EKG ROUNDS Bundle Branch Blocks 07. 04. 2005 Nadim Lalani

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
EKG ROUNDSBundle Branch Blocks
07. 04. 2005
Nadim Lalani

OUTLINE
• RBBB• LBBB• HEMiBLOCKS/ FaSCicULAR BLOCKS

Case
• A 13-year-old male.presents with a history of Syncpoe:
• What else do you want to know on hx?


Brugada Syndrome: • Described in 1992:
• Syndrome consisting of syncopal episodes and/or sudden death in patients with a structurally normal heart.
• Characteristic ECG with a pattern of right bundle branch block with an ST segment elevation in leads V1 to V3 was
• In 1998 recognised poor prognosis of patients with the syndrome not receiving an implantable defibrillator.

Brugada Syndrome:
• Epid:incidence of 0.05% to 0.6%. Mostly SE Asian / Japanan autosomal dominant mode of transmission.
• Who?: Adults 30-40 (first case reports were kids)
• Related to defect of SCN5a Fast sodium channel predisposing pt to re-entry circuit.
Brugada Syndrome: Clinical manifestations
• The complete syndrome is characterised by episodes of rapid polymorphic VT in patients. Resulting in syncopal attacks.
• When the episodes are sustained, cardiac arrest and eventually sudden death occur.
• There exist asymptomatic individuals in whom the atypical ECG is detected during routine examination.
• NB now known some variation in the EKG (three types of ST changes/ a-fib &c)

Brugada Syndrome:
• Diagnosis:• the typical ECG pattern and there is a history of aborted
sudden death or syncopes caused by a polymorphic VT. • There are also many patients with a normal ECG.
Syndrome only recognised a posteriori when the typical pattern appears in a follow-up ECG or after the administration of pro-arrythmics.
• Additional diagnostic problems are caused by the changes in the ECG induced by the autonomous system and by antiarrhythmic drugs.

Brugada Syndrome:
• Prognosis and treatment:
implantation of a cardioverter-defibrillator is mandatory in these patients.
Case report of a 23 yold patient being managed on amiodarone until implantation

Case
• Mrs M. 39 yo female had a pulmonary artery prosthesis and ASD repair 3 weeks ago. Helathy otherwise . On Lipitor. Presents with migratory arthralgias/myalgias.
• EKG Diagnosis?• Axis?

RBBB, axis 0-30 deg
RBBB
• Three phases:Septal depolarisation.Left ventricular depolarization. Delayed stimulation of the right
ventricle.

RBBB
septal depolarization produces a small septal r wave in V1 and a small septal q wave in V6
depolarization of LV produces an S in V1 and an R in V6
delayed right ventricular depolarization produces a wide R wave in V1 and a wide S wave in V6

RBBB Summary
• Right Leads ( V1 eg) show an rSR’ complex with a wide R wave.
• Occasionally, however, the S wave never quite makes its way below the baseline. Consequently, the complex in lead V1 has the appearance of a large notched R wave (“rabbit ears”)
• Left Leads (I,V6) show a qRS pattern with a wide S wave.

Case 2
• Mr R . 55 yo admited to FMC after head-on MVC in which he sustained Multiple rib #s,# L Hip and # L ulna. 2 days post-admit develops acute SOB with sat 80%.
• EKG Diagnosis?• Axis?• Comment on T waves?
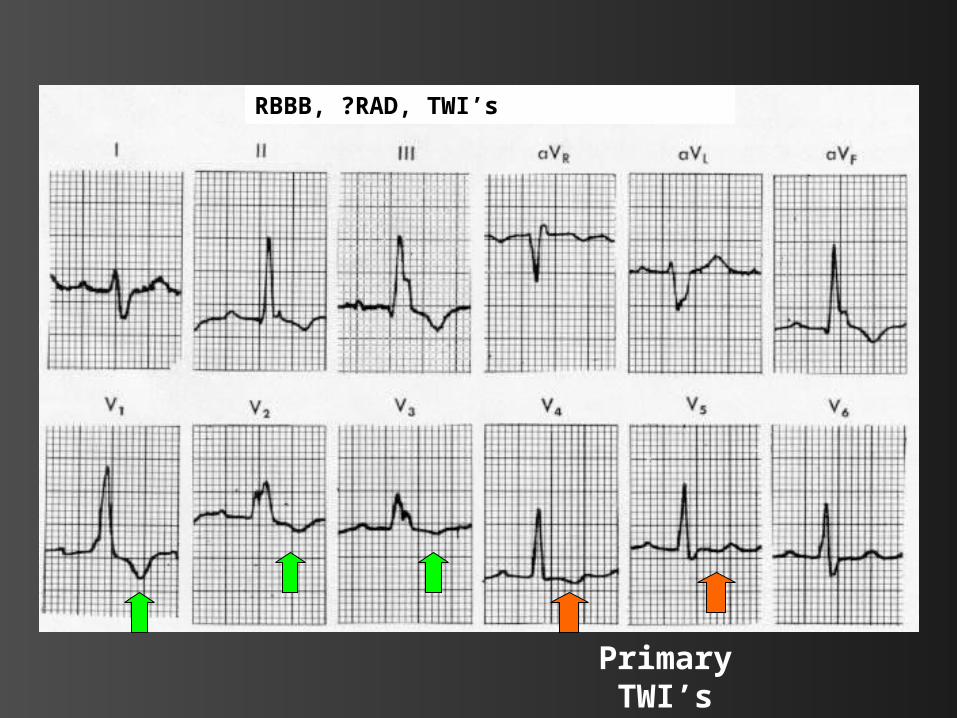
RBBB, ?RAD, TWI’s
Primary TWI’s

ST changes
• TWI’s in the right chest leads are a characteristic finding with RBBB.
• These inversions are referred to as secondary changes because they reflect just the delay in ventricular stimulation.
• By contrast, TWI’s in V5,V6 are primary T wave abnormalities reflect an actual change in repolarization (ie ischemia &c.)

Case 3
• 80 yo guy with HTN. Presents with this EKG:

RBBB, Axis apprx 30-90deg, Atrial Flutter

Sometimes can be Rate Dependent

COMPLETE AND INCOMPLETE RBBB
• Depends on the width of the QRS complex:
Complete RBBB is defined by a QRS that is 0.12 second or more with an rSR in lead V1 and a qRS in lead V6.
Incomplete RBBB shows the same QRS patterns, but its duration is between 0.1 and 0.12 second


Case 4:
• 77 yo M with HTN, and known CAD:

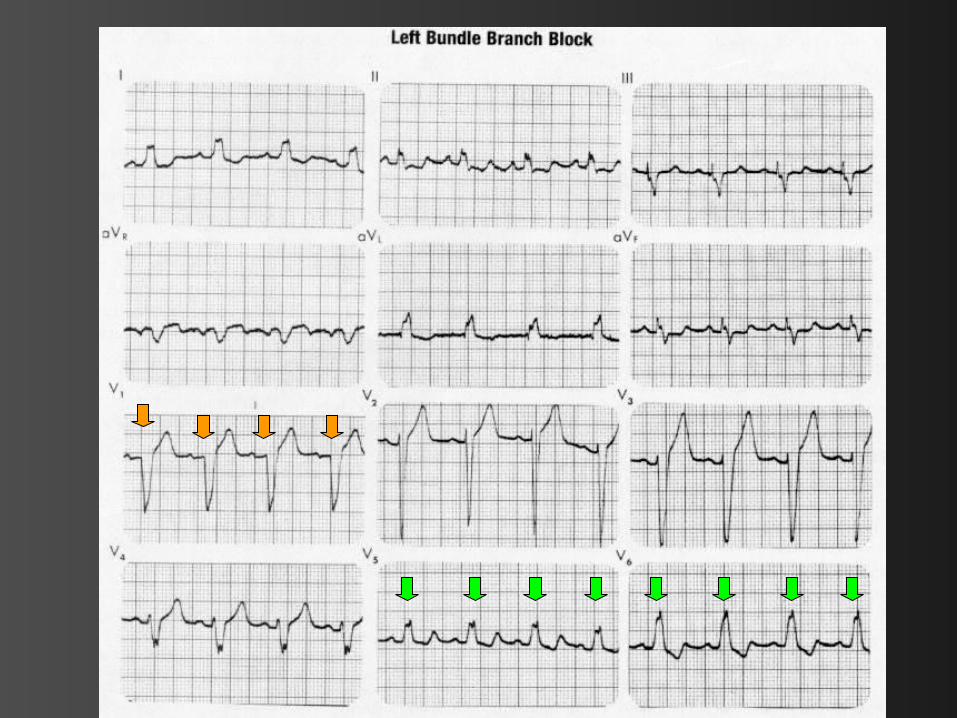
LBBB

Left Bundle Branch Block
• With LBBB the septum depolarizes from right to left .Therefore the EKG loses the normal septal r wave in lead V1 and the normal septal q wave in lead V6.
• Left ventricular depolarization is prolonged, yielding a wide QRS.
• Lead V6 you see a wide, entirely positive (R) wave.
• In the right chest leads (e.g., V1 ) you see a negative QRS (QS) complex.

Lose septal r in V1
And septal q in V6
Wide QS (sometimes rS) in V1
Wide R in Left Leads

• Congenital septal lesions, CAD, anterior MI (occlusion of proximal LAD), pulmonary
hypertension, normal variant in 0.2% adults

Summary RBBB vs LBBB:

r
S
R’
q
R
S
QS
R

Fascicular Blocks (Hemiblocks)
• The RBB is a single pathway consisting of just one main fascicle or bundle.
• In contrast the LBB has an anterior fascicle and a posterior fascicle.

The “Trifascicular Highway”

EKG Changes:
• Hemiblock (unlike a full LBBB or RBBB) does not widen the QRS complex.
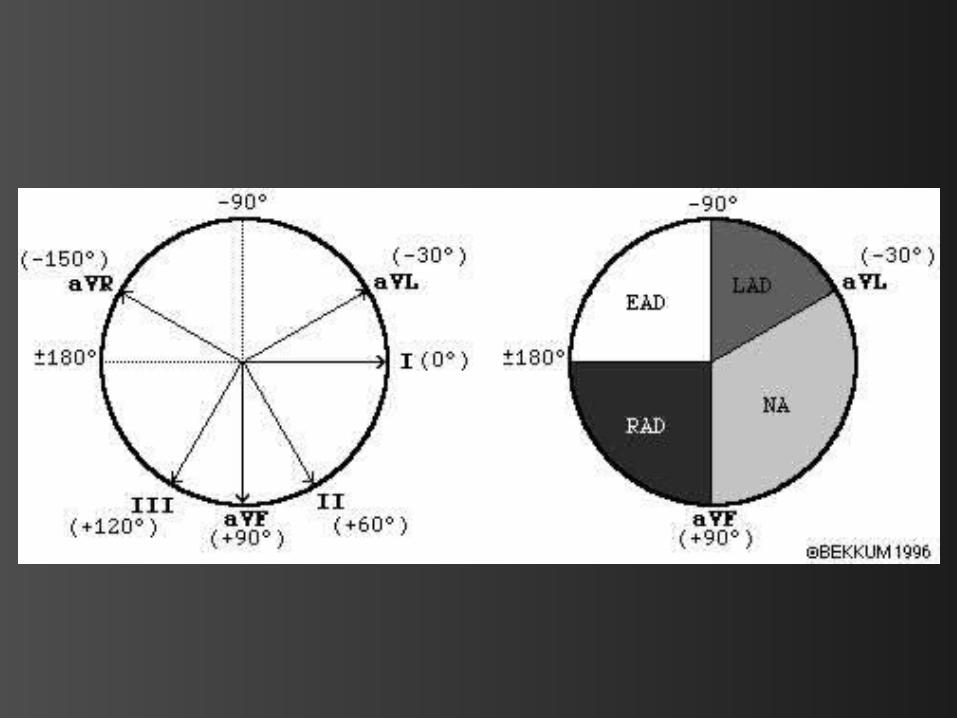
• Main effect is a change in the QRS axis: Left anterior fascicular block results in
marked left axis deviation (-30° or more) Left posterior fascicular block produces
marked right axis deviation (+120° or more).
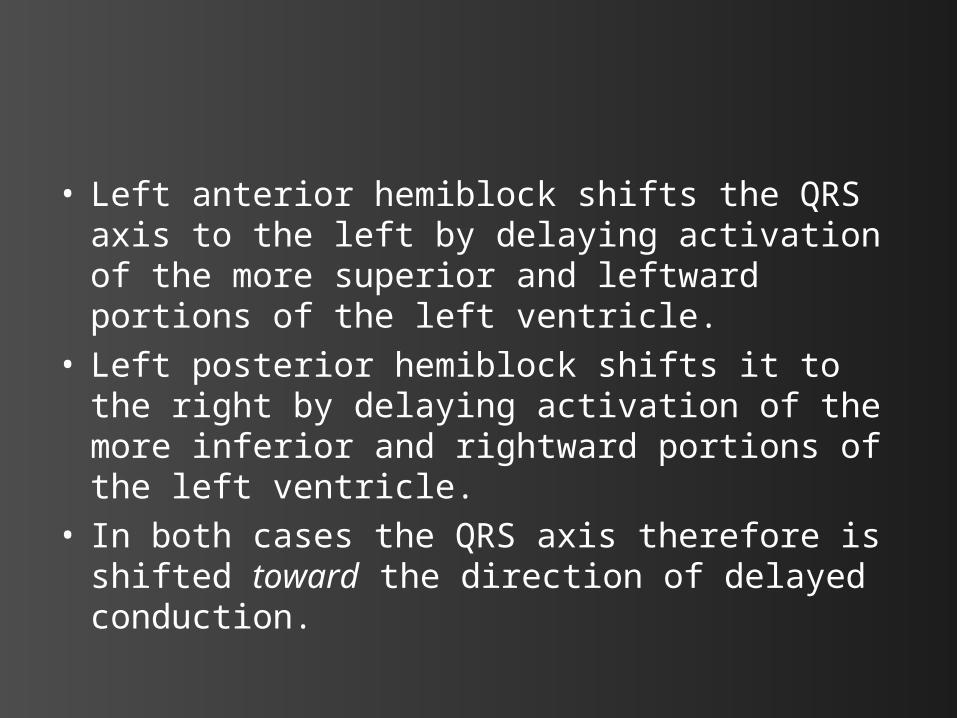
• Left anterior hemiblock shifts the QRS axis to the left by delaying activation of the more superior and leftward portions of the left ventricle.
• Left posterior hemiblock shifts it to the right by delaying activation of the more inferior and rightward portions of the left ventricle.
• In both cases the QRS axis therefore is shifted toward the direction of delayed conduction.

Axis?
Between -30 and -90 deg LAD

Axis?RAD

Case
• 67 yo M Obese, Hx CHF. Presents with SOB:
• EKG Dx?• Is he having an MI?

LBBB and acute MI

Sgarbossa et. al. :
• 131 patients from GUSTO-I trial who had LBBB with MI. Matched with controls. Came up with following criteria:
ST-segment elevation . 1 mm concordant with QRS complex – 73 % sens and 92 % spec for acute MI.
ST-segment depression . 1 mm in lead V1, V2 or V3 – highly specific (96%) but less sensitive (25%) for MI
ST-segment elevation . 5 mm discordant with QRS complex – 31 % sens, 92 % spec.

ST ↓Concordant
ST ↑
Discordant
ST ↑ ST ↓

Shlipak MG, Lyons WL, Go AS, et al. Should the electrocardiogram be used to guide therapy for patients with left bundle branch block and suspected myocardial infarction?
JAMA 1999;281:714–19.:
• Reviewed patients presenting with LBBB and an acute cardiopulmonary history and assessed the usefulness of the Sgarbossa criteria.
• Criteria had a sensitivity of 10% and a specificity of 100%.
• Most (90%) patients with AMI will not meet the criteria.
• Support thrombolysing all patients (except those with contraindications) who have a history suggestive of AMI and LBBB.

Practice Time:
Case A
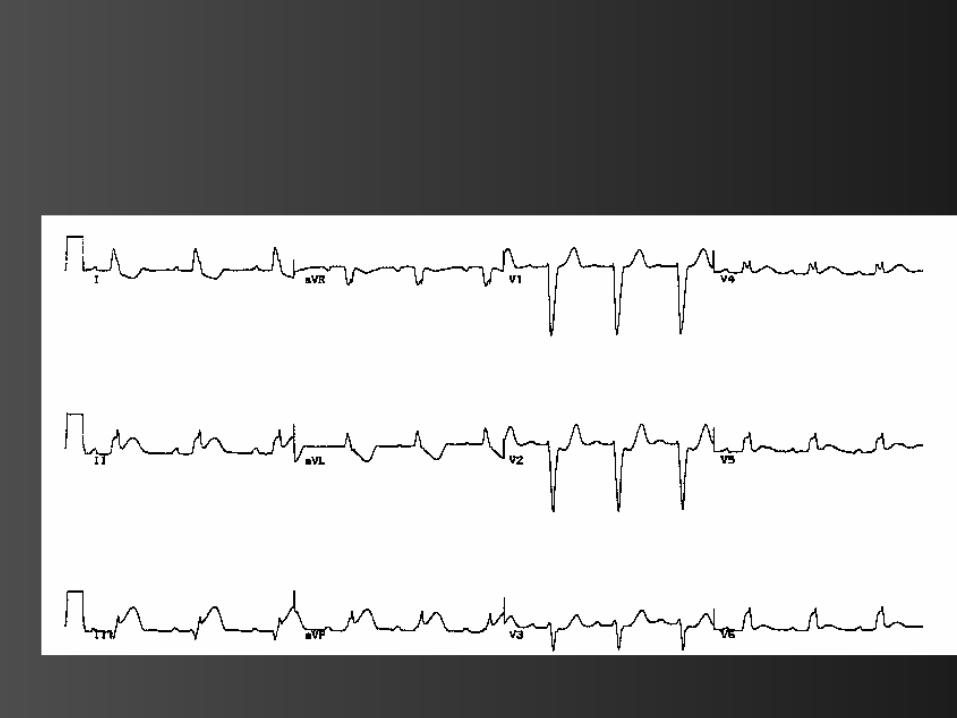
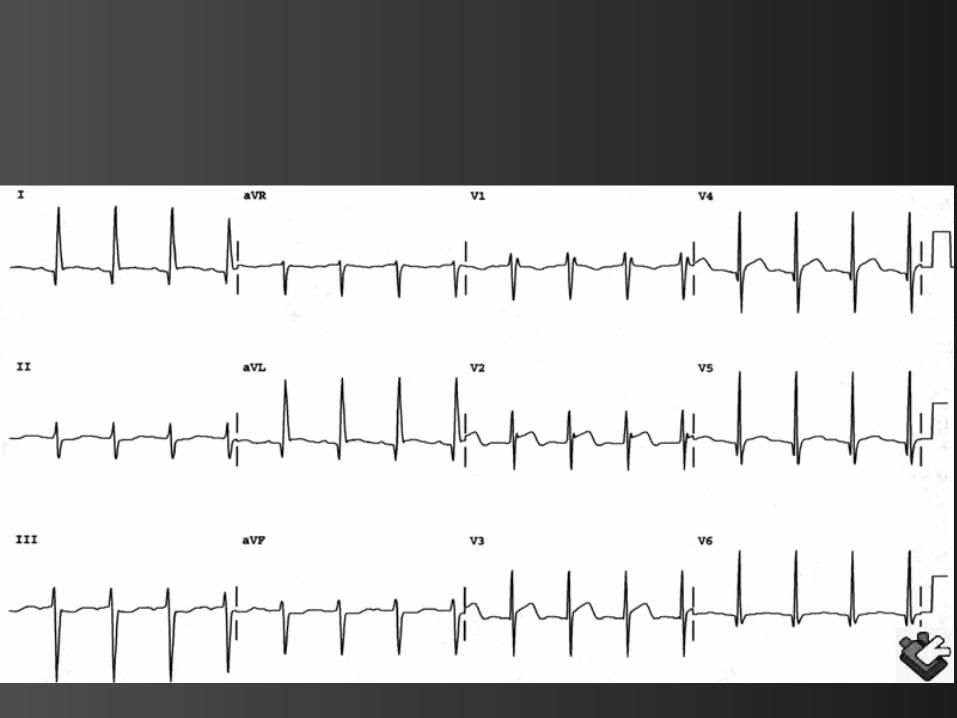
• 65 yo M smoker with DM presents with 4 hours RSCP:
• EKG Diagnosis?• Axis?

Case BRBBB, ? Primary TWI’s V4,V5

Case CLBBB
Case D

LBBB, ? LAD

Case ERBBB

Case FLBBB
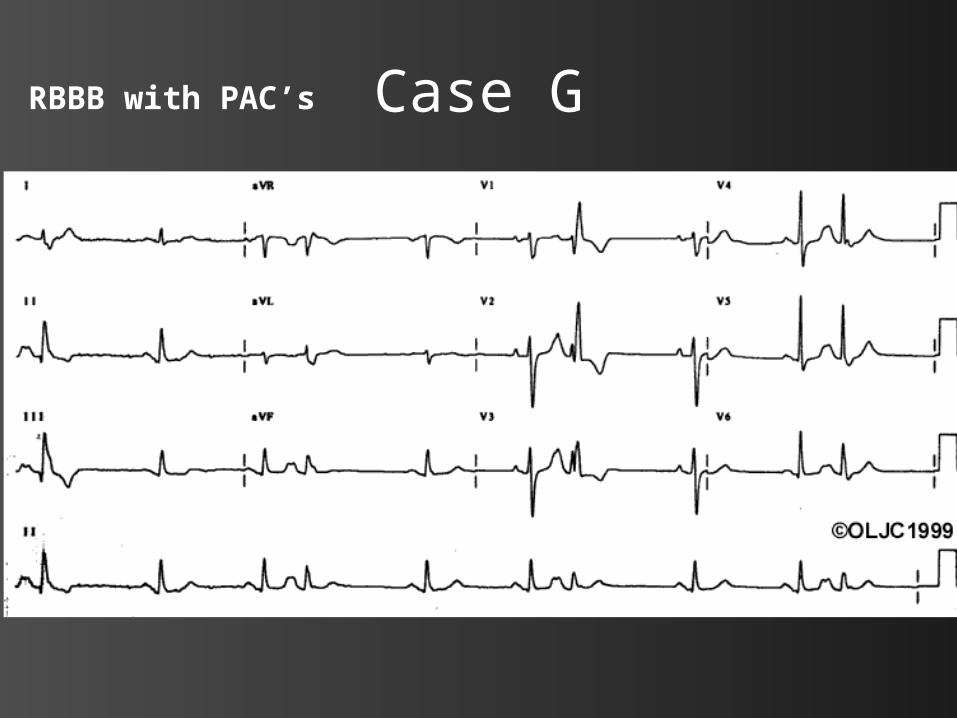
Case GRBBB with PAC’s

Case HBifascular: RBBB with LAFB

Case IRBBB with Primary TWI’s

Case J
RAD

Case KRAD ?LPFB

References
• Goldberger: Clinical Electrocardiography: A Simplified Approach, 6th ed.,1999 Mosby, Inc.
• Brugada P, Brugada J: Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol 1992 Nov 15; 20(6): 1391-6
Related Documents