EM Teaching Michael D. Hill, MD MSc FRCPC Calgary Stroke Program

EM Teaching Michael D. Hill, MD MSc FRCPC Calgary Stroke Program.
Dec 24, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EM Teaching
Michael D. Hill, MD MSc FRCPCCalgary Stroke Program

Alcohol Warning LabelsIf the government really wants to help they should put useful warning labels on products. For instance alcohol should come with labels warning consumers of these unintended side effects:1.The consumption of alcohol may make you think you are whispering when you are not.2.The consumption of alcohol is a major factor in dancing like a retard.3.The consumption of alcohol may cause you to tell your friends over and over again that you love them.4.The consumption of alcohol may cause you to think you can sing.5.The consumption of alcohol may lead you to believe that ex-lovers are really dying for you to telephone them at four in the morning6.The consumption of alcohol may make you think you can logically converse with other members of the opposite sex without spitting7.The consumption of alcohol may make you think you have mystical Kung Fu powers, resulting in you getting your ass kicked8.The consumption of alcohol may cause you to roll over in the morning and see something really scary.9.The consumption of alcohol is the leading cause of inexplicable rug burns on the forehead.10.The consumption of alcohol may create the illusion that you are tougher, smarter, faster and better looking than most people.11.The consumption of alcohol may lead you to believe you are invisible.12.The consumption of alcohol may lead you to think people are laughing WITH you.13.The consumption of alcohol may cause a disturbance in the time-space continuum, whereby gaps of time may seem to literally disappear.

What is a stroke? (Important slide #1)
Stroke is a syndrome with multiple possible underlying etiologies. Stroke is a sudden vascular problem in the brain.

Stroke Types
• AIS – Acute Ischemic Stroke and TIA – Transient Ischemic Attack (85%)– Large vessel disease– Cardioembolic– Lacunar– Other
• ICH – Intracerebral hemorrhage (7-8%)– Lobar– Deep
• SAH – Sub-arachnoid hemorrhage (7-8%)• Sinovenous thrombosis (<<1%)
– Large sinus– Cortical vein

Cause of Death Worldwide
World Deaths x 10^6 % deaths
Coronary heart dx 7.20 12.2
Stroke 5.71 9.7
Lower resp infections 4.18 7.1
COPD 3.02 5.1
Diarrhoeal diseases 2.16 3.7
HIV/AIDS 2.04 3.5
Tuberculosis 1.46 2.5
Pulmonary cancers 1.32 2.3
MVA 2.27 2.2
Prematurity/LBW 1.18 2.0

Clinical Syndromes and Pathophysiology of Stroke
Michael D. Hill, MD, MSc, FRCPCAssociate ProfessorUniversity of CalgaryDirector, Stroke UnitStaff, Foothills Medical CentreCalgary, Alberta

7 of 39
Learning Objectives
After reviewing this presentation, you will be better able to:
1. Understand that stroke is a syndrome consisting of multiple etiologies
2. Understand mechanisms of ischemia
3. Understand the pathophysiology of cardioembolic stroke
4. Understand mechanisms of intra-cranial cerebral atherosclerosis

8 of 39
Stroke is a Syndrome
• Stroke (“apoplexy”)
– From the Greek – “to cripple by a stroke”
– A sudden vascular event leading to focal neurological dysfunction
– The clinical presentation alone does not allow differentiation between hemorrhage or ischemia

9 of 39
Stroke Types
• Ischemia [85% of all stroke]– Transient ischemic attack
• “mini-stroke”– Acute ischemic stroke
• Intracerebral hemorrhage (ICH) [7-8% of stroke]
• Sub-arachnoid hemorrhage (SAH) [7-8% of stroke]

10 of 39
Mechanisms of Ischemia
• Ischemia lack of blood flow resulting in tissue deprivation of nutrients
• The brain can tolerate hypoxia for many tens of minutes or hours; the brain does not tolerate ischemia for more than a few minutes

11 of 39
Brain Ischemia
ThrombusThrombus
Collateral FlowCollateral Flow
12 of 39
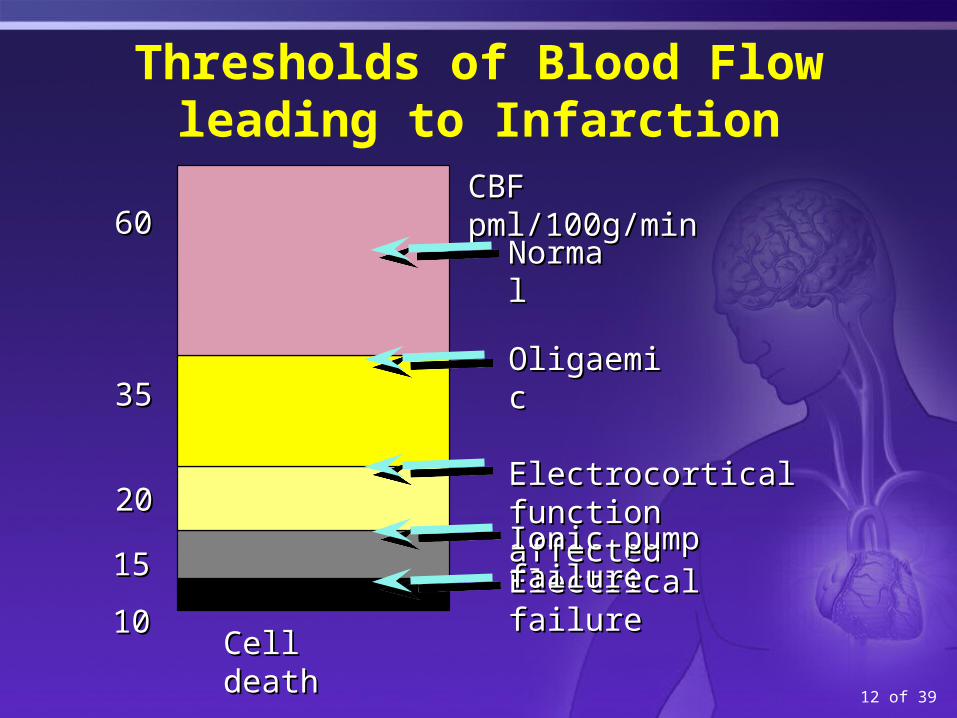
Thresholds of Blood Flow leading to Infarction
Cell deathCell death
CBF pml/100g/minCBF pml/100g/min
NormalNormal
OligaemicOligaemic
Electrocortical function Electrocortical function affectedaffected
Electrical failureElectrical failureIonic pump failureIonic pump failure
3535
2020
1515
1010
6060

13 of 39
Reversible Reversible reduced reduced functionfunction
0
20
50
Normal flow, normal function
Low flow, raised O2 extraction, normal function
Irreversible Irreversible reduced reduced functionfunctionC
BF
(m
l/100
g br
ain)
Time
Cerebral Ischemia and Time

14 of 39
Cerebral Ischemia
• Plumbing problem
• Blocked artery in the brain

15 of 39
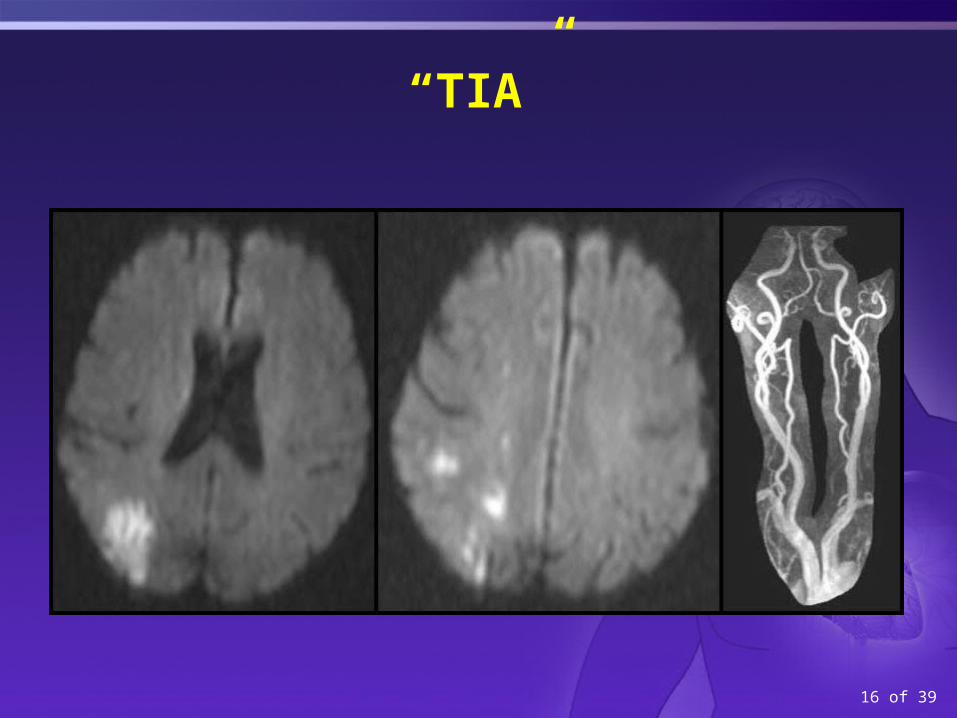
TIA vs. Stroke
• TIA stroke where all symptoms have resolved within 24h (WHO definition)
• Recent call for modified definition using 1 hour as the time point and modified by MR findings.
• Ischemic Stroke residual findings after 24 hours, however minor
N Engl J Med 2002: 347(21): 1713-1720N Engl J Med 2002: 347(21): 1713-1720
16 of 39
“TIA”

17 of 39
Mechanism of Ischemic Stroke
• Classification• Large Artery• Cardioembolic• Lacunar/small artery• Other known cause• Two or more causes• Cryptogenic• Unknown
Ann Neurol 2005;58:688–697Ann Neurol 2005;58:688–697

18 of 39
Large Artery Stroke (20%)
• Arteroembolic Stroke
– Thrombus in carotid or vertebral artery on an atherosclerotic plaque which embolises to the brain – arteroembolic event – COMMON
– Thrombus on an intracranial arterial stenosis (akin to an acute coronary syndrome) – UNCOMMON

19 of 39
Unstable plaque Stable plaque
Thin fibrous cap
Thrombus
Thick fibrous cap
Smooth muscle cells
Lipid rich coreand
macrophages
Media
Pathophysiology of Stable and Unstable Plaques

20 of 39
Cardioembolic Stroke (25-30%)
• Proximal embolic event
– Cardiac source• Atrial fibrillation/flutter• Valvular heart disease (eg. endocarditis, prosthetic valve)• Post-MI mural thrombus• Proximal aortic atheromatous disease causing arteroembolic
stroke (most often classified in the cardioembolic group even though large artery disease is the true mechanism)
• Paradoxical embolus via RL intra-cardiac shunt as seen in large PFO with atrial septal aneurysm
• A thrombus breaks off and embolises to a brain artery blocking an intracranial artery

21 of 39
Lacunar Stroke (25%)
• Small vessel disease– Occlusion of small, deep end-arteries– Associated strongly with hypertension and diabetes
mellitus– Mechanisms are:
• Lipohyalinosis with arterial wall collapse• Microatheroma with in situ thrombus• Small embolic material to these penetrating arteries

22 of 39
Other Known Causes (<5%)
• Multiplicity of other causes:– Dissection– Metabolic stroke
• Fabry’s disease• MELAS• Hypercoagulable states
(eg. essential thrombocytosis)
55 yo woman with a dissected ICA seen here on angiogram55 yo woman with a dissected ICA seen here on angiogram

23 of 39
Cryptogenic (20%)
• Despite complete and thorough investigation, the cause of stroke is unknown
– Commoner in younger patients
– ~20% of patients will have no cause identified
24 of 39
Pathology of Stroke Mechanism
• Atherosclerosis
– Relevant directly to about 20% of strokes – the large artery strokes
– In these patients, the analogy to coronary artery disease is direct
– Typical risk factors contribute to cerebral atherosclerosis – elevated lipids, smoking, hypertension, diabetes mellitus

25 of 39
Intra-cranial Cerebral Atherosclerosis
• Intracranial atherosclerosis is uncommon in western populations; greater prevalence in Asia
• When present in Caucasians it is most often seen in diabetics who smoke

26 of 39
Pathology: Cardioembolic Stroke
• Commonest cardioembolic source in the western world is atrial fibrillation– Hypertension as risk factor– Heart failure (most often due to CAD) as a risk factor
• Thus, indirectly atherosclerosis of the coronary arteries has an effect on stroke via the heart

27 of 39
Cardioembolic Stroke
• Multiple other causes of cardioembolic stroke– Infective endocarditis – blood cultures
and ESR should be done acutely on all patients with fever at stroke onset
– Marantic endocarditis
– Rheumatic heart disease
– Mitral stenosis
– Mural thrombus due to MI, dilated cardiomyopathy
– Cardiac tumours (atrial myxoma, fibroelastoma)
TTE showing atrial myxomaTTE showing atrial myxoma

28 of 39
Cardioembolic Stroke
• Mitral valve prolapse not a risk factor for stroke
• Mitral annual calcification weakly associated with stroke
29 of 39
Pathology Lacunar Stroke
• Small artery disease lacunar stroke
• End arteries
• Susceptible to occlusion due to lipohyalinosis of the relatively thin muscular arterial layer
• Embolism (arteroembolism, cardioembolism) to the perforating arteries is known to occur but is less common a cause of lacunar stroke
30 of 39
Other Causes of Stroke
• Dissection
– Tear in the intima of the artery wall
– Most commonly spontaneous
– Associated with trauma in some cases
– May be iatrogenic due to endovascular treatment
– May occur in vertebral or carotid artery systems; 15% of the time dissection occurs in two or more arteries concurrently
N Engl J Med 2001: 344 (12): 898-906N Engl J Med 2001: 344 (12): 898-906

31 of 39
Other Causes: Hypercoagulable States
• Myeloproliferative disorders :
– essential thrombocytosis, polycythemia rubra vera, CML
• Antiphospholipid Antibody syndrome
• Genetic deficiencies (eg. AT3, protein C, S, APC resistance, prothrombin and factor XII mutations) are not a direct cause of arterial ischemic stroke. They may be relevant in paradoxical embolus due to their well-defined role in venous thromboembolism.

32 of 39
Other Causes: Vasculitis
• Intracranial cerebral vasculitis– Idiopathic granulomatous angiitis of the CNS
– Amyloid angiopathy vasculitis
– Systemic angiitis affecting the CNS• Lympomatoid granulomatosis• Wegener’s• PAN
• Distinguish from segmental vasospasm induced by drugs, blood

33 of 39
Key Concept: Determining Ischemic Stroke Mechanism
• Stroke mechanism is determined by inference based upon investigations completed after the fact– Eg. atrial fibrillation with normal carotid arteries
infer that the mechanism is cardioembolic
• Only about 20% of stroke is akin to coronary artery disease – ie. large artery
• The term atherothrombotic stroke is not a useful way to think about the cause of stroke because atherosclerosis is only relevant in a minority of ischemic stroke

34 of 39
ICH Type
• Anatomic Classification– Lobar
• Superficial hemorrhage extending to the cortical surface
– Sub-cortical• Basal ganglia• Thalamus• Dentate• Pontine

35 of 39
Mechanism of ICH
• Mechanistic classification– Primary (=spontaneous,
idiopathic)
• Amyloid angiopathy
• Hypertensive hemorrhage– Secondary
• AVM
• Cavernoma (venous angioma)
• Tumour
• Coagulopathy-associated
• Sympathomimetic drug-related (eg. cocaine, pseudoephedrine)
• Vasculitis
• Iatrogenic
• Traumatic
Typical deep hypertensive hemorrhage in the putamen
36 of 39
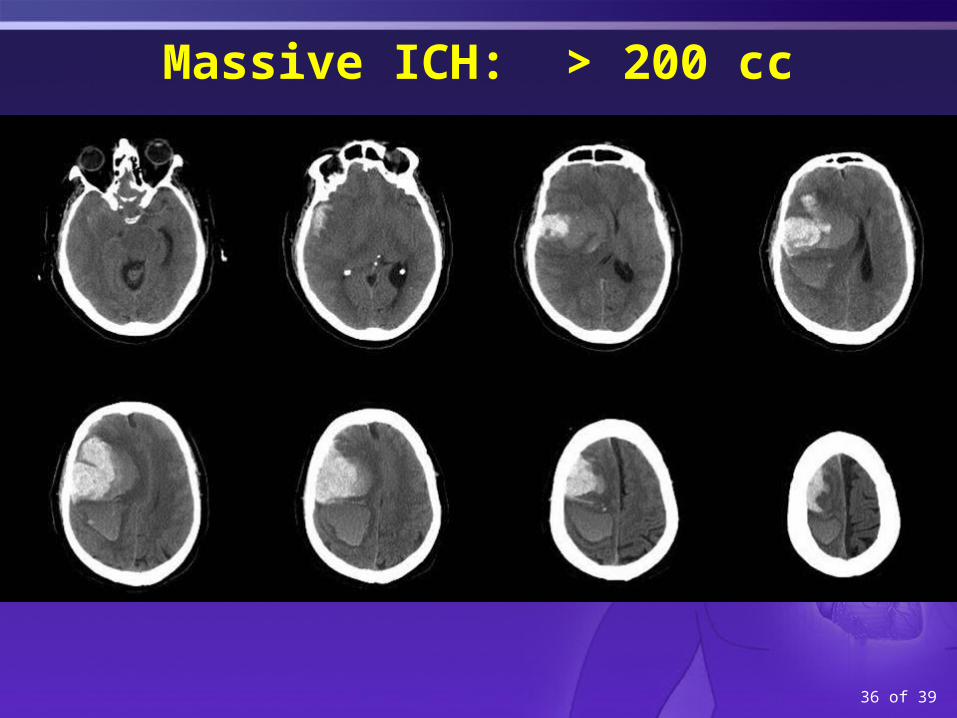
Massive ICH: > 200 cc

37 of 39
Mechanisms of SAH
• SAH – the most common cause is blunt trauma to the head
• Usually, when we discuss SAH, we are speaking of atraumatic SAH
• Cause rupture of an aneurysm of a proximal intracranial artery, usually at the circle Willis (“Berry Aneurysm”)
N Engl J Med 2006;354:387-96N Engl J Med 2006;354:387-96
38 of 39
SAH
• Atraumatic SAH
– Angiogram negative ~15% of the time (no aneurysm or arterial abnormality)
• Perimesencepalic may be the commonest angio-negative SAH
• Superficial cortical SAH may occur secondary to:
– amyloid angiopathy, venous occlusion and ischemic stroke (with and without thrombolysis). This is a relatively rare phenomenon.
• Angiography may be negative and repeat studies may show a ruptured aneurysm

39 of 39
Angiogram Negative SAH

40 of 39
ADDITIONAL RESOURCE SLIDES

41 of 39
Multiple Causes of Ischemic Stroke
Stroke 2001;32:2735Neurology 1994;44:626
Large Artery Disease Small Vessel Disease
Cardioembolic Disease
Other or No Cause Found

42 of 39
Small Vessel Arteriosclerosis – Hypertension
Occlusion
Leakage
Lacunar stroke
ICH

43 of 39
Noncardioembolic Stroke Causes
Stroke 2001;32:2735Neurology 1994;44:626
Large Artery Disease Small Vessel Disease
Other or No Cause Found

Agenda1) We best learn from our mistakes, and I have had a few of them! A few
cases of where the ED md's could have done a better job is always of high interest to residents and ED staff.
2) Risk stratification is always on the top of our minds as we see people
presenting with a miriad of symptoms and we can always get better at risk stratifying.
3) Stroke mimics and how to differentiate these from the real deal. 4) Basilar stroke presentations and how to identify them, especially when
there are bilateral symptoms. A second to that, a discussion on bilateral findings and when they are not worrying and when they are not.
5) Up and coming stroke therapies and protocols.
Risk Stratification
• Prognosis exercise
• Distinguish clearly between:– Prognostic factors– Effect modifying factors

Risk Stratification: Therapy and disposition
• Is an acute intervention warranted?
• What is the correct disposition of my patient?– Discharge home?– Outpatient clinic? If so, when?– Admit –ie. consult

Risk Stratification: Therapy and disposition
• Thrombolysis• BP treatment
– ICH– AIS / TIA– SAH
• Antithrombotic therapy (ASA, heparin)• TIA / minor stroke stratification

CT – 4.5h into stroke77yo man, tourist visiting Banff
~4h into his stroke
Intubated, coma, L hemiplegia

CTA-SI-not salvageable-palliated

50
Stroke Mimics: Diagnosing Stroke
Michael “give the juice” Hill, MD MSc FRCPC
a “get on with it” productionby “I like the smell of tPA in the morning” studio

51
Stroke Mimics
1. Migrainous phenomena2. Somatization3. Seizure4. Old stroke with emergent symptoms
Less commonly:5. Space occupying lesion – subdural, glioma, metastasis6. Metabolic toxic – hypoglycemia, alcohol, drugs7. Other stroke type – SAH8. Local – hip #, brachial or sup fem artery occlusion

52
Cases
54 yo man presents with --history of sudden collapse but no witness and so the etiology and timing is uncertain-awake, alert, mute, staring-eyes straight ahead (no gaze deviation)-plegic L side
Discussion?

53
Case
25 yo woman
-visiting from New Zealand
-presents with sudden onset diplopia, headache, neck stiffness, dysphagia, inability to move the tongue
-awake, alert, distraught affect, moves all limbs actively against gravity
-agitated, hard to get consistent exam, possibly ataxic in all four limbs, unable to walk
Thoughts?

54
Case
75 yo woman-visiting a friend in hospital-on way out of the hospital going to her car, she collapses, can’t get up-witnessed; brought to ER within 20 min-awake and alert, speaking normally, no evident hemispatial neglect-cannot move L leg
Thoughts?

55
Pitfalls
Age of patientTake a social historyExamine the patient
Remember – Most people will present with an unusual presentation of a common disease rather than an unusual disease (with a common or uncommon presentation). [Corollary of Occam’s razor but of course, Occam died of multiple causes]

Stroke Mimics in the ER
Saturday Morning Workshops

Learning Objectives:
1. To review the other conditions that present like acute ischemic stroke (mimics)
2. To have a bedside strategy to quickly and efficiently rule out these stroke “mimics” a. To avoid incorrectly over-treating a stroke mimic
b. To avoid delays in correctly treating true acute ischemic strokes and stroke mimics

Stroke is often initially a clinical diagnosis aided by a standard imaging modality that has limitations
There is a better imaging modality but it has its own limitations (mainly availability)
There is overlap in the signs of true stroke and stroke mimics
There is a treatment for true stroke that has constraints (time) and risks (hemorrhage)
The Challenge !

10. What is the risk of thrombolyzing a stroke mimic?
True stroke
(n = 243)
Stroke mimics
(n = 7)
Angioedema 3 (1.2 %) 0
Symptomatic ICH
13 (5.3%) 0
Asymptomatic ICH
30 (12.3 %) 0
Thrombolysis in Stroke Mimics. Stroke 2009

Misdiagnosis of Stroke in TPA Treated Patients. Ann Emerg Med 2003.

66 yr female brought to ER by husband
Sudden onset (~ 2 hrs ago) of slurred speech, right facial droop, and right arm weakness Headache & mild nausea earlier in the day; c/o “chills” Hx of hypertension; remote hx of complex migraine; moderate
Alzheimer’s On ASA, amlodipine, donepezil
BP = 173/94 HR = irreg (80 - 120) RR = 20 T = 38.2 PERL, normal EOM (but eyes favor the left), no carotid bruits Right lower facial droop (UMN) 3/5 strength right arm, 4/5 strength right leg Speech slurred and slightly confused

1. What should be done immediately next?
a. Complete & comprehensive neurological examination
b. Administration of 160 mg acetylsalicylic acid (ASA)
c. Blood glucose & SaO2
d. CT scan
e. ECG

5th & 6th VITAL SIGNS:

2. What is going on here?
a. Ischemic stroke
b. Subarachnoid hemorrhage
c. Stroke mimic
d. Stroke chameleon
e. Any of the above

3. What is the difference between a stroke & a stroke mimic?
Stroke ~ sudden onset of a focal neurological deficit in a recognizable intracranial vascular distribution resulting in a common clinical syndrome due to vascular occlusion or hemorrhage
Stroke mimic ~ a nonvascular condition that may simulate stroke

4. What are some common stroke mimics?
METABOLIC / SYSTEMIC CONDITIONS: Hypoglycemia / hyperglycemia Hepatic encephalopathy Hypertensive encephalopathy
CNS CONDITIONS: Post-ictal state with focal neurological signs (Todd’s paresis) Nonconvulsive status epilepticus Hemiplegic migraine Subdural hematoma Brain abscess Intracranial tumour (primary / metastatic) Multiple sclerosis
PSYCHIATRIC CONDITIONS: Conversion disorder Factitious disorder

5. How common are stroke mimics?
a. 9%
b. 4%
c. 13%
d. 1.2%
e. All of the above

Norris(1982)
Libman (1995)
Kothari(1995)
Alder(1999)
Ay (1999)
When was diagnosis made?
At stroke unit admission
After initial ED
assessment
At admission from ED
Within 6 hrs of onset
Unclear
Who diagnosed the stroke?
Intern, family physician, neurology resident
Emergency physician
Emergency physician
Unclear; likely
neurologists
Neurologists
What studies were done to arrive at the diagnosis?
History, physical
History, physical
History, physical, labs, CT
Unclear CT, labs
Were other studies eventually performed?
Multiple, few CTs
Some CTs Unclear MRI, MRA, DMI, PMI
MRI, DMI
How many stroke mimics were there? 13% 19% 4% 9% 1.2%
Huff. Emerg Med Clin N Am. 2002

6. What features suggest that this is a stroke? Age? Risk factors? Current BP? Irregular heart rate? Recognizable vascular distribution / clinical pattern?
7. What features suggest that this is a mimic? Headache & nausea? Chills & fever? Migraine history? Workshop title?

Incidence of Stroke Mimics by Age Groups. J Stroke Cerebrovasc Dis 2008.
Nearly 1/3 of older patients with true stroke had features of stroke mimic

Hand et al. The Brain Attack Study. Stroke 2006;37:769
Prospective observational study, single center, N = 350 Univariate analysis = 47 parameters
FAVORING MIMIC: Hx of cognitive impairment Confusion, loss of consciousness, seizure at onset No neurological signs, signs that do not lateralize/localize, or signs that do
not fit a vascular territory or clinical syndrome Abnormal findings in other systems
FAVORING STROKE: Hx of CAD or PVD Exact time of onset Definite lateralizing /localizing neurological symptoms, demonstrable
neurological signs Signs consistent with clinical stroke syndrome

The Brain Attack Study. Stroke 2006

Recognition of Stroke in the Emergency Room (ROSIER). Lancet Neurol 2005

FAVORING MIMIC:
Confusion Loss of consciousness Seizure at onset No neurological signs Signs that do not
lateralize Signs that do not fit a
vascular territory or clinical syndrome
Signs in other systems
FAVORING STROKE:
CVD history IHD, PVD Exact time of onset Definite neurological
symptoms Demonstrable
neurological signs Signs consistent with
clinical stroke syndrome

Glucose = 6.6 Normal routine chemistry Platelets = 455 INR = 1.2 ECG = atrial fibrillation Prior to CT she vomits once & receives 10 mg IV
metoclopramide On return from CT her neurological symptoms are
rapidly improving CT is normal Subsequent MRI & MRA is normal

Migraine Equivalent:
Migraine without pain (5%)AKA migraine variantProlonged aura (can be atypical)Focal neurological signs ICHD-2 (2004)
Hemiplegic migraine Opthalmoplegic migraine Retinal migraine Vertiginous migraine Acute confusional migraine

8. How long can hemiplegic migraine last?
a. Less than 1 hr
b. Less than 4.5 hrs
c. Less than 24 hrs
d. Less than 72 hrs
e. More than 72 hrs

9. What is the longest hemiplegic migraine reported on the internet?
77 days

Summary (cont’d):
Differentiation of some can be difficult Consult liberally Where feasible MR can be diagnostic
Neurologist on-call Radiologist on-call

52 yr male
EMS Report: Found on floor in restaurant restroom Mâitre-d’ recognizes him having walked in alone 50
minutes ago; he was walking and talking “okay” Waiter reports that he seemed “normal” when he
ordered a drink 30 minutes ago, asked where the restrooms were, and walked there “like normal”
Incontinent of urine & stoolWallet – businessman from Alberta; home phone
number ~ no answer; no NOK listed

EMS ~ “code-stroke” ~ stroke center bypass
No previous chart; only history is from EMS BP = 158/84 HR = 100 RR = 12 SaO2 = 98% T = 36.4
Markedly slurred speech; appears confused PERL, normal EOM (but eyes favor the left) 3/5 strength left arm, 2/5 strength leg Strong odor of alcohol on his breath Very large BMI
60

1. What should be done immediately next?
a. Blood glucose
b. Mobilize staff for CT scan
c. Venous access
d. CBC, INR, routine chemistry
e. All of the above can be done concurrently

2. What is going on here?
a. Ischemic stroke
b. Subarachnoid hemorrhage
c. Stroke mimic
d. Too many martinis at today’s business lunch
e. Any of the above

3. What features suggest that this is a mimic? Confusion? Incontinence? Alcohol on breath? His age?
4. So, is this a mimic?

Glucose = 11.5 Normal routine chemistry Platelets = 125 INR = 1.1 CT is normal ECG = minor LV strain His neuro exam is
unchanged
5. What will you do next?
90

Collateral from local businessman who was to meet him at restaurant Just met at conference today Patient was upset
Brother had recently had a stroke and is bed-ridden Hated seeing him that way (“better off dead”)
Said he himself was healthy
His neuro exam is unchanged
6. What will you do next?120

Search of his briefcase (brought by local businessman) Bottle of pills His neuro exam is unchanged
7. What might this be & what will you do next?
145

8. What is Todd’s paresis? Occurs in up to 13% of seizures Most common after GM seizures Mechanism unclear
9. How long can it last? Usually hours, but rare cases up to several
days

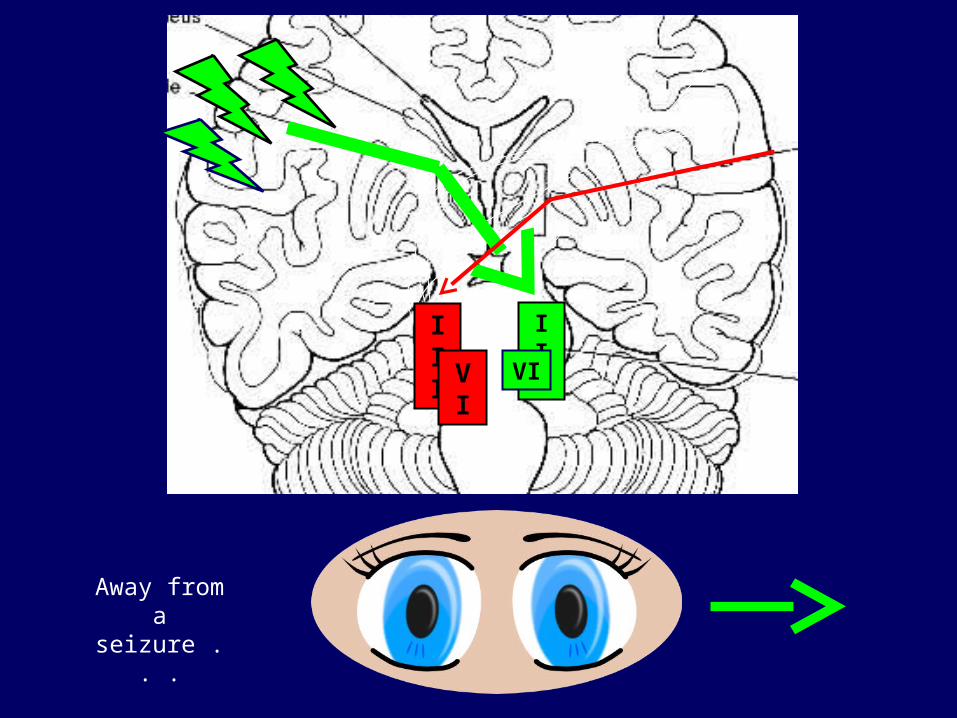
11. Why do both patients look left?
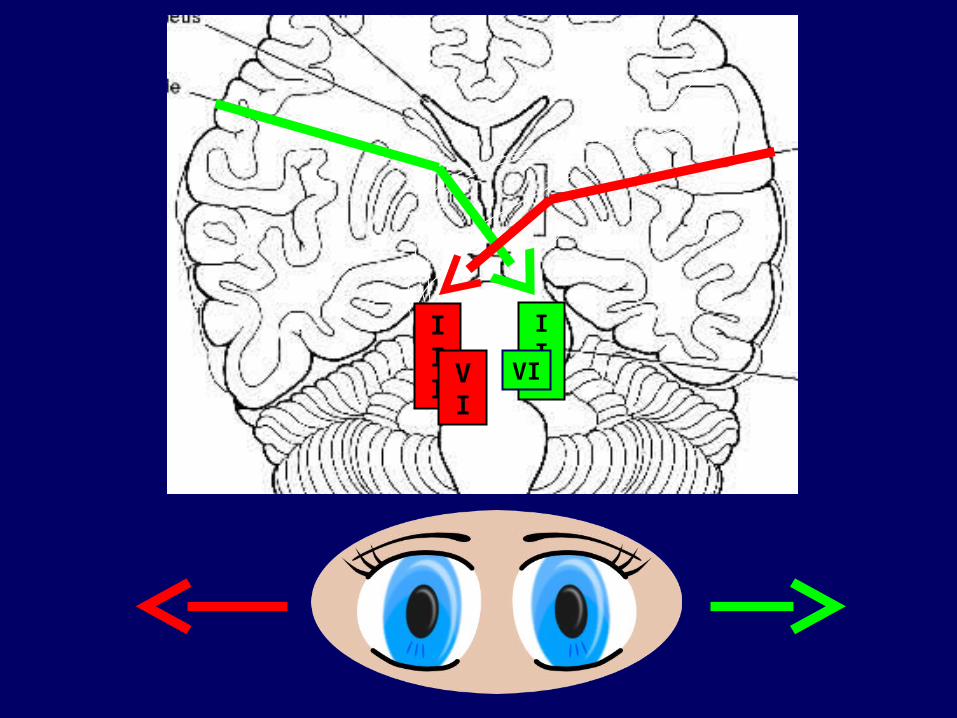
III III
VI VI
III III
VI VI
Away from a seizure . . .

III III
VI VI
Towards a stroke . . .

A few more mimics not to miss . . . what
are these?

Any questions????

Summary:
Stroke mimics occur in 2 – 20% of acute neurologic deficits
Most commonly hypoglycemia, migraine equivalent, Todd’s paresis
Most others will be diagnosed by imaging & labs
Most important is to efficiently identify those with true strokes who may benefit from thrombolytic therapy

Approach to Coma
Related Documents











