End of Life Care End of Life Care in Liver Disease in Liver Disease Dr Allister Grant Dr Allister Grant Consultant Hepatologist Consultant Hepatologist Leicester Liver Unit Leicester Liver Unit East Leicestershire and Rutland CCG PLT East Leicestershire and Rutland CCG PLT 3rd Sept 3rd Sept

End of Life Care in Liver Disease Dr Allister Grant Consultant Hepatologist Leicester Liver Unit East Leicestershire and Rutland CCG PLT 3rd Sept.
Dec 21, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

End of Life Care End of Life Care in Liver Diseasein Liver Disease
Dr Allister GrantDr Allister Grant
Consultant HepatologistConsultant Hepatologist
Leicester Liver UnitLeicester Liver Unit
East Leicestershire and Rutland CCG PLT 3rd SeptEast Leicestershire and Rutland CCG PLT 3rd Sept

Death rates for liver diseaseDeath rates for liver disease
FactsFacts
Liver disease is the 5th largest cause of Liver disease is the 5th largest cause of death in the U.K. death in the U.K.
The average age of death from liver disease The average age of death from liver disease is 59 years, compared to 82-84 years for is 59 years, compared to 82-84 years for heart & lung diseaseheart & lung disease
UK is one of few developed nations with an UK is one of few developed nations with an upward trend in mortality.upward trend in mortality.

Expanded Portal Tracts(Blue)
Prognosis- Child Pugh ScorePrognosis- Child Pugh Score
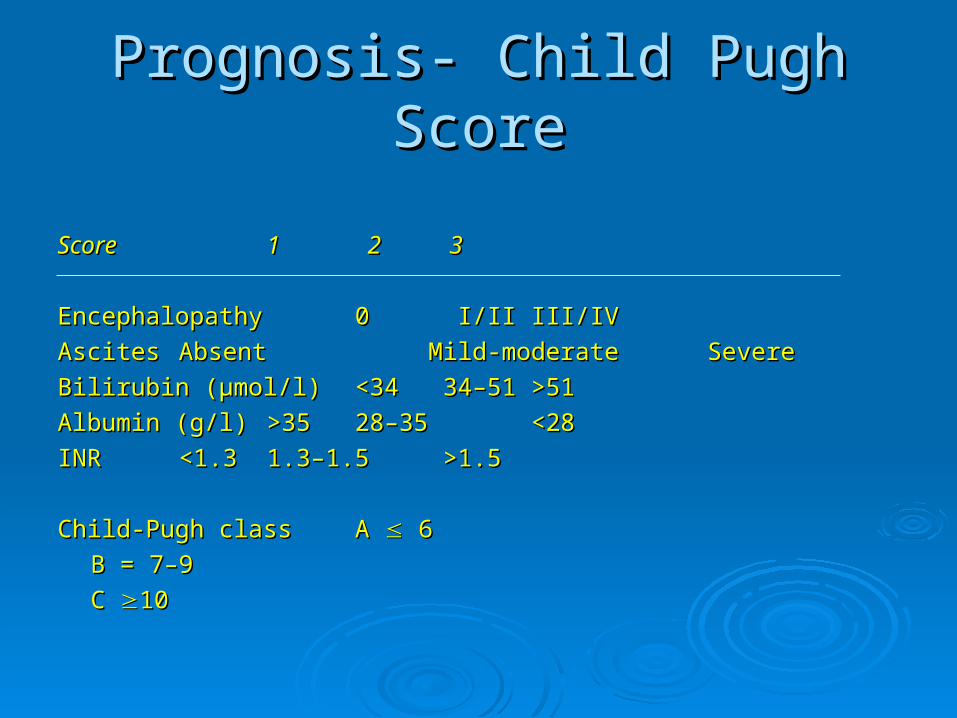
ScoreScore 1 1 2 2 3 3
EncephalopathyEncephalopathy 0 0 I/II I/II III/IVIII/IV
Ascites Ascites Absent Absent Mild-moderate Mild-moderate SevereSevere
Bilirubin (µmol/l) Bilirubin (µmol/l) <34 <34 34–51 34–51 >51>51
Albumin (g/l) Albumin (g/l) >35>35 28–35 28–35 <28<28
INR INR <1.3 <1.3 1.3–1.5 1.3–1.5 >1.5>1.5
Child-Pugh classChild-Pugh class A A 6 6
B = 7–9B = 7–9
C C 10 10

PrognosisPrognosis
1 Year Survival1 Year Survival
– – Child Pugh A Child Pugh A 80 - 100%80 - 100%
– – Child Pugh B Child Pugh B 60 - 80%60 - 80%
– – Child Pugh C Child Pugh C 35 - 45%35 - 45%

Complications of End Stage Liver Complications of End Stage Liver DiseaseDisease
Decompensated CirrhosisDecompensated Cirrhosis Variceal bleedingVariceal bleeding AscitesAscites EncephalopathyEncephalopathy
Other Other Sepsis (SBP)Sepsis (SBP) Hepatorenal syndromeHepatorenal syndrome Hepatocellular carcinomaHepatocellular carcinoma

Disease ProgressionL
iver
fu
nct
ion
100%
Cirrhosis
Liver FailureTransplantDeathYears
A
B
C

Disease ProgressionL
iver
fu
nct
ion
50%
Cirrhosis
Liver FailureTransplantDeath
Months


Portal Portal CirculationCirculation

Oesophageal varicesOesophageal varices

Management of Bleeding VaricesManagement of Bleeding Varices
PreventionPrevention
ResuscitationResuscitation
Endoscopy -Endoscopy - Band LigationBand LigationSclerotherapySclerotherapy
Pharmacotherapy- TerlipressinPharmacotherapy- Terlipressin
Balloon TamponadeBalloon Tamponade
TIPS/TransplantationTIPS/Transplantation

Oesophageal varicesOesophageal varices

Bleeding Gastric VaricesBleeding Gastric Varices

Variceal BanderVariceal Bander

Variceal Band LigationVariceal Band Ligation

Variceal Band LigationVariceal Band Ligation

Variceal Bleeding in Palliative CareVariceal Bleeding in Palliative Care
May be occult and present as encephalopathyMay be occult and present as encephalopathy--GastricGastric-Duodenal-Duodenal-Colonic-Colonic
Resuscitate if appropriateResuscitate if appropriate Correct coagulopathyCorrect coagulopathy Give Terlipressin if known varicesGive Terlipressin if known varices
As effective as balloon tamponadeAs effective as balloon tamponade As effective as endoscopic therapyAs effective as endoscopic therapy
?Give PPI?Give PPI / sucralfate / tranexamic acid/ sucralfate / tranexamic acid Colonic varices- rectal balloon tamponadeColonic varices- rectal balloon tamponade

AscitesAscites
Causes of Ascites Causes of Ascites
20% of patients with ascites have a non hepatic cause20% of patients with ascites have a non hepatic cause
5% of patients with hepatic ascites have a second cause5% of patients with hepatic ascites have a second cause
Peritoneal disease- carcinomatosis, TBPeritoneal disease- carcinomatosis, TBHeart failureHeart failureDiabetic nephropathyDiabetic nephropathyHypoalbuminaemia of other causesHypoalbuminaemia of other causes

The Development of AscitesThe Development of Ascites
Peripheral arterial dilatation
Reduced effective blood volume Hypoalbuminaemia
Activation of renin-angiotensin-aldosterone systemSympathetic nervous systemADH
Na retention &Water retention
Low urinary NaDilutional hyponatraemia
AscitesSchrier et al Hepatol
Plasma volume expansion
NaCl
Ascites and Oedema

General ManagementGeneral Management
Hepatic Ascites and OedemaHepatic Ascites and Oedema
Salt restrictionSalt restriction
DiureticsDiureticsspironolactonespironolactonefrusemidefrusemide
Water restriction if sodium < 125 mmolWater restriction if sodium < 125 mmol
ParacentesisParacentesisdiagnostic (SBP, tumour)diagnostic (SBP, tumour)therapeutic (Total vs partial + therapeutic (Total vs partial +
colloids)colloids) Daily weightDaily weight

Sampling of AscitesSampling of Ascites
Coagulopathy is not a contraindication to diagnostic paracentesis Coagulopathy is not a contraindication to diagnostic paracentesis (unless clinically evident fibrinolysis or DIC)(unless clinically evident fibrinolysis or DIC)
FFP/platelets are not requiredFFP/platelets are not required
In uncomplicated hepatic ascites request cell count and [Albumin] In uncomplicated hepatic ascites request cell count and [Albumin]
PMN>250 cells/mmPMN>250 cells/mm33 indicates SBP indicates SBP
transudate/exudate <25g/L/>25g/Ltransudate/exudate <25g/L/>25g/L
serum/ascites albumin gradient >11g/L= Portal Hypserum/ascites albumin gradient >11g/L= Portal Hyp
Runyon et al Ann Int Med 1992

Spontaneous Bacterial PeritonitisSpontaneous Bacterial Peritonitis
Definition-Definition-
““SBP is a bacterial infection of ascitic fluid which arises in the SBP is a bacterial infection of ascitic fluid which arises in the absence of any other source of sepsis within the peritoneum absence of any other source of sepsis within the peritoneum or adjacent tissues”or adjacent tissues”
PMN>250 cells/mmPMN>250 cells/mm33
Mortality rate similar to that of a variceal bleed (20-40%)Mortality rate similar to that of a variceal bleed (20-40%)

Secondary prevention of SBPSecondary prevention of SBP Patients who survive SBP have a 1y recurrence rate of 40-Patients who survive SBP have a 1y recurrence rate of 40-
70%70%
Norfloxacin 400mg/day reduces recurrence from 68% to 20% Norfloxacin 400mg/day reduces recurrence from 68% to 20%
Locally we use Septrin 960mg od Mon-FriLocally we use Septrin 960mg od Mon-Fri
Median survival of these patients is 9moMedian survival of these patients is 9mo
These patients should be considered for liver transplantation/ These patients should be considered for liver transplantation/ GSFGSF

Sepsis in CirrhosisSepsis in Cirrhosis
Incidence- Incidence-
1% of 1% of allall admissions to hospital are due to sepsis admissions to hospital are due to sepsis
30-50% of cirrhotic patients admitted to hospital due to 30-50% of cirrhotic patients admitted to hospital due to sepsissepsis
Once admitted 15-35% of cirrhotics develop infection Once admitted 15-35% of cirrhotics develop infection (c.f. 5-7% general hospital population)(c.f. 5-7% general hospital population)

General ManagementGeneral Management
EncephalopathyEncephalopathy
Treat precipitantsTreat precipitants• • SepsisSepsis• • GI bleedGI bleed• • Medications (over-diuresis)Medications (over-diuresis)
• Stop sedatives, hypnotics, opiatesStop sedatives, hypnotics, opiates• ConstipationConstipation
Lactulose (NG/PR/PO)Lactulose (NG/PR/PO)
Metronidazole/ Rifaximin/ neomycin -deafnessMetronidazole/ Rifaximin/ neomycin -deafness

Acute Kidney Injury in CLDAcute Kidney Injury in CLD
Exclude urinary infectionExclude urinary infection Exclude obstructive uropathyExclude obstructive uropathy Trial of volumeTrial of volume Avoid nephrotoxinsAvoid nephrotoxins
• • NSAIDsNSAIDs
• • IV contrastIV contrast Avoid over-diuresisAvoid over-diuresis Avoid hypotensionAvoid hypotension Hepatorenal Failure carries grave prognosisHepatorenal Failure carries grave prognosis

Hepatorenal SyndromeHepatorenal Syndrome Hepatorenal Syndrome is a severe complication of end Hepatorenal Syndrome is a severe complication of end
stage liver disease associated with an 80%-95% stage liver disease associated with an 80%-95% mortality at 2 weeks.mortality at 2 weeks.
The only interventions that have been shown to improve The only interventions that have been shown to improve survival are liver transplantation, the vasopressin survival are liver transplantation, the vasopressin analogues and TIPSanalogues and TIPS
Type 1 (Acute)Type 1 (Acute)
Type 2 (Chronic)Type 2 (Chronic)

HRS SurvivalHRS Survival
Gines et al Lancet 2003

The Development of HRSThe Development of HRS
Reduced effective blood volume
Activation of renin-angiotensin-aldosterone systemSympathetic nervous systemADH
Na retention &Water retention
Low urinary NaDilutional hyponatraemia
AscitesSchrier et al Hepatol
Plasma volume expansion
Renal vasoconstrictionReduced GFR
NSAIDAminoglycosides
Diuretics Sepsis
NaCl
Ascites and OedemaHRS
Increases TerlipressinSplanchnicvasoconstriction
↓↓ ↓
X
Peripheral arterial dilatation
↑Renal Perfusion
Albumin

Hepatocellular CarcinomaHepatocellular Carcinoma
All UK cirrhotic patients undergo 6 monthly All UK cirrhotic patients undergo 6 monthly HCC surveillance with USS and AFPHCC surveillance with USS and AFP
AFP >400 is diagnostic of HCCAFP >400 is diagnostic of HCC
Focal lesion – MRI/triple phase CTFocal lesion – MRI/triple phase CT Arterialised nodule, washout in venous phaseArterialised nodule, washout in venous phase

Surveillance in Cirrhosis Surveillance in Cirrhosis
Surveillance for HepatomaSurveillance for Hepatoma
6 monthly AFP and USS


PruritisPruritis
After exclusion of other causes of Itching considerAfter exclusion of other causes of Itching consider
Biliary ObstructionBiliary Obstruction PBC in the absence of JaundicePBC in the absence of Jaundice Cholestasis/JaundiceCholestasis/Jaundice DrugsDrugs

PruritisPruritis
Biliary ObstructionBiliary Obstruction
StonesStones StrictureStricture 11 or 2 or 2 Tumour Tumour NodesNodes

MRCPMRCP

ERCPERCP

ERCPERCP

Drugs for PruritisDrugs for Pruritis Non-Specific ManagementNon-Specific Management
Lubricants/Topical agentsLubricants/Topical agents Reduce irritationReduce irritation Prevent scratchingPrevent scratching Systemic Anti-pruriticsSystemic Anti-pruritics
• AtaraxAtarax• Fexofenidine etcFexofenidine etc
Liver DiseaseLiver Disease CholestyramineCholestyramine Ursodeoxycholic acidUrsodeoxycholic acid RifampicinRifampicin Opioid antagonists, naloxone , naltrexoneOpioid antagonists, naloxone , naltrexone OndansetronOndansetron

Other TreatmentsOther Treatments
• Ultraviolet light exposureUltraviolet light exposure
• Plasmapheresis Plasmapheresis
• Liver TransplantationLiver Transplantation

FutureFuture Liver disease is an important cause of mortality in the Liver disease is an important cause of mortality in the
U.K. U.K. In 2000 it killed more men than Parkinson’s disease In 2000 it killed more men than Parkinson’s disease and more women than cancer of the cervix.and more women than cancer of the cervix.
~1% of population HCV positive~1% of population HCV positive
Mortality from Alcoholic liver disease doubled in 10 yearsMortality from Alcoholic liver disease doubled in 10 years
Incidence of liver cancer has doubled in 10 yearsIncidence of liver cancer has doubled in 10 years
4% of the population have abnormal liver function4% of the population have abnormal liver function
50% people with colorectal cancer develop liver 50% people with colorectal cancer develop liver metastases, 20% resectablemetastases, 20% resectable

The EndThe End“All right, let's not panic.
I'll make the money by selling one of my livers.I can get by with one “
Doh!
Related Documents











