doi: 10.1136/hrt.2009.177014 2010 96: 289-297 Heart S Maréchaux, C Pinçon, M Poueymidanette, et al. regurgitation of mitral valve tenting in functional mitral determinant Doppler echocardiography is a key Elevated left atrial pressure estimated by http://heart.bmj.com/content/96/4/289.full.html Updated information and services can be found at: These include: References http://heart.bmj.com/content/96/4/289.full.html#ref-list-1 This article cites 38 articles, 17 of which can be accessed free at: service Email alerting box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the Notes http://heart.bmj.com/cgi/reprintform To order reprints of this article go to: http://heart.bmj.com/subscriptions go to: Heart To subscribe to group.bmj.com on March 6, 2010 - Published by heart.bmj.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

doi: 10.1136/hrt.2009.177014 2010 96: 289-297Heart
S Maréchaux, C Pinçon, M Poueymidanette, et al. regurgitationof mitral valve tenting in functional mitral
determinantDoppler echocardiography is a key Elevated left atrial pressure estimated by
http://heart.bmj.com/content/96/4/289.full.htmlUpdated information and services can be found at:
These include:
References http://heart.bmj.com/content/96/4/289.full.html#ref-list-1
This article cites 38 articles, 17 of which can be accessed free at:
serviceEmail alerting
box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://heart.bmj.com/cgi/reprintformTo order reprints of this article go to:
http://heart.bmj.com/subscriptions go to: HeartTo subscribe to
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from
Elevated left atrial pressure estimated by Dopplerechocardiography is a key determinant of mitral valvetenting in functional mitral regurgitation
S Marechaux,1,2 C Pincon,3 M Poueymidanette,1 M Verhaeghe,1 A Bellouin,1
P Asseman,1 T Le Tourneau,1,2 T H LeJemtel,4 P Pibarot,5 P V Ennezat1,2
ABSTRACTBackground Functional mitral regurgitation (FMR) mayoccur in patients with reduced or preserved leftventricular ejection fraction (LVEF) and has beenassociated with excess valvular tenting only in patientswith reduced LVEF. This study aimed at identifying thepredictors of FMR and to determine whether or not theyare different in patients with reduced versus preservedLVEF.Methods 190 consecutive patients free of congenital orprimary valvular disease had a comprehensiveechocardiographic assessment of LV remodelling andfunction, diastolic function and FMR severity.Results 112 patients had depressed LVEF (<50%) and78 had preserved LVEF. FMR was present in 30 patientswith preserved LVEF and in 65 with reduced LVEF. HigherE/Ea, E/A and larger mitral tenting were independentpredictors of FMR regardless of LVEF. The mitral tentingarea was an independent predictor of FMR severity inpatients with reduced or preserved LVEF (p¼ 0.04 andp¼ 0.0045) in addition to E/A (p¼ 0.0007), E/Ea(p¼ 0.004) in patients with reduced and preserved LVEF,respectively. Higher E/Ea was independently associatedwith larger mitral tenting in patients with reduced andpreserved LVEF. Mitral tenting area was linearly related toE/Ea (r¼ 0.30, p<0.0001) and E/A (r¼ 0.43, p<0.0001)and LA enlargement (r¼ 0.54, p<0.0001) after havingpaired 96 patients with and without FMR on indices of LVremodelling.Conclusions In both patients with preserved andreduced LVEF, mitral tenting that leads to FMR is mainlydetermined by both mitral tethering forcesdthat is,displacement of papillary muscles and by pushingforcesdthat is, increased left atrial pressure. This studyunderscores that LV preload is a key determinant of FMR.
Functional mitral regurgitation (FMR) occurscommonly in symptomatic patients with chronicheart failure as a consequence of left ventricular(LV) dysfunction despite the absence of significantstructural abnormalities of the leaflets andsubvalvular apparatus.1 2 FMR results froma complex interaction of several factors includingglobal and/or local LV remodelling resulting inpapillary muscle (PM) displacement, mitral annulardilation, LV systolic dysfunction anddyssynchrony.3e8 These alterations result in animbalance between leaflet tethering forces andclosing forces, which leads to mitral leafletsmiscoaptation.9
FMR is associated with worse symptomaticstatus and prognosis in patients with chronic heart
failure.10e14 The most commonly used pharmaco-logical or surgical treatments of this clinical entitygenerally yield suboptimal results.15 Hence, betterunderstanding of the mechanisms of FMR is crucialto identify potential therapeutic targets. We havelong been intrigued by the clinical observation thatFMR may be observed in patients with preservedleft ventricular ejection fraction (LVEF), thussuggesting that beyond global and local LV remod-elling, annular dilation and intra-LV dyssynchrony,other unidentified factors may be involved in thepathogenesis of FMR.The objectives of the present study were thus to
identify the independent predictors of FMR and todetermine whether or not these predictors differ inpatients with reduced versus preserved LVEF.
METHODSPatient populationWe retrospectively analysed the echocardiographicstudies of 190 consecutive patients who werereferred within a 3-month period to the LilleMedical University Centre for echocardiographicexamination. Exclusion criteria were as follows:any structural abnormality of mitral leaflets orsubvalvular apparatus including leaflet prolapse(even focal), redundant leaflets and significantannular calcific deposits, any other valvular disease(>trivial aortic regurgitation, aortic valve sclerosisor stenosis), prosthetic heart valve, incompleteechocardiographic examination or inadequateimaging quality, recent (<3 months) myocardialinfarction, arrhythmia, bradycardia related to atrio-ventricular or sinus blocks, cardiac pacemaker,constrictive pericarditis, hypertrophic, restrictive orinfiltrative cardiomyopathy and congenital heartdisease.
Echocardiographic measurementsLV systolic and diastolic functionMeasurements of LV volumes and ejection fractionwere performed as recommended by the AmericanSociety of Echocardiography.16 17 Wall motion scoreindex was semi-quantitatively assessed by a 17-segment model. LV systolic and diastolic sphericitywere calculated as the ratio of the major to theminor axis from the apical four-chamber view.Interventricular and intra-LV dyssynchrony wereevaluated as previously described.6
Diastolic functionPeak early filling mitral flow velocity (E); peakfilling velocity at atrial contraction (A velocity);
1Centre Hospitalier Regional etUniversitaire de Lille,Department of Ultrasound andPhysiology, Lille, France2EA 2693, Universite de Lille 2,Faculte de Medecine, Lille,France3Department of Biostatistics,Faculte de Pharmacie, Universitede Lille, Lille, France4Division of Cardiology, TulaneUniversity School of Medicine,New Orleans, Louisiana, USA5Institut Universitaire deCardiologie et de Pneumologiede Quebec/Quebec Heart andLung Institute, Laval University,Quebec, Canada G1V-4G5
Correspondence toDr Pierre Vladimir Ennezat,Intensive Care Unit, CardiologyHospital, Bd Pr J Leclercq,59037 Lille Cedex, France;[email protected]
Accepted 13 October 2009
Heart 2010;96:289e297. doi:10.1136/hrt.2009.177014 289
Valvular heart disease
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from

E/A ratio; and deceleration time of the peak E velocity (DTE)were measured using pulsed-wave Doppler. Early diastolic lateraland medial mitral annular velocities were measured by tissueDoppler echocardiography and averaged.18 Previous studies havedemonstrated the E/Ea ratio to be a reliable predictor of anelevated mean LV diastolic pressure and thereby of left atrial (LA)pressure even in the presence of MR.19 20 The LA area wasmeasured from the apical four-chamber view.
Mitral valve geometry and mitral regurgitationMitral annulusMeasurements of mitral annular diameter were made at end-diastole (d) and end-systole (s). The anteroposterior (AP)dimension was determined from the parasternal long-axis viewwith callipers at the junction between the posterior leaflet andleft atrial posterior wall and the anterior leaflet and the aorticvalve. In the apical four-chamber view, callipers were placed atthe junctions between the anterior leaflet and the atrial septumand the posterior leaflet and the left atrial lateral wall (4C). Themitral annular area (MAA) was calculated with the equationassuming an elliptical shape as follows: MAA ¼ p3 4C3AP/4.The mitral annular contractility was calculated as follows:(MAAd � MAAs) 3 100/MAAd.
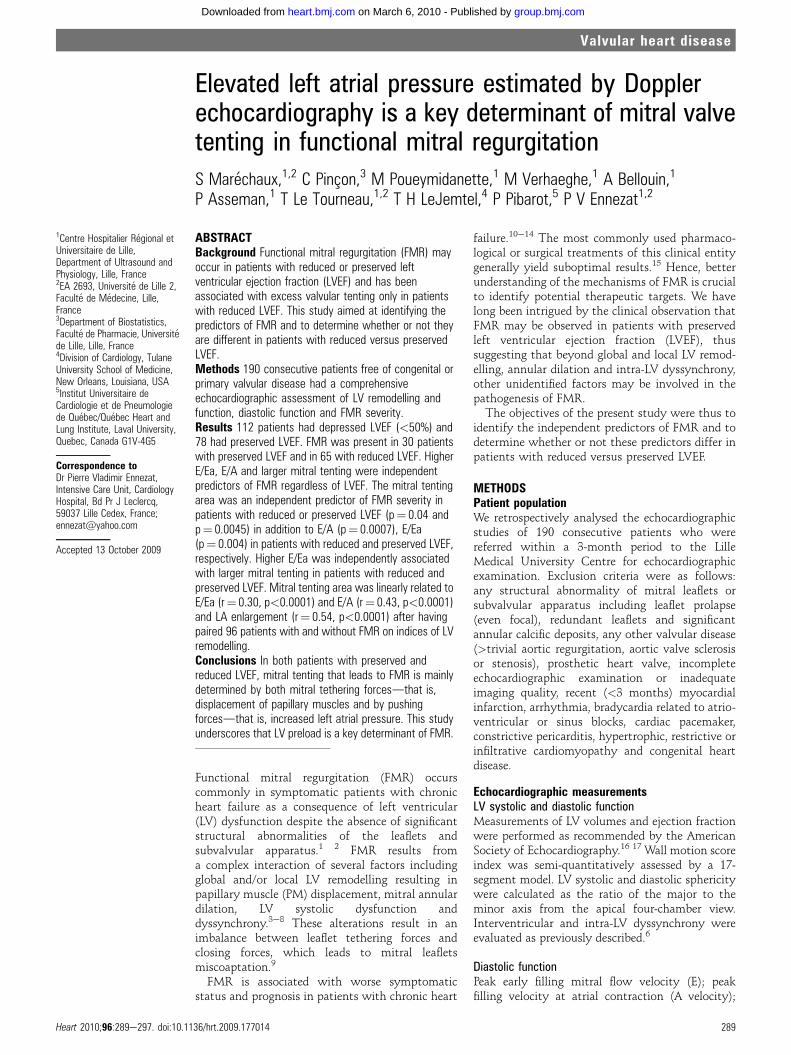
Position of the papillary musclesIn the two-apical chamber view, the distances from the mitralannulus to the anterolateral PM tips (APM � posterior annulusdistance and APM e anterior annulus distance) reflecting theanterior displacement of the anterolateral PM were measured atmid-systole (fig 1B).21 The distance between the posterior tip ofthe PM and the intervalvular fibrosa and the posterior annulus(PPM e intervalvular fibrosa distance and PPM e posteriorannulus, reflecting apical displacement of the PPM) wasmeasured from the apical long axis view (fig 1C). Separationbetween papillary muscles (PPM e APM distance) was measureddirectly from the parasternal short axis view (fig 1D).21
A mitral tenting area, that reflects the degree of restrictiveleaflets motion and moving of coaptation zone from the mitralannulus toward the apex, was measured by the area enclosedbetween the annular plane and the mitral leaflets from theparasternal long-axis view.4
Mitral regurgitationDegree of FMR was quantified by two methods: (1) the prox-imal flow convergence method,6 and (2) the volumetric methodestimating the FMR severity by subtracting the net forwardstroke volume from the total LV stroke volume. The results ofthese two methods were averaged to calculate the effectiveregurgitant orifice (ERO) area and the regurgitant volume (RV).
Statistical analysisData are presented as mean (SD) for continuous variables and asproportions for categorical variables. As different mechanismsmay contribute to FMR in patients with either preserved orreduced LVEF, an interaction term including the categoricalvariable LVEF $50% was systematically tested against eachoutcome. Analyses were carried out separately in patients withreduced or preserved LVEF when a significant interaction wasfound (p<0.10).
Mean values of echocardiographic variables for patientswithout FMR were compared with those of patients with FMReither with two-sided Student t tests for independent samplesin case of continuous variables or with c2 tests in case ofcategorical variables.
A logistic regression analysis was performed to identifyechocardiographic variables associated with the presence ofFMR. For each continuous variable, two models were built:a first model containing the variable alone and a second onecontaining the variable and its square. A variable was selected formultivariate analysis if the level of significance in one of themodels was <0.2. The log-linearity assumption was tested incomparing the models with an F-test for nested models, thisassumption being rejected for a test level of significance<0.05. Inthis case, the continuous variable was transformed into a dummyvariable, the cut-off value for dichotomisation being the valueminimising the Akaike’s information criterion.A forward stepwise multiple logistic regression was used to
identify independent predictors of FMR, the variables enteringthe model were considered significant with a p value <0.05.Goodness of fit of the multivariate model was assessed by usingthe Hosmer-Lemeshow test to measure the model’s calibrationand by computing the area under the ROC curve to measure itsdiscrimination. In the subset of patients with FMR, determi-nants of FMR severity as estimated by the ERO were studiedwith the use of a forward stepwise multiple linear regressionanalysis. The procedure to select the predictors and build themultivariate model was similar to that of the logistic regressiondetailed above. The variables entering the multivariate modelwere considered as significant if the p value was <0.05 anda tolerance measure >0.7 to ensure that multicolinearitybetween echocardiographic parameters do not affect the regres-sion. Goodness of fit of the multivariate model was assessed byresidual analysis, the hypothesis of homoscedasticity beingtested with the White’s test, and the hypothesis of normalitybeing checked with the normal probability plot of the residuals.Determinants of mitral tenting area were also investigated witha linear regression analysis, as explained above.To further examine the contribution of LA pressure to the
mitral tenting and FMR, we performed a 1:1 case matchcomparison. Patients with FMR were matched with patientswithout FMR according to LVEF (+/� 5%), EDV index (+/� 5ml/m2) and diastolic sphericity index (+/� 0.25). Mean values ofechocardiographic variables for patients with FMR werecompared with those of patients without MR with two-sidedStudent t tests for independent samples in this analysis. Statis-tical analysis was performed using the SAS system (SAS v8, SASInstitute) after approval by the CNIL (French computers andprivacy commission).
RESULTSCharacteristics of the populationThe study cohort consisted of 190 patients (127 men, 67%) witha mean age of 66 (15) years; 112 patients had a depressed LVEF(<50%) and 78 had a preserved LVEF. Fifty-three per cent ofpatients had hypertension, 21% had type 2 diabetes, and 58% hadischaemic heart disease. FMR was present in 30 patients (38%)with preserved LVEF and in 65 (58%) patients with reduced LVEF.The mitral ERO was slightly lower in patients with FMR andpreserved LVEF than in those with FMR and reduced LVEF (4 (3)mm2 vs 6 (7) mm2, p¼ 0.06). Patients with preserved LVEF andFMR were older ((73 (12) years vs 60 (19) years, p¼ 0.001), moreoften female (73% vs 44%, p¼ 0.01) and hypertensive (80% vs69%, p¼ 0.05) than patients with preserved LVEF and no FMR.
Determinants of the presence of FMRIndices of global LV function and remodelling of patients withand without FMR are presented in table 1. Both LVEF and
290 Heart 2010;96:289e297. doi:10.1136/hrt.2009.177014
Valvular heart disease
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from
systolic annular velocities were significantly (p#0.001) lower inpatients with FMR compared to patients without FMR. LVend-diastolic index and wall motion score index were higher inpatients with FMR (both p¼ 0.004). Both systolic and diastolicLV sphericity index were lower in patients with MR (bothp<0.0001), whereas intra-LV dyssynchrony was increased inpatients with FMR compared with those without MR (p¼ 0.02).
Indices of mitral valve deformation are shown in table 1.Systolic mitral tenting area was markedly increased in presenceof FMR (p<0.0001) whereas mitral annular contractility wasdepressed in presence of FMR (p¼ 0.04). PM separation andincreased apical, anterior and posterior displacement of the PMswere larger in patients with FMR (table 1).
Indices of elevated LA pressuresdthat is, E/A ratio, E/Ea ratioand LA area, were markedly higher in patients with FMRcompared to patients without FMR (all p<0.0001). No interac-tion was found between LVEF$50% and all other indices for theprediction of the presence of FMR, so that no further analyseswere carried out separately in patients with either preserved orreduced LVEF.
On multivariate analysis, higher E/A ratio, E/Ea ratio andincreased systolic mitral valvular tenting area emerged as inde-
pendent predictors of the presence of FMR (area under the ROCcurve: 0.91, table 1).
Determinants of FMR severitySeveral interactions (p<0.10) were found significant betweenLVEF $50% and other indices such as interventricular and intra-LV dyssynchrony, E/Ea ratio and lateral S wave for the predictionof the severity of FMR as evaluated by mitral ERO. Accordingly,further analyses were carried out separately in patients withpreserved and reduced LVEF.
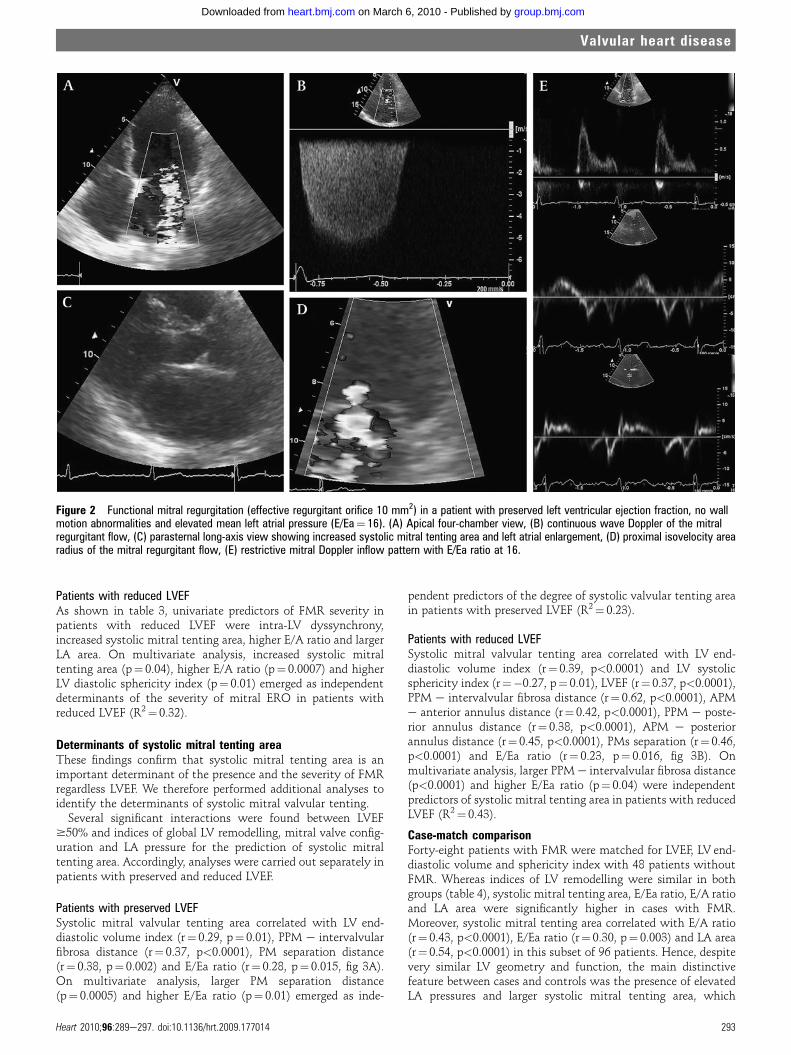
Patients with preserved LVEFAs shown in table 2, univariate predictors of mitral EROwere LVend diastolic volume index, lateral mitral annulus systolicvelocity, mitral tenting area and E/Ea ratio (table 2). On multi-variate analysis, higher E/Ea ratio (p¼ 0.004), larger mitraltenting area (p¼ 0.0045), and increased lateral mitral annulussystolic velocity (p¼ 0.014) were independently associated withFMR severity in patients with preserved LVEF (R2¼ 0.53).Figure 2 shows an echocardiogram obtained in a patient with
preserved LVEF and mild FMR. LA size is enlarged and LA pres-sure is increased as demonstrated by increased E/Ea.
Figure 1 Position of the papillary muscles (PM) by two-dimensional echocardiography in a patient with reduced left ventricular ejection fraction andfunctional mitral regurgitation (apical four-chamber view, A). APM posterior annulus is the distance from the anterolateral papillary muscle to theposterior mitral annulus and APM anterior annulus is the distance from the anterolateral papillary muscle to the anterior mitral annulus, both measured inthe apical two-chamber view (B). PPM posterior annulus is the distance from the posterior papillary muscle to the posterior mitral annulus and PPMintervalvular fibrosa is the distance from the posterior papillary muscle to the intervalvular fibrosa, both measured in the apical long-axis view (C). The PMseparation is the distance measured between the posterior papillary muscle and the anterior papillary muscle in the parasternal short-axis view (D).
Heart 2010;96:289e297. doi:10.1136/hrt.2009.177014 291
Valvular heart disease
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from
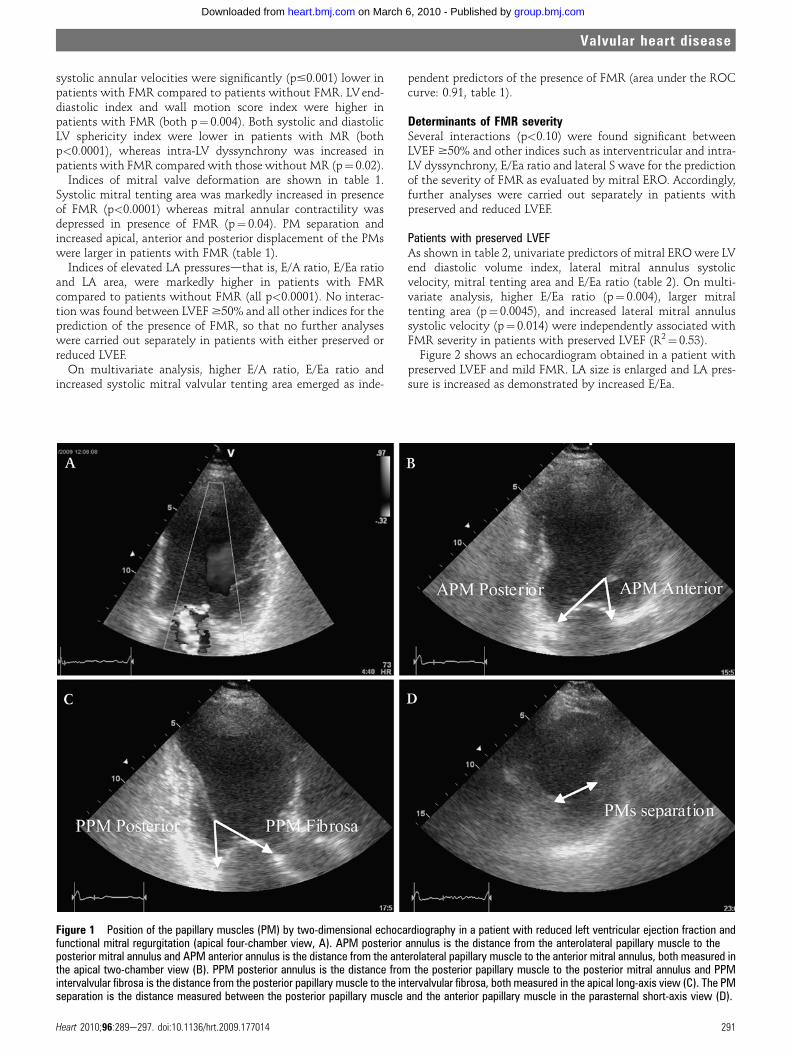
Table 1 Univariate and multivariate determinants of the presence of functional mitral regurgitation
Overall
Univariate analysis Multivariate analysis
WithoutMR With MR
Univariatep value OR (95% CI)
Multivariatep value
Global LV function and LV remodelling
LVEF (%) 43 (18) 48 (17) 38 (17) <0.0001
Wall motion score index 1.60 (0.50) 1.49 (0.48) 1.70 (0.50) 0.004
LV end diastolic volume index (ml/m2) 67 (33) 55 (23) 79 (37) <0.0001
Interventricular dyssynchrony (ms) 12 (17) 11 (16) 14 (17) 0.15
Intra-LV dyssynchrony (ms) 19 (30) 15 (28) 25 (32) 0.02
Lateral S-wave (cm/s) 6.40 (2.40) 6.98 (2.41) 5.84 (2.26) 0.0011
Septal S-wave (cm/s) 5.48 (1.97) 6.24 (1.95) 4.75 (1.71) <0.0001
LV diastolic sphericity index 1.85 (0.34) 1.96 (0.33) 1.74 (0.33) <0.0001
LV systolic sphericity index 2.10 (0.60) 2.31 (0.69) 1.91 (0.45) <0.0001
Mitral deformation and LV local remodelling
Mitral annular contractility (%) 21 (14) 24 (16) 18 (13) 0.037
Mitral tenting area (cm2) 2.74 (1.39) 2.09 (0.91) 3.40 (1.47) <0.0001 2.02 (1.35 to 3.03) 0.0006
APM anterior annulus (mm) 26.3 (5.4) 24.9 (4.2) 27.5 (5.9) 0.0015
APM posterior annulus (mm) 36.1 (6.8) 34.3 (6.0) 37.6 (7.0) 0.0018
PMs separation (mm) 27.2 (9.0) 24.3 (8.2) 29.9 (8.9) <0.0001
PPM intervalvular fibrosa (mm) 37.6 (8.0) 34.5 (6.9) 40.5 (7.9) <0.0001
PPM posterior annulus (mm) 27.9 (6.2) 26.8 (6.0) 28.9 (6.1) 0.02
Diastolic function and LV preload
E/A ratio 1.43 (1.13) 0.98 (0.46) 1.90 (1.41) <0.0001 2.5 (1.2 to 5.0) 0.0121
E-wave deceleration time (ms) 182 (69) 190 (58) 173 (78) 0.09
E/Ea ratio 13.3 (6.5) 9.4 (3.8) 17.2 (6.2) <0.0001 12.3 (5.3 to 28.8) <0.0001*
Left atrial area (cm2) 26.0 (8.1) 21.7 (6.2) 30.5 (7.4) <0.0001
*E/Ea ratio dichotomised as a dummy variable (E/Ea $12 and <12).APM, anterior papillary muscle; EF, ejection fraction; LV, left ventricle; PPM, posterior papillary muscle.
Table 2 Univariate and multivariate determinants of the severity of functional mitral regurgitation in thesubgroup of patients with preserved left ventricular ejection fraction and functional mitral regurgitation(n¼ 30)
B (SD) RUnivariatep value
Multivariatep value
Global LV function and LV remodelling
LVEF (%) 0.84
Wall motion score index 0.85
LV end diastolic volume index(ml/m2)
1.6 (1.2) 0.24 0.20
Interventricular dyssynchrony (ms) 0.73
Intraventricular dyssynchrony (ms) 0.96
Lateral S-wave ($6 cm/s) 0.4 (0.2) 0.33 0.08 0.014
Septal S-wave (cm/s) 0.79
LV diastolic sphericity 0.93
LV systolic sphericity 0.40
Mitral deformation and LV local remodelling
Mitral annular contractility($6.6%)
0.1 (0.1) 0.26 0.19 0.004
Mitral tenting area (cm2) 0.7 (0.6) 0.24 0.19 0.004
APM anterior annulus (mm) 0.49
APM posterior annulus (mm) 0.88
PMs separation (mm) 0.73
PPM intervalvular fibrosa (mm) 0.70
PPM posterior annulus (mm) 0.86
Diastolic function and LV preload
E/A ratio 0.44
E-wave deceleration time (ms) �0.01 (0.006) �0.32 0.08
E/Ea ratio 0.1 (0.1) 0.30 0.11 0.004
Left atrial area 0.89
APM, anterior papillary muscle; EF, ejection fraction; LV, left ventricle; PPM, posterior papillary muscle.
292 Heart 2010;96:289e297. doi:10.1136/hrt.2009.177014
Valvular heart disease
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from
Patients with reduced LVEFAs shown in table 3, univariate predictors of FMR severity inpatients with reduced LVEF were intra-LV dyssynchrony,increased systolic mitral tenting area, higher E/A ratio and largerLA area. On multivariate analysis, increased systolic mitraltenting area (p¼ 0.04), higher E/A ratio (p¼ 0.0007) and higherLV diastolic sphericity index (p¼ 0.01) emerged as independentdeterminants of the severity of mitral ERO in patients withreduced LVEF (R2¼ 0.32).
Determinants of systolic mitral tenting areaThese findings confirm that systolic mitral tenting area is animportant determinant of the presence and the severity of FMRregardless LVEF. We therefore performed additional analyses toidentify the determinants of systolic mitral valvular tenting.
Several significant interactions were found between LVEF$50% and indices of global LV remodelling, mitral valve config-uration and LA pressure for the prediction of systolic mitraltenting area. Accordingly, analyses were carried out separately inpatients with preserved and reduced LVEF.
Patients with preserved LVEFSystolic mitral valvular tenting area correlated with LV end-diastolic volume index (r¼ 0.29, p¼ 0.01), PPM e intervalvularfibrosa distance (r¼ 0.37, p<0.0001), PM separation distance(r¼ 0.38, p¼ 0.002) and E/Ea ratio (r¼ 0.28, p¼ 0.015, fig 3A).On multivariate analysis, larger PM separation distance(p¼ 0.0005) and higher E/Ea ratio (p¼ 0.01) emerged as inde-
pendent predictors of the degree of systolic valvular tenting areain patients with preserved LVEF (R2¼ 0.23).
Patients with reduced LVEFSystolic mitral valvular tenting area correlated with LV end-diastolic volume index (r¼ 0.39, p<0.0001) and LV systolicsphericity index (r¼�0.27, p¼ 0.01), LVEF (r¼ 0.37, p<0.0001),PPM e intervalvular fibrosa distance (r¼ 0.62, p<0.0001), APMe anterior annulus distance (r¼ 0.42, p<0.0001), PPM e poste-rior annulus distance (r¼ 0.38, p<0.0001), APM e posteriorannulus distance (r¼ 0.45, p<0.0001), PMs separation (r¼ 0.46,p<0.0001) and E/Ea ratio (r¼ 0.23, p¼ 0.016, fig 3B). Onmultivariate analysis, larger PPM e intervalvular fibrosa distance(p<0.0001) and higher E/Ea ratio (p¼ 0.04) were independentpredictors of systolic mitral tenting area in patients with reducedLVEF (R2¼ 0.43).
Case-match comparisonForty-eight patients with FMR were matched for LVEF, LV end-diastolic volume and sphericity index with 48 patients withoutFMR. Whereas indices of LV remodelling were similar in bothgroups (table 4), systolic mitral tenting area, E/Ea ratio, E/A ratioand LA area were significantly higher in cases with FMR.Moreover, systolic mitral tenting area correlated with E/A ratio(r¼ 0.43, p<0.0001), E/Ea ratio (r¼ 0.30, p¼ 0.003) and LA area(r¼ 0.54, p<0.0001) in this subset of 96 patients. Hence, despitevery similar LV geometry and function, the main distinctivefeature between cases and controls was the presence of elevatedLA pressures and larger systolic mitral tenting area, which
Figure 2 Functional mitral regurgitation (effective regurgitant orifice 10 mm2) in a patient with preserved left ventricular ejection fraction, no wallmotion abnormalities and elevated mean left atrial pressure (E/Ea¼ 16). (A) Apical four-chamber view, (B) continuous wave Doppler of the mitralregurgitant flow, (C) parasternal long-axis view showing increased systolic mitral tenting area and left atrial enlargement, (D) proximal isovelocity arearadius of the mitral regurgitant flow, (E) restrictive mitral Doppler inflow pattern with E/Ea ratio at 16.
Heart 2010;96:289e297. doi:10.1136/hrt.2009.177014 293
Valvular heart disease
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from

supports the concept that pushing forces generated by increasedLA pressure, may contribute to the tenting of mitral valve andthereby to the occurrence of FMR.
DISCUSSIONThe main findings of this study are: (1) FMR may be found inpatients with preserved LVEF regardless of the presence ofsegmental wall motion abnormalities, (2) non-invasively esti-mated LV filling pressure and thereby LA pressure are majordeterminants of FMR regardless of LVEF, (3) systolic mitralvalvular tenting, a well-established determinant of the presenceand severity of FMR, is directly and independently related to localLV remodellingdthat is, tethering forces, but also to increased LApressure and LA enlargementdthat is, pushing forces (fig 4).
Functional MR commonly occurs secondary to LV dysfunc-tion despite structurally normal mitral valve leaflets and chordae
tendinae.1 Although FMR is often clinically silent,22 severalstudies have demonstrated that it is a powerful independent riskfactor for poor outcome in the setting of heart failure or postmyocardial infarction.10 12 23 Yiu and co-workers were the first toreport the important contribution of global or local LV remod-elling in the pathogenesis of FMR in patients with reduced LVEF.4
In agreement with the findings of Yiu et al and of other investi-gators,24 25 a larger systolic mitral tenting area was found to be anindependent predictor of the presence and severity of MR inpatients with reduced LVEF in the present study. We also foundan independent relation between systolic mitral tenting area andindices of PM misalignment. Very recently, Park et al elegantlydemonstrated that LA enlargement and diastolic dysfunctionassessed by the mitral Doppler inflow pattern contribute to FMRin patients with dilated cardiomyopathy.26 Our study confirmsand extends these findings. Indeed, the finding that larger mitral
Table 3 Univariate and multivariate determinants of the severity of functional mitral regurgitation in thesubsample of patients with reduced left ventricular ejection fraction and functional mitral regurgitation(n¼ 65)
B (SD) RUnivariatep value
Multivariatep value
Global LV function and LV remodelling
LVEF (%) �0.16 (0.08) �0.24 0.06
Wall motion score index 0.55
LV end diastolic volume index (ml/m2) 0.05 (0.03) 0.25 0.05
Interventricular dyssynchrony (ms) 0.09 (0.06) 0.19 0.12
Intraventricular dyssynchrony (ms) 0.05 (0.03) 0.25 0.04
Lateral S-wave (cm/s) 0.43
Septal S-wave (cm/s) 0.26
LV diastolic sphericity index $1.47 3.0 (2.1) 0.18 0.15 0.01
LV systolic sphericity index 0.48
Mitral deformation and LV localremodelling
Mitral annular contractility (%) �0.22 (0.12) �0.28 0.06
Mitral tenting area (cm2) 1.5 (0.6) 0.31 0.01 0.04
APM anterior annulus (mm) 0.81
APM posterior annulus (mm) 0.21 (0.14) 0.19 0.16
PMs separation (mm) 0.21 (0.13) 0.20 0.12
PPM intervalvular fibrosa (mm) 0.19 (0.13) 0.19 0.14
PPM posterior annulus (mm) 0.21 (0.15) 0.18 0.17
Diastolic function and LV preload
E/A ratio 7.4 (1.9) 0.44 0.0005 0.0007*
E-wave deceleration time (ms) �0.02 (0.01) �0.20 0.11
E/Ea ratio 0.65
Left atrial area (cm2) 0.28 (0.12) 0.29 0.019
*E/A ratio dichotomised as a dummy variable (E/A $2.9 and <2.9).APM, anterior papillary muscle; EF, ejection fraction; LV, left ventricle; PPM, posterior papillary muscle.
Figure 3 Relation between mitral flow E velocity to mitral annulus diastolic Ea velocity and mitral tenting area in patients with either preserved leftventricular ejection fraction (A) or reduced left ventricular ejection fraction (B). The line is the linear regression line.
294 Heart 2010;96:289e297. doi:10.1136/hrt.2009.177014
Valvular heart disease
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from

tenting area and elevated LA pressure determine the presence ofFMR may explain at least partially why some patients withreduced LVEF may exhibit an increased mitral tenting areaassociated with increased local LV remodelling but no MR.
Our work builds on previous studies by also assessing FMR inthe context of preserved LVEF. Increased systolic mitral tentingarea and indices of LA pressure were also identified as powerfulindependent predictors of the presence and the severity of MR inthese patients with preserved LVEF. Finally the combination of(1) elevated mean LA pressure that decreases the net atrioven-tricular pressure gradient and thereby mitral closing forces and(2) increased local LV remodelling that increases mitral valvetethering appears sufficient to trigger FMR in patients regardlessof LVEF. In addition, the case-match approach underscores thatof two patients having similar LV local and global remodelling,the one with FMR will exhibit larger LA size and higher LApressure than the one without FMR, and that LA enlargementmay be viewed as a chronic harbinger of elevated LV preload.
Intriguingly, the E/A ratio was found to be a strongerpredictor of FMR severity than the E/Ea ratio in patients withreduced LVEF, whereas the opposite was found in the subset ofpatients with preserved LV function. Such a finding is notunexpected, as the E/A ratio may be more reliable to predict LApressure than the E/Ea ratio in patients with advanced systolicheart failure, large LV volumes and impaired cardiac indices.27
Of note in our series, patients with FMR and preserved LVEFwere older and more frequently hypertensive women, asfrequently observed in patients with heart failure and preservedLVEF (HFpEF). Increased LA pressure as evidenced non-inva-sively by elevated E/Ea is commonly encountered in patientswith heart failure and preserved LVEF.28 Of note intermittentincrease in FMR during dynamic exercise was found to be asso-ciated with an acute increase in LV preload as assessed by E/Earatio in patients with HFpEF.29 One could thus speculate thatincreased LA pressure contributes to the development of FMRand therefore to the worsening of heart failure in these patients.
The results of the present study may have important clinicalimplications. Indeed, the surgical correction of FMR still remains
a source of debate in patients with LV systolic dysfunction. Inthe series reported by McGee et al, one-third of patients withischaemic heart disease and FMR had recurrent 3+ or 4+ MR 6months after mitral annuloplasty.30 Several studies have shown
Table 4 Case-match comparisons of patients with and without functional mitral regurgitation
Without MR(n[ 48)
With MR(n[ 48) p Value
LVEF (%) 42 (15) 42 (15) By design
Wall motion score index 1.64 (0.46) 1.64 (0.46) 0.96
LV end diastolic volume index (ml/m2) 62 (24) 62 (23) By design
Interventricular dyssynchrony (ms) 14 (21) 9 (10) 0.15
Intraventricular dyssynchrony (ms) 22 (36) 21 (31) 0.89
Lateral S-wave (cm/s) 6 (2) 6 (2) 0.87
Septal S-wave (cm/s) 6 (2) 5 (2) 0.06
LV diastolic sphericity index 1.86 (0.31) 1.90 (0.31) By design
LV systolic sphericity index 2.12 (0.67) 2.12 (0.44) 0.99
Mitral annular contractility (%) 21 (13) 20 (11) 0.83
Mitral tenting area (cm2) 2.1 (0.9) 3.2 (1.4) <0.0001APM anterior annulus (mm) 26 (4) 27 (5) 0.60
APM posterior annulus (mm) 36 (6) 36 (7) 0.68
PMs separation (mm) 27 (8) 27 (8) 0.98
PPM intervalvularfibrosa (mm) 36 (7) 38 (6) 0.27
PPM posterior annulus (mm) 29 (6) 28 (5) 0.39
E/A ratio 0.98 (0.51) 1.61 (1.05) 0.0009
E-wave deceleration time (ms) 186 (55) 176 (74) 0.46
E/Ea ratio 9 (3) 16 (6) <0.0001Left atrial area (cm2) 23 (6) 29 (7) <0.0001
LV, left ventricle; EF, ejection fraction; APM, anterior papillary muscle; PPM, posterior papillary muscle.
Figure 4 Apical long axis view illustrating that mitral tenting area mayresult from tethering forces (local LV remodelling, arrow 1) and pushingforces (increased LA pressure and size, arrows 2).
Heart 2010;96:289e297. doi:10.1136/hrt.2009.177014 295
Valvular heart disease
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from

that this procedure fails to adequately reduce mitral valve teth-ering in a substantial proportion of the patients with FMR31e33
but may not consistently result in functional capacity improve-ment.34 In light of the finding that LA pressure is a major inde-pendent determinant of functional MR, treatment of FMRshould be primarily focused on the optimisation of medicaltreatment including diuretics, nitrates and inhibitors of therenin-angiotensin system in order to reduce LA pressure andafterload. To this effect, previous studies have demonstratedthat these medications may successfully reduce the degree ofFMR.35 36 Surgery may be envisioned in the challenging subset ofpatients in whom an intensive medical therapy has failed toachieve significant reduction in MR severity.
Limitations of the studyOne limitation is the retrospective nature of this study, whichlimits our ability to determine the clinical correlates, prevalenceand incidence of FMR in the subsets of patients with reduced orpreserved LVEF. Prospective studies are needed to address theseissues.
There are conflicting data on the accuracy of E/Ea as a surro-gate of LV filling pressure in patients with FMR. Some investi-gators reported that E/Ea ratio accurately predicts LV fillingpressure in patients with FMR,19 20 whereas others found a poorcorrelation in patients with severe MR of various aetiologies.37 Inthis regard, the ratio of isovolumetric relaxation time to the timeinterval between the onset of early diastolic mitral inflowvelocity (E) and annular early diastolic velocity (Ea) by tissueDoppler imaging (IVRT/TE e Ea) better predicts LV filling pres-sure than the E/Ea ratio, especially in patients with MR andpreserved LVEF.38 The utilisation of this ratio might thus haveyielded an even stronger association between estimated LApressure, mitral valve tenting and FMR. This ratio was, however,not measured in the present study. In addition, invasivemeasurement of pulmonary capillary wedge pressure was notavailable.
Another limitation is the cross-sectional design of the study,which limits the conclusion with regard to causality. FMR maylead to an increase in LA pressure but, on the other hand, assuggested by the present findings, elevated LA pressure may alsocontribute to the development and/or worsening of FMR,thereby feeding a vicious cycle where FMR begets FMR. Furtherlongitudinal studies will be necessary to address this issue.Nonetheless, the findings of this study, and especially those ofthe case-match comparison give support to the concept thatincreased LA pressure is a major determinant of FMR.
ConclusionThe combination of increased tethering forces (mainly depen-dent on local LV remodelling) and pushing forces (mainlydependent on increased LV preload) both worsen systolic mitralvalve tenting and thereby predispose to the occurrence of FMRnot only in patients with reduced LVEF but also in those withpreserved LVEF. Hence, these findings suggest that elevated LApressure is a key determinant of FMR. These results may haveimportant implications with regard to the evaluation andtreatment of this complex condition.
Funding PP received honoraria, consulting fees, and/or research grants from St JudeMedical, Edwards Life Sci, Medtronic and Sorin Medical.
Competing interests None.
PP holds the Canada Research Chair in Valvular Heart Diseases, Canadian Institutes ofHealth Research (Ottawa, Canada).
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1. Ennezat PV, Marechaux S, Asseman P, et al. Functional mitral regurgitation and
chronic heart failure. Minerva Cardioangiol 2006;54:725e33.2. Levine RA, Hung J, Otsuji Y, et al. Mechanistic insights into functional mitral
regurgitation. Curr Cardiol Rep 2002;4:125e9.3. Boltwood CM, Tei C, Wong M, et al. Quantitative echocardiography of the mitral
complex in dilated cardiomyopathy: the mechanism of functional mitral regurgitation.Circulation 1983;68:498e508.
4. Yiu SF, Enriquez-Sarano M, Tribouilloy C, et al. Determinants of the degree offunctional mitral regurgitation in patients with systolic left ventricular dysfunction:a quantitative clinical study. Circulation 2000;102:1400e6.
5. Agricola E, Oppizzi M, Galderisi M, et al. Role of regional mechanical dyssynchrony asa determinant of functional mitral regurgitation in patients with left ventricular systolicdysfunction. Heart 2006;92:1390e5.
6. Ennezat P, Marechaux S, Le Tourneau T, et al. Myocardial asynchronism isa determinant of changes in functional mitral regurgitation severity during dynamicexercise in patients with chronic heart failure due to severe left ventricular systolicdysfunction. Eur Heart J 2006;27:679e83.
7. Marechaux S, Pincon C, Gal B, et al. Functional mitral regurgitation at rest determinesthe acute hemodynamic response to cardiac resynchronization therapy during exercise:an acute exercise echocardiographic study. J Am Soc Echocardiogr 2009;22:464e71.
8. Ennezat PV, Gal B, Kouakam C, et al. Cardiac resynchronisation therapy reducesfunctional mitral regurgitation during dynamic exercise in patients with chronic heartfailure: an acute echocardiographic study. Heart 2006;92:1091e5.
9. He S, Fontaine AA, Schwammenthal E, et al. Integrated mechanism for functionalmitral regurgitation: leaflet restriction versus coapting force: in vitro studies.Circulation 1997;96:1826e34.
10. Grigioni F, Enriquez-Sarano M, Zehr K, et al. Ischemic mitral regurgitation: long-termoutcome and prognostic implications with quantitative Doppler assessment.Circulation 2001;103:1759e64.
11. Enriquez-Sarano M, Rossi A, Seward J. Determinants of pulmonary hypertension inleft ventricular dysfunction. J Am Coll Cardiol 1997;29:153e9.
12. Ennezat PV,Marechaux S, Huerre C, et al. Exercise does not enhance the prognosticvalue of Doppler echocardiography in patients with left ventricular systolic dysfunctionand functional mitral regurgitation at rest. Am Heart J 2008;155:752e7.
13. Patel J, Borgeson D, Barnes M, et al. Mitral regurgitation in patients with advancedsystolic heart failure. J Card Fail 2004;10:285e91.
14. Ennezat PV, Bellouin A, Marechaux S, et al. Pivotal role of bedside Dopplerechocardiography in the assessment of patients with acute heart failure and mitralregurgitation. Cardiology 2009;113:249e59.
15. Magne J, Senechal M, Dumesnil JG, et al. Ischemic mitral regurgitation: a complexmultifaceted disease. Cardiology 2009;112:244e59.
16. Schiller NB, Shah PM, Crawford M, et al. Recommendations for quantitation of theleft ventricle by two-dimensional echocardiography. American Society ofEchocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr 1989;2:358e67.
17. Schiller NB. Two-dimensional echocardiographic determination of left ventricular volume,systolic function, and mass. Summary and discussion of the 1989 recommendations of theAmerican Society of Echocardiography. Circulation 1991;84:I280e7.
18. Dokainish H, Zoghbi WA, Lakkis NM, et al. Optimal noninvasive assessment of leftventricular filling pressures: a comparison of tissue Doppler echocardiography and B-type natriuretic peptide in patients with pulmonary artery catheters. Circulation2004;109:2432e9.
19. Agricola E, Galderisi M, Oppizzi M, et al. Doppler tissue imaging: a reliable method forestimation of left ventricular filling pressure in patients with mitral regurgitation. AmHeart J 2005;150:610e15.
20. Bruch C, Stypmann J, Gradaus R, et al. Usefulness of tissue Doppler imaging forestimation of filling pressures in patients with primary or secondary pure mitralregurgitation. Am J Cardiol 2004;93:324e8.
21. Nordblom P, Bech-Hanssen O. Reference values describing the normal mitral valveand the position of the papillary muscles. Echocardiography 2007;24:665e72.
22. Desjardins VA, Enriquez-Sarano M, Tajik AJ, et al. Intensity of murmurs correlateswith severity of valvular regurgitation. Am J Med 1996;100:149e56.
23. Ennezat PV, Darchis J, Lamblin N, et al. Left ventricular remodeling is associated withthe severity of mitral regurgitation after inaugural anterior myocardialinfarctiondoptimal timing for echocardiographic imaging. Am Heart J2008;155:959e65.
24. Otsuji Y, Handschumacher MD, Schwammenthal E, et al. Insights from three-dimensional echocardiography into the mechanism of functional mitral regurgitation:direct in vivo demonstration of altered leaflet tethering geometry. Circulation1997;96:1999e2008.
25. Gorman RC, McCaughan JS, Ratcliffe MB, et al. Pathogenesis of acute ischemicmitral regurgitation in three dimensions. J Thorac Cardiovasc Surg 1995;109:684e93.
26. Park SM, Park SW, Casaclang-Verzosa G, et al. Diastolic dysfunction and left atrialenlargement as contributing factors to functional mitral regurgitation in dilatedcardiomyopathy: data from the Acorn trial. Am Heart J 2009;157:762, e763e2, e710.
27. Mullens W, Borowski AG, Curtin RJ, et al. Tissue Doppler imaging in the estimation ofintracardiac filling pressure in decompensated patients with advanced systolic heartfailure. Circulation 2009;119:62e70.
28. Oh JK, Hatle L, Tajik AJ, et al. Diastolic heart failure can be diagnosed bycomprehensive two-dimensional and Doppler echocardiography. J Am Coll Cardiol2006;47:500e6.
296 Heart 2010;96:289e297. doi:10.1136/hrt.2009.177014
Valvular heart disease
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from

29. Ennezat PV, Lefetz Y, Marechaux S, et al. Left ventricular abnormal response duringdynamic exercise in patients with heart failure and preserved left ventricular ejectionfraction at rest. J Card Fail 2008;14:475e80.
30. McGee EC, Gillinov AM, Blackstone EH, et al. Recurrent mitral regurgitation afterannuloplasty for functional ischemic mitral regurgitation. J Thorac Cardiovasc Surg2004;128:916e24.
31. Zhu F, Otsuji Y, Yotsumoto G, et al. Mechanism of persistent ischemic mitralregurgitation after annuloplasty: importance of augmented posterior mitral leaflettethering. Circulation 2005;112:I396e401.
32. Kuwahara E, Otsuji Y, Iguro Y, et al. Mechanism of recurrent/persistent ischemic/functional mitral regurgitation in the chronic phase after surgical annuloplasty:importance of augmented posterior leaflet tethering. Circulation 2006;114:I529e34.
33. Magne J, Pibarot P, Dagenais F, et al. Preoperative posterior leaflet angle accuratelypredicts outcome after restrictive mitral valve annuloplasty for ischemic mitralregurgitation. Circulation 2007;115:782e91.
34. Magne J, Senechal M, Mathieu P, et al. Restrictive annuloplasty for ischemic mitralregurgitation may induce functional mitral stenosis. J Am Coll Cardiol2008;51:1692e701.
35. Keren G, Bier A, LeJemtel TH. Improvement in forward cardiac output withouta change in ejection fraction during nitroglycerin therapy in patients with functionalmitral regurgitation. Can J Cardiol 1986;2:206e11.
36. Stevenson LW, Bellil D, Grover-McKay M, et al. Effects of afterload reduction(diuretics and vasodilators) on left ventricular volume and mitral regurgitation in severecongestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy.Am J Cardiol 1987;60:654e8.
37. Olson JJ, Costa SP, Young CE, et al. Early mitral filling/diastolic mitral annular velocityratio is not a reliable predictor of left ventricular filling pressure in the setting of severemitral regurgitation. J Am Soc Echocardiogr 2006;19:83e7.
38. Diwan A, McCulloch M, Lawrie GM, et al. Doppler estimation of left ventricular fillingpressures in patients with mitral valve disease. Circulation 2005;111:3281e9.
Heart 2010;96:289e297. doi:10.1136/hrt.2009.177014 297
Valvular heart disease
group.bmj.com on March 6, 2010 - Published by heart.bmj.comDownloaded from
Related Documents