EHRs & Care Management: Mandates & Opportunities MICHAEL NEWELL, RN, MSN PRESIDENT LIFESPAN CARE MANAGEMENT Personal Healthcare Concierge Service www.LifeSpanCM.com Presented to Case Management Department Children’s Hospital of Philadelphia

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EHRs &
Care Management:
Mandates & Opportunities
MICHAEL NEWELL, RN, MSN
PRESIDENT
LIFESPAN CARE MANAGEMENTPersonal Healthcare Concierge Service www.LifeSpanCM.com
Presented to Case Management Department
Children’s Hospital of Philadelphia
Objectives•Describe the critical components of the
Electronic Heath Record Evolution
•Explain how “Meaningful Use” will
enhance the standard of medical care
as Electronic health records are
implemented
•Describe How Case Managers can use
these innovations to improve transitions
of care and avoid adverse events.
Personal Healthcare Concierge Service www.LifeSpanCM.com
© Copyright 2010. LifeSpan Care Management, LLC. All rights reserved.

The First
Electronic Medical Record

Willem Einthoven first demonstrated electrical heart
conduction using an electrocardiograph in 1906, winning
the Nobel Prize for this invention in 1924


What does the data mean?

68%
16% 16%

Why
Who
What
When
Where
How








Who
• Office of the National Coordinator (ONC)
for Health Information Technology
• Health Information Technology for
Economic and Clinical Health Act
(HITECH Act) of 2009
• $20B Funded by the American Recovery
and Reinvestment Act of 2009 (ARRA)

What + Where
• Primary Care Providers taking Medicare
offered $44,000 each to purchase and use
an EMR
• Eligible providers for Medicaid may apply
for up to $63,750 per clinician
• A base payment of $2 million for eligible
hospitals and critical access hospitals,
depending on certain criteria
• All must show “Meaningful Use”

WhenMeaningful Use Stages

Clinical Information System(s)
Business Process
System(s)
= EMR +PHR
=EHR
+
Clinical
Decision Support
Outcomes
Care coordination
Client satisfaction
Errors
Costs

MU
• Updates to face sheet
• New diagnoses get free text box to enable
details
• Once appropriate details about the diagnosis
or problem are recorded, such as quality,
duration, timing, and complicating factors,
the provider clicks a box marked “add to the
problem list.”

MU-2
• Medication reconciliation
• Summary of encounter provided to patient at
time of discharge, including:
– Chief complaint/reason for visit
– Findings/diagnosis
– Plan of Care
– Meds, diagnostics, treatments ordered
• Notification of care transitions to pertinent
providers
• Summary of care at transition points

Population Health
Management
Defined as:
• Intensive care management for
individuals at the highest level of risk
• Personal health management for those at
lower levels of predicted health risk

H.I.E.

HIE solutions
• Achieving health goals through health
information exchange
• Improving long-term and post-acute care
transitions
• Consumer-mediated information exchange
• Enabling enhanced query for patient care
• Fostering distributed population-level
analytics

HIE To-Do List
• Create and implement up-to-date privacy
and security requirements for HIE
• Coordinate with Medicaid and state public
health programs to establish an integrated
approach
• Monitor and track meaningful use HIE
capabilities in their state

Summary Of Care Record
• Patient name.
• Referring or transitioning provider's name and office
contact information (EP only).
• Procedures.
• Encounter diagnosis
• Immunizations.
• Laboratory test results.
• Vital signs (height, weight, blood pressure, BMI).
• Smoking status.
• Functional status, including activities of daily living,
cognitive and disability status

SoC list…
• Demographic information (preferred language, sex, race,
ethnicity, date of birth).
• Care plan field, including goals and instructions.
• Care team including the primary care provider of record
and any additional known care team members beyond
the referring or transitioning provider and the receiving
provider.
• Reason for referral
• Current problem list (EPs may also include historical
problems at their discretion).
• Current medication list, and
• Current medication allergy list.

SoC List…
• Problem List – At a minimum a list of current, active and
historical diagnoses. The EP is not limited to just include
diagnoses on the problem list.
• Active/current medication list – A list of medications
that a given patient is currently taking.
• Active/current medication allergy list – A list of
medications to which a given patient has known allergies
& any exaggerated immune response or reaction to
substances that are generally not harmful.
• Care Plan …

PoCThe structure used to define the management
actions for the various conditions, problems, or
issues. A care plan must include at a minimum the
following components:
• problem (the focus of the care plan),
• goal (the target outcome) and any
• instructions that the provider has given to the
patient.
A goal is a defined target or measure to be
achieved in the process of patient care (an
expected outcome).

Functional Independence
Measures (FIM--WeeFIM)
Self-Care
• Grooming
• Bathing
• Dressing Upper
• Eating
• Dressing Lower
• Toileting
– Sphincter Control
• Bladder Management
• Bowel Management
Motor– Transfers
• Chair, Wheelchair
• Toilet
• Tub, Shower
– Locomotion
• Walk, Wheelchair
• Stairs
COGNITIVE
• Comprehension
• Expression
• Social Interaction
• Problem Solving
• Memory

FIM Decision Tree
7: Complete Independence Client completes activitywithout help, assistive device,in a reasonable time andwithout safety concerns
6: Modified Independence Needs more time or assistdevice
5: Supervision Needs set-up, cueing or contactguarding
4: Minimal Assistance Completes 75-100% of task
3: Moderate Assist Completes 50-75% of task
2: Maximal Assist Completes 25-50% of task
1: Total Assist Completes little or none by self

WeeFIM Polar Graph


MOS SF-36
• Self/phone/interview administered in 10 minutes
• Uses Likert scale, acute, chronic & disease-
specific versions
• Correlates .70 to .80 with actual health exams
• Discriminates stages, severity of disease and
moderate size treatment effects

SF-36 Health Domains
• General health
perceptions
• Physical functioning
• Role limitations due to
physical and
emotional problems
• Social functioning
• Pain
• Emotional well-being
• Vitality
• Changes in health
HSQ adds 3 question
depression screener

Working with HSQ Data
0
20
40
60
80
100
Phys
Func
Role
/Phy
sPai
n
Mntl
Hlth
Role
-Em
ot
Soc
FxVita
l
Gen
Hlth
Baseline 2nd Visit 1st F/U Adj Norms

Clinical Quality Measures
• Appropriate testing for children with Pharyngitis
• Weight assessment & counseling for nutrition & physical
activity for children & adolescents
• Use of appropriate medication for Asthma
• Childhood immunization status
• Preventive care & screening: influenza immunization
• HA1c test for pediatric patients
• Appropriate Tx for children with URIs
• ADHD: f/u care for children prescribed ADHD meds
• Children who had dental decay or cavities
• +HIV testing f/u

Goals for the
U.S. Healthcare
SystemAs per the Institute of Medicine
of the
National Academy of Science
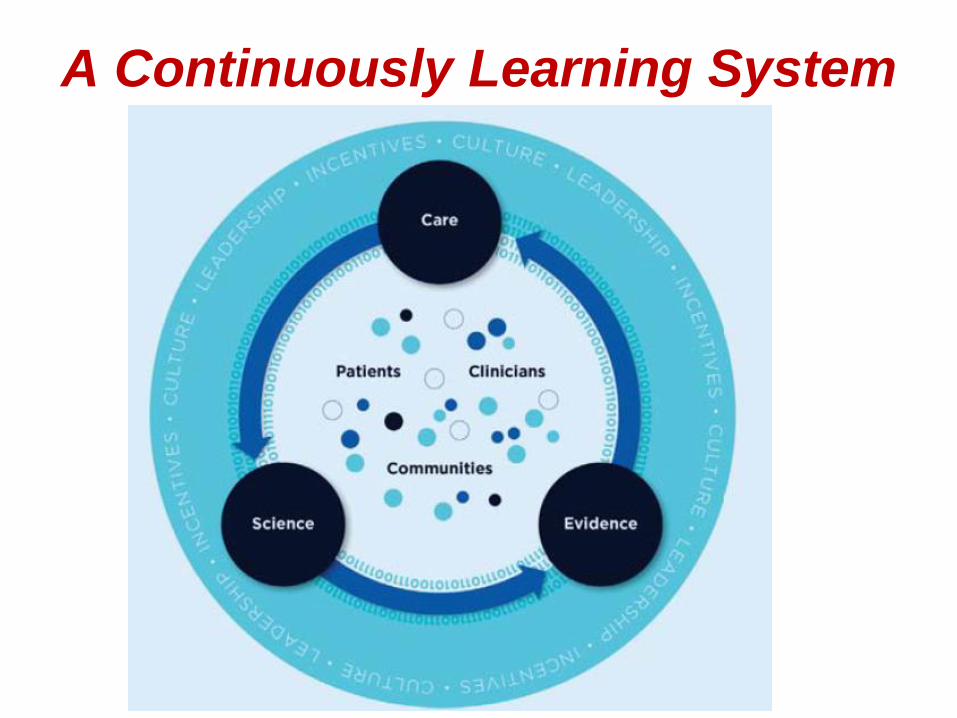
A Continuously Learning System


References:
Best Care at Lower Cost: The Path to Continuously Learning
Health Care in America (2102) Mark Smith, Robert Saunders, Leigh
Stuckhardt, J. Michael McGinnis, Editors; Committee on the Learning
Health Care System in America; Institute of Medicine, National
Academies Press, Washington DC.
Blumenthal, D., Tavenner, M. (2010). The “Meaningful Use” Regulation
for Electronic Health Records. The New England Journal of Medicine,
363, 501-504.
Halamka, John D. (2009). Making Smart Investments in Health
Information Technology: Core Principles. Health Affairs. 385-289.
DOI: 10.1377/hlthaff.28.2.w385
McBride, S., Delaney, J. Tietze, M. (2012). Health Information
Technology and Nursing. American Journal of Nursing. 112;8. 36-42.
DOI: 10.1097/01.NAJ.0000418095.31317.1b
http://www.cms.gov/regulations-and-
guidance/legislation/ehrincentiveprograms/stage_2.html
Related Documents


![New Years Poster [Peds] 8 - FFF Enterprises · Title: New Years Poster [Peds] 8.5x11 Subject: New Years Poster [Peds] 8.5x11 Keywords: New Years Poster [Peds] 8.5x11 Created Date:](https://static.cupdf.com/doc/110x72/5fd6db4c8a000945d6684aca/new-years-poster-peds-8-fff-title-new-years-poster-peds-85x11-subject-new.jpg)








