Emerging Approaches to Emerging Approaches to Antiplatelet Antiplatelet Therapy for PCI: Therapy for PCI: Prasugrel Prasugrel David J. Cohen, M.D., M.Sc. David J. Cohen, M.D., M.Sc. Director, Cardiovascular Research Director, Cardiovascular Research Saint Saint - - Luke Luke ’ ’ s Mid America Heart Institute s Mid America Heart Institute Professor of Medicine Professor of Medicine University of Missouri University of Missouri - - Kansas City Kansas City

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Emerging Approaches to Emerging Approaches to AntiplateletAntiplatelet Therapy for PCI:Therapy for PCI:
PrasugrelPrasugrel
David J. Cohen, M.D., M.Sc.David J. Cohen, M.D., M.Sc.
Director, Cardiovascular ResearchDirector, Cardiovascular ResearchSaintSaint--LukeLuke’’s Mid America Heart Institutes Mid America Heart Institute
Professor of MedicineProfessor of MedicineUniversity of MissouriUniversity of Missouri--Kansas CityKansas City

DisclosuresDisclosures
Grant Support/DrugsGrant Support/Drugs−− Eli Lilly/DaiichiEli Lilly/Daiichi--SankyoSankyo -- Merck/Schering PloughMerck/Schering Plough−− Eisai PharmaceuticalsEisai Pharmaceuticals
Grant Support/DevicesGrant Support/Devices−− MedRADMedRAD -- Boston ScientificBoston Scientific−− Edwards Edwards LifesciencesLifesciences -- Abbott VascularAbbott Vascular−− MedtronicMedtronic
Consulting/Advisory BoardsConsulting/Advisory Boards−− MedtronicMedtronic -- Eli Lilly/DaiichiEli Lilly/Daiichi--SankyoSankyo−− CordisCordis -- BoehringerBoehringer--IngelheimIngelheim
DJC: 4/11

AspirinAspirin
TiclopidineClopidogrelTiclopidineClopidogrel
AbciximabEptifibatide
Tirofiban
AbciximabEptifibatide
Tirofiban

PrasugrelPrasugrelPrasugrel

PrasugrelPrasugrelPrasugrel
Prasugrel: Key Properties• Novel thienopyridine• Prodrug more efficient generation of active
metabolite than clopidogrel No meaningful genetic heterogeneity in
pharmacokinetics or pharmacodynamics• Achieves high levels of IPA rapidly and reliably• 1x/day dosing
Prasugrel: Key Properties• Novel thienopyridine• Prodrug more efficient generation of active
metabolite than clopidogrel No meaningful genetic heterogeneity in
pharmacokinetics or pharmacodynamics• Achieves high levels of IPA rapidly and reliably• 1x/day dosing

Prasugrel vs. Clopidogrel: Active Metabolite Formation
Clopidogrel4-8
85% Inactive Metabolite8
hCE1
2nd Oxidation
CYP1A22B6
2C19CYP3A2B62C9
2C19
Active MetaboliteGenetic variation in CYP2C19 can impair metabolism
1st Oxidation
Hydrolysis
*Prasugrel is not 100% converted to the active metabolite; a portion of the dose is metabolized to inactive metabolites.
Hydrolysis 1st OxidationPrasugrel1-3
hCE2 Active Metabolite*No relevant effect of genetic variation in CYP2C19CYP3A
2B62C92C19
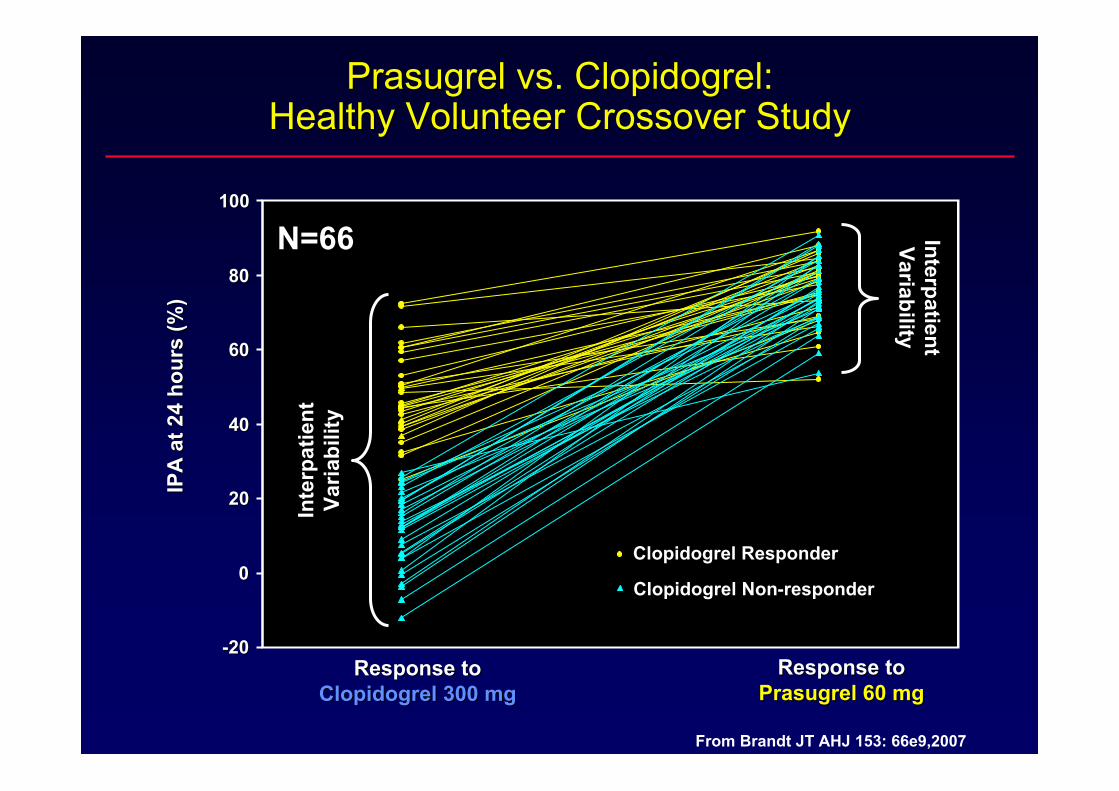
Prasugrel vs. Clopidogrel: Prasugrel vs. Clopidogrel: Healthy Volunteer Crossover StudyHealthy Volunteer Crossover Study
--2020
00
2020
4040
6060
8080
100100IP
A a
t 24
hour
s (%
)IP
A a
t 24
hour
s (%
)
Response to Response to Prasugrel 60 mgPrasugrel 60 mg
Response to Response to Clopidogrel 300 mgClopidogrel 300 mg
Clopidogrel ResponderClopidogrel Responder
Clopidogrel NonClopidogrel Non--responderresponder
Inte
rpat
ient
Inte
rpat
ient
Varia
bilit
yVa
riabi
lity
InterpatientInterpatientVariabilityVariability
From Brandt JT AHJ 153: 66e9,2007
N=66

Inhibition of Platelet Aggregation (IPA):Prasugrel and Clopidogrel Loading Dose
80
60
40
20
0
100
0 4 8 12 16
Time After Administration (h)
Inhi
bitio
n of
Pla
tele
t A
ggre
gatio
n (%
) 20 μM Adenosine Diphosphate*
The relationship between IPA and clinical activity has not been established.
20 24
†P<0.01Mean ± SD
Prasugrel 60 mg Clopidogrel 300 mg
† †††
†
†† †
1. Brandt et al. Am Heart J. 2007;153:66.e9-16.2. Effient Full Prescribing Information.
1 2 6
*Represents healthy subjects in a crossover study who were not on concurrent ASA therapy (n=64).

TRial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet InhibitioNWith Prasugrel (TRITON)-TIMI 38
TRITON-TIMI 38
Double-blind
ACS (STEMI or UA/NSTEMI) & Planned PCIASA
PRASUGREL60 mg LD/ 10 mg MD
CLOPIDOGREL300 mg LD/ 75 mg MD
1o endpoint: CV death, MI, Stroke
Safety endpoints: TIMI major bleeds, Life-threatening bleedsKey Substudies: Pharmacokinetic, Genomic
Median duration of therapy = 14.5 months
N= 13,608
12
10
8
6
4
2
0
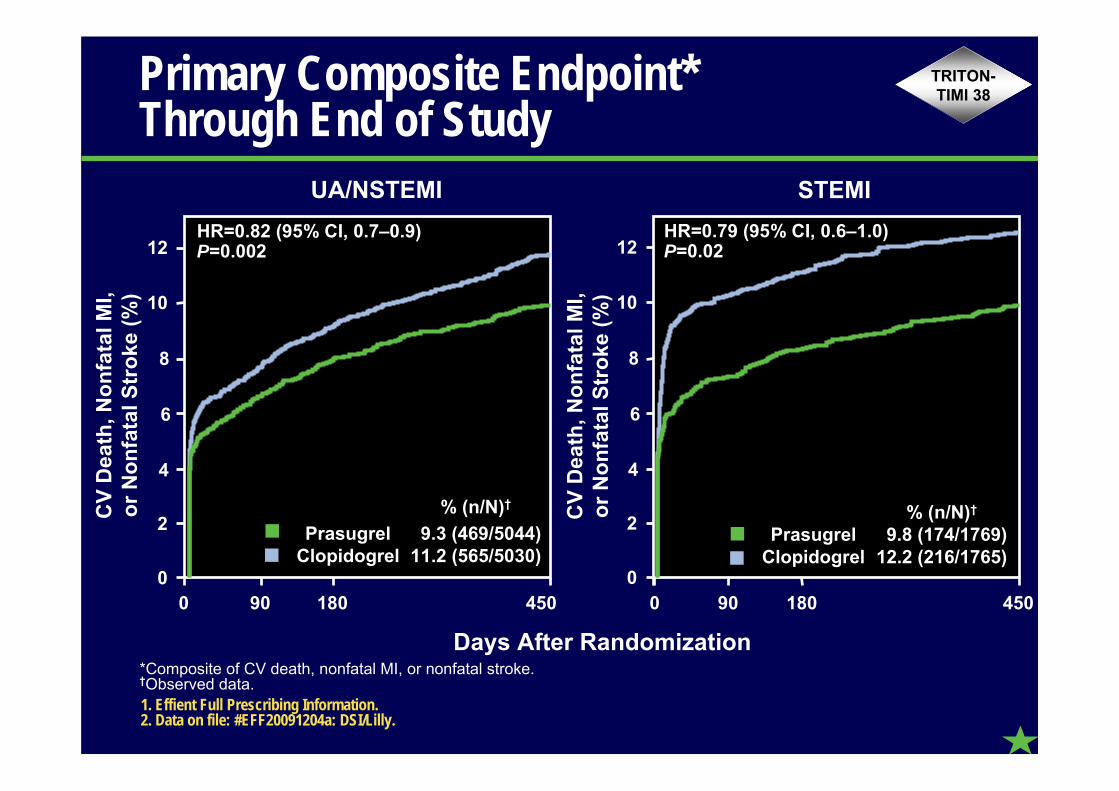
Primary Composite Endpoint* Through End of Study
UA/NSTEMI STEMI
Days After Randomization
12
10
0 90 180 450
8
6
4
2
0
HR=0.82 (95% CI, 0.7–0.9)P=0.002
0 90 180 450
HR=0.79 (95% CI, 0.6–1.0)P=0.02
% (n/N)†
Prasugrel 9.3 (469/5044) Clopidogrel 11.2 (565/5030)
% (n/N)†
Prasugrel 9.8 (174/1769) Clopidogrel 12.2 (216/1765)
1. Effient Full Prescribing Information.2. Data on file: #EFF20091204a: DSI/Lilly.
*Composite of CV death, nonfatal MI, or nonfatal stroke.†Observed data.
CV
Dea
th, N
onfa
tal M
I,or
Non
fata
l Str
oke
(%)
TRITON-TIMI 38
CV
Dea
th, N
onfa
tal M
I,or
Non
fata
l Str
oke
(%)

UA/NSTEMI1
3.3
2.4
12.2
9.8†
8.8
6.7†
1.8
1.8
0.8
0.8
7.1*
9.2
9.3*
11.2
2.0
2.2
0.9
0.9
7.0‡
9.1
9.4‡
11.5
CV Death, Nonfatal MI, or Nonfatal
Stroke
Nonfatal MI
NonfatalStroke
CV Death
1240 8
STEMI1 All-ACS2,3
Endpoint (%)
PrasugrelClopidogrel
1.1
1.2
1240 8 1240 8
*P<0.003 vs clopidogrel †P<0.02 vs clopidogrel ‡P<0.001 vs clopidogrel
In the overall study, approximately 40% of MIs occurred periprocedurally and were detected solely by changes in CK-MB.
1. Effient Full Prescribing Information. 2. Data on file: #EFF20091204a: DSI/Lilly. 3. Data on file: #EFF20091204e: DSI/Lilly.
Primary Composite Endpoint* and Components
TRITON-TIMI 38
*Composite of CV death, nonfatal MI, or nonfatal stroke.
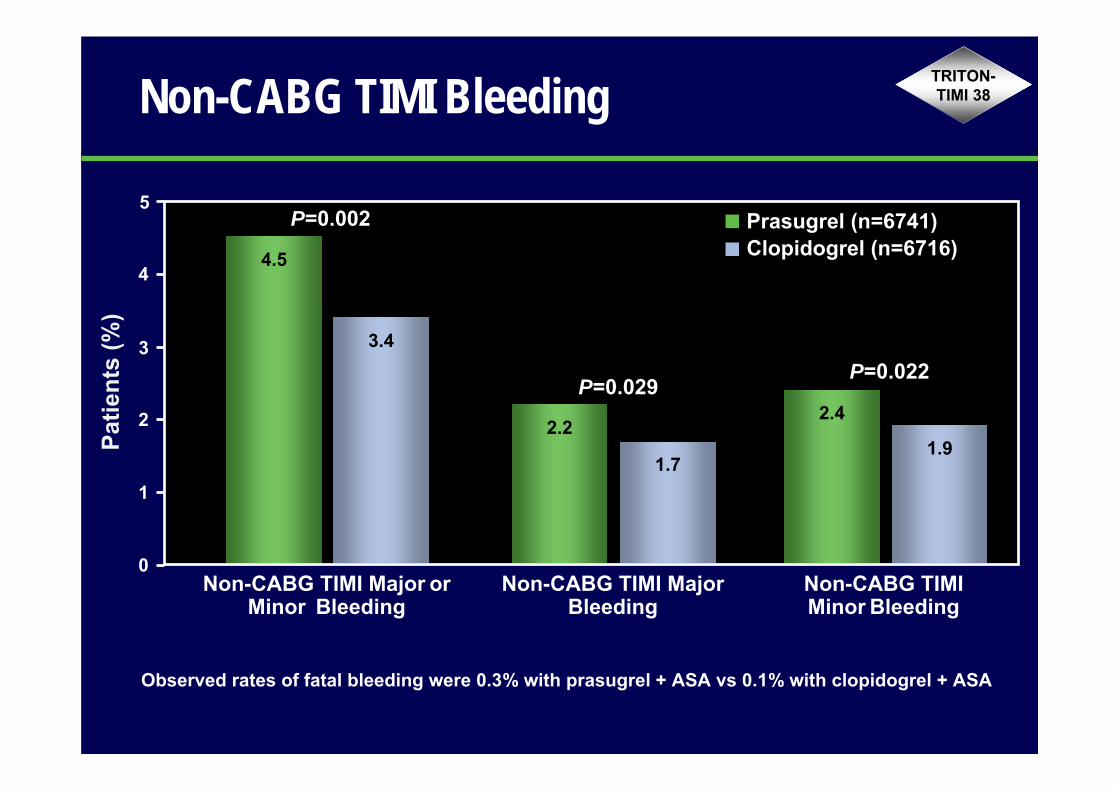
Non-CABG TIMI Bleeding
5
Patie
nts
(%)
4.5
3.4
2.2
1.7
2.4
1.9
P=0.002
P=0.029P=0.022
Prasugrel (n=6741)Clopidogrel (n=6716)
Non-CABG TIMI Major or Minor Bleeding
Non-CABG TIMI MajorBleeding
Non-CABG TIMI Minor Bleeding
0
1
2
3
4
Observed rates of fatal bleeding were 0.3% with prasugrel + ASA vs 0.1% with clopidogrel + ASA
TRITON-TIMI 38

The trial only used a 300 mg loading The trial only used a 300 mg loading dose of clopidogreldose of clopidogrel–– we generally use we generally use
600 mg these days600 mg these days
Issues with Prasugrel/TRITONIssues with Prasugrel/TRITON--TIMI 38TIMI 38

PRINCIPLE-TIMI 44: Comparison of Prasugrel with Higher Dose Clopidogrel
P<0.0001 for each
IPA (%; 20 M ADP)
Hours 14 Days
IPA (%; 20 M ADP)P<0.0001
Prasugrel 10 mg
Clopidogrel 150 mg
N=201
Prasugrel 60 mg
Clopidogrel 600 mg
Wiviott S, et al. Circulation 2007
0
2
4
6
8
0 1 2 3
1
0 306090 180 270 360 450
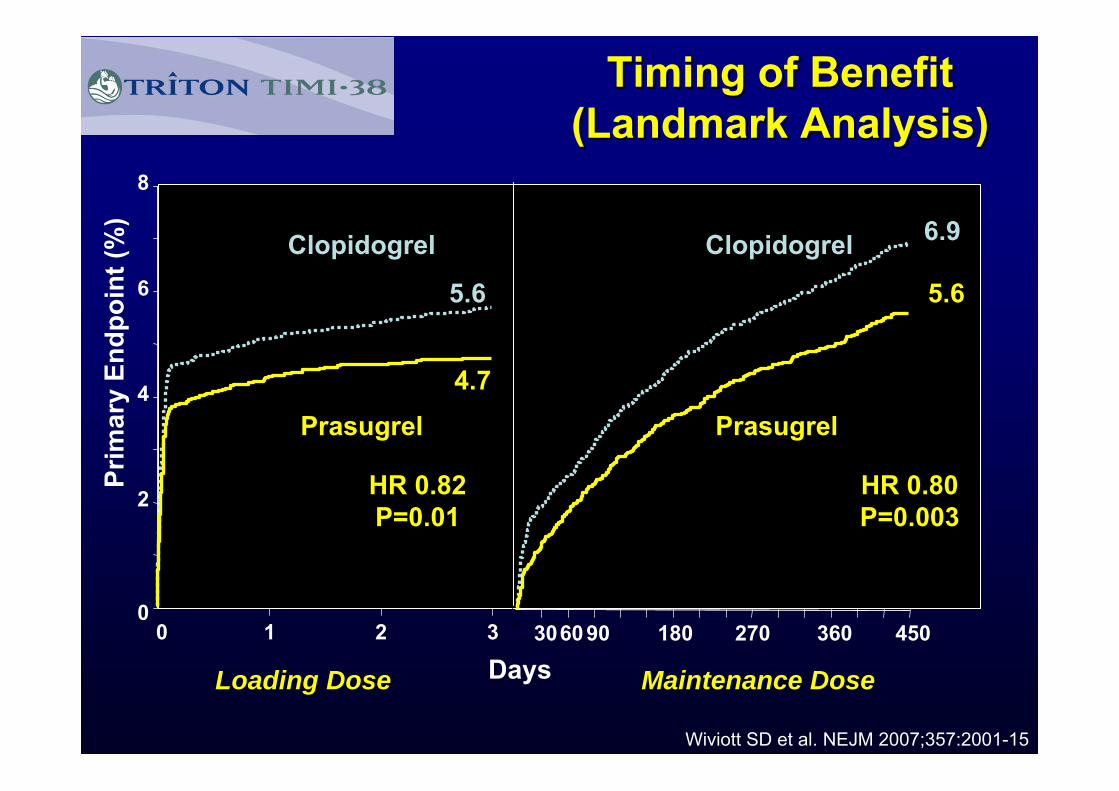
HR 0.82P=0.01
HR 0.80P=0.003
5.6
4.7
6.9
5.6
Days
Prim
ary
Endp
oint
(%)
Prasugrel
Clopidogrel
Prasugrel
Clopidogrel
Loading Dose Maintenance Dose
Timing of BenefitTiming of Benefit(Landmark Analysis)(Landmark Analysis)
Wiviott SD et al. NEJM 2007;357:2001-15

The benefit of prasugrel was driven The benefit of prasugrel was driven entirely by a reduction in nonentirely by a reduction in non--fatal MIfatal MI
Issues with Prasugrel/TRITONIssues with Prasugrel/TRITON--TIMI 38TIMI 38

Prasugrel (n=6813)Clopidogrel (n=6795)
Cum
ulat
ive
Inci
denc
e (%
)
Type 1Spontaneous
Type 2Secondary
Type 3Sudden
Cardiac Death
Type 4PCI-Related
Type 5Peri-CABG
1
0
2
3
4
5
6
7
2.5
n=150
3.4
n=209
0.3
n=19
0.4
n=230.0n=1
0.1n=4
0.1n=4
0.0n=3
Morrow et al. Circulation. 2009;119:2758-2764.
In the TRITON-TIMI 38 trial, there were a total of 1218 MIs. This retrospective analysis classified these MIs using the newly developed classification system from the universal definition of MI, which was developed after the study protocol was complete.
Application of Universal MI Classification to TRITON-TIMI 38 MI Events
4a4.7
6.4
n=424
4a4.1
4.8
n=324
4b0.8
4b1.7
TRITON-TIMI 38
Type of MI

Cum
ulat
ive
Inci
denc
e (%
)
0.90.7
0.60.5
1.81.4
2.8
2.1
3.8
2.8
1
0
2
3
4
1–<2 x ULN 2–<3 x ULN 3–<5 x ULN 5–<10 x ULN ≥10 x ULN
Prasugrel (n=6813)Clopidogrel (n=6795)
n=109
n=70
n=212
n=331
n=441
Morrow et al. Circulation. 2009;119:2758-2764.
Application of Universal MI Classification to TRITON-TIMI 38 MI Events
TRITON-TIMI 38
Level of CK Elevation
In the TRITON-TIMI 38 trial, there were a total of 1218 MIs. This retrospective analysis classified these MIs using the newly developed classification system from the universal definition of MI, which was developed after the study protocol was complete.

The stent thrombosis rates in TRITON The stent thrombosis rates in TRITON seem very highseem very high–– we donwe don’’t see anything t see anything
like this in our practicelike this in our practice
Issues with Prasugrel/TRITONIssues with Prasugrel/TRITON--TIMI 38TIMI 38

Stent Thrombosis: All ACS
Days After Randomization
Sten
t Thr
ombo
sis*
(%)
Any Stent PostAny Stent Post--RandomizationRandomization
0
1
2
3
0 50 100 200 300 400 450
HR=0.48 (95% CI, 0.4–0.6)P<0.0001
350250150
% (n/N)†
Prasugrel 1.1 (68/6422) Clopidogrel 2.2 (142/6422)
1. Wiviott et al. Lancet. 2008;371:1353-1363. 2. Data on file: #EFF20091204b: DSI/Lilly.
*Stent thrombosis defined as Academic Research Consortium definite or probable.†Observed data.
TRITON-TIMI 38

0 30 60 90 120 150 180 210 240 270 300 330 360 3900
3
4
5
Sten
t Thr
ombo
sis
(%)
Days from Randomization
2
1
Stent Thrombosis (Protocol Defn.)Stent Thrombosis (Protocol Defn.)Drug-eluting Stents (DES) vs. Bare Metal Stents (BMS)Drug-eluting Stents (DES) vs. Bare Metal Stents (BMS)
EstimateP
(log rank)
≥1 DES (N=4630)0.38
2.2%
1 year
All BMS (N=2528) 2.3%
All (N=7158) 2.2%

11--Year Stent Thrombosis: Year Stent Thrombosis: Impact of Impact of Implanted Stent TypeImplanted Stent Type
3.3% 3.3% 3.4% 3.4%
HR [95%CI] =HR [95%CI] =0.98 [0.640.98 [0.64--1.51]1.51]
P = 0.93P = 0.93
22612261 21712171 21472147 21232123 20972097 19001900872872 832832 818818 805805 791791 720720
Number at riskNumber at riskAny DESAny DESBMS onlyBMS only
Def
/Pro
b St
ent T
hrom
bosi
s (%
)D
ef/P
rob
Sten
t Thr
ombo
sis
(%)
00
11
22
33
44
Time in daysTime in days00 3030 6060 9090 120120 150150 180180 210210 240240 270270 300300 330330 365365
Any DESAny DESBMS OnlyBMS Only

InvasiveStent thrombosis
Ticagrelor(n=6,732)
Clopidogrel(n=6,676)
HR for ticagrelor(95% CI)
p value*
Stent thrombosis, %
Definite
Probable or definite
Possible, probable, or definite
1.0
1.7
2.2
1.6
2.3
3.1
0.62 (0.45–0.85)
0.72 (0.56–0.93)
0.72 (0.58–0.90)
0.003
0.01
0.003
¶ Evaluated in patients with any stent during the studyTime-at-risk is calculated from the date of first stent insertion in the study or date of randomization* By univariate Cox model
The increased risk of bleeding outweighs The increased risk of bleeding outweighs any benefit in reduced MI and stent any benefit in reduced MI and stent
thrombosisthrombosis
Issues with Prasugrel/TRITONIssues with Prasugrel/TRITON--TIMI 38TIMI 38

Antiplatelet Therapy in ACSAntiplatelet Therapy in ACS
0
1 08
Placebo APTC CURE TRITON-TIMI 38Single
Antiplatelet RxDual
Antiplatelet RxHigher
IPA
ASA ASA +Clopidogrel ASA +
Prasugrel- 22%
- 20%
- 19%
+ 60% + 38% + 32%
ReducedIschemicEvents
Increased Major
Bleeds

Major or Minor Bleeding in UA/NSTEMI and STEMI Populations
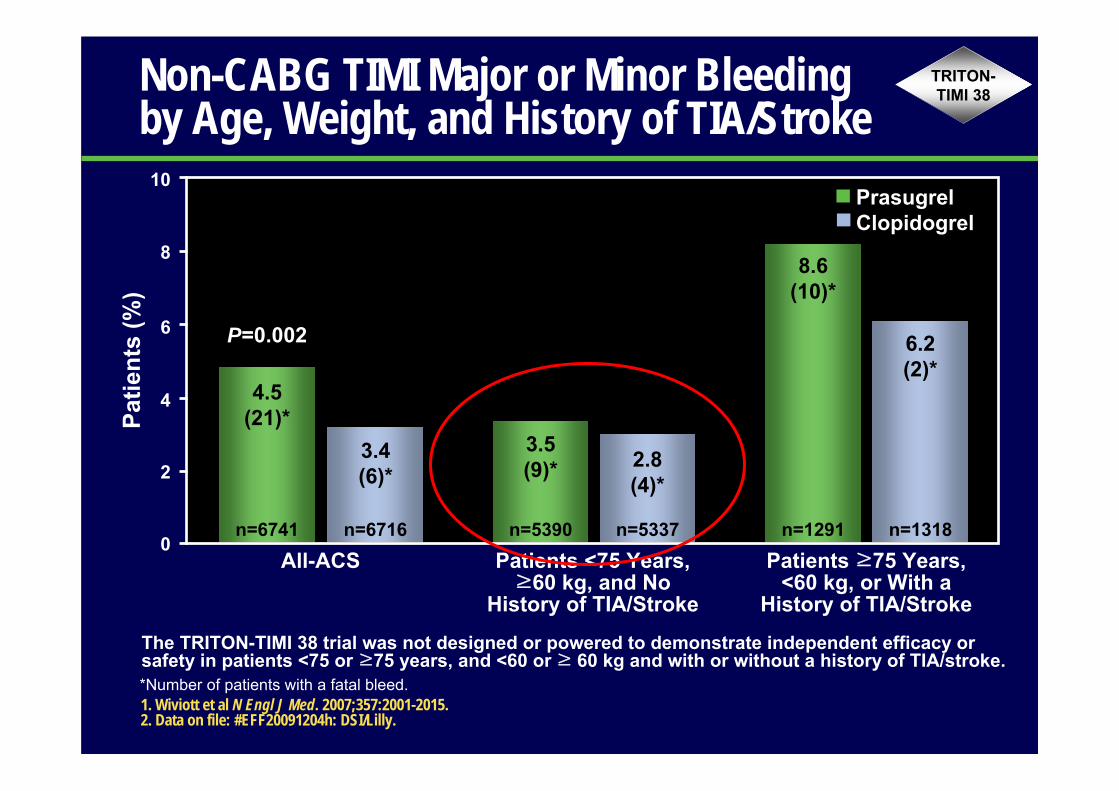
Non-CABG TIMI Major or Minor Bleeding by Age, Weight, and History of TIA/Stroke
10
6
8
Prasugrel Clopidogrel
All-ACS Patients <75 Years, ≥60 kg, and No
History of TIA/Stroke
Patie
nts
(%)
4
2
0Patients ≥75 Years,
<60 kg, or With a History of TIA/Stroke
4.5(21)*
n=6741
3.4(6)*
n=6716
3.5(9)*
n=5390
2.8(4)*
n=5337
8.6(10)*
n=1291
6.2(2)*
n=1318
P=0.002
1. Wiviott et al N Engl J Med. 2007;357:2001-2015.2. Data on file: #EFF20091204h: DSI/Lilly.
*Number of patients with a fatal bleed.
The TRITON-TIMI 38 trial was not designed or powered to demonstrate independent efficacy or safety in patients <75 or ≥75 years, and <60 or ≥ 60 kg and with or without a history of TIA/stroke.
TRITON-TIMI 38

•• While current antiplatelet therapies are efficacious, While current antiplatelet therapies are efficacious, there is substantial room for improvementthere is substantial room for improvement–– particularly particularly in the ACS settingin the ACS setting
•• Prasugrel is the first agent to demonstrate that greater, Prasugrel is the first agent to demonstrate that greater, more rapid, and more uniform platelet inhibition can more rapid, and more uniform platelet inhibition can further reduce ischemic events, but it does come at further reduce ischemic events, but it does come at the price of greater major bleeding. the price of greater major bleeding.
•• Careful patient selection is critical to optimizing the Careful patient selection is critical to optimizing the riskrisk--benefit profile of prasugrelbenefit profile of prasugrel
–– Clinical Factors: Age, Weight, ACS type, diabetesClinical Factors: Age, Weight, ACS type, diabetes–– Novel Factors: Genetics, Platelet function testingNovel Factors: Genetics, Platelet function testing
Conclusions: Emerging Platelet InhibitorsConclusions: Emerging Platelet Inhibitors

Prasugrel is just too expensivePrasugrel is just too expensive–– especially especially compared with generic clopidogrelcompared with generic clopidogrel
Issues with Prasugrel/TRITONIssues with Prasugrel/TRITON--TIMI 38TIMI 38

Incremental Costs/Cost Offsets with Prasugrel* Incremental Costs/Cost Offsets with Prasugrel*
-800
-600
-400
-200
0
200
400
PCI-$621
CABG-$21
Other Vasc.Interventions
$12
Other$82
Total-$517
Bleeding$69Angina
$20
MI (no PCI)-$57
Prasugrel Clopidogrel Difference (P-C)
Index Hospitalization Costs $19,740 $19,752 -$12
Rehospitalization Costs $4,465 $4,982 -$517
Study Drug Costs $1,862 $1,554 $308
TOTAL COSTS $26,067 $26,288 -$221

CostCost--Effectiveness: Effectiveness: Base Case Base Case
-$3,000
-$2,000
-$1,000
$0
$1,000
$2,000
$3,000
-0.4 -0.3 -0.2 -0.1 0.0 0.1 0.2 0.3 0.4
Life Years (Prasugrel – Clopidogrel)
C
ost
(Pra
sugr
el –
Clo
pido
grel
)
Cost = -$221 Life Exp. = 0.102 yrsICER = Dominant
% Dominant: 79.7%
Cost = -$221 Life Exp. = 0.102 yrsICER = Dominant
% Dominant: 79.7%
% <$50,000/LYG: 99.8%% <$50,000/LYG: 99.8%

Impact of Generic ClopidogrelImpact of Generic Clopidogrel
Treatment Over Full Trial DurationTreatment Over Full Trial DurationCost of Generic Clopidogrel = $1/dayCost of Generic Clopidogrel = $1/day
-$3,000
-$2,000
-$1,000
$0
$1,000
$2,000
$3,000
-0.4 -0.3 -0.2 -0.1 0.0 0.1 0.2 0.3 0.4
Life Years (Prasugrel – Clopidogrel)
C
ost
(Pra
sugr
el –
Clo
pido
grel
)
Cost = +$996 Life-years= 0.102ICER = $9,727/LYG
% Dominant: 0%
Cost = +$996 Life-years= 0.102ICER = $9,727/LYG
% Dominant: 0%
% <$50,000/LYG: 98.2%% <$50,000/LYG: 98.2%
Related Documents











