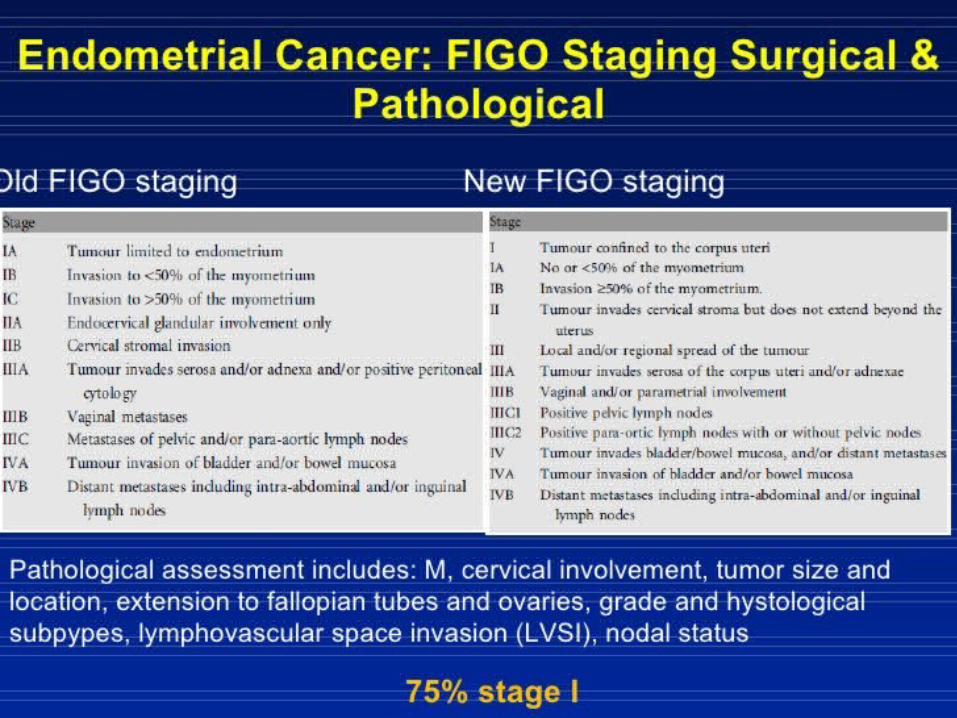
– Higher survival rate due to early diagnosis ( 75% diagnosed in Stage I).
– Estrogen has been implicated as a causative factor.
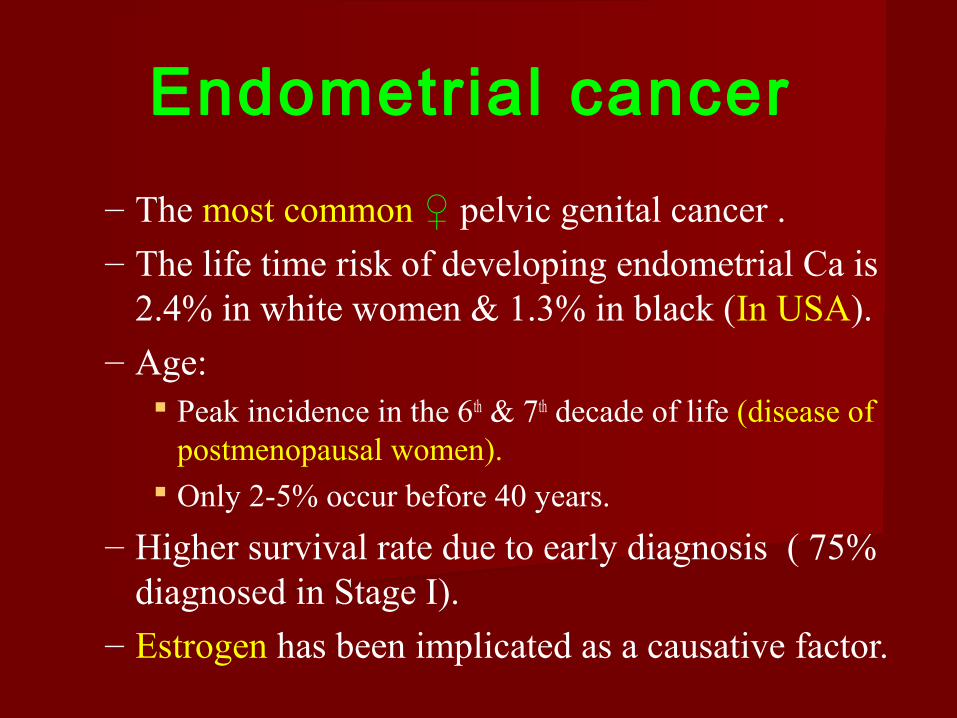
These risk factors are only helpful in identifying women at risk for type I disease.
Risk factors for endometrial cancer OLD AUNT
O=Obesity
L=Late menopause
D=Diabetes mellitus
A=cAncer: ovarian, breast, colon
U=Unopposed estrogen: PCOS, anovulation, HRT
N=Nulliparity
T=Tamoxifen, chronic use
Causes of high unopposed estrogen Exogenous Estrogen: Estrogen Replacement
Therapy in postmenopausal women. Endogenous Estrogen:
– Increased secretion : e.g. feminizing ovarian tumors (granulose cell tumor).
– Increased androgen precursors: e.g. androgen secreting tumors, liver diseases, chronic an-ovulation (PCOS), or stress.
– Increased aromatization: e.g. obesity, liver diseases, or hyperthyroidism.
– Increased free estrogen due to decreased level of SHBG.
Protective Factors1. Oral contraceptives: Protective effect probably due to progesterone
Decreases both the risk of ovarian and endometrial cancer (RR = 0.6 if
used for one year…effect lasts for 15 years!)
1. Physical activity
2. Pregnancy and breast-feeding :The risk may be lower in women with a
higher number of pregnancies and who breast-feed for more than 18 months.
3. Diet: low in saturated fats and high in fruits and vegetables and soy -based foods as
a regular part of the diet may lower the risk of endometrial cancer.
4. Smoking
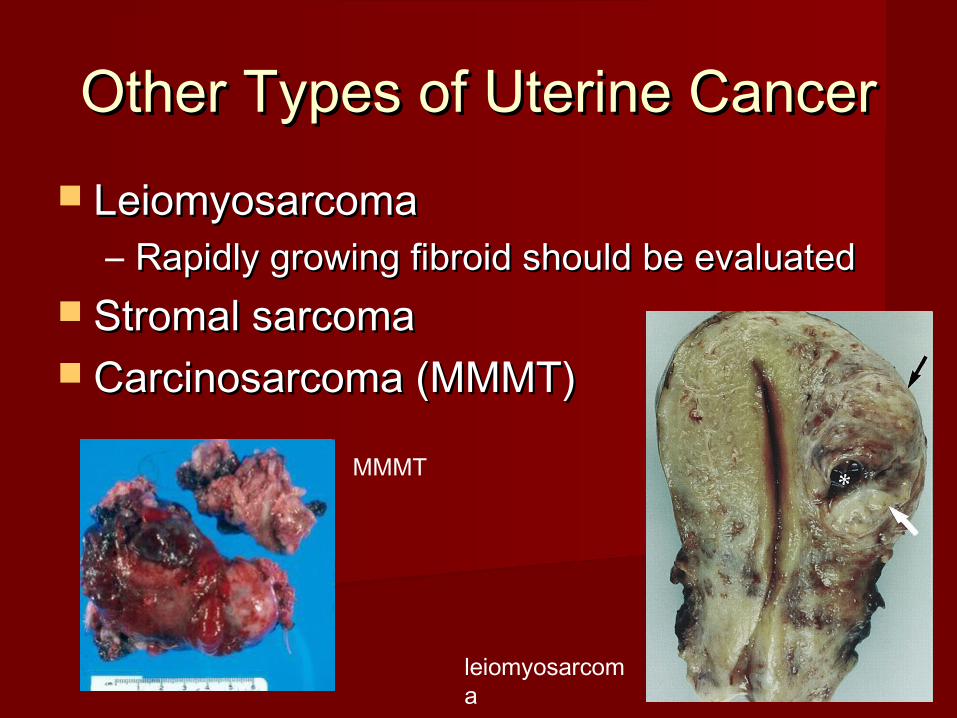
Other Types of Uterine CancerOther Types of Uterine Cancer LeiomyosarcomaLeiomyosarcoma
– Rapidly growing fibroid should be evaluated Rapidly growing fibroid should be evaluated Stromal sarcomaStromal sarcoma Carcinosarcoma (MMMT)Carcinosarcoma (MMMT)
leiomyosarcoma
MMMT
Spread PatternsSpread Patterns Direct extension Direct extension
– most commonmost common Transtubal Transtubal LymphaticLymphatic
– Pelvic usually first, then para-aorticPelvic usually first, then para-aortic HematogenousHematogenous
– Lung most commonLung most common– Liver, brain, boneLiver, brain, bone
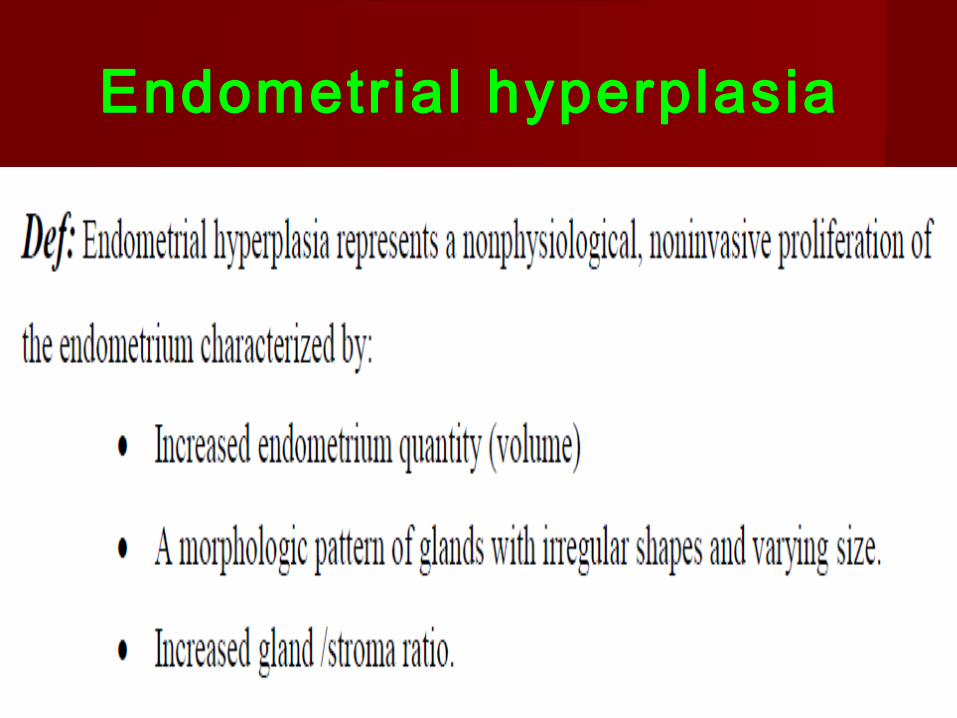
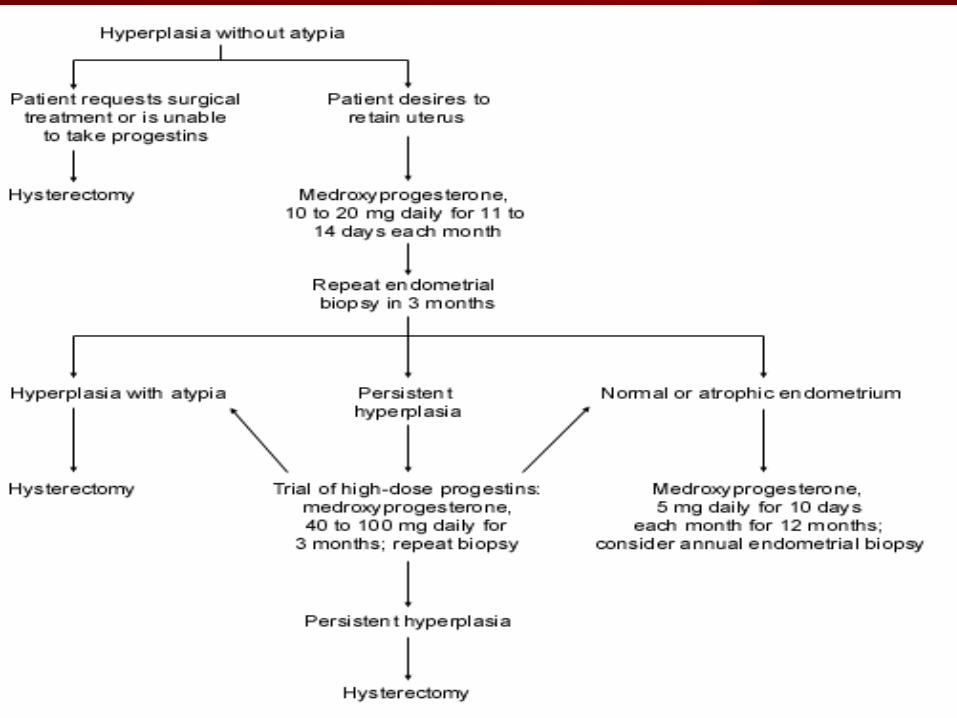
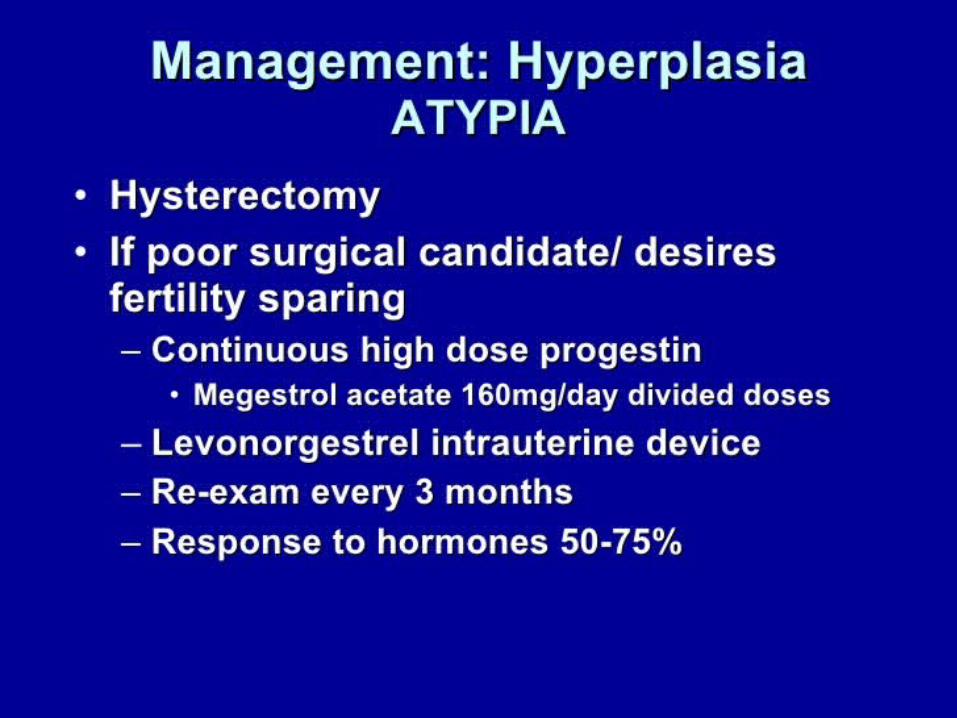
Endometrial hyperplasia
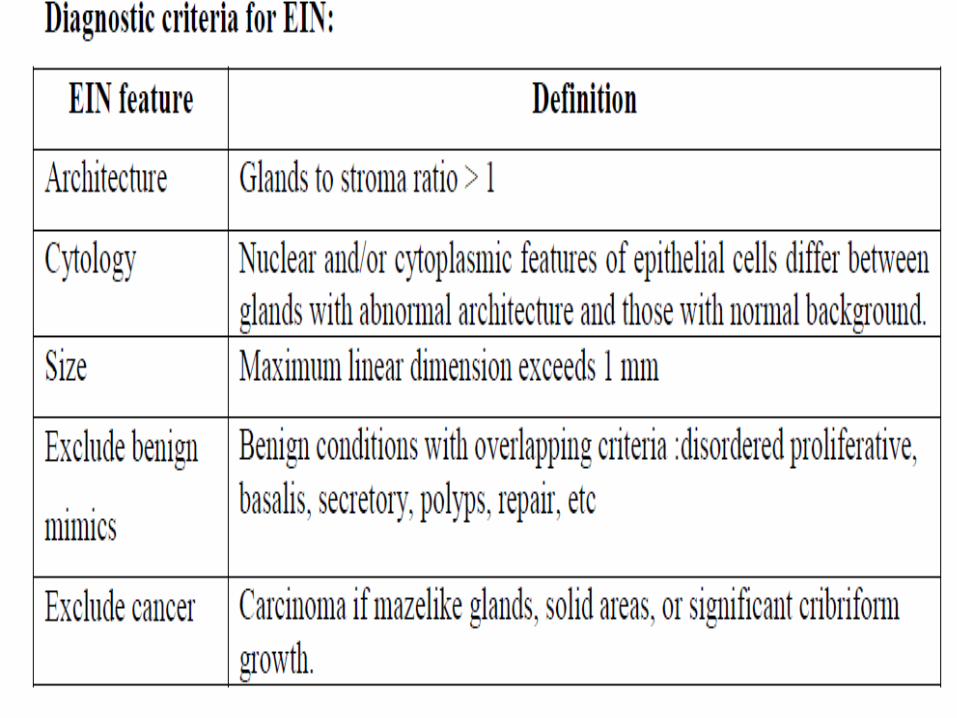
Endometrial Intraepithelial Neoplasia (EIN) system
Def: EIN is a histopathological presentation of premalignant
endometrial disease which elevated the risk of {endometrioid
(Type I) endometrial adenocarcinoma}.
Significance:
– Women with endometrial hyperplasia subdivided into EIN
versus non-EIN categories.
– Progression to cancer more than one year following
EIN diagnosis is 45 times more likely compared to
women without EIN.

RepresentationRepresentation Asymptomatic : Endometrial cells on PapAsymptomatic : Endometrial cells on Pap BB: : The “classic symptom” is abnormal uterine Bleeding
20-30% of women with post-menopausal bleeding will have uterine cancer.
( the risk is higher the farther they are away from menopause)
CC DD EE P (Pain, Pressure)P (Pain, Pressure) MetastasisMetastasis
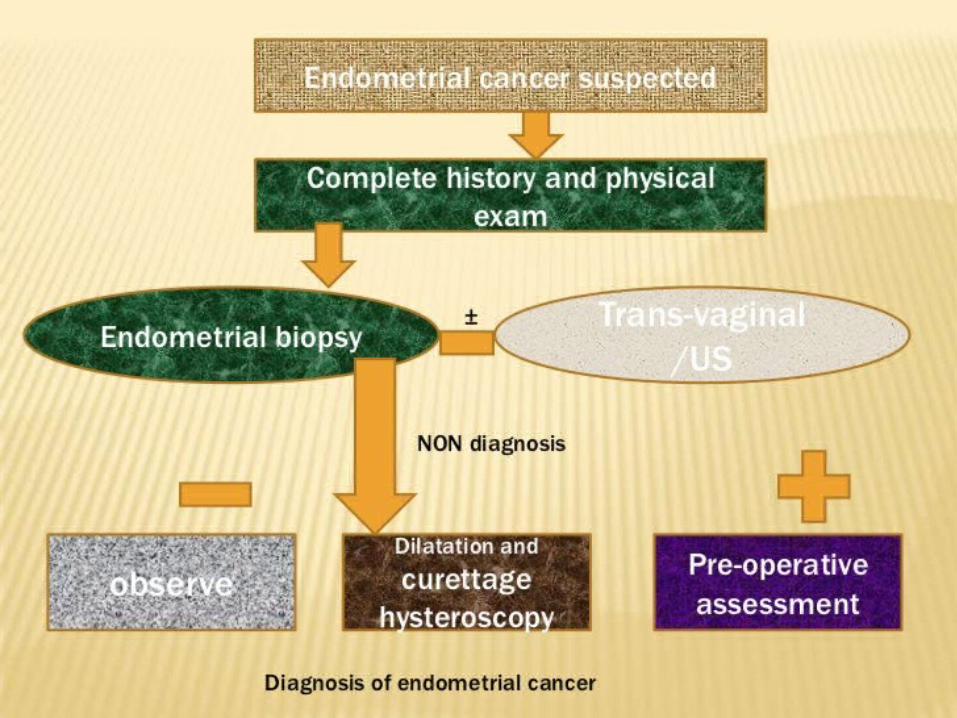
Diagnostic evaluation Outpatient endometrial biopsy with the Pipelle catheter is
reliable and accurate for the detection of disease in most cases of
endometrial cancer (level of evidence: A).
Detection rates by pipelle was :Detection rates by pipelle was :
– 91 and 99% for endometrial ca. 91 and 99% for endometrial ca.
– 81% for hyperplasia was81% for hyperplasia was
Hysteroscopic-guided endometrial biopsy remains the gold
standard for endometrial cancer diagnosis (level of evidence:
A ).
Diagnostic evaluation
Transvaginal ultrasonography is highly sensitive
and specific in predicting the presence of endometrial
cancer and can be used to select patients for
endometrial biopsy (level of evidence: B).
If symptomatology persists despite negative findings
from the previously cited tests, further evaluation is
justified because none of these tests have 100%
sensitivity (level of evidence: B).
Metastatic evaluation
Routine preoperative assessment of endometrial cancer
patients with imaging tests evaluating for metastasis is not
necessary as it is surgically staged disease (level of evidence:
A).
Serum CA125 measurement may be useful in management
planning of selected endometrial cancer patients but cannot
currently be recommended for routine clinical use (level of
evidence: C).
Treatment
Treatment of endometrial hyperplasia .
Treatment of endometrial cancer.
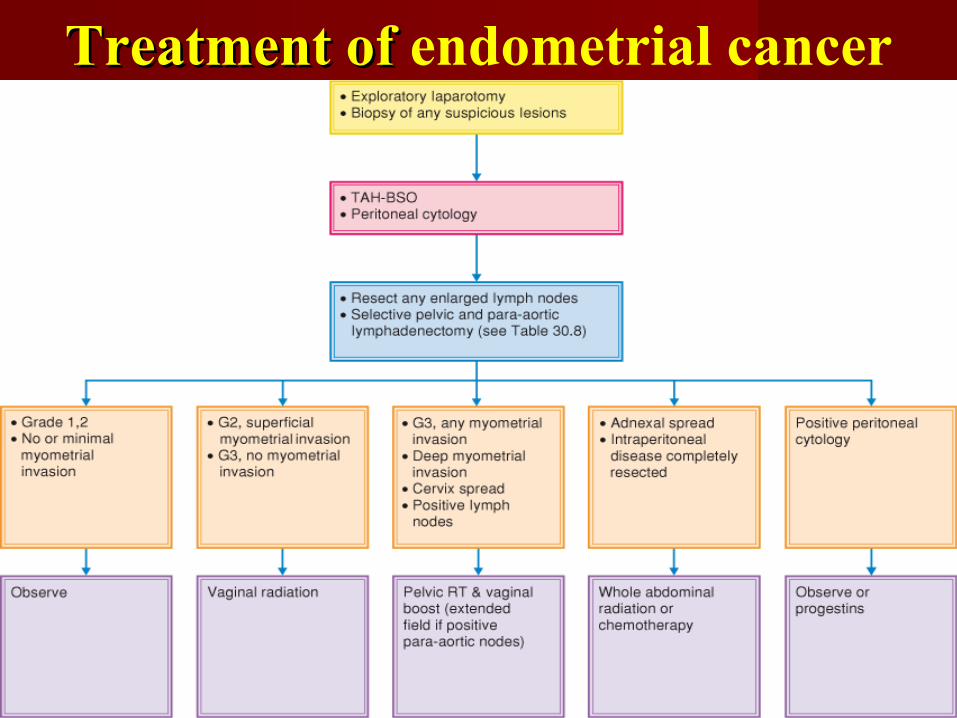
Treatment of Treatment of endometrial cancer
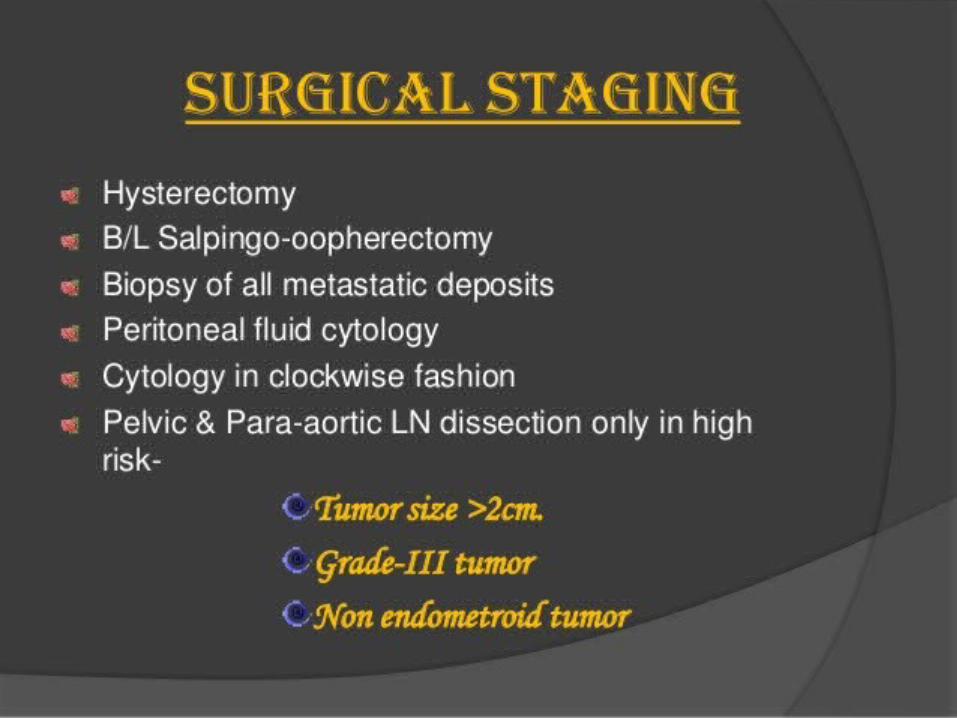
Approach to endometrial cancer: best practices
The initial management of endometrial cancer should include
total hysterectomy, bilateral salpingo-oophorectomy, and
pelvic and para-aortic lymphadenectomy. Exceptions to this
approach should be made only after consultation with a
gynecologic oncologist (level of evidence: A).
Laparoscopy should be embraced as the standard surgical
approach for comprehensive surgical staging in women with
endometrial cancer (level of evidence: A).
Approach to endometrial cancer: best practices
Vaginal hysterectomy may be an appropriate
treatment in select patients who are at high risk
for surgical morbidity (level of evidence: C).
Robotic-assisted laparoscopic staging is feasible
and safe in women with endometrial cancer (level
of evidence: B).
Role of lymphadenectomy
Patients with grade 1–2 endometrioid tumors, less than 50%myometrium invasion, and tumor of 2 cm or less seem to be at low risk for recurrence and may not require a surgical lymphadenectomy (level of evidence: B).
Lymphadenectomy may alter or eliminate the need for adjuvant therapy and its associated morbidity (level of evidence: B).
Sentinel lymph node dissection may reduce the morbidity associated with standard lymphadenectomy and may enhance the therapeutic benefit of surgical staging in early endometrial cancer (level of evidence: I).
Surgical approach for advanced endometrial cancer
Aggressive surgical cytoreduction improves progression-free and overall survival in patients with advanced or recurrent endometrial cancer (level of evidence: C).
Exenteration offers the only curative option in patients with recurrent endometrial cancer who have received previous irradiation (level of evidence: C).

Adjuvant Therapy inEndometrial Cancer
Stage I Intermediate-Risk Endometrial Cancers
External beam pelvic radiotherapy
– 1. Pelvic radiation has been shown to reduce local
recurrence in low to intermediate-risk endometrial
carcinoma. (II-1)
– 2. Pelvic radiation has been shown to reduce local
pelvic and vaginal recurrences in intermediate- to
high-risk endometrial carcinoma. (II-1)
Stage I Intermediate-Risk Endometrial Cancers
Vaginal brachytherapy
– 3. Vaginal brachytherapy alone in the treatment of women with
intermediate- to high-risk endometrial cancer has been shown to have
outcomes in local control and overall survival that are similar to those
of pelvic radiotherapy in a well-defined intermediate- to high-risk
group. (I)
– 4. Vaginal brachytherapy has the same outcome as external beam
radiotherapy with respect to overall survival in the defined
intermediate- to high-risk group. (I)
Stage I Intermediate-Risk Endometrial Cancers
Chemotherapy– 5. Chemotherapy has not been well studied in
stage I intermediateto high-risk endometrial cancers. There is no strong evidence for or against chemotherapy in this population at present. The benefits of chemotherapy in addition to adjuvant radiotherapy specifically in surgically stage I patients with high-risk features are not clearly defined. (III)
Stage I Intermediate-Risk Endometrial Cancers
Expectant Management– 6. Patients in the intermediate-risk category who
are managed expectantly have a higher recurrence
rate than those who are treated, although there has
not been a lack of survival benefit demonstrated.
Patients who are managed expectantly report
higher scores in quality of life studies because of
less gastrointestinal toxicity. (II-3)
Advanced Stage (II to IV) Endometrial Cancer
– 7. Chemotherapy with cisplatin and doxorubicin
or carboplatin and paclitaxel has demonstrated
efficacy in advanced uterine cancer in published
phase III studies. (II-2)
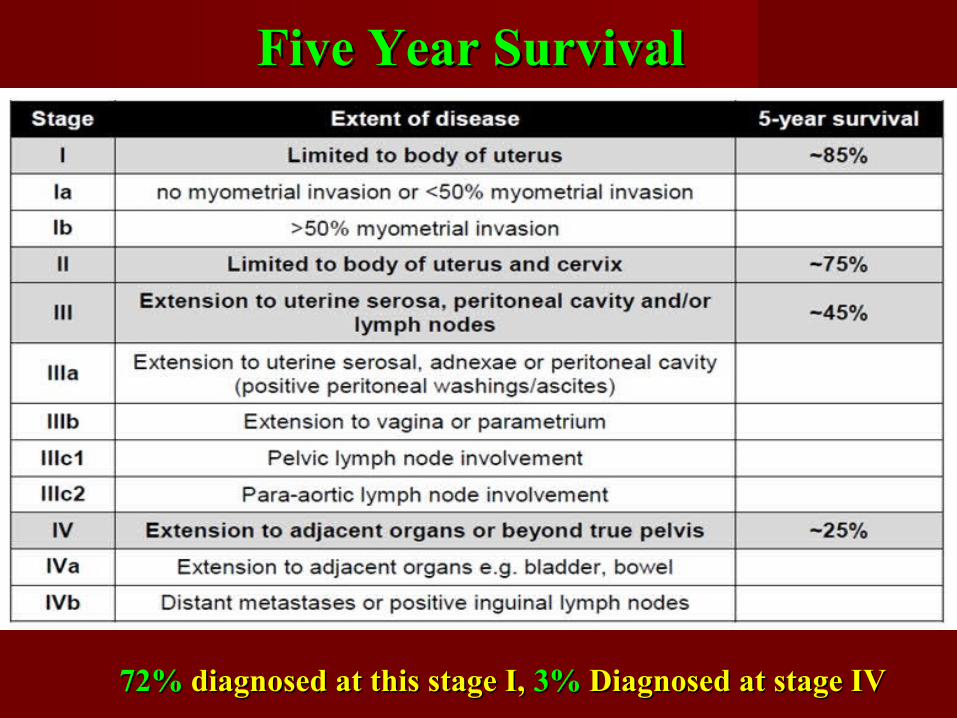
Five Year SurvivalFive Year Survival
72%72% diagnosed at this stage I, diagnosed at this stage I, 3%3% Diagnosed at stage IV Diagnosed at stage IV
Conclusions
Endometrial carcinoma is the commonest female
genital tract cancer.
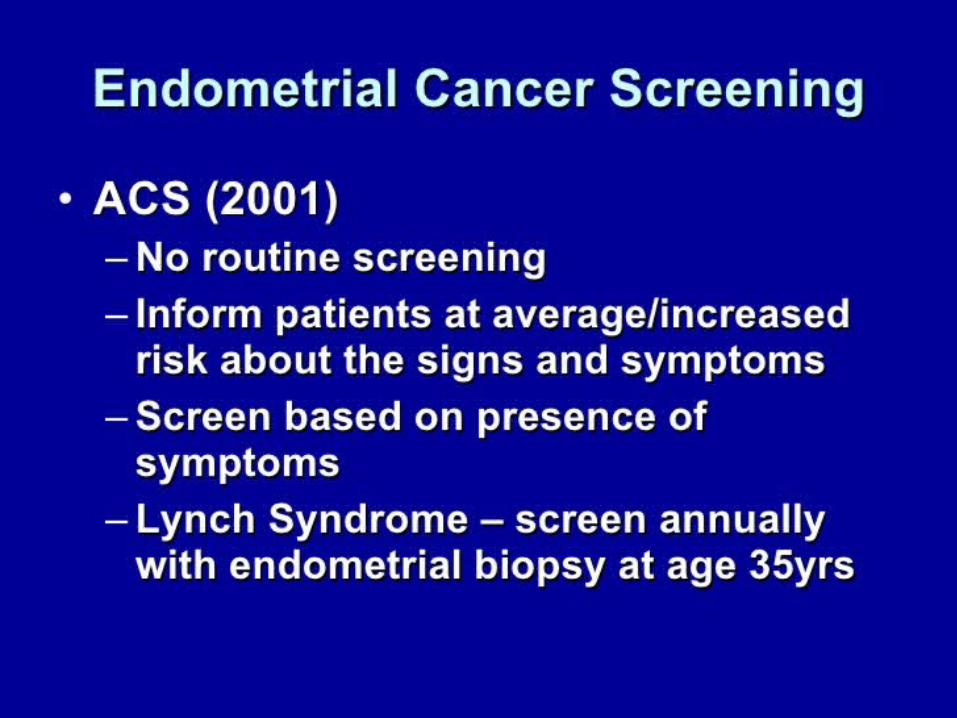
Routine screening for EC is not recommended.
However annual screening is recommended in
women at risk for hereditary nonpolyposis colorectal
cancer.
Endometrial carcinoma is a surgically staged disease.
Conclusions
The initial management of endometrial cancer should include total hysterectomy, bilateral salpingo-oophorectomy, and pelvic and para-aortic lymphadenectomy.
Primary radiotherapy or hormonal treatment may be recommmended in special situations.
Adjuvant radiotherapy and /or chemotherapy are recommended in patients with high risk for recurrence.
Conclusions
Endometrial carcinoma has the best prognosis
due to early presentation (PMB).
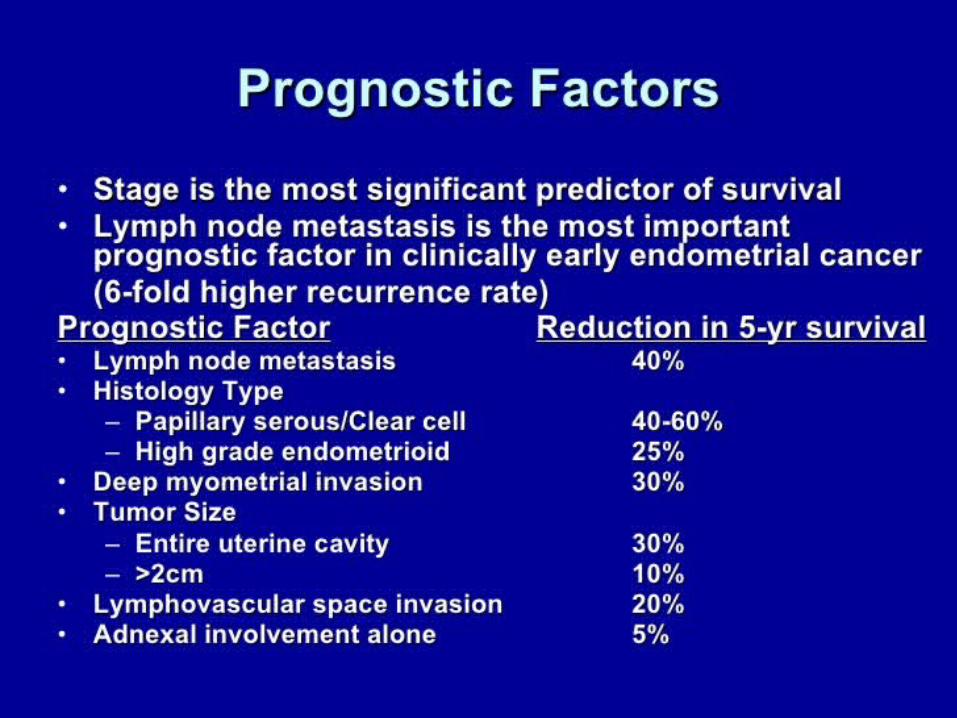
Disease stage is the most predictive factor for
survival.
Lymph node metastasis is the most predictive
factor for survival in early stage endometrial
carcinoma.

Related Documents