•salts or minerals in body fluids •contain electrically charged particles called ions •principal source of osmotic forces which control volume or location of fluid Cations- positively charged; Na, K, Ca, Mg Anions- negatively charged; CL, HCO3, PO4 ELECTROLYTES Major electrolytes in ICF Major electrolytes in ECF

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 1/90
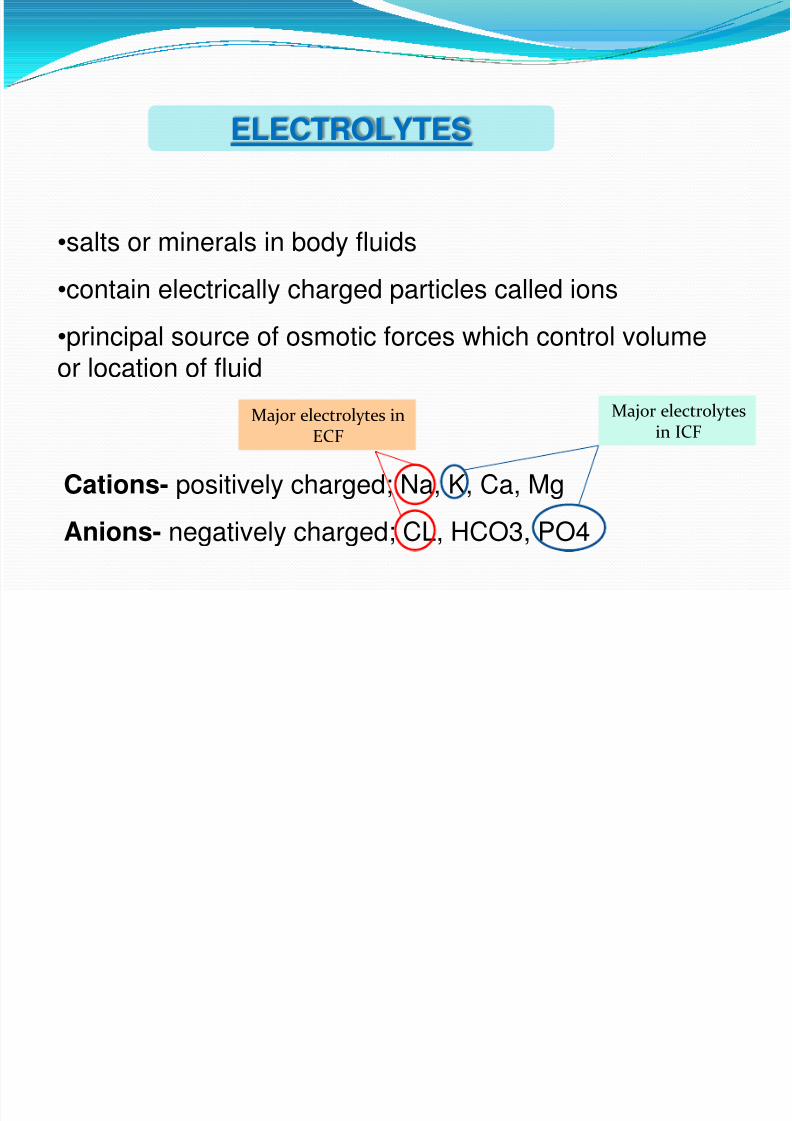
•salts or minerals in body fluids
•contain electrically charged particles called ions
•principal source of osmotic forces which control volumeor location of fluid
Cations- positively charged; Na, K, Ca, Mg
Anions- negatively charged; CL, HCO3, PO4
ELECTROLYTES
Major electrolytesin ICF
Major electrolytes inECF

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 2/90
IONS An atom or a group of atoms that has an electric
charge. Positive ions, or cations, are formed by the lossof electrons; negative ions, or anions, are formed by the gain of electrons.
The American Heritage® Science Dictionary
Copyright © 2002. Published by Houghton Mifflin

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 3/90

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 4/90
Major extracellular
electrolytes Sodium
Chloride
Calcium
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 5/90
Major intracellular
electrolytes Potassium
phosphate
magnesium
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 6/90
ELECTROLYTES Na+: most abundant electrolyte in the body
K+: essential for normal membrane excitability for nerve impulse
Cl-: regulates osmotic pressure and assists in regulating acid-basebalance
Ca+: usually combined with phosphorus to form the mineral salts of bones and teeth, promotes nerve impulse and musclecontraction/relaxation
Mg+: plays role in carbohydrate and protein metabolism, storage anduse of intracellular energy and neural transmission. Important in thefunctioning of the heart, nerves, and muscles
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 7/90
Sodium Regulates ECF volume and dist.
Maintains blood volume
Transmits nerve impulses and contracting muscles

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 8/90
Chloride Major ECF anion
HCl production
Regulates acid base balance Buffer in O2- CO2 exchange in RBC
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 9/90
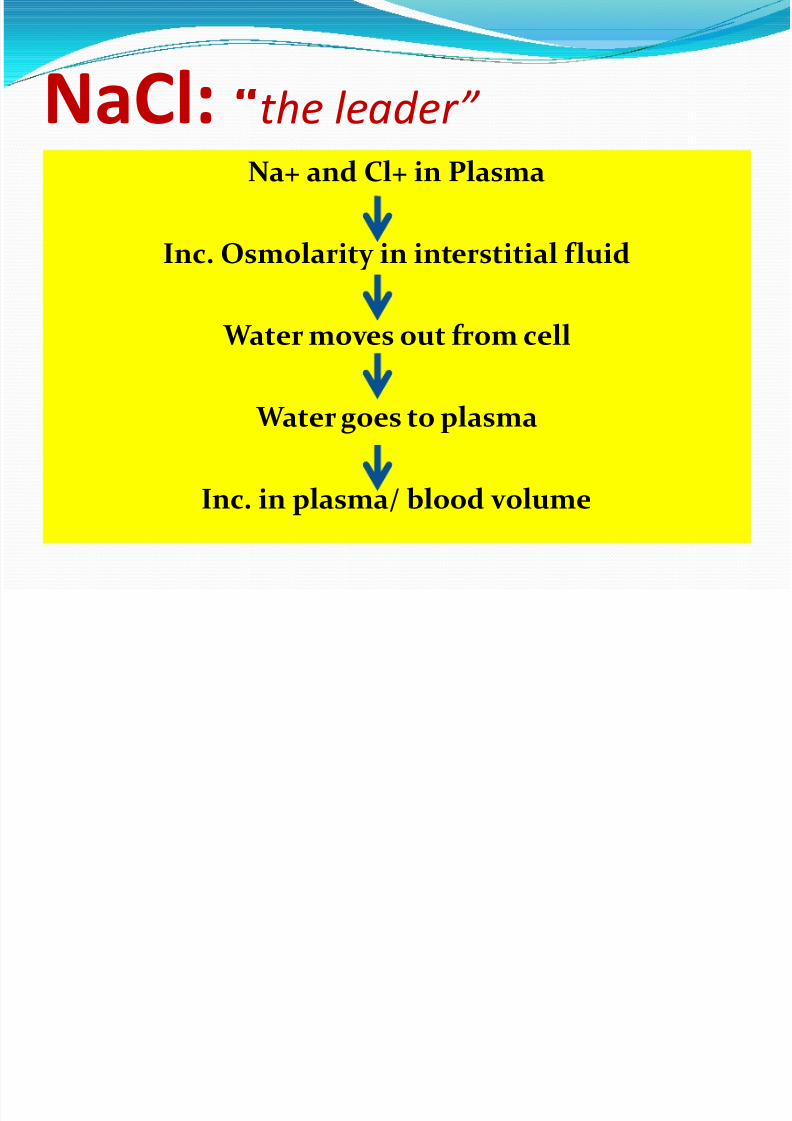
NaCl: “the leader” Na+ and Cl+ in Plasma
Inc. Osmolarity in interstitial fluid
Water moves out from cell
Water goes to plasma
Inc. in plasma/ blood volume

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 10/90
Calcium Muscle contraction and relaxation
Calcitriol, parathyroid hormone
Calcitonin
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 11/90
CalcitoninBone:
suppresses resorption of bone by inhibiting the
activity of osteoclasts, a cell type that "digests" bonematrix, releasing calcium and phosphorus into blood.
Kidney:
Calcium and phosphorus are prevented from being
lost in urine by reabsorption in the kidney tubules.Calcitonin inhibits tubular reabsorption of these twoions, leading to increased rates of their loss in urine

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 12/90
Phosphate Major ICF anion
Formation of bones and teeth (reciprocal rel. w/ Ca)
Metabolism

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 13/90
Calcitiol, Parathyroid hormone, Calcitonin
Dec. Ca in blood/ Inc. PO4
Release of Parathyroid hormone and calcitriol
Release of Ca from bones to ECF/ dec. absorp. Of PO4Inc. absorption of Ca in Intestines/ Excretion of PO4
Inc. Ca plasma level/ dec. in PO4
Calcitonin
Inc. deposition of Ca in Bones
Dec. Ca plasma level / Inc. PO4

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 14/90
Potassium Major ICF cation
Maintains ICF balance
Skeletal, cardiac, smooth muscle activity Regulates acid- base balance

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 15/90
Potassium RegulationICF ECF
Insulin AldosteroneTissue damage and acidosis
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 16/90
Mg Production of ATP
CHON and DNA synthesis
Nerve impulses and cardiac function regulation Intestinal absorption is increased w/ Vit D and PTH

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 17/90
MAJOR ELECTROLYTE IMBALANCES
Hyponatremia (sodium deficit < 130mEq/L)
Hypernatremia (sodium excess >145mEq/L)
Hypokalemia (potassium deficit <3.5mEq/L)
Hyperkalemia (potassium excess >5.1mEq/L)
Chloride imbalance (<98mEq/L or >107mEq/L)
Magnesium imbalance (<1.5mEq/L or >2.5mEq/L)

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 18/90
HypoNatremia Sodium deficiency
Serum level below 135 mEq/L (N: 135-145)
Results from excessive sodium loss or excessive watergain
Causes
Fluid loss Adrenal insufficiency
SIADH
Excessive water gain with deficient Na fluids

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 19/90
HypoNatremia S/s
Anorexia, N/V
Muscle cramps Altered LOC (lethargy, disorientation, Headache,
confusion, convulsion)
Labs
Serum Na less than 135 mEq/L Low urine Na & specific gravity – if cause is Na loss
High if the cause is SIADH
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 20/90
Nursing Management Maintain Fluid Balance
Monitor I & O
Weigh daily
Assess for s/s of fluid volume excess Administer Na supplements orally/NGT/parenterally
Infuse hypotonic solutions cautiously
Prevent injury
Assess neurologic (LOC, muscle twitching, seizures) and GIstatus (anorexia, NV, abdominal cramping)
Maintain seizure precautions
Monitor serum Na levels
Maintain water restriction if cause is fluid volume excess

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 21/90
Hypernatremia Sodium excess
Above serum Na level of 145 mEq/L
Causes: Water loss (diarrhea, fever, hyperventilation, Diabetes
insipidus)
Inadequate water replacement (elderly, cognitively
impaired, coma pts) Inability to swallow
Excessive intake of Na in any routes

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 22/90
HyperNatremia S/s
Thirst
Tented skin turgor
Edematous dry skin and sticky mucous membrane Elevated body temperature
Lethargy and restlessness
Peripheral and pulmonary edema
Labs Elevated serum Na >145 mEq/L
Serum osmolality > 295 mOsm/kg
Elevated urine specific gravity and urine osmolality
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 23/90
Nursing Management Maintain normal fluid balance
I&O accurately
Weigh daily
Increase OFI as appropriate
Use hypertonic sol’n cautiously
Monitor serum Na level
Protect from injury
Assess VS, Skin turgor, neurologic status and for thirst
Reposition frequently
Keep side rails up, bed in low position, call light within reach
Secure all invasive lines

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 24/90
HypoKalemia Potassium deficiency
Serum potassium < 3.5mEq/L
Causes: Inadequate dietary intake of potassium
Excessive loss Tx like amphotericin B, diuretics, coricosteroid therapy, IVT
without K replacement GI disorders (diarrhea, vomiting, fistula)
Diaphoresis & renal disorders
Metabolic alkalosis
Hyperaldosteronism
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 25/90
HypoKalemia S/s
Anorexia
N/V
Fatigue Muscle weakness, leg cramps or paresthesia
Cardiac arrthymias
Decrease bowel motility, ileus, abdominal distention
Labs Serum K+ <3.5 mEq/L
ECG : f lattened T wave, prominent U wave, depressed STsegment, prolonged PR interval
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 26/90
Nursing Management Encourage potassium rich foods
Administer potassium replacement orally (K durules)
Infuse parenteral potassium supplement. (diluted in atleast 100cc of solution, administered through infusionpump or side drip, monitor ECG)
Never administer potassium per IV push or IM
Monitor I&O, serum K Assess for abdominal distention
Prevent injury in client’s taking digitalis

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 27/90
HyperKalemia Potassium excess
Serum K+ >5.5 mEq/L
Causes:
Decreased renal excretion due to renal failure
Hypoaldosteronism
Acidosis Severe tissue damage (burns, massive infection)
Excessive intake of K supplement
Hemolysis
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 28/90
HyperKalemia S/s
Cardiac arrythmias
Muscle weakness, paresthesias, paralysis
Irritability and anxiety
Abdominal cramps with diarrhea
Labs
Serum K+ >5.5mEq/L ECG: tall tented T waves, prolonged PR interval and
QRS duration, absent P waves, and ST depression

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 29/90
Nursing Management Decrease intake of K+ rich foods Cation Exchange resins (e.g. kayexalate) Ca gluconate – antagonizes the effects in cardiac
conduction Parenteral NaH2CO3 – alkalinizes plasma and causes
temporary shift of K+ to cells Administration of D50-50 Hemodialysis
Assess s/s of hyperkalemia Assess ECG and serum K+ level Do not prolong use of torniquet in drawing blood Caution in use of salt substitutes and K+ sparing diuretics

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 30/90
HypoCalcemia Calcium deficiency Serum Ca of <8 mg/dL
Causes: Primary or surgical hypoparathyroidism due to
thyroidectomy Pancreatitis Inadequate Vit. D intake or synthesis Renal failure Drug therapy (e.g. aminoglycosides, corticosteroids,
caffeine) Insufficient Ca intake

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 31/90
HypoCalcemiaS/s
Tetany (tingling in fingers and circumoral area, musclespasms associated with pain in extremities and face)
Positive Trousseau sign Positive Chevostek sign
Carpopedal spasms
Hyperactive deep tendon reflexes due to neuromuscular
irritability Labs:
Serum Ca <8.5 mg/dL
ECG: prolonged QT interval

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 32/90
Nursing Management Increase Ca rich foods in the diet (e.g. dilis, etc)
Increase Vit. D rich foods intake
Regular exercise
Monitor serum Ca
Institute seizure precautions
Administer parenteral Ca. (caution: tissue necrosis if IV line – infiltrated)
Do not add Ca in solns with bicarbonate orphosphorus – can cause precipitation
Caution in the Ca administration in pts taking digitalis

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 33/90
HyperCalcemia Calcium excess
Serum Ca > 10.5 mg/dL
Causes:
Excessive calcium administration or intake
Movement of calcium from bones to serum
Decreased renal excretion due to renal failure
Drug therapy with thiazide diuretics
hyperparathyroidism

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 34/90
HyperCalcemia S/s
Anorexia, N/V
Constipation
Muscular weakness, incoordination ALOC (slurred speech, confusion, lethargy, coma)
Polyuria, polydypsia
Cardiac arrythmias
Hypoactive DTR Labs
Serum Ca >10.5 mg/dL
ECG: shortened QT interval, bradycardia and heart blocks
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 35/90
Nursing Management Teach importance of early ambulation to prevent calcium
loss during hospitalization
Participate in weight bearing exercises
Safety measures when there is mental confusion Assess for DHN, mental confusion, psychotic behavior
Encourage 3-4 quarts of fluid daily and dietary fiber
Parenteral saline solution to dilute serum Ca
Administer parenteral phosphate Administer furosemide
Treatment of underlying cause, calcitonin forhyperparathyroidism, corticosteroids for CA

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 36/90
HypoMagnesemia Magnesium deficiency
Serum Mg <1.5 mEq/L
Causes:
Poor nutrition
Alcoholism
GI and renal losses without replacement

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 37/90
HypoMagnesemia S/s
(+) Trousseau & Chevostek signs
Neuromuscular irritability
Insomia Mood changes
Cardiac arrythmias
Labs: Serum Mg < 1.5 mEq/L
ECG: f lattened T wave, prominent U wave, anddepressed ST segment
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 38/90
Nursing Management Discuss the misuse of diuretics and laxatives Dietary sources of Mg (nuts, whole grains, cornmeal,
bananas, etc)
Administer parenteral Mg in infusion pump Monitor for s/s of magnesium toxicity (hot, flushed skin,diaphoresis, anxiety or lethargy, hypotension, laryngealstridor)
Monitor ECG and pulse
Monitor Serum Mg levels Maintain on seizure precautions Institute safety measures for mental confusion Assess ability to swallow cause by dysphagia Monitor clients on digitalis (predisposes to toxicity)

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 39/90
HyperMagnesemia Mg excess
Serum Mg level > 2.5 mEq/L
Causes:
Renal failure
Overuse of Mg-containing antacids
Excessive Mg administration
Overuse of enemas or laxatives containing Mg
Severe dehydration, as in DKA

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 40/90
HyperMagnesemia S/s
Hot, flushed skin
Hypoactive reflexes
Hypotension, bradycardia Depressed respirations, lethargy, drowsiness, and absent
DTR
Cardiac arrythmias
Labs Serum Mg level >2.5 mEq/L
ECG: prolonged QT interval and AV blocks

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 41/90
Nursing Management Health teaching on antacid or cathartic use as well as OTC
drugs containing Mg Discontinue all parenteral or oral Mg
During respiratory or cardiac emergencies, collaborate withthe RT providing respiratory support Administer Ca gluconate to antagonize effect of Mg Prepare for hemodialysis as necessary Administer diuretics and 0.45% NSS – excretion of Mg
Monitor serum Mg level Monitor VS, CV status, Respiratory status, patellar reflexes,
LOC Institute safety precautions
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 42/90
HypoPhosphatemia Phosphorus deficiency
Serum Phosphorus < 2.5 mg/dL
Causes:
Overzealous intake or administration of CHO
TPN administration
Prolonged intense hyperventilation, alcohol withdrawal, DKA
Excess phosphorus binding antacids
Severe DHN, as occurs in DKA

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 43/90
HypoPhosphatemia S/s:
Irritability, apprehension, weakness, numbness,confusion, seizure, coma
Hypoxia leading to an increase RR and respiratory alkalosis
Muscle weakness, muscle pain
Bruising, bleeding due to platelet dysfunction
Increase susceptibility to infection Labs:
Serum Mg level <2.5 mEq/L
Increase urine Mg
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 44/90
Nursing Management Assess VS, s/s of apprehension, confusion, ALOC
Institute seizure precautions
Prevention of infection since may change granulocytes Introduce TPN gradually to prevent rapid shift of
phosphorus into the cells
Monitor serum level of Phosphorus (N: 2.5-4.5mEq/L)
Monitor possible complication of phosphorus – hypoCa

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 45/90
HyperPhosphatemia Phosphorus excess
Serum phosphorus > 4.5 mEq/L
Causes:
Renal failure
Chemotherapy for neoplastic disease
High phosphorus intake
Profound muscle necrosis
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 46/90
HyperPhosphatemia S/s
Soft tissue calcification
Tetany
Anorexia, N/V
Muscle weakness, hyperreflexia, tachycardia
Labs:
Serum phosphorus level >4.5 mEq/L Xray studies show skeletal changes with abnormal bone
development
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 47/90
Nursing Management Avoid foods high in phosphorus (hard cheese, cream,
nuts, whole grains, dried foods, dried vegetables)
Avoid phosphate containing substances (laxatives,enemas that contain phosphate)
Institute seizure precautions
Monitor serum phosphorus level
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 48/90

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 49/90
Hydrogen Ion and pHImportance:
Membrane integrity
Metabolic enzyme reactionsConcentration:
0.0000001 mg/L
pH = power of hydrogen
pH = -log [H+] = 10 -7 = pH 7.0

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 50/90
Hydrogen Ion and pH greater the H+ = more acidic = lower pH
lesser the H+
= more basic = higher pH
body fluid pH = 7.35 – 7.45 (narrow range)
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 51/90
pHH+
concentration

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 52/90

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 53/90
Regulation of Acid-Base Balance
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 54/90
BUFFERS
absorb excessive hydrogen (H+) (acid) or hydroxyl ion
(OH-) (base)
contains salts of either weak acids or weak bases thateither: combine with H+ when H+ increase in body fluids release H+ when H+ decrease in body fluids
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 55/90
1. PO4
3-
buffer system
Reaction:
HPO4
2-
+ H
+↔
H2PO4
-
monohydrogen hydrogen dihydrogen
phosphate ion ion phosphate ion
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 56/90
2. Proteins amino acid side chains
contains: Carboxyl group ( -COOH )
Amine group ( -NH2 )

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 57/90
Reaction:
-COO- + H+↔ -COOH
carboxyl hydrogen carboxyl
group ion group
-NH2 + H+↔ -NH 3
amine group hydrogen ammonium
ion group
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 58/90
3. Bicarbonate (HCO3
-
)Reaction:
CO2 + H2O↔
H2CO 3 ↔
H
+
+ HCO 3
-
Carbon water carbonic hydrogen bicarbonate
dioxide acid ion ion
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 59/90
responds rapidly to a change in pH and
function to bring the pH back to itsnormal range
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 60/90
powerful regulator of pH, but responds moreslowly than does the respiratory system
nephrons → secretion of H+ into the urine andreabsorption of bicarbonate → directly regulates pH
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 61/90
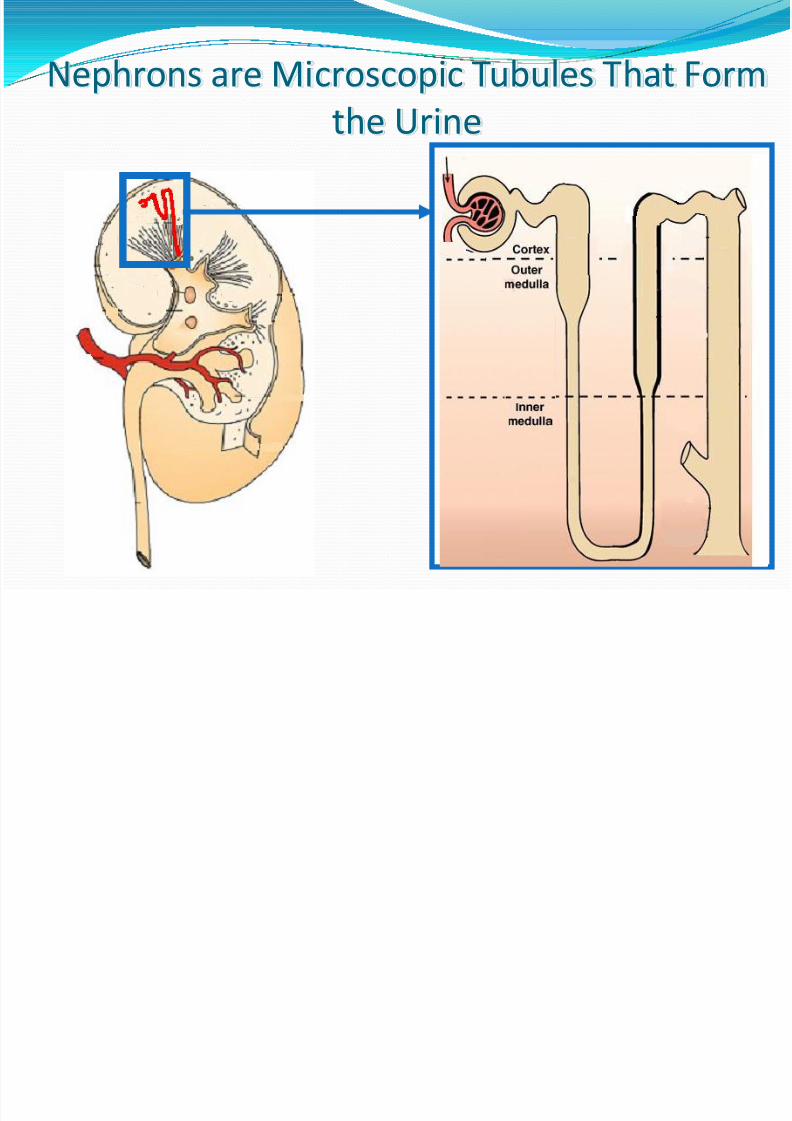
Nephrons are Microscopic Tubules That Form
the Urine
Insert fig 23-4

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 62/90
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 63/90
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 64/90
pH falls below 7.35
major effect: CNS malfunctions → can become comatose

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 65/90
pH increases above 7.45
major effect: hyperexcitability of thenervous system

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 66/90
Respiratory acidosis Respiratory alkalosis
Increased PCO2
Increased carbonic acid
Increased H+ = low pH
(<7.35)
Increased bicarbonate
Decreased PCO2
Decreased carbonic acid
Decreased H+ = high pH
(>7.45)
Decreased bicarbonate
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 67/90
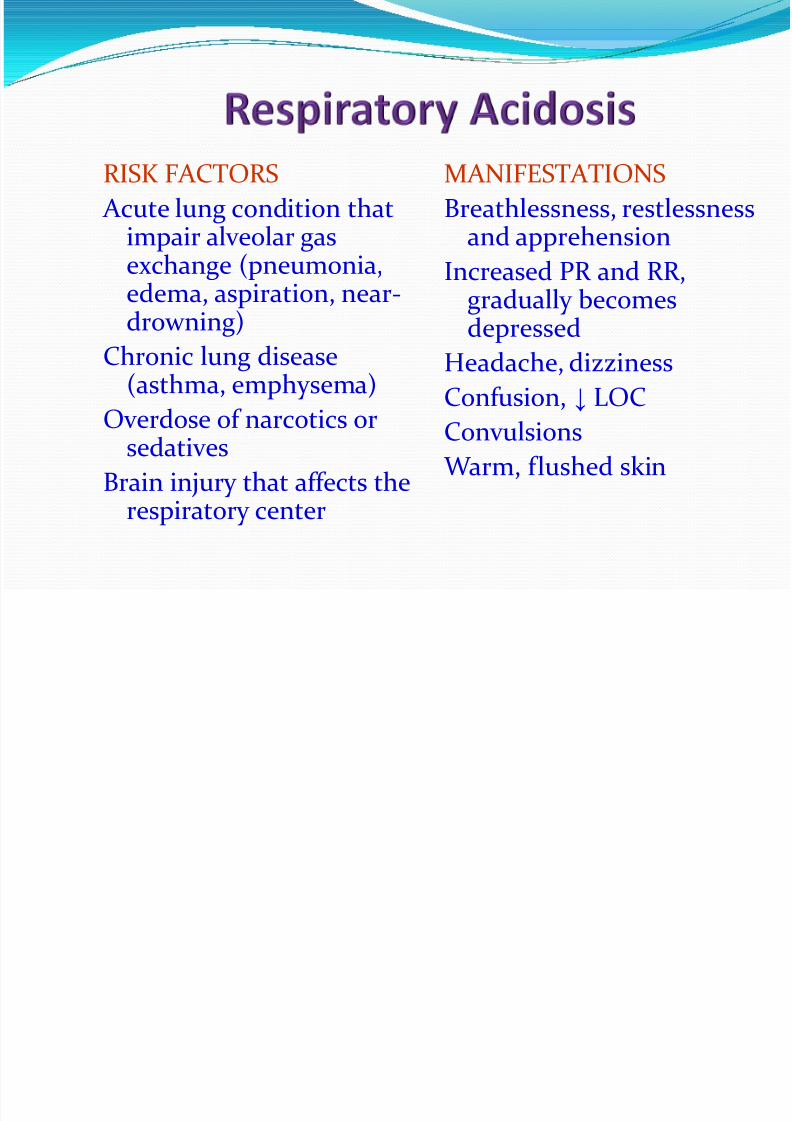
RISK FACTORS
Acute lung condition thatimpair alveolar gasexchange (pneumonia,
edema, aspiration, near-drowning)
Chronic lung disease(asthma, emphysema)
Overdose of narcotics orsedatives
Brain injury that affects therespiratory center
MANIFESTATIONS
Breathlessness, restlessnessand apprehension
Increased PR and RR,gradually becomesdepressed
Headache, dizziness
Confusion, ↓ LOC
Convulsions Warm, flushed skin
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 68/90
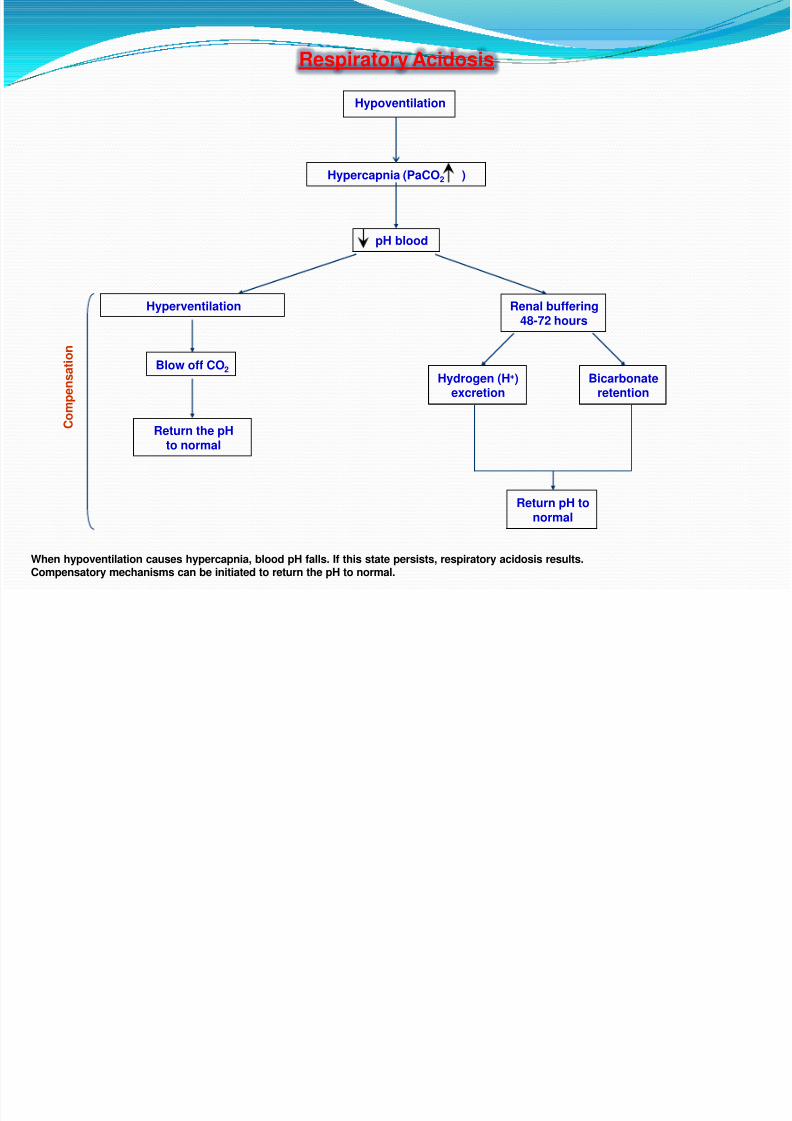
Respiratory Acidosis
Hypoventilation
Hypercapnia (PaCO2 )
pH blood
Hyperventilation Renal buffering48-72 hours
Blow off CO2
Return the pHto normal
Hydrogen (H+)excretion
Bicarbonateretention
Return pH tonormal
C
o m p e n s a t i o n
When hypoventilation causes hypercapnia, blood pH falls. If this state persists, respiratory acidosis results.Compensatory mechanisms can be initiated to return the pH to normal.

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 69/90
RISK FACTORS
Hyperventilation due to:
Extreme anxiety
Elevated body temperature
Overventilation with amechanical ventilator
Hypoxia
Salicylate overdose
MANIFESTATIONS
Shortness of breath, chesttightness
Light-headedness,numbness, tingling of theextremities
Difficulty concentrating
Tremulousness, blurred vision

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 70/90
Respiratory Alkalosis
Hyperventilation
Hypercapnia (PaCO2 )
pH blood
Hypoventilation Renal buffering48-72 hours
Retain CO2
Return the pHto normal
Hydrogen (H+)retention
Bicarbonateexcretion
Return pH tonormal
C
o m p e n s a t i o n
When hyperventilation causes hypocapnia, the blood pH elevates. If this state persists, respiratory alkalosis results.Compensation by the lungs and kidneys will usually be initiated to return the pH to normal.

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 71/90
Metabolic acidosis Metabolic alkalosis
Increased H+ = low pH
(<7.35)
Decreased bicarbonate
Heavier breathing causes
decreased PCO2
Decreased H+ = high pH
(>7.45)
Increased bicarbonate
Lighter breathing causes
increased PCO2

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 72/90
RISK FACTORS
Conditions that ↑ nonvolatile
acids in the blood ( renal
impairment, DM,starvation )
Conditions that ↓ bicarbonate ( prolonged
diarrhea )Excessive infusion of
chloride-containing IV fluids ( NaCl )
MANIFESTATIONS
Kussmaul’s respirations
Lethargy, confusion
Headache
Weakness
Anorexia, nausea, vomitingand diarrhea
M b li A id i
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 73/90
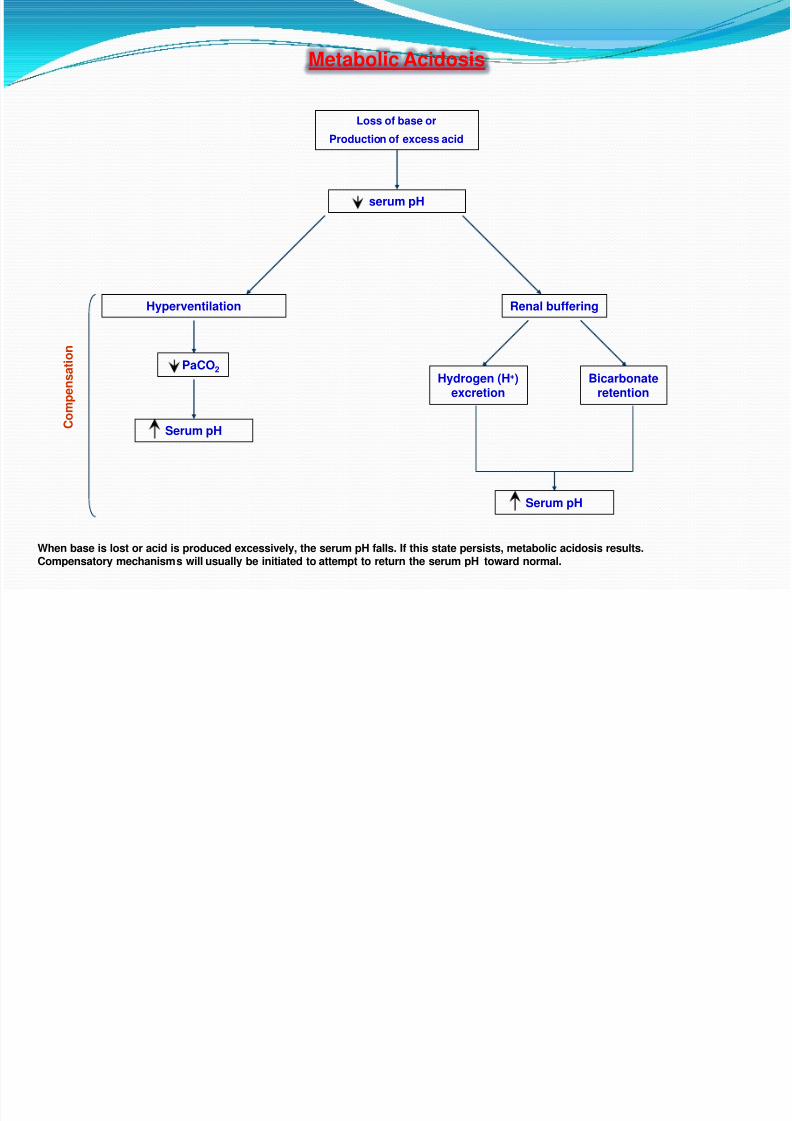
Metabolic Acidosis
Loss of base or
Production of excess acid
serum pH
Hyperventilation Renal buffering
PaCO2
Serum pH
Hydrogen (H+)excretion
Bicarbonateretention
C
o m p e n s a t i o n
When base is lost or acid is produced excessively, the serum pH falls. If this state persists, metabolic acidosis results.
Compensatory mechanisms will usually be initiated to attempt to return the serum pH toward normal.
Serum pH

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 74/90
RISK FACTORSExcessive acid losses due to:
Vomiting
Gastric suction
Excessive use of K-losing diuretics
Excessive adrenal corticoidhormones due to:
Cushing’s syndrome
Hyperaldosteronism
Excessive bicarbonate intake from:
Antacids
Parenteral NaHCO3
MANIFESTATIONS Decreased RR and depth
Dizziness
Numbness and tingling of theextremities
Hypertonic muscles, tetany
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 75/90
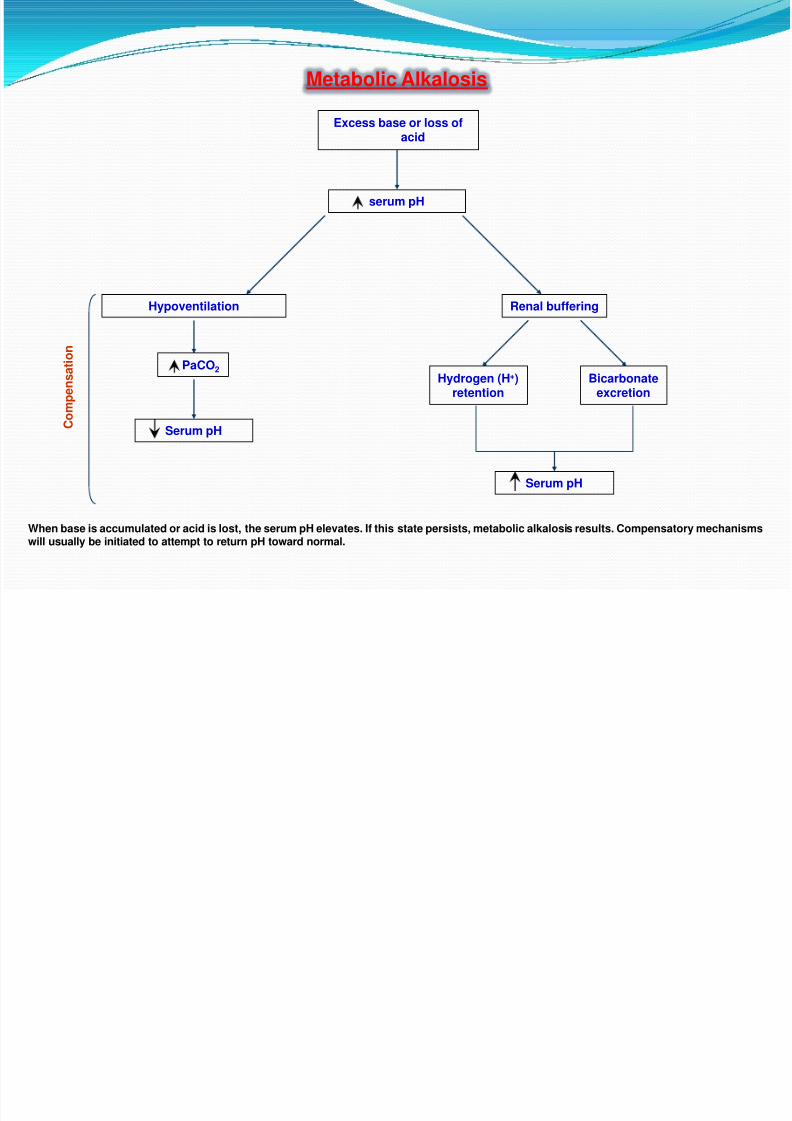
Metabolic Alkalosis
Excess base or loss ofacid
serum pH
Hypoventilation Renal buffering
PaCO2
Serum pH
Hydrogen (H+)retention
Bicarbonateexcretion
C
o m p e n s a t i o n
When base is accumulated or acid is lost, the serum pH elevates. If this state persists, metabolic alkalosis results. Compensatory mechanismswill usually be initiated to attempt to return pH toward normal.
Serum pH
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 76/90

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 77/90
Arterial Blood Gases
performed to evaluate the client’s acid-base
balance and oxygenation
arterial blood – provides a truer reflection of gas exchange in the pulmonary system
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 78/90
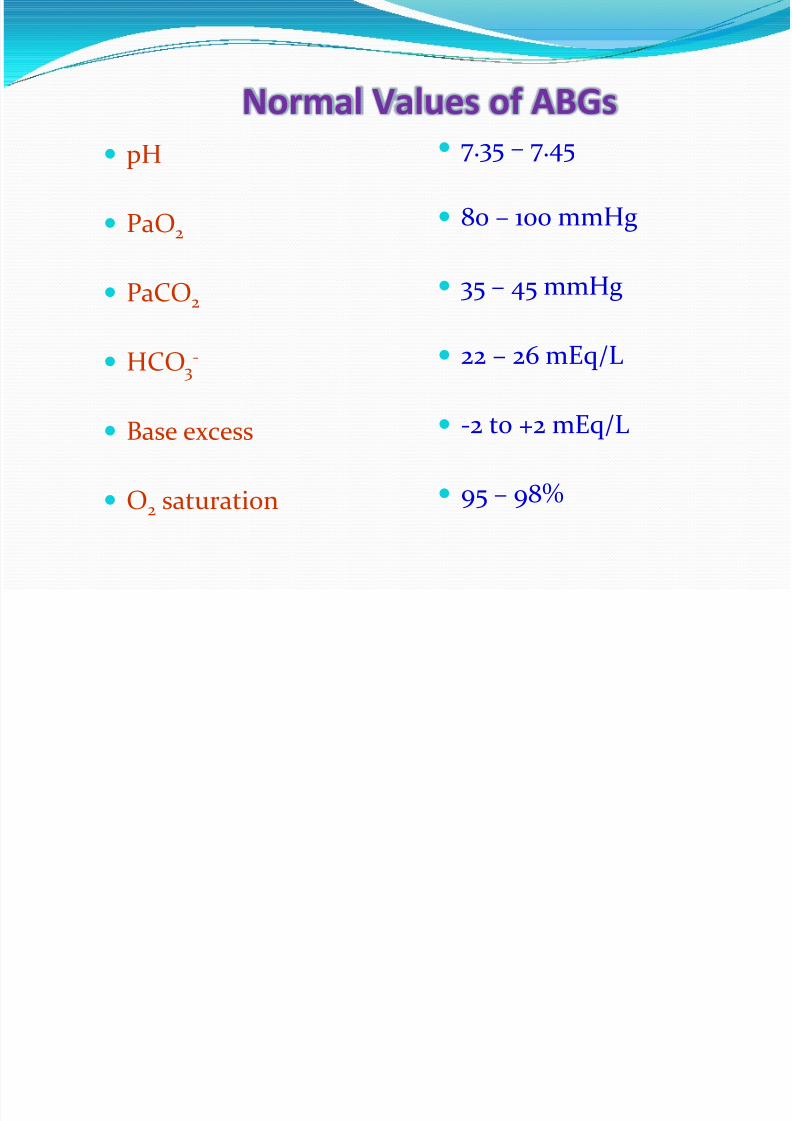
Normal Values of ABGs
pH
PaO2
PaCO2
HCO3-
Base excess
O2 saturation
7.35 – 7.45
80 – 100 mmHg
35 – 45 mmHg
22 – 26 mEq/L
-2 to +2 mEq/L
95 – 98%
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 79/90
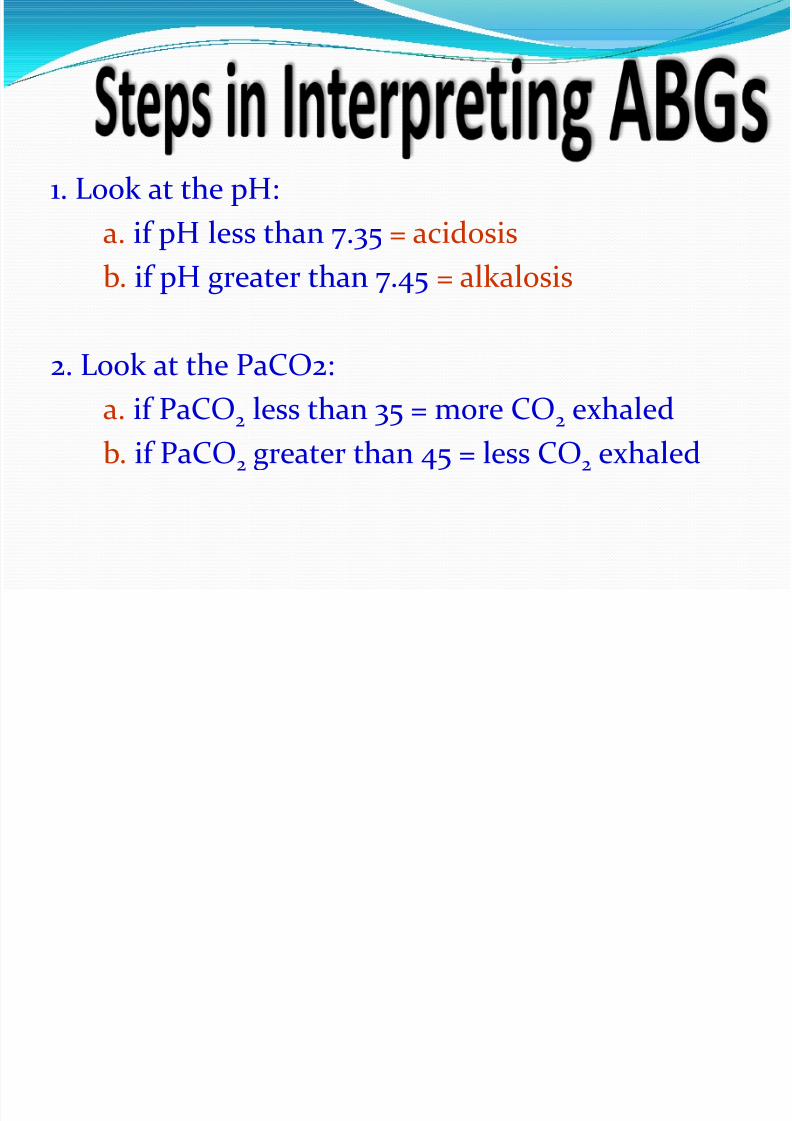
1. Look at the pH:
a. if pH less than 7.35 = acidosis
b. if pH greater than 7.45 = alkalosis
2. Look at the PaCO2:
a. if PaCO2
less than 35 = more CO2
exhaled
b. if PaCO2 greater than 45 = less CO2 exhaled

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 80/90
3. Assess the pH and PaCO2 relationship for apossible respiratory problem:
a. if pH less than 7.35 (acidosis) and PaCO2
isgreater than 45 mmHg, retained CO2 →
respiratory acidosis
b. if pH greater than 7.45 (alkalosis) and PaCO2 is less than 35 mmHg, lack of CO2 →
respiratory alkalosis
8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 81/90
4. Look at the bicarbonate:
a. if HCO3 is less than 22 mEq/L = lower
bicarbonate levelb. if HCO3 is greater than 26 mEq/L = higherbicarbonate level

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 82/90
5. Assess pH, HCO3, and base excess (BE) values
for a possible metabolic problem:
a. if pH less than 7.35 (acidosis), HCO3 less than22 mEq/L and BE below -2mEq/L = low
bicarbonate levels = metabolic acidosis
b. if pH greater than 7.45 (alkalosis), HCO3
greater than 26 mEq/L and BE above +2mEq/L = high bicarbonate level =metabolic
alkalosis

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 83/90
6. Look for evidence of COMPENSATION:
a. Respiratory acidosis: pH < 7.35PaCO2 > 45 mmHgIf : HCO3 is greater than 26 mEq/L = kidneys maintaining
bicarbonate to minimize acidosis = RENALCOMPENSATION
b. Respiratory alkalosis: pH > 7.45PaCO2 < 35 mmHg
If : HCO3 is less than 22 mEq/L = kidneys excretingbicarbonate to minimize alkalosis = RENAL
COMPENSATION

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 84/90
c. Metabolic acidosis: pH < 7.35
HCO3 < 22 mEq/LIf : PaCO2 is less than 35 mmHg = CO2 being “blown off”
to minimize acidosis = RESPIRATORY COMPENSATION
d. Metabolic alkalosis: pH > 7.45
HCO3 > 26 mEq/L
If: PaCO2 is greater than 45 mmHg = CO2 being retainedto compensate for excess base = RESPIRATORY
COMPENSATION

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 85/90

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 86/90
1. pH 7.30
pCO2 55 mmHg
HCO3 25 mmHg
2. pH 7.49
pCO2 38 mmHg
HCO3 32 mmHg

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 87/90
3. pH 7.28
pCO2 42 mmHg
HCO3 19 mmHg
4. pH 7.51
pCO2 29 mmHg
HCO3 25 mmHg

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 88/90
5. pH 7.30
pCO2 38 mmHgHCO3 19 mmHg
6. pH 7.33
pCO2 33 mmHg
HCO3 19 mmHg
7. pH 7.35pCO2 29 mmHg
HCO3 19 mmHg

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 89/90
8. pH 7.28
pCO2 55 mmHgHCO3 26 mmHg
9. pH 7.32pCO2 55 mmHg
HCO3 31 mmHg
10. pH 7.35
pCO2 55 mmHg
HCO3 34 mmHg

8/3/2019 Electrolytes 1016
http://slidepdf.com/reader/full/electrolytes-1016 90/90
Related Documents











