WATER AND ELECTROLYTES BALANCE IN ICU SAMIR EL ANSARY ICU PROFESSOR AIN SHAMS CAIRO

Electrolyte balance in critically ill patients
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

WATER AND ELECTROLYTES BALANCE
IN ICU
SAMIR EL ANSARYICU PROFESSOR
AIN SHAMSCAIRO
Global Critical Carehttps://www.facebook.com/groups/1451610115129555/#!/groups/145161011512
9555/ Wellcome in our new group ..... Dr.SAMIR EL ANSARY

Objectives
• Explain in flow chart form how the rates of sodium and water excretion are affected by:
–Drinking isotonic saline
–Partial constriction of a single renal artery
–Profuse sweating
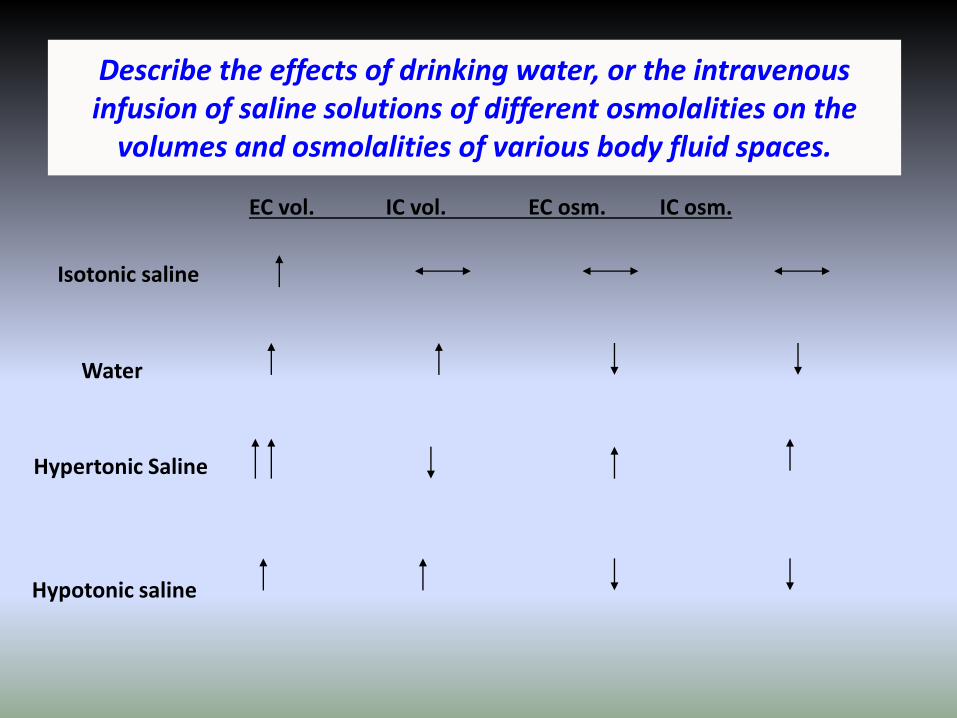
Describe the effects of drinking water, or the intravenous infusion of saline solutions of different osmolalities on the
volumes and osmolalities of various body fluid spaces.
EC vol. IC vol. EC osm. IC osm.
Isotonic saline
Water
Hypertonic Saline
Hypotonic saline
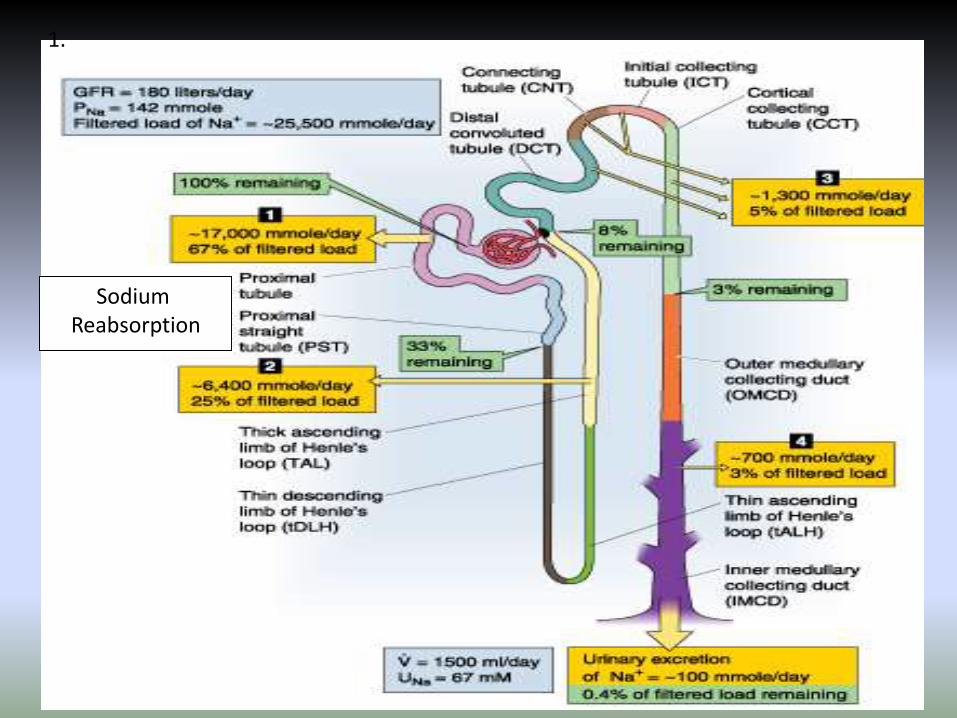
1.
Sodium Reabsorption

Sodium balance
Most NaCl intake added during food preparation
Sweat output depends on body temperature
Urine output of NaCl is regulated by blood pressure

Water balance
Metabolically produced by oxidation of H-containing nutrients
Insensible loss: expiration of 37 saturated air, evaporation through skin (different from sweat)
Urine output regulated by vasopressin (antidiuretic hormone ADH)
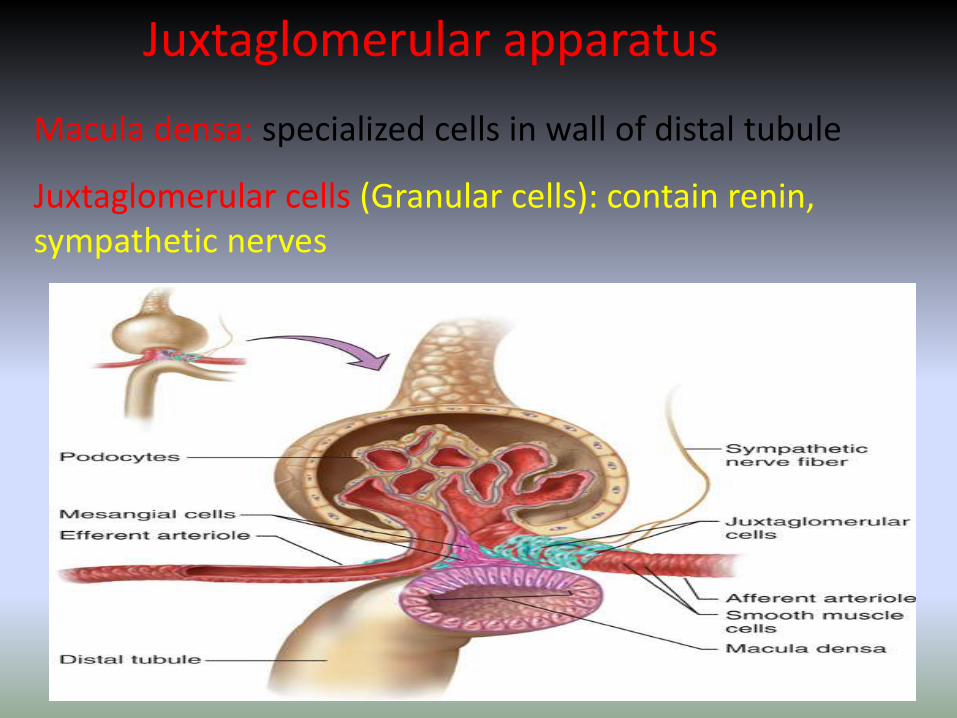
Juxtaglomerular apparatus
Macula densa: specialized cells in wall of distal tubule
Juxtaglomerular cells (Granular cells): contain renin, sympathetic nerves

Forces of filtration

Substance X: filtered & entirely secreted (rare)
Substance Y: filtered & partially reabsorbed (Na+, K+, water)
Substance Z: filtered & entirely reabsorbed (glucose, amino acids)
Kidney handling of various substances

Water LoadingDrink Water
Plasma Osmolality
Activation of osmoreceptors inanterior hypothalamus
ADH secretion from Post. Pituitary
Water permeability in late DT and CT
Water Reabsorption
Urine Osmolality Urine Volume
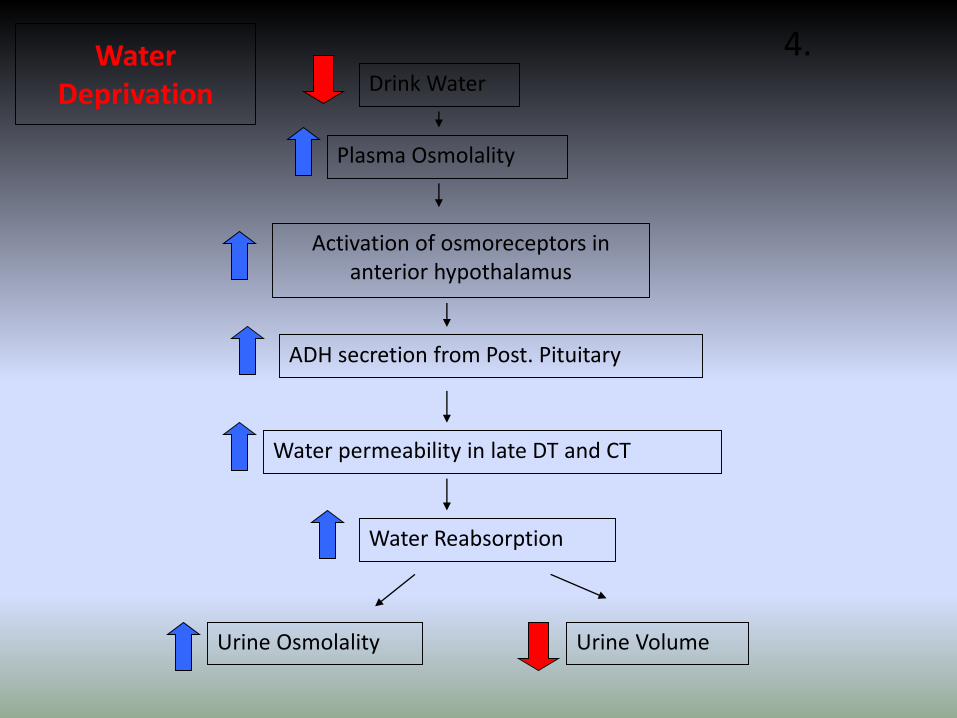
Water Deprivation Drink Water
Plasma Osmolality
Activation of osmoreceptors inanterior hypothalamus
ADH secretion from Post. Pituitary
Water permeability in late DT and CT
Water Reabsorption
Urine Osmolality Urine Volume
4.

Review: Hormones of Water and Sodium Regulation
• Angiotensin-II
• Anti-diuretic hormone/vasopressin/AVP
• Aldosterone
• Atrial natriuretic peptide (ANP)


Reninangiotensinaldosteronesystem
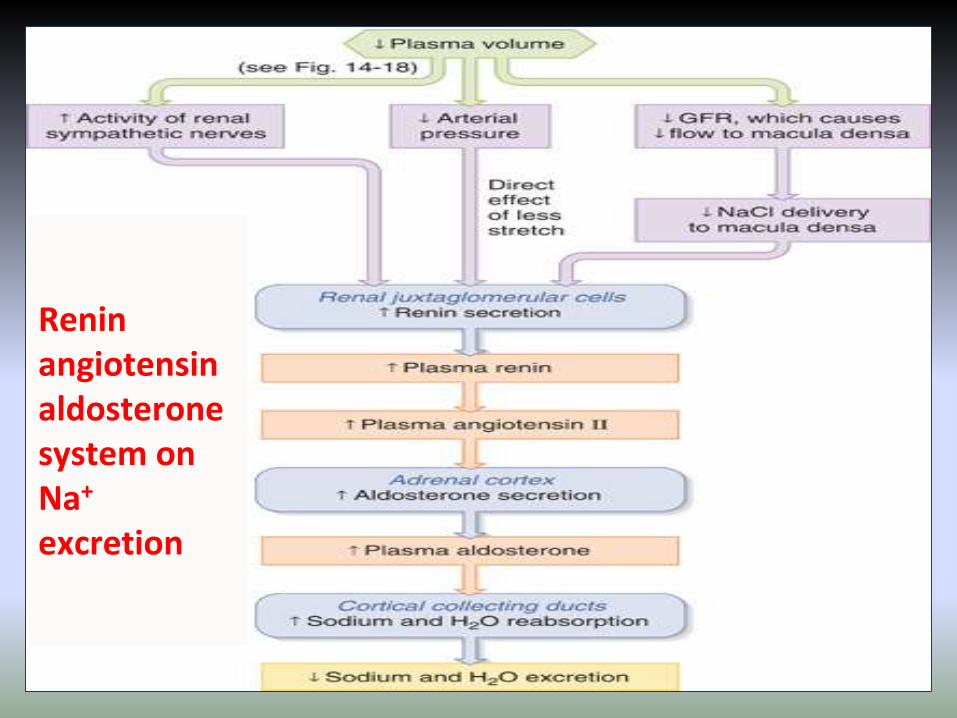
Reninangiotensinaldosteronesystem on Na+
excretion

Macula densa: specialized cells in wall of distal tubule
Juxtaglomerular cells (Granular cells): contain renin, sympathetic nerves
Juxtaglomerular apparatus
Mesangial cells.
1.
2.
3. Pressure (less stretch)
Decreased NaCl sensing
Sympathetic NS
RENIN
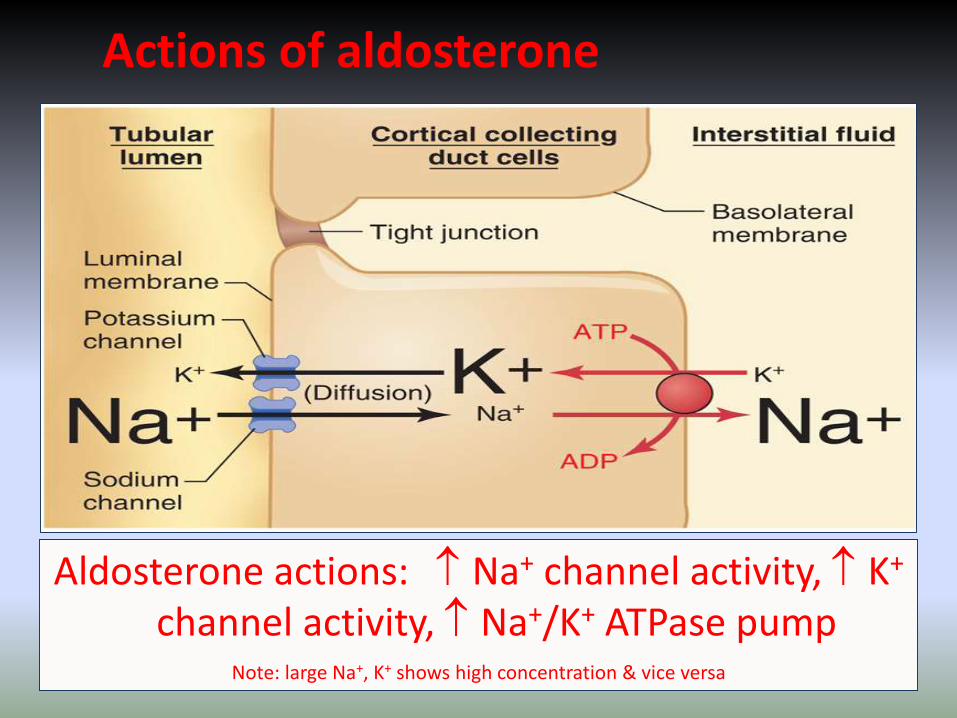
Actions of aldosterone
Aldosterone actions: Na+ channel activity, K+
channel activity, Na+/K+ ATPase pumpNote: large Na+, K+ shows high concentration & vice versa
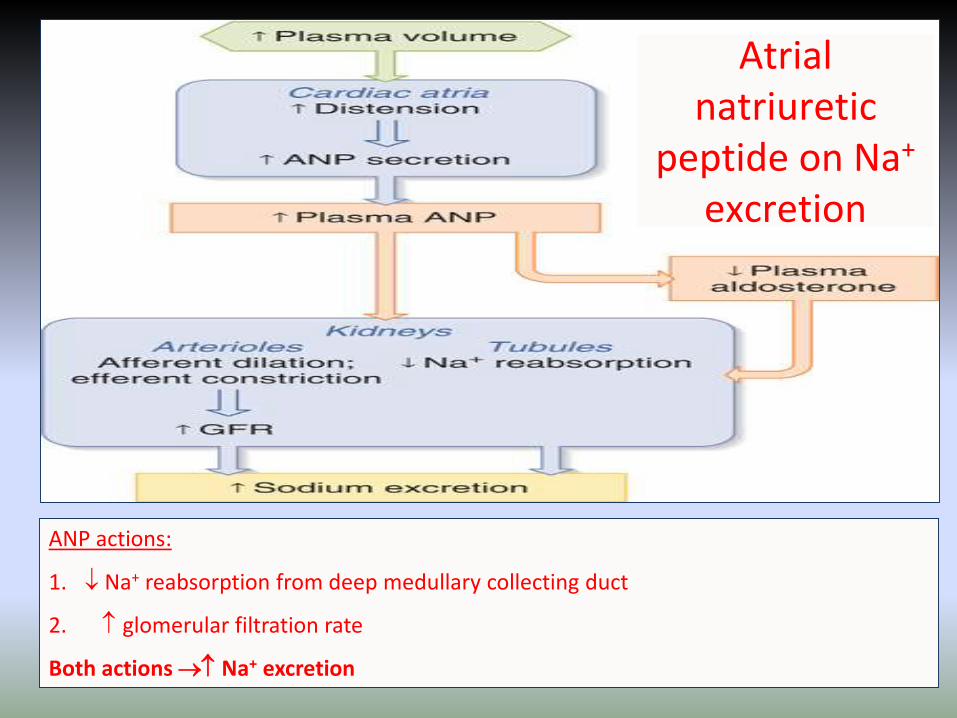
ANP actions:
1. Na+ reabsorption from deep medullary collecting duct
2. glomerular filtration rate
Both actions Na+ excretion
Atrialnatriuretic
peptide on Na+
excretion

Vasopressin (ADH) release & actions
Vasopressin release stimulated by:
1.slight (1%) increase in plasma osmolality
2.large (~10-15%) reduction in plasma volume
Vasopressin action:
Increases permeability of collecting duct to water

Vasopressin (ADH) release & actions
Renal medulla
has osmotic gradient from 300 mOsm/kg at cortical border to 1200 mOsm/kg at deepest part of medulla
ADH levels collecting duct
permeability water reabsorption urine volume with osmolality

Diabetes Insipidus
• Loss of ADH secretion or insensitivity of kidneys to ADH
• Large severely dilute amounts of urine
• Increased intake of water
• Danger lies in hyponatremia and ultimate central nervous system edema and death.
Types of Diabetes Insipidus
• Central– Damage to hypothalamus – no ADH
• Nephrogenic– Kidneys cannot respond to ADH
– Usually genetic (rare) 90% cases due to V2receptor mutation, 10% due to Aquaporinmutation.

Types of Diabetes Insipidus
• Dipsogenic–Damage to thirst center – making patient
abnormally thirsty
• Gestational–During pregnancy women produce
vasopressinase which breaks down ADH, increasing urine output.
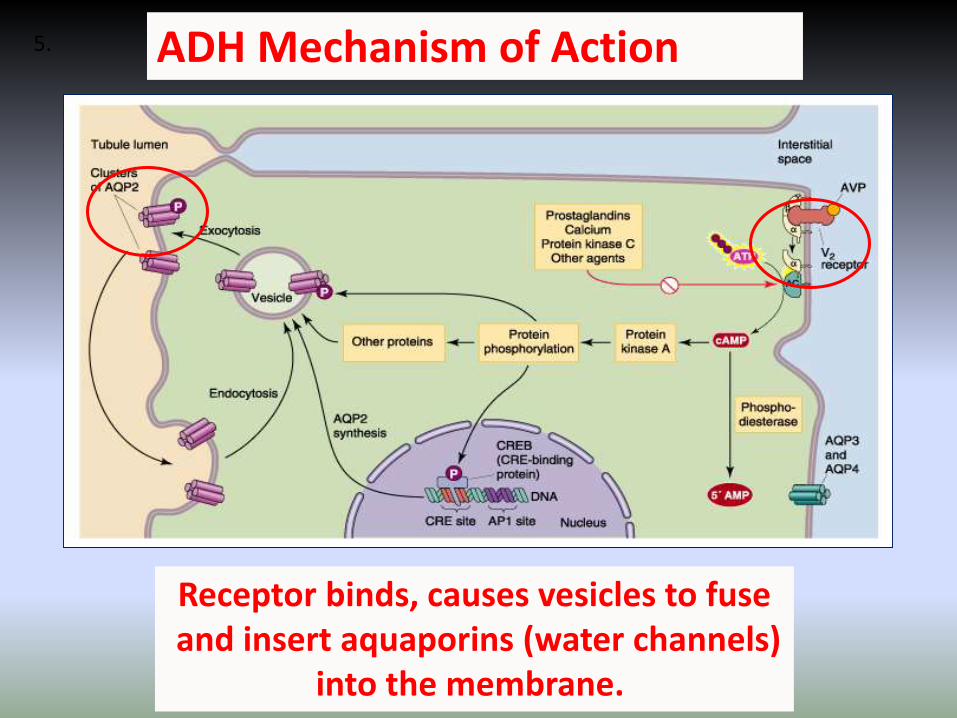
ADH Mechanism of Action
Receptor binds, causes vesicles to fuseand insert aquaporins (water channels)
into the membrane.
5.
How to test for it?
• Water deprivation test– If water deprivation results in dilute voluminous
urine, then cause is likely not dipsogenic (but central or nephrogenic)
• Desmopressin test (ADH analog)– Central and Gestational respond to this treatment
– Nephrogenic does not
• If kidneys are insensitive, then they won’t respond.

SIADH (syndrome of inappropriate ADH
secretion)
• Excessive ADH secretion• Not “turned off” by drop in osmolality from
drinking water and water retention.
• Hyponatremia is also the main concern
• Causes– Head trauma
– Ectopic lung tumor (secretes ADH).
– Treatment – water deprivation or removal of tumor

Water transport & vasopressin actions

Sweat is hypotonic (i.e. osmolality < plasma)
Sweating without water replacement
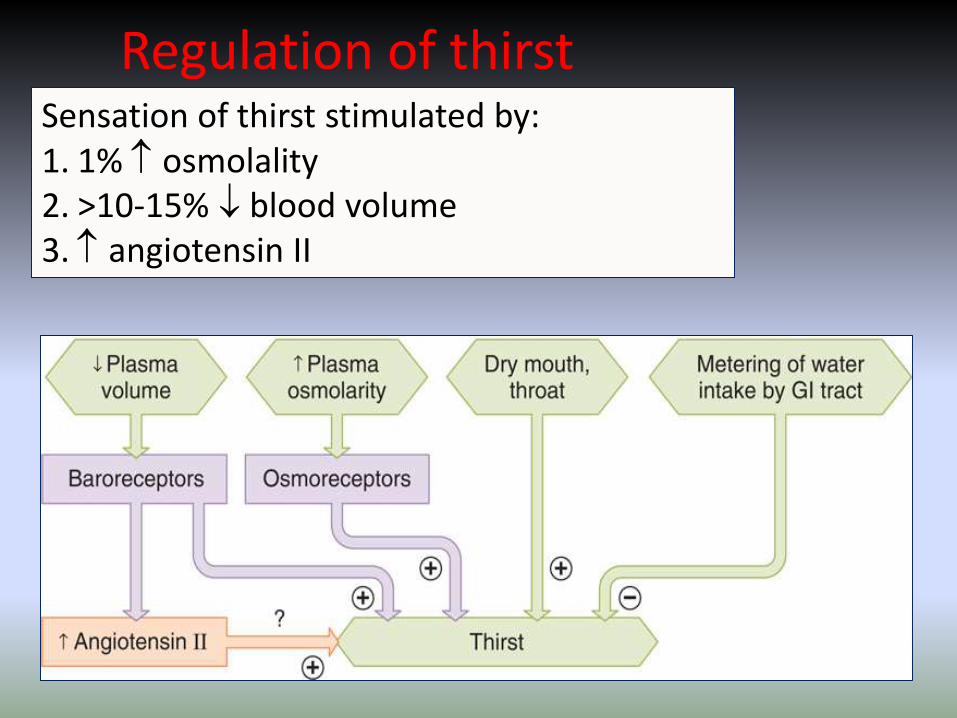
Regulation of thirstSensation of thirst stimulated by:1. 1% osmolality2. >10-15% blood volume3. angiotensin II

Isotonic saline
Extracellular volume
Blood pressure
Renin, angiotensinaldosterone
Sympathetic NS
Sodium excretion
Plasma osmolality
Atrial Natriuretic peptide
ADH secretion
Water excretion
-
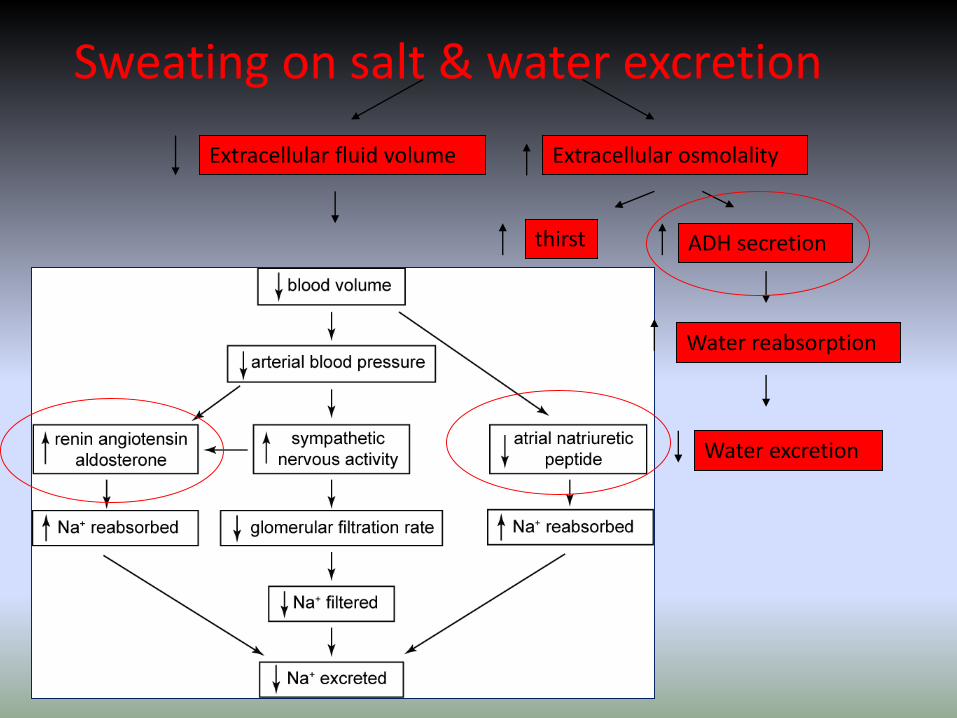
Extracellular fluid volume Extracellular osmolality
thirst ADH secretion
Water reabsorption
Water excretion
Sweating on salt & water excretion

Contstriction of renal artery
Afferent arteriole pressure
RENIN
Angiotensin-II
Aldosterone
Increase Na+
reabsorption
Plasma osmolality
vasoconstriction
ADH
Salt and water retention
Water excretion
Extracellular & vascular volume
Increased systemic blood pressure
GFR
Sodium filtered
Sodium excreted

What is renal hypertension? (renovascular hypertension)
BEFORE
AFTER
1) “ESSENTIAL” HYPERTENSION
-no specific cause-body unable to regulate blood pressure-systolic BP >140, diastolic > 90mmHg -Managed with meds, diet, and fluid regulation(ACE inhibitors/diuretics)
2) SECONDARY HYPERTENSION
-most common cause isrenal artery stenosis due to atherosclerosis.-usually diagnosed after long-standingHTN becomes unmanageable. -results in very high BP-systolic >200, diastolic >100 mmHg. -decreased RBF (sensed as a drop in BP) results in increases in RENIN, thus causing further peripheral vasoconstriction, sodium/water retention and increases in BP.
PLAQUES ORFIBROSIS
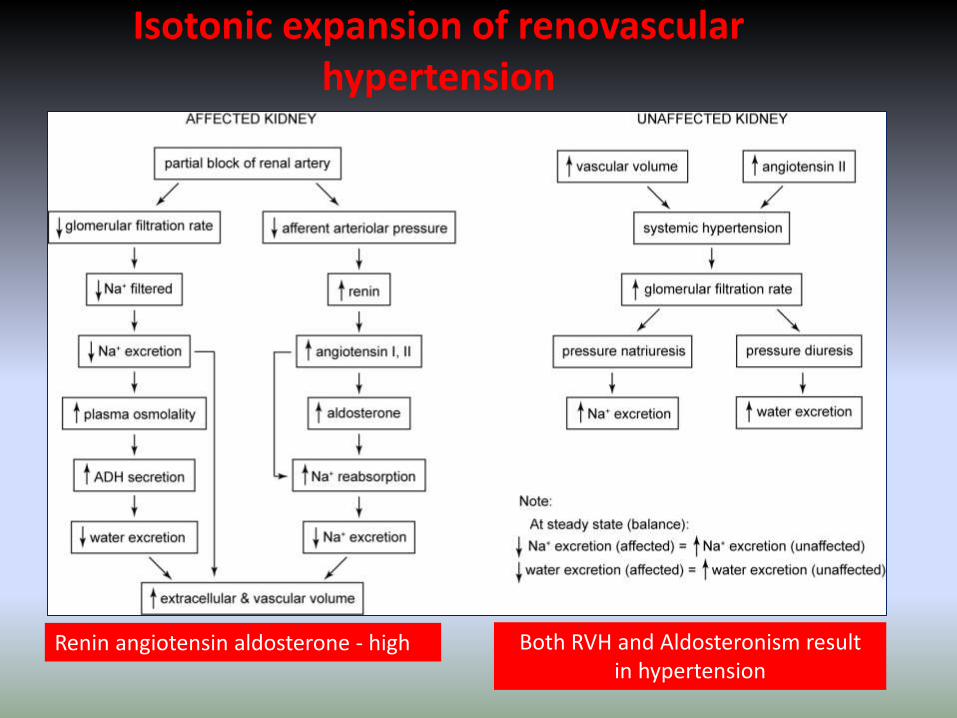
Isotonic expansion of renovascularhypertension
Renin angiotensin aldosterone - high Both RVH and Aldosteronism resultin hypertension

AldosteroneCase E2
“hypertensive 43 y/o F”
Case E5“nausea, weakness,wt. loss 32 y/o M”
Tonicity TonicityVolumeVolume
[Na+] (144)[K+] (2.9)
[Na+] (123)[K+] (6.4)
HTN Bun/Cr = 26
Differentials
Isotonic Expansion
-hypertension-renovascular hypertension-aldosteronism
Hypotonic Contraction
-chronic salt loss w/water replac.-diuretic use (chronic)
-Addison’s disease
Diagnosis Conn’s syndromePrimary aldosteronism
(elevated Aldosterone/low renin)
Treatment/Tests
Surgical removal of tumorSpironolactone
Addison’s disease(low Na, high K, acidosis,
low glucose, tanned appearance)
Measure [corticosteroid]
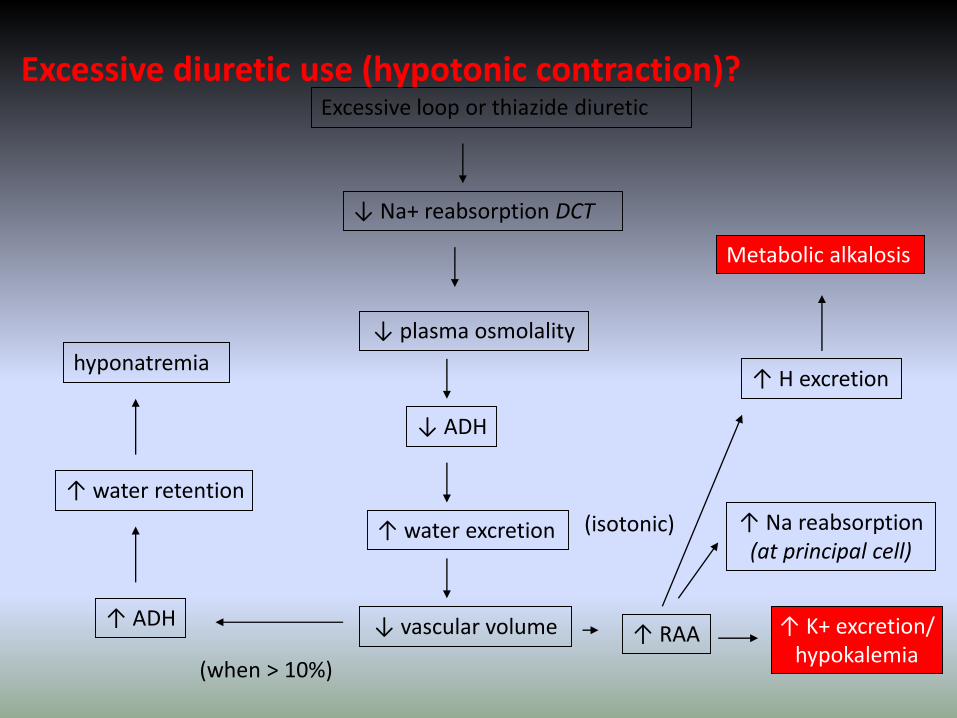
Excessive diuretic use (hypotonic contraction)?Excessive loop or thiazide diuretic
↓ Na+ reabsorption DCT
↓ plasma osmolality
↓ ADH
↑ water excretion
↑ K+ excretion/hypokalemia
(isotonic)
↓ vascular volume ↑ RAA
↑ Na reabsorption(at principal cell)
↑ H excretion
Metabolic alkalosis
(when > 10%)
↑ ADH
↑ water retention
hyponatremia

Addison’s disease (hypotonic contraction)?
↓ aldosterone/glucocorticoids
↓ Na+ reabsorption (principal cell)
↓ plasma osmolality
↓ ADH
↑ water excretion
↓ K+ excretion/hyperkalemia
(isotonic)
↓ vascular volume
↓ H+ excretion/Metabolic acidosis
(when > 10%)
↑ ADH
↑ water retention
hyponatremia
(osmotic response)
hypoglycemia
(pressure response)

Anti-diuretic hormone
Case E3“head trauma MVA”
Case E6“SOB, wt. loss, hemoptysis
and wheezing”
Tonicity TonicityVolume Volume
[Na+] (162)[K+] (3.8)
[Na+] (110)[K+] (4.5)
Bun/Cr = 5.7U[80]mOsmolhemoconcentration
P[230]mOsmolU[496]mOsmol
Differentials
Hypertonic Contraction
-dehydration – bun? Urine vol?-acute renal failure – urine too dilute-diabetes insipidus
Hypotonic Expansion
-polydipsia – [urine]?-Addison’s disease -SIADH
Diagnosis Diabetes Insipidus (low ADH)High plasma osmolality,
Low urine osmolality
Treatment/Tests
Desmopressin test(response – neurogenic)(no response – nephrogenic)
SIADH (high ADH)Low plasma osmolalityHigh urine osmolality
Chest X-rayRemove ADH secreting tumor
water loss > salt loss salt loss > water loss
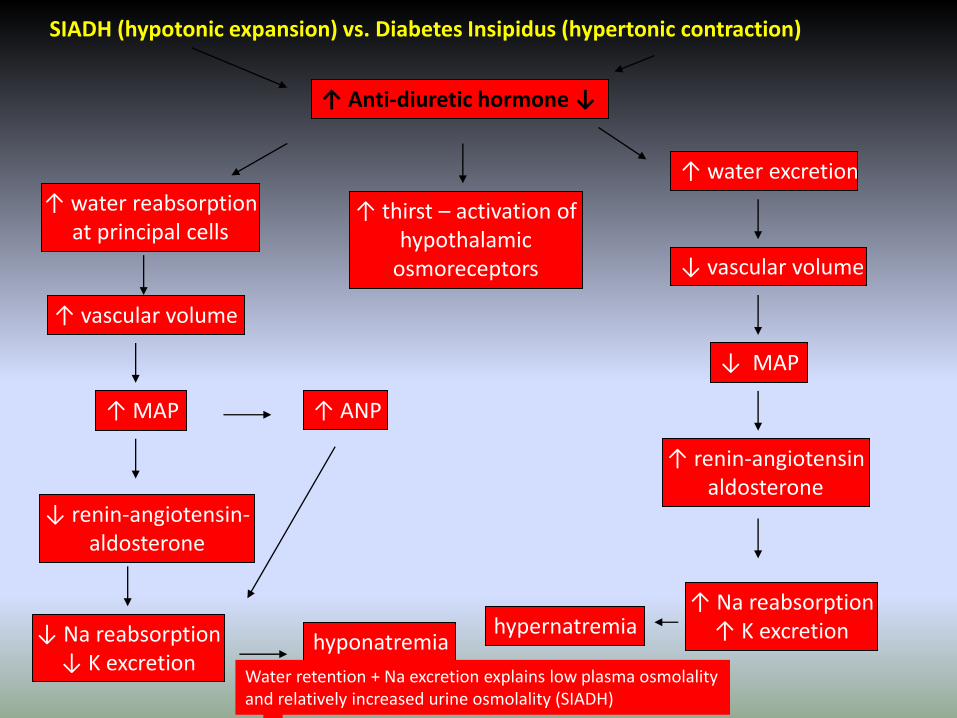
SIADH (hypotonic expansion) vs. Diabetes Insipidus (hypertonic contraction)
↑ Anti-diuretic hormone ↓
↑ thirst – activation ofhypothalamic
osmoreceptors
↓ Na reabsorption↓ K excretion
↓ renin-angiotensin-aldosterone
↑ MAP
↑ water reabsorptionat principal cells
↑ vascular volume
↑ water excretion
↓ MAP
↓ vascular volume
hyponatremia
Water retention + Na excretion explains low plasma osmolalityand relatively increased urine osmolality (SIADH)
↑ ANP
↑ renin-angiotensinaldosterone
↑ Na reabsorption↑ K excretionhypernatremia
Global Critical Carehttps://www.facebook.com/groups/1451610115129555/#!/groups/145161011512
9555/ Wellcome in our new group ..... Dr.SAMIR EL ANSARY

Related Documents











