Ending Pandemics Ini.a.ve Adam W. Crawley, MPH ISDS Webinar – January 22, 2016

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
EndingPandemicsIni.a.ve
AdamW.Crawley,MPHISDSWebinar–January22,2016
SkollGlobalThreats–EndingPandemics• OurApproach• FasterDetec0onandRepor0ngThroughNovel
SurveillanceSystems• Verifica0onThroughCrowdsourcedEpidemicIntelligence• Coordina0onThroughRegionalDiseaseSurveillance
Networks• AssessingProgressThroughMeasurement
SGTFApproachforEndingPandemics
• Ourvisionistoendpandemics.Weworktodecreasethelikelihoodofapandemiceventoccurringbyshorteningthe0mefromoutbreakstarttodetec0on,withafocusondiseasehotspots,whereviruseswithpandemicpoten0alarelikelytoemerge.
• Weaimtoachievethisbyenablingpartners,throughtheuseofinnova0veapproaches,to:
• Quicklycaptureandshareinforma0ontodetecthuman&animaloutbreaks;• Trainandlinkfieldepidemiologiststoverifyoutbreaksfaster;and• Supportandconnectregionaldiseasesurveillancesystemstoencouragecollabora0on
betweenna0onalpublichealthsystems.
• Ourhypothesisisthatindividualprojects,leveragingnewtechnologiesandinnova0veapproaches,willspreadbeyondpilotcountriesthroughregionalsurveillancenetworksandotherconvenings.
1. We are measuring global baseline in more detail to determine best impact measure
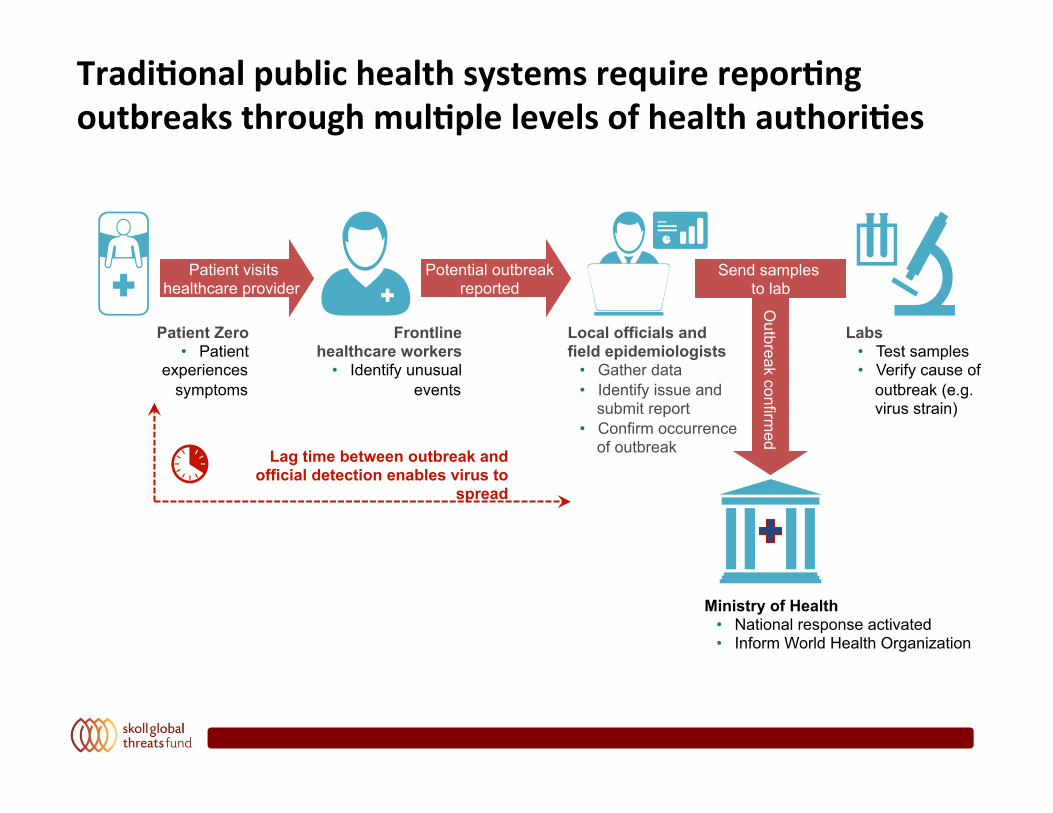
Tradi.onalpublichealthsystemsrequirerepor.ngoutbreaksthroughmul.plelevelsofhealthauthori.es
Patient Zero • Patient
experiences symptoms
Frontline healthcare workers
• Identify unusual events
Local officials and field epidemiologists
• Gather data • Identify issue and
submit report • Confirm occurrence
of outbreak
Labs • Test samples • Verify cause of
outbreak (e.g. virus strain)
Ministry of Health • National response activated • Inform World Health Organization
Potential outbreak reported
Patient visits healthcare provider
Outbreak confirm
ed Send samples
to lab
Lag time between outbreak and official detection enables virus to
spread
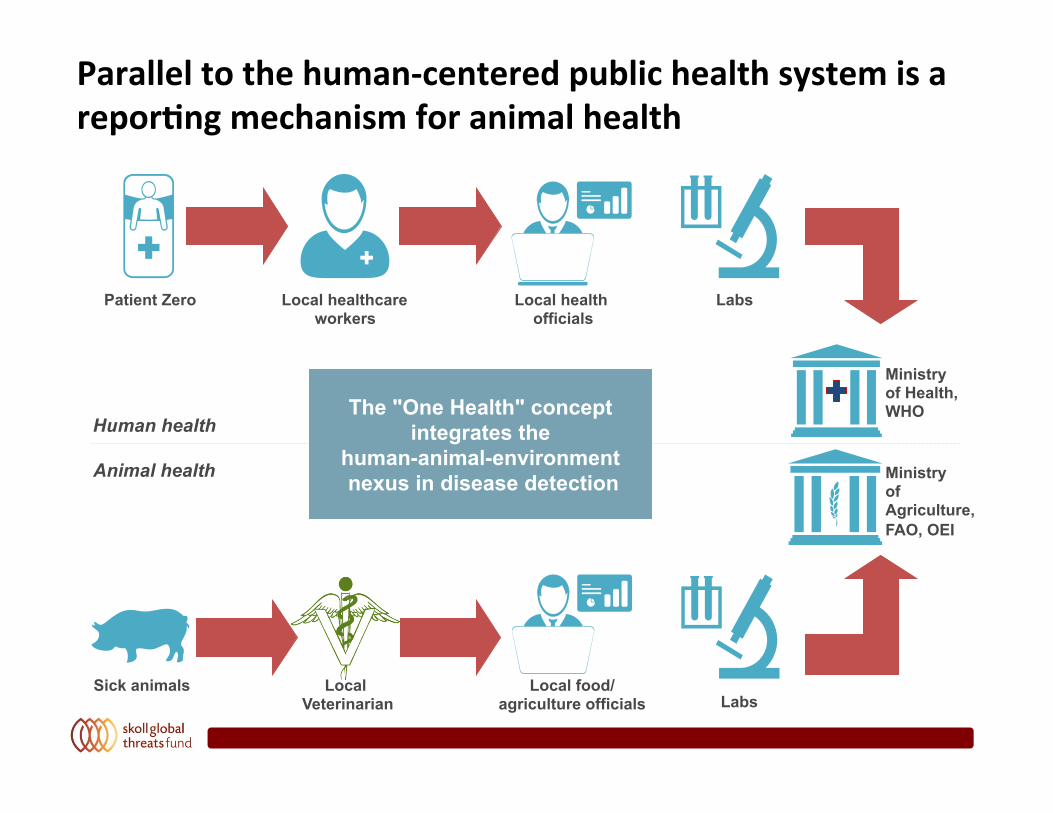
Paralleltothehuman-centeredpublichealthsystemisarepor.ngmechanismforanimalhealth
Patient Zero Local health officials
Labs
Sick animals Local Veterinarian Labs
Local healthcare workers
Local food/ agriculture officials
Ministry of Health, WHO
Ministry of Agriculture, FAO, OEI
Human health
Animal health
The "One Health" concept integrates the
human-animal-environment nexus in disease detection
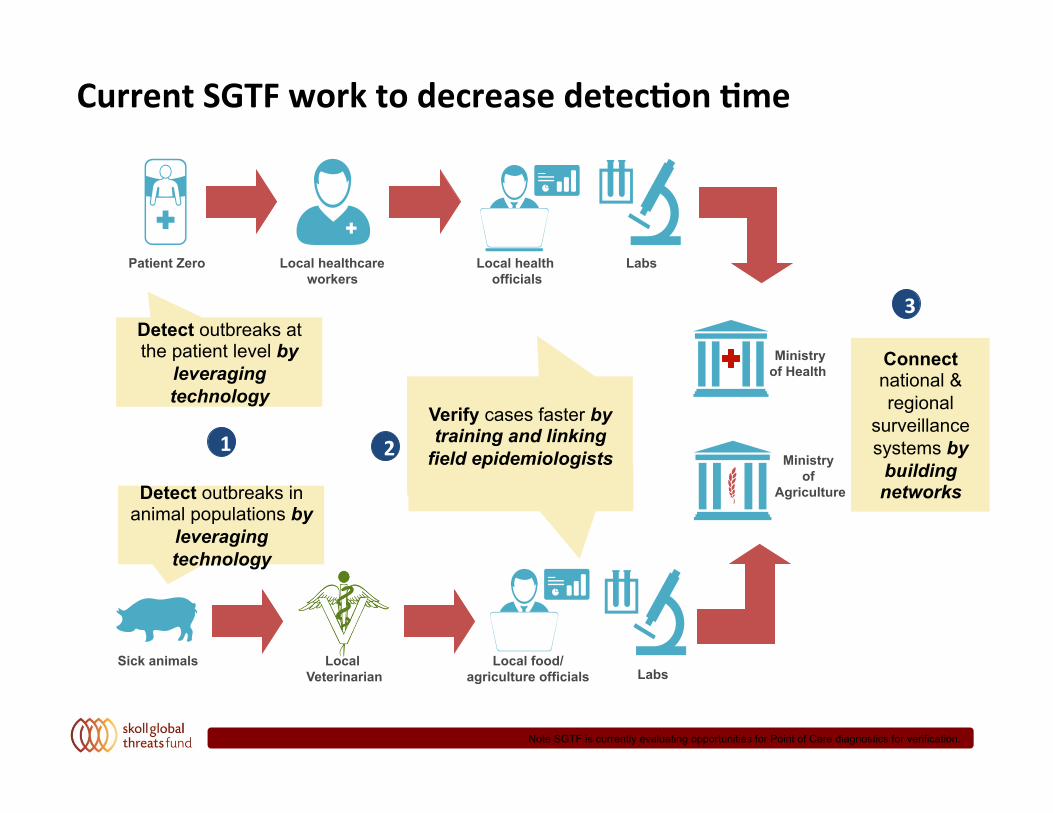
CurrentSGTFworktodecreasedetec.on.me
Note SGTF is currently evaluating opportunities for Point of Care diagnostics for verification.
Connect national & regional
surveillance systems by
building networks
Patient Zero Local health officials
Labs
Sick animals Local Veterinarian Labs
Local healthcare workers
Local food/ agriculture officials
Ministry of Health
Ministry of
Agriculture
Detect outbreaks at the patient level by
leveraging technology
Detect outbreaks in animal populations by
leveraging technology
Verify cases faster by training and linking
field epidemiologists 1 2
3
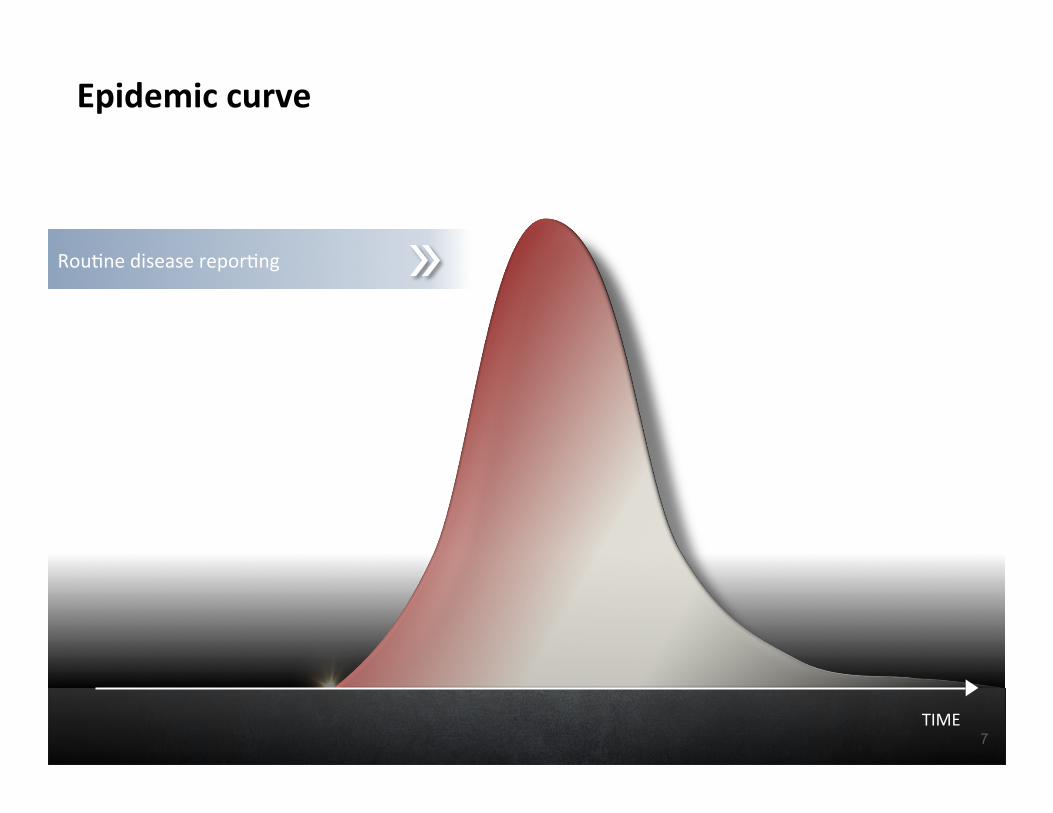
Epidemiccurve
Rou0nediseaserepor0ng
TIME
CASES
7
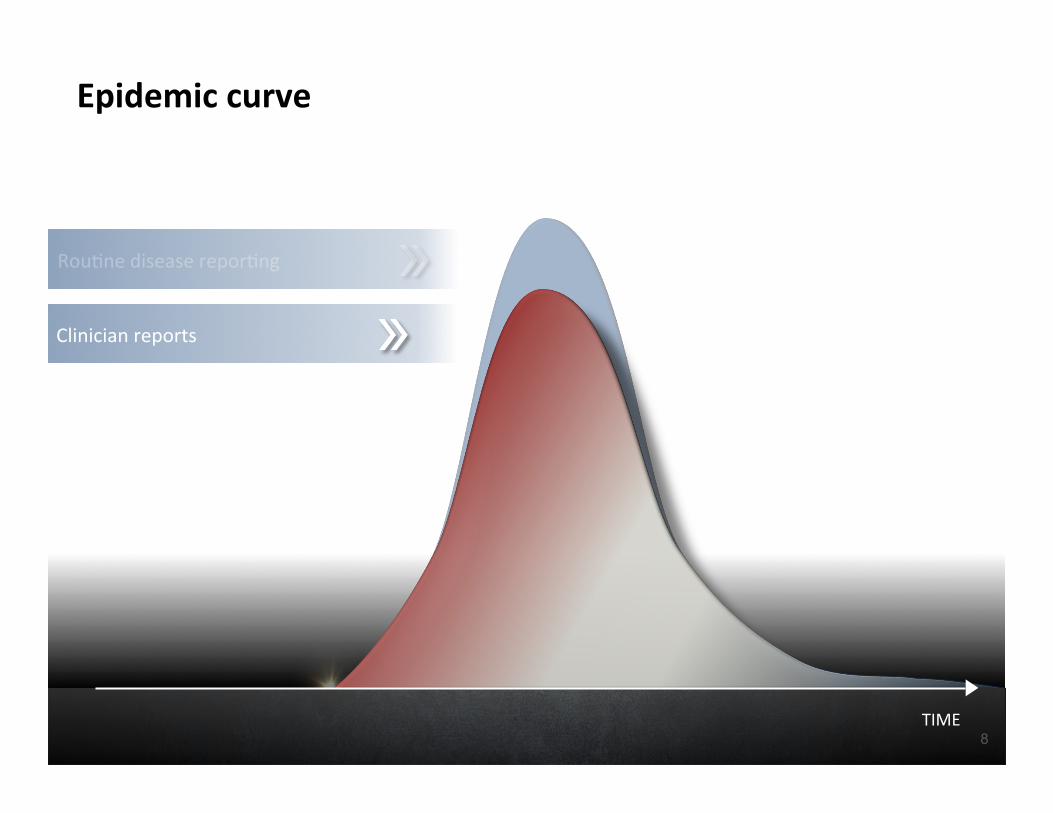
Epidemiccurve
Rou0nediseaserepor0ng
Clinicianreports
TIME
CASES
8
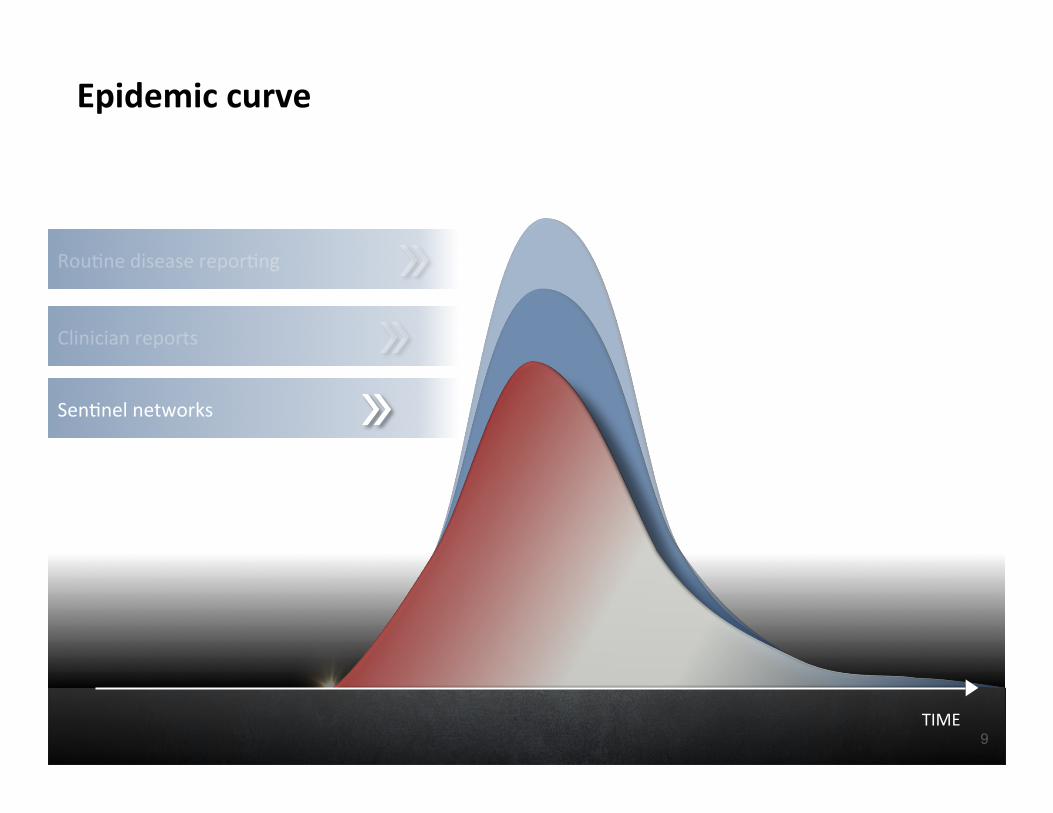
Epidemiccurve
Rou0nediseaserepor0ng
Clinicianreports
Sen0nelnetworks
TIME
CASES
9
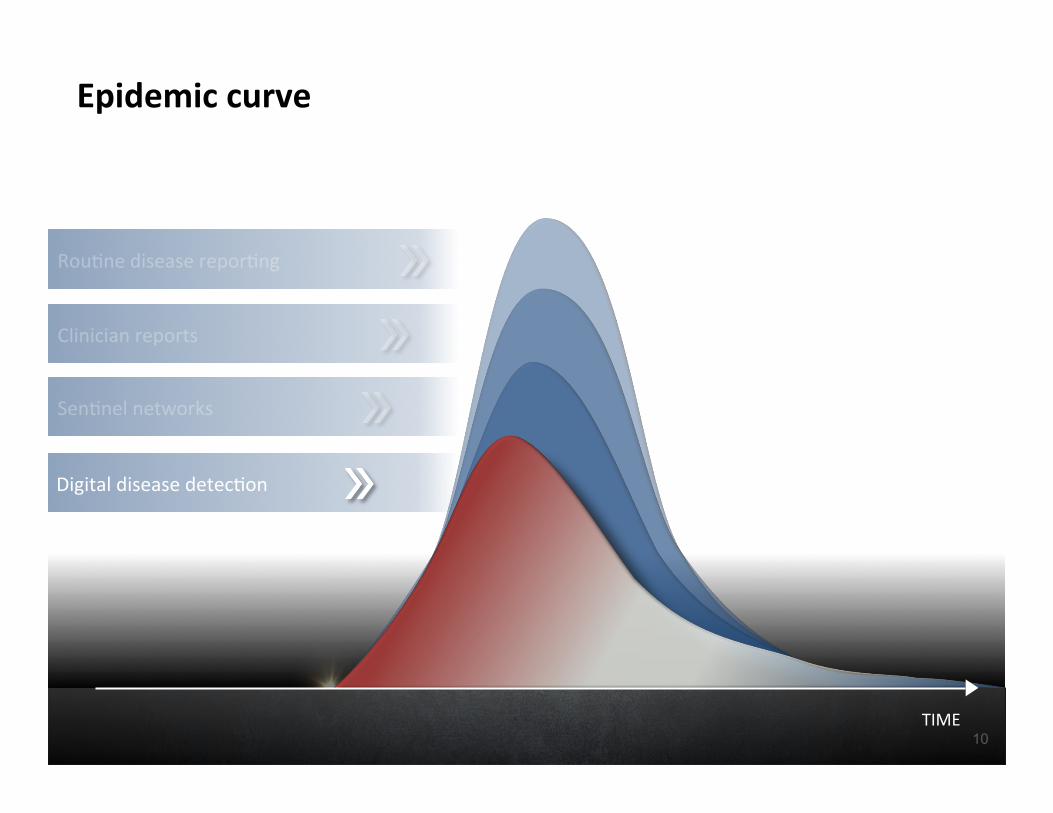
Epidemiccurve
Rou0nediseaserepor0ng
Clinicianreports
Sen0nelnetworks
Digitaldiseasedetec0on
TIME
CASES
10
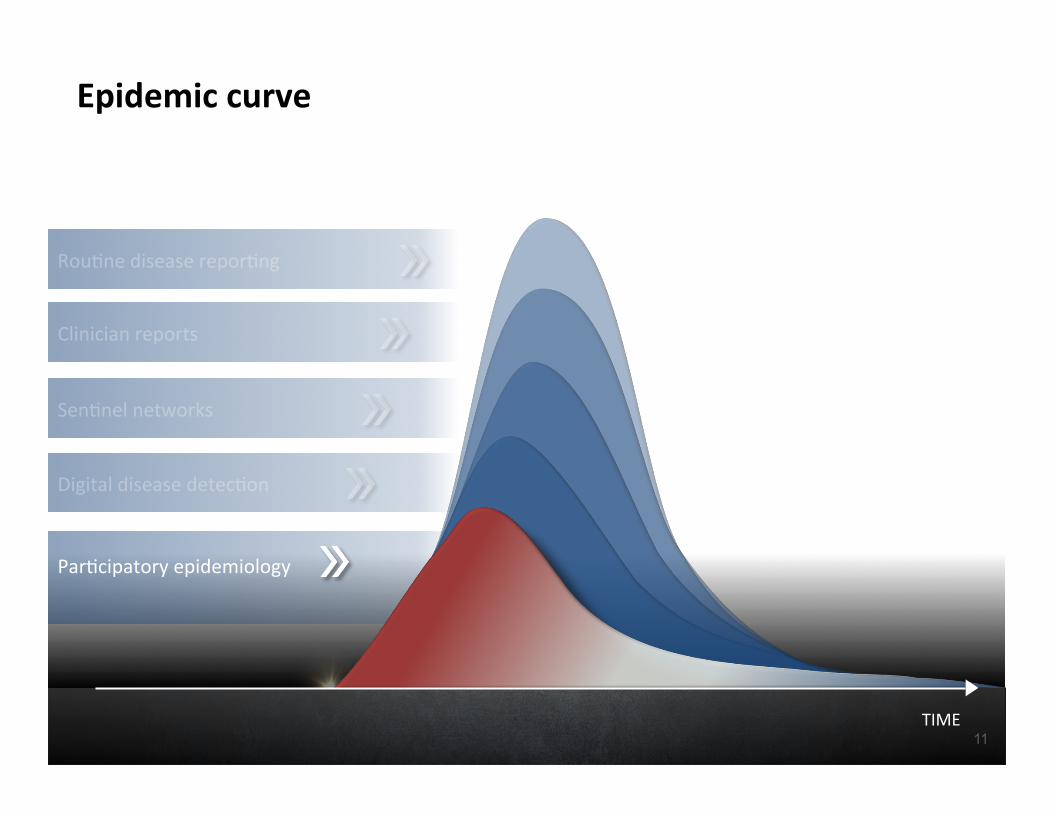
Epidemiccurve
Rou0nediseaserepor0ng
Clinicianreports
Sen0nelnetworks
Digitaldiseasedetec0on
Par0cipatoryepidemiology
TIME
CASES
11
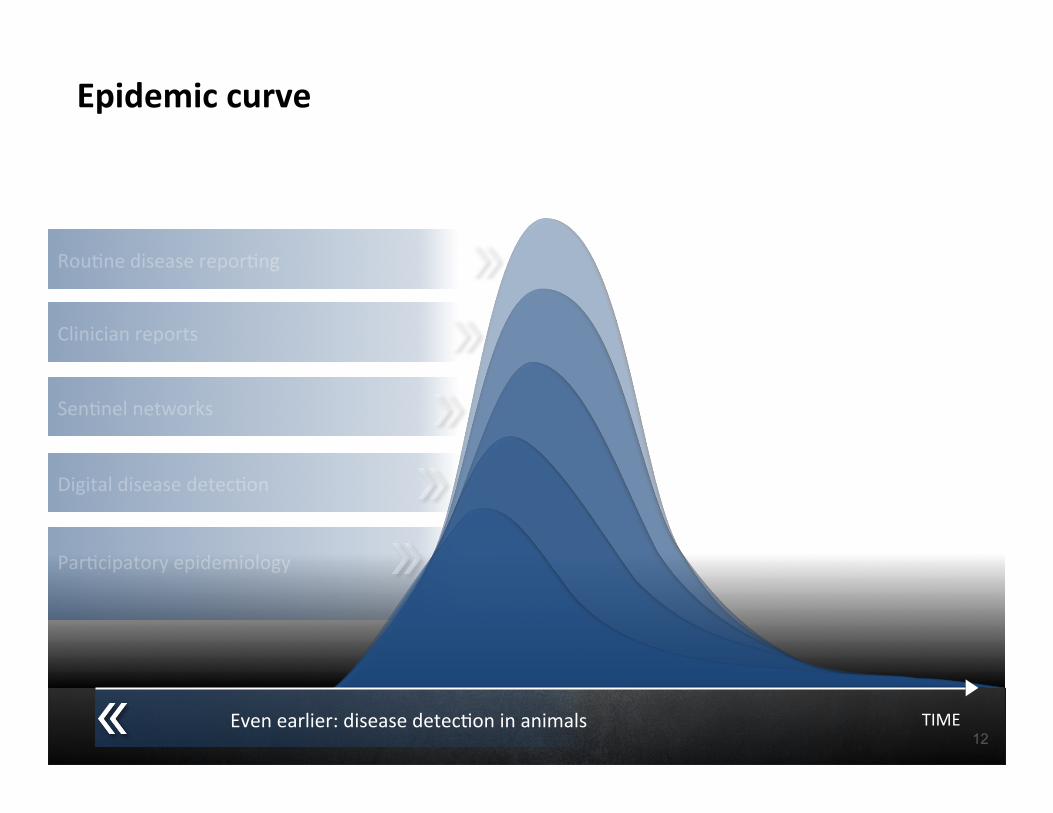
Epidemiccurve
Rou0nediseaserepor0ng
Clinicianreports
Sen0nelnetworks
Digitaldiseasedetec0on
Par0cipatoryepidemiology
TIME
CASES
Evenearlier:diseasedetec0oninanimals12
Fondation Mérieux, in partnership with the Ministry of Health of Senegal and PATH, is building a scalable mobile phone and web platform to transfer epidemiological data from 120 medical laboratories across Senegal to the Ministry of Health (MoH) to shorten the time between detection and response to reduce biothreats and stop pandemics.
FasterLaboratoryRepor.ngUsingMobile
Digital,informalsurveillancesystemsaregenera0nganincreasingamountofsignalsEpiCorewilllinkvolunteerepidemiologiststovalidateearlysignalsofdiseaseoutbreaksFieldEpidemiologyTrainingProgramsin55countrieswillhaveaccesstotrainingindigitaldiseasedetec0onmethods
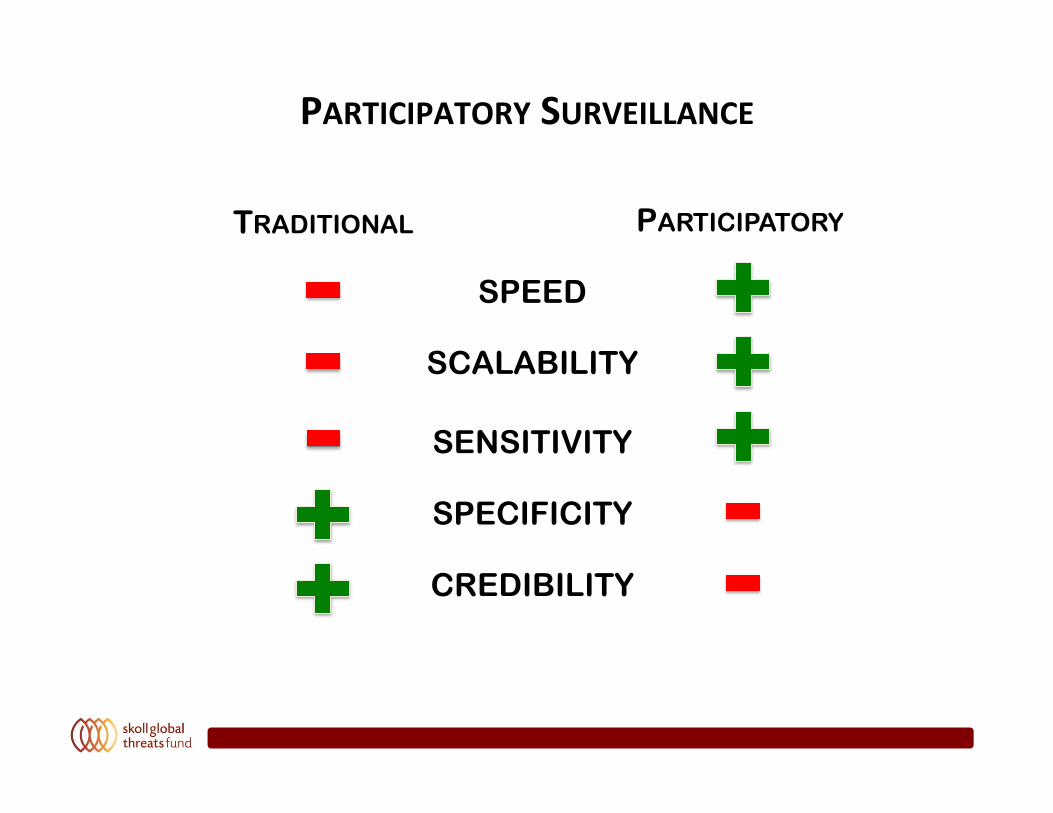
PARTICIPATORYSURVEILLANCE
TRADITIONAL PARTICIPATORY
SPEED
SCALABILITY
SENSITIVITY
SPECIFICITY
CREDIBILITY
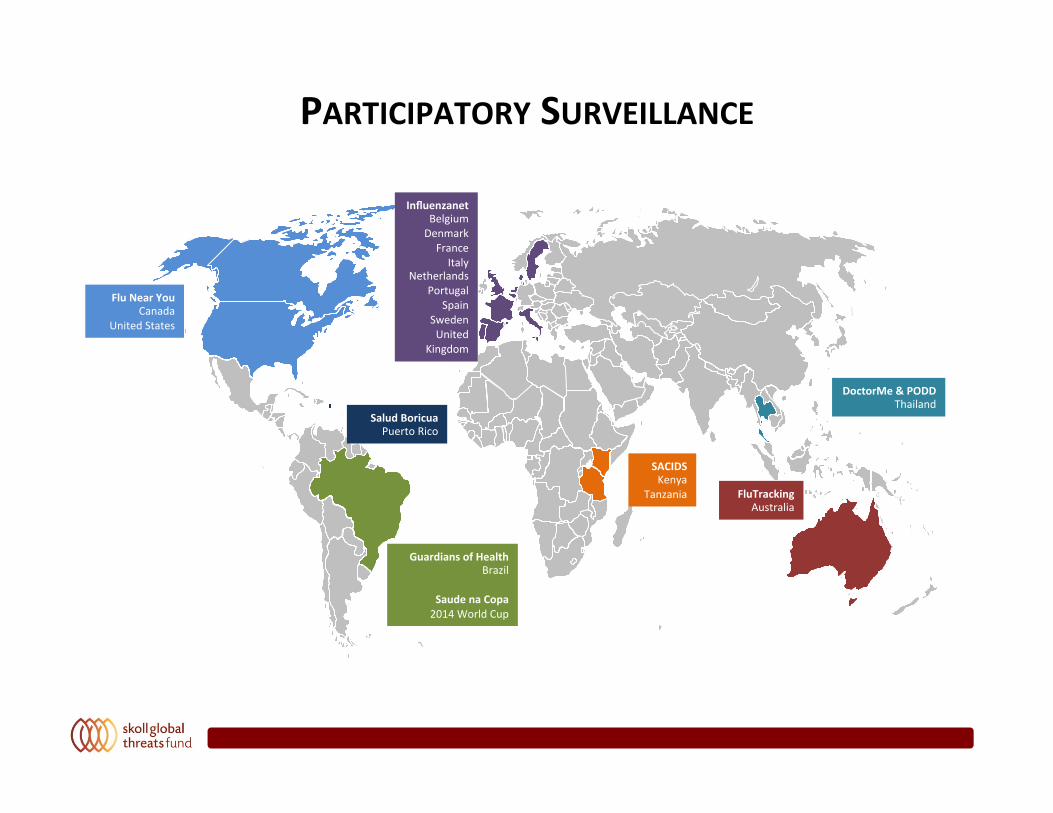
PARTICIPATORYSURVEILLANCE
InfluenzanetBelgiumDenmarkFranceItaly
NetherlandsPortugal
SpainSwedenUnited
Kingdom
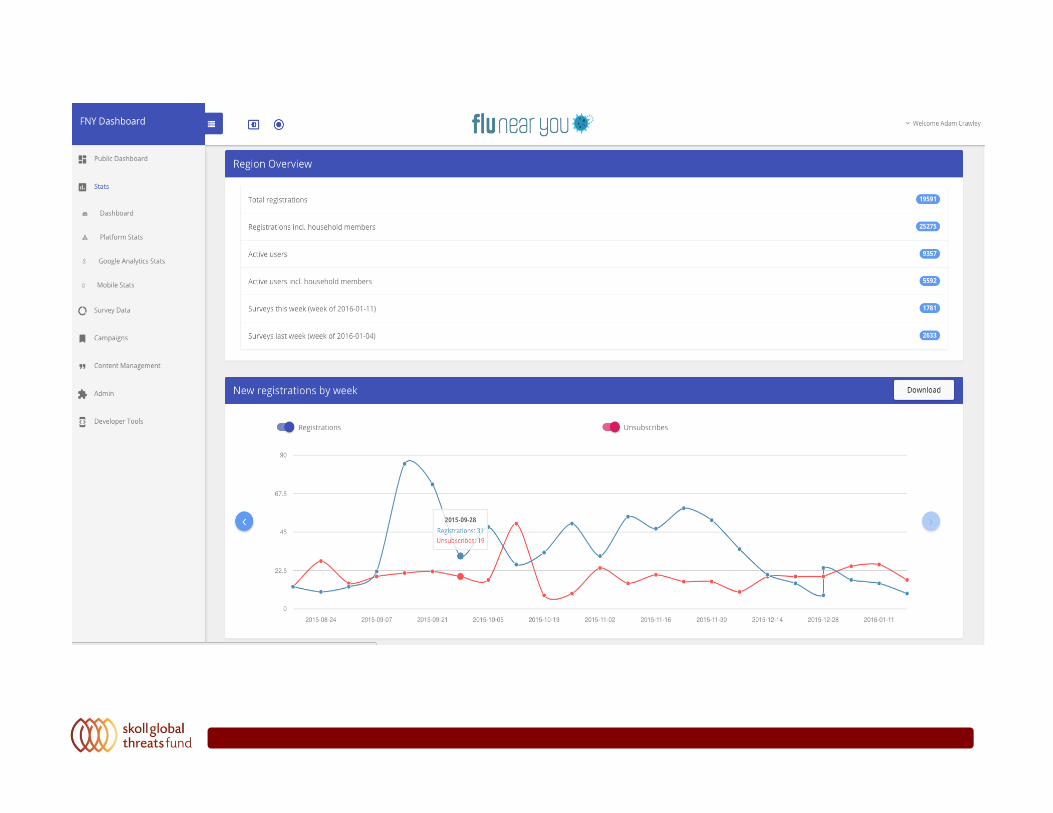
FluNearYouCanada
UnitedStates
GuardiansofHealthBrazil
SaudenaCopa2014WorldCup
SACIDSKenya
Tanzania
DoctorMe&PODDThailand
FluTrackingAustralia
SaludBoricuaPuertoRico

MassGatheringPar.cipatorySurveillanceinBrazil
World Cup 2014 & Olympics 2016
BrazilMinistryofHealthhaschampionedtheWorldCuppilottoengagefanstoreportsymptomsofillness
SGTFisleadingdiscussionswiththeInterna.onalOlympicsCommi\eetobuild
onthissuccessforthe2016gamesinRio

MassGatheringPar.cipatorySurveillanceinBrazil
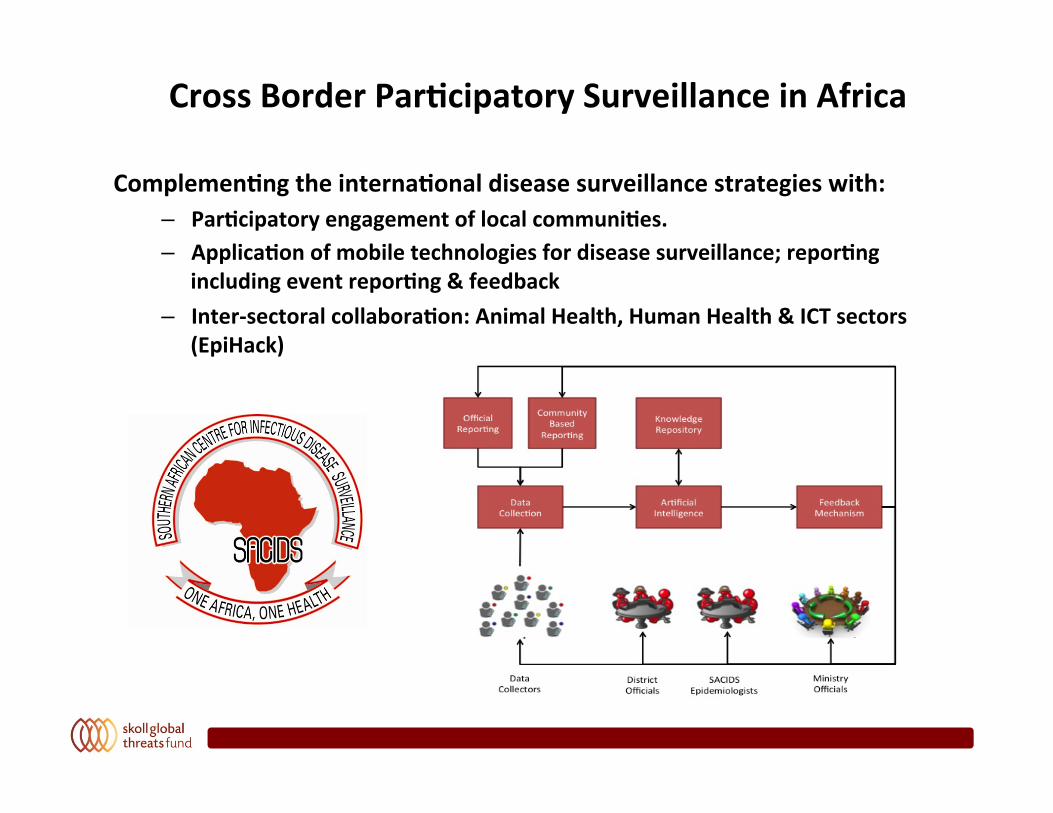
CrossBorderPar.cipatorySurveillanceinAfrica
Complemen.ngtheinterna.onaldiseasesurveillancestrategieswith:– Par.cipatoryengagementoflocalcommuni.es.– Applica.onofmobiletechnologiesfordiseasesurveillance;repor.ng
includingeventrepor.ng&feedback– Inter-sectoralcollabora.on:AnimalHealth,HumanHealth&ICTsectors
(EpiHack)
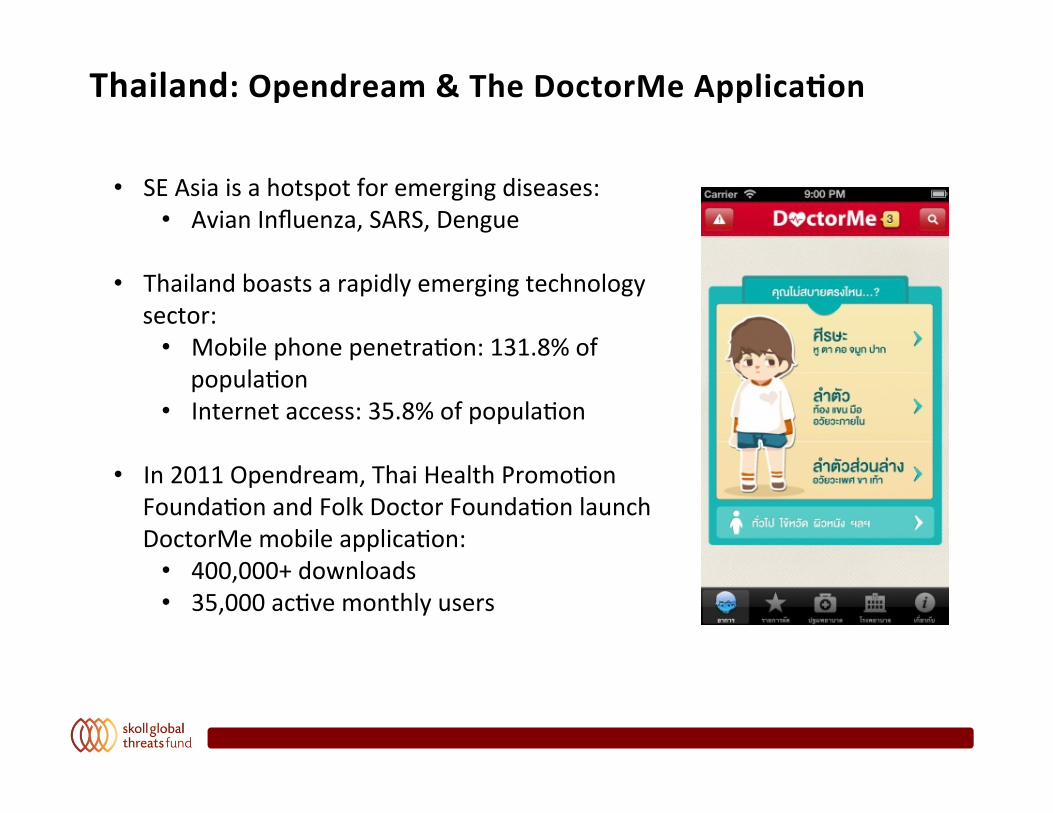
Thailand:Opendream&TheDoctorMeApplica.on
• SEAsiaisahotspotforemergingdiseases:• AvianInfluenza,SARS,Dengue
• Thailandboastsarapidlyemergingtechnologysector:
• Mobilephonepenetra0on:131.8%ofpopula0on
• Internetaccess:35.8%ofpopula0on
• In2011Opendream,ThaiHealthPromo0onFounda0onandFolkDoctorFounda0onlaunchDoctorMemobileapplica0on:
• 400,000+downloads• 35,000ac0vemonthlyusers
!
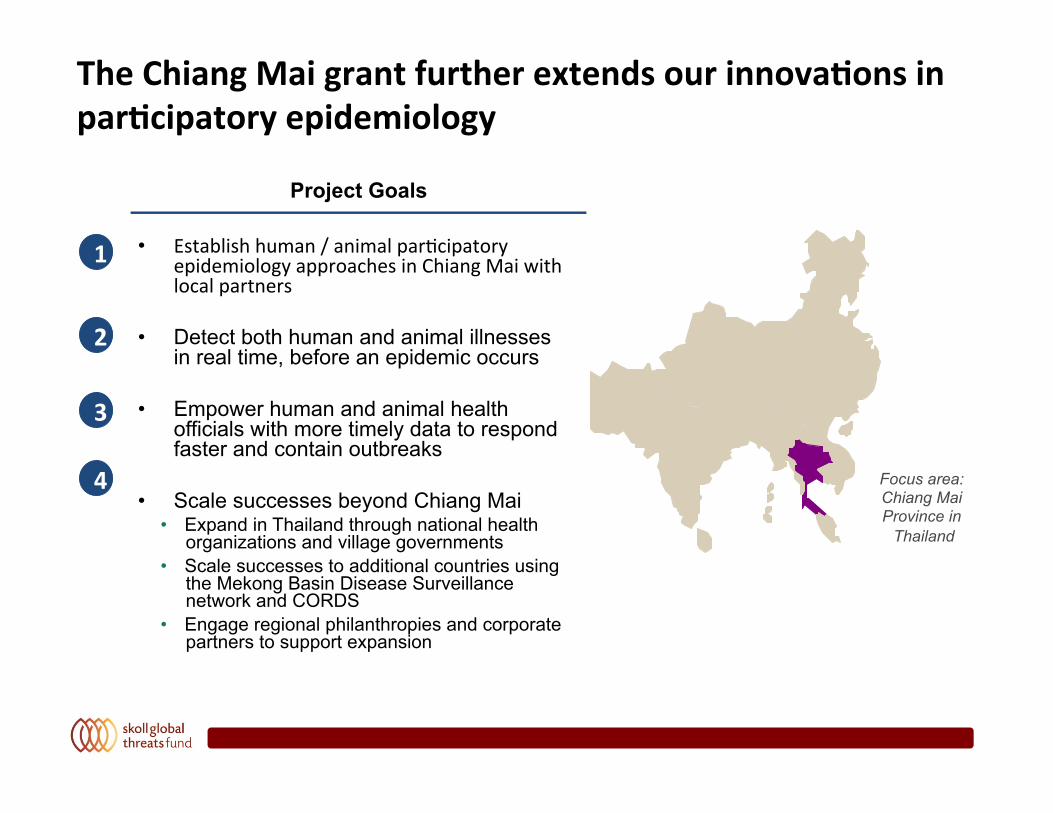
TheChiangMaigrantfurtherextendsourinnova.onsinpar.cipatoryepidemiology
• Establishhuman/animalpar0cipatoryepidemiologyapproachesinChiangMaiwithlocalpartners
• Detect both human and animal illnesses in real time, before an epidemic occurs
• Empower human and animal health officials with more timely data to respond faster and contain outbreaks
• Scale successes beyond Chiang Mai • Expand in Thailand through national health
organizations and village governments • Scale successes to additional countries using
the Mekong Basin Disease Surveillance network and CORDS
• Engage regional philanthropies and corporate partners to support expansion
Focus area: Chiang Mai Province in
Thailand
1
2
3
4
Project Goals
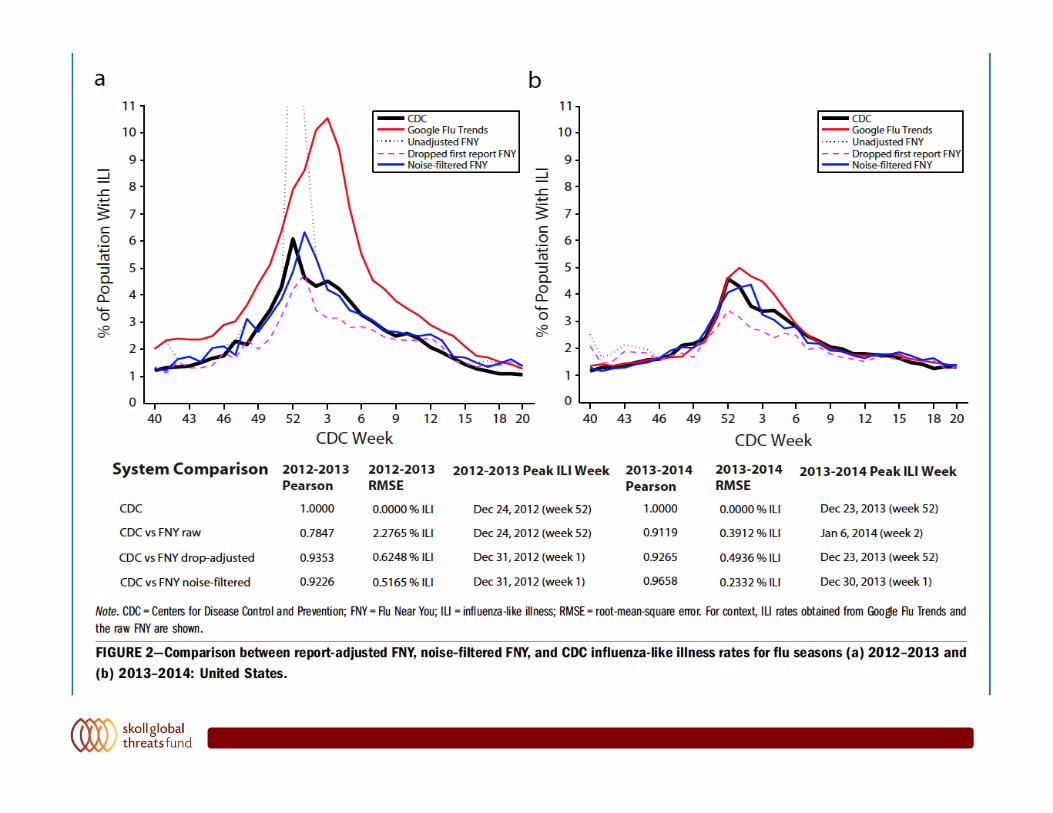
Smolinskietal.(2015)AmericanJournalofPublicHealth
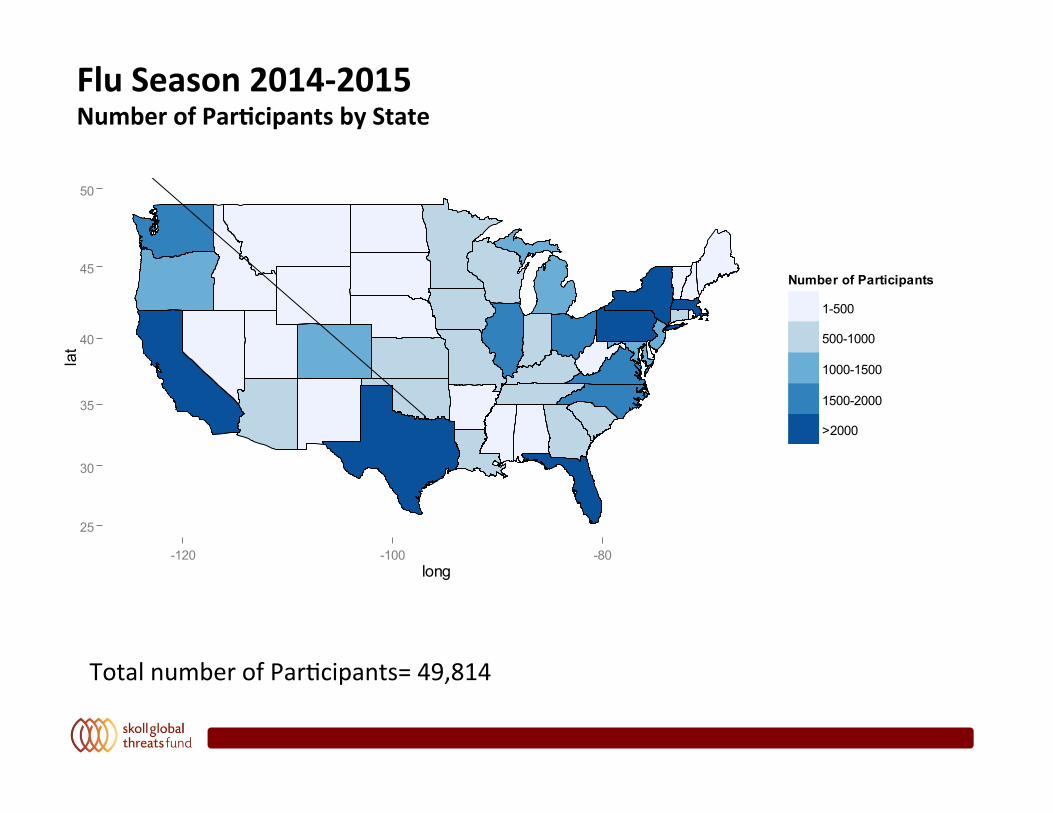
FluSeason2014-2015NumberofPar.cipantsbyState
25
30
35
40
45
50
-120 -100 -80long
lat
Number of Participants
1-500
500-1000
1000-1500
1500-2000
>2000
TotalnumberofPar0cipants=49,814
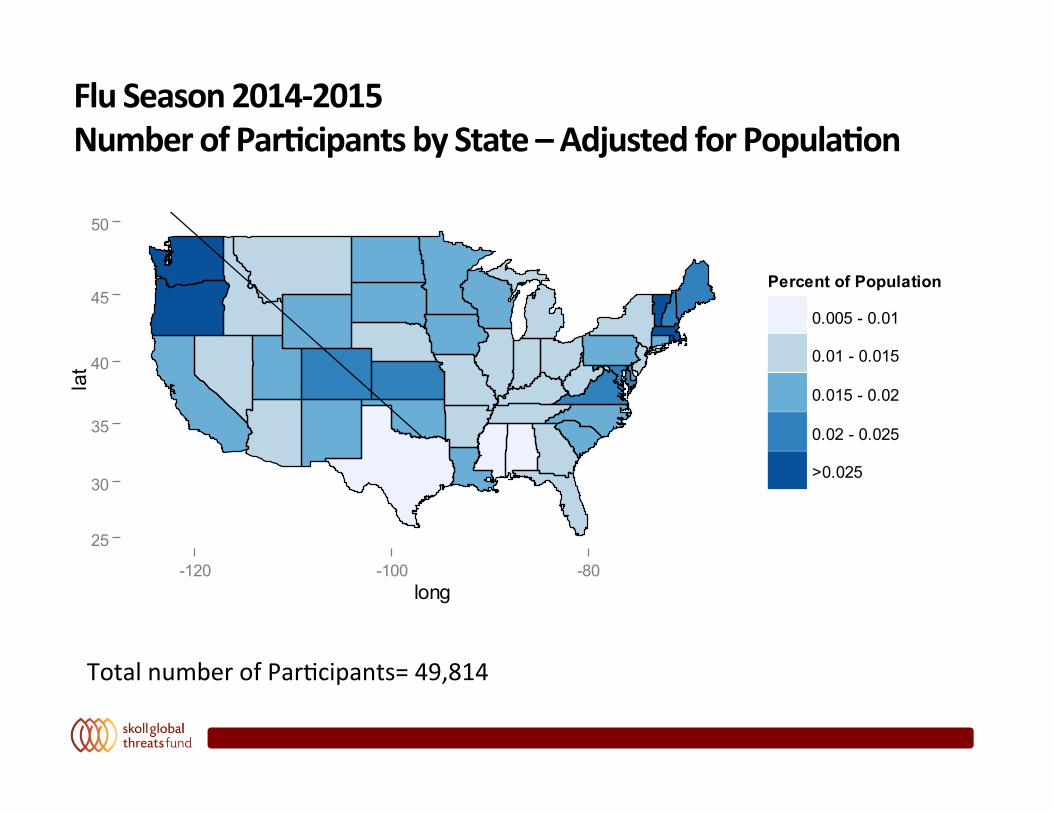
FluSeason2014-2015NumberofPar.cipantsbyState–AdjustedforPopula.on
TotalnumberofPar0cipants=49,814
25
30
35
40
45
50
-120 -100 -80long
lat
Percent of Population
0.005 - 0.01
0.01 - 0.015
0.015 - 0.02
0.02 - 0.025
>0.025
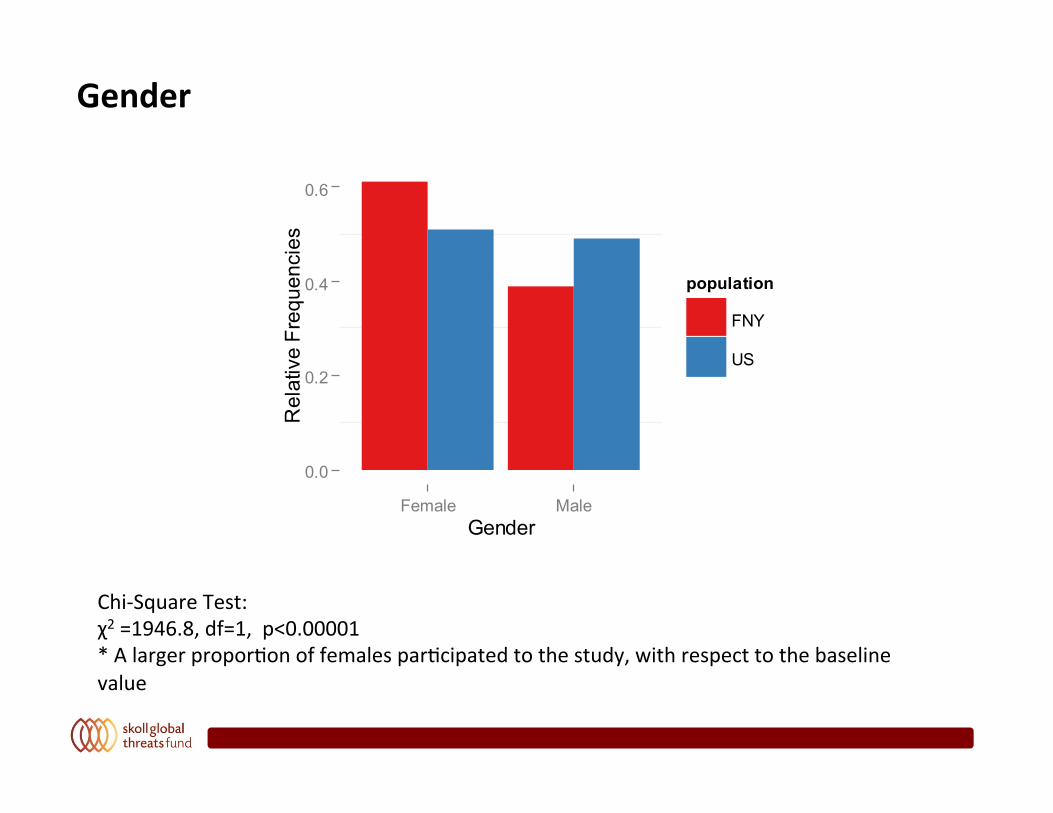
Gender
Chi-SquareTest:χ2=1946.8,df=1,p<0.00001*Alargerpropor0onoffemalespar0cipatedtothestudy,withrespecttothebaselinevalue
0.0
0.2
0.4
0.6
Female MaleGender
Rel
ativ
e Fr
eque
ncie
spopulation
FNY
US
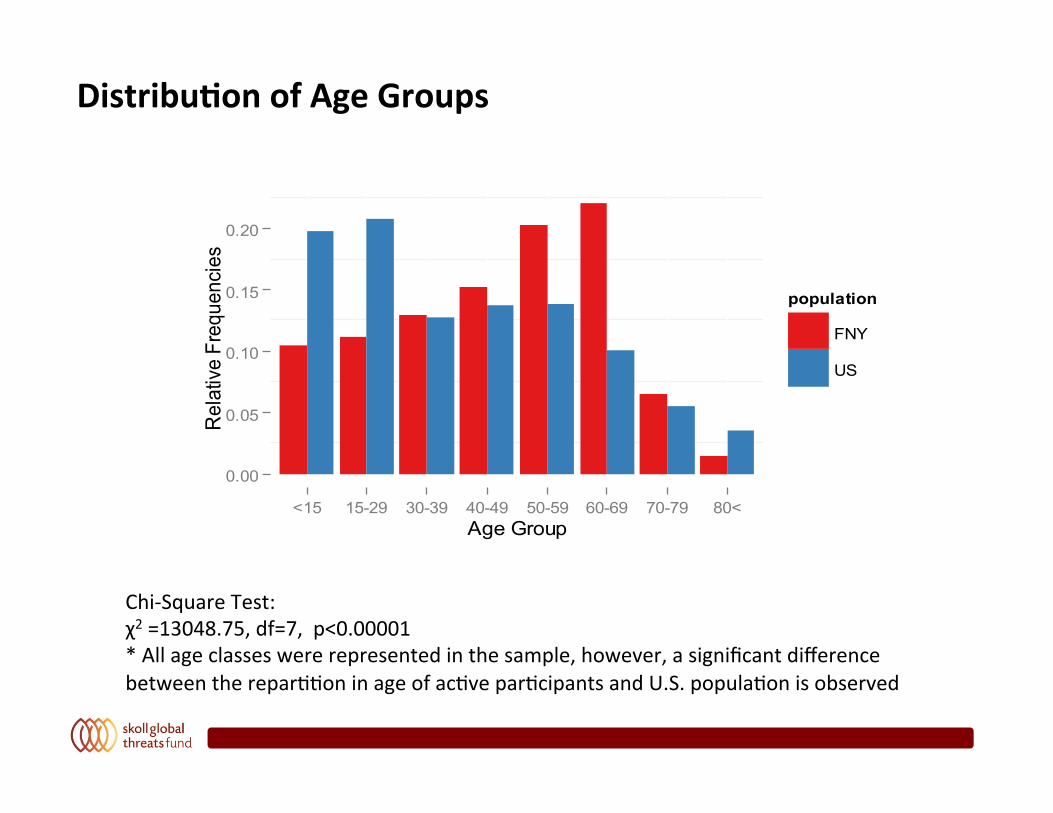
Distribu.onofAgeGroups
Chi-SquareTest:χ2=13048.75,df=7,p<0.00001*Allageclasseswererepresentedinthesample,however,asignificantdifferencebetweentherepar00oninageofac0vepar0cipantsandU.S.popula0onisobserved
0.00
0.05
0.10
0.15
0.20
<15 15-29 30-39 40-49 50-59 60-69 70-79 80<Age Group
Rel
ativ
e Fr
eque
ncie
s
population
FNY
US
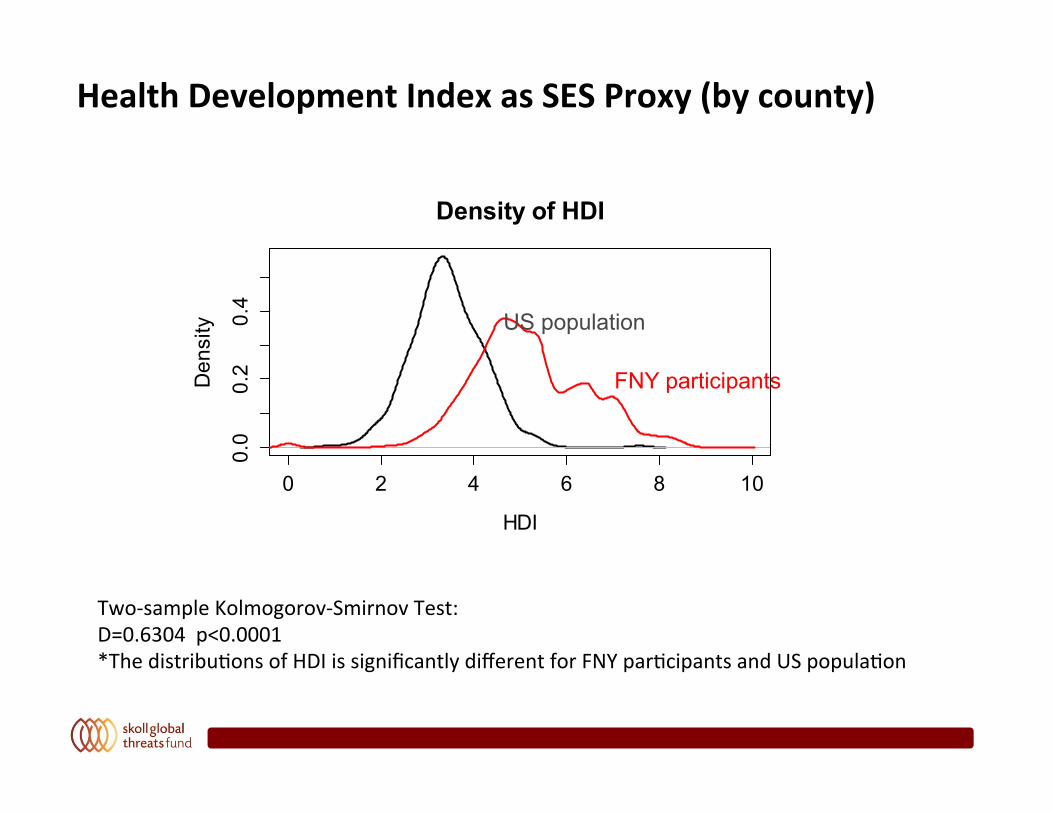
HealthDevelopmentIndexasSESProxy(bycounty)
Two-sampleKolmogorov-SmirnovTest:D=0.6304p<0.0001*Thedistribu0onsofHDIissignificantlydifferentforFNYpar0cipantsandUSpopula0on
0 2 4 6 8 10
0.0
0.2
0.4
Density of HDI
HDI
Density US population
FNY participants
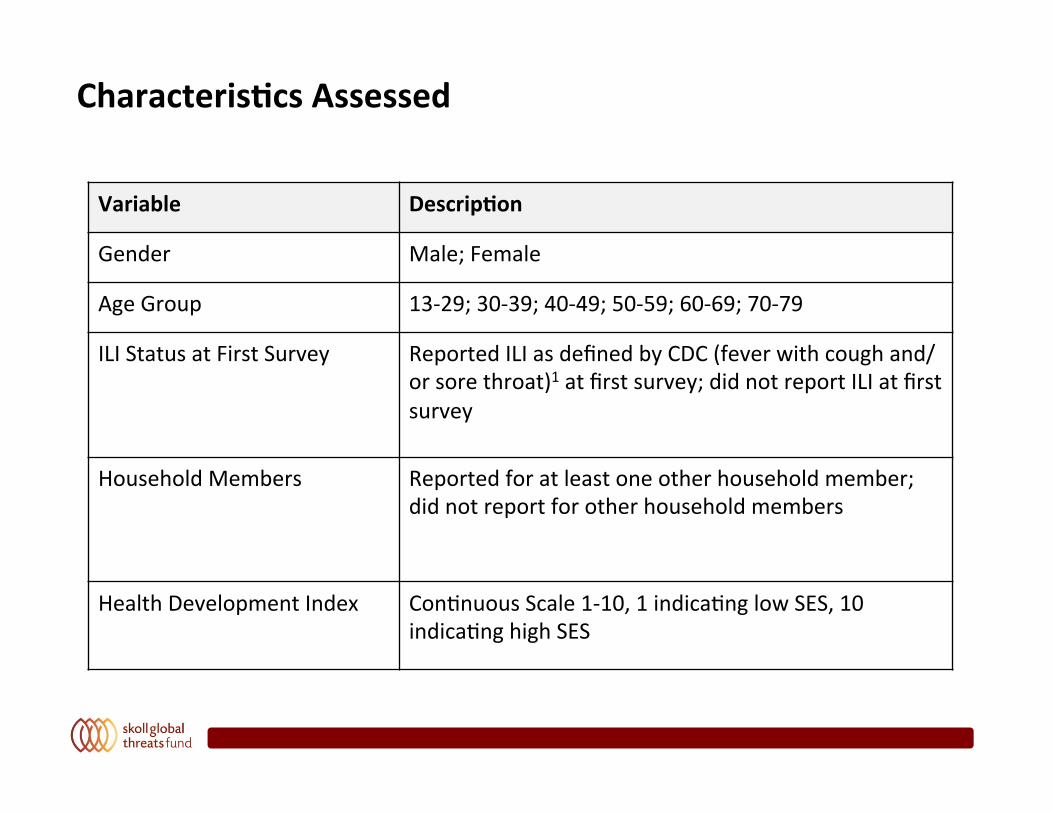
Characteris.csAssessed
Variable Descrip.on
Gender Male;Female
AgeGroup 13-29;30-39;40-49;50-59;60-69;70-79
ILIStatusatFirstSurvey ReportedILIasdefinedbyCDC(feverwithcoughand/orsorethroat)1atfirstsurvey;didnotreportILIatfirstsurvey
HouseholdMembers Reportedforatleastoneotherhouseholdmember;didnotreportforotherhouseholdmembers
HealthDevelopmentIndex Con0nuousScale1-10,1indica0nglowSES,10indica0nghighSES
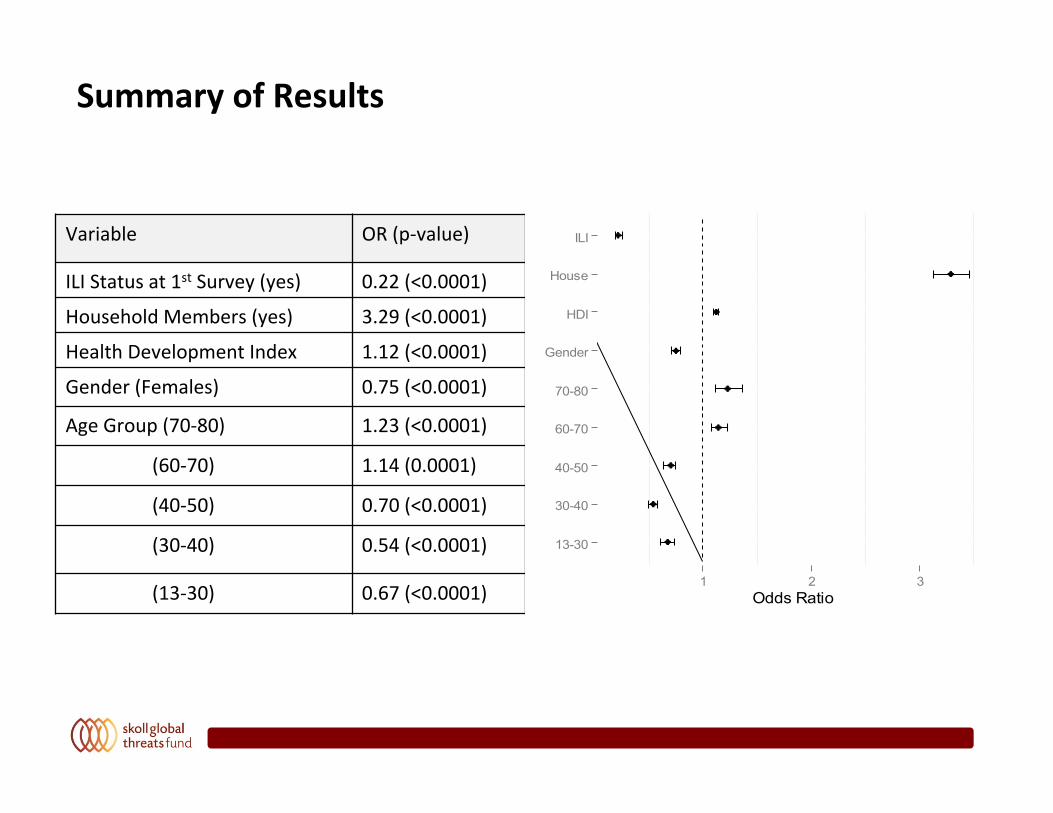
SummaryofResults
Variable OR(p-value)
ILIStatusat1stSurvey(yes) 0.22(<0.0001)
HouseholdMembers(yes) 3.29(<0.0001)
HealthDevelopmentIndex 1.12(<0.0001)
Gender(Females) 0.75(<0.0001)
AgeGroup(70-80) 1.23(<0.0001)
(60-70) 1.14(0.0001)
(40-50) 0.70(<0.0001)
(30-40) 0.54(<0.0001)
(13-30) 0.67(<0.0001)
13-30
30-40
40-50
60-70
70-80
Gender
HDI
House
ILI
1 2 3Odds Ratio
Related Documents