Endodermal Sinus Tumor of the Vagina and Cervix LARRY J. COPELAND, MD,* NOUR SNEIGE, MD,t NELSON G. ORDONEZ. MD,t KENNETH C. HANCOCK, MD,' DAVID M. GERSHENSON, MD,* PATTON B. SAUL, MD,' AND JOHN J. KAVANAGH, MD" This report describes six patients with endodermal sinus tumor of the vagina and cervix, a polypoid friable tumor whose clinical presentation in girls younger than age 3 years simulates the presentation of sarcoma botryoides. In four of the six patients, the referring diagnosis was sarcoma botryoides. Five patients were treated with excisional surgery, and all six with chemotherapy. One patient with pulmonary metastases maintained a complete clinical response to vincristine, actinomycin-D, and cyclophosphamide (VAC) for 11 months. This is the first report of such a response. One patient with a vaginal lesion remains clinically free of disease 2 years after local excision and 18 months of VAC chemotherapy. This is the first report of apparently successful therapy that allowed retention of childbearing potential. Four of the six patients have been disease-free from 2 to 23 years. After examining the world literature, it is concluded that a combination of chemotherapy and surgery offers a reasonable prospect of cure with a minimum of serious side effects. Cancer 55: 2558-2565, 1985. NDODERMAL SINUS TUMORS (EST) of the vagina E and cervix are rare and have been reported in a number of reviews and case reports as neoplasms of various terminology (Table 1). Since the early 197Os, when Nonis et d.' and Allyn et d2 published articles describing this neoplasm, it has been better recognized as a distinctive tumor. The controversy as to whether it is an extragonadal germ cell tumor or a tumor from mesonephric remnants, remains unresolved. Its clinical presentation is similar to that of sarcoma botryoides and, as reflected in this report, the evolution of therapy also bears resemblance to that of sarcoma botryoides. This article presents the experience of The University of Texas M. D. Anderson Hospital and Tumor Institute (MDAH) in managing this rare neoplasm. Materials and Methods Five cases of endodermal sinus tumor of the vagina, cervix, or uterus were registered at MDAH between 1944 and 1983. Because of the inconsistent terminology (Table 1) applied to this tumor, all patients younger than age 26 years with a carcinoma or sarcoma diagnosis for the vulva, vagina, cervix, and uterus were reviewed. A sixth case, diagnosed and managed at Wilford Hall Medical Center, San Antonio, Texas, was contributed to this series by one of the authors (K.H.). The histologic material from all case reports was reviewed by two of the authors (N.S. and N.O.). For each patient, they studied the slides of the primary tumor stained with hematoxylin and eosin (H & E) and periodic acid-Schiff (PAS) before and after diastase digestion. The average number of blocks of tumor tissue per case was nine. The following histologic features were evaluated: histologic growth pattern (reticular, festoon, polyvesicular vitelline, solid, or hepat~id),~.~ mitotic activity and the presence of PAS-positive, diastase-resis- tant hyaline globules. The amount of intracytoplasmic glycogen and the number of PAS-positive, diastase-resis- tant hyaline globules were rated on a scale of If to 3-t. For immunohistochemistry, 5-pm-thick sections of tumor tissue fixed in formaldehyde solution and embed- TABLE 1. Various Terminology Applied to Endodermal Sinus Tumors of the Vagina or Cervix From the Departments of *Gynecology and tPathology. The Uni- versity of Texas M. D. Anderson Hospital. and Tumor Institute at Houston, Houston, Texas. Address for reprints Larry J. Copeland, MD, Department of Gyne- cology, The University of Texas M. D. Anderson Hospital and Tumor Institute, 6723 Bertner Avenue, Houston, TX 77030. Accepted for publication June 8, 1984. Adenocarcinoma Clear cell adenocarcinoma Mesonephroma Mesonephric carcinoma Wolffian duct carcinoma Papillary adenocarcinoma Sarcoma, unclassified Embryonal rhabdomyosarcoma Sarcoma botryoides Alveolar rhabdomyosarcoma Endodermal sinus tumor Embryonal cell carcinoma Carcinoma of infant vagina 2558

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Endodermal Sinus Tumor of the Vagina and Cervix
LARRY J. COPELAND, MD,* NOUR SNEIGE, MD,t NELSON G. ORDONEZ. MD,t KENNETH C. HANCOCK, MD,' DAVID M. GERSHENSON, MD,* PATTON B. SAUL, MD,' AND JOHN J. KAVANAGH, MD"
This report describes six patients with endodermal sinus tumor of the vagina and cervix, a polypoid friable tumor whose clinical presentation in girls younger than age 3 years simulates the presentation of sarcoma botryoides. In four of the six patients, the referring diagnosis was sarcoma botryoides. Five patients were treated with excisional surgery, and all six with chemotherapy. One patient with pulmonary metastases maintained a complete clinical response to vincristine, actinomycin-D, and cyclophosphamide (VAC) for 11 months. This is the first report of such a response. One patient with a vaginal lesion remains clinically free of disease 2 years after local excision and 18 months of VAC chemotherapy. This is the first report of apparently successful therapy that allowed retention of childbearing potential. Four of the six patients have been disease-free from 2 to 23 years. After examining the world literature, it is concluded that a combination of chemotherapy and surgery offers a reasonable prospect of cure with a minimum of serious side effects.
Cancer 55: 2558-2565, 1985.
NDODERMAL SINUS TUMORS (EST) of the vagina E and cervix are rare and have been reported in a number of reviews and case reports as neoplasms of various terminology (Table 1). Since the early 197Os, when Nonis et d.' and Allyn et d 2 published articles describing this neoplasm, it has been better recognized as a distinctive tumor. The controversy as to whether it is an extragonadal germ cell tumor or a tumor from mesonephric remnants, remains unresolved. Its clinical presentation is similar to that of sarcoma botryoides and, as reflected in this report, the evolution of therapy also bears resemblance to that of sarcoma botryoides. This article presents the experience of The University of Texas M. D. Anderson Hospital and Tumor Institute (MDAH) in managing this rare neoplasm.
Materials and Methods
Five cases of endodermal sinus tumor of the vagina, cervix, or uterus were registered at MDAH between 1944 and 1983. Because of the inconsistent terminology (Table 1 ) applied to this tumor, all patients younger than age 26 years with a carcinoma or sarcoma diagnosis for the vulva, vagina, cervix, and uterus were reviewed. A sixth case, diagnosed and managed at Wilford Hall
Medical Center, San Antonio, Texas, was contributed to this series by one of the authors (K.H.).
The histologic material from all case reports was reviewed by two of the authors (N.S. and N.O.). For each patient, they studied the slides of the primary tumor stained with hematoxylin and eosin (H & E) and periodic acid-Schiff (PAS) before and after diastase digestion. The average number of blocks of tumor tissue per case was nine. The following histologic features were evaluated: histologic growth pattern (reticular, festoon, polyvesicular vitelline, solid, or h e p a t ~ i d ) , ~ . ~ mitotic activity and the presence of PAS-positive, diastase-resis- tant hyaline globules. The amount of intracytoplasmic glycogen and the number of PAS-positive, diastase-resis- tant hyaline globules were rated on a scale of I f to 3-t .
For immunohistochemistry, 5-pm-thick sections of tumor tissue fixed in formaldehyde solution and embed-
TABLE 1. Various Terminology Applied to Endodermal Sinus Tumors of the Vagina or Cervix
From the Departments of *Gynecology and tPathology. The Uni- versity of Texas M. D. Anderson Hospital. and Tumor Institute at Houston, Houston, Texas.
Address for reprints Larry J. Copeland, MD, Department of Gyne- cology, The University of Texas M. D. Anderson Hospital and Tumor Institute, 6723 Bertner Avenue, Houston, TX 77030.
Accepted for publication June 8, 1984.
Adenocarcinoma Clear cell adenocarcinoma Mesonephroma Mesonephric carcinoma Wolffian duct carcinoma Papillary adenocarcinoma Sarcoma, unclassified Embryonal rhabdomyosarcoma Sarcoma botryoides Alveolar rhabdomyosarcoma Endodermal sinus tumor Embryonal cell carcinoma Carcinoma of infant vagina
2558
No. I I EST OF THE VAGINA AND CERVIX - Cupeland et a/. 2559
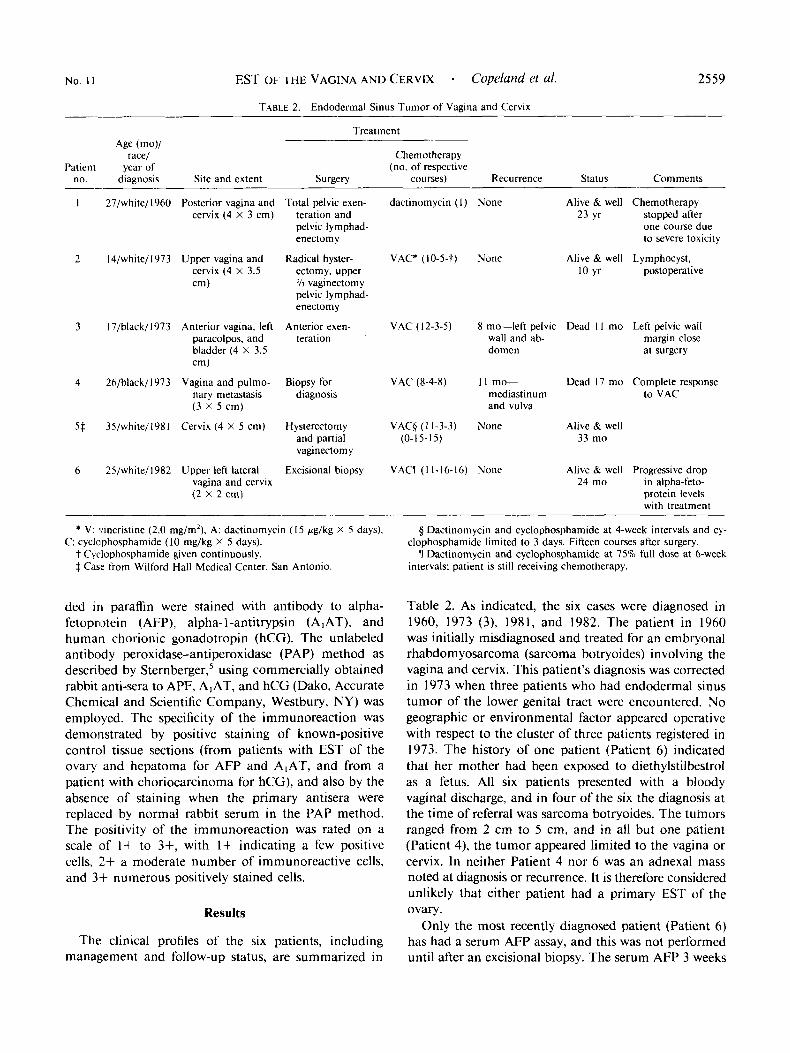
TABLE 2. Endodermal Sinus Tumor of Vagina and Cervix -- Treatment
Age (mo)/ race/ Chemotherapy
Patient year of (no. of respective no. diagnosis Site and extent Surgery courses) Recurrence Status Comments
I 27/white/1960 Posterior vagina and Total pelvic exen- dactinomycin ( I ) None Alive & well Chemotherapy cervix (4 X 3 cm) teration and 23 yr stopped after
~-
pelvic lymphad- one course due enectomy to severe toxicity
2 14/white/1973 Upper vagina and Radical hyster- VAC* (lo-5-t) None Alive & well Lymphocyst, cervix (4 X 3.5 ectomy, upper 10 yr postoperative
3 I7/black/
4 26/black/
973 Anterior vagina, left paracolpos, and bladder (4 X 3.5 cm)
973 Vagina and pulmo- nary metastasis (3 X 5 cm)
*/I vaginectomy pelvic lymphad- enectomy
Anterior exen- VAC (12-3-5) 8 mo-left pelvic Dead I I mo Left pelvic wall teration wall and ab- margin close
domen at surgery
Biopsy for VAC (8-4-8) 1 1 mo- Dead 17 mo Complete response diagnosis mediastinum to VAC
and vulva
5 $ 35/white/1981 Cervix (4 X 5 cm) Hysterectomy VAC# ( 1 1-3-3) None and partial (0- 15-1 5) vaginectomy
6 25/white/l982 Upper left lateral Excisional biopsy VAClT ( I 1-16-16) None vagina and cervix (2 X 2 cm)
Alive & well 33 mo
Alive & well Progressive drop 24 mo in alpha-feto-
protein levels with treatment
* V: vincristine (2.0 mg/m2), A: dactinomycin (15 Fg/kg X 5 days), C: cyclophosphamide (10 mg/kg X 5 days).
t Cyclophosphamide given continuously. $ Case from Wilford Hall Medical Center. San Antonio.
ded i n paraffin were stained with antibody to alpha- fetoprotein (AFP), alpha-I-antitrypsin (AIAT), and human chorionic gonadotropin (hCG). The unlabeled antibody peroxidase-antiperoxidase (PAP) method as described by Sternberger,' using commercially obtained rabbit anti-sera to APF, AIAT, and hCG (Dako, Accurate Chemical and Scientific Company, Westbury, NY) was employed. The specificity of the immunoreaction was demonstrated by positive staining of known-positive control tissue sections (from patients with EST of the ovary and hepatoma for AFP and A,AT, and from a patient with choriocarcinoma for hCG), and also by the absence of staining when the primary antisera were replaced by normal rabbit serum in the PAP method. The positivity of the immunoreaction was rated on a scale of I + to 3+, with 1+ indicating a few positive cells, 2+ a moderate number of immunoreactive cells, and 3+ numerous positively stained cells.
Results
The clinical profiles of the six patients, including management and follow-up status, are summarized in
rj Dactinomycin and cyclophosphamide at 4-week intervals and cy-
ll Dactinomycin and cyclophosphamide at 75% full dose at 6-week clophosphamide limited to 3 days. Fifteen courses after surgery.
intervals; patient is still receiving chemotherapy.
Table 2. As indicated, the six cases were diagnosed in 1960, 1973 (3), 1981, and 1982. The patient in 1960 was initially misdiagnosed and treated for an embryonal rhabdomyosarcoma (sarcoma botryoides) involving the vagina and cervix. This patient's diagnosis was corrected in 1973 when three patients who had endodermal sinus tumor of the lower genital tract were encountered. No geographic or environmental factor appeared operative with respect to the cluster of three patients registered in 1973. The history of one patient (Patient 6) indicated that her mother had been exposed to diethylstilbestrol as a fetus. All six patients presented with a bloody vaginal discharge, and in four of the six the diagnosis at the time of referral was sarcoma botryoides. The tumors ranged from 2 cm to 5 cm, and in all but one patient (Patient 4), the tumor appeared limited to the vagina or cervix. In neither Patient 4 nor 6 was an adnexal mass noted at diagnosis or recurrence. It is therefore considered unlikely that either patient had a primary EST of the ovary.
Only the most recently diagnosed patient (Patient 6) has had a serum AFP assay, and this was not performed until after an excisional biopsy. The serum AFP 3 weeks
2560 CANCER June I 1985 Vol. 55
TABLE 3. Histologic and lmmunohistochemical Findings in Six Patients With Endodermal Sinus Tumor of the Vagina
Immunohistochemistry
no. Dattern dobules Glvcoaen AFP A,AT hCG Patient Histologic Hyaline
1 Festoon, +++ ++ +++ -
solid, and reticular
2 Festoon, + +++ +++ + - reticular, and solid
- 3 Festoon and + +++ + - reticular
4 Festoon and ++ +++ + + -
solid
5 Festoonand ++t +++ + ++ solid
6 Festoon and + +++ + ++ -
reticular
-: absent; +: few or little amount; ++: moderate number or amount;
AFP: alpha-fetoprotein: A,AT: alpha-I-antitrypsin; hCG: human go- +++: numerous or abundant amount.
nadotropin.
postoperatively was 590 ng/ml, and when the next assay was performed 4 weeks later it was within normal range.
Grossly, the tumors were polypoid and protruded
into the vaginal lumen. The sizes of the greatest dimen- sion vaned from 2 cm to 5 cm. Cut surfaces were variegated, white-tan, and yellow. In the four patients in whom the uterus, ovaries and pelvic lymph nodes were examined. no tumor had spread to these sites.
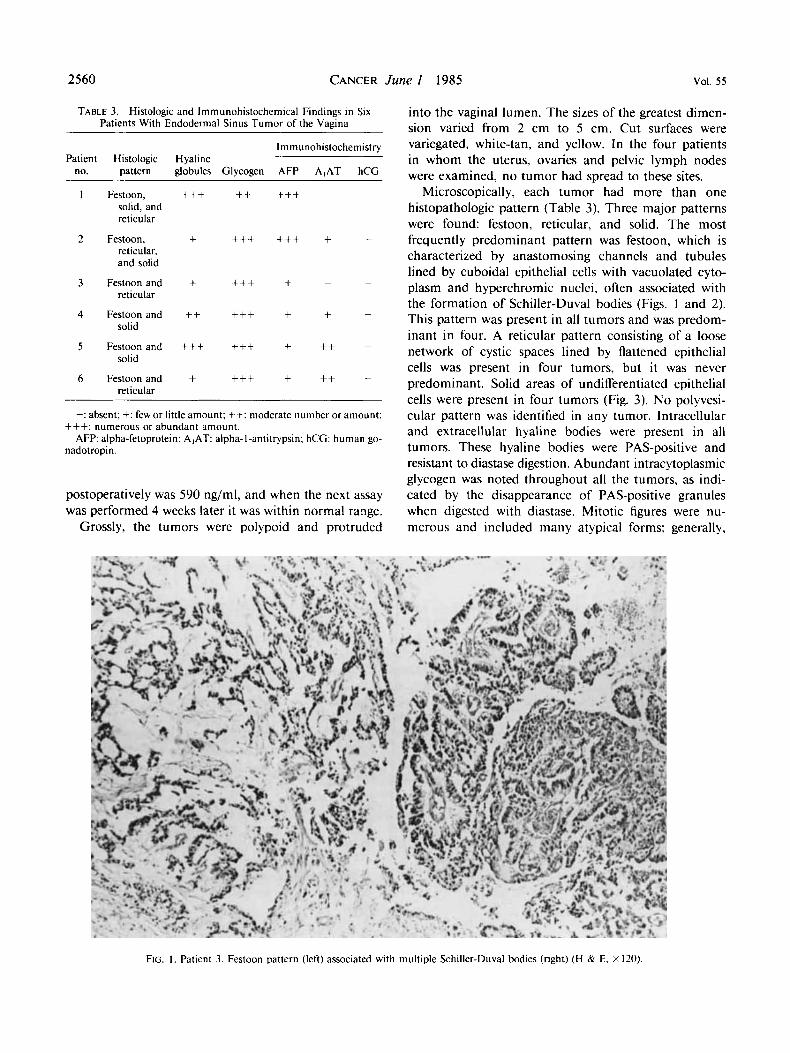
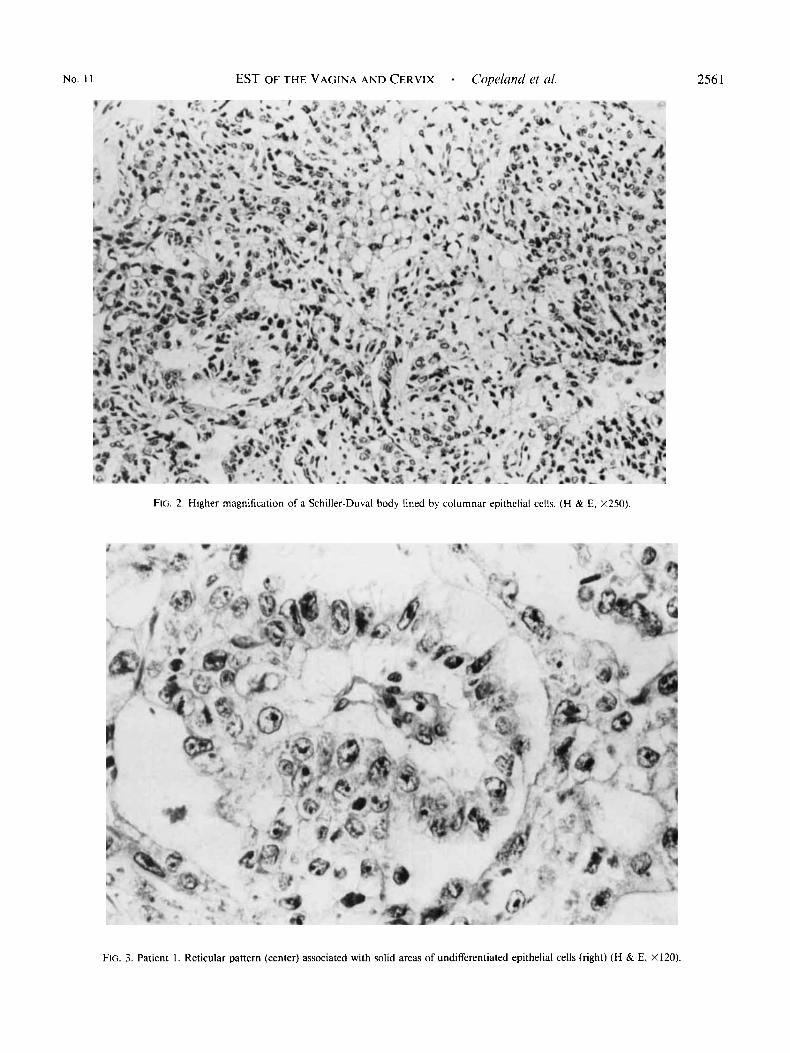
Microscopically, each tumor had more than one histopathologic pattern (Table 3). Three major patterns were found: festoon, reticular, and solid. The most frequently predominant pattern was festoon, which is characterized by anastomosing channels and tubules lined by cuboidal epithelial cells with vacuolated cyto- plasm and hyperchromic nuclei, often associated with the formation of Schiller-Duval bodies (Figs. 1 and 2). This pattern was present in all tumors and was predom- inant in four. A reticular pattern consisting of a loose network of cystic spaces lined by flattened epithelial cells was present in four tumors, but it was never predominant. Solid areas of undifferentiated epithelial cells were present in four tumors (Fig. 3). No polyvesi- cular pattern was identified in any tumor. Intracellular and extracellular hyaline bodies were present in all tumors. These hyaline bodies were PAS-positive and resistant to diastase digestion. Abundant intracytoplasmic glycogen was noted throughout all the tumors, as indi- cated by the disappearance of PAS-positive granules when digested with diastase. Mitotic figures were nu- merous and included many atypical forms; generally,
FIG. I . Patient 3. Festoon pattern (left) associated with multiple Schiller-Duval bodies (right) (H & E, X120).
No. I 1 EST OF THE VAGINA AND CERVIX . Copeland et al.
Flc;. 2 . Higher magnification of a Schiller-Duval body lined by columnar epithelial cells. (H & E, X250).
256 I
FIG. 3. Patient I . Reticular pattern (center) associated with solid areas of undifferentiated epithelial cells (right) (H & E, Xl20).
2562 CANCER June I 1985 Vol. 5 5
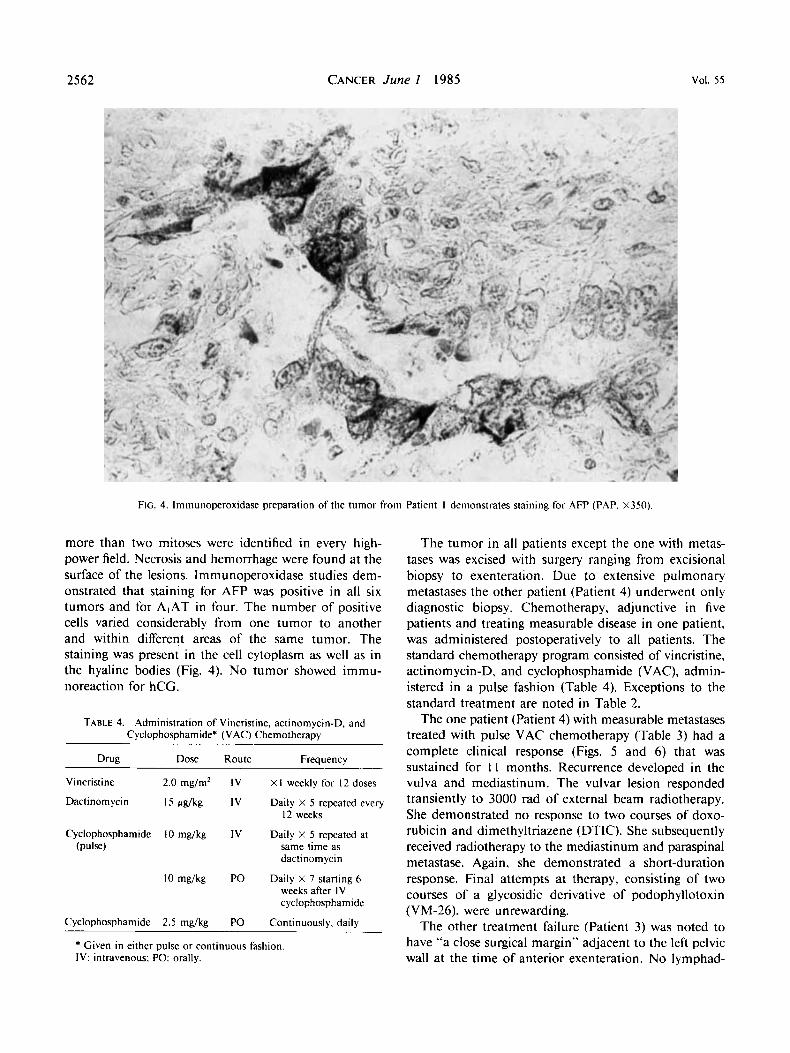
FIG. 4. lmmunoperoxidase preparation of the tumor from Patient I demonstrates staining for AFP (PAP, X350).
more than two mitoses were identified in every high- power field. Necrosis and hemorrhage were found at the surface of the lesions. Immunoperoxidase studies dem- onstrated that staining for AFP was positive in all six tumors and for AIAT in four. The number of positive cells varied considerably from one tumor to another and within different areas of the same tumor. The staining was present in the cell cytoplasm as well as in the hyaline bodies (Fig. 4). No tumor showed immu- noreaction for hCG.
TABLE 4. Administration of Vincristine, actinornycin-D, and Cycl~phosphamide~ (VAC) Chemotherapy
Drug Dose Route Frequency
Vincristine 2.0 mg/m2 IV X I weekly for 12 doses
Dactinorn ycin 15 pg/kg IV Daily X 5 repeated every
Cyclophosphamide 10 mg/kg IV Daily X 5 repeated at
12 weeks
(Pulse) same time as dactinom ycin
10 mg/kg PO Daily X 7 starting 6 weeks after IV cyclophosphamide
Cyclophosphamide 2.5 mg/kg PO Continuously, daily
* Given in either pulse or continuous fashion IV: intravenous; PO: orally.
The tumor in all patients except the one with metas- tases was excised with surgery ranging from excisional biopsy to exenteration. Due to extensive pulmonary metastases the other patient (Patient 4) underwent only diagnostic biopsy. Chemotherapy, adjunctive in five patients and treating measurable disease in one patient, was administered postoperatively to all patients. The standard chemotherapy program consisted of vincristine, actinomycin-D, and cyclophosphamide (VAC), admin- istered in a pulse fashion (Table 4). Exceptions to the standard treatment are noted in Table 2.
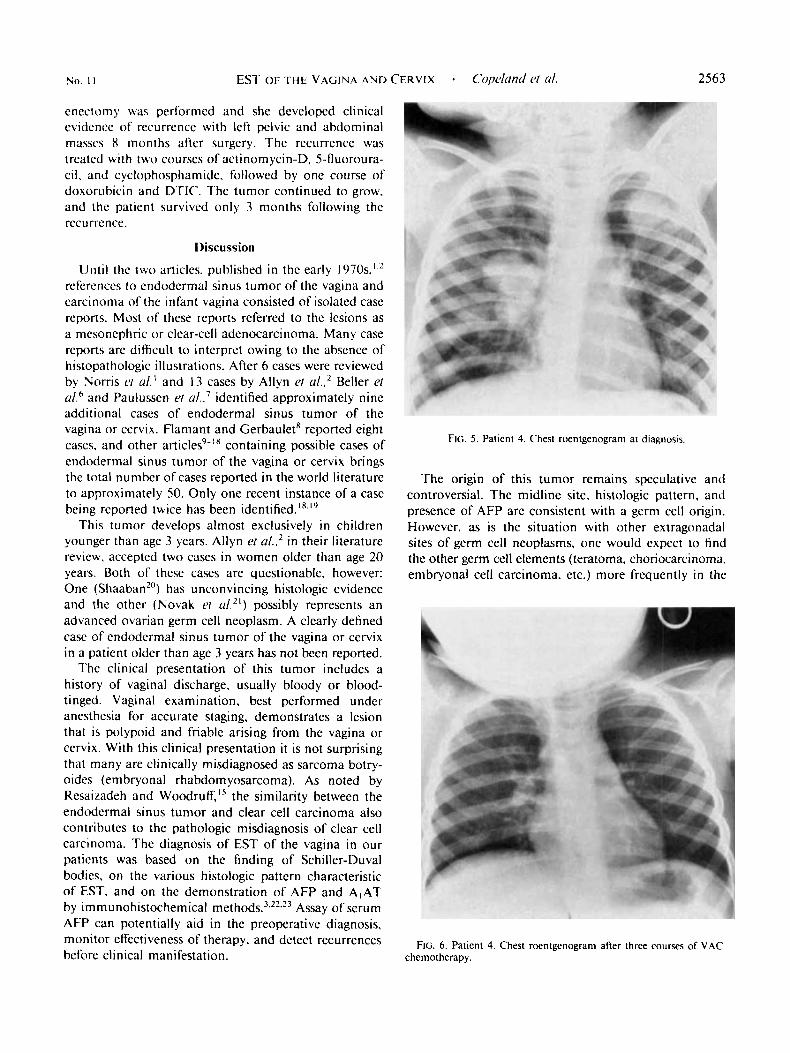
The one patient (Patient 4) with measurable metastases treated with pulse VAC chemotherapy (Table 3) had a complete clinical response (Figs. 5 and 6 ) that was sustained for 1 1 months. Recurrence developed in the vulva and mediastinum. The vulvar lesion responded transiently to 3000 rad of external beam radiotherapy. She demonstrated no response to two courses of doxo- rubicin and dimethyltriazene (DTIC). She subsequently received radiotherapy to the mediastinum and paraspinal metastase. Again, she demonstrated a short-duration response. Final attempts at therapy, consisting of two courses of a glycosidic derivative of podophyllotoxin (VM-26), were unrewarding.
The other treatment failure (Patient 3) was noted to have “a close surgical margin” adjacent to the left pelvic wall at the time of anterior exenteration. No lymphad-
2563
enectomy was performed and she developed clinical evidence of recurrence with left pelvic and abdominal massrs 8 months after surgery. The recurrence was treated with two courses of actinomycin-D, 5-lluoroura- cil. and cyclophosphamide. followed by one course of doxorubicin and DTIC. The tumor continued to grow. and the patient survived only 3 months following the recurrence.
Discussion
Until the two articles. published in the early 1970~, ’ .~ referenccs to endodermal sinus tumor of the vagina and carcinoma of the infant vagina consisted of isolated case reports. Most of these reports referred to the lesions as a mesonephric or clear-cell adenocarcinoma. Many case reports are difficult to interpret owing to the absence of histopathologic illustrations. After 6 cases were reviewed by Noms PI a/. ’ and 13 cases by Allyn P\ u I . . ~ Beller (’1 u/.6 and Paulussen (’1 a/..’ identified approximately nine additional cases of endodermal sinus tumor of the vagina or cervix. flamant and Gerbaulet* reported eight cases. and other article^^-'^ containing possible cases of endodermal sinus tumor of the vagina or cervix brings the total number of cases reported in the world literature to approximately 50. Only one recent instance of a case being reported twice has been identified.”.”
This tumor develops almost exclusively in children younger than age 3 years. Allyn el a/..’ in their literature review. accepted two cases in women older than age 20 years. Both of these cases are questionable. however: One (Shaaban”) has unconvincing histologic evidence and the other (Novak el u1.21) possibly represents an advanced ovarian germ cell neoplasm. A clearly defined case of endodermal sinus tumor of the vagina or cervix in a patient older than age 3 years has not been reported.
The clinical presentation of this tumor includes a history of vaginal discharge. usually bloody or blood- tinged. Vaginal examination, best performed under anesthesia for accurate staging, demonstrates a lesion that is polypoid and friable arising from the vagina or cervix. With this clinical presentation it is not surprising that many are clinically misdiagnosed as sarcoma botry- oides (embryonal rhabdomyosarcoma). As noted by Resaizadeh and Woodruff,” the similarity between the endodermal sinus tumor and clear cell carcinoma also contributes to the pathologic misdiagnosis of clear cell carcinoma. The diagnosis of EST of the vagina in our paticnts was based on the finding of Schiller-Duval bodies, on the various histologic pattern characteristic of E.ST. and on the demonstration of AFP and A,AT by i m m u nohistoc hem ical met hod^.',^^.'^ Assay of serum AFP can potentially aid in the preoperative diagnosis. monitor eff‘ectiveness of therapy, and detect recurrences before clinical manifestation.
FIG. S . Patient 4. Chest roentgenogram at diagnosis.
The origin of this tumor remains speculative and controversial. The midline site. histologic pattern, and presence of AFP are consistent with a germ cell origin. However. as is the situation with other extragonadal sites of germ cell neoplasms, one would expect 10 tind the other germ cell elements (teratoma. choriocarcinoma. embryonal cell carcinoma, etc.) more frequently in the
FIG. 6. Patient 4. Chest roentgenogram after three courses of VAC chemotherapy.

2564 CANCER June 1 1985 Vol. 5 5
TABI.E 5.
Age at diagnosis
Reported 5-Year Survivors of Endodermal Sinus Tumor of the Vagina or Cervix --
Source (date) (mo) Tumor si7e & site Treatment Status Comments
Allyn et a/.’(1971) 1 1 3-4 cm posterior Hysterectomy, Disease-free Pelvic lymph node recurrence vagina vaginectomy, and two 7 years ( 5 mo) treated with pelvic
courses of chemotherapy lymphadenectomy, 4800 rad external beam radiation. and 7 courses of dactinomycin over 22 m o
Nonis et a/.’ ( 1970) 12 2 cm upper lateral Hysterectomy, Disease-free (Case 5) vagina vaginectomy, and 6 years
Dewhurst and 8 2 cm upper posterior Extended hysterectomy. Disease-free Ferreira’’ (1981) vagina bilateral salpingo- 7 years
radiotherapy
oophorectomy. upper ’14 vaginectomy, and pelvic I ymphadenectom y
lower genital tract, occasionally admixed with the en- dodermal sinus tumor pattern. Such is not the case.
Of the estimated 50 cases of EST reported in the world literature. the tumor site is not clearly defined in approximately 3070 to 40%; 10% to 15% of the tumors originate in the cervix and 5070 in the vagina. Endoder- ma1 sinus tumor of the vulva and corpus is exceedingly rare.24-27
Although the majority of reports reflect unsuccessful treatment programs, apparent cures have been described with a number of treatment approaches, including sur- gery alone,” surgery plus radiotherapy,’ and surgery plus chemotherapy.2 Our four patients who remain alive and well all were treated with surgery followed by chemotherapy. The extent of surgery in our patients has vaned drastically from pelvic exenteration to simple excision. Patient I , diagnosed in 1963 as having a sarcoma botryoides, had a total pelvic exenteration, the recommended therapy in that era. The most recent experience (Patients 5 and 6) suggests that a combination of “excisional” surgery and postoperatively combination chemotherapy may offer satisfactory results.
Although this tumor has demonstrated sensitivity to radiation, the role of radiation therapy is unclear. Siege1 et a1.28 reported a patient free of disease at 2 years after treatment with 6000 rad. Other reports reflect that radiotherapy alone is not curative, albeit the therapy described would not meet today’s radiotherapy stan- dard~.~’ -~’ Uns~ccessful’~~ and successful’ outcomes have been reported with programs combining surgery and radiation. Flamant and Gerbaulet’ reported that the use of radiotherapy in conjunction with surgery and che- motherapy produced a 75% cure rate at 3 years follow- up. Their general treatment approach was to administer chemotherapy (methotrexate, actinomycin-D, cyclo- phosphamide. vincristine, and doxorubicin) initially,
and to follow this with either radiation alone or a combination of surgery and radiation.
Four of our five patients with disease limited to the pelvis were living and disease-free at or beyond 2 years. This suggests that radiotherapy is not essential in the treatment. Avoiding radiation in these young patients is desirable in order to preserve ovarian function and avoid possible radiation effects on developing bone structure.
Preoperative chemotherapy may minimize the extent of surgery required. The results with the most recent patient in this report (Patient 6 ) suggest that small localized tumors have the potential of successful treat- ment while preserving childbearing potential.
In addition to the chemotherapy regimen of Flamant and Gerbaulet, other apparently successful adjunctive chemotherapy programs (actinomycin-D’,2 and actino- mycin-D, doxorubicin. vincrinstine, and cyclophospha- mide6) have been reported. Five of the six patients in our review received VAC chemotherapy. The complete response in a patient with pulmonary metastases clearly demonstrated the activity of this regimen.
Recurrent disease after initial therapy is a major problem: only one treatment success has been reported.2 In our two patients who developed recurrence, second- line chemotherapy caused no tumor reduction and only short-term palliation.
Of the 50 cases reported in world literature, survival information is available for about 35. The median length of survival of these patients is in the vicinity of 1 1 months. An additional 10% to 15% of patients die within the next 2 years. If patients show no clinical evidence of disease at 2 years, it is estimated that only 10% will have a recurrence, most of them within the following 12 months. In addition to our two patients, only three patients with endodermal sinus tumor of the vagina have been reported as surviving 5 years (Table 5) .

No. I 1 EST OF THE VAGINA A N D CERVIX - Copeland et a/. 2565
Schoneich ' ' also reported a possible 5-year survivor: however. the lack of a histologic confirmation of this tumor puts the diagnosis in question
The dismal prognosis reported for endodermal sinus tumor of the lower female genital tract is overly pessi- mistic. A combination of chemotherapy and surgery offers a reasonable chance of cure with a minimum of life-long side effects.
REFERENCFS
I . Norris HJ. Bagley GP. Taylor HB. Carcinoma of the infant vagina: A distinctive tumor. .4rch fa/hol 1970: 90:473-479.
2. Allyn DL, Silverberg SG. Salzberg AM. Endodermal sinus tumor of the vagina: Report of a case with 7-year survival and literature review of so-called "mesonephromas." Cancer I97 1 : 27: I23 1- 1238.
3. Teilum G. Special Tumors of Ovary and Testis and Related Extragonadal Lesions: Comparative Pathology and Histological Iden- tification. ed. 2. Philadelphia: J. B. Lippincott. 1976; 32-1 18.
4. Prat J, Bhan AK, Dickersin RB, Robboy AJ. Scully RE. Hepatoid yolk s ic tumor of the ovary (endodermal sinus tumor with hepatoid differentiation): A light microscopic. ultrastructural, and immunohis- tocheniical study of seven cases. Canwr 1982: 50:2355-2368.
5 . Sternberger LA. Immunocytochemistry. ed. 2. New York: John Wiley & Sons, 1979; 104-169.
6. Beller FK, Nienhaus H, Schmundt-v.Gizycki B. Schellong G, Runte H. Schmandt W. Endodermal germ cell carcinoma (endodermal sinus lumor) of the vagina in infant girls. J Cancer Rcc Clin Oncol 1979; '94:295-306.
7. F'aulussen F. Maintz EJ, Gropp A. Hensen SD. Das mesonephro- gene Karzinom in Kindesalter. (irhrirt.rchr/fe Fruiienhnilkd 197 1 ; 3 I : 228-240.
8. Flamant F. Gerbaulet A. Traitment conservateur des tumeurs vulvo vaginales malignes de I'enfant par une approche multidisciplinaire (i I'exclusion des adenocarcinomes a cellules clairs). Brill C'anc-er (Puri.7) 198 1: 68: 154- 157.
9. Pollack RS. Taylor HC. Carcinoma of the cervix during the first two decades of life. ,4171 .I O h w Gynecol 1947; 53:135-141.
10. Royes DA. Hardie M. Agnew AM. Carcinoma of the cervix in an incant. A m .I Ohstrt Gynecol 1956; 72:1353-1356.
I 1 . Shoneich R. Vaginalkarzinom bei einem 2jahrigne Kinde: bisher 12-Jahresheilung. Rodiohiol Radiolhrr 1965; 6:97- 103.
I ? . Gibson AAM. Embryonal carcinoma of vagina in infancy (Abstr). .4rch Dic Child 1973; 48:163.
13. ltoh T, Shirai T. Naka A. Matsumoto S. Yolk sac tumor and
a-fetoprotein: Clinicopathological study of four cases. Gunn 1974: 65: 215-222.
14. Grumbach Y, Piussan C. Remond A. Audehert M. Minh H-N. Requet C. Un nouveau cas de tumeur du sinus endodermique du vagin chez le nourrizzon. Ann fedialr (faris) 1976; 23207-2 I I .
15 . Rezaizadeh MM. Woodruff JD. Endodermal sinus tumor of the vagina. G,vnreol Oncol 1978; 6:459-463.
16. Norgaard-Pedersen B, Lundberg CJ, Laursen AM, Hagerstranti 1. Infantile vagina tumour with alpha-fetoprotein synthesis. .4( , / ( / Po////// hficrohiid Immimol Scand [A] 1979: 87:2?3-226.
17. Gallippi G. Carrozza G, Martines F, Raimondi E. Picardi P. Stigliano V. II tumore del seno endodermico a localizzazione vaginal.
18. Underhill R. Neoplasm of the vagina in infants: Two cases. Pro(, R Soc Med 1975; 68:229-23 I .
19. Dewhurst J. Ferreira HP. An endodermal sinus tumour of the vagina in an infant with seven year survival. Br J Oht/i,/ (;,wrwl 1981: R8:859-862.
20. Shaaban M M . Primary adenocarcinoma of the vagina of rne- sonephric pattern. Am1 N Z .I 0h.uet Gynaecol 1970; 10:55-58.
21. Novak E, Woodruff JD. Novak ER. Probable mesonephric origin of certain female genital tumors. Am J Oh.c/et Gvnc*co/ 1954; 68: 1222- 1242.
22. Gonzalez-Crussi F. The human yolk sac and yolk sac (endodermal sinus) tumors: A review. fro.vpect ferliot Porhol 1979; 5: 179-2 I I .
23. Palmer PE. Wolfe HJ. lmmunohistochemical localization of oncodevelopmental proteins in human germ cell and hepatic tumors. .I Histochem C~~iochern 1978: 26:523-53 I .
24. Ungerleider RS, Donaldson SS, Warnke RA, Wilbur JR. En- dodermal sinus tumor: The Stanford experience and first reported case arising in the vulva. Canciv 1978; 41:1627-1634.
25. Krishnamurthy SC. Sampat MR. Endodermal sinus (yolk sac) tumor of the vulva in a pregnant female. Gynecol 0nc.d 1'981: I I : 379-382.
26. Dudley AG. Young RH, Lawrence WD, Schuuy RE. Endodermal sinus tumor of the vulva in an infant. Ohstel Cvnocol 1983; 6l:76S- 79s.
27. Pilen S. Martinelli G. Serra L. Bassocchi F. Endodermal sinus tumor arising in the endometrium. Oh.r/et Gvnwol 1980: 56:3Y 1-396.
28. Siege1 HA, Sagerman R. Berdon WE. Wigger HJ. Mesonephric adenocarcinoma of the vagina in a 7-month-old infant simulating sarcoma botryoides. successful control with supervoltage radiotherapy. J fediatr Siirg 1970: 5:468-470.
29. Lovegren E. Carcinoma vaginae in zwelten Lehensjahre. 4 c . t ~ fal,diatr I 93 I ; 10:37 I :378.
30. Ortmann KK. Uber Carcinoma der weihlichen Genitalien hei Kindern. Krehsfor.rchztng 1932; 37:283-292.
31. Hoge RH. Benn V A . Carcinoma of the vulva and vagina i n infancy. Am J Ohtet Gynecol 1943: 46:286-290.
fa/h/dogica 1980; 72:427-543.
Related Documents











