ENDOCRINOLOGY (for dummies) Wednesday 28 th November Dr. Charlotte Hopper & Dr. Andy Hird

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ENDOCRINOLOGY (for dummies)
Wednesday 28th November
Dr. Charlotte Hopper & Dr. Andy Hird

Plan
• Initial pop-quiz of key endocrinology topics followed by basic need to know info, incl:– The Adrenals (Addisons, Conns, Phaeochromocytoma)– Pituitary (Cushings)– Thyroid– Calcium & bone (hyper/hypocalcaemia, Osteoporosis)– We do not plan to cover…
• Picture quiz• Interactive AKT style questions• Summary & handout
Presenter
Presentation Notes
A number of things such as diabetes, acromegaly, reproductive endocrinology and the weird and wonderful other than what is next! Initial pop-quiz of key endocrinology topics followed by basic need to know info, incl: The Adrenals (Addisons, Conns, phaeochromocytoma) Pituitary (Cushings) Thyroid Calcium & bone (hyper/hypocalcaemia, osteoporosis) We do not plan to cover… reproductive endocrinology & diabetes as this has been covered previously Picture quiz Interactive AKT style questions Summary

The adrenals…

Addisons: True or False?
• Some women with Addisons may develop premature ovarian failure?

TRUE
Presenter
Presentation Notes
5% may develop premature ovarian failure and likely to be those with autoimmune Addisons.

True or false?
• In secondary hypoadrenalism patients often show increased pigmentation?

FALSE
Presenter
Presentation Notes
Only those with primary adrenal failure show increased pigmentation due to increased ACTH secretion

Addisons(hypoadrenalism)
• Presenting symptoms: often insidious…– Pigmentation (buccal, scars, palmer creases,
generalized)– Weight loss– Abdominal pain– Fatigue– Nausea & vomiting– Diarrhoea– Postural hypotension
Presenter
Presentation Notes
Don’t forget Addisons can present in a crisis: coma, hypoglycaemia, hypotension – give steroids immediately

All below may precipitate a crisis:
• Inadequate steroid replacement
• Sudden cessation of long-term steroid treatment eg. For severe asthma
• Infection
• Major surgery
• Any serious illness

Addisonian crisis
GIVE STEROIDS
IMMEDIATELY!
IV HYDROCORTISONE 200MG
Addisons – causes…• PRIMARY
– Destruction of adrenal gland• Autoimmune (90%)• TB• Metastases
• SECONDARY – Inadequate ACTH production e.g. pituitary tumour,
chronic steroid therapy
• Associated diseases: – Hypothyroidism, type 1 DM, pernicious anaemia,
vitiligo…
Presenter
Presentation Notes
50% of those with autoimmune Addisons may develop another autoimmune conditions such as Graves disease or pernicious anaemia… Chronic steroid therapy suppresses ACTH levels thus producing adrenal cortex atrophy. Physical stress or over-quick steroid withdrawal can then provoke acute adrenal failure

Addisons – Ix and Mx
• Short synacthen
• Hyponatraemia
• Hydrocortisone (to replace steroid i.e. cortisol)
• Fludrocortisone (to replace mineralocorticoid i.e. aldosterone)
Presenter
Presentation Notes
Plasma cortisol is measured before and 30 and 60 minutes after injection of Synacthen, a synthetic ACTH analogue. In Addisons, cortisol at 60 minutes is low or there is an inadequate rise from baseline. Need to check other bloods too – may have a low glucose as well plus high potassium and calcium… Often given the hydrocortisone in the morning and both hydrocortisone and a dose of fludrocortisone in evening.

Conns: True or false?
• Patients with Conns have a high potassium?

FALSE
Presenter
Presentation Notes
Will be low most often, sometimes normal.
Conns(excess aldosterone)
• Presenting signs/symptoms:– Hypertension
– Hypokalaemia
– Hypernatraemia
– Aldosterone/renin ratio increased
Presenter
Presentation Notes
Hypertension with a low potassium should lead you to think of requesting the aldosterone (HIGH) renin (LOW) ratio to query Conns. The high aldosterone level increases reabsorption of sodium (salt) and water and the loss of potassium by the kidneys, resulting in high blood pressure Very low potassium may cause myopathy, polyuria, nocturia or rarely tetany.

Conns – causes…
• Tumour - unilateral adrenocortical adenoma– Excess aldosterone
– 60%
• Overgrowth – bilateral adrenal hyperplasia– 40%

Conns – Ix and Mx
• Iodine scanning
• CT/MRI
• Spironolactone (aldosterone antagonist)
• Surgical resection of tumour/hyperplasia

Phaeochromocytoma: true or false?
• It is associated with neurofibromatosis

TRUE

Phaeochromocytoma(Adrenal medulla tumour)
• Presenting signs/symptoms:– Episodic flushing
– Palpitations
– Sweating
– Headache
– Hypertension
– Pallor
Presenter
Presentation Notes
I generally try and think of a very panicked person, you know, perhaps me before a presentation…

Phaeochromocytoma - causes
• Unilateral, benign tumour– 90%
• Multiple, malignant tumours– 10%
• Secrete catecholamines: noradrenaline and adrenaline

Phaeochromocytoma – Ix and Mx
• 24hr urinary catecholamines x3– +ve then adrenal MRI and other scans
• Refer if suspected:– Adrenalectomy
– Phenoxybenzamine – α and β blockade required.
Presenter
Presentation Notes
Hypertension is mediated by alpha-adrenergic vasoconstriction. Tachycardia is mediated by the positively-inotropic effect of stimulation of beta-adrenergic receptors in the heart.

Phaeochromocytoma crisis
• Precipitants: – Beta blockers (unopposed)
– General anaesthetic
– Iv radiological contrast
– Opiates, TCAs, metoclopramide
• Hypertension, sweating, tachy’, arrythmias, HF
• Admit, correct dehydration immediately
Presenter
Presentation Notes
I think it would be difficult to decide if you were dealing with a crisis or an initial clinical presentation given the above list in comparison to the first…

The pituitary…
Kind of…(!)
Cushings: true or false?
• The commonest cause of Cushings is the administration of exogenous steroids.

TRUE

Cushings (excess cortisol)
• Presenting symptoms:– Weight gain– Recurrent infections– Depression– Low libido– Hirsuitism– Osteoporosis
Signs:– Moon face– Buffalo hump– Striae– Centripetal obesity– Proximal myopathy– Thin skin– Bruising– Hypertension

Cushings - causes
• Exogenous: iatrogenic, steroids, xs alcohol
• Pituitary overproduction of ACTH adrenals produce cortisol ++
• Cushing’s disease (pituitary tumour)
• Ectopic ACTH secretion by other tumours: Adrenal tumour/hyperplasia, small cell lung cancer
Presenter
Presentation Notes
Iatrogenic: doctors! Or more specifically medical treatment.
Cushings: Ix and Mx
• 24hr urinary collection – free cortisol• Low-dose dexamethasone suppression test:
confirm whether ACTH can be suppressed• High-dose dexamethasone suppression test:
differentiate between pituitary and ectopic ACTH secretion
• Treat the cause e.g. trans-sphenoidal surgery for Cushing’s disease, if syndrome then metyrapone, ketoconazole or adrenalectomy…
Presenter
Presentation Notes
Give dex’ at midnight then measure serum cortisol at 09.00 Low dose – give 0.5mg cortisol 6hourly for 48hr and should lead to complete suppression of cortisol – if not suppressed then likely Cushings

Thyroid…

Facial puffiness can be a sign of hypothyroidism?
True or False…

True

– Mentally slow
– Depression
– Psychosis (myxoedema madness)
– Lethargy
– Deafness
– Facial puffiness
– Husky voice
– Bilateral carpel tunnel
– Slow relaxing reflexes
– Non-pitting oedema
– Weight gain
– Cold intolerance
– Hair loss
– Dry skin
– Bradycardia
– Pericardial effusion
– Premature IHD
– Constipation
– Menstrual disturbance
• Menorrhagia (Fe def anaemia)
• Amenorrhoea (rarely)
Hypothyroid - Feats
Presenter
Presentation Notes
Hypothyroidism: common illness affecting 10% women >60yo, W:M 8:1 Autoimmune causes most commonly (hashimotos thyroiditis, atrophic hypothyroidism) Insideous onset, may go undiagnosed for years. Always consider hypothyroidism when a patient has non specific sx incl depression; fatigue; lethargy; or general malaise Other symptoms incl weight gain, constipation, hoarse voice, dry skin/hair. Signs are often absent- there may be goite, slow relaxing reflexes or non-pitting oedema of hands feet or eyelids

• TFTs– Who to investigate?
– with peristent sx of lethargy without clear cause
– on amiodarone
– h/o radioactive iodine use
– Those with
» hypercholestrolaemia, obesity
» infertility,
» depression & dementia,
» Diabetes and other autoimmune diseases,
» turners syndrome or congenital hypothyroidism.
Hypothyroid - Ix
Presenter
Presentation Notes
Investigate those with peristent sx of lethargy without clear cause. Those on amiodarone or with h/o radioactive iodine administration With hypercholestrolaemia, infertility, depression, dementia, obesity, Diabetes and other autoimmune diseases, turners syndrome or congenital hypothyroidism.
• Prescription costs
• <65 & healthy: – 150microg levothyroxine od
– Recheck TFTs 3/12
• Elderly or pre-exisiting heart disease– Start 25 microg levothyroxine od
– Increase every 4/52 as per TFTs
– ?Propranolol instead
Hypothyroid - Mx
Presenter
Presentation Notes
Remember those taking thyroid replacement medications are entitled to apply for free NHS prescriptions <65yo and healthy:150 micrograms od of levothyroxine, recheck TFTs after 3/12 and adjust dose to keep TSH in ‘normal ‘range, once dose is stable and TFTs acceptable monitor annually, or sooner if symptomatic or worries about compliance Elderly or pre-existing heart disease: start 25 microg od & increase dose every 4 weeks according to TFTs, consider adding propranolol if h/o IHD as levothyroxine can provoke angina. Withdrawal of levothyroxine: usually req’d lifelone, though if diagnosis is in doubt stop and re-measure TFTs after 4-6 weeks.

DeQuervains thyroiditis is the most common cause of hyperthyroidism?
True or False…

False…
Presenter
Presentation Notes
Graves Disease is the most common cause of hyperthyroidism accounting for 75% of cases

– Anxiety
– Palpitations
– Hyperactivity
– Irritability
– Wt loss
– Heat intolerance
– Hyperhidrosis
– Clubbing (very rare)
– Fine tremor
– Menstrual disturbance
– Infertility
– Alopecia
– Proximal myopathy
– Difficulty climbing stairs reaching for high up objects
– Heart failure due to
– AF
– Cardiomyopathy (rare)
– Diarrhoea
– Pretibial myxoedema
– Thyroid eye disease…
Hyperthyroid - features

Thyroid eye disease
Presenter
Presentation Notes
Patients with thyroid eye disease may present with: Double vision Eye discomfort +- protrusion (exopthalmos and proptosis) Lid lag Opthalmoplegia (esp of upward gaze) TFTs can by ^ or normal) Management: Refer to opthalmology, if reduced VA or loss of colour vision then refer urgently as there may be optic nerve compression

• TFTs
• Thyroid autoantibodies (thyroid peroxidase & anti-thryroglobulin Ab) – suggest autoimmune aetiology
• Endocrinologists may go on to do imaging (thyroid uptake scan/ 99Technetium scan) to help determine cause
Hyperthyroid - Ix

• Graves Disease
• Multinodular goitre
• Single hot nodule
• Thyroiditis
• Other
Hyperthyroid - Causes
Presenter
Presentation Notes
Graves:75% of cases. W 5:M 1, peak age 30-50yo. Associated with smoking and stressful life events. It is an autoimmune disease in which antibodies to the TSH receptor are produced. Can find a diffuse goitre +- thyroid bruit due to ^ vascularity Multinodular goitre:(15% of cases of hyperthryoidism, predominantly older women with h/o goitre) and Single hot nodules (5% of cases of hyperthryoid) both relapse after medical treatment and req surgical or radiotherapy. Thyroiditis:5% of cases of hyperthyroidism: Viral (DeQuervains) thyroiditis (eg mumps, coxsakie, adenovirus), see ^ESR, o/e painful enlarged thyroid, have ^ in T4 for 4-6/52 which normalises by 6/12 or is hypothyroid Other:1% cases: Drugs (eg amiodarone), excessive T4 replacement, extrathyroid T4: ovarian tumours (struma ovarii) hypothalamic-oituitary disease (eg pituitary tumour secreting TSH) Or hCG (human chorionic gonadotrophin) mediated stimulation of the thyroid
• Refer to endocrinology at presentation
• B-blockers
• Carbimazole
• Radioactive Iodine
• Surgey
Hyperthyroid - Mx
Presenter
Presentation Notes
Refer to endocrinology at presentation B-blockers (propranolol, atenolol) useful for sx control until anti-thyroid drug therapy takes effect Carbimazole – inhibits synthesis of thyroid hormones. Ineffective for treatment of thyroiditis. May be given short term to render a pt euthyroid prior to surgery/treatment with radioactive iodine or long term (12-18/12 in an attempt to induce remission (but >50% relapse. 3:1000 pts have serious ADR incl agranulocytosis, hepatitis, aplastic anaemia **must advise all patients starting carbimazole to stop the drug and seek urgent medical attention if they develop sore throat or other infection** Radioactive iodine: takes 3-4/12 to become apparent. Withdraw carbimazole >4/7 prior to treatment and do not restart until >3/7 after, women of child bearing age should avoid pregnancy for 4/12. Most become hypothyroid at some point and need regular TFTs. Associated with small increased risk of thyroid malignancy Surgery – partial or total thyroidectomy – reserved for pts with large goitres or who decline radioactive Iodine. Carries risk of damage to recurrent laryngeal nerve or parathyroids

Thyroid bruits are always present in thyrotoxic storm?
True or False…

False…
Presenter
Presentation Notes
They can be but not always
• Thyrotoxic storm:
– 2% of patients with hyperthyroidism
– Risk factors incl recent thyroid surgery or radioactive iodine, infection, trauma or MI
• Clinical features:
– Fever
– agitation +- confusion
– Coma
– tachycardia/AF
– D&V
– acute abdomen
– May have goitre +- thyroid bruits
• Mx: ADMIT to hospital as an emergency
Hyperthyroid - Emergency
Presenter
Presentation Notes
Thyrotoxic strom: Affects 2% of pts with hyperthyroidism Risk factors incl recent thyroid surgery or radioactive iodine infection trauma MI Clinical features: Fever agitation +- confusion coma tachycardia/AF D&V acute abdomen May have goitre +- thyroid bruits Mx: admit to hospital as an emergency, tretament must be strated before biochemical confirmation which takes too long, mainstay of treatment is high dose b-blockers with carbimazole, iodine, fluids and steroids
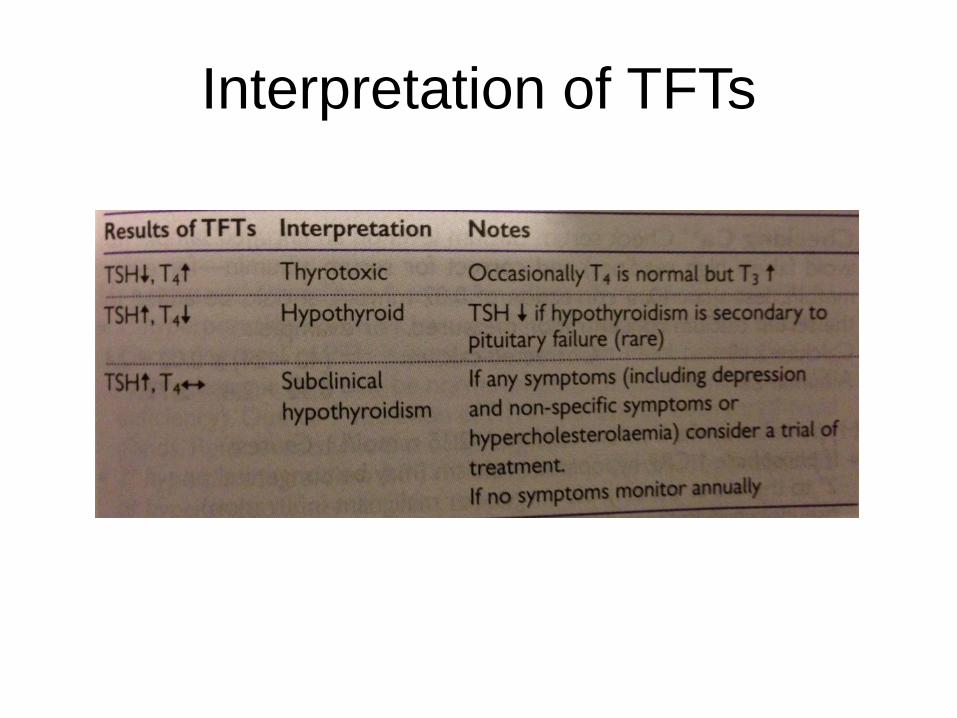
Interpretation of TFTs
• Pancreatitis can cause hypocalcaemia?
True or False…

True

• If PO4 increased:
– Chronic renal failure
– Hypoparathyroidism
– Pseudohypoparathyroidism
• If PO4 normal or low:
– Vit D def
– Malabsorption,
– Overhydration,
– Pancreatitis
Hypocalcaemia
Presenter
Presentation Notes
If PO4 incr: Chroninc renal failure Hypoparathyroidism (Congenital, 2ry to thyroid or parathyroid surgery, Malignant infiltration) Pseudohypoparathyroidism (insensitivity to parathyroid hormone) If PO4 normal or low: Vit D def (osteomalacia, rickets) Malabsorption, overhydration, pancreatitis

• Tetany
• Irritability, depression or psychosis
• Perioral parasthesia
• Carpopedal spasm
• Neuromuscular excitability (Chvostek’s sign)
Hypocalcaemia - Feats
Presenter
Presentation Notes
May be subtle, includes: Tetany Irritability, depression or psychosis Perioral parasthesia Carpopedal spasm (wrist flexion and fingers drawn together) Neuromuscular excitability (tapping over parotid causes facial muscles to contract – Chvostek’s sign) Apparent hypocalcaemia may be an artifact of hypoalbuminaemia
• Supplement with calcium
• Usually requires secondary care referral
Hypocalcaemia - Mx
Presenter
Presentation Notes
Supplement with calcium Secondary care referral is usually needed to investigate and treat the underlying cause

• Milk alkali syndrome is a recognised cause of hypercalcaemia?
True or False…
True
Presenter
Presentation Notes
True – an uncommon yet recognised cause

Hypercalcaemia
Common causes
• 1ry hyperparathyroidism
• Malignancy
• Chronic renal failure
Uncommon causes
• Familial benign hypercalcaemia
• Sarcoidosis
• Thyrotoxicosis
• Milk alkali syndrome
• Vitamin D treatment
Presenter
Presentation Notes
Common cuases include: Primary hyperparathyroidism Malignancy (10% tumours – usually myeloma, breast, lung, kidney, thyroid, prostate, ovary or colon) Chronic renal failure Uncommon causes include: Familial benign hypercalcaemia Sarcoidosis Thyrotoxicosis Milk alkali syndrome (usually due to the ingestion of OTC indigestion remedies Vitamin D treatment

Hypercalcaemia - Feats
• Tiredness
• Lethargy
• Weakness
• Mild aches and pains
• Anorexia
• Wt loss
• Low mood
• Stone formation
• N&V (often intractable)
• Polyuria & polydipsia
• Abdo pain
• Constipation
• Confusion
• Corneal calcification
‘Bones, stones, groans and abnormal moans’
Presenter
Presentation Notes
Often very non-specific, but if left untreated increasing serum calcium can be fatal, may be incidental finding. Remember ‘Bones, stones, groans and abnormal moans’ Tiredness Lethargy Weakness Mild aches and pains Anorexia Wt loss Low mood Stone formation N&V (often intractable) Polyuria & polydipsia Abdo pain Constipation Confusion Corneal calcification

• Treat underlying cause
• If calcium > 3.5 mmol/L or severe symptoms:– Admit
• Unclear diagnosis? - Refer endocrine
Hypercalcaemia - Mx
Presenter
Presentation Notes
Treat underlying cause, eg malignancy or hyperparathyroidism If calcium > 3.5 mmol/L or severe symtoms – admit for lowering of Ca2+ with forced diuresis & IV bisphosphonate If diagnosis unclear, refer endocrine (urgency depends on serum Ca and severity of symptoms

• Hyperparathyroidism is more common in men than women?
True or False…

True

• 1ry hyperparathyroidism:• Most common cause of hypercalcaemia
• 80% of cases caused by parathyroid adenoma
• Surgical intervention
• 2ry hyperparathyroidism:• response to chronic hypocalcaemia or
hypophosphataemia
• Mx is to treat underlying cause
Hyperparathyroidism
Presenter
Presentation Notes
It is the increased secretion of PTH 1ry hyperparathyroidism: Most common cause of hypercalcaemia Incidence 0.5/1000, peak age 40-60yo, M2:W1 Circulating level of PTH is inappropriately high, most patients are hypercalcaemic (but may be normocalcaemic if coexistent vit D def) Due to increased secretion of PTH from one or more parathyroid glands. In 80% the pathology is a single parathyroid adenoma Occasionally diffuse hyperplasia of all 4 glands occurs Very rarely Multiple Endocrine Neoplasia I or II are present Management – refer – surgical intervention 2ry hyperparathyroidism: ^ PTH in response to chronic hypocalcaemia or hypophosphataemia – Mx is to treat underlying cause
• Osteoporosis is defined by a T-score if > -2.5?
True or False…

True

• Definition:
Bone mineral density >2.5 standard deviations below the young adult mean (T score of -2.5)
Osteoporosis
Presenter
Presentation Notes
Bone mineral density >2.5 standard deviations below the young adult mean (T score of -2.5)

Osteoporosis – Risk factors
• Prev fracture (<50yo)
• FHx
• Female
• Increasing age
• Race
• Current smokers
• BMI <20 F & <25 M
• Excessive alcohol & caffeine
• Immobility
• H/o falls
• Low calcium and vitamin-D intake
• Medications
• Untreated hypogonadism
Presenter
Presentation Notes
The risks of osteoporosis and fragility fractures include the following: history of fracture (incl low trauma <age 50yo) family history (may be genetic link) Females are at a greater risk of osteoporosis, however, secondary causes of osteoporosis are more common in menIncreasing age – as BMD decreases with age the risk of osteoporosis increases Caucasian & Asian current smokers BMI <20 women and <25 men excessive consumption of alcohol, caffeine lack of physical activity and immobility history of fallslow calcium and vitamin-D intake medications (androgen deprivation therapy anticonvulsants glucocorticoids high dose thyroxine) untreated hypogonadism in men and women e.g. - premature menopause, bilateral oophorectomy or orchidectomy, inflammatory bowel disease, thyroid disorders

• Often diagnosed after pathological fracture
• Bone mineral density measurement/DEXA
• FRAX
Osteoporosis - Ix
Presenter
Presentation Notes
often diagnosed clinically following a pathological fracture, usually of the distal radius, spine or hip. These can be low impact fractures – occuring from a fall at or below standing height Bone mineral density (BMD) measurement has been used to predict risk of fracture and diagnose osteoporosis. BMD at the femoral neck is used as the reference The WHO define osteoporosis as a bone mineral density of 2.5 standard deviations or more below the young female adult mean (ie a T score < or = to -2.5) This definition however encompasses a large proportion of the elderly population and it is therefore not the only consideration in determining treatment. In addition to bone mineral density, one needs to consider the patients other risk factors which are independent of bone mineral density e.g. - previous fragility fracture, maternal history of hip fracture, risk factors for falling and increased levels of bone resorption markers. Clinical risk factors used in the WHO FRAX tool include: current age Gender prior osteoporotic fracture prior clinical vertebral fracture or a hip fracture is an especially strong risk factor femoral neck BMD low body mass index oral glucocorticoids for more than 3 months at a dose of prednisolone of 5mg daily or more (or equivalent doses of other glucocorticoids) current smoking parental history of hip fracture alcohol intake (3 or more units a day) rheumatoid arthritis secondary osteoporosis e.g. - type I diabetes, untreated long-standing hyperthyroidism, hypogonadism or premature menopause (<45 years), chronic malnutrition, or malabsorption etc.

• Lifestyle advice
• Falls risk assessment
• Hip protectors
• Medications:
– Calcium & vit D supps
– Bisphosphonates
– Raloxifene
– Strontium
– HRT
• NICE guideline
Osteoporosis - Mx
Presenter
Presentation Notes
Management of osteoporosis is not generic and varies dependent on multiple factors – rather than regurgitating NICE guidelines may we suggest reviewing these indivisually

Picture round…
Diagnose the following clinical features and with what illness
are they usually linked to?

Picture1
Presenter
Presentation Notes
Depression: Hypothyroid, hypo&hypercalcaemia

Picture 2
Presenter
Presentation Notes
Alopecia Hyperthyroid

Picture 3
Presenter
Presentation Notes
Hyperpigmentation: Addisons

Picture 4
Presenter
Presentation Notes
Abdominal striae: Cushings

Picture 5
Presenter
Presentation Notes
Facial puffiness Hypothyroidism

Picture 6
Presenter
Presentation Notes
Corneal ulcer: 2ry to thyroid eye disease (hyperthyroidism)

Picture 7
Presenter
Presentation Notes
Moon face: Cushings

Picture 8
Presenter
Presentation Notes
Chvostek’s sign: Hypocalcaemia
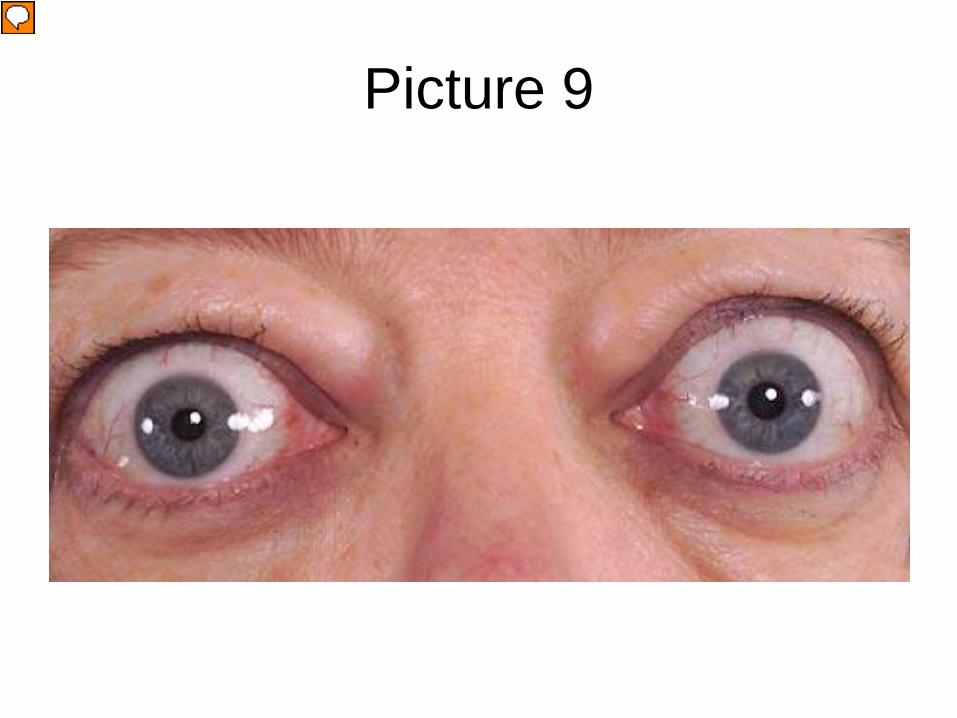
Picture 9
Presenter
Presentation Notes
Proptosis: hyperthyroid

• AKT style questions…
Interactive group work

References
• Oxford Handbook of Endocrinology and Diabetes
• Oxford Handbook of General Practice
• GP notebook
• Medicine at a Glance
• www.labtestsonline.org.uk
Related Documents











