British Journal of Obstetrics and Gynaeco1og.v October 1984, Vol. 9 1, pp. 948-967 Endocrinology of human parturition : a review ANNA-RIITTA FUCHS & FRITZ FUCHS Department of Obstetrics and Gynecology, Cornell University Medical College, 525 East 68th Street, New York, New York 10021, USA Summary. The existing data on the hormonal factors involved in human parturition indicate that the steroid hormones, progesterone and the oestrogens, play only a facilitatory role in the initiation of labour. A definite role for fetal adrenal steroids in this process has yet to be established, and they too may serve only a facilitating function. The stimulation of the uterine muscle during labour results from an interaction of oxytocin and prostaglandin (PG) F,. Recent evidence suggests that oxytocin is most important for the initial phase of labour, whereas increased synthesis of PGF,, is essential for the progression of labour. The role of PGE, remains unclear, but this PG may play an important role in the ripening of the cervix which in turn is essential for successful parturi- tion. The finding of maximal oxytocin receptor concentrations in the myometrium in labour adds strong support to the notion that oxytocin is the trigger for uterine contractions. The factors which control oxytocin receptor formation are therefore important; this may be one of the processes where the steroids play a crucial role. Oxytocin is also one of the stimuli that increase uterine PG synthesis; the coupling of oxytocin receptor occupancy and PG synthetase activity in uterine tissues may be another crucial factor in the mechanism of labour. The formation of gap junctions between the myometrial cells also seems essential for the synchronization and progression of myometrial activity. We propose, therefore, that the co-ordinating of oxytocin receptor formation, P G synthesis and gap junction formation is a key to the initiation and main- tenance of human labour. The fetus may fulfil such a co-ordinating role through its influence on placental oestrogen production, through mechanical distention of the uterus, and through its secretion of neuro- hypophysial hormones and other stimulators of PG synthesis. During parturition the function of the different parts of the reproductive tract must be integrated to assure the expulsion of the fetus without compromising the perfusion of the placenta and the circulation of the fetus. The timely and proper function of the myometrium and the cervix obviously are of great importance and evidence is accumulating for an important role for the fetal membranes and the uterine decidua as sources of prostaglandins that may be required to maintain labour and prepare the cervix. The ovaries should also be considered because in pregnant women they are the main and perhaps only source of relaxin; the latter is emerging as a potentially important factor in preparation of the birth canal for parturition. We do not know whether the different tissues are under the control of a common factor or are functionally interdepen- dent, one part triggering the other in a chain reac- tion. It is our purpose to review the factors that, we currently believe, participate in the process of 948

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

British Journal of Obstetrics and Gynaeco1og.v October 1984, Vol. 9 1, pp. 948-967
Endocrinology of human parturition : a review
ANNA-RIITTA FUCHS & FRITZ FUCHS Department of Obstetrics and Gynecology, Cornell University Medical College, 525 East 68th Street, New York, New York 10021, USA
Summary. The existing data on the hormonal factors involved in human parturition indicate that the steroid hormones, progesterone and the oestrogens, play only a facilitatory role in the initiation of labour. A definite role for fetal adrenal steroids in this process has yet to be established, and they too may serve only a facilitating function. The stimulation of the uterine muscle during labour results from an interaction of oxytocin and prostaglandin (PG) F,. Recent evidence suggests that oxytocin is most important for the initial phase of labour, whereas increased synthesis of PGF,, is essential for the progression of labour. The role of PGE, remains unclear, but this PG may play an important role in the ripening of the cervix which in turn is essential for successful parturi- tion. The finding of maximal oxytocin receptor concentrations in the myometrium in labour adds strong support to the notion that oxytocin is the trigger for uterine contractions. The factors which control oxytocin receptor formation are therefore important; this may be one of the processes where the steroids play a crucial role. Oxytocin is also one of the stimuli that increase uterine PG synthesis; the coupling of oxytocin receptor occupancy and PG synthetase activity in uterine tissues may be another crucial factor in the mechanism of labour. The formation of gap junctions between the myometrial cells also seems essential for the synchronization and progression of myometrial activity. We propose, therefore, that the co-ordinating of oxytocin receptor formation, P G synthesis and gap junction formation is a key to the initiation and main- tenance of human labour. The fetus may fulfil such a co-ordinating role through its influence on placental oestrogen production, through mechanical distention of the uterus, and through its secretion of neuro- hypophysial hormones and other stimulators of PG synthesis.
During parturition the function of the different parts of the reproductive tract must be integrated to assure the expulsion of the fetus without compromising the perfusion of the placenta and the circulation of the fetus. The timely and proper function of the myometrium and the cervix obviously are of great importance and evidence is accumulating for an important role for the fetal membranes and the uterine decidua as sources of prostaglandins that may be required to maintain labour and prepare the cervix. The ovaries should
also be considered because in pregnant women they are the main and perhaps only source of relaxin; the latter is emerging as a potentially important factor in preparation of the birth canal for parturition. We do not know whether the different tissues are under the control of a common factor or are functionally interdepen- dent, one part triggering the other in a chain reac- tion.
It is our purpose to review the factors that, we currently believe, participate in the process of
948
Endocrinology of human parturition 949
Under the influence of oestrogens, the membrane potential rises and in the rat uterus maximal resting potentials are recorded during oestrogen treatment (Jung 1964). When the membrane potential is high, the threshold for excitation is increased and the membrane is therefore more stable and the muscle mechanically quiescent (Fuchs 1978; Downing & Porter 1980). Contrary to common belief, uterine muscle is quiescent when the blood levels of oestrogen are raised, whereas acute withdrawal of oestrogens is associated with a marked increase in the genera- tion of spontaneous myometrial activity. Under physiological conditions, uterine quiescence is observed during the pro-oestrus surge of oestrogens in rats and during the preparturient surge of oestrogens in pregnant rats (Fuchs 1978). The withdrawal effect is observed in late oestrus and metoestrus (Ishikawa & Fuchs 1978a) and during the early postpartum period, when strong spontaneous contractions accompany the beginning of uterine involution (Fuchs & Poblete 1970).
Oestrogens also participate in the formation of gap junctions between adjoining myometrial cells (Garfield et al. 1980); there is good correlation between gap junction formation and an increase in circulating oestrogens, at least in the uterus of the rat or guinea-pig (Puri & Garfield 1982). These junctions provide low resistance pathways for the conduction of electrical activity from cell to cell and thus promote synchronization of uterine activity. During pro-oestrus, the electrical and mechanical activities of the rat uterus in ICUO are very rapidly conducted along the uterus and therefore are well synchronized, whereas during dioestrus these activities are much less syn- chronized (Ishikawa & Fuchs 1978a). During pregnancy, irregular asynchronous activity prevails in all animal species studied, whereas a good synchronization and rapid propagation of contraction waves are observed just before and during parturition. The electromyographic recordings made in women during labour also indicate increasing synchronization with advancing labour (Wolfs & Van Leeuwen 1979). We have shown that in the rat the development of synchronous activity is a prerequisite for parturi- tion to proceed; unpropagated, localized contrac- tions do not result in the expulsion of live young regardless of the intensity of the contractions (Fuchs 1978).
A further oestrogen effect is the formation of membrane receptors for certain oxytocic agents.
parturition at term. Recent data have made it possible to formulate a hypothesis which incor- porates the known facts, but it must be stressed that not all the factors involved in the final steps of myometrial activation and cervical softening have been elucidated as yet.
Myometrial function
The myometrial cells are similar to vascular smooth muscle cells in regard to contractile proteins, structural organization, and the regula- tion of the contraction-relaxation cycle by intra- cellular Ca2'. The two types of muscle cells resemble each other also in the relative paucity of sarcoplasmic reticulum and sarcolemmal vesicles which sequester Ca2+. Consequently, both types of muscle cells are much more dependent on extracellular Ca2+ than are skeletal muscle and even cardiac muscle. Similar mechanisms are involved in the transport of Ca2+ across the cell membrane of the vascular and myometrial cells; they consist of voltage-dependent Ca2+ chan- nels, ATP-dependent Ca2+ pumps, Na+-Ca2+ exchange mechanisms and receptor-controlled Ca2+ gates.
The myometrium is, however, unique in regard to the extent of ovarian hormonal control over the biosynthesis of contractile proteins and other cellular constituents of importance for the excitability of the cells and the propagation of excitation from cell to cell. In contrast to vascular smooth muscle, myometrial muscle cells have a sparse innervation which is further reduced during pregnancy (Sjoberg 1967) and the regula- tion of the contractile function of the myo- metrium is largely humoral or depends on intrinsic myogenic factors.
Role of ovarian hormones
Oestrogens
Animal studies have made it clear that oestrogens, particularly oestradiol- 17p, are essen- tial for the induction of protein synthesis in the uterus, including the structural and contractile proteins and the enzymes that provide energy for the contractile process. Oestrogen also affects the molecular constituents of the cell membrane that regulate the cell permeability for sodium, potassium, and chloride ions which are largely responsible for the resting potential of the myo- metrial cells and their electrical excitability.
950 A:R. FUChs & F. FUchs
Most important are the oxytocin receptors (Soloff 1975; Nissenson et al. 1978: Fuchs e f al. 1983h. c) and a-adrenergic receptors (Roberts et al. 1981). Increase in receptor numbers lowers the threshold for stimulation and increases the response to a given dose by recruiting more units to contract, thus increasing the pharmacological excitability of the myometrium. The effect of oestrogens is selective; thus the receptors for prostaglandin (PG) E, and F, do not appear to be increased by oestrogex (Wakeling & Wyngarden 1974), and the number of 0- adrenergic receptors is decreased (Roberts et al. 198 1).
Oestrogens stimulate the synthesis of numerous other enzymes and cellular house- keeping products, including many proteolytic, collagenolytic and lysosomal enzymes. Oestrogens also appear to stimulate prosta- glandin synthesis in a rather complex fashion that requires interaction with progesterone (Castracane I% Jordan 1975).
Oestrogens thus influence myornetrial function in several ways: they increase the capacity of the uterus to contract and promote the synchroniza- tion of the contractile units, and they render the control of myornetrial contractions more precise by suppressing locally generated spontaneous activity while increasing the excitability by humoral agents.
Progesterone
The effect of progesterone on the myometrium is two-fold; it suppresses the action of oestrogens by inhibiting the replenishment of cytosolic oestrogen receptors and it exerts a direct effect on the biosynthetic processes of the uterus via its own cellular receptors (Clark & Peck 1979). Uterine protein synthesis is maintained under the influence of progesterone and the accumulation of total protein is increased, probably because the synthesis of oestrogen-induced proteolytic enzymes is suppressed; the proteins synthesized under the influence of progesterone are partially different, including some progesterone-specific proteins.
The contractile capacity is maintained under the influence of progesterone, as indicated by the development of tension in the electrically stimulated uterus of progesterone-treated rabbits or rats (Csapo 1956).
The influence of progesterone on the excitability of the myometrium differs in various
species. In rabbits, progesterone acts syner- gistically with oestrogens to maintain high membrane potential and membrane stability which results in suppression of spontaneous activity (Goto & Csapo 1959; Kao & Nishiyama 1964). In rats, on the other hand, progesterone lowers the membrane potential in oestrogen- pretreated animals (Jung 1964); this is associated with the generation of increased spontaneous activity (Fuchs 1978). Likewise, in the rhesus monkey increased uterine activity coincides with the highest plasma progesterone levels (Taylor et al. 1983). In rats the conduction velocity of electrical impulses is reduced, and the propagation of contractions along the uterus is impaired (Marshall 1962). The contractions elicited in various parts of the uterus therefore remain asynchronous and localized (Csapo & Takeda 1965; Fuchs 1978).
The electrical and mechanical characteristics of the progesterone-dominated uterus in these animal species may be due to the paucity or even total absence of gap junctions, demonstrated in rats and guinea-pigs by Garfield et al. (1980, 1982). The inhibition of gap junction formation by progesterone is probably the main reason why progesterone withdrawal is essential for the delivery of live young in so many species. The control of the gap junctions found in human myo- metrium after the onset of labour has yet to be elucidated (Garfield & Hayashi 1981).
Progesterone also inhibits the formation of oxytocin receptors, at least in the uterus of rats and rabbits (Fuchs et al. 19836, c ; Nissenson et al. 1978): and the formation of b-receptors is increased (Roberts et al. 198 1). Activation of the latter receptors leads to the relaxation of the myo- metrial cells, as in vascular smooth muscle, and this is the basis for tocolytic therapy with b- mimetics in preterm labour. PGF, and PGE, receptors, on the other hand, are not inhibited by progesterone; on the contrary, they appear to be increased, at least in rats, hamsters, and rhesus monkeys (Wakeling & Wyngarden 1974). The finding that progesterone enhances the myo- metrial response to PGE,, PGE, and PGF,, in rats (Fuchs 1974) corroborates these findings. Since these prostanoids stimulate the human myometrium even in midgestation, progesterone also appears to promote prostaglandin receptor formation in human myometrium.
Progesterone action in the human uterus differs from that in the rat and rabbit at least in one important aspect: it does not inhibit the forma-
Endocrinology of human parturition 95 1
tion of oxytocin receptors, as is the case in rabbits and rats.
Relaxin
Relaxin is an ovarian hormone which is produced in the corpora lutea of pregnancy (Weiss et al. 1977), but is found also in the decidua (Bigazzi ef a/. 1980). Relaxin is of considerable importance for the process of parturition in species such as guinea-pig, mouse, rat, pig and possibly also sheep, cow and mare, though the effect is on the pelvic ligaments. Its importance for human parturition is still unclear, although some evidence for a possible role in cervical ripening (MacLennan et al. 1980) and rupture of membranes (Koay et al. 1983) has recently been presented. In rodent uteri, relaxin has a clear inhibitory effect on spontaneous contractions. as demonstrated both in vitro and in vivo (Wiqvist 1959; Porter et al. 1979). Relaxin may well act synergistically with oestrogen in causing the preparturient myometrial quiescence, since a surge of relaxin is observed at about the same time as the preparturient rise in plasma oestrogens (Sherwood et al. 1980). The effects of relaxin on human myometrium are inconsistent, perhaps due to the fact that only porcine relaxin has been available in pure form for physiological studies. Human relaxin might differ significantly from the porcine hormone in its configuration.
Role of adrenal hormones
Cortisol
No specific action on myometrial contractility has been reported for the glucocorticoids, although they must be of importance for general housekeeping functions of the myometrial cells. Adrenalectomized pregnant rats maintained on saline give birth to their young without apparent difficulty at normal term. Fetal corticoid produc- tion may partially compensate for the lack of maternal glucocorticoids, but the rise in maternal adrenal secretion usually associated with parturi- tion is, at least, not essential. Conversely, long- term treatment with dexamethasone does not influence the onset or duration of labour in pregnant women (Gennser et a/. 1977). This is in contrast to the findings in sheep, goat, and cow, where fetal cortisol production is of prime importance for the onset of labour (Liggins 198 1). In these species, the effect of cortisol on myo-
metrial function is an indirect one, achieved through the induction of 17-OH hydroxylase activity which results in the suppression of either placental (sheep) or ovarian (goat) progesterone production and a concomitant stimulation of oestrogen secretion. These changes in steroid secretion are associated with increased PGF,, production in uterine tissues.
Fetal cortisol production increases also in monkeys (Jaffe et a/. 1978) and man (Murphy 1982), although the rise is less conspicuous than in sheep and goats and does not seem to play the same crucial role for the onset of parturition. In women, the transplacental passage of gluco- corticoids is extensive and maternally derived cortisol, and especially cortisone, account for a large proportion of the glucocorticoids in the fetal circulation even in late gestation (Murphy et al. 1974).
Dihydro-epiandrosterone (DHEA) and oestrogens
It is interesting that uterine activity in pregnant rhesus monkeys shows a diurnal pattern (Ducsay et al. 1983; Taylor et a/. 1983), coinciding with variations in fetal adrenal activity (Challis et al. 1980). The greatest activity coincides with the peak of DHEA sulphate and progesterone in the fetal circulation, and the circadian variation in uterine activity disappears after fetal death (Taylor et al. 1983).
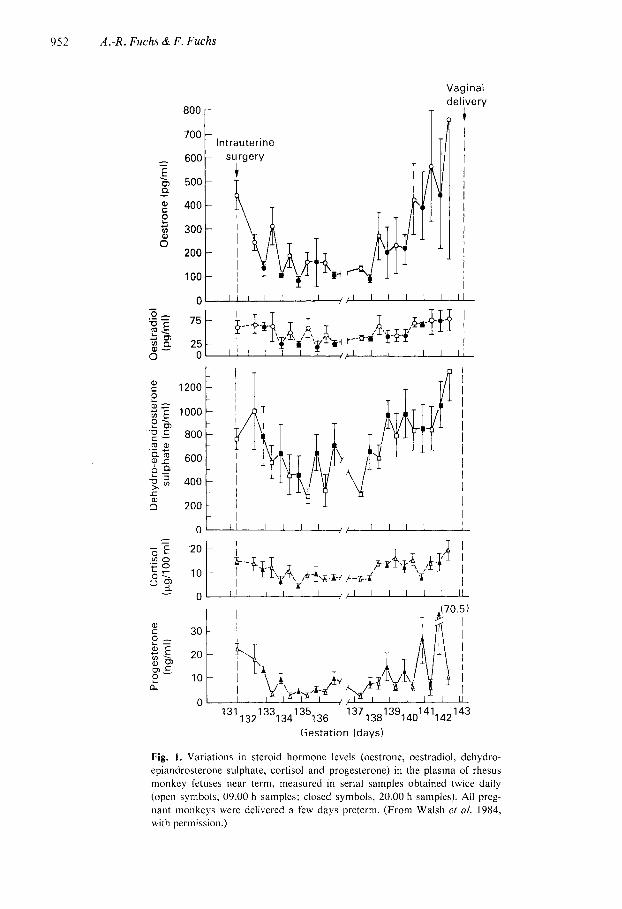
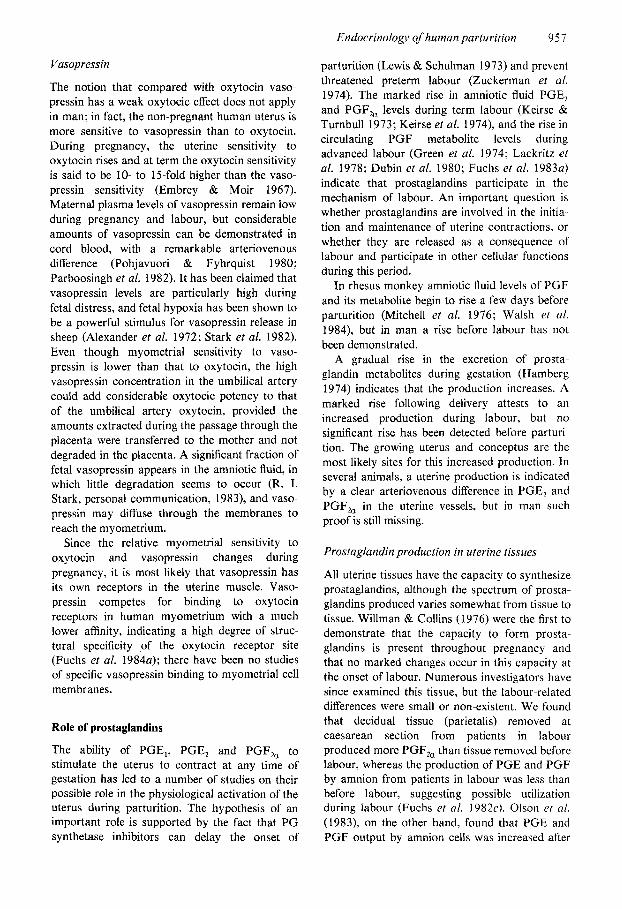
The increase in amniotic fluid prostaglandins seen before spontaneous or ACTH-induced delivery in the rhesus monkey may be related to an increase in fetal oestrogens (Mitchell et al. 1976). A recent study by Walsh et al. (1984) indicates that the concentration of oestrone and to a lesser degree DHEA sulphate in fetal plasma increases progressively during the last 3 4 days preceding delivery, with no fall in progesterone levels (Fig. I). Amniotic fluid oestrone levels showed a rising trend but were not significantly raised until the day of delivery; PGF metabolite levels in amniotic fluid rose in parallel.
In man, synthesis of the fetal oestrogen precursor, DHEA, increases during the latter half of gestation (Parker et al. 1982). An increasing proportion is converted to oestriol (EJ, raising the ratio of E, to oestrone (E,) plus oestradiol (E,) in the maternal circulation from about the 34th week onwards (Tulchinsky et al. 1972). Despite their rapid conjugation, unconjugated oestrone and oestradiol levels rise in the fetal circulation
952 A.-R. Fuchs & F. Fuchs
Vaginal deli,very
800
700
- 600 E 31 500 a
400 e Z 300
200
-
-
8
100
0
Intrauterine surgery
t T T
t I I I I I I I I I I
10
137 1381 39,401 411421 43 31 i 3 2 l 3 3 ~ 3 4 l 3 5 ~ 36
Gestation (days)
Fig. 1. Variations in steroid hormone levels (oestrone, oestradiol, dehydro- epiandrosterone sulphate, cortisol and progesterone) in the plasma of rhesus monkey fetuses near term, measured in serial samples obtained twice daily (open symbols, 09.00 h samples: closed symbols, 20.00 h samples). All preg- nant monkeys were delivered a few days preterm. (From Walsh et 01. 1984, with permission.)

Endocrinology ofhuman parturition 953
and relatively large amounts are present at term (Tulchinsky 1973). The possible significance of fetal oestrogens for uterine PG synthesis in human pregnancy is not clear.
Catecholamines
The innervation of the uterus is predominantly sympathetic: the nerve fibres contain mainly nor- adrenaline, but dopamine- and serotonin- containing fibres have also been detected in the cervix and vagina (Owman et a/. 1967). The distribution of the nerve fibres is uneven; oviduct, cervix and vagina have a dense innervation, while the uterine corpus and fundus have a relatively sparse distribution. The content of neurotrans- mitters is regulated by ovarian hormones; oestrogen increases and progesterone decreases the uterine content of noradrenaline (Sjoberg 1968a). Similar changes occur during pregnancy, and after an initial increase in early pregnancy, histochemically-demonstrable catecholamines virtually disappear from the corpus and fundus of the uterus, whereas the nerve fibres around the cervix and vagina as well as oviduct and mesenteric arteries retain their neurotransmitter content (Sjoberg 19686). Neural activity, there- fore, cannot have much influence on myometrial function at the time of parturition.
The uterus contains a- and p receptors and adrenaline secreted from the adrenal medulla and taken up from the systemic circulation can there- fore influence uterine function. Beta-mimetic drugs, given after the onset of labour either at term or preterm, are able to inhibit uterine contractions. Since adrenaline mainly stimulates B-adrenergic receptors, endogenous adrenaline can fulfil a similar function. However, the administration of p-blocking drugs has little effect on uterine contractions, suggesting that under normal conditions the influence of endogenous 0- mimetics on uterine function is small.
The fetal adrenal medulla. in contrast to the cortex, remains histologically and biochemically relatively immature during most of fetal life (Artal 1980). but para-aortic, extra-adrenal chromaffin tissues which can be demonstrated early in fetal life contain significant amounts of noradrenaline and dopamine (Hervonen 197 I ) . The adrenal medulla contains measureable noradrenaline by 15 weeks. but the concentration remains low during fetal life. According to Niemineva & Pekkarinen (1952), noradrenaline accounts for approximately threc-quarters of the total
catecholamine content of human fetal adrenal glands regardless of gestational age. The placenta degrades catecholamines very effectively and little labelled noradrenaline injected into the mother is recovered unchanged in the fetus (Saarikoski 1974). Fetal catecholamines are probably degraded too and a direct role for fetal catechola- mines appears unlikely.
Since fetal catecholamines are excreted in urine into the amniotic fluid they may have an etrect on the fetal membranes. The content of adrenaline, noradrenaline and dopamine in the amniotic fluid rises with advancing gestation (Ben Jonathan & Munsick 1980; Divers et al. 1981), probably reflecting the maturation of the fetal adrenal gland. Adrenaline can function as a cofactor in PG synthesis and stimulates the PGF, output of the rat uterus (Ishikawa & Fuchs 19786). It is conceivable that it may have a similar effect on PGF, production of amniotic cells.
The output of fetal catecholamines increases during labour (Eliot et al. 1980) but like maternal catecholamines, the increase appears to be a consequence rather than cause of labour (Zuspan 1970).
Role of oxytocin
Plasma levels
Oxytocin is the most potent known endogenous uterotonic agent. It is capable of eliciting contrac- tions of the human uterus at term in concentra- tions calculated to be as low as 3-10 pU/ml (5-20 pmol/l) (Saameli 1963). Measurements in our laboratory of plasma oxytocin levels during induction of labour with oxytocin have confirmed these estimates which were calculated on the basis of infusion rates, estimated plasma volumes and the half-life for oxytocin in the circulation (Fuchs et al. 1983a). During infusions of 1 to 2 mU/min, plasma levels were 10-12 pU/ml, with infusions of 4-6 mU/rnin the levels rose to 20-30 pU/min (Table 1). At term, a rate of 1-2 mU/min suffices to stimulate contractions and 4-6 mU/min can maintain labour in most patients. Considering these low levels, it is not surprising that it has been difficult to demonstrate the presence of oxytocin in maternal blood during labour.
The difficulties are compounded by the short half-life of oxytocin, estimated to be about 3 min, and the spurt-like pattern of release which necessitates frequent serial sampling. The failure of some investigators (Sellers et a!. 1981) to detect any rise in plasma oxytocin during labour,
954
Table 1. Plasma oxytocin levels in serial samples from 17 women in spontaneous and 15 in oxytocin-induced labour at term0
A.-R. Fuchs & F. Fuchs
Spontaneous labour Oxytocin-induced labour
Cervical Plasma Infusion Plasma dilatation oxytocin rate oxytocin
(cm) (pU/ml n (mU/min) ( N m O n
Before labour
During labour (2 l l . S ( l . 8 4 ) 16 Before 10.3 (2.9) 15
(4 28.1 (4.5)* 14 1-3 12.6(3.8) 8 4-6 27.6 (4.6)* 13 4-6 29.2 (6.5)* 12 7-9 25.6 (3.9)* 19 7-9 35.0(5.9)* 16 10 27.3 (2. I)* 7 10-16 65.5 (13 .5 ) * 10
aThe results, shown as means (SEM), are arranged according to the cervical dilatation or the infusion rate at the time of sampling. Adapted from Fuchs et al. (1983~). *Significantly different from values before the onset of labour.
or a rise only during the expulsive phase (Leake et al. 198 l), has led to conflicting opinions about the role of endogenous oxytocin in the initiation and maintenance of human labour. Measurements in our laboratory on serial samples, taken during the first stage of spontaneous labour at term, indicated that the levels were similar to those observed during infusion rates of 4-6 mU/min, and significantly higher than in serial samples collected in control patients not in labour (Fuchs et al. 1983a) (Table 1). During the second stage of labour, oxytocin levels rise further according to most authors (cf. review by Dawood 1983), suggesting a Ferguson-type reflex release in response to vaginal distention. Our observations that oxytocin levels during spontaneous labour rarely exceed those observed during infusion rates of 4-6 mU/min agree with those reported by Wolfs & Van Leeuwen (1979) who studied the effect of oxytocin on the electromyographic recordings of human uterine activity. Only at infusion rates of <5 mU/min were the patterns similar to those recorded in spontaneous labour.
Receptor levels
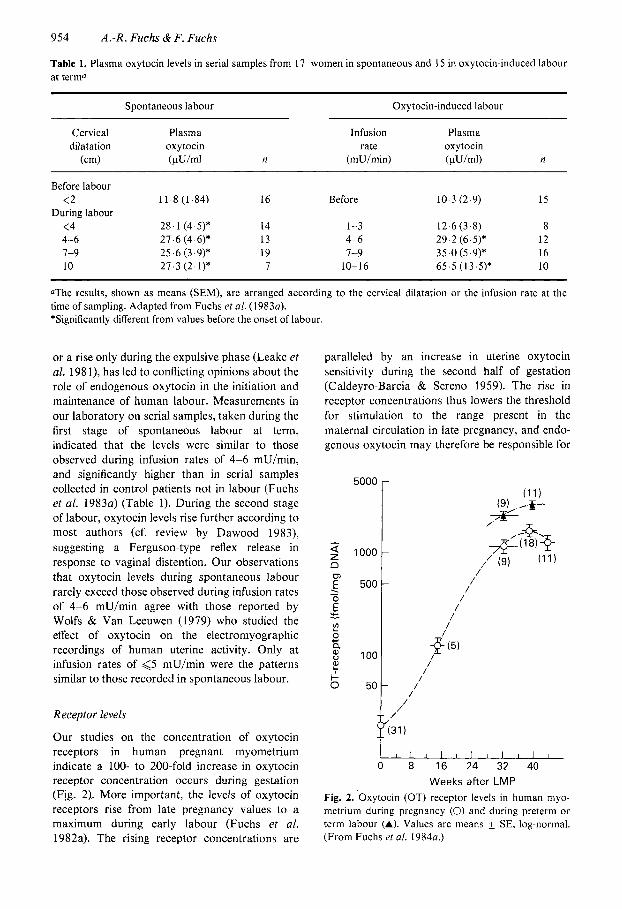
Our studies on the concentration of oxytocin receptors in human pregnant myometrium indicate a 100- to 200-fold increase in oxytocin receptor concentration occurs during gestation (Fig. 2) . More important, the levels of oxytocin receptors rise from late pregnancy values to a maximum during early labour (Fuchs et al. 1982a). The rising receptor concentrations are
paralleled by an increase in uterine oxytocin sensitivity during the second half of gestation (Caldeyro-Barcia & Sereno 1959). The rise in receptor concentrations thus lowers the threshold for stimulation to the range present in the maternal circulation in late pregnancy, and endo- genous oxytocin may therefore be responsible for
5000
- 2 1000
E
n E" 500 . -
'c L?
4- a 8 100 ?? $ 0 50
I l l l l l l l l l l 8 16 24 32 40
Weeks after LMP Fig. 2. Oxytocin (OT) receptor levels in human myo- metrium during pregnancy (0) and during preterm or term labour (A). Values are means SE, log-normal. (From Fuchs et al. 1984a.)
Endocrinology of human parturition
L T
955
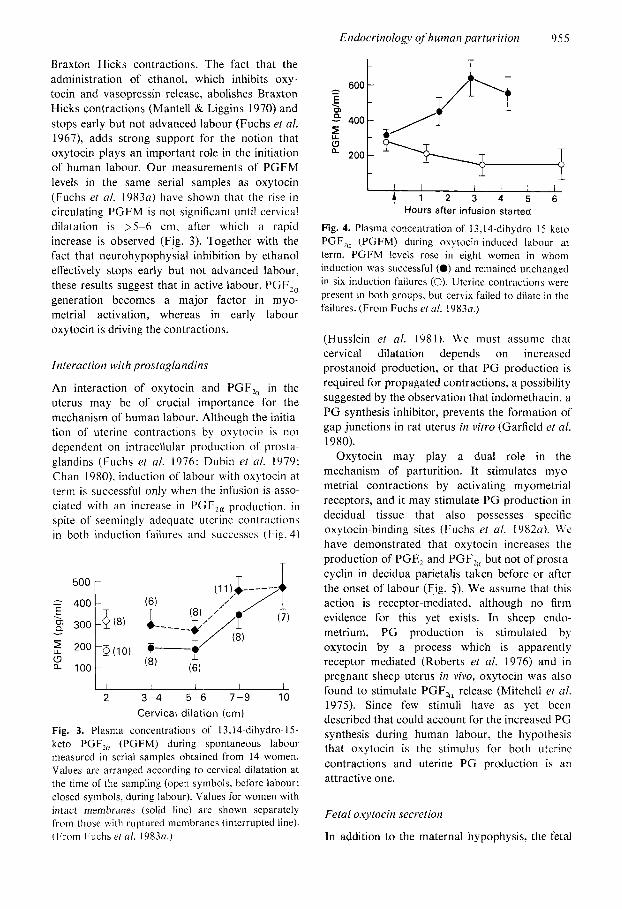
Braxton Hicks contractions. The fact that the administration of ethanol, which inhibits oxy- tocin and vasopressin release, abolishes Braxton Hicks contractions (Mantell & Liggins 1970) and stops early but not advanced labour (Fuchs et al. 1967), adds strong support for the notion that oxytocin plays an important role in the initiation of human labour. Our measurements of PGFM levels in the same serial samples as oxytocin (Fuchs et a/. 19830) have shown that the rise in circulating PGFM is not significant until cervical dilatation is >5-6 cm, after which a rapid increase is observed (Fig. 3). Together with the fact that neurohypophysial inhibition by ethanol effectively stops early but not advanced labour, these results suggest that in active labour, PGF,, generation becomes a major factor in myo- metrial activation, whereas in early labour oxytocin is driving the contractions.
Interaction with prostaglandins
An interaction of oxytocin and PGF, in the uterus may be of crucial importance for the mechanism of human labour. Although the initia- tion of uterine contractions by oxytocin is not dependent on intracellular production of prost:i- glandins (Fuchs et a/. 1976: Dubin et al. 1979: Chan 1980). induction of labour with oxytocin at term is successful only when the infusion is asso- ciated with an increase in l’GF2, production. i t1
spite of seemingly adequate utcrine contractions in both induction failures and succcsscs (f~.ig. 4 )
1 rnn
7 + T
2 3-4 5-6 7-9 10 Cervical dilation (cm)
Fig. 3. Plasma concentrations of 13,l.l-dihydro- 15- keto PGF,, (PGFM) during spontaneous labour measured in serial samples obtained from 14 women. Values are arranged according to cervical dilatation at the time of the sampling (open symbols, before labour; closed symbols. during labour). Values for women with intact membranes (solid line) are shown separately lion1 those with ruptured membranes (interrupted line). (I:rom Fuchs et al. 19830.)
5 400
200
T /l ‘t .Y I
T /I
6 ! I 2 3 4 5 6
Hours after infusion started
Fig. 4. Plasma concentration of 13,14-dihydro- 15-keto PGF,, (PGFM) during oxytocin-induced labour at term. PGFM levels rose in eight women in whom induction was successful (0) and remained unchanged in six induction failures (0). Uterine contractions were present in both groups, but cervix failed to dilate in the failures. (From Fuchs ef al. 19830.)
(Husslein et a/ . 1981). We must assume that cervical dilatation depends on increased prostanoid production, or that PG production is required for propagated contractions, a possibility suggested by the observation that indomethacin, a PG synthesis inhibitor, prevents the formation of gap junctions in rat uterus in vitro (Garfield el al. 1980).
Oxytocin may play a dual role in the mechanism of parturition. It stimulates myo- metrial contractions by activating myometrial receptors, and it may stimulate PG production in decidual tissue that also possesses specific oxytocin-binding sites (Fuchs et a/. 19820). \i c have demonstrated that oxytocin increases the production of PGE, and PGF, but not of prosta- cyclin in decidua parietalis taken before or after the onset of labour (Fig. 3) . We assume that this action is receptor-mediated, although no firm evidence for this yet exists. In sheep endo- metrium, PG production is stimulated by oxytocin by a process which is apparently receptor mediated (Roberts et al. 1976) and in pregnant sheep uterus in vivo, oxytocin was also found to stimulate PGF, release (Mitchell et al. 1975). Since few stimuli have as yet been described that could account for the increased PG synthesis during human labour, the hypothesis that oxytocin is the stimulus for both uterine contractions and uterine PG production is an attractive one.
Fetal oxytocin secretion
In addition to the maternal hypophysis, the fetal
956 A:R. Fuchs & F. Fuchs
D M A D M A D M A
PG E PGF 6-0xo-PG F,
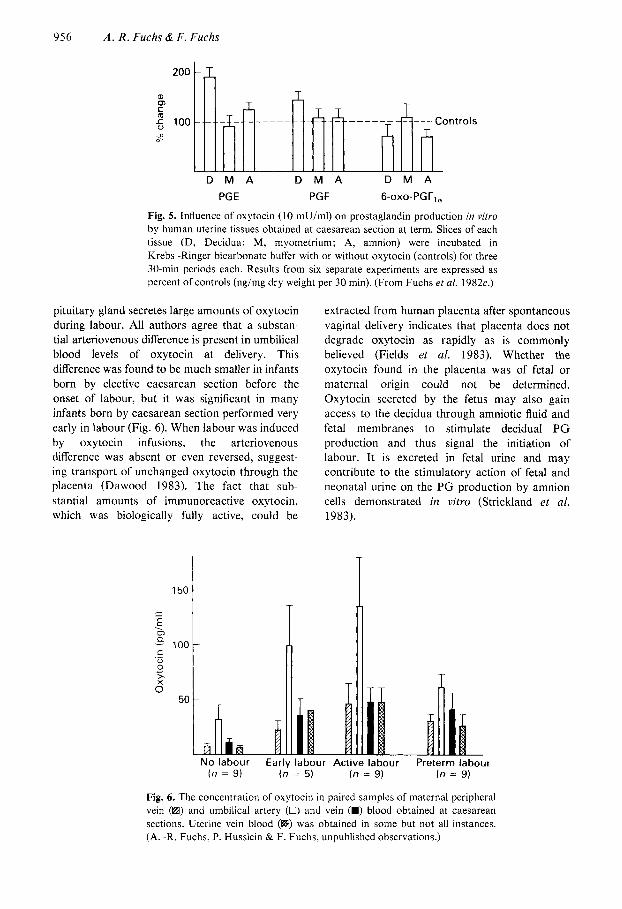
Fig. 5 . Influence of oxytocin (10 mU/ml) on prostaglandin production in vitro by human uterine tissues obtained at caesarean section at term. Slices of each tissue (D, Decidua; M, myometrium; A, amnion) were incubated in Krebs-Ringer bicarbonate buffer with or without oxytocin (controls) for three 30 min periods each. Results from six separate experiments are expressed as percent of controls (ng/mg dry weight per 30 min). (From Fuchs ef al. 1982c.)
pituitary gland secretes large amounts of oxytocin during labour. All authors agree that a substan- tial arteriovenous difference is present in umbilical blood levels of oxytocin at delivery. This difference was found to be much smaller in infants born by elective caesarean section before the onset of labour, but it was significant in many infants born by caesarean section performed very early in labour (Fig. 6). When labour was induced by oxytocin infusions, the arteriovenous difference was absent or even reversed, suggest- ing transport of unchanged oxytocin through the placenta (Dawood 1983). The fact that sub- stantial amounts of immunoreactive oxytocin, which was biologically fully active, could be
I 150
extracted from human placenta after spontaneous vaginal delivery indicates that placenta does not degrade oxytocin as rapidly as is commonly believed (Fields et al. 1983). Whether the oxytocin found in the placenta was of fetal or maternal origin could not be determined. Oxytocin secreted by the fetus may also gain access to the decidua through amniotic fluid and fetal membranes to stimulate decidual P G production and thus signal the initiation of labour. It is excreted in fetal urine and may contribute to the stimulatory action of fetal and neonatal urine on the PG production by amnion cells demonstrated in vitro (Strickland e t al. 1983).
50
No labour Earlv labour Active labour Preterm labour
T
( n = 9) (n := 5 ) (n = 9) (n = 9)
Fig. 6. The concentration of oxytocin in paired samples of maternal peripheral vein (B) and umbilical artery (0) and vein (m) blood obtained at caesarean sections. Uterine vein blood (B) was obtained in some but not all instances. (A. -R. Fuchs. P. Husslein & F. Fuchs, unpublished observations.)
Endocrinology of human parturition 95 7
Vasopressin
The notion that compared with oxytocin vaso- pressin has a weak oxytocic effect does not apply in man; in fact, the non-pregnant human uterus is more sensitive to vasopressin than to oxytocin. During pregnancy, the uterine sensitivity to oxytocin rises and at term the oxytocin sensitivity is said to be 10- to 15-fold higher than the vaso- pressin sensitivity (Embrey & Moir 1967). Maternal plasma levels of vasopressin remain low during pregnancy and labour, but considerable amounts of vasopressin can be demonstrated in cord blood, with a remarkable arteriovenous difference (Pohjavuori & Fyhrquist 1980; Parboosingh et al. 1982). It has been claimed that vasopressin levels are particularly high during fetal distress, and fetal hypoxia has been shown to be a powerful stimulus for vasopressin release in sheep (Alexander et al. 1972; Stark et al. 1982). Even though myometrial sensitivity to vaso- pressin is lower than that to oxytocin, the high vasopressin concentration in the umbilical artery could add considerable oxytocic potency to that of the umbilical artery oxytocin, provided the amounts extracted during the passage through the placenta were transferred to the mother and not degraded in the placenta. A significant fraction of fetal vasopressin appears in the amniotic fluid, in which little degradation seems to occur (R. I. Stark, personal communication, 1983), and vaso- pressin may diffuse through the membranes to reach the myometrium.
Since the relative myometrial sensitivity to oxytocin and vasopressin changes during pregnancy, it is most likely that vasopressin has its own receptors in the uterine muscle. Vaso- pressin competes for binding to oxytocin receptors in human myometrium with a much lower affinity, indicating a high degree of struc- tural specificity of the oxytocin receptor site (Fuchs et al. 1984a); there have been no studies of specific vasopressin binding to myometrial cell membranes.
Role of prostaglandins
The ability of PGE,, PGE, and PGF, to stimulate the uterus to contract at any time of gestation has led to a number of studies on their possible role in the physiological activation of the uterus during parturition. The hypothesis of an important role is supported by the fact that P G synthetase inhibitors can delay the onset of
parturition (Lewis & Schulman 1973) and prevent threatened preterm labour (Zuckerman et al. 1974). The marked rise in amniotic fluid PGE, and PGF, levels during term labour (Keirse & Turnbull 1973; Keirse et al. 1974), and the rise in circulating PGF metabolite levels during advanced labour (Green et al. 1974; Lackritz et al. 1978; Dubin et al. 1980; Fuchs et al. 1983a) indicate that prostaglandins participate in the mechanism of labour. An important question is whether prostaglandins are involved in the initia- tion and maintenance of uterine contractions, or whether they are released as a consequence of labour and participate in other cellular functions during this period.
In rhesus monkey amniotic fluid levels of P G F and its metabolite begin to rise a few days before parturition (Mitchell et al. 1976; Walsh et al. 1984), but in man a rise before labour has not been demonstrated.
A gradual rise in the excretion of prosta- glandin metabolites during gestation (Hamberg 1974) indicates that the production increases. A marked rise following delivery attests to an increased production during labour, but no significant rise has been detected before parturi- tion. The growing uterus and conceptus are the most likely sites for this increased production. In several animals, a uterine production is indicated by a clear arteriovenous difference in PGE, and PGF, in the uterine vessels, but in man such proof is still missing.
Prostaglandin production in uterine tissues
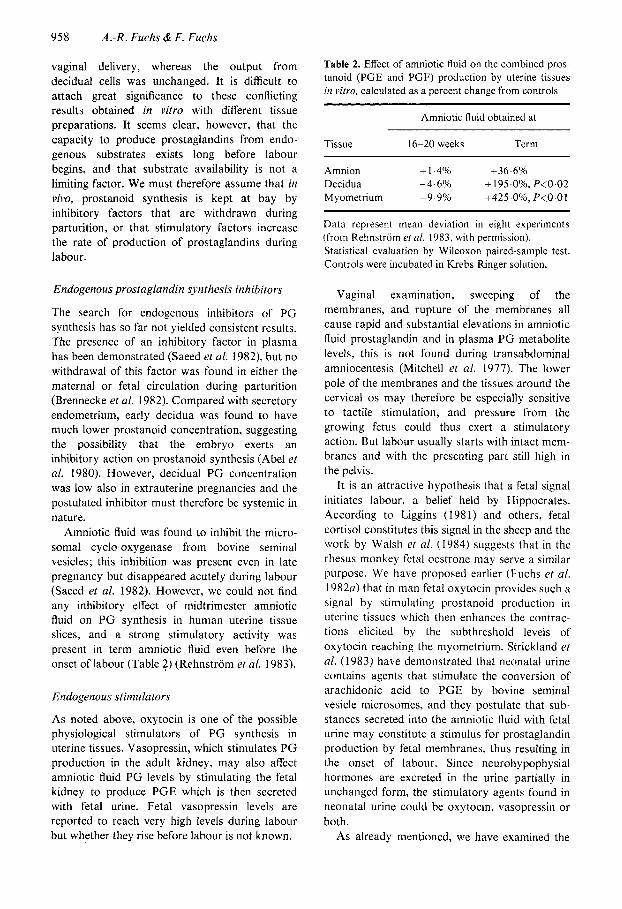
All uterine tissues have the capacity to synthesize prostaglandins, although the spectrum of prosta- glandins produced varies somewhat from tissue to tissue. Willman & Collins (1976) were the first to demonstrate that the capacity to form prosta- glandins is present throughout pregnancy and that no marked changes occur in this capacity at the onset of labour. Numerous investigators have since examined this tissue, but the labour-related differences were small or non-existent. We found that decidual tissue (parietalis) removed at caesarean section from patients in labour produced more PGF, than tissue removed before labour, whereas the production of PGE and PGF by amnion from patients in labour was less than before labour, suggesting possible utilization during labour (Fuchs et al. 1 9 8 2 ~ ) . Olson el a/. (1983), on the other hand, found that PGE and PGF output by amnion cells was increased after
958 A:R. Fuchs & F. Fuchs
vaginal delivery, whereas the output from decidual cells was unchanged. It is difficult to attach great significance to these conflicting results obtained in vitro with different tissue preparations. It seems clear, however, that the capacity to produce prostaglandins from endo- genous substrates exists long before labour begins, and that substrate availability is not a limiting factor. We must therefore assume that in vivo, prostanoid synthesis is kept at bay by inhibitory factors that are withdrawn during parturition, or that stimulatory factors increase the rate of production of prostaglandins during labour.
Endogenous prostaglandin synthesis inhibitors
The search for endogenous inhibitors of PG synthesis has so far not yielded consistent results. The presence of an inhibitory factor in plasma has been demonstrated (Saeed et al. 1982), but no withdrawal of this factor was found in either the maternal or fetal circulation during parturition (Brennecke et al. 1982). Compared with secretory endometrium, early decidua was found to have much lower prostanoid concentration, suggesting the possibility that the embryo exerts an inhibitory action on prostanoid synthesis (Abel et al. 1980). However, decidual P G concentration was low also in extrauterine pregnancies and the postulated inhibitor must therefore be systemic in nature.
Amniotic fluid was found to inhibit the micro- soma1 cyclo-oxygenase from bovine seminal vesicles; this inhibition was present even in late pregnancy but disappeared acutely during labour (Saeed et al. 1982). However, we could not find any inhibitory effect of midtrimester amniotic fluid on P G synthesis in human uterine tissue slices, and a strong stimulatory activity was present in term amniotic fluid even before the onset of labour (Table 2) (Rehnstrom et al. 1983).
Endogenous stimulators
As noted above, oxytocin is one of the possible physiological stimulators of PG synthesis in uterine tissues. Vasopressin, which stimulates P G production in the adult kidney, may also affect amniotic fluid PG levels by stimulating the fetal kidney to produce PGE which is then secreted with fetal urine. Fetal vasopressin levels are reported to reach very high levels during labour but whether they rise before labour is not known.
Table 2. Effect of amniotic fluid on the combined pros- tanoid (PGE and PGF) production by uterine tissues in vitro, calculated as a percent change from controls
Amniotic fluid obtained at
Tissue 16-20 weeks Term
Amnion + 1.4% +36.696 Decidua -4.6% + 195.096, P<0.02 M yometrium -9.9%) +425.0?6, P<O.OI
Data represent mean deviation in eight experiments (from Rehnstrom et al. 1983, with permission). Statistical evaluation by Wilcoxon paired-sample test. Controls were incubated in Krebs-Ringer solution.
Vaginal examination, sweeping of the membranes, and rupture of the membranes all cause rapid and substantial elevations in amniotic fluid prostaglandin and in plasma PG metabolite levels, this is not found during transabdominal amniocentesis (Mitchell et al. 1977). The lower pole of the membranes and the tissues around the cervical 0s may therefore be especially sensitive to tactile stimulation, and pressure from the growing fetus could thus exert a stimulatory action. But labour usually starts with intact mem- branes and with the presenting part still high in the pelvis.
It is an attractive hypothesis that a fetal signal initiates labour, a belief held by Hippocrates. According to Liggins (1981) and others, fetal cortisol constitutes this signal in the sheep and the work by Walsh et al. (1984) suggests that in the rhesus monkey fetal oestrone may serve a similar purpose. We have proposed earlier (Fuchs et al. 1982a) that in man fetal oxytocin provides such a signal by stimulating prostanoid production in uterine tissues which then enhances the contrac tions elicited by the subthreshold levels of oxytocin reaching the myometrium. Strickland et al. (1983) have demonstrated that neonatal urine contains agents that stimulate the conversion of arachidonic acid to PGE by bovine seminal vesicle microsomes, and they postulate that sub- stances secreted into the amniotic fluid with fetal urine may constitute a stimulus for prostaglandin production by fetal membranes, thus resulting in the onset of labour. Since neurohypophysial hormones are excreted in the urine partially in unchanged form, the stimulatory agents found in neonatal urine could be oxytocin, vasopressin or both.
As already mentioned, we have examined the
Endocrinology of human parturition 959
ment; in other stages of the cycle no stimulation occurred (Ishikawa & Fuchs 19786). Siiteri & Seron-Ferre (I98 1 ) have suggested that the increase in the fetal production of DHEA may result in increased oestrogen synthesis in the placenta and fetal membranes and inhibit the conversion of fetal pregnenolone to progesterone, causing a shift in the local oestrogen/progesterone ratio. No direct evidence for such a local shift has yet been presented; in placenta, chorion and amnion the conversion of pregnenolone to progesterone was higher after the onset of labour than before, and no labour-related changes in progesterone concentrations were observed (Khan-Dawood et al. 1983). In the myometrium, oestrogen and progesterone levels largely reflect the plasma levels, and both steroid concentra- tions increase towards term with no significant differences before and after the onset of labour (Batra et al. 1983). At term the ratio of oestrogen to progesterone is higher than at midgestation, but the significance of this ratio for PG synthesis is not clear.
Besides PGE, and PGF,,, prostacyclin and to a lesser degree thromboxane and PGD, are formed within the human uterus. Decidua and myometrium produce large amounts of prosta- cyclin. and lesser amounts of PGF,, and PGE,, whereas amnion produces almost exclusively PGE, and placenta forms PGE2, PGD, and TXA, (Dembele--Duchesne et al. 1981: Fuchs et al. 1982~). Since PGF,, appears to be the most important prostanoid in the mechanism of labour, decidua may be more important than amnion as a site for prostanoid biosynthesis at the onset of labour. The fact that PGF,, production continues at a high rate after the fetus and placenta with membranes are delivered (Fuchs et al. 19826) also supports this.
Both decidua and myometrium are highly vascularized tissues, and prostacyclin may be formed in their vascular compartments. This powerful vasodilator and anti-aggregatory agent may be of importance for the uteroplacental blood flow. Thromboxane formation is restricted to the placenta where under normal conditions its synthesis is inhibited by an inhibitor present in the cytosol (Dembele-Duchesnc et a/ . 1981) but it may become important at delivery when the internal milieu suddenly changes. Placental thromboxane production may contribute to the haemostasis at placental separation. We have demonstrated that a major surge of PGE and
influence of amniotic fluid on the synthesis of prostanoids by human uterine tissues and found that term, but not midtrimester amniotic fluid, had a strong stimulating activity on PG synthesis by decidua and myometrium, whereas the effect on amnion was not significant (Table 2) (Rehnstrom et al. 1983). The stimulatory effect could be explained only partially by the fact that amniotic fluid contains free arachidonic acid which is known to increase in late pregnancy. The absence of a significant stimulatory effect on amnion suggests that in vivo the fetal signal must reach the decidua and myometrium to be effec- tive, and one should therefore look at permeability changes in the fetal membranes, or at other transport mechanisms for such active substances.
Influence of steroid hormones
The synthesis of prostaglandins in the uterine tissues is influenced by steroid hormones but just how is not fully understood. The uterine content of prostaglandins and their release into uterine venous blood varies according to the stage of the cycle in most animal species, the output increasing towards the end of the cycle when progesterone levels fall (Horton & Poyser 1976). Oestradiol treatment increases the uterine content and release of PGF, but pretreatment with progesterone appears to enhance the effect of oestrogen; some studies suggest that oestradiol is incapable of switching on the synthesis and release of PGF,, from the uterus in vivo in the absence of progesterone. Iir vitro, progesterone appears to increase the release of PGF from the rat uterus. It is interesting that in pregnant monkeys, systemic oestradiol treatment had no effect on amniotic fluid PGF levels whereas they were raised by intra-amniotic application of oestradiol (Mead et ol. 1981). Because vehicle or progesterone application also raised amniotic fluid PGF levels albeit less than application of oestradiol, the data are not quite conclusive with regard to oestrogen action.
Oestradiol treatment alters the composition of prostaglandins produced in the uterus, it suppresses the production of PGIz and PGE, whereas PGF production is unchanged (rat uterus) or increased (guinea-pig uterus) (Thaler- Dao el al. 1982). Oestrogens also seem to alter the cofactor requirements: a great stimulation OF PGF, synthesis by adrenaline was observed in the pro-oestrus stage and after oestradiol treat-
960 A . - R . Fuchs & F. Fuchs
PGF is released during the third stage of labour. probably from the placenta and probably contributes to the expulsion of the placenta (Fuchs et a/. 1982b).
Cervical function
Before the onset of labour, the cervix undergoes a ‘ripening’ process which results in softening and this permits dilatation by uterine contractile activity. The biochemical mechanisms by which the structure of the human cervix changes are still poorly understood. Cervical tissue is largely collagenous: in the non-pregnant cervix the collagen appears as dense interlacing fibrils bound by glycosaminoglycans (Danforth et a/. 1960, 1974), but at parturition the cervix has less collagen and glycoproteins, increased water content and more hydrophilic glycosamino- glycans, and the fibrils are shorter and more loosely dispersed. There is some disagreement whether the amount of collagen in the human cervix decreases with advancing gestation: but its solubility is definitely increased and perhaps a partial degradation takes place. The biochemical changes also include a considerable increase in hyaluronic acid, which is a large molecule of low density and is rapidly hydrated. It has been suggested that the accumulation of hyaluronic acid between the collagen fibrils may cause their dispersal (Hillier & Poppleton 1983).
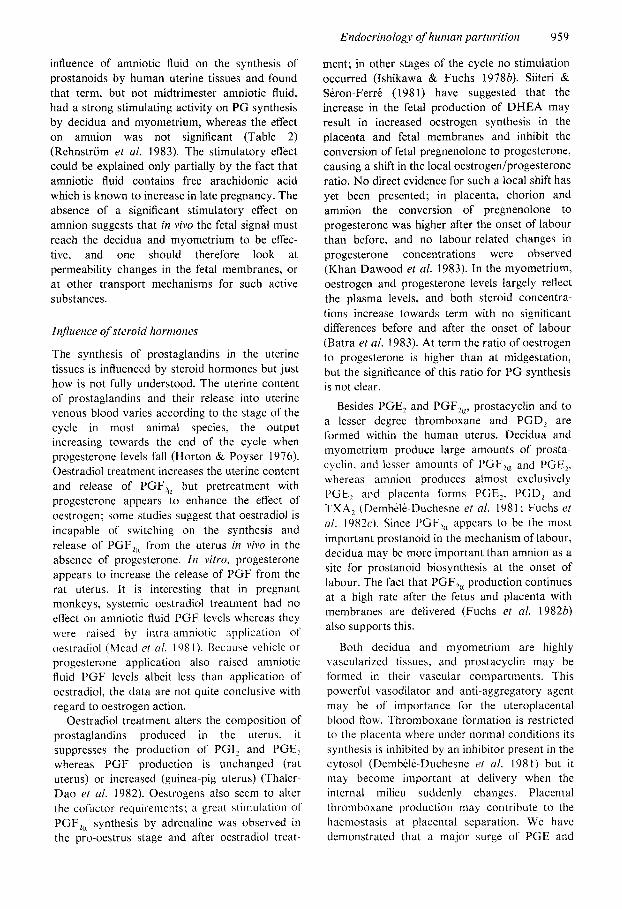
Oestrogen, progesterone, relaxin, and prosta glandins all play a part in controlling the cervical changes during pregnancy that lead to the increasing compliance in advanced gestation. We have shown that myometrial oxytocin sensitivity and cervical ‘ripeness’, expressed in cervical scores, increase in parallel during the last 7 days before parturition (Fig. 7) (Kofler et a/. 1983). Oxytocin could therefore be the stimulus for the sporadic contractions that appear with increasing frequency in late pregnancy: these in turn may contribute to the rapid increase in cervical efface- ment in the last days of gestation.
The question whether cervical innervation plays any role in the initiation of labour has not been given much thought since the days of Theobald (1968). As mentioned earlier, cervical innervation is much denser than that of the corpus uteri, and no loss of neurotransmitter content occurs during pregnancy (Owman et a/. 1967) and therefore it remains functional. Theobald & Lundborg (1962) showed that labour could be induced by electrical stimulation of para-
cervical tissue: they also showed that uterine oxytocin sensitivity appeared to be increased after nerve stimulation. This finding is supported by a remarkable observation by Riisse & Marshall (1970) who stimulated the hypogastric nerve in guinea-pigs in oestrus with various frequencies. At low frequencies that in themselves were unable to elicit uterine contractions they observed a highly significant increase in the uterine reponse to oxytocin; this was abolished by pretreatment with a-blocking agents. Adrenergic nerve activity may thus modulate the tissue excitability by oxytocin and possibly by other agents such as prostaglandins.
Adrenergic nerve activity also results in the release of PGE,, at least in the spleen, heart and gut: if the same applies to the cervix, nerve activity could be of importance for cervical ripening. The remarkable release of prosta- glandins in response to vaginal examination and sweeping of the membranes could perhaps also be mediated, at least in part, by nerve activity. The
T ?? T
*r T
I I I I I I I 7 6 5 4 3 2 1 0
Days before onset of labour
Fig. 7. Daily changes (mean & SD) in uterine oxytocin sensitivity and cervical status in a group of 23 pregnant women at term. Standardized OT tests were administered daily beginning on the expected day of delivery and cervical examinations to determine a modified Bishop score were performed daily until dclivcry. (Adapted from Kofler c/ ( I / . 1983. with pcrtnission.)
Endocrinology o fhuman parturition 96 I
receptors at term and after the onset of labour have failed to reveal any significant labour- related changes in the concentrations of these re- ceptors (Giannopoulos & Tulchinsky 1979; Giannopoulos et al. 1980). At term, cytoplasmic receptors for both hormones are non-detectable. probably because of down-regulation by the high endogenous hormone levels. Total nuclear receptor levels for both oestradiol and progesterone are also lower in pregnant women at term than in non-pregnant women, whereas the percentage of occupied nuclear receptors is some- what higher in pregnant than in non-pregnant women. A slight reduction in both oestrogen and progesterone nuclear receptor levels was observed in samples taken during labour at emergency caesarean sections. This decline could be an arti- fact of sample collection, since we have shown that samples taken at low vertical incisions in advanced labour derive from a different site than those taken at similar incisions before the onset of labour. At least in regard to oxytocin. different concentrations of receptors were found in these two sites, which represent the upper and lower end of the lower uterine segment (Fuchs et al. 19820. 19840).
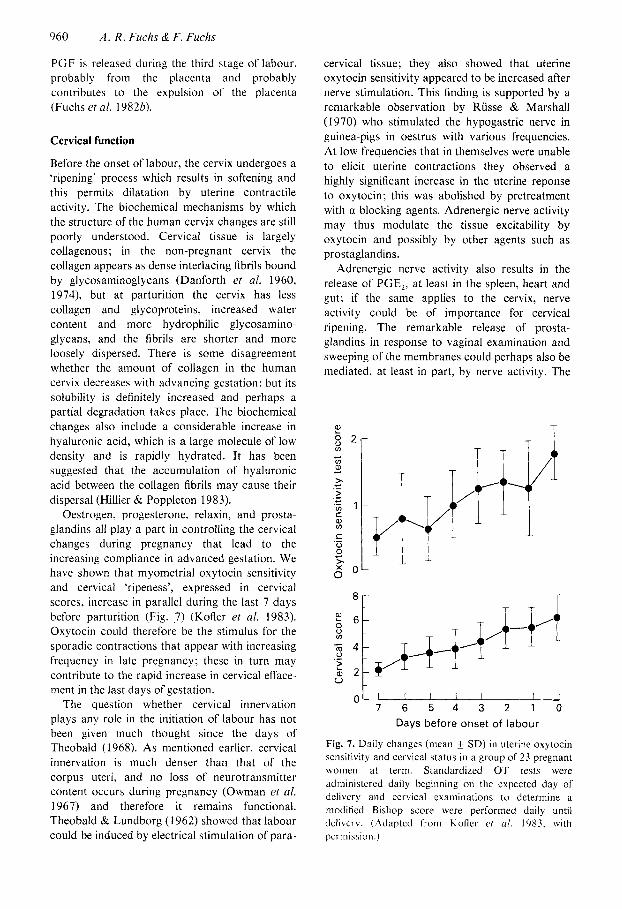
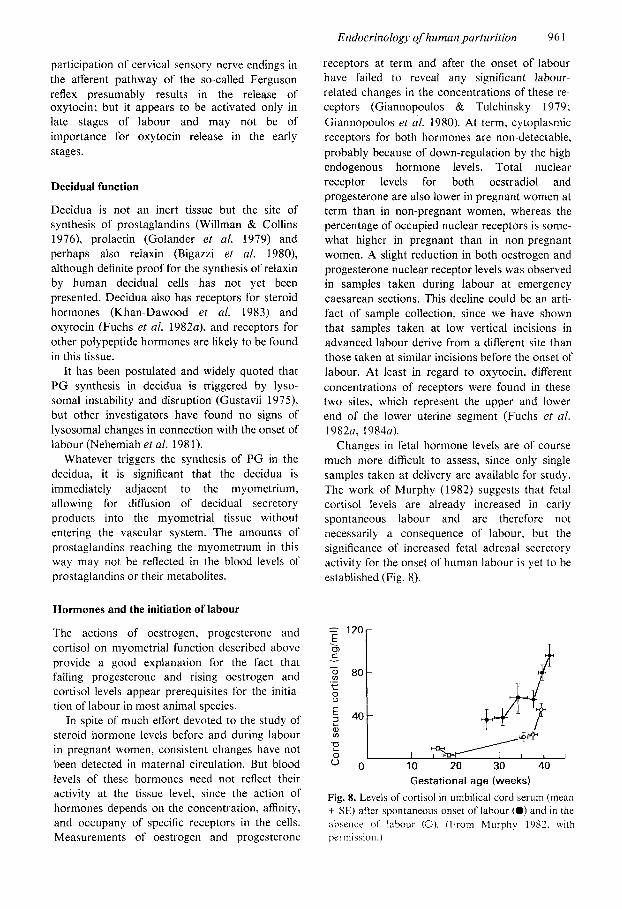
Changes in fetal hormone levels are of course much more difficult to assess, since only single samples taken at delivery are available for study. The work of Murphy (1982) suggests that fetal cortisol levels are already increased in early spontaneous labour and are therefore not necessarily a consequence of labour, but the significance of increased fetal adrenal secretory activity for the onset of human labour is yet to be established (Fig. 8).
participation of cervical sensory nerve endings in the afferent pathway of the so-called Ferguson reflex presumably results in the release of oxytocin; but it appears to be activated only in late stages of labour and may not be of importance for oxytocin release in the early stages.
Decidual function
Decidua is not an inert tissue but the site of synthesis of prostaglandins (Willman & Collins 1976), prolactin (Golander et al. 1979) and perhaps also relaxin (Bigazzi et al. 1980), although definite proof for the synthesis of relaxin by human decidual cells has not yet been presented. Decidua also has receptors for steroid hormones (Khan-Dawood et al. 1983) and oxytocin (Fuchs et al. 1982a), and receptors for other polypeptide hormones are likely to be found in this tissue.
It has been postulated and widely quoted that P G synthesis in decidua is triggered by lyso- somal instability and disruption (Gustavii 1975), but other investigators have found no signs of lysosomal changes in connection with the onset of labour (Nehemiah et al. 1981).
Whatever triggers the synthesis of PG in the decidua, it is significant that the decidua is immediately adjacent to the myometrium, allowing for diffusion of decidual secretory products into the myometrial tissue without entering the vascular system. The amounts of prostaglandins reaching the myometrium in this way may not be reflected in the blood levels of prostaglandins or their metabolites.
Hormones and the initiation of labour
The actions of oestrogen, progesterone and cortisol on myometrial function described above provide a good explanation for the fact that falling progesterone and rising oestrogen and cortisol levels appear prerequisites for the initia- tion of labour in most animal species.
In spite of much effort devoted to the study of steroid hormone levels before and during labour in pregnant women, consistent changes have not been detected in maternal circulation. But blood levels of these hormones need not reflect their activity at the tissue level, since the action of hormones depends on the concentration, affinity, and occupany of specific receptors in the cells. Measurements of oestrogen and progesterone
I 10 Gestational age (weeks)
Fig. 8. Levels of cortisol in umbilical cord serum (mean f SE) after spontaneous onset of labour (0) and in the absence of labour (0). (From Murphy 1982. wi th permission.)
962 A.-R. Fuchs & F. Fuchs
Serial sampling of fetal blood in rhesus monkeys revealed only insignificant changes in fetal cortisol levels before delivery (Fig. l), whereas fetal oestrone levels were found to increase significantly during the last days preceding delivery (Walsh et a/. 1984). There is so far no evidence for a preparturient rise in fetal oestrogen production in man.
Oxytocic hormones and the initiation of labour
In the absence of dramatic changes in the levels of steroids, one must assume that uterine activity is initiated by one or more of the oxytocic hormones, such as oxytocin, vasopressin or the prostaglandins.
As discussed above, definite increases in PG levels were detected neither in the maternal circulation nor in amniotic fluid before, or at the onset of. labour in women, although marked increases occur during labour. Rupture of mem- branes is the only known labour-related stimulus that increases PG production (Mitchell et al. 1977; Husslein et a/. 1983) and in instances where the membranes rupture before the onset of labour maternal serum P G levels are significantly raised (see Fig. 3) (Husslein et al. 1981; Fuchs et al. 1983a). Failure of labour to start in several instances after premature rupture of the mem- branes, in spite of raised PG levels, suggests that PGF,, production alone is not sufficient to initiate labour; other factors must be present for uterine contractions to begin.
The finding that oxytocin receptor levels rise dramatically during gestation and reach a maxi- mum level in early labour strongly implicates oxytocin as the initiating factor for uterine contractions. In our prospective study in which oxytocin sensitivity and cervical changes were determined by daily examinations until labour began, we could demonstrate a clear correlation between the onset of labour and uterine oxytocin sensitivity, while the correlation with cervical changes was less good (Kofler et a/. 1983). No woman in our study went into labour with an unresponsive uterus, whereas when labour began, several still had a relatively unripe cervix. We have also shown that infusions of oxytocin which initiate contractions at term do not raise oxytocin levels significantly over those seen in many pregnant women in late gestation (Fuchs et al. 1983a). Thus the increase in oxytocin concentra- tions sensitizes the uterus to the normally existing levels of oxytocin and therefore seems to be the
crucial event that initiates contractions at term. The collective data presented above suggest
that increased production of PGF,, is essential for the maintenance of labour and for cervical dilatation. In addition, an interaction of oxytocin and PGF, seems necessary for the establish- ment of adequate uterine contractions.
The primary importance of initial oxytocin action may reside in the fact that oxytocin, being systemically released into the circulation. reaches all parts of the myometrium simultaneously, whereas prostaglandins, being produced locally in the uterus, initially reach only parts of the myo- metrium. This co-ordinating function of oxytocin is evident in instances of premature rupture of membranes, where local production of prosta- glandins is quite significant as shown by the blood levels, but infusioI1s of oxytocin are nevertheless required to initiate adequate contractions (Husslein et al. 1981). Likewise, in hypertonic saline-induced abortions, oxytocin infusions are capable of inducing co-ordinated contractions before they evolve spontaneously (Lauersen et al. 1974) as a result of the hypertonic saline-induced local PGF, production (Fuchs et a/. 19846). Oxytocin may serve a similar co-ordinating func- tion in the normal course of labour.
The factor(s) that control oxytocin receptor concentrations in the human uterus thus constitute a crucial element in the initiation of labour. As already mentioned. oestrogen promotes and progesterone inhibits oxytocin receptor formation in the rat uterus (Fuchs et al. 1 Y83b). In the human uterus. oestrogen probably has the same effect as in rats whereas progesterone has an opposite effect, acting syner- gistically with oestrogen to promote oxytocin receptor formation (Fuchs et al. 19840). Disten- tion of the uterus of pregnant rats also enhances the effects of oestrogen on oxytocin receptor con- centrations (Fuchs et a/. 1983~). and may be of importance in human pregnancy as well.
The coupling of oxytocin receptor occupancy to PG synthetase activity in decidua may also be of crucial importance for the initiation of human labour, since even oxytocin-induced labour fails to progress in the absence of a rise in PGF,, formation.
References Abel, M. H., Smith S. K. & Baird D.T. (1980)
Suppression of endometrial prostaglandin in early intra-uterine and ectopic pregnancy in women. J EndocrinolSS, 379-386.
Endocrinology of human parturition 963
Dembele-Duschesne, M. J., Thaler-Dao, H., Chavis, C. & Crastes de Paulet, A. (1981) Some new prospects in the mechanism of control of arachidonate meta- bolism in human placenta and membranes. Prosta- glandins 22,979.
Divers, W. A., Wilkes, M. M., Babaknia, A. & Yen, S. S. C. (1981) An increase in catecholamines and metabolites in the amniotic fluid compartment from middle to late gestation. Am J Obstet Gvnecol 139,
Downing, S. J. & Porter, D. G. (1980) Oestrogen induced myometrial quiescence in the post partum rat is not mediated by adrenaline or by a- or 0- adrenoceptor activation. J Endocrinol 85, 405 413.
Dubin, N.H., Ghodgaonkar, R.B. & King, T .M. (1979) Role of prostaglandin production in spontaneous and oxytocin-induced uterine contrac- tile activity in in vitro pregnant rat uteri. Endo- crinology 105,47-5 1.
Dubin, N. H., Johnson, J. W. C., Calhoun, S., Ghodgaonkar, R. B. & Beak. J. C. (1980) Plasma prostaglandin in pregnant women with term and preterm deliveries. Obstet Gynecol51,203-206.
Ducsay, C. A,, Cook, M. J., Walsh, S. W. & Novy. M. J. (1983) Circadian patterns and dexa- methasone-induced changes in uterine activity in pregnant rhesus monkeys. Am J Obstet Gynecol
Embrey, M. P. & Moir, J. C. (1967) A comparison of the oxytocic effects of synthetic vasopressin and oxytocin. J Obstet Gynecol Br Commonw 14, 648- 652.
Eliot, R. J. , Lam, R., Leake, R. D., Hobel, C. J. & Fisher, D. A. (1980) Plasma catecholamine concentrations in infants at birth and during the first 48 hours of life. Pediatrics 96,3 11-3 15.
Fields, P. A., Eldridge, R. K., Fuchs, A. -R., Fields, M. J. & Roberts, R. F. (1983) Human placental and bovine luteal oxytocin. Endocrinology 112, 1544.
Fuchs. A. -R. (1974) Myometrial response to prosta- glandins enhanced by progesterone. Am J Obstet Gq’neCOl 118, 1093-1098.
Fuchs, A. -R. (1978) Hormonal control of myometrial function during pregnancy and parturition. Acta Endocrinol Suppl221, 1-69.
Fuchs, A. -R., Fuchs, F., Husslein, P., Soloff, M. S. & Fernstrom, M. J. ( 1 9 8 2 ~ ) Oxytocin receptors and human parturition: a dual role for oxytocin in the initiation of labor. Science 215, 1396.
Fuchs, A. -R., Fuchs, F., Husslein, P., Fernstrom, M. J. & Soloff, M. S. (19840) Oxytocin receptors in the human uterus during pregnancy and parturition. A m J Obstet Gynecol in press.
Fuchs. A. -R.. Goeschen. K., Husslein. P., Rasmussen. A. B. &. Fuchs. F. ( 1 9 8 3 ~ ) Oxytocin and the initia- tion of human parturition: 111. Plasma concentra- tions of oxytocin and 13.14-dihydro-15-keto- prostaglandin F,, in spontaneous and oxytocin-
483-486.
145, 389-396.
Alexander, D. P., Forsling, M. L. & Martin, M. J. (1972) The effect of maternal hypoxia on fetal pituitary hormone release. Biol Neonate 21,219.
Artal, R. (1980) Fetal adrenal medulla. Clin Obstet Gjxecol23,825-836.
Batra, S., Bengtsson, L. Ph. & Ingemarsson, I. (1983) The role of estradiol and progesterone in the regula- tion of myometrial activity for the onset of labor. Aria Obstet Gynecol Scand 62,207.
Ben Jonathan, N. & Munsick, R. A. (1980) Dopamine and prolactin in human pregnancy. J Clin Endocrinol Metab 51, 1019-1025.
Bigazzi, M., Nardi, E., Bruni, P. & Petrucci, F. (1 980) Relaxin in human decidua. J Clin Endocrinol Metab 51,939-947.
Brennecke, S. P., Bryce, R. L. & Turnbull, A. C. (1982) The prostaglandin synthase inhibiting ability of maternal plasma and the onset of human labour. Eur J Obstet Gynecol Reprod 14,8 1-88.
Caldeyro-Barcia, R. & Sereno. J. A. (1959) The response of the human uterus to oxytocin through- out pregnancy. In Oxytocin (Caldeyro-Barcia. R. & Hkller, H., eds), Pergamon Press, London, pp. 177- 202.
Castracane, V. D. & Jordan, V. C. (1975) The effect of estrogen and progesterone on uterine P G bio- synthesis in the ovariectomized rat. Biol Reprod 13,
Challis, J. R . G., Socol, M., Murata, V., Manning, F. A. & Martin, C. B. (1980) Diurnal variations in maternal and fetal steroids in pregnant rhesus monkeys. Endocrinology 106, 1283-1288.
Chan, W. Y. (1980) The separate uterotonic and PG- releasing actions of oxytocin. Evidence and comparison with angiotensin and methacholine in the isolated rat uterus. J Pharmacol Exp Ther 213, 575.
Clark, J. W. & Peck, E. J. (1979) Female Sex Steroid Receptors and Functions Monographs on endo- crinology, Springer, Berlin.
Csapo, A. (1956) The mechanism of effect of the ovarian steroids. Rec Prog Horm Res 12,405-43 I .
Csapo, A. &. Takeda. H. (1965) Effect of progesterone o n the electric activity and intrauterine pressure of pregnant and parturient rabbits. A m J Obstet Gq’necol91,221-23 1.
Danforth, D. N., Buckingham, J. C. & Roddic, J. W. (1960) Connective tissue changes incident to cervical effacement. A m J Obstet Gynecol 80, 939- 945.
Danforth, D. N., Veis, A., Breen, M., Weinstein, H. G., Buckingham, J. C. &. Manalo, P. (1974) The effect of pregnancy and labor on the human cervix: changes in collagen, glycoprotein and glycos- aminoglycans. Am J Obstet Gjwecol 120,641-65 1.
Dawood. M. Y. (1983) Neurohypophyseal hormones. In Endocrinolog~~ of Pregnancy 3rd edn. (Fuchs, F. eC Klopper. A.. eds). Harper &. Row. Philadelphia.
587-596.
pp. 204-228.
964 A:R. Fuchs & F. Fuchs
induced labour at term. Am J Obstet Gynecol 147, 497-502.
Fuchs, A. -R., Husslein, P., Sumulong, L. & Fuchs, F. (1982b) The origin of circulating 13,14-dihydro-15- keto-PGF,, during delivery. Prostaglandins 24, 715-722.
Fuchs, A. -R., Fuchs, F., Husslein, P. & Weksler, B. B. (1982~) Differential effects of oxytocin and labor on prostacyclin and prostaglandin F and E production in human uterus. Program of the 64th Annual Meeting of the Endocrine Society San Francisco. Calif. A, no. 1035, p. 838.
Fuchs, A. -R., I’criyasami. S., Alexandrova. M. & Soloff, M. S. (19836) Correlation between oxytocin receptor concentration and responsiveness to oxytocin in pregnant rat myometrium: effect of ovarian studies. Endocrinologji 113, 742-749.
Fuchs. A. -R.. Pcriyasami, S. & Soloff. M. S. (1983~) Systemic and local control of oxytocin receptor concentrations in pregnant rat uterus. Can J Cell B i d Biochrm 61,6 15-624.
Fuchs. A. -R. & Poblete, V. F. Jr (1970) Oxytocin and uterine function in pregnant and parturient rats. Biol Reprod 2, 387-400.
Fuchs. A.-R., Rasmussen, A. B.. Rehnstriim, J. & Toth, M . (1984b) Prostaglandin Flu, oxytocin and uterine activation in hypertonic saline induced abor- tions. A m J Obsret Gjxecol in press.
Fuchs, A. -R.. Smitasiri, Y. & Chantharasksri, U. (1976) The effect of indomethacin on uterine contractility and luteal regression in pregnant rats at term. J Reprod Fertil48,33 1-340.
Fuchs, F., Fuchs, A. -R., Poblete. F. Jr & Risk, A. (1967) Effect of alcohol on threatened premature labor. Am J Obstet Gjwecol99,627-637.
Garfield. R. E.. Daniel, E. E., Dukes, M. & Fitzgerald, J. D. (1982) Changes of gap junctions in myo- metrium of guinea pig at parturition and abortion. Can J Ph.vsio1 Pharrnacol60,335.
Garfield. R. E. & Hayashi, R. H. (1981) Appearance of gap junctions in the myometrium of women during labor. Am J Obstet Gjwecol 140,254-260.
Garfield. R. E.. Kannan. M. S. & Daniel. E. E. (1980) Gap junction formation in myometrium: control by estrogens. progesterone and prostaglandins. A m J Physiol238C, 81-89.
Gennser. G., Ohrlander. S. & Eneroth, P. (1977) Fetal cortisol and the initiation of labour in the human. In The Fetus and Birth Ciba Foundation Symposium (new series). Elsevier/Excerpta Medica/North- Holland. Amsterdam. pp. 401-420.
Giannopoulos. G. & Tulchinsky. D. (1979) Cyto- plasmic and nuclear progestin receptors in human myometrium during the menstrual cycle and in pregnancy at term. J Clin Endocrinol Metab 49,
Giannopoulos, G., Goldberg, P., Shea, T. B. & Tulchinsky. D. (1980) Unoccupied and occupied estrogen receptors in myometrial cytosol and nuclei
100- 106.
from nonpregnant and pregnant women. J Clin Endocrinol Metab 5 1, 702-710.
Golander, A., Hurley, T., Barrett, J. & Handwerger, S. (1979) Synthesis of prolactin by human decidua in vitro. J Endocrinol82,263-267.
Goto, M. & Csapo, A. (1959) The effect of ovarian steroids on the membrane potential of uterine muscle. J Gen Phvsiol43,455.
Green, K., Bygdeman, M., Toppozada, M. & Wiqvist, N. (1974) The role of PGF,, in human parturition. Endogenous plasma levels of 15-keto-13.14- dihydroprostaglandin F,, during labor. A m J Obstef Gynecol120,25-31.
Gustavii, B. (1975) Release of lysosomal acid phos- phatase into the cytoplasm of decidual cells before the onset of labour in humans. B,r J Obstet Gynaecol82, 177- 18 1.
Hamberg, M. (1974) Quantitative studies of prosta- glandin synthesis in man. Excretion of the major urinary metabolite of PGF,, and F,, during pregnancy. Life Sci 14,247-252.
Hervonen, A. (197 1) Development of catecholamine storing cells in human fetal paraganglia and adrenal medulla. Aeta Phj,siol Scand Suppl368, 1-94.
Hillier, K. & Poppleton, H. (1983) The hormonal control of the pregnant human cervix. In Biology of Rela+ Proc of Intl Conference 1982, Florence, Exccrpta Medica lntl Congr Series, vol. 610, pp 93- 106.
Horton, E. & Poyser, N. L. (1976) Uterine luteolytic hormones. A physiological role for PCIF~,. Physiol Rev 56, 595.
Husslein. P., Fuchs, A. -R. & Fuchs. F. (1981) Oxytocin and the initiation of parturition. I . Prosta- glandin release during induction of labor with oxytocin. A m J Obstet Gynecol 141,688-693.
Husslein, P., Kofler. E., Rasmussen, A. B.. Sumulong, L.. Fuchs, F. & Fuchs. A. -R. (1983) Oxytocin and the initiation of human parturition: IV. Plasma con- centrations of oxytocin and 13.14-dihydro.15-keto- prostaglandin F,,L during labor induced by artificial rupture of membranes. Am J Obsret Gynecol 147, 503-507.
Ishikawa, M . & Fuchs. A. -R. (1978a) Electrical and mechanical activity of rat uterus in vivo during the estrous cycle. Am J Obstet Gynecol 132,6 11-6 19.
Ishikawa. M. & Fuchs, A. -R. (1978b) Effects of epine- phrine and oxytocin on the release of prostaglandin F from rat uterus in vitro. Prostaglandins 15,89.
J a t k R. B.. Seron-Ferre, M., Parer, J. T. & Lawrence, C. C. (1978) The primate fetal pituitary-adrenal axis in the perinatal period. Am J Obsret Gynecol 131, 164.170.
Jung. H. (1964) Die Wirkung der Ovarial-und der Placentar-Hormone. In Pharmacologv of Smooth Muscle Proc 2nd Intl Pharmacol Meeting, Prague. 20-23 August 1963, Pergamon Press. Oxford, pp. 113-126.
Kao, C. Y. & Nishiyama, A. (1964) Ovarian hormones
Endocrinology of human parturition 965
and resting potential of rabbit uterine smooth muscle. Am J Phj.siol201, 793.
Keirse, M. J . N. C. & Turnbull, A. C. (1973) E prosta- glandins in amniotic Huid during late pregnancy and labour. J Obsret G~viaecol Br Commonw 80, 970- 973.
Keirse, M. J . N. C., Flint, A. P. F. & Turnbull, A. C. (1974) F prostaglandins in amniotic Huid during pregnancy and labour. J Obstet Gynaecol Br Conimonw 8 1, 13 1 ~ 135.
Khan-Dawood, F. S . , Saughnessy, E. A. & Dawood. M. Y. (1 983) In vitro conversion of pregnenolone to progesterone, progesterone receptors and hormone levels in term human placenta and fetal mem- brancs. Abstract 479. p. 261. presented at 30th Annual Meeting. Society for Gynecologic Investigation. Washington DC. 17-20 March.
Koay. E.S.C., Too, C. K.L., Greenwood, F .C. & Bryant Greenwood. G. D. ( 1 983) Relaxin stimulates collagenase and plasminogen activator secretion by dispersed human amnion and chorion cells in vitro. J Clin Endocrinol Mefab 56, 1332.
Kofler, E.. Husslein, P., Langer, M., Fuchs, A. -R. & Fuchs, F. ( 1 983) Die Bedeutung der Oxytocinemp- findlichkcit fur den spontanen Wehenbeginn beim Menschen. Geburtshilfe Fruuenheilk 43,533.
Lackritz. P., Tulchinsky. D.. Ryan. K. L. & Levine, L. (1978) Plasma prostaglandin metabolites in human labor. Am J Obstet G.~~necol 131,484-489.
Laucrsen, W. H.. Wilson, K. H., Beling. G. & Fuchs, F. (1074) Comparison of prostaglandin F,,, and hypertonic saline for induction of midtrimester abortion. A m J Obstet Gynecol 120,875-889.
Leake. R. D.. Weitzman, R. E., Glatz. T. H. & Fisher, D. A. ( I 98 I ) Plasma oxytocin concentration in man. nonpregnant women and pregnant women before and during spontaneous labor. J Clin Endo- crinol hlercib 53, 730-733.
Lewis, R. B. & Schulman, J. D. (1973) Influence of acetylsalicylic acid. an inhibitor of prostaglandin synthesis, on the duratioa of human gestation and labour. Lancet ii, 1159-1 161.
Liggins, G. C. (1981) Endocrinology of parturition. In f e r a l Endocritiology (Novy. M. J. & Resko. J. A., eds). Academic Press, New York, pp. 21 1-237.
MacLcnnan. A. H.. Breen, R. D. & Greenwood, G. D. (1980) Ripening of the human cervix and induction of labour with purified porcine relaxin. L,ance/ i, 220-223.
Mant-ll, C. D. & Liggins, G. C. (1970) The effect of ethanol on the inyometrial response to oxytocin in women at term. J Ohstet G.vnaecol Br Cornmonw 77,976-98 1.
Marshall, J . M. (1962) Regulation of activity in uterine ' smooth muscle. Physiol Reis 42,213.
Mead, G.. Walsh, S. W., Dolney. A. M. & Novy, M. J. (1981) Amniotic fluid steroid implants: effect on gestational length and prostaglandins in rhesus monkeys. Prog 28rh A n n Meeting of the Soc
G.vnecol Inoestig 19-21 March, St Louis, MO, A. no. 128, p. 77.
Mitchell, D., Flint, A. P. F., Bibby. J., Brunt, J., Arnold, J . M.. Anderson, A. B. M. & Turnbull, A. C. (1977) Rapid increases in plasma prosta- glandin concentrations after vaginal examination and amniotomy. Br MedJi i , 1183-1 185.
Mitchell, M . D., Flint, A. P. F. & Turnbull, A. C. (1975) Stimulation by oxytocin of prostaglandin F levels in uterine venous effluent in pregnant and puerperal sheep. Prostuglandins 9,47.
Mitchell. M. D., Patrick, J. E., Robinson, J . S . & Turnbull, A. C. (1976) Prostaglandins in the plasma and amniotic fluid of rhesus monkeys during preg- nancy and after intra-uterine fetal death. J Etido- c r i n o l l l , 67-76.
Murphy, B. E. P. (1982) Human fetal serum cortisol levels related to gestational age: evidence of mid- gestational fall and a steep late rise, independent of sex or mode of delivery. Am J Obsrer Gynecol 144, 276-282.
Murphy, B. E. P., Clark, S. J., Donald, I. R., Pinsky, M. & Vedady. D. (1974) Conversion of maternal cortisol to cortisone during placental transfer to the human fetus. A m J Obstet Gynecol 118, 538-54 1.
Nehemiah, J . L.. Schwitzer. J. A., Schulman, H. & Novikoff, A. B. ( 1 98 I ) Human chorionic tropho- blasts. decidual cells, and macrophages: a histo- chemical and electron microscopy analysis. A m J Obsrer Gynecol 140, 26 1-268.
Niemineva, K. & Pekkarinen, A. (1952) The noradrenaline and adrenaline content of human fetal adrenal glands and aortic bodies. Ann Med ESP Biol Fenn 30, 274.
Nissenson. R.. Flouret, G. & Hechter. 0. (1978) Opposing effects of estradiol and progesterone on oxytocin receptors in rabbit uterus. Proc Null Acad Sci USA 15,2044.
Olson, I). M., Skinner. K. & Challis, J. R. C. (1983) Prostaglandin output in relation to parturition by cells dispersed from human intrauterine tissues. J Clin Endocrinol hlerab 57, 694-699.
Owman. C. H.. Rosengren. E. & SjCiberg, N. -0. (1967) Adrenergic innervation of the human female reproductive organs: a histochemical and chemical investigation. Obsfer Gynecol30, 763-773.
Parboosingh, J., Lederis, K. & Singh, N. (1982) Vaso- pressin concentration in cord blood: correlation with method of delivery and cord pH. Obstet Gynecol60, I 79- 183.
Parker. C. R. Jr., Leveno. K., Carr. B. R., Hauth. J. & MacDonald, P. C. (1982) Umbilical cord plasma levels of dehydroepiandrosterone sulfate during human gestation. J Clin Endocrinol Metab 54, 12 16- 1220.
Pohjavuori. M. & Fyhrquist, F. ( 1 980) Hemodynamic significance 01' vasopressin in the newborn infant. J Ptdicrtr. 91, 462.
Porter. D. (3.. Downing. S . J . & Bradshaw. J. hl . ('.
966 A.-R. Fuchs & F. Fuchs
(1979) Relaxin inhibits spontaneous and prosta- glandin driven myometrial activity in anesthetized rats. J Endocrinol83, 183-192.
Puri, C. P. & Garfield, R. E. (1982) Changes in hormone levels and gap junctions in the rat uterus during pregnancy and parturition. Biol Reprod 27, 967-975.
Rehnstrom, J.. Ishikawa, M.. Fuchs, F. & Fuchs. A.-R. (1984) Stimulation of myometrial and decidual production by amniotic fluid from term but not niidtrimester pregnancies. Prostaglandins, 26, 973- 982.
Roberts, J. M.. Insel, P. A. & Goldfien. A. (1981) Regulation of myometrial adrenoreceptors and adrenergic response by sex steroids. Mol Pharmacol20,52.
Roberts. J. S., McCracken, J. A., Gavagan, J. E. & Soloff. M . S. (1976) Oxytocin stimulated release of prostaglandin F,-alpha from ovine endometrium in vitro. Correlation with estrous cycle and oxytocin receptor. Endocrinology 99, 1107-1 114.
Russe, M. W. & Marshall. J. M. (1970) Uterine response to adrenergi: nerve stimulation in the guinea pig. Biol Reprod 3, 13-22.
Saameli, K. (1963) An indirect method for the estima- tion of oxytocin blood concentrations and half-life in pregnant women near term. A m J Obsfet Gynecol 85, 186- 192.
Saarikoski, S. (1974) Fate of noradrenaline in the human foetoplacental unit. Acta Physiol Scand Suppl421, I .
Saeed. S. A,, Strickland, D. M.. Young, D. C.. Danc, H. N . H. & Mitchell. M. D. (1982) Inhibition of prostaglandin synthesis by human amniotic Ruid: acute reduction in inhibitory activity of amniotic fluid obtained during labor. J Clin Endocrinol Mefab 55,801-803.
Sellers. S . M., Hodgson, H. T., Mountford, L. A,. Mitchell. M. D.. Anderson. A. B. M. & Turnbull. A. C. (1981) Is oxytocin involved in parturition? Br J Ohstel Gjwaecol88, 725-729.
Sherwood. 0. D.. Crnekovic. V. E., Gordon, W. L. & Rutherford, J . E. (1980) Radioimmunoassay of relaxin throughout pregnancy and during parturi- tion in the rat. Endocrinology 107,691-698.
Siiteri, R. K . &. Seron-Fcrre. M. (1981) Some new thoughts on fetoplacental iinit and parturition in primates. In Fetal Endocrinology (Novy. M. J. & Resko. .I. A.. eds). Academic Press. Ncw York.
Sjiiberg. N.-0. (1967) The adrenergic transmitter of the female reproductive tract: distribution and func- tional changes. Acta Phvsiol Scand Suppl 305, 5 .
Sjiiberg. N.-O.i 1968h) Considerations on the cause of the disappearance of the adrenergic transmitter in uterine nerves during pregnancy. Acta Phj7siol Scand 12, 5 10.
S.jliberg. N . -0 . ( 1 968a) Increase in transmitter content of adrenergic nerves in the reproductive tract of
p. 1.
female rabbits after oestrogen treatment. Acta Endocrinol (Copenhagen) 57,405-423.
Soloff, M. S. (1975) Uterine receptor for oxytocin: effects of estrogen. Biochem Bi0phc.s Res Comm 65, 205.
Stark. R. I., Wardlaw, S. L., Daniel, S. S., Husain, M. K., Sanocka, U. M., James, L.S. & Vande Wiele, R. L. (1982) Vasopressin secretion induced by hypoxia in sheep: developmental changes and relationship to @-endorphin release. A m J Obstet Gvnecol 143, 204-2 15.
Strickland, D. M., Saeed, S. A., Casey, L. M. & Mitchell, M. D. ( 1 983) Stimulation of prosta- glandin biosynthesis by urine of the human fetus may serve as a trigger for parturition. Science 220, 521.
Taylor. N. F., Martin. M. C., Nathanielsz, P. W. & Skron-Ferre. M. (1983) The fetus determines circadian oscillation of myometrial electromyo- graphic activity in the pregnant rhesus monkey. A m J Ohstet Gvnecol 146,557-567.
Thaler-Dao, H., Romonaxto. M., Saintot, M.. Chaintreciel. J. & Crastes de Paulet. A. (1982) Effect of estradiol-178 on prostaglandin bio- synthesis by the uterus of ovariectomized rat and guinea pig. Prostaglandins 24, 149.
Theobald, G. W. (1968) Nervous control of uterine activity. Clin Obstet Gjwiecol 11, 15-33.
Theobald, G. W. & Lundborg, R. A. (1962) Changes in myometrial sensitivity to oxytocin provoked in different ways. J Obstet Gynaecol Br Commonw 69, 4 11-427.
Tulchinsky. D.. Hobel, C. J.. Yeager, E. & Marshall. J. R. (1972) Plasma estrone. estradiol. estriol, progesterone and 17 OH-progesterone in human pregnancy. ,4171 J Obstet Gjwecol 112, 1095- 1100.
Tulchinsky. D. (1973) Placental secretion of unconjugated estrone. estradiol. and estriol into the maternal and fetal circulation. J Clin Endocrinol Metah 36, 1079-1087.
Wakeling. A. E. &. Wyngarden, L. J. (1974) Prosta- glandin receptors in the human. monkey and hamster uterus. Endocrinologj~ 95,55-64.
Walsh. S. W.. Stanczyk, F. Z. & Novy, M . J. (1984) Daily hormonal changes in the maternal, fetal and amniotic fluid compartments before parturition in a primate species. J Clin Endocrinol Metah 58, 629- 639.
Weiss. G . E.. O’Byrne. E. M., Hochman, J. A,, Gold- smith. D.. Rifkin. I . & Steinctz. B. G. (1977) Secre- tion of progesterone and relaxin by the human corpus luteum at midpregnancy and at term. Ohstet Gj7neco150, 679-681.
b’illman. E. A. & Collins. W. P. (1976) Distribution of f’GE, and Fbr within the foetoplacental unit throughout human pregnancy. J Endocrinol 69, 4 13-4 19.
Li’iqvist. N. (1959) Immediate and prolonged effects of

Endocrinology of human parturition 967
relaxin on the spontaneous activity of the mouse Zuckerman. H.. Rciss. lJ. Sr Rubinsteiti. I . (1974) and rat uterus. Acta Endocrinol Suppl46, 1 - 1 1. Inhibition of human premature labor by indo-
Wolfs. G. M. J . A. RC Van Leeuwen. M. (1979) Electro- nieihacin. Ohstet Gjwcol44, 787-792. tnyographic observations on the human uterus Zuspan. I;. P. (1970) Urinary excretion of epinephrine during labour. Acta Ohstet Gjwecol Scand Suppl and norepinephrine during pregnancy. J Clin Endo- 90, 1-61. crinol30, 357.
Related Documents