DOI 10.1378/chest.102.1.216 1992;102;216-220 Chest J Tuchschmidt, J Fried, M Astiz and E Rackow improves outcome in septic shock. Elevation of cardiac output and oxygen delivery http://chestjournal.chestpubs.org/content/102/1/216 can be found online on the World Wide Web at: The online version of this article, along with updated information and services ) ISSN:0012-3692 http://chestjournal.chestpubs.org/site/misc/reprints.xhtml ( without the prior written permission of the copyright holder. reserved. No part of this article or PDF may be reproduced or distributed Chest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights of been published monthly since 1935. Copyright1992by the American College is the official journal of the American College of Chest Physicians. It has Chest © 1992 American College of Chest Physicians by guest on July 10, 2011 chestjournal.chestpubs.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DOI 10.1378/chest.102.1.216 1992;102;216-220Chest
J Tuchschmidt, J Fried, M Astiz and E Rackow improves outcome in septic shock.Elevation of cardiac output and oxygen delivery
http://chestjournal.chestpubs.org/content/102/1/216
can be found online on the World Wide Web at: The online version of this article, along with updated information and services
) ISSN:0012-3692http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(without the prior written permission of the copyright holder.reserved. No part of this article or PDF may be reproduced or distributedChest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights
ofbeen published monthly since 1935. Copyright1992by the American College is the official journal of the American College of Chest Physicians. It hasChest
© 1992 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from

216 Improved Outcome In Septic Shock (Tuchschmidtet&)
Elevation of Cardiac Output and OxygenDelivery Improves Outcome in SepticShock*James Tuchschmidt, M.D., FC.C.P;Jeffrey Fried, M.D., FC.C.P;
Mark Astiz, M.D., F.C.C.P; and Eric Rackou� M.D., F.C.C.P
Septic shock is characterized by hypoperfusion and tissueenergy defects. We prospectively evaluated the therapeutic
benefit of augmenting cardiac output and therefore oxygen
delivery (Do,) on mortality in patients with septic shock.
Twenty-five patients were randomized to a normal treat-
ment (NT) group and 26 patients were randomized to an
optimal treatment (�YF) group. All patients had a clinically
evident site of infection, sepsis as defined by a systemic
response to the infection, and shock indicated by systemic
hypoperfusion. Patients were treated during the initial 72
h by an algorithm differing only in the end point ofresuscitation. The cardiac index (CI) was increased to 3.0
Ijmin/m’ in the NT group and to 6 IJniin/m’ in the OT
group. There were no significant differences in cardiores-
piratory parameters in the NT and OT groups on entrance
into the study. During treatment, CI averaged 3.6 ± 0.2 L/
min/m’ and Do, averaged 8.6±0.8 mI/mm/kg in the NT
group and CI averaged 5. 1 ±0.2 Lfmin/m’ and Do, aver-
aged 12.2±0.7 mI/mm/hg in the OT group (p<O.Ol). A
significant correlation between Do, and survival was oh-
served. Seventy-two percent of the (Yf patients died vs 50
percent ofthe NT patients (p 0.14) Surviving NT patients
stayed 13.7±3 days in the ICU vs 7.4±0.6 days (p<O.OS)
for the OT patients. Since some of the NT patients were
spontaneously hyperdynamic and some of the (fl patients
did not achieve their desired end point, patients were
arbitrarily subsetted using a midpoint CI of 4.5 IJmin/m’.
The NT <4.5 group had a CI of3.1±0.2 L/min/m’ and
Do, of 10.9± 1.0 mI/mm/kg while the (YI� group >4.5 L/
min/m’ had a CI of 5.7±0.2 L/min/m’ and a Do, of
13.8±0.7 mI/mm/kg (p<O.Ol) Mortality in the NT <4.5
group was 74 percent as compared with 40 percent in the
OT >4.5 group (p<0.05). (Chest 1992; 102:216-20)
Clcardiac index; COcardiac output; Dooxygen dcliv-cry; NT = normal treatment; OT optimal treatment;PAOPpulmonary artery occlusion pressure; SAP systolicarterial pressure; Vo, oxygen consumption
Septic shock is characterized by an imbalance be-
tween systemic oxygen demand and oxygen sup-
ply. The marked lactic acidosis observed during septic
shock is indicative of a severe tissue energy deficit. ‘�
Primary metabolic failure, shifts in the oxygen disso-
ciation curve, and circulatory flow abnormalities have
all been postulated to contribute to impaired oxygen
utilization during sepsis.4 Experimental studies have
demonstrated a relationship between tissue energy
deficits and effective organ perfusion.56 Clinical ob-
servations of regional hypoperfusion and altered mi-
crovascular response to reactive hyperemia are consis-
tent with circulatory maldistribution.7’8 These studies
suggest the potential for reversing tissue energy defi-
cits by increasing oxygen delivery during septic shock.
The optimal levels of oxygen delivery appear to be
significantly higher than under normal physiologic
conditions both because of increased metabolic de-
mands and decreased oxygen extraction.9”#{176} Recently,
Shoemaker et al’#{176}and Edwards et al” reported
improved survival in critically ill patients, some of
*From the Section of Pulmonary Disease and Critical Care Medi-
cine, the Department of Medicine, the University of SouthernCalifornia School of Medicine, Los Angeles (Drs. Tuchschmidtand Fried), and Section ofCritical Care Medicine, Department ofMedicine, St. Vincent�s Hospital and Medical Center ofNew York,New York Medical College, New York, NY(Drs. Astiz and Rackow).
Manuscript received September 17; revision accepted January 31.Reprint requests: Dr Schobe#{231} St. Vsncent�s Hospital Medical Center,LS3 West 11th Street, New York City 10011
whom were septic, when therapy was titrated to
increased indices of flow and oxygen metabolism.
The purpose of this study was to prospectively
evaluate the therapeutic effect of augmenting cardiac
output and therefore oxygen delivery on mortality in
patients with septic shock. Our data suggest that
mortality may be reduced by increasing cardiac output
and oxygen delivery.
METHODS
Patients
All patients admitted over a 24-month period to the Critical Care
Service at Los Angeles County/University of Southern California
Medical Center, Los Angeles, with a suspected diagnosis of septic
shock had their conditions evaluated. The study was approved by
the Institutional Review Board. Infection was confirmed in patientswith bacteremia or an identifiable site ofinfection. Sites of infection
were identified by positive bacterial cultures with evidence of
inflammatory cells on Gram stain of exudates. Sepsis was defined
as a systemic response to infection as characterized by four of the
following clinical signs: (1) fever (temperature >38.3#{176}C) or hypo-thermia (temperature <35.5#{176}C); (2) tachycardia (heart rate >90
heats/mm); (3) tachypnea (>20 breathsfmin); (4) leukocytosis (WBC
>11,00Wcu mm3); or (5) delirium. Shock was identified by any oneof the following signs: (1) systolic intra-arterial pressure <90 mm
Hg on two measurements, 1 h apart; (2) intravenous (IV) infusion of
dopamine for greater than 1 h to maintain intra-arterial systolic
pressure �90 mm Hg; or (3) arterial lactate �3.0 mmolfL. All
patients were entered within 4 h of diagnosing shock and enrolled
with a suspected site of infection, evidence of sepsis, and criteria
for shock. Patients without an identified site of infection at 48 h
were removed from the study. Once entered, the patients were
assigned to the normal treatment (NT) group or optimal treatment
© 1992 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from

Table 1-Hemodyna,nic Profiles PYcresusCitatiOn and Postresuscitation in the Normal Treatment (NT) and Optimal
Treatment (OT) Patients
Preresuscitation Fbstresuscitation
NT cir r�’r irVariable (n 25) (n = 26) (n 25) (n 26)
Age,yr 53±4 49±3 - -
Apache!! 21±1 22±1 - -
Temp. #{176}C 37.7±0.17 37.8±0.11 37.3±0.11 37±0.06
RR,breaths/min 24±2 26±1 22±3 22±1
Pulse,beats/min 124±4 112±4 112±3 110±3
MAP,mmHg 74±3 74±3 73±2 75±2
MPAP,mmHg 27±2 26±1 30±1 27±1
PAOP, mm Hg 13± 1 15± 1 16 ± 1 16±1
CI, 11mm/rn’ 3.9±0.3 4.0±0.3 3.6±0.2 5.1±2*
HGB, g/dl 11.0±0.5 11.0±0.4 10.3±0.4 10.2±0.3Do,, mi/mitt/kg 14.9±1.5 16.1±1.2 14.0±0.3 18.8±0.4*
Vo,, mI/mm/kg 3.5±0.2 3.6±0.3 3.7±0.6 3.7±0.1
Lactate,mmolfL 5.1±0.6 4.7±0.1 4.5±0.8 3.8±0.6
*N5 vs 0’!’, p<O.Ol.
CHEST I 102 I 1 I JULY, 1992 217
(OlD group by dynamic randomization.
Patient Management
After obtaining appropriate blood and site cultures, all patients
received gentamicin 2 mg/kg IV followed by 1.7 ms/kg IV every 8
h (monitored with serum levels) and clindamycin 900 mg IV every
8 h. Additional antibiotics were added depending on the presumed
site of infection and suspected becteriolog� Once an organism was
identified, the antibiotic regimen was tailored appropriately. Every
effort was made to identify and drain infected sites.
Resuscitation from shock was standardized by the use ofa printed
algorithm, which also served as a notification ofgroup assignment.
The algorithms for the NT and OT groups were identical except
with respect to the end point ofresuscitation. The NT resuscitativeefforts were considered to be complete when a cardiac index (CI)�3.0 Llmin/m’ and a systolic arterial pressure (SAP) of �90 mm
Hg were achieved. A CI �6.0 Llmin/m’ and a SAP �90 mm Hg
defined resuscitative end points for the OT patients. The algorithm
consisted of first determining whether patients satisfied the resus-
citation goals. Ifthey did not, 5 percent albumin was administered
by aliquots to achieve a pulmonary artery occlusion pressure (PAOP)
�15 mm Hg. In hypotensive patients with a PAOP �15 mm Hg, a
dopamine infusion was titrated to maintain a SAP �90 mm Hg.
When the PAOP was �15 mm Hg, the SAP was �90 mm Hg, and
the CI was below the desired goal, dobutamine was infused andtitrated to obtain the desired CI. Patients receiving dopamine with
a PAOP <15 mm Hg, who otherwise met the assigned goals� were
fluid challenged with 5 percent albumin in an effort to withdraw
vasopressor support.
The resuscitative goals were maintained for 72 h. Patients were
transfused to maintain a hemoglobin ofat least 10 g/dl. All patientswere intubated and mechanically ventilated. Supplemental oxygen
and PEEP were adjusted to maintain the arterial oxygen saturation
�90 percent, with the least possible Flo,. Nutritional support was
initiated in all patients after hemodynamic stability was achieved,
usually within 48 to 72 h ofhospital admission.
HemOdynamiC Measurements
Intravascular pressures were measured with strain gauge trans-
ducers (Baxter Edwards Laboratories, Irvine, Calil), zeroed to
atmospheric pressure at the midaxillary line, and calibrated against
a mercury manometer. Cardiac output (CO) values were obtainedin triplicate by thermodilution using iced saline solution cooled to
<1#{176}C.Hemoglobin saturation was measured with a COoximeter
(282, Instrumentation Laboratories, Lexington, Mass). Hemody-
namic variables, arterial and mixed venous blood gases, and arterial
lactate were obtained simultaneously, at least every 6 h. Oxygen
delivery (Do,) was calculated as Do,= CO x CaO,; and oxygen
consumption (Vo,) as VO2 = CO x (CaO,- CvO,). Oxygen content
was calculated as follows: CaO, 1 .39 x (Hgb) x SaO, and
CvO, = 1.39 x (Hgb) x SvO,, where SaO, and SvO, are the arterial
and mixed venous oxygen saturations, respectively.
Statistical Analysis
We compared continuous variable data using the Student’s t test
and compared mortality data using x’ analysis. The CI and other
variables were averaged over the 72-h period following the initial
resuscitative efforts (>6 h after entry) to obtain the postresuscitation
values.
Some patients assigned to the NT group exceeded their treatment
goal on admission to the study, and some patients randomized to
the �YF group failed to achieve a CI �6.0 Iimin/m2. We therefore
subsetted patients into two groups using a midpoint CI value of 4.5
lJmin/m’ and compared the NT group with a postresuscitation CI
<4.5 LJmiWm’ to the OT group with a CI >4.5 11mm/rn’. These
groups were then compared using the same statistical methods.
Results are reported as mean±SEM. Statistical significance isreported at a p<O.05.
RESULTS
Seventy patients were enrolled during the course of
the study. Nineteen of these were not included in the
analysis for the following reasons: in nine patients,
blood and site cultures were negative; six patients died
prior to treatment; three patients did not meet shock
criteria. Fifty-one subjects were analyzed, 25 patients
in the NT group and 26 patients in the OT group. The
most common infections were pneumonia in 53 per-
cent, urosepsis in 10 percent, and peritonitis in 8
percent. Fifty-seven percent of the patients had posi-
tive blood cultures. Sixty-five percent of the patients
had Gram-negative infections and 35 percent had
Gram-positive infections.
Normal vs Optimal Treatment
The clinical and hemodynamic profiles of the pa-
tients on entry into the study are shown in Table 1.
© 1992 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from
fI��
0 6 12 18 24 30 36 42 48 54 60 66 72TIME (HRS)
0-8.5 9042.9 13.0.16.9 17.0-20.9 21.0.24.9 25.0.
6
218 Improved Outcome in Septic Shock (Tuchschmidt et a!)
2
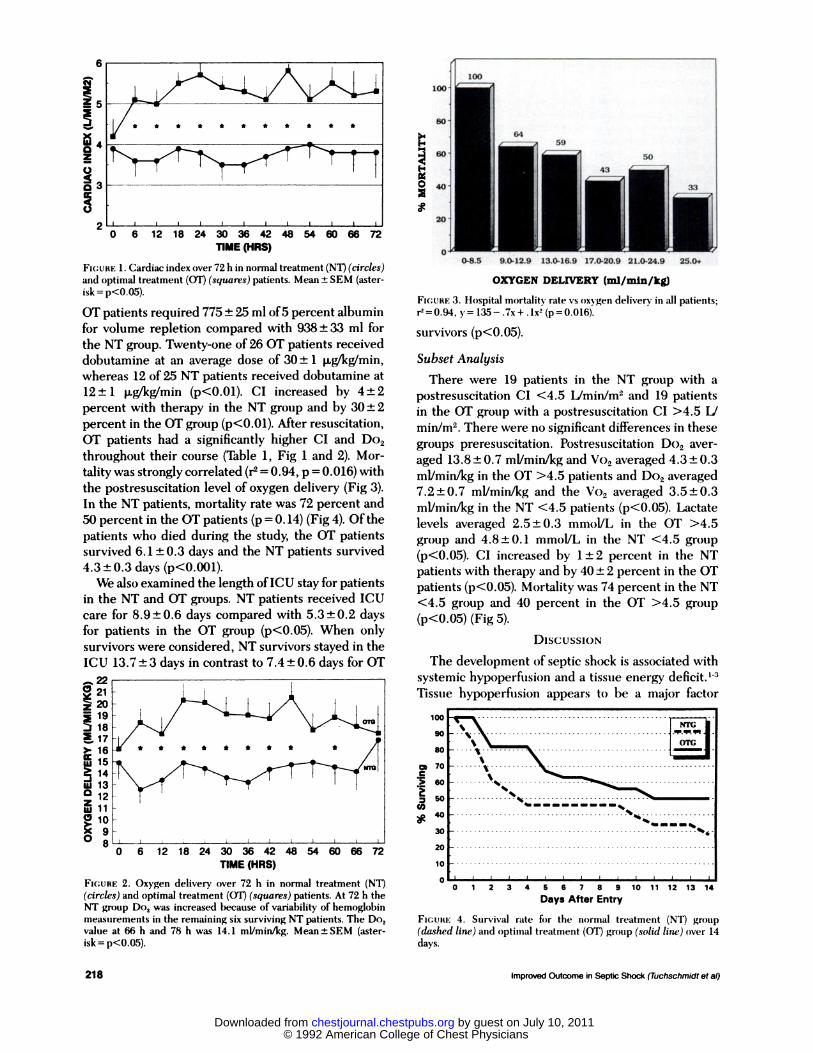
FIGURE 1 . Cardiac index over 72 h in normal treatment (NT) (circles)and optimal treatment (OT) (squares) patients. Mean ± SEM (aster-
isk p<O.05).
OT patients required 775 ± 25 ml of5 percent albumin
for volume repletion compared with 938 ± 33 ml for
the NT group. Twenty-one of 26 OT patients received
dobutamine at an average dose of 30 ± 1 p�gfkg/min,
whereas 12 of 25 NT patients received dobutamine at
12 ± 1 p�gfkg’min (p<O.Ol). CI increased by 4 ± 2
percent with therapy in the NT group and by 30 ± 2
percent in the OT group (p<O.Ol). After resuscitation,
OT patients had a significantly higher CI and Do2
throughout their course (Table 1 , Fig 1 and 2). Mor-
tality was strongly correlated (r� 0.94, p = 0.016) with
the postresuscitation level of oxygen delivery (Fig 3).
In the NT patients, mortality rate was 72 percent and
50 percent in the OT patients (p = 0. 14) (Fig 4). Of the
patients who died during the study, the OT patients
survived 6. 1 ± 0.3 days and the NT patients survived
4.3±0.3 days (p<O.00l).
We also examined the length ofICU stay for patients
in the NT and OT groups. NT patients received ICU
care for 8.9 ± 0.6 days compared with 5.3 ± 0.2 days
for patients in the OT group (p<0.05). When only
survivors were considered, NT survivors stayed in the
ICU 13.7 ± 3 days in contrast to 7.4 ± 0.6 days for OT
0 21z� 19
18�17>. 16� 15� 14‘U 13� 12w 11
� 10
0 6 12 18 24 30 36 42 48 54 60 66 72
TIME (HRS)
FIGURE 2. Oxygen delivery over 72 h in normal treatment (NT)
(circles) and optimal treatment (OT) (squares) patients. At 72 h theNT group Do2 was increased because of variability of hemoglobin
measurements in the remaining six surviving NT patients. The Do,value at 66 h and 78 h was 14.1 mI/mm/kg. Mean±SEM (aster-
isk = p<O.O5).
OXYGEN DELWERY (mi/mm/kg)
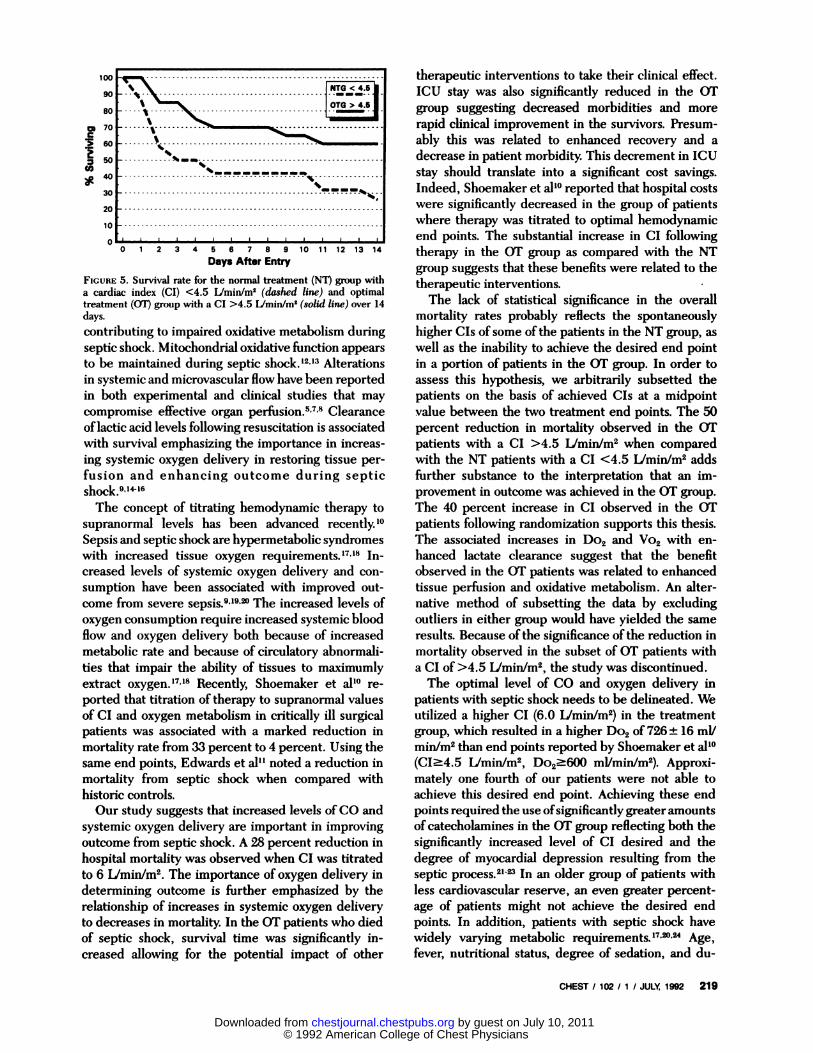
FIcURE 3. Hospital mortality rate vs oxygen delivery in all patients;
r�O.94,y=135-.7x+.1x2(p=0.016).
survivors (p<O.O5).
Subset Analysis
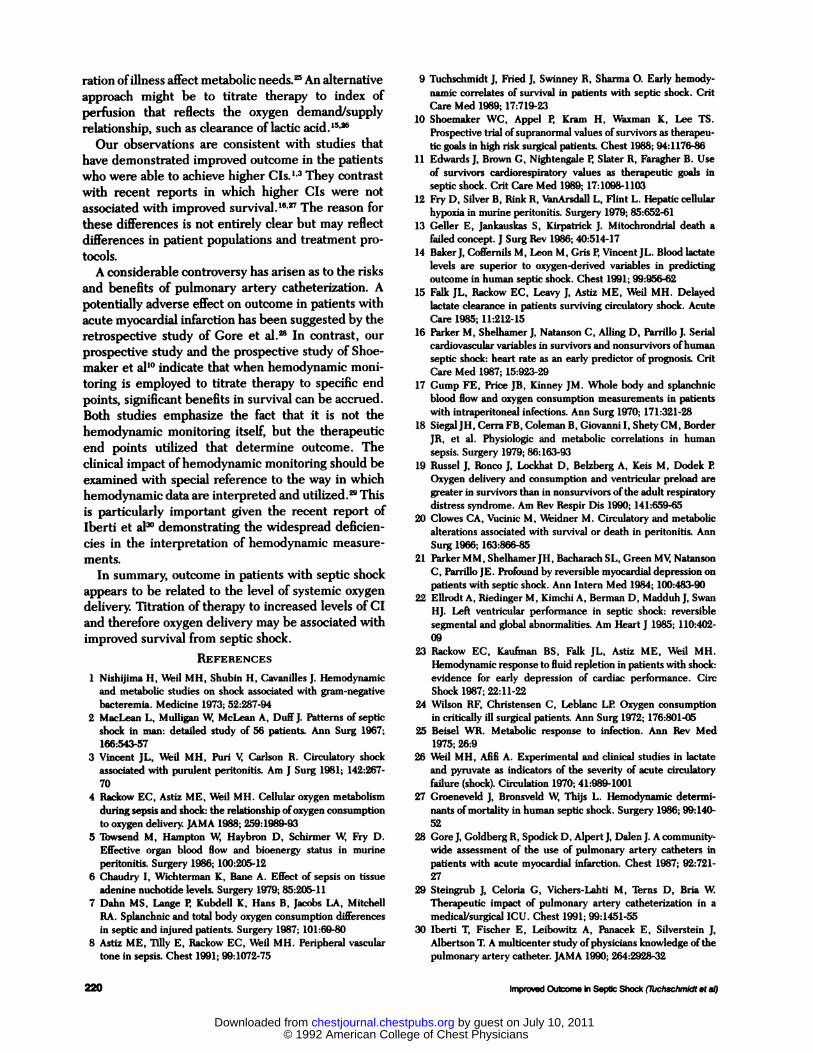
There were 19 patients in the NT group with a
postresuscitation CI <4.5 IJmin/m and 19 patients
in the OT group with a postresuscitation CI >4.5 L/
minim2. There were no significant differences in these
groups preresuscitation. Postresuscitation Do2 aver-
aged 13.8 ± 0.7 mI/mm/kg and Vo2 averaged 4.3 ± 0.3
mi/mm/kg in the OT >4.5 patients and Do2 averaged
7.2 ± 0.7 mI/mm/kg and the Vo2 averaged 3.5 ± 0.3
mi/mm/kg in the NT <4.5 patients (p<O.O5). Lactate
levels averaged 2.5±0.3 mmolJL in the OT >4.5
group and 4.8±0.1 mmolIL in the NT <4.5 group
(p<O.O5). CI increased by 1 ± 2 percent in the NT
patients with therapy and by 40 ± 2 percent in the OT
patients (p<O.OS). Mortality was 74 percent in the NT
<4.5 group and 40 percent in the OT >4.5 group
(p<O.OS) (Fig 5).
DISCUSSION
The development of septic shock is associated with
systemic hypoperfusion and a tissue energy deficit. ‘-�
Tissue hypoperfusion appears to be a major factor
U)
100
90
80
70
60
50
40
30
20
10
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Days After Entry
FIGURE 4. Survival rate for the normal treatment (NT) group
(dashed line) and optimal treatment (OT) group (solid line) over 14
days.
© 1992 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from
CHEST I 102 I 1 I JULY, 1992 219
100 _____90
80
m 70C
�60
n 50U)�4o
30
20
10
0-.�-�0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Days After Entry
FIGURE 5. Survival rate for the normal treatment (NT) group with
a cardiac index (CI) <4.5 Lfmin/m’ (dashed line) and optimaltreatment (OT) group with a CI >4.5 Lfmin/m’ (solid line) over 14
days.
contributing to impaired oxidative metabolism during
septic shock. Mitochondrial oxidative function appears
to be maintained during septic shock.’2”3 Alterations
in systemic and microvascular flow have been reported
in both experimental and clinical studies that may
compromise effective organ perfusion.5’7’8 Clearance
oflactic acid levels following resuscitation is associated
with survival emphasizing the importance in increas-
ing systemic oxygen delivery in restoring tissue per-
fusion and enhancing outcome during septic
1416
The concept of titrating hemodynamic therapy to
supranormal levels has been advanced ‘#{176}
Sepsis and septic shock are hypermetabolic syndromes
with increased tissue oxygen requirements.’7”8 In-
creased levels of systemic oxygen delivery and con-
sumption have been associated with improved out-
come from severe sepsis.9”9’2#{176}The increased levels of
oxygen consumption require increased systemic blood
flow and oxygen delivery both because of increased
metabolic rate and because of circulatory abnormali-
ties that impair the ability of tissues to maximumly
extract xy’7”8 Recently, Shoemaker et albo re-
ported that titration of therapy to supranormal values
of CI and oxygen metabolism in critically ill surgical
patients was associated with a marked reduction in
mortality rate from 33 percent to 4 percent. Using the
same end points, Edwards et al” noted a reduction in
mortality from septic shock when compared with
historic controls.Our study suggests that increased levels of CO and
systemic oxygen delivery are important in improving
outcome from septic shock. A 28 percent reduction in
hospital mortality was observed when CI was titrated
to 6 Iimin/m2. The importance of oxygen delivery in
determining outcome is further emphasized by the
relationship of increases in systemic oxygen delivery
to decreases in mortality. In the OT patients who died
of septic shock, survival time was significantly in-
creased allowing for the potential impact of other
therapeutic interventions to take their clinical effect.
ICU stay was also significantly reduced in the OT
group suggesting decreased morbidities and more
rapid clinical improvement in the survivors. Presum-
ably this was related to enhanced recovery and a
decrease in patient morbidity. This decrement in ICU
stay should translate into a significant cost savings.
Indeed, Shoemaker et al’#{176}reported that hospital costs
were significantly decreased in the group of patients
where therapy was titrated to optimal hemodynamic
end points. The substantial increase in CI following
therapy in the OT group as compared with the NT
group suggests that these benefits were related to the
therapeutic interventions.
The lack of statistical significance in the overall
mortality rates probably reflects the spontaneously
higher CIs of some of the patients in the NT group, as
well as the inability to achieve the desired end point
in a portion of patients in the OT group. In order to
assess this hypothesis, we arbitrarily subsetted the
patients on the basis of achieved CIs at a midpoint
value between the two treatment end points. The 50
percent reduction in mortality observed in the (IF
patients with a CI >4.5 L/min/m2 when compared
with the NT patients with a CI <4.5 L/min/m2 adds
further substance to the interpretation that an im-
provement in outcome was achieved in the (IF group.
The 40 percent increase in CI observed in the OT
patients following randomization supports this thesis.
The associated increases in Do2 and Vo2 with en-
hanced lactate clearance suggest that the benefit
observed in the (IF patients was related to enhanced
tissue perfusion and oxidative metabolism. An alter-
native method of subsetting the data by excluding
outliers in either group would have yielded the same
results. Because of the significance of the reduction in
mortality observed in the subset of (IF patients with
a CI of >4.5 Llmin/m2, the study was discontinued.
The optimal level of CO and oxygen delivery in
patients with septic shock needs to be delineated. We
utilized a higher CI (6.0 L/min/m2) in the treatment
group, which resulted in a higher Do2 of 726 ± 16 ml!
min/m2 than end points reported by Shoemaker et al’#{176}
(CI�4.5 Llmin/m2, Do2�600 mI/minim2). Approxi-
mately one fourth of our patients were not able to
achieve this desired end point. Achieving these end
points required the use ofsignificantly greater amounts
ofcatecholamines in the (IF group reflecting both the
significantly increased level of CI desired and the
degree of myocardial depression resulting from the
septic process.2� In an older group of patients with
less cardiovascular reserve, an even greater percent-
age of patients might not achieve the desired end
points. In addition, patients with septic shock have
widely varying metabolic requirements.’7’� Age,
fever, nutritional status, degree of sedation, and du-
© 1992 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from
220 Improved Outcome in Septic Shock (Tuchschm!dtetal)
ration oflilness affect metabolic needs.� An alternative
approach might be to titrate therapy to index of
perfusion that reflects the oxygen demand/supply
relationship, such as clearance oflactic acid.’5’�
Our observations are consistent with studies that
have demonstrated impmved outcome in the patients
who were able to achieve higher CIs.”3 They contrast
with recent reports in which higher CIs were not
associated with improved rviallS,V The reason for
these differences is not entirely clear but may reflect
differences in patient populations and treatment pro-
tocols.
A considerable controversy has arisen as to the risks
and benefits of pulmonary artery catheterization. A
potentially adverse effect on outcome in patients with
acute myocardial infarction has been suggested by the
retrospective study of Gore et al.� In contrast, our
prospective study and the prospective study of Shoe-
maker et al’#{176}indicate that when hemodynamic moni-
toring is employed to titrate therapy to specific end
points, significant benefits in survival can be accrued.
Both studies emphasize the fact that it is not the
hemodynamic monitoring itself, but the therapeutic
end points utilized that determine outcome. The
clinical impact ofhemodynamic monitoring should be
examined with special reference to the way in which
hemodynamic data are interpreted and utiuized.� This
is particularly important given the recent report of
Iberti et al30 demonstrating the widespread deficien-
cies in the interpretation of hemodynamic measure-
ments.
In summary, outcome in patients with septic shock
appears to be related to the level of systemic oxygen
delivery. Titration of therapy to increased levels of CI
and therefore oxygen delivery may be associated with
improved survival from septic shock.
REFERENCES
1 Nishijima H, Weil MH, Shubin H, Cavanilles J. Hemodynamicand metabolic studies on shock associated with gram-negative
bacteremia. Medicine 1973; 52:267-94
2 MacLoan L, Mulligan W, McLean A, DUffJ. Patterns of septic
shock in man: detailed study of 56 patients. Ann Surg 1967;166:543-57
3 Vincent JL, Weil MH, Purl V, Carlson R. Circulatory shock
associated with purulent peritonitis. Am J Surg 1981; 142:267-
70
4 Rackow EC, Astiz ME, Weil MH. Cellular oxygen metabolismduring sepsis and shock: the relationship ofoxygen consumptionto oxygen delivery. JAMA 1988; 259:1989-93
5 Towsend M, Hampton W, Haybron D, Schirmer W, Fry D.Effective organ blood flow and bioenergy status in murine
peritonitis. Surgery 1986; 100:205-12
6 Chaudry I, Wichterman K, Bane A. Effect of sepsis on tissue
adenine nuchotide levels. Surgery 1979; 85:205-117 Dahn MS. Lange P. Kubdell K, Hans B, Jacobs LA, Mitchell
BA. Splanchmc and total body oxygen consumption differences
in septic and injured patients. Surgery 1987; 101:69-808 Astlz ME, Tilly E, Backow EC, Weil MH. Peripheral vascular
tone in sepsis. Chest 1991; 99:1072-75
9 Tuchschmidt J, Fried J, Swinney R, Sharma 0. Early hemody-namic correlates of survival in patients with septic shock. Cnt
Care Med 1989; 17:719-23
10 Shoemaker WC, Appal P. Kram H, Waxman K, Lee TS.Prospective trial ofsupranormal values of survivors as therapeu-
tic goals in high risk surgical patients. Chest 1988; 94:1176-8611 Edwards J, Brown C, Nightengale P. Slater R, Faragher B. Use
of survivors cardiorespiratory values as therapeutic goals in
septic shock. Crit Care Med 1989; 17:1098-1103
12 Fry D, Silver B, Rink R, VanArsdall L, Flint L. Hepatic cellular
hypoxia in murine peritonitis. Surgery 1979; 85:652-61
13 Geller E, Jankauskas 5, Kirpatrick J. Mitochrondrial death a
failed concept. J Surg Rev 1986; 40:514-17
14 BakerJ, Coffernils M, Leon M, Gris P. VincentJL. Blood lactatelevels are superior to oxygen-derived variables in predicting
outcome in human septic shock. Chest 1991; 99:956-62
15 Fallc JL, Rackow EC, Leavy J, Astiz ME, Weil MH. Delayedlactate clearance in patients surviving circulatory shock. Acute
Care 1985; 11:212-1516 Parker M, Shelhamer J, Natanson C, Ailing D, Parrillo J. Serial
cardiovascular variables in survivors and nonsurvivors of humanseptic shock: heart rate as an early predictor of prognosis. Crit
Care Med 1987; 15:923-2917 Gump FE, Price JB, Kinney JM. Whole body and splanchnic
blood flow and oxygen consumption measurements in patients
with intraperitoneal infections. Ann Surg 1970; 171:321-28
18 SiegalJH, Cerra FB, Coleman B, Giovanni I, Shety CM, Border
JR. et al. Physiologic and metabolic correlations in human
sepsis. Surgery 1979; 86:163-93
19 Russel J, Ronco J, Lockhat D, Belzberg A, Keis M, Dodek P.
Oxy gen delivery and consumption and ventricular preload are
greater in survivors than in nonsurvivors ofthe adult respiratory
distress syndrome. Am Rev Respir Dis 1990; 141:659-65
20 Clowes CA, Vucinic M, Weidner M. Circulatory and metabolic
alterations associated with survival or death in peritonitis. Ann
Surg 1966; 163:866-8521 Parker MM, ShelhamerJH, Bacharach SL, Green MV, Natanson
C, Parrillo JE. Profound by reversible myocardial depression on
patients with septic shock. Ann Intern Med 1984; 100:483-9022 Ellrodt A, Riedinger M, Kimchi A, Berman D, Madduh J, Swan
HJ. Left ventricular performance in septic shock: reversible
segmental and global abnormalities. Am Heart J 1985; 110:402-09
23 Rackow EC, Kaufman BS, Falk JL, Astiz ME, Weil MH.
Hemodynamic response to fluid repletion in patients with shock:
evidence for early depression of cardiac performance. CiscShock 1987; 22:11-22
24 Wilson RF, Christensen C, Leblanc 12. Oxygen consumption
in critically ill surgical patients. Ann Surg 1972; 176:801-05
25 Beisel WR. Metabolic response to infection. Ann Rev Med1975; 26:9
26 Weil MH, Afifi A. Experimental and clinical studies in lactate
and pyruvate as indicators of the severity of acute circulatory
failure (shock). Circulation 1970; 41:989-1001
27 Groeneveld J, Bronsveld W, Thijs L. Hemodynamic determi-nants ofmortality in human septic shock. Surgery 1986; 99:140-
52
28 Gore J, Goldberg R, Spodick D, AlpertJ, DalenJ. A community-wide assessment of the use of pulmonary artery catheters inpatients with acute myocardial infarction. Chest 1987; 92:721-
27
29 Steingrub J, Celoria G, Vichers-Lahti M, Terns D, Bria W.Therapeutic impact of pulmonary artery catheterization in a
medical/surgical ICU. Chest 1991; 99:1451-55
30 Iberti T, Fischer E, Leibowitz A, Panacek E, Silverstein J,Albertson T. A multicenter study ofphysicians knowledge of the
pulmonary artery catheter. JAMA 1990; 264:2928-32
© 1992 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from
DOI 10.1378/chest.102.1.216 1992;102; 216-220Chest
J Tuchschmidt, J Fried, M Astiz and E Rackowshock.
Elevation of cardiac output and oxygen delivery improves outcome in septic
July 10, 2011This information is current as of
http://chestjournal.chestpubs.org/content/102/1/216Updated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/102/1/216#related-urlsThis article has been cited by 32 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlonline at: Information about reproducing this article in parts (figures, tables) or in its entirety can be foundPermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the "Services" link to
Citation Alerts
slide format. See any online figure for directions. articles can be downloaded for teaching purposes in PowerPointCHESTFigures that appear in Images in PowerPoint format
© 1992 American College of Chest Physicians by guest on July 10, 2011chestjournal.chestpubs.orgDownloaded from
Related Documents











