I “EFFICACY OF LASHUNA RASAYANA IN MANIBANDHA MARMABHIGHATA” By Dr. Manasa Rao B.A.M.S Dissertation submitted to the Rajiv Gandhi University of Health Sciences Karnataka, Bengaluru In partial fulfillment of the requirement for the degree of “AYURVEDA VACHASPATI” DOCTOR OF MEDICINE (Ayu) In KAYACHIKITSA GUIDE DR. G. SHRINIVASA. ACHARYA M.D. (AYU) Professor and HOD Department of Post Graduate Studies in Kayachikitsa and Manasaroga Shri Dharmasthala Manjunatheshwara College of Ayurveda, Udupi. DEPARTMENT OF POST GRADUATE STUDIES IN KAYACHIKITSA SHRI DHARMASTHALA MANJUNATHESHWARA COLLEGE OF AYURVEDA, KUTHPADY UDUPI 2017-2018

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
I
“EFFICACY OF LASHUNA RASAYANA IN MANIBANDHA
MARMABHIGHATA”
By
Dr. Manasa Rao B.A.M.S
Dissertation submitted to the Rajiv Gandhi University of Health Sciences
Karnataka, Bengaluru
In partial fulfillment of the requirement for the degree of
“AYURVEDA VACHASPATI”
DOCTOR OF MEDICINE (Ayu)
In
KAYACHIKITSA
GUIDE
DR. G. SHRINIVASA. ACHARYA M.D. (AYU)
Professor and HOD
Department of Post Graduate Studies in Kayachikitsa and Manasaroga
Shri Dharmasthala Manjunatheshwara College of Ayurveda, Udupi.
DEPARTMENT OF POST GRADUATE STUDIES IN KAYACHIKITSA
SHRI DHARMASTHALA MANJUNATHESHWARA COLLEGE OF
AYURVEDA, KUTHPADY UDUPI
2017-2018
Scanned by CamScanner
Scanned by CamScanner
Scanned by CamScanner
I
ABBREVIATIONS
A.H. - ASHTANGA HRIDAYAM
A.S - ASHTANGA SANGRAHA
A.T. - AFTER TREATMENT
B.P. - BHAVAPRAKASHA
B.R. - BHAISHAJYA RATNAVALI
BS.R. - BASAVARAJEEYAM
B.T. - BEFORE TREATMENT
C.S. - CHARAKA SAMHITA
M.N. - MADHAVA NIDANA
S.S. - SUSHRUTA SAMHITA
Y.R. - YOGARATNAKARA
XIII
LIST OF TABLES
S.No Tables Page No.
1. Samprapti ghataka of manibandha marmabhighata. 32
2. List of pathya of vatavyadhi / manibandha marmabhighata 41-43
3. List of apathya of vatavyadhi / manibandha marmabhighata 44
4. Showing responses 51
5. Distribution of the 15 patients according to their Age / gender 54
6. Distribution of the15 patients according to their Religion /
Marital status 55
7. Distribution of the15 patients according to their Profession /
Economic status 56
8. Diet and sleep of 15 patients 57
9. Day sleep and habit identified in 15patients 58
10. Family history of 15 patients 59
11. Distribution of 15 patients according to the initial recording of
Bodyweight and BMI 60
12. Distribution of 15 patients according to their prakriti 61
13. Distribution of 15 patients according to their Sara 62
14. Distribution of 15patients according to their Satva 63
15. Distribution of 12 patients according to their
Abhyavaranashakti 64
16. Distribution of 15 patients according to their Mode of onset 65
17. symptom supta of 15 patients 66
18. Effect of Lashuna rasayana on symptom severity of the illness 68
19. Effect of Lashuna rasayana on functional disability status 69
20. Effect of Lashuna rasayana on VAS pain score 70
21. Effect of Lashuna rasayana on VAS numbness score 71
22. Effect of Lashuna rasayana on hand grip strength 72
23. The overall effect of the Lashuna rasayana 73
I
LIST OF GRAPHS &FIGURES
Sl.No Figures & Graphs Page. No
1. Distribution according to Age 54
2. Distribution according to Religion 54
3. Distribution according to Religion 55
4. Distribution as per Marital status 55
5. Distribution according to Profession 56
6. Distribution according to Socio economic status 56
7. Diet of 15 patients 57
8. Nature of sleep of 15patients 57
9. Day sleep identified in 15 patients 58
10. History of addiction in 15 patients 58
11. Family history in 15 patients 59
12. Distribution according to Bodyweight 60
13. BMI of 15 patients 60
14. Distribution of 15 patients according to their prakriti 61
15. Distribution according to Sara 62
16. Distribution according to Samhanana 62
17. Distribution according to Satva 63
18. Distribution as per Vyayama Shakti 63
19. Distribution as per Abhyavaranashakti 64
20. Distribution as per Jaranashakti 64
21. Distribution According to Mode of Onset 65
22. Symptom ruk in 15 patients 65
23. Symptom supta of 15 patients 66
24. Effect of Lashuna rasayana on symptom severity of the illness 68
25. Effect of Lashuna rasayana on functional disability status 69
26. Effect of Lashuna rasayana on VAS pain score 7
27. Effect of Lashuna rasayana on VAS numbness score 71
28. Effect of Lashuna rasayana on hand grip strength 72
29. The overall effect of the lashuna rasayana 73
II
30. Lashuna 118
31. Lashuna Capsules 118
32. Lashuna Rasayana 118
33. Eranda Taila 118
34. Visual Anologue Scale 119
35. Hand Dynamometer 119
I
ABSTRACT
“EFFICACY OF LASHUNA RASAYANA IN MANIBANDHA
MARMABHIGHATA”
Background
Manibandha marmabhighta is a multifactorial disease caused by
santarpana nidana as well as by physical strain .Hence it demands a drug
which pacifies vata dosha as well as clears margavarna where Lashuna
proves to be best. Hence this study is carried out.
Objectives
To assess Efficacy of a Lashuna rasayana on disease severity in patients
suffering from Manibandha marmabhighata / Carpal tunnel syndrome. (2) Effect on
functional disability in patients of Manibandha marmabhighata / Carpal tunnel
syndrome treated with Lashuna rasayana.
Method-
Design
Study type – Interventional; Allocation – Non randomized; Endpoint
classification - Efficacy study; Intervention Model - Single Group Assignment;
Masking - Open Label; Primary Purpose – Treatment.
II
Intervention
Day 1 - Oral administration of eranda taila in empty stomach, in a dose of 20
ml in the morning along with 100 ml of warm water as after drink;
Day 2 to 16 - Oral administration of Lashuna rasayana in a dose of 12 g in
empty stomach half an hour before breakfast along with 100 ml of milk as after drink;
Day 17 - Oral administration of eranda taila in empty stomach, in a dose of 20
ml in the morning along with 100 ml of warm water as after drink.
Results-
There was significant reduction in all the primary & secondary outcome
measures like symptom severity, functional status, VAS for pain, VAS for numbness
and hand grip. All these improvements when analyzed by the statistical tests of
significance proved highly significant results i.e. p <0.001.
INTERPRETATION & CONCLUSION: Lashuna rasayana is effective in both
clearing the co morbidity of margavarana as well as pacification of vitiated vata dosha
thus significantly reducing the signs and symptoms of Manibandha marmabhighata /
Carpal tunnel syndrome.
KEYWORDS: Manibandha marmabhighata, Lashuna rasayana, Carpal tunnel
syndrome
Introduction
Efficacy of lashuna rasayana in manibandha marmabhighata Page 1
INTRODUCTION
“EFFICACY OF LASHUNA RASAYANA IN MANIBANDHA
MARMABHIGHATA”
Vata vyadhi is considered as most virulent among the tridosha. Among the
diseases caused by vitiation of vata dosha, samanya & nanatmaja vyadhi presents with
distinct features. Literature quotes 80 types of nanatmaja vata vyadhi that is specified
as aavishkritatama vata vyadhi1. The description of some of these diseases is vivid in
the literature and elaboration of some is restricted to guidelines. In general, vata dosha
is diagnosed based on symptoms of aggravation of vata dosha and location of
affliction. Nakha Bheda, Paada Shola, Paada Supthi are just the examples.
Kuntata2 is a disorder characterised by the paralysis related to the activities of
hand. Scanning of literature explores the better explanation of the condition with due
consideration of abhighata nidana in Manibandha as Rujakara marma3.
Etiological factors of vata vyadhi such as strain caused due to exposure of
vyayama, abnormal positioning during different activities is worth considering. These
etiological factors have direct bearing on joints. To be more precise the excessive and
abnormal activities of involving the hand may affect the Manibandha marma.
Affection of Manibandha marma is the key pathology as per the understanding of
marmabhighata.
The Manibandha marmabhighata can happen for two reasons, they are the
internal factor & external factor4. External by the way of different activities related
to bahya abhighata involving the Manibandha. In contrast to santarpana nidana
causing excessive kapha & medas can lead to avarana vata vyadhi and can involve the
Introduction
Efficacy of lashuna rasayana in manibandha marmabhighata Page 2
Manibandha marma leading to margavaranajanya Manibandha marmabhighata similar
to the samprapti of urustamabha5.
Here the marga refers to vatavaha srotas. Manibandha marmabhighata is
caused either external factors or internal factors like santarpana nidana resulting in
vata vyadhi. Literature affirms the role of marmabhighata in causation of vatavyadhi.
Manibandha marmabhighata when it happens for above said reasons result in
manifestation of supta, ruja, vastushukairavakirna, shosha, parvashopha, kuntata.
These symptoms, comprising of Manibhandha marmabhighata; parallels with
symptom of carpal tunnel syndrome. The symptoms of Manibhandha marmabhighata
include suptata (paresthesia), ruja (pain) and kuntata (paralysis of the hand leading to
functional disability) .Thus these symptoms match with that Carpal tunnel syndrome.
Carpal tunnel syndrome may be caused due to obesity, trauma, pregnancy and
inflammation etc. These etiological factor either belonging to the category of
santarpana nidana or injury to wrist by physical activities. The pathology of
margavarana / abhighata in manibhandha is parallel to median nerve entrapment in
carpel tunnel. Surgical intervention in this syndrome will give good relief, whereas
conservative management have failed to overcome the disease as it gives just the
temporary relief. This syndrome is common in the working population related to the
increased use of activities of hand. Complications will leads to hindrance of routine
activity. A survey study revealed that 53 per 10,000 working adults have evidence of
Carpel Tunnel Syndrome6. These observations add to the seriousness of this
Manibandha marmabhighata or Carpel tunnel syndrome.
Manibandha marmabhighata and the resulting vatavyadhi is treated according to
the treatment of vatavyadhi by snehana, svedana, brimhana and rasayana. . Balanced
approach rectifying the kapha and medas and simultaneously normalizing the
Introduction
Efficacy of lashuna rasayana in manibandha marmabhighata Page 3
functions of the vatadosha is the sheet anchor of treating Manibandha marmabhighata
leading to kuntata. Needless to say Rasayana cikitsa has got an edge over any other
conservative management.
Also Lashuna rasayana is effective in both clearing the co morbidity of
margavarana as well as pacification of vitiated vata dosha thus proving its superiority
in the management of Manibandha marmabhighata.
Reviewing the clinical trials carried out in relation to the efficacy of Lashuna
rasayana carried out in different research institutions unravels the following truths.
In an Open idealistic clinical trial evaluating the effect of Lashuna rasayana in
Gradrasi / sciatica was conducted on 23 patients , where result showed patients had
90.58% relief from Stambha, 87.28% relief from Ruk,85.36% relief from Toda, 85.36
from Spandana, 100% relief from Aruchi, 147% relief from pain, 63% improvement
in neurological deficits, 50% improvement in functional ability, 68.61% relief from
functional disability, 117% improvement in active SLR test, 117% improvement in
passive SLR test, 38.81% improvement in walking for a distance of 30 feet, 18%
improvement in taking 10 sit ups, 32% relief in climbing 10 steps, 31.38%
improvement in floor hand distance.
In another Open Randomized Comparative Clinical Study on Lashuna
Rasayana and vaitarana Basti in gridhrasi on 40 patients was done. It was found that
75 % of patients had major improvement, 20 % had moderate improvement, 5 % had
mild improvement and none of the patients had the symptoms unchanged.
From the fore going it is clear that Manibandha marmabhighata is a multi-
factorial disease. Physical strain at the Manibandha marma or the santarpana nidana
leading to accumulation of kapha and medas at the Manibandha marma obstructing
the vatavaha srotas may precipitated the Manibandha marmabhighata and that mimics
Introduction
Efficacy of lashuna rasayana in manibandha marmabhighata Page 4
the clinical presentation of Carpal tunnel syndrome. Enough clinical study is carried
out on Lashuna rasayana on different diseases but no study is carried out on
Manibandha marmabhighata.
Pilot study has shown favorable response in patient suffering from
Manibandha marmabhighata treated with Lashuna rasayana. Hence this study is
intended to evaluate the therapeutic effect of Lashuna rasayana in patient suffering
from Manibandha marmabhighata / Carpel tunnel syndrome.
This dissertation consists of literary review drug review methods observation
results discussion and conclusion. Historical review, etiology, symptomatology,
diagnosis and treatment is the subject matter of chapter literary review. Details of the
Lashuna rasayana are given in the chapter of drug review. Complete details of the
design of the study are presented in the chapter entitled methods. The demographic
profile of the sample is elaborated in the observation chapter. The effect of treatment
with Lashuna rasayana with statistical analysis is recorded in the chapter of results.
Rationality of the treatment and the result obtained is discussed in the chapter of
discussion including mode of action. The conclusion obtained from this study is the
subject matter of the chapter conclusion.
Objectives
Efficacy of lashuna rasayana in manibandha marmabhighata Page 5
OBJECTIVES
Efficacy of Lashuna rasayana on disease severity in patients suffering from
Manibandha marmabhighata / Carpal tunnel syndrome.
Effect on functional disability in patients of Manibandha marmabhighata /
Carpal tunnel syndrome treated with Lashuna rasayana.
Historical Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 6
HISTORICAL REVIEW
Marma are the unique vital points in the body. Strong blow on these marma
can cause significant injury and may even prove fatal. Contrary to this a mild touch of
these vital points can cause healing. The whole practice of marma therapy is based on
this understanding. The knowledge of marma is essential for planning surgical
interventions. The seriousness of any trauma is judged by the involvement of marma.
The same marma knowledge is used in the martial arts to kill the opponent. Most
recently the same knowledge is utilized to treat certain diseases. To be clearer, the
knowledge of marma is traced back to Vedic literature and has progressed to the
present marma therapy practiced in the southern part of the India known by the name
Kalaripayattu. The full account of this history related to the marma and Manibandha
marma is elaborated below.
Vedic period (1500 BC)
The concept of marma is well documented in Vedic literature and mostly
related to the martial arts. From the citations in the Rig-Veda and others it is clear that
marma points in the body were well protected by wearing specific armors during the
wars. These amour was said to protect the vulnerable marma points in the body during
war injuries and thereby saving the life7. A citation in Rig-Veda says that
Vishwakarma sharpened the weapon Vajrayudha of lord Indra and by using this
weapon lord Indra attacked the marma point of the demon by name Vratra.8 Also in
Rig-Veda it is said that, best protection of the marma was achieved by chanting the
specific mantra (kavacha). Atharva Veda quotes the possibility of death due to injury
to the marma. The word kavacha is used referring the corselet or breast plate worn to
Historical Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 7
protect the marma during wars. It is worth mentioning about the surgical intervention
made by divine doctor’s Ashvini on Shayava at three locations of his body to make
him to move again9.
Also other than the weapons the fire was used as a great weapon to injure the
marma points during wars10
. Among the four sub veda, Dhanurveda deals with martial
arts. Much is discussed about the marma points in this literature.
Upanishad period:
Much information related to the anatomy of the marma is available in
Upanishad. The descriptions include description of vessels & blood circulation11
,
vascular injuries12
, Characteristics of sira and dhamani13
, anatomy and physiology of
hridaya14
, marma and kavacha15
, marma16
, dhamani17
. To be more specific elaboration
of marma is found in Garbhopanishad18
and Yogopanishad.
Epics period:
Citations of marma are found in Ramayana as well as Mahabharata. In a story
in Ramayana it is said that king Dasharatha shot an arrow accidentally on a marma
point of Shravana Kumara. He died due to this injury on his marma19
. Duryodhana
was said to have a vital marma point on his thigh and was revealed by lord Krishna to
Bheema during battle between Bheema and Duryodhana20
. Lord Krishna was shot
dead by a hunter Jara with an arrow injuring the marma point at his foot21
Historical Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 8
Samhita period:
Detailed description of the locations of marma, clinical illness when injured
and its management is detailed in the literatures of this period. Following details
substantiate the adequate description of marma in these literatures.
Charaka samhita (2nd century B.C):
In charaka samhita, the total number of marma in the body is accepted as 107.
Ample emphasis is given on three marma that include Shiras, hridaya and basti.
Exclusive chapters are allocated in the sutra sthana, chikitsa sthana and siddhi sthana.
The disease related these three marma locations with their treatment are discussed at
length. It is accepted that vata dosha predominated in the pathology of affliction of
marma and hence basti is regarded as best treatment in such situations. Also it is said
that injury to any marma can happen for internal and external causes22
. Vitiated dosha
afflicting the marma is accepted as internal cause of marma injury. External trauma is
regarded as external cause of injury of marma. It is crucial to note that vatavyadhi can
happen due to the injury to the internal marma. Also kapha and medas suppressing the
movement of vata leading the vatavyadhi is described as margavarana leading to
marma injury.
From the same concept to internal dosha causing the injury of the marma added with
margavarana due to kapha and medas; this present concept of Manibandha
marmabhighata is formulated.
Historical Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 9
Bhela Samhita
Harita Samhita
Sushruta samhita (2nd century AD):
Detailed description of 107 number of marma is described in the sushruta
samhita with the angle of surgical intervention. It is said that marma points should be
avoided during surgical intervention or utmost care should be taken lest the patient
may land in serious complications or lose his life. Injury to the marma and its clinical
implication is detailed at full length either is due to trauma or error in the surgical
intervention. Marma is defined as a vital point in the body structurally formed by the
combination of five structures of mamsa, sira ,snayu ,asthi sandhi and injury to this
may cause immediate death, late death, disability or severe pain. Marma is classified
differently on the basis of predominant composition of body elements, location in the
body, result of injury and also its size. The elaborate description of the treatment of
these marma is also given in the text23
.
Kashyapa samhita:
In the third chapter of sharira sthana along with the ten locations of prana the
major three marma are enlisted and named as maha marma24
.
Astanga sangraha and hridaya (6th century A.D.):
Detailed description of marma is given in both the texts in the sharira sthana.
Marma are described as in sushruta samhita giving importance to the external trauma
and the avoidance of marma points during the surgical intervention. Marma are
classified in accordance with their location, size, affect and composition. The full
account of the treatment of the same is available25, 26
.
Historical Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 10
Medieval period:
Most of the works in this period followed the description of marma as
described in the treatises of samhita period. However the books like chakradatta
yogaratnakara and sharangadhara have skipped the description of marma and injury to
marma.
Madhavakara (7th Century A.D.)
Citation of marma is limited to mentioning of involvement of marma in certain
diseases. Symptoms of injury to different types of marma are given in the chapter on
sadyovrana27
. Other than this, marma is mentioned in the samprapti of Dhatu gata
jvara, Chinna shvasa, Kaphaja unmada, Hridroga, Kshavathu, gara, Prognosis of
certain diseases is decided by the involvement or non-involvement of marma. The
examples include Vatarakta, Prameha pidaka, Shotha, Arbuda, Vrana, Visarpa,
Masurika, Balasa, Vidhradhi. Citation of 107 marma is made in the commentaries of
Madavanidana that include Madhukosha and Atanka darpana in the context of
Mutrakricchra28
.
Kalyanakaraka (9th
century AD)
The third chapter of Kalyanakaraka deals with the anatomy of human body. In
this chapter the total number of marma in the body is said as 10729
. Details of these is
not given in this chapter. But the full account in terms of location and symptoms of
injury of marma is given in the 20th
chapter. It is said that the manibhandha marma in
the hand matches with the gulpha marma of the leg and the injury to this marma
causes stabdhata, supti and ruk30
.
Historical Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 11
Bhavaprakasha: 16th Century A.D
In the first part of the purva khanda the third chapter is garbha prakarana. In
this chapter the detailed anatomy of the body is written. This description includes the
mentioning of the 107 marma in the body31
. The classification of the marma is made
as in sushruta samhita. Pair of manibhandha marma is listed as one among the 22
marma located in the arms. It is also said that the diseases involving the marma are
difficult to cure32
Modern period
Yogarathnakara (17 century AD)
The citation of marma is limited to the mentioning in samprapti and prognosis
of certain diseases like hridroga and vidradhi33
.
Bhaishajya rathnavali 18th
century AD
Details of the location of the marma, symptoms of injury and treatment of
marma injury are not included in the text. More to add until the medieval period the
clinical understanding of marma was restricted to injury to the marma, clinical
presentation of injury of marma and its treatment. Contrary to this in the modern
period the principle of treating different diseases by massaging and manipulating the
marma is developed.
Siddha system of medicine was developed in the southern part of the India.
Much importance was given to the knowledge of marma in the books on siddha
system of medicine. In the siddha medicine marma is known by the name varma. The
Vedic sage by name Agastya rishi is said as the founder of the siddha system of
medicine. In this system it is believed that in the disease states the energy is blocked
Historical Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 12
in specific marma. This can happen due to external trauma or internal factor of fear or
anger. It is conceptualized that the blockage of psychic energy in the marma locations.
This blockage of energy can be released by measures of mantra pranayama and
meditation. Also, injury to the marma is attributed to the astrological events. The
knowledge of marma was extended to the martial art where in knowledge of marma is
used for both defensive as well as offensive purposes. Martial art tradition of
Kalaripayattu34
is the example for this. Tamil tradition mentions 108 marma in the
body and the kalari tradition of Kerala considers 365 marma points. The relation
between the seven chakra in the body and marma is also elaborated in this science. 12
marma points are listed and the injury to this marma may lead to sudden death. It is
said that this martial art is founded by the sage Parasurama and this knowledge is said
to be derived from Dhanurveda (Science of War/Archery), Ayurveda, and Yoga35
.
Also massaging of the specific marma point is practiced to heal and cure a variety of
diseases.
Carpal tunnel syndrome:
During 1854 the first description of median nerve entrapment was recorded in
the history. A century later the term carpal tunnel syndrome came in to print. The
alternative diagnosis made for this disease included Acroparasthesia, motor branch of the
median nerve or the brachial plexus compression. The first description related to the
surgical intervention of CTS dates back to 193336. The first article on idiopathic CTS
was published during 194637. Tourniquet test was described for the diagnosis of carpal
tunnel syndrome during 1953 by Gilliatt and Wilson38
. During 1956,
electromyography was found to be effective in the diagnosis of CTS39
. From 1960
onwards the carpal tunnel syndrome became the common diagnosis.
Nirukti & Paribhasha
Efficacy of lashuna rasayana in manibandha marmabhighata Page 13
NIRUKTI & PARIBHASHA.
The word Manibandha marmabhighata has three component as manibandha,
marma and abhighata. For descriptive purposes these three are dealt separately.
Manibandha:
The Sanskrit word manibandha in masculine gender is formed by the
combination of two component terms of Mani and bandha with the addition of suffix
ghanj40
. Mani refers to the jewels41
. Bandha42
refers to the act of fastening or binding.
Put together, etymologically the fastening of the jewel is known as manibandha. This
implies, the wrist is the part where bracelets of precious stones are bound and hence
termed as manibandha.
The joint between the forearm and hand is called as manibandha 43
. It is
identified as the base of hand44
and is located in the proximal palm.45
Marma:
The Sanskrit word marma is derived from the root mrin maranae meaning to kill
/ death46
. Etymologically the word marma is translated as point that can kill. The word
marma is also derived in another way. Mah and ma are the component terms of
marma. The word maha connotes prana and the term ma means residence. Put
together the location of prana in the body is termed as marma.Marma refers to a body
location and injury to which tend to cause death47
In the Ayurveda literatures the
marma is defined as juncture of the body where two or more tissues of mamsa,sira
snayu ,asthi and sandhi48
The location in the body injury to which causes syandana
(pulsations) pidana (physical or mental distress) and ruk (pain) is also known as
Nirukti & Paribhasha
Efficacy of lashuna rasayana in manibandha marmabhighata Page 14
marma. Or else the part of the body and the injury to which causes serious illness
similar to death is known by the term marma. The word marma also means hidden
secret.
Synonym: varma is the other name of marma in siddha system of medicine
Abhighata:
The Sanskrit word abhighata in masculine gender is derived from the Sanskrit
root “han” with the prefix “abhi”. The Sanskrit root “han” refers to the activity of
striking or attack. The prefix “abhi” implies severe intensity49
Thus etymologically
abhighata means severe attack and implies traumatic injuries.
By definition the traumatic injury caused by sticks50
or wild animals is called
as abhighata. It is worth mentioning here that in the context of marmabhighata the
word abhighata simply means injury and refers to both internal and external injury.
The injury caused by external factors like falling, weapons, wild animals or non-
human beings is known as abhighata. Also the injury of the marma caused by vitiated
dosha is considered as internal abhighata 52
Carpal tunnel syndrome:
The English word carpal is originated from Modern
Latin word carpus meaning wrist53
. Literally the word carpal is an adjective meaning
pertaining to the wrist. Artificial underground passage is known by the word tunnel.
Anatomically the word carpal tunnel refers to an osteofibrous canal situated in the
volar wrist. The median nerve passes through this canal. Group of symptoms which
consistently occur together is known by the word syndrome. Put together the

Nirukti & Paribhasha
Efficacy of lashuna rasayana in manibandha marmabhighata Page 15
syndrome involving the carpal tunnel is known as carpal tunnel syndrome. By
definition compression of the median nerve within the carpal tunnel presenting with
characteristic clinical manifestation of numbness, paresthesia, and pain in the median
nerve distribution is termed as carpal tunnel syndrome.
Nidana
Efficacy of lashuna rasayana in manibandha marmabhighata Page 16
NIDANA
Paraesthesia54
and paralysis of the hand is the typical presentation of the
Manibandha marmabhighata. Hence this illness comes under the umbrella of
vatavyadhi. Hence all the nidana, purvarupa, rupa and samprapti of the Manibandha
marmabhighata is discussed under the pretext of vatavyadhi. Thus the etiological
factors of vatavyadhi are discussed as nidana of Manibandha marmabhighata. The
vatavyadhi in general or Manibandha marmabhighata in particular may happen due to
the apatarpana nidana or santarpana nidana. Apatarpana nidana are mostly the nidana
of vatavyadhi that directly causes the vitiation of vata dosha. Contrary to this the
santarpana nidana causes accumulation of the medas that obliterates the vatavaha
srotas causing the vatavyadhi. These two categories of etiological factors are
discussed separately.
Apatarpana nidana
Following are the apatarpana nidana segregated from the general etiology of
vatavyadhi. The same is categorized into dietary, behavioral, traumatic, psychological
factors and pre-existing illness for descriptive purposes55
.
Dietary factors: Excessive and habitual consumption of foods that are pungent ,bitter
or astringent in taste; Excessive and habitual intake of food articles having properties
like un-unctuousness or coldness; Excessive and habitual consumption of foods
having the property of lightness; the rice stored for long; recently harvested rice may
cause morbidity of vata dosha; Excessive and habitual consumption of specific cereals
and pulses that include Nishpava (Dolichos lablab Linn), Shyamaka (Echinochola
Nidana
Efficacy of lashuna rasayana in manibandha marmabhighata Page 17
frumentacea Linn), Mudga (- Phaseolus radiatus Linn), Masuri (Lens culinaris
Medic), Makushtaka (Phaseolus aconitifolius Jacq), Chanaka (Cicer arietinum Linn),
adaki (Cajanus cajan Mills), Kodrava (Paspalum scorbiculatum Linn) and Kalaya
(Lathyrus sativus Linn), Either excessive or much limited amount of food
consumption and starvation .
Behavioral factors
Excessive sexual indulgence; Excessive walking; Excessive physical exercise:
Exhaustion due to physical activities, Frequent traversing by leaps or jumps, Frequent
swimming, Frequent use of uncomfortable bed, Frequent use of uncomfortable seat,
Falling or racing while riding on an elephant, Falling or racing while riding on a
camel, Falling or racing while riding on a horse, Excessive physical activities,
Frequent staying awake at night, Day sleep, Exposing oneself to the easterly wind,
Exposure to snowy weather, Suppression of naturally manifesting urges like
defecation.
Psychological factors
Emotional disturbance of anxiety; Emotional disturbance of grief, Emotional
disturbance of anger, Emotional disturbance of fear& Emotional disturbance of sexual
love.
Traumatic factors
Trauma by different exogenous factors like beating with the stick & Injury to
the vital organs

Nidana
Efficacy of lashuna rasayana in manibandha marmabhighata Page 18
Iatrogenic factors
Excessive loss of dosha while undergoing shodhana treatment, Excessive loss
of dosha during the treatment of Vamanakarma, Excessive loss of dosha during the
treatment of Virechana karma.56
Preexisting illness
Depletion of body elements secondary to any illness, Excessive emaciation
due to any illness, Morbidity of ama leads to development of margavarana, Excessive
excretion of fecal matter during diseases states like atisara.57
Seasonal and environmental factors
Rainy season; winter season; unusual delay of digestion; late part of the night.
From the above the excessive physical strain involving the wrist joint has direct
bearing on the Manibandha marmabhighata. Different etiological factors related to
external traumatic injury have direct bearing on the Manibandha marmabhighata.
Santarpana nidana
Over nourishment predisposes to excessive accumulation of the medas which
in turn obstructs the vatavaha srotas and causes vatavyadhi58
. Following etiological
factors are worth mentioning59
.
Dietary factors
Excessive consumption of foods that is unctuous, sweet, slimy and heavy for
digestion; consumption of new cereals; intake of new alcoholic beverages,
consumption of meat of wet land and animals, excessive intake of sea foods, habitual
Nidana
Efficacy of lashuna rasayana in manibandha marmabhighata Page 19
consumption of dairy products, frequent consumption of molasses, excessive
consumption of foods prepared from cereal flour, consumption of foods that cause
accumulation of kapha in the body.
Behavioral factors
Lack of physical activity, day sleep, prolonged resting on comfortable chair or bed.
Psychological factors
Lack of mental activity .These factors increase kapha and medas predisposing
entrapment of vatavaha srotas causing vatavyadhi.
Etiology of carpal tunnel syndrome:
Carpal tunnel syndrome is considered as idiopathic. However any disease or
condition that generates pressure on the median nerve with in the anatomical structure
of carpal tunnel leads to carpal tunnel syndrome. The diseases that can predispose to
carpal tunnel syndrome include obesity, hypothyroidism, arthritis, diabetes and
trauma60
. Genetic factor also has some role in the causation of carpal tunnel
syndrome. The risk of carpal tunnel syndrome is said to increase with the
consumption of oral contraceptive pills. Even certain diseases at the wrist that
compress the carpal tunnel compromising the space with in the tunnel can cause the
carpal tunnel syndrome and is possible in conditions like lipoma, ganglion and
vascular malformation. Profession involving repetitive flexion and extension of the
wrist may precipitate carpal tunnel syndrome. Cumulative trauma on the wrist in the
form of repetitive movement and manipulating activities at the wrist that may be
possible in certain profession may increase the risk of Carpal tunnel syndrome.
Poorvaroopa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 20
POORVAROOPA
In general in most of the vata vyadhi the development of the symptoms of the
disease in the milder form in the beginning of the illness is known as purvarupa61
.
This is also applicable in case of Manibandha marmabhighata. Initial development of
pain and numbness in the hand may be accepted as purvarupa of Manibandha
marmabhighata. With the pretext of carpal tunnel syndrome it may be further
specified as milder form of paresthesia involving thumb middle and radial half of ring
finger is the premonitory symptom of Manibandha marmabhighata.62
Roopa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 21
ROOPA
Manibandha marma is enlisted as one among the 107 marma located in the
body. It is said that there are 11 marma in each arm. Among these manibandha marma
is located at the base of the hand. Following details give the full account of the
marma.
Location type
Manibandha marma is considered as sakthi marma, as is related to the
extremities. Among the extremities also, manibandha marma is located in the arms at
the joint between the forearm and hand63
.
Dimension type: 2 angula is the dimension of manibandha marma.64
Component type: Structurally the manibandha marma is considered as sandhi
marma 65
since it formed by the joint between the fore arm and hand.
Illness type: Pain is the major clinical manifestation due to the manibandha
marmabhighata hence is noted as rujakara marma66
.
Based on these specifications the following symptoms occur in manibandha
marmabhighata.
Supti
The morbid vata dosha by virtue of its lightness as well as instability causes
lack of sensation in different body parts and is known as supti. The effected part
becomes numb, senseless and fails to carry out its motor activity. Person fails to
appreciate the pain when the affected part is injured by nails and others. More to add,
Roopa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 22
the person fails to experience the very existence of the affected part. In regards to the
Manibandha marmabhighata supti involves the hand67
.
Ruk
The symptom of continuous and uninterrupted pain which is of either
moderate or severe intensity is known as ruk. Manibandha marma belongs to the
category of rujakara marma and pain in the hands is the leading symptom.
Vastushukairavakirna:
The subjunctive symptom as if the body part is afflicted with awn of grains is
the symptom of vastushukairavakirna. To be clearer, the feeling of pins and needles is
refered by this work vastushukairavakirna. This is the typical symptom of any sandhi
marma68
. As the manibandha marma is the sandhi marma sensation of pins and
needles involving the hand is a clinical presentation.
Shosha: The symptom shosha refers to either dehydration or diminution of different
body parts. Dehydration of the body fluids is said by the term shosha69
. Dryness and
lightness are two properties of the vata dosha that are responsible for the occurrence
of the symptom shosha. To quote an example, reduced bulk of the muscle in different
parts of the body or emaciation of the whole body is referred as shosha. The atrophy
of the muscles of the hand is typical of manibandha marmabhighata.
Parvashopha : Swelling around the finger joints is the symptom of sandhi marma70
Kuntata : Paralysis of the hand.
Roopa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 23
Carpal tunnel syndrome
Numbness and tingling, pain, weakness as well as dysautonomia form the
complete list of symptoms of carpal tunnel syndrome.
Numbness and tingling
This is the most common symptom of carpal tunnel syndrome. Frequently the
patient may complain that their hands fall asleep or at times the thing held in the
affected fingers without their noticing. Some patients may complain of loss of grip.
Few other patients may complain that frequently thing drop from their hands without
their notice.
Pain: Numbness of the hand is usually associated with an aching pain sensation
distributed in the ventral part of the wrist. This pain may exhibit radiation from the
wrist distally to the palm and fingers. Even the pain may extend proximally from the
wrist along the ventral forearm.
Weakness: Reduction of the power in the hand can occur in considerable number of
patients. This may lead to clumsiness in the precision of the grip involving the thumb.
Autonomic symptoms: Median nerve carries autonomous nerves fibers to the hand
hence some autonomic symptoms are seen in patients suffering from carpal tunnel
syndrome. Feeling of tightness or swelling distributed in the hands is the presentation
of autonomic presentation. At times even variation in temperature of the hands either
being cold or hot all the time may be felt in the affected hand. Some patient may even
have sensitivity to changes in temperatures. Patients hand may turn pale on exposure
to cold.
Roopa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 24
Onset and course: gradual or insidious onset of symptoms is typical of Carpal tunnel
syndrome. Usually the symptoms are intermittent rather continuous. The activities
listed in the aggravating factors may initiate the symptoms of Carpal tunnel
syndrome.
Aggravating factors: The most common specific activities that may trigger the
symptoms of Carpal tunnel syndrome include driving the vehicles, reading the
newspaper, knitting the woolen coat, painting any art. Symptom may even become
worse at night hours and may make the patient to wake up.
Relieving factors: Usually the symptoms of Carpal tunnel syndrome get reduced by
shaking the hand/wrist71
.
Laterality: Carpal tunnel syndrome may be unilateral but is usually bilateral. Also it
is noted that it is the dominant hand that affected first than the non-dominant hand.
More to add the symptoms are comparatively severe in dominant hand.
Symptom distribution: Symptoms are limited to the area or sensory distribution of
the median nerve that includes palmar aspect of the first to the fourth fingers and the
distal palm. It should be remembered that if the numbness is predominantly
experienced in fifth finger or extending to the thenar eminence or dorsum of the hand
then is not suggestive of Carpal tunnel syndrome. Contrary to this a significant
number of patients are not able to clearly explain the distribution of numbness.
Roopa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 25
Physical examination findings: Sensory examination motor examination and special
test helps in the confirmation of the diagnosis of Carpal tunnel syndrome.
Sensory examination: Different modalities of sensory abnormalities are noticed in
the palmar aspect of thumb index and middle fingers and radial one half of the index
finger. Also the tow point discrimination is most sensitive in clinching the diagnosis.
The pin prick test is equally sensitive72
.
Motor examination
Wasting as well as weakness of the hand muscles innervated by the median
nerve is characteristic73
. The muscles affected include First and second lumbricals,
Opponens pollicis, Abductor pollicis brevis and Flexor pollicis brevis.
Special tests
The special tests that are helpful in the confirmation of the diagnosis of Carpal
tunnel syndrome are Hoffmann tinel sign, phalen sign, carpal compression test
palpatory diagnosis and square wrist sign.
Hoffmann tinel sign74
: A gentle tap is made on median nerve at the region of carpal
tunnel of the wrist. This elicits tingling sensation in the distribution of median nerve.
Though this test is commonly done it is considered as less sensitive test.
Phalen sign75
: The wrist is held in fully flexed position for a minimum of 60 seconds.
This activity triggers tingling in the median nerve distribution. This is the positive
phalen sign. Tingling sensation in the distribution of the median nerve may be
Roopa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 26
induced by holding the wrist in fully extended position for not less than 60 seconds.
This is known as reverse phalen sign. Though these tests are very specific but are
found to be low sensitive.
Carpal compression test: Firm pressure is applied on the carpal tunnel by applying
the thumb and is maintained for 30 seconds. This will trigger the symptoms of carpal
tunnel syndrome76
. This test is found to be sensitive by 89 to 96 %.
Palpatory diagnosis: This test is carried out by examining the soft tissues overlying
the median nerve at the wrist for any mechanical restriction77
.
Square wrist sign. The thickness and the width of the wrist is measured and its ratio
is calculated. If the ratio is greater than 0.7 then is positive for carpal tunnel
syndrome78
.
Investigations
Nerve-conduction studies are highly sensitive detecting the median nerve
damage. Muscle activity may be studied by electromyography.
Bheda
Efficacy of lashuna rasayana in manibandha marmabhighata Page 27
BHEDA
From the foregoing chapters it is clear that Manibandha marmabhighata
belongs to the category of nanatmaja vata vyadhi. Hence the etiopathogenesis of vata
vyadhi also holds well in Manibandha marmabhighata. Vatavyadhi is categorized into
two on the basis of basic causes of vatavyadhi as dhatu kshayaja vata vyadhi as well
as margavaranja vata vyadhi79
.The same is applicable to Manibandha marmabhighata.
Margavaranja marmabhighata
In general the accumulation of the medas in the body leads to the pathology of
avarana. In the context of Urustambha it is said that excessive accumulation of the
medas in the thigh region obliterates the channels that carry vata dosha and the patient
suffers from urustambha. Identical to this the accumulation of medas in the
manibandha can obliterate the vatavaha sira which is on among the content of marma
in general; can precipitate the clinical presentation of Manibandha marmabhighata.
Dhatu kshayaja marmabhighata
Dhatu in the context of vatavyadhi refers to snayu upadhatu. The degeneration
of this is termed as dhatu kshaya in general. Among the different nidana of vata
vyadhi excessive physical strain involving wrist precipitates the depletion of the
snayu with in the wrist joint this will lead to the manibandha marmabhighata.
Samprapthi
Efficacy of lashuna rasayana in manibandha marmabhighata Page 28
SAMPRAPTHI
Vitiated vata dosha afflicting the sira and snayu at the manibandha marma
leads to the clinical manifestation of the Manibandha marmabhighata. The following
paragraphs will give the full account of different samprapti ghataka involved in the
Manibandha marmabhighata.
Dosha: Vata dosha is invariably involved in the samprapti of Manibandha
marmabhighata. Manibandha marma belongs to the category of rujakara marma and
raja is the major symptoms of morbid vata dosha. More to add the symptoms of Supti,
Ruk, Vastushukairavakirna, Shosha and Kuntata of Manibandha marmabhighata all
are caused by vata dosha. On the other hand when the santarpana nidana is
precipitating the margavarana leading to the marmabhighata, the santarpana nidana
causes accumulation of kapha and medas in the body. In this pathology kapha dosha
may be involved in the causation of margavarana.
Dhatu: Mamsa is a component of any marma including the manibandha marma hence
its rationale to consider the mamsa dhatu in the pathogenesis of Manibandha
marmabhighata. Moreover, the symptom of shosha of manibandha marmabhighata is
pathognomonic of mamsa dhatu80
. Considering the etiopathogenesis of santarpana
nidana and the involvement of medas in the causation of margavarana reveals the
medas as a samprapti ghataka of Manibandha marmabhighata.
Upadhatu: Snayu is an invariable component of any marma including manibandha
marma. Localized or generalized paralysis in the body is attributed to snayu gata
vata81
. Considering the symptom of kuntata presenting with paralysis of the hand the
Samprapthi
Efficacy of lashuna rasayana in manibandha marmabhighata Page 29
morbid involvement snayu upadhatu in the samprapti of manibandha marmabhighata
is justified.
Mala: No specific mala is involved in the samprapti of Manibandha marmabhighata
Manas: No symptom of Manibandha marmabhighata indicates the involvement of
manas.
Indriya: Vata dosha is instrumental in the activities of indriya including the
sparshanendriya82
. Sensation is the function of sparshanendriya. Sensation of pins
and needles as well as numbness of the hand indicates the affliction of the
sparshanendriya.
Srotas: Sensation and motor activity in the body is said to be mediated through the
vatavaha sira83
and vatavaha dhamani84
. Sira and dhamani and snayu are component
of any marma and so also the manibandha marma. Loss of sensation is
pathognomonic of affliction of vatavaha dhamani. In contrast to this the paralysis of
the hand is indicative of affliction of vatavaha sira. Again in case of the santarpana
nidana the rasavaha srotas as well as medovaha srotas is invariably involved.
Srotodushti prakara: Motor activity is the function of vatavaha sira. This function is
greatly affected in the symptom of kuntata. Thus the sanga of the vatavaha sira is
justified. On the other hand different modality of sensation is the function of vatavaha
dhamani. The numbness in Manibandha marmabhighata is indicates sanga of
vatavaha dhamani. More to add sanga of the rasavaha srotas as well as medovaha
Samprapthi
Efficacy of lashuna rasayana in manibandha marmabhighata Page 30
srotas is instrumental in morbid increase of medodhatu that obstructs the vatavaha
dhamani and sira.
Agni: Pathological state of Agni is unrelated in the samprapti of the manibandha
marmabhighata caused by the nidana. Contrary to this dhatvagnimandya is evident in
santarpana nidana. The impairment of rasa dhatvagni facilitates excessive production
of medodhatu from the rasa dhatu.
Ama: When the manibandha marmabhighata is caused by indulgence of etiology of
vata vyadhi, ama is not involved in the pathogenesis. On the contrary rasa dhatu gata
ama is argued in the samprapti of santarpana nidana. The excessive intake of unctuous
and sweet foods causes abnormal accumulation of kapha and medas in the initial rasa
dhatu. This morbid accumulation of medas in the rasa dhatu is termed as amarasa85
.
This eventually causes over weight and obesity. Again thus produced medas is
responsible for the entrapment of the vatavaha dhamani and sira at the manibandha.
Udbhava sthana: Vata dosha is exclusively involved in the samprapti of Manibandha
marmabhighata of the type caused by nidana. Hence the pakvashaya86
as the origin of
the illness is justified. Contrary to this kapha and medas are additional in the
samprapti of Manibandha marmabhighata due to margavarana. Hence amashaya87
and
pakvashaya together is accepted as origin of the illness.
Dosha sanchara sthana: Over stain of the wrist during different activities
predisposes to vitiation of vata dosha and causes Manibandha marmabhighata. In this
samprapti the symptoms are distributed in the wrist as well as hand and are the
sanchara sthana of the dosha. On the other hand in the santarpana nidana, kapha and
Samprapthi
Efficacy of lashuna rasayana in manibandha marmabhighata Page 31
medas circulate all over the body presenting with overweight and obesity indicating
the whole body as the sanchara sthana of the dosha. It is same morbid medas at the
wrist predisposes to Manibandha marmabhighata.
Vyakta sthana: Numbness pain and paralysis related to the wrist and hand are the
cardinal manifestation of the Manibandha marmabhighata. Based on this it can be said
that manibandha sandhi and pani as the vyakta sthana of the manibandha
marmabhighata.
Rogamarga: Involvement of manibandha sandhi and marma justifies the madhyama
roga marga 88
of the illness.
Vyadhi svabhava: It is said that any disease involving the marma / madhyama roga
marga is difficult to cure. Accordingly any marmabhighata is described as
“krichratama vyadhi”89
i.e. the illness is treatable only by energetic and meticulous
planning.
Samprapthi
Efficacy of lashuna rasayana in manibandha marmabhighata Page 32
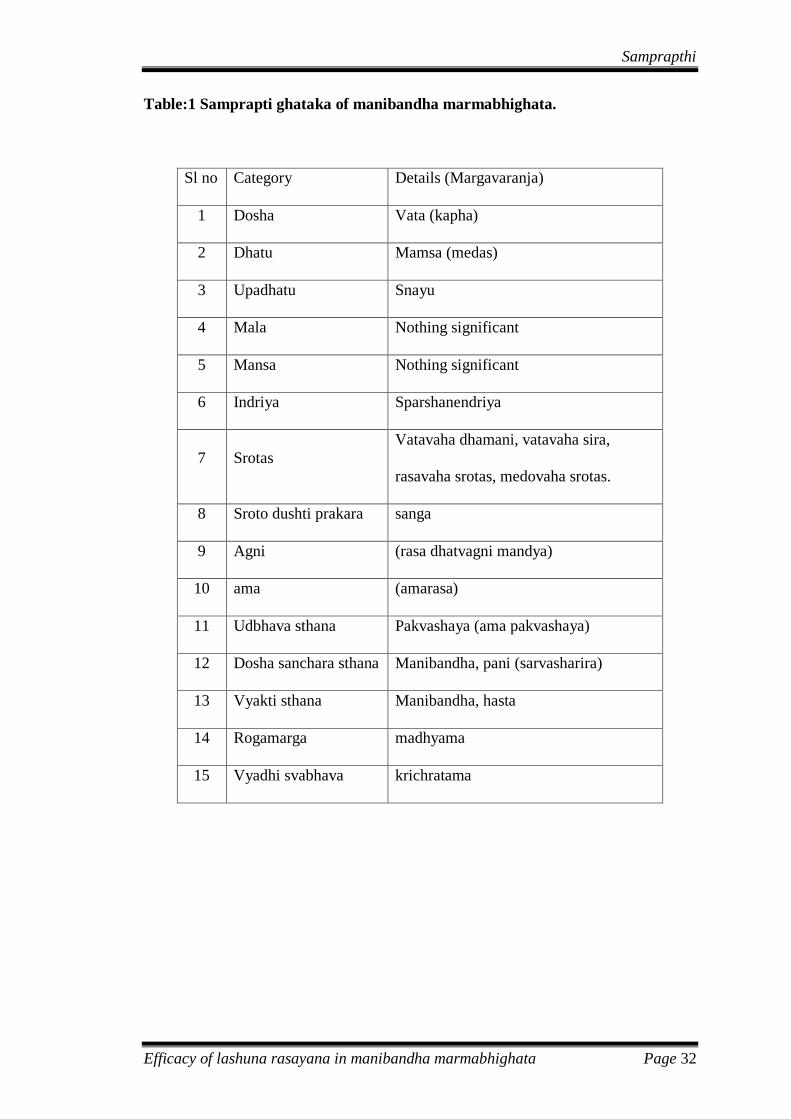
Table:1 Samprapti ghataka of manibandha marmabhighata.
Sl no Category Details (Margavaranja)
1 Dosha Vata (kapha)
2 Dhatu Mamsa (medas)
3 Upadhatu Snayu
4 Mala Nothing significant
5 Mansa Nothing significant
6 Indriya Sparshanendriya
7 Srotas
Vatavaha dhamani, vatavaha sira,
rasavaha srotas, medovaha srotas.
8 Sroto dushti prakara sanga
9 Agni (rasa dhatvagni mandya)
10 ama (amarasa)
11 Udbhava sthana Pakvashaya (ama pakvashaya)
12 Dosha sanchara sthana Manibandha, pani (sarvasharira)
13 Vyakti sthana Manibandha, hasta
14 Rogamarga madhyama
15 Vyadhi svabhava krichratama
Samprapthi
Efficacy of lashuna rasayana in manibandha marmabhighata Page 33
Pathophysiology of carpal tunnel syndrome.
Carpal tunnel syndrome happens due to the entrapment of the median nerve90
.
This happens with in the rigid confines of the carpal tunnel. To begin with, there
exists high carpal tunnel pressure. This increased pressure obstructs the venous out
flow. Obstructed venous outflow in term increases the back pressure and development
of edema. This edema within the Carpal tunnel ultimately leads to ischemia of the
nerve. This ischemia initiates the median nerve damage. Initially due to the
entrapment the median nerve undergoes demyelination. This is followed by axonal
degeneration. In this pathophysiology the sensory nerve fibers are affected first. This
is followed by affliction of motor nerve fibers91
. More to add the autonomous fibers
with in the median nerve also get affected.
Upadrava
Efficacy of lashuna rasayana in manibandha marmabhighata Page 34
UPADRAVA
In regards to the marma in general, it is said that either permanent
disability or death is the complication of marmabhighata. To be more precise; it is
said that in case of poor management or sever injury of the rujakara marma eventually
leads to permanent disability92
. From these descriptions it is clear that permanent
disability is the complication of manibandha marmabhighata. The permanent
disability in relation to the manibandha marmabhighata is described as kuntata or
paralysis. Hence the kuntata or paralysis of the hand is accepted as complication of
manibandha marmabhighata. Paralysis, complete loss of sensation and atrophy of
muscles is regarded as complications of vatavyadhi in general. By implication
paralysis of the hand, loss of sensation of the hand and atrophy of the hand muscles is
the complications of manibandha marmabhighata
Complications of carpal tunnel syndrome: Timely and meticulous treatment is
essential in case of carpal tunnel syndrome lest it will lead to permanent irreversible
damage to the median nerve. This will result in decrease in hand function, atrophy of
thenar muscle and disability of hand.
Sadya-Asadyata
Efficacy of lashuna rasayana in manibandha marmabhighata Page 35
SADYA-ASADYATA
Multiple factors determine the prognosis of the Manibandha marmabhighata.
Following factors are worth considering in the context of sadhya asadhyata of
Manibandha marmabhighata.
Morbidity of vata dosha.
Vatadosha is the most important and virulent dosha present in the body.
Among the dosha vata is considered as svatantra dosha or independent dosha. Pitta
and kapha are capable of moving when mobilized by the vata dosha. Vata is circulates
in the whole body and hence causes severe diseases. Morbidity of vata dosha is hence
treated as most difficult among the vitiation of three dosha. Manibandha
marmabhighata causes vata vyadhi hence is difficult to cure.
Avarana vyadhi.
In general diseases caused by the avarana is said to be difficult to cure.
Santarpana nidana causes accumulation of medas in the wrist. This entrapts the
vatavaha srotas manifesting as avarana eventually leading to manibandha
marmabhighata. Needless to say, the manibandha marmabhighata manifesting as a
sequel of avarana is difficult to cure.
Marmagata vyadhi.
By all means the diseases related to the marma are difficult to cure. Even
minor injury to any marma should be considered seriously and it should be
meticulously treated with priority. Any error in the treatment may either lead to
permanent disability or death. Usually the rujakara marma proves causing permanent
Sadya-Asadyata
Efficacy of lashuna rasayana in manibandha marmabhighata Page 36
disability if not fatal. It is said that since the mamsa, sira, snayu, asthi and sandhi are
collectively present the injury to the marma is always serious93
. Physiologically the
prana exist in the marma and hence injury to any marma should be considered as
serious injury. The characters of agni and vayu predominate in the rujakara marma
including manibandha marmabhighata94
. This unique combination tends to cause
permanent disability of kuntata or paralysis of hand.
Madhyama roga marga vyadhi.
Involvement of manibandha sandhi and marma substantiates the Manibandha
marmabhighata as sandhi and marma gata vyadhi. Hence is enlisted as one among the
madhyama roga marga. In general it is said that any disease involving the madhyama
roga marga is difficult cure, so also the Manibandha marmabhighata.
Prognosis of carpal tunnel syndrome.
Usually the Carpal tunnel syndrome is progressive over time. Symptoms may
fluctuate from week to week. In a long run it may lead to permanent median nerve
damage. Conservative management works well in significant number of cases.
Surgical correction gives prompt relief and prevents the permanent damage. However
recurrence is possible when treated conservatively and also after surgical intervention.
When the Carpal tunnel syndrome is secondary to some preexisting illness like
diabetes or wrist fracture then the prognosis is poor. Patients with negative nerve
conduction study reports have good prognosis.
Chikitsa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 37
CHIKITSA
Internal or external injury can cause affliction of marma. Vitiated dosha
afflicting the marma forms the pathophysiology of internal doshaja marmabhighata.
Manibandha marmabhighata of to internal injury type, caused by affliction with
doshaja marmabhighata leading to vatavyadhi is the subject matter of this chapter.
Again the santarpana nidana causing accumulation of medas at the wrist; which in
turn, obliterating the vatavaha srotas is the unique pathology of doshaja manibandha
marmabhighata. Thus clearing the effects of santarpana nidana and rectifying the
resulting vatavyadhi forms the crux of the treatment of Manibandha marmabhighata.
With this pretext following line of treatment of doshaja Manibandha marmabhighata
is discussed95
.
Srotas Shodhana: In general shodhana is contraindicated in vatavyadhi. But if the
vatavyadhi is associated with other dosha or else the pathology of avarana is involved
then the shodhana should be planned at the outset. In this regard it is said that by
mistake if the snehana and other treatment of vata dosha is initiated at outset the
symptoms are likely to be worsened96
. Hence shodhana is indicated. Santarpana
nidana leading excess of medas accumulated in the manibandha is the unique
pathology of manibandha marmabhighata hence shodhana is ideal at the outset. Since
the pathology of medas is ubiquitously spread in the body sequential administration of
dipana pachana, snehapana, snigdha sveda, virechana karma and samsarjana krama
should be adapted. This will clear the medas accumulation in the wrist clearing the
avarana of vatavaha srotas.
Chikitsa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 38
Anabhishyandi sneha: Since kapha and medas is instrumental in initiating the
pathology of vata dosha both factors should be give equal importance while planning
snehana chikitsa as part and parcel of shodhana chikitsa. Snehapana is essential
prerequisite to achieve shodhana treatment and at the same time snehapana tend to
worsen the kapha and medas which is the initial pathology. Thus considering this the
anabhishyandi sneha is advised97
in the treatment of avarana. The ghee processed with
drugs that alleviate kapha and medas like pippali and guggulu should be prescribed to
the patient. In this regard guggulu tikta is an ideal medication for ensuring the sneha
effect prior to the shodhana in patients suffering from manibandha marmabhighata.
Mridu sramsana: Shodhana may worsen the vitiation of the vata dosha. Hence when
the patient physically strong and fit for shodhana treatment; mild shodhana in the
form of mridu sramsana should be adapted. Such balanced treatment clears the kapha
and medas and at the same time do not increase the virulence of vata dosha.
Sneha virechana: Virechana is ideal shodhana in accumulation of medas causing
avarana. At the same time resulting morbidity of vata dosha should be considered and
is made possible by adapting the sneha virechana. Virechana medicines in the sneha
form serve the purpose of sneha virechana. Thus oral administration of Eranda taila98
is an ideal prescription to accomplish sneha virechana.
Kapha pitta aviruddha chikitsa: At every stage of the treatment one should
remember that the vatavyadhi manifestation of Manibandha marmabhighata is
associated with morbidity of kapha and medas. Hence treatment of vata vyadhi that
does not worsen the kapha and medas should be judiciously planned.
Chikitsa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 39
Vatanulomana chikitsa: All measure of vata shamana like snigdha sveda should be
planned following shodhana chikitsa. Also one should plan with such measures that
do not worsen the kapha and medas.
Yapana basti: In general yapana basti is indicated in all vata vyadhi caused by
avarana. This yapana basti has the duel effect of shodhana as well as brimhana effect.
Shodhana effect is ideal to negate the effect of kapha and medas and the brimhana
effect negates the influence morbid vata dosha.
Rasayana: Rasayana chikitsa is always effective in avarana vata vyadhi. The
rasayana that are effective in avarana vatavyadhi include Shilajatu loha rasayana,
Bhargavaprokta rasayana, Guggulu rasayana with the anupana of milk and Haritaki
rasayana. Lashuna rasayana is worth mentioning in this regard. The Lashuna rasayana
is indicated both in dhatu kshayaja as well as avarana vatavyadhi99
. Lashuna rasayana
would be an ideal prescription in avarana manibandha marmabhighata.
Vyatyaasaat ushna anushna krama: Alternative employment of heat and cold
measures are is the balanced approach of treating the avarana vatavyadhi. This
implies the rukshana treatment of kapha and medas is followed by snehana chikitsa of
vata dosha should be adapted treating both the medas as well as morbid vata dosha.
Haritaki or yava is advisable in the form of rukshana chikitsa for about a week
followed by next one week medication with bala taila is suitable in avarana vata. Such
an alternative approach of treatment is justified in Manibandha marmabhighata.
Chikitsa
Efficacy of lashuna rasayana in manibandha marmabhighata Page 40
Bahiparimarjana chikitsa: Snigdha sveda is advisable in general in patients
suffering from vatavyadhi. This is also true in cases of Manibandha marmabhighata.
Also kapha and medas is involved in the avarana spearheading the samprapti of
Manibandha marmabhighata; ruksha sveda may be preferred in comparison to snigdha
sveda. Since part affected is hand different forms of ekanga sveda is most suitable.
Svedana may be done by adapting nadi sveda or avagaha sveda limited to the hand.
Even upanaha sveda is effective in avarana Manibandha marmabhighata. Sveda is
effective in relieving the pain and swelling and hence the pain of Manibandha
marmabhighata is best treated by ruksha or upanaha sveda.
Patya-Apatya
Efficacy of lashuna rasayana in manibandha marmabhighata Page 41
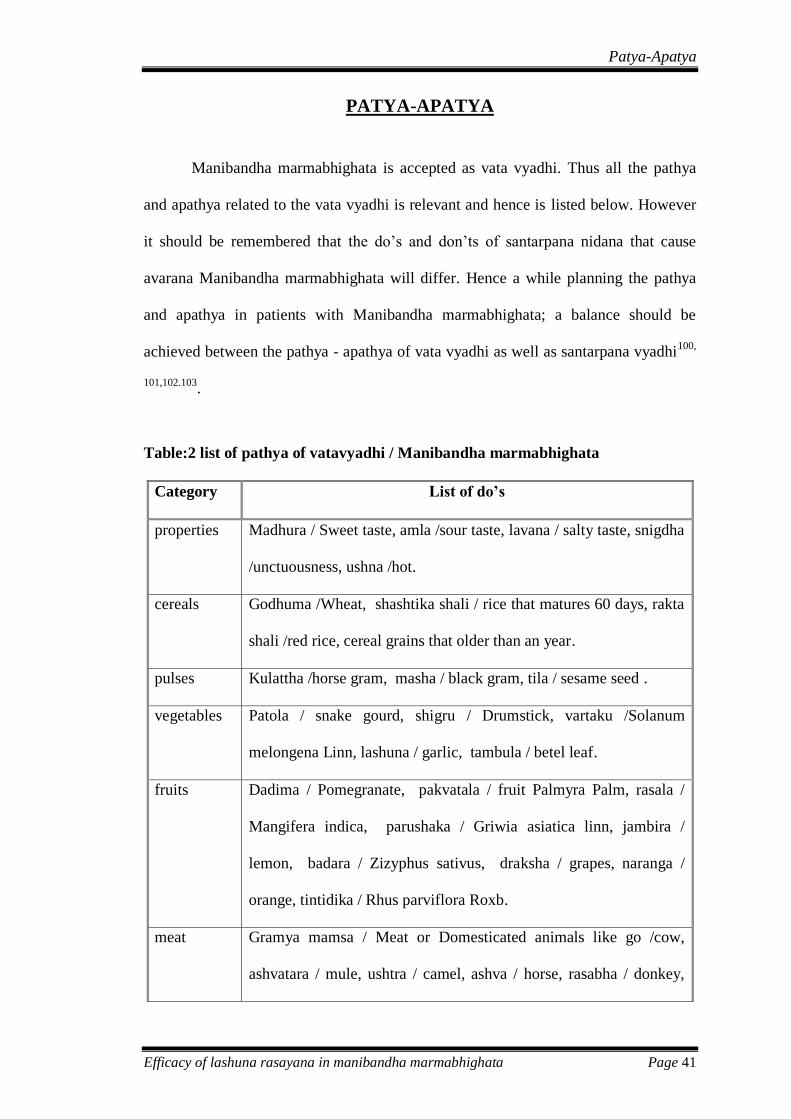
PATYA-APATYA
Manibandha marmabhighata is accepted as vata vyadhi. Thus all the pathya
and apathya related to the vata vyadhi is relevant and hence is listed below. However
it should be remembered that the do’s and don’ts of santarpana nidana that cause
avarana Manibandha marmabhighata will differ. Hence a while planning the pathya
and apathya in patients with Manibandha marmabhighata; a balance should be
achieved between the pathya - apathya of vata vyadhi as well as santarpana vyadhi100,
101,102.103.
Table:2 list of pathya of vatavyadhi / Manibandha marmabhighata
Category List of do’s
properties Madhura / Sweet taste, amla /sour taste, lavana / salty taste, snigdha
/unctuousness, ushna /hot.
cereals Godhuma /Wheat, shashtika shali / rice that matures 60 days, rakta
shali /red rice, cereal grains that older than an year.
pulses Kulattha /horse gram, masha / black gram, tila / sesame seed .
vegetables Patola / snake gourd, shigru / Drumstick, vartaku /Solanum
melongena Linn, lashuna / garlic, tambula / betel leaf.
fruits Dadima / Pomegranate, pakvatala / fruit Palmyra Palm, rasala /
Mangifera indica, parushaka / Griwia asiatica linn, jambira /
lemon, badara / Zizyphus sativus, draksha / grapes, naranga /
orange, tintidika / Rhus parviflora Roxb.
meat Gramya mamsa / Meat or Domesticated animals like go /cow,
ashvatara / mule, ushtra / camel, ashva / horse, rasabha / donkey,
Patya-Apatya
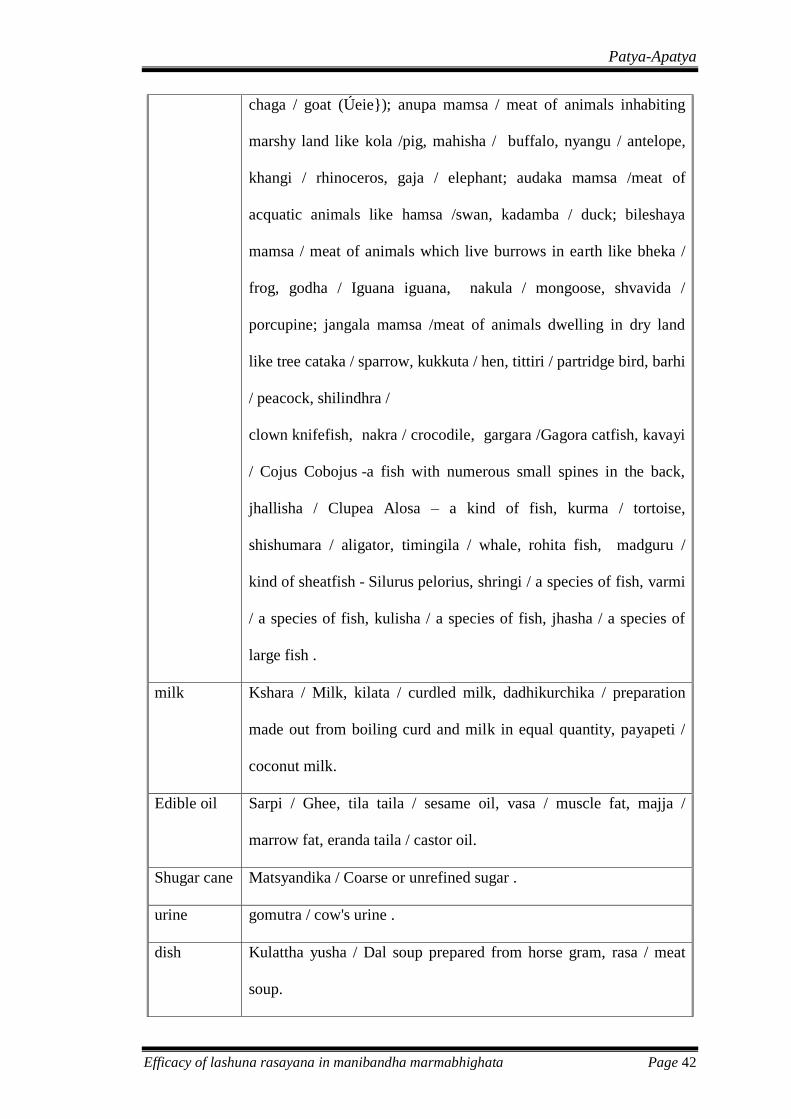
Efficacy of lashuna rasayana in manibandha marmabhighata Page 42
chaga / goat (Úeie}); anupa mamsa / meat of animals inhabiting
marshy land like kola /pig, mahisha / buffalo, nyangu / antelope,
khangi / rhinoceros, gaja / elephant; audaka mamsa /meat of
acquatic animals like hamsa /swan, kadamba / duck; bileshaya
mamsa / meat of animals which live burrows in earth like bheka /
frog, godha / Iguana iguana, nakula / mongoose, shvavida /
porcupine; jangala mamsa /meat of animals dwelling in dry land
like tree cataka / sparrow, kukkuta / hen, tittiri / partridge bird, barhi
/ peacock, shilindhra /
clown knifefish, nakra / crocodile, gargara /Gagora catfish, kavayi
/ Cojus Cobojus -a fish with numerous small spines in the back,
jhallisha / Clupea Alosa – a kind of fish, kurma / tortoise,
shishumara / aligator, timingila / whale, rohita fish, madguru /
kind of sheatfish - Silurus pelorius, shringi / a species of fish, varmi
/ a species of fish, kulisha / a species of fish, jhasha / a species of
large fish .
milk Kshara / Milk, kilata / curdled milk, dadhikurchika / preparation
made out from boiling curd and milk in equal quantity, payapeti /
coconut milk.
Edible oil Sarpi / Ghee, tila taila / sesame oil, vasa / muscle fat, majja /
marrow fat, eranda taila / castor oil.
Shugar cane Matsyandika / Coarse or unrefined sugar .
urine gomutra / cow's urine .
dish Kulattha yusha / Dal soup prepared from horse gram, rasa / meat
soup.
Patya-Apatya
Efficacy of lashuna rasayana in manibandha marmabhighata Page 43
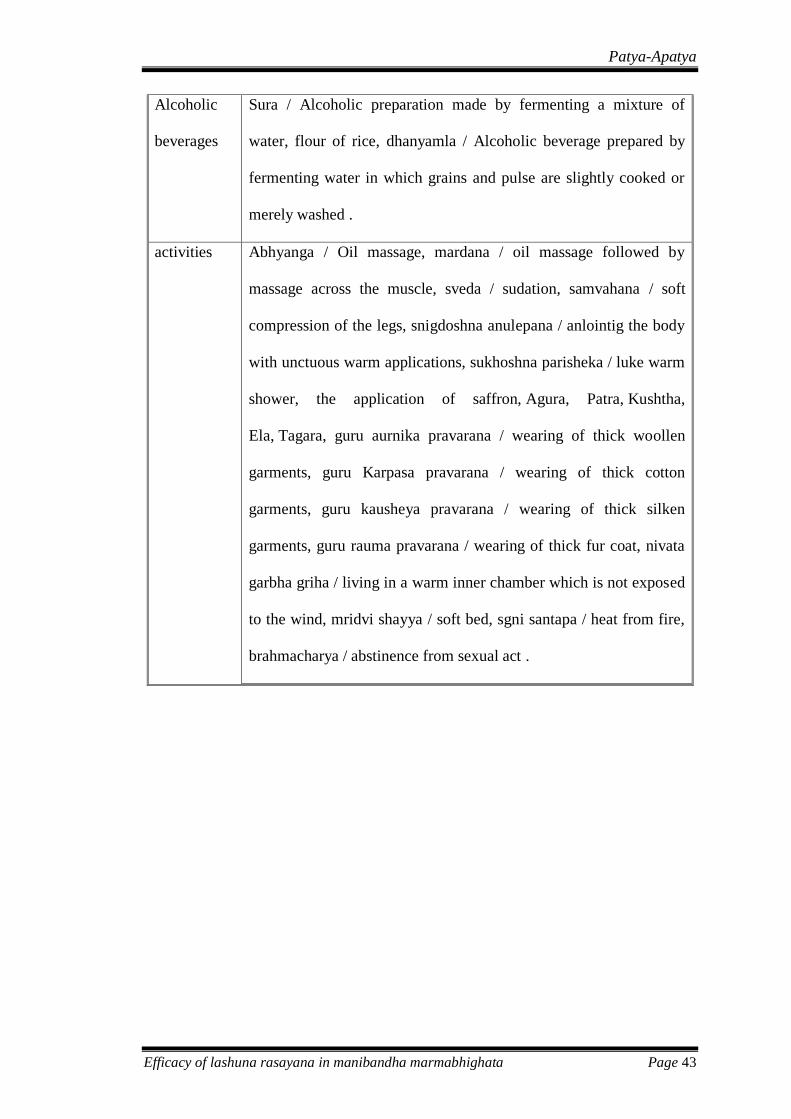
Alcoholic
beverages
Sura / Alcoholic preparation made by fermenting a mixture of
water, flour of rice, dhanyamla / Alcoholic beverage prepared by
fermenting water in which grains and pulse are slightly cooked or
merely washed .
activities Abhyanga / Oil massage, mardana / oil massage followed by
massage across the muscle, sveda / sudation, samvahana / soft
compression of the legs, snigdoshna anulepana / anlointig the body
with unctuous warm applications, sukhoshna parisheka / luke warm
shower, the application of saffron, Agura, Patra, Kushtha,
Ela, Tagara, guru aurnika pravarana / wearing of thick woollen
garments, guru Karpasa pravarana / wearing of thick cotton
garments, guru kausheya pravarana / wearing of thick silken
garments, guru rauma pravarana / wearing of thick fur coat, nivata
garbha griha / living in a warm inner chamber which is not exposed
to the wind, mridvi shayya / soft bed, sgni santapa / heat from fire,
brahmacharya / abstinence from sexual act .
Patya-Apatya
Efficacy of lashuna rasayana in manibandha marmabhighata Page 44
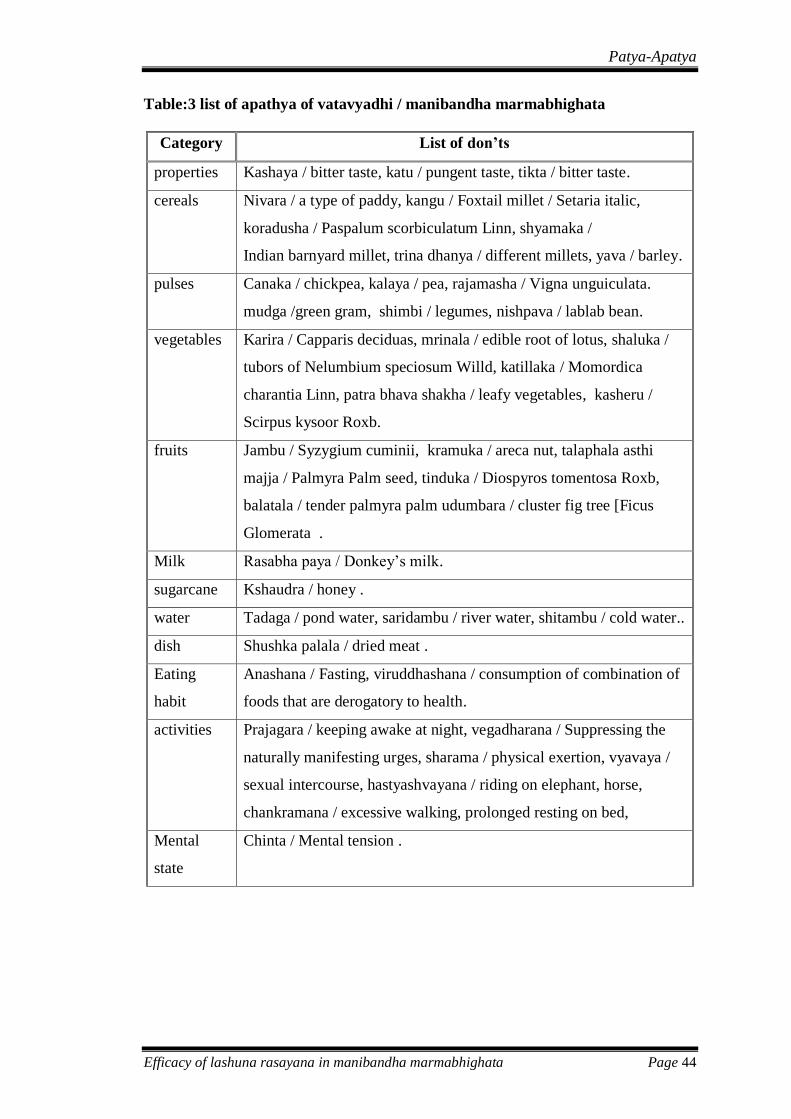
Table:3 list of apathya of vatavyadhi / manibandha marmabhighata
Category List of don’ts
properties Kashaya / bitter taste, katu / pungent taste, tikta / bitter taste.
cereals Nivara / a type of paddy, kangu / Foxtail millet / Setaria italic,
koradusha / Paspalum scorbiculatum Linn, shyamaka /
Indian barnyard millet, trina dhanya / different millets, yava / barley.
pulses Canaka / chickpea, kalaya / pea, rajamasha / Vigna unguiculata.
mudga /green gram, shimbi / legumes, nishpava / lablab bean.
vegetables Karira / Capparis deciduas, mrinala / edible root of lotus, shaluka /
tubors of Nelumbium speciosum Willd, katillaka / Momordica
charantia Linn, patra bhava shakha / leafy vegetables, kasheru /
Scirpus kysoor Roxb.
fruits Jambu / Syzygium cuminii, kramuka / areca nut, talaphala asthi
majja / Palmyra Palm seed, tinduka / Diospyros tomentosa Roxb,
balatala / tender palmyra palm udumbara / cluster fig tree [Ficus
Glomerata .
Milk Rasabha paya / Donkey’s milk.
sugarcane Kshaudra / honey .
water Tadaga / pond water, saridambu / river water, shitambu / cold water..
dish Shushka palala / dried meat .
Eating
habit
Anashana / Fasting, viruddhashana / consumption of combination of
foods that are derogatory to health.
activities Prajagara / keeping awake at night, vegadharana / Suppressing the
naturally manifesting urges, sharama / physical exertion, vyavaya /
sexual intercourse, hastyashvayana / riding on elephant, horse,
chankramana / excessive walking, prolonged resting on bed,
Mental
state
Chinta / Mental tension .
Drug Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 45
DRUG REVIEW
In the present study on efficacy of Lashuna rasayana104
in Manibandha
marmabhighata; the patient is initially treated with eranda taila for koshta shodhana
followed by administration of lashuna rasayana. The dravya guna of both lashuna and
eranda is given in this chapter.
LASHUNA 105
Lashuna is the only one content of the lashuna rasayana. For the purpose of
rasayana the garlic was administered in the freeze dried form filled in 500 mg capsule.
The full account of the dravya guna of the lashuna is given below.
Latin Name - Allium sativum.
Family Name – Liliacehe
Synonyms - Rasona, Yavanesta.
Vernacular Names
English : Garlic.
Hindi : Lahsun.
Kannada : Balluci.
Malayalam : Vellulli, Nelluthulli.
Properties
Rasa - Katu prdhana amla varjita sadrasa.
Guna - Snigdha, Tiksna, Picchila, Guru, Sara.
Veerya - Ushna.
Drug Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 46
Vipaka - Katu.
DoshaKarma- Kaphavatashamaka.
Rogaghnakarma-Brmhana, vrsya, pacana, saraka, bhagnasandhaanaya, kanthya
raktavardaka, balya, varnya, medya, netrahita, rasayana, hridya, jirnajvaraghna,
Kuksisulaghna, vibandha, gulmaghna, rucikara, kasaghna, sothaghna, kustaghna,
dipana, krimighna, svasaghna, kaphanisaraka.
Constituents–volatile oil containing Allyldisulphide and Diallyldisulphide. It also
contain Allin, Allicin, Mucilage and Albumin.
Substituents and adultrents-
Bulbs of Allium ampeloprasm Linn. Which is large in size and have two to four
cloves are considered as a good substitute for medical use in some parts of northern
India. A single clove variety of Allium sativum is grown in Rajastan for medicine
use.
ERANDA TAILA- This was administered for kosta shodhana before and after
treatment in the dose of 20 ml.
Eranda106
Latin name : RicinusCommunis Linn.
Family name : Euphorbiaceae.
Synonyms : Gandharvahasta, Panchaangula,vatari.
Drug Review
Efficacy of lashuna rasayana in manibandha marmabhighata Page 47
Vernacular Names
English : Castor Oil plant.
Hindi : Eranda, Rendee, andu.
Kannada : Haralu.
Malayalam : Avanakku, Abanakka.
Pharmacodynamics
Rasa : Madhura, Katu, Kashaya.
Guna : sukshma, Snigdha and Tiksna.
Veerya : Ushna.
Vipaka: Madhura.
DoshaKarma:kaphavatasamaka.
Rogaghnakarma- Shulagna, sothaghna, katisulagna, bastirogahara, sirasulahara,
udararogahara, jvaraghna, svasghna, kasaghna, Kusthaghna, amavatahara, saumya,
samsrana, stanyajanana, dahasamaka, vrsya, bhedani, svedopaga,
angamardaprasamana, adhobhagahara, snehana, vedanasthapana, krmighna.
Chemical Constituents: The alkaloids, fixed oil, glycerides, recinole acid etc.
Methodology
Efficacy of lashuna rasayana in manibandha marmabhighata Page 48
METHODOLOGY
Objective of Study-
Efficacy of a Lashuna rasayana on disease severity in patients suffering from
Manibhandha marmabhighata / Carpal tunnel syndrome.
Effect on functional disability in patients of Manibhandha marmabhighata /
Carpal tunnel syndrome treated with lashuna rasayana.
MATERIALS AND METHODS -
Source of data:
15 patients diagnosed as manibandha marmabhighata / carpel tunnel syndrome
were taken for study from OPD and IPD of Sri Dharmasthala Manjunatheshwara
Ayurveda Hospital, Kuthpady, 574118. The freeze dried powder of lashuna is
obtained in the 500 mg capsule from the Sri Dharmasthala Manjunatheshwara
Ayurveda Pharmacy.
Method of collection of data:
A specific proforma was prepared incorporating all points of history taking,
physical signs, and symptoms as mentioned in Ayurveda as well as bio medicine.
DESIGN OF THE STUDY:
Study Type : Interventional
Actual Enrollment : 15 participants
Allocation : Non-Randomized
Endpoint Classification : Efficacy Study
Intervention Model : Single Group Assignment
Masking : Open Label
Primary Purpose : Treatment
Study Start Date : October 2017
Study Completion Date : February 2018

Methodology
Efficacy of lashuna rasayana in manibandha marmabhighata Page 49
The patients were selected irrespective of gender, cast, race, religion, based on
the diagnostic inclusion and exclusion criteria. All the parameter of signs, symptoms
is scored as enlisted in the assessment criteria and the result obtained was statistically
analyzed by the paired t test.
Diagnostics Criteria:
Signs and symptoms Manibandha marmabhighata / Carpal tunnel syndrome
(paresthesia in the distribution of median nerve distal to wrist, weak hand grip,
wasting of muscles at the thenar eminence and positive tinels and phalen sign).
Inclusion Criteria:
Subjects with a clinical diagnosis of Manibandha marmabhighata / Carpal
tunnel syndrome.
Subjects must be between 16 to 70 years of age (both ages inclusive).
Subjects of both genders.
Having signed a written informed consent form.
Exclusion Criteria:
Patients with uncontrolled Diabetes Mellitus & Hypertension.
Patients with Fracture of wrist.
Subjects with history of excessive menstruation.
Patients who are pregnant by patient report or intending to become pregnant
during the study.
Patients that have been previously diagnosed with cervical radiculopathy.
ASSESSMENT CRITERIA
Primary outcome measures
Questionnaire of Levine et al for Clinical Assessment of Carpal Tunnel
Syndrome [Time Frame: Baseline, day 17]
Secondary outcome measures:
Change in Grip strength (Dynamometer) [Time Frame: Baseline, day 17]
Change in Visual Analog Scale for pain [Time Frame: Baseline, day 17]
Methodology
Efficacy of lashuna rasayana in manibandha marmabhighata Page 50
Participants Assessment of numbness Over Time by the method of visual
analog scale (VAS) ranging from 0 (best) to 10 (worst) cm
[Time Frame: Baseline, day 17]
Intervention:
Koshta shodhana on Day 1 : Oral administration of eranda taila in empty
stomach, in a dose of 20 ml in the morning
along with 100 ml of warm water as after
drink.
Lashuna Rasayana on Day 2
to 16
: Oral administration of lashuna rasayana in a
dose of 12 g in empty stomach half an hour
before breakfast along with 100 ml of milk107
as after drink.
Pitta virechana108
on Day 17 : Oral administration of eranda taila in empty
stomach, in a dose of 20 ml in the morning
along with 100 ml of warm water as after drink
Follow up duration: 30 days
Total duration of study: 47days.
Clinical Assessment of Carpal Tunnel Syndrome (Levine et al)
A self-administered questionnaire can be used to assess the severity of
symptoms and functional impairment in patients with the carpal tunnel syndrome.
This can be used over time to monitor the effect of therapeutic interventions on the
course of the disease.
Parts to questionnaire:
(1) Symptoms severity scale
(2) Functional status scale
Symptom Severity Scale- over the past 2 weeks
(1) Severity of pain at night
(2) Waking up from pain
(3) Pain during daytime
(4) Frequency of daytime pain
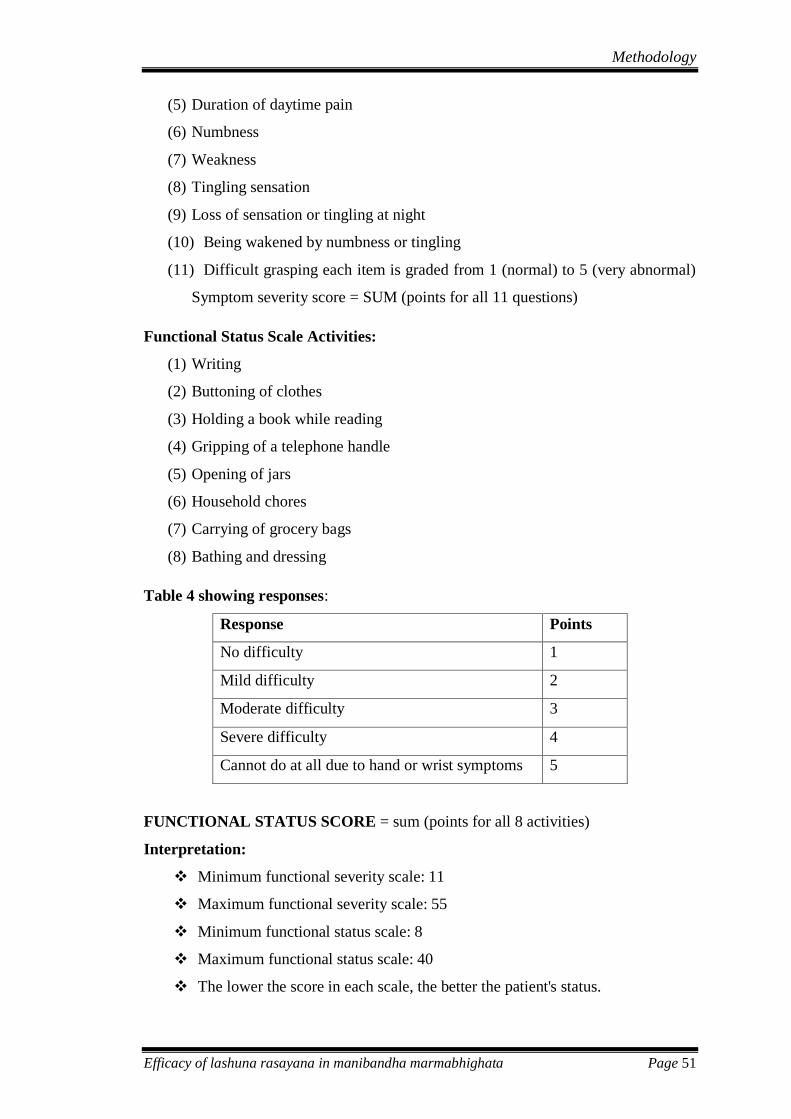
Methodology
Efficacy of lashuna rasayana in manibandha marmabhighata Page 51
(5) Duration of daytime pain
(6) Numbness
(7) Weakness
(8) Tingling sensation
(9) Loss of sensation or tingling at night
(10) Being wakened by numbness or tingling
(11) Difficult grasping each item is graded from 1 (normal) to 5 (very abnormal)
Symptom severity score = SUM (points for all 11 questions)
Functional Status Scale Activities:
(1) Writing
(2) Buttoning of clothes
(3) Holding a book while reading
(4) Gripping of a telephone handle
(5) Opening of jars
(6) Household chores
(7) Carrying of grocery bags
(8) Bathing and dressing
Table 4 showing responses:
Response Points
No difficulty 1
Mild difficulty 2
Moderate difficulty 3
Severe difficulty 4
Cannot do at all due to hand or wrist symptoms 5
FUNCTIONAL STATUS SCORE = sum (points for all 8 activities)
Interpretation:
Minimum functional severity scale: 11
Maximum functional severity scale: 55
Minimum functional status scale: 8
Maximum functional status scale: 40
The lower the score in each scale, the better the patient's status.
Methodology
Efficacy of lashuna rasayana in manibandha marmabhighata Page 52
Change in grip strength (dynamometer)
Hand Dynamometer used here was measuring isometric grip force from 0-
130 kg. It was handy and reliable. It was made of plastic material. Patient had to
squeeze the hand dynamometer with maximum isometric efforts.
Visual analog scale for pain / numbness
It is a continuous scale comprising a horizontal visual analog scale 0- 10
readings. Lesser the reading by patient less is the pain where as more the reading
more is the pain.
Results
Efficacy of lashuna rasayana in manibandha marmabhighata Page 67
EFFECT OF TREATMENT
15 Patients suffering from manibandha marmabhighata were diagnosed and
screened under strict diagnostic, inclusion and exclusion criteria and were registered
for the study. These patients were invited to participate in the study after signing a
detailed informed consent prior to beginning of the study. These subjects were given
koshta shodhana on the day one of the intervention with oral administration of eranda
taila in empty stomach, in a dose of 20 ml in the morning along with 100 ml of warm
water as after drink. From day 2 to 16 patients were given lashuna rasayana in a dose
of 12 g in empty stomach half an hour before breakfast along with 100 ml of milk as
after drink. On the 17 the day pitta virechana was done by oral administration of
eranda taila in empty stomach, in a dose of 20 ml in the morning along with 100 ml of
warm water as after drink. All 15 patients completed the full treatment course
comfortably with no any adverse manifestations. Results of the intervention were
assessed by the following outcome measures and same is elaborated in this chapter.
Primary outcome measures
Symptom severity.
Functional disability status.
Secondary outcome measures:
Pain .
Numbness.
Grip strength (Dynamometer).
Overall effect.
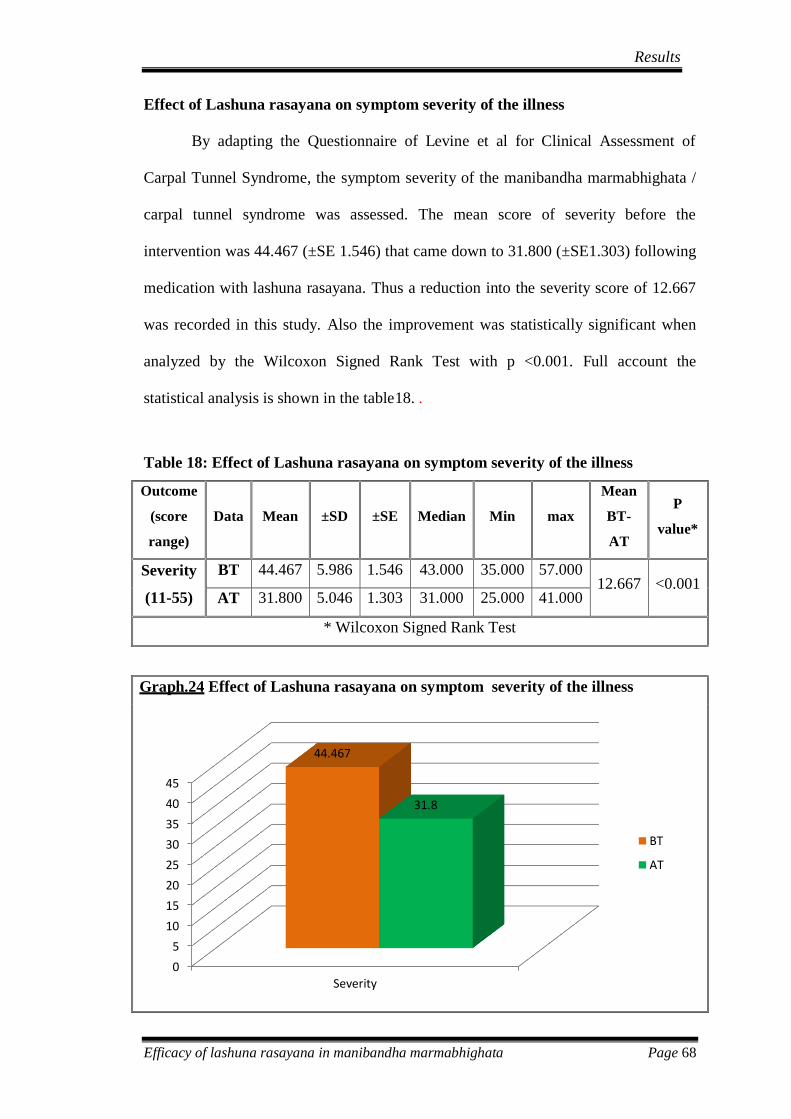
Results
Efficacy of lashuna rasayana in manibandha marmabhighata Page 68
Effect of Lashuna rasayana on symptom severity of the illness
By adapting the Questionnaire of Levine et al for Clinical Assessment of
Carpal Tunnel Syndrome, the symptom severity of the manibandha marmabhighata /
carpal tunnel syndrome was assessed. The mean score of severity before the
intervention was 44.467 (±SE 1.546) that came down to 31.800 (±SE1.303) following
medication with lashuna rasayana. Thus a reduction into the severity score of 12.667
was recorded in this study. Also the improvement was statistically significant when
analyzed by the Wilcoxon Signed Rank Test with p <0.001. Full account the
statistical analysis is shown in the table18. .
Table 18: Effect of Lashuna rasayana on symptom severity of the illness
Outcome
(score
range)
Data Mean ±SD ±SE Median Min max
Mean
BT-
AT
P
value*
Severity
(11-55)
BT 44.467 5.986 1.546 43.000 35.000 57.000 12.667 <0.001
AT 31.800 5.046 1.303 31.000 25.000 41.000
* Wilcoxon Signed Rank Test
Graph.24 Effect of Lashuna rasayana on symptom severity of the illness
0
5
10
15
20
25
30
35
40
45
Severity
44.467
31.8
BT
AT
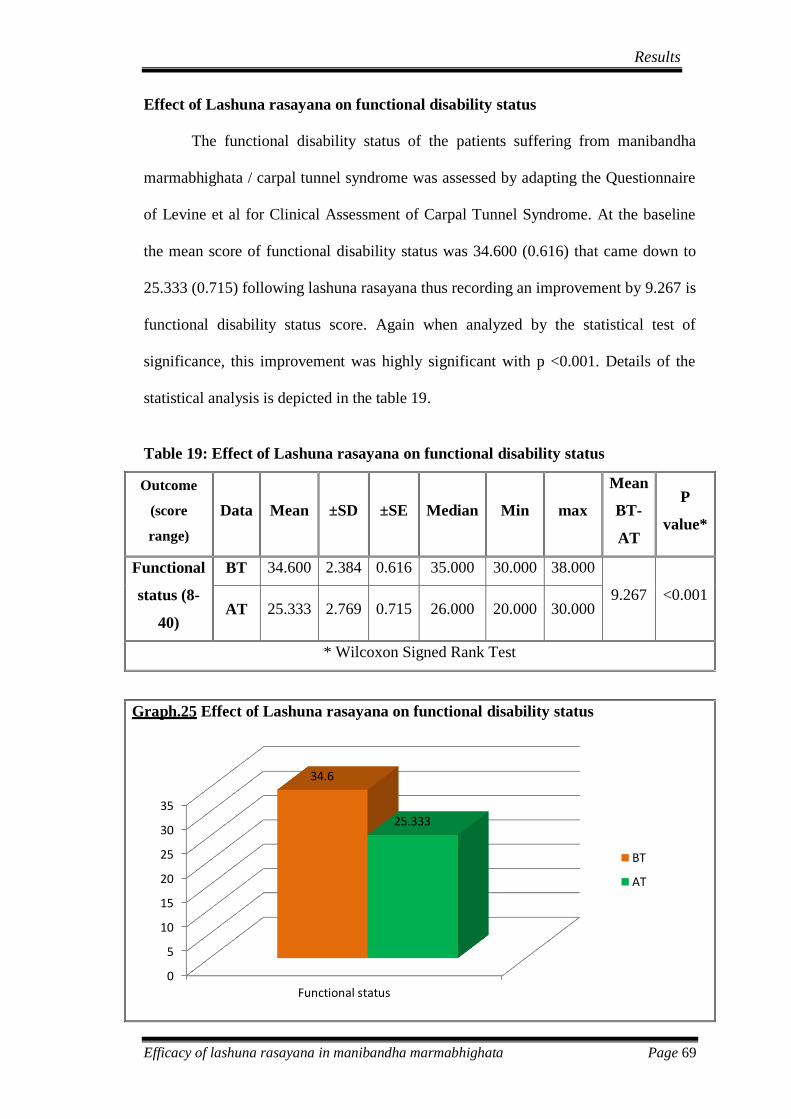
Results
Efficacy of lashuna rasayana in manibandha marmabhighata Page 69
Effect of Lashuna rasayana on functional disability status
The functional disability status of the patients suffering from manibandha
marmabhighata / carpal tunnel syndrome was assessed by adapting the Questionnaire
of Levine et al for Clinical Assessment of Carpal Tunnel Syndrome. At the baseline
the mean score of functional disability status was 34.600 (0.616) that came down to
25.333 (0.715) following lashuna rasayana thus recording an improvement by 9.267 is
functional disability status score. Again when analyzed by the statistical test of
significance, this improvement was highly significant with p <0.001. Details of the
statistical analysis is depicted in the table 19.
Table 19: Effect of Lashuna rasayana on functional disability status
Outcome
(score
range)
Data Mean ±SD ±SE Median Min max
Mean
BT-
AT
P
value*
Functional
status (8-
40)
BT 34.600 2.384 0.616 35.000 30.000 38.000
9.267 <0.001 AT 25.333 2.769 0.715 26.000 20.000 30.000
* Wilcoxon Signed Rank Test
Graph.25 Effect of Lashuna rasayana on functional disability status
0
5
10
15
20
25
30
35
Functional status
34.6
25.333
BT
AT
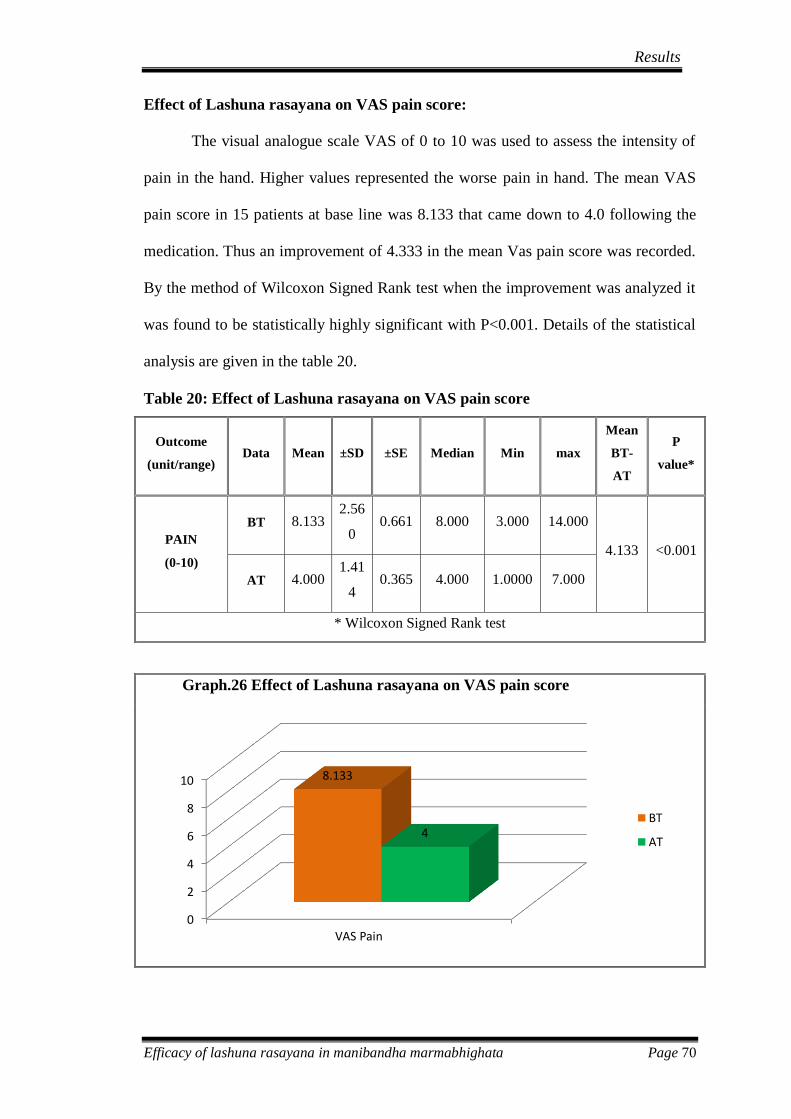
Results
Efficacy of lashuna rasayana in manibandha marmabhighata Page 70
Effect of Lashuna rasayana on VAS pain score:
The visual analogue scale VAS of 0 to 10 was used to assess the intensity of
pain in the hand. Higher values represented the worse pain in hand. The mean VAS
pain score in 15 patients at base line was 8.133 that came down to 4.0 following the
medication. Thus an improvement of 4.333 in the mean Vas pain score was recorded.
By the method of Wilcoxon Signed Rank test when the improvement was analyzed it
was found to be statistically highly significant with P<0.001. Details of the statistical
analysis are given in the table 20.
Table 20: Effect of Lashuna rasayana on VAS pain score
Outcome
(unit/range) Data Mean ±SD ±SE Median Min max
Mean
BT-
AT
P
value*
PAIN
(0-10)
BT 8.133 2.56
0 0.661 8.000 3.000 14.000
4.133 <0.001
AT 4.000 1.41
4 0.365 4.000 1.0000 7.000
* Wilcoxon Signed Rank test
Graph.26 Effect of Lashuna rasayana on VAS pain score
0
2
4
6
8
10
VAS Pain
8.133
4 BT
AT
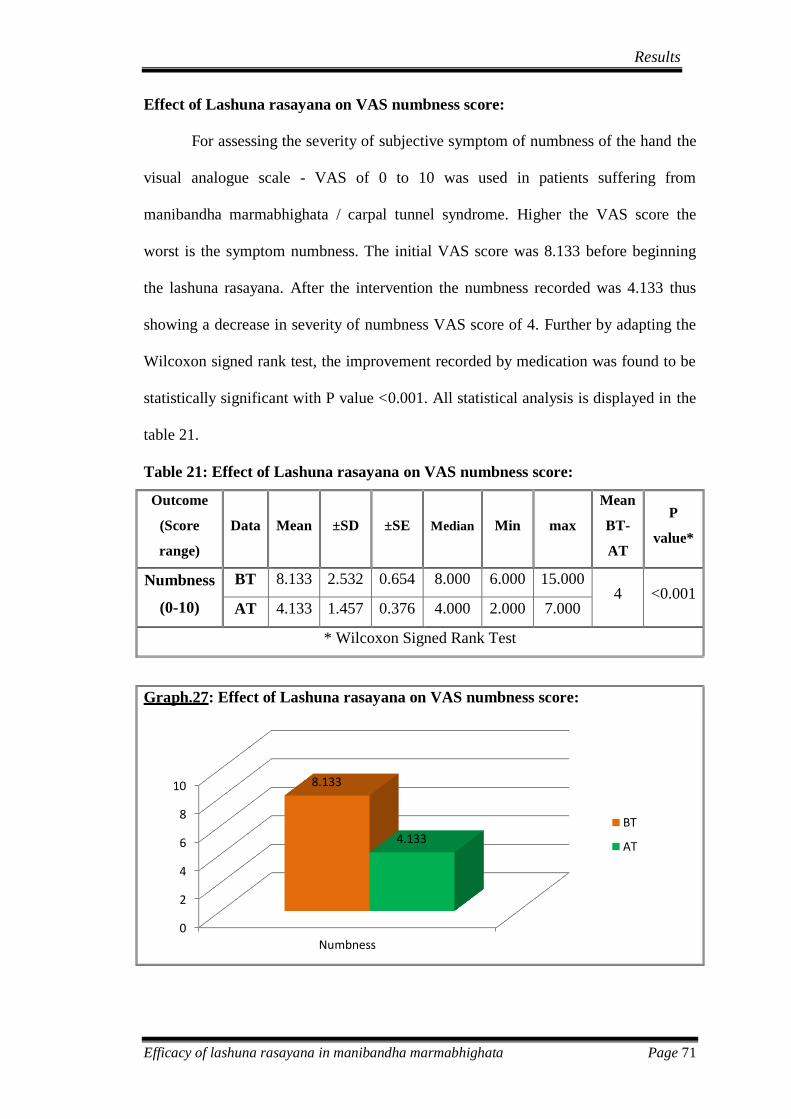
Results
Efficacy of lashuna rasayana in manibandha marmabhighata Page 71
Effect of Lashuna rasayana on VAS numbness score:
For assessing the severity of subjective symptom of numbness of the hand the
visual analogue scale - VAS of 0 to 10 was used in patients suffering from
manibandha marmabhighata / carpal tunnel syndrome. Higher the VAS score the
worst is the symptom numbness. The initial VAS score was 8.133 before beginning
the lashuna rasayana. After the intervention the numbness recorded was 4.133 thus
showing a decrease in severity of numbness VAS score of 4. Further by adapting the
Wilcoxon signed rank test, the improvement recorded by medication was found to be
statistically significant with P value <0.001. All statistical analysis is displayed in the
table 21.
Table 21: Effect of Lashuna rasayana on VAS numbness score:
Outcome
(Score
range)
Data Mean ±SD ±SE Median Min max
Mean
BT-
AT
P
value*
Numbness
(0-10)
BT 8.133 2.532 0.654 8.000 6.000 15.000 4 <0.001
AT 4.133 1.457 0.376 4.000 2.000 7.000
* Wilcoxon Signed Rank Test
Graph.27: Effect of Lashuna rasayana on VAS numbness score:
0
2
4
6
8
10
Numbness
8.133
4.133 BT
AT
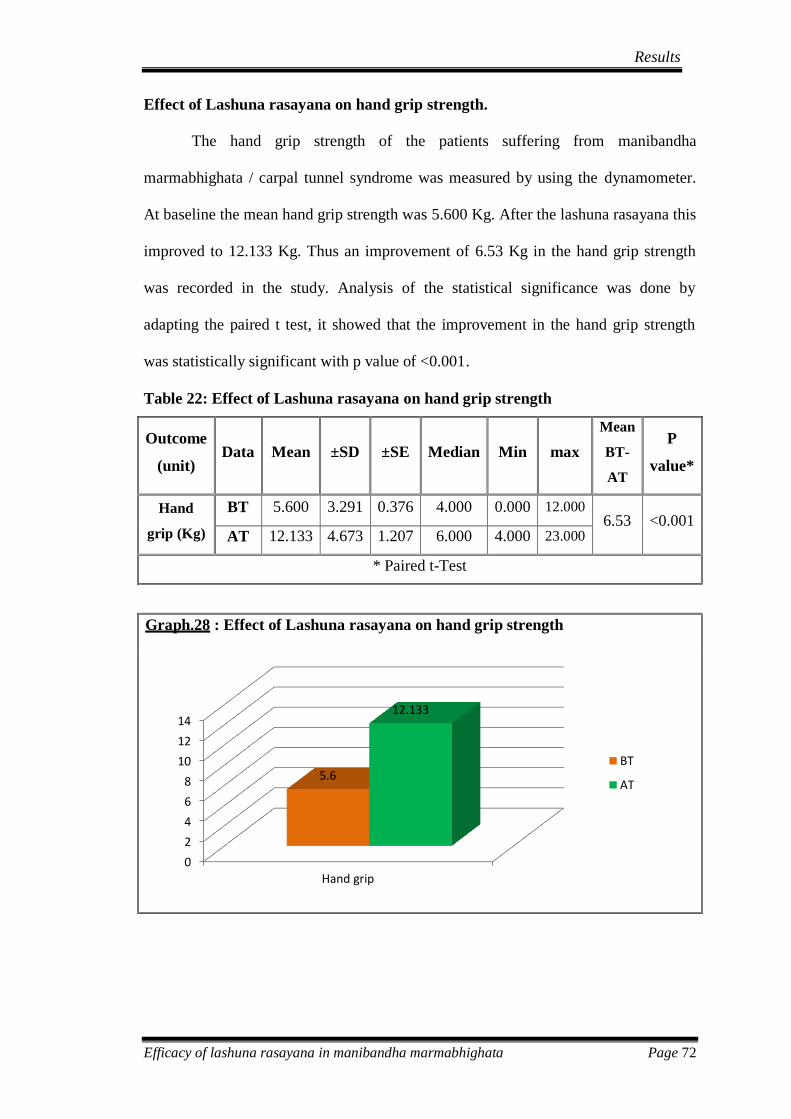
Results
Efficacy of lashuna rasayana in manibandha marmabhighata Page 72
Effect of Lashuna rasayana on hand grip strength.
The hand grip strength of the patients suffering from manibandha
marmabhighata / carpal tunnel syndrome was measured by using the dynamometer.
At baseline the mean hand grip strength was 5.600 Kg. After the lashuna rasayana this
improved to 12.133 Kg. Thus an improvement of 6.53 Kg in the hand grip strength
was recorded in the study. Analysis of the statistical significance was done by
adapting the paired t test, it showed that the improvement in the hand grip strength
was statistically significant with p value of <0.001.
Table 22: Effect of Lashuna rasayana on hand grip strength
Outcome
(unit) Data Mean ±SD ±SE Median Min max
Mean
BT-
AT
P
value*
Hand
grip (Kg)
BT 5.600 3.291 0.376 4.000 0.000 12.000 6.53 <0.001
AT 12.133 4.673 1.207 6.000 4.000 23.000
* Paired t-Test
Graph.28 : Effect of Lashuna rasayana on hand grip strength
0
2
4
6
8
10
12
14
Hand grip
5.6
12.133
BT
AT
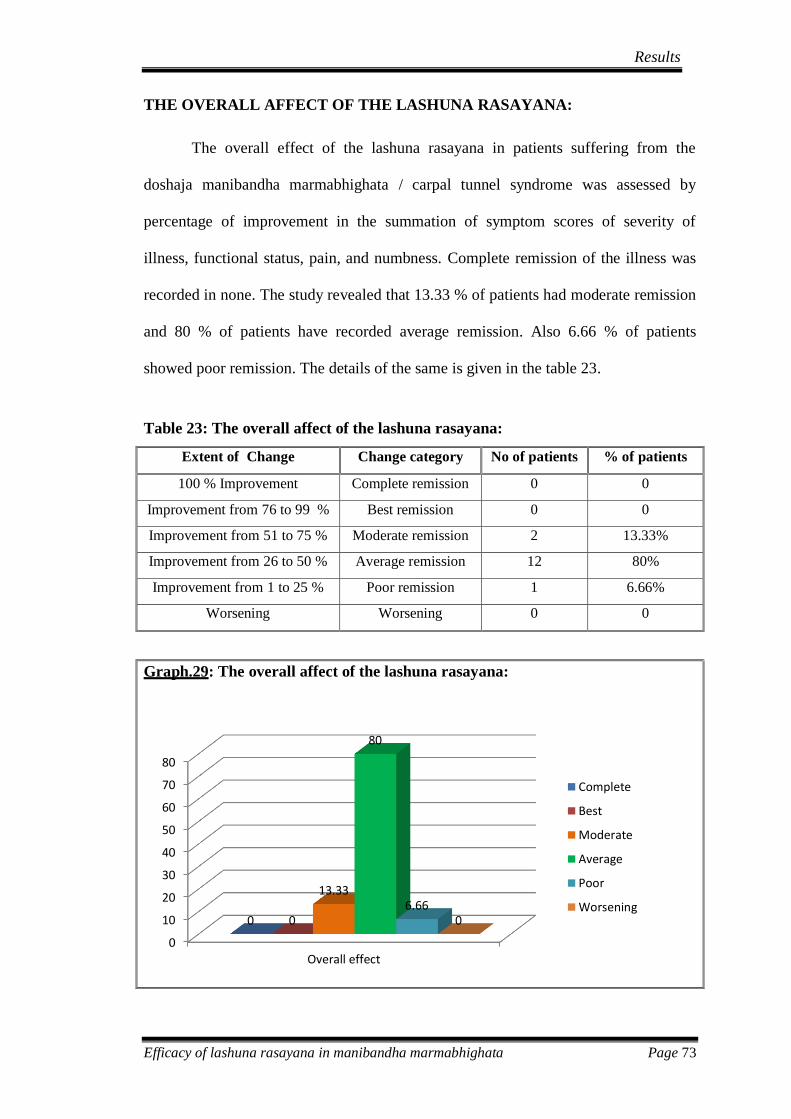
Results
Efficacy of lashuna rasayana in manibandha marmabhighata Page 73
THE OVERALL AFFECT OF THE LASHUNA RASAYANA:
The overall effect of the lashuna rasayana in patients suffering from the
doshaja manibandha marmabhighata / carpal tunnel syndrome was assessed by
percentage of improvement in the summation of symptom scores of severity of
illness, functional status, pain, and numbness. Complete remission of the illness was
recorded in none. The study revealed that 13.33 % of patients had moderate remission
and 80 % of patients have recorded average remission. Also 6.66 % of patients
showed poor remission. The details of the same is given in the table 23.
Table 23: The overall affect of the lashuna rasayana:
Extent of Change Change category No of patients % of patients
100 % Improvement Complete remission 0 0
Improvement from 76 to 99 % Best remission 0 0
Improvement from 51 to 75 % Moderate remission 2 13.33%
Improvement from 26 to 50 % Average remission 12 80%
Improvement from 1 to 25 % Poor remission 1 6.66%
Worsening Worsening 0 0
Graph.29: The overall affect of the lashuna rasayana:
0
10
20
30
40
50
60
70
80
Overall effect
0 0
13.33
80
6.66 0
Complete
Best
Moderate
Average
Poor
Worsening
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 74
DISCUSSION
Hand is prehensile, multi fingered appendage located at end of forearm in
humans. It plays an important function in body language and sign language. Ten
digits of two hands and twelve phalanges of four fingers have given rise to systems
and calculation techniques. Wrist joint support movements of hand and forearm
.sports and manual works involve complicated and coordinated activities of hand and
wrist joint. It is second most active joint after ankle joint. This joint is affected in the
doshaja Manibandha marmabhighata / Carpal tunnel syndrome.
The perceptions of marma are discussed with two distinct perspectives in the
literature. External trauma and internal injury due to morbid dosha may present with
clinical condition of marmabhighata. The surgical school of thought has described the
marma with more emphasis on traumatic injury and surgical intervention. On the
other hand the same topic is marma is elaborated in the medical school of thought
with the objective of diagnosing internal injury due to morbid dosha and conservative
medical management. This is also true in relation to Manibandha marmabhighata. The
description of marmabhighata comes under the topic of possible external injuries. In
the medical school of thought marmabhighata is mostly cited in under the umbrella
term of nanatmaja vata vyadhi.
Vata vyadhi is considered as most virulent among the tridosha. Among the
diseases caused by vitiation of vata dosha, samanya & nanatmaja vyadhi presents with
distinct features. Literature quotes 80 types of nanatmaja vata vyadhi that is specified
as aavishkritatama vata vyadhi. The description of some of these diseases is vivid in
the literature and elaboration of some is restricted to guidelines. In general vata dosha
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 75
is diagnosed based on symptoms of aggravation of vata dosha and location of
affliction. Nakha bheda, Paada shola, Paada supthi are just the examples.
Kuntata is a disorder characterised by the paralysis related to the activities of
hand. Scanning of literature explores the better explanation of the condition with due
consideration of abhighata nidana in manibandha as rujakara marma.
Etiological factors of vata vyadhi such as strain caused due to exposure of
vyayama, abnormal positioning during different activities is worth considering. These
etiological factors have direct bearing on joints. To be more precise the excessive and
abnormal activities of involving the hand may affect the manibandha marma.
Affection of manibandha marma is the key pathology as per the understanding of
marmabhighata.
The Manibandha marmabhighata can happen for two reasons, they are the
internal factor & external factor. External by the way of different activities related
to bahya abhighata involving the manibandha. In contrast to santarpana nidhana
causing excessive kapha & medas can lead to avarana vata vyadhi and can involve the
manibhandha marma leading to margavaranajanya Manibandha marmabhighata
similar to the samprapti of urustamabha. Here the marga refers to vatavaha srotas.
Manibandha marmabhighata is caused either external factors or internal factors like
santarpana nidana resulting in vata vyadhi. Literature affirms the role of
marmabhighata in causation of vatavyadhi.
Manibandha marmabhighata when it happens for above said reasons result in
manifestation of supta, ruja, kuntata, vastushukairavakirna,shosha,parvashopha.These
symptoms, comprising of Manibandha marmabhighata; parallels with symptom of
Carpal tunnel syndrome. The symptoms of Manibandha marmabhighata include
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 76
suptata (paresthesia), ruja (pain) and kuntata (paralysis of the hand leading to
functional disability) .Thus these symptoms match with that Carpal tunnel syndrome.
Carpal tunnel syndrome may be caused due to obesity, trauma, pregnancy and
inflammation etc.These etiological factor either belonging to the category of
santarpana nidana or injury to wrist by physical activities. The pathology of
margavarana / abhighata in manibandha is parallel to median nerve entrapment in
carpal tunnel.
Manibandha marmabhighata and the resulting vatavyadhi is treated according
to the treatment of vatavyadhi by snehana, svedana, brimhana and rasayana. Balanced
approach rectifying the kapha and medas and simultaneously normalizing the
functions of the vatadosha is the sheet anchor of treating Manibandha marmabhighata
leading to kuntata.
Needless to say rasayana cikitsa has got an edge over any other conservative
management. Also Lashuna rasayana is effective in both clearing the co morbidity of
margavarana as well as pacification of vitiated vata dosha thus proving its superiority
in the management of Manibandha marmabhighata. Pilot study has shown favorable
response in patient suffering from Manibandha marmabhighata treated with Lashuna
rasayana. Hence this study is intended to evaluate the therapeutic effect of Lashuna
rasayana in patient suffering from Manibhandha marmabhighata / Carpal tunnel
syndrome.
Review of literature
Marma are the unique vital points in the body. Strong blow on these marma
can cause significant injury and may even prove fatal. Contrary to this a mild touch of
these vital points can cause healing. The whole practice of marma therapy is based on
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 77
this understanding. The knowledge of marma is essential for planning surgical
interventions. The seriousness of any trauma is judged by the involvement of marma.
The same marma knowledge is used in the martial arts to kill the opponent. Most
recently the same knowledge is utilized to treat certain diseases. To be clearer, the
knowledge of marma is traced back to Vedic literature and has progressed to the
present marma therapy practiced in the southern part of the India known by the name
Kalaripayattu.
Nirukti and paribhasha-
The word Manibandha marmabhighata has three component as manibhandha
marma and abhighata.The Sanskrit word manibandha in masculine gender is formed
by the combination of two component terms of Mani and bandha with the addition of
suffix ghanj. Mani refers to the jewels. Bandha refers to the act of fastening or
binding. Put together, etymologically the fastening of the jewel is known as
manibhandha. The joint between the forearm and hand is called as manibandha. It is
identified as the base of hand and is located proximal to the palm. Marma refers to a
body location and injury to which tend to cause death. The Sanskrit word abhighata in
masculine gender is derived from the Sanskrit root “han” with the prefix “abhi”. The
Sanskrit root “han” refers to the activity of striking or attack. Again this injury may be
due to external trauma or internal injury caused by morbid dosha. In short, internal or
external injury to the vital organ of wrist is known as manibandha marmabhighata.
NIDANA
Manibandhamarmaghata happens due to santarpananidana and
apatarpananidana. . Therefore considering the nidana, maximum patients suffering
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 78
from the apatarpananidana were witnessed in this study. About 80% of the patients
belonged to this category. This may be due to injury or professional causes. Patient in
the study, were found with excessive usage of hands in their activities may be the
involving the house hold activities like lifting heavy materials ,washing cloths etc..
Professionally tailors and bankers were found to be the culprits of this disease.
Considering the santarpananidana only 20% of patients were found who were obese,
as carpal tunnel syndrome occurs due to fat deposition in the wrist around the carpal
bone hence compressing the median nerve which passes within it.
ROOPA
Manibandha marmabhighata will present with symptoms like suptata, ruk,
Vastushukairavakirna, shosha, parvashopa, all the patients in the present study had
pain and numbness in their thumb, forefinger, middle finger and radial half of ring
finger which signifies the median nerve entrapment. In physical examination sensory,
motor deficits and the specific tests like Hoffmann tinel sign, Phalen sign were
present in the patient.
SAMPRAPTHI
Vitiated vatadosha afflicting the sira and snayu at the manibandha marma
leads to the clinical manifestation of the manibandha marmabhighata. The
pathophysiology of the disease goes in two modes according to the nidana. Injury to
any marma can happen due to santarpana or aptarpananidana. Santarpananidana
results into fat accumulation around the surface of wrist, thus causing compression to
the carpal tunnel eventually leading to entrapment of median nerve. Apatarpana
factors are any kind of injury or professional cause i.e. over usage of hands, example-
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 79
tailors, typists, etc. Exposure to the different nidana like physical activities and
external traumatic factors mentioned in vatavyadhi, leads to vitiation of vatadosha in
the effected part leading to symptoms like supta, ruk, kuntata, shosha,
vastuhukaivakirna and parvashopha leading to Manibandha marmabhighata.
Considering the santarpana nidana, exposure of santarpana nidana in terms of
ahara and vihara, leads to increase kapha and medas obstructing the marga leading to
aggravation of vata causing the Manibandha marmabhighata. The pathophysiology
may be different in two case but it has a common culprit, the vatadosha leading to
Manibandha marmabhighata at the end.
UPADRAVA
The morbid event developed by the manifestation of main disease after its
genesis is upadrava. It is the complication of the disease seen after the fully
manifested disease. Hence considering the manibandha marmabhighata where
“kuntata” is seen as the upadrava. Kuntata is defined as “karasyaakarmanyavat” ie
functional loss of the hand. In parallel science we can consider it functional loss in the
activities due to immense pain or paresthesia leading to disability of hand and atrophy
of thenar eminence seen in carpal tunnel syndrome.
CHIKITSA
Literature specifies various kinds of treatment mentioned in vata roga. Though
samprapti is different for the mode of causation of disease according to the factors but
at the end it is vatadosha that is to be controlled and pacified. Hence demand of such a
drug is necessary which will not only pacify vata but also does the samprapthi
vighatana of the both samprapti and there by curing the disease. The pathology may
be further complicated by the margavarana at the manibandha by the kapha and
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 80
medas that causes pain, numbness etc. Balanced approach rectifying the kapha and
medas and simultaneously normalizing the functions of the vatadosha is the sheet
anchor of treating manibandha marmabhighata leading to kuntata. Needless to say
rasayana cikitsa has got an edge over any conservative management. Also lashuna
rasayana is effective in both clearing the co morbidity of margavarana as well as
pacification of vitiated vatadosha thus proving its superiority in the management of
margavaranja manibandha marmabhighata as well as the one caused by external
factor.
Pathya – Apathya.
Manibandha marmabhighata is a vatavyadhi .hence pataypathya of vatavyadhi
is to be followed. Literature specifies dietetic, lifestyle rules and regimens, which on
following brings the morbid vatadosha to the normalcy.
In case of Vatavyadhi, Vatashamaka Ahara Vihara has been given
importance. In general, Mamsarasa, Paya, Madhura, Amla, Lavana Rasa yuktadravya,
and Brimhana have been advised. Hence one has to balance the food according to the
causation of disease. If the pathology is margavarana then one has to avoid the
santarpana ahara vihara along with vatashamaka drugs so that the dosha is maintained
in their normalcy.
Carpal tunnel syndrome.
Manibandha marmabhighata is compared to that of carpal tunnel syndrome. It
is caused by entrapment of median nerve within the carpal tunnel either due to injury
or by the fat deposition around the wrist compressing the median nerve within the
carpal tunnel. It presents with with typical symptoms, paresthesia of thumb,

Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 81
forefingers, middle finger and radial half of ring finger, atrophy of thenar eminence
etc.. causing the sensory and the motor deficits. The definite diagnostic signs are the
tinel’s sign and phalen’s sign. The treatment among the modern medicine is limited
just to steroids and painkillers. If not controlled by both of these surgery is the
ultimate option without the assurance of its cure.
Drug Review
Lashuna rasayana is chosen as the drug as it is a best drug of choice for both
the pathologies. It is said to be best in the vataroga as well as in clearing the
margavarana. Hence this drug is taken for the study and administered in avara dose
.The freeze dry powder of this drug was used in capsules containing 500mg each as it
is more palatable than the crude drug. 12 g was given for total of 15 days with prior
koshta shodhana with eranda taila .Eranda is said to be best in vata roga as well as
clearing the margavarana. At the end pitta virechana was done due to the usual
tendency of aggravation of pitta dosha and is achieved by oral administration of
eranda taila.
Methodology
As discussed in chikitsa, Lashuna rasayana is used to treat patient suffering
from manibandha marmabhighata / carpal tunnel syndrome. An open label, single
arm, non randomized efficacy study was planned to evaluate the therapeutic effect of
Lashuna rasayana. The patients were selected with no any restriction of gender and
cast for the study by strict screening as per the diagnostic, inclusion and exclusion
criteria.
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 82
Signs and symptoms of manibandha marmabhighata / carpal tunnel syndrome
(paresthesia in the distribution of median nerve distal to wrist, weak hand grip,
wasting of muscles at the thenar eminence and positive tinels and phalen sign) is
taken as diagnostic criteria. Patients of both genders between the age group of 16 to
70 years of age were included in the study. Also the patients with uncontrolled
Diabetes Mellitus, uncontrolled hypertension, fracture of wrist, history of excessive
menstruation, pregnant / lactating females and patients with cervical radiculopathy
were excluded from the study. 15 participants who have signed a written informed
consent form were registered in the study.
The participants included in the study received koshta shodhana on the day
one of the treatment as shodhana is mandatory prior to any rasayana treatment. For
this purpose Eranda taila was orally administered in a dose of 20 ml in the morning
along with 100 ml of warm water as after drink. Lashuna rasayana was administered
on Day 2 to 16 in a dose of 12 g in empty stomach half an hour before breakfast along
with 100 ml of milk as after drink. This was followed by Pitta virechana on Day 17 in
the form of oral administration of Eranda taila in empty stomach, in a dose of 20 ml in
the morning along with 100 ml of warm water as after drink. It is said that Lashuna
rasayana tend to cause accumulation of the pitta dosha hence to clear the
accumulation of pitta dosha pitta virechana is planned by the end of Lashuna
rasayana. For recording the results the patients are assessed by way of primary and
secondary out come measures at base line and 17th
day.
Observation
Out of 15 patients included in the study 6.66% of patient belonged to age
group of 16-30 years .33.33% belonged to 31-50 years and 60% belonged to 51-70
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 83
years. Patients are more in age group of 51-70 years as these set of patients are more
exposed to the trauma and professional wear and tear. Patients within the age group of
31-50 were the second highest ones as they were next to the maximum exposed ones.
Maximum of patients were females comprising total of 86.66%. Most of the
females are engaged in house hold activities which involves maximum usage of
hands. For example cleaning utensils, cooking, washing clothes etc. Probably this has
accounted for the higher incidence of the illness in the present sample. 86.66% of the
patients were of Hindu religion in this study. This only represent the dominance of
Hindu population in and around Udupi, from where this sample is taken. As such the
Hindu religion has nothing to do with the causation of the illness.
As the study was carried out in adults excluding children and seniors, 93.3%
of the patients were married and only 6.66% were widowed in the present study.
Out of the 15 patients, 66.66% were housewives and 20% were working as
tailors. These people use their wrist extensively in the professional activities and
hence have bearing in the causation of illness Manibandha marmabhighata / Carpal
tunnel syndrome.
Majority of the patient belonged to middle class family as these people do
enough physical activities for their lively hood tend to suffer from Manibandha
marmabhighata in comparison to the people of higher class who lead a leisurely life.
The participants of the study are selected from the costal belt, and hence a
maximum of 73.33% patients had mixed diet and they mostly consume sea food.
Excessive consumption of such foods may predispose to overweight and obesity. This
in turn may contribute to the etiopathogenesis of manibandha marmabhighata. This
fact should be considered when planning pathya-apathya in such patients.

Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 84
Disturbed sleep was recorded in 75% of the patients in this study. Partially the
disturbance is due to the discomfort in the hand related to the Manibandha
marmabhighata / carpal tunnel syndrome.
In most of the other patient the exact cause of the disturbed sleep could not be
confirmed. 80% of patients had the habit of sleeping in the afternoon. This is obvious
as majority housewives were involved in the study who would be tired at the noon
due to household work.
An enquiry about the habit revealed that all patients had the habit of taking
tea or coffee. Around 13.33% of the patients were addicted to tobacco chewing or
smoking cigarettes.
20% of the patient had a family history of Carpal tunnel syndrome. This is
because 3 patients had family history of obesity. Other 80% did not have family
history of carpal tunnel.
Out of 15 patients 46.66% of the patients belonged to each of vata pitta and
kapha vata prakriti. 6.66% belonged to pitta kapha prakriti. 80 % of the patients had
madhyama sara. 40% of the patients showed madhyama samhanaana. A majority of
66.66% had madhyama satva. Madhyama type of vyayama shakthi was recorded in
46.66% of patients. 73.33% of the patients had madhyama abhyavaharana shakthi
Majority of 80% patients of the study had madhyama jaranashakthi followed by
another 13.33% with the avara jaranashakthi.
Out of the 15 patients, 73.33 % of patients had gradual onset of symptoms as
against 26.66% of patients complained of sudden onset of illness. The symptom of
ruk / pain, supti / numbness and kuntata / reduced hand grip was recorded in all the 15
patients of manibandha marmabhighata / carpal tunnel syndrome. In 80 % of patients
the over strain of the wrist during different professional or house hold activity is
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 85
recognized as major cause of illness in the form of bahya abhighata. No such cause
could be recorded in 20 % of patients pointing towards the internal injury as the cause
of Manibandha marmabhighata / carpal tunnel syndrome.
RESULTS
The mean score of severity before the intervention was 44.467 (±SE 1.546)
that came down to 31.800 (±SE1.303) following medication with Lashuna rasayana.
Thus a reduction into the severity score of 12.667 was recorded in this study. At the
baseline the mean score of functional disability status was 34.600 (0.616) that came
down to 25.333 (0.715) following Lashuna rasayana thus recording an improvement
by 9.267 is functional disability status score. The visual analogue scale VAS of 0 to
10 was used to assess the intensity of pain in the hand. Higher values represented the
worse pain in hand. The mean VAS pain score in 15 patients at base line was 8.133
that came down to 4.0 following the medication. Thus an improvement of 4.333 in the
mean Vas pain score was recorded. The initial VAS score was 8.133 (±SE 0.654)
before beginning the Lashuna rasayana. After the intervention the numbness recorded
was 4.133 (±SE 0.376) thus showing a decrease in severity of numbness VAS score of
4. At baseline the mean hand grip strength was 5.600 Kg. After the Lashuna rasayana
this improved to 12.133 Kg. Thus an improvement of 6.53 Kg in the hand grip
strength was recorded in the study. All these changes following medication with
Lashuna rasayana was subjected to Wilcoxon Signed Rank Test or Paired t-Test
depending upon the type of variables and the improvement observed was found to be
statistically highly significant with P value <0.001. Thus it can be said that the
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 86
improvement observed is definitely because of the Lashuna rasayana and not due to
chance factor or sampling variability.
Excessive physical activities involving the wrist will have direct bearing on
the manibandha marma. Marmabhighata being one of the important etiologies of
vatavyadhi, the injury to the manibandha marma is clinically important for the same.
Pain stinging muscles atrophy and paralysis related to the hand are the symptoms of
Manibandha marmabhighata. Considering these symptoms this illness of Manibandha
marmabhighata is paralleled to Carpal tunnel syndrome of biomedicine. Again the
clinical presentation of manibandha marmabhighata is attributed to the morbidity of
vata dosha. Lashuna rasayana is indicated both dhatu kshayaja and margavarana
vatavyadhi.
In the present study significant reduction in the severity of symptoms of pain
numbness and paralysis is recorded proving the definite amelioration of the vata
dosha. Again it is observed that almost all the symptoms have shown partial
remission. None of the symptoms have completely cleared in this study. By
implication, definitely this treatment is effective but some more medication is
required for the complete amelioration of the illness. In general the Lashuna rasayana
dosage is fixed to 16 or 30 days. Selection of other Lashuna rasayana schedules
consisting of more prolonged medication may show complete remission of the illness.
Or else shamana medication is continued for about 30 days followed by planning the
second course of the Lashuna rasayana may prove more beneficial. Needless to say
this study will open scope for newer clinical studies in treatment of Manibandha
marmabhighata with different dosage schedule and there by proving its efficacy
against surgical interventions.
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 87
In regards to the etiopathogenesis of Carpal tunnel syndrome it is said that the
entrapment of the nerve causes local ischemia and inflammation of the injured median
nerve at the location of the carpal tunnel. Thus developed local ischemia eventuates
degeneration of the nerves related to the median nerve. This degeneration of the
median nerve causes clinical symptoms like Numbness, tingling, pain, weakness as
well as dysautonomia related to palmar aspect of the first to the fourth fingers and the
distal palm. It is interesting to note that the studies have proved the improvement of
circulation and reversal of ischemia of the entrapped nerves by the administration of
the garlic. Thus the Lashuna rasayana is effective in ensuring the reversal in the
pathology of nerve ischemia and thus proves effective in the management of
Manibandha marmabhighata.
Though this clinical study involved larger doses of Lashuna rasayana, all 15
patients tolerated the medicine very well with no any adverse reactions. Presence of
morbidity of pitta or pitta prakriti is contraindication of the administration of Lashuna
rasayana. No patients were excluded in the study on the basis of prakriti. Patients
having pitta dosha involved in the prakriti also treated with Lashuna rasayana.
The pitta virechana was done by the completion of the course of rasayana.
However even the patients with pitta dosha in their prakriti showed no symptoms of
pitta morbidly. Hence it can be said that this medication very effective and also
equally safe.
In short, marmabhighata is looked differently in surgical and medical schools
of thought. Surgical school of thought describes the marmabhighata with the
rationality of external injury and surgical interventions. Medical school of thought
emphasized the internal injury causing marmabhighata and medical management of
the same. Thus the marmabhighata is regarded as an important etiology of vata
Discussion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 88
vyadhi. Manibandha marmabhighata presents with features of affliction of sandhi
marma in general and manibandha marma in particular. Supti / numbness, Ruk / pain,
Vastushukairavakirna / stinging, Shosha / muscle atrophy, Parvashopha / swelling of
the finger joints and Kuntata / paralysis of the hand are the symptoms of manibandha
marmabhighata. Shodhana, shaman, brimhana and rasayana form the principle of
treatment of vata vyadhi and is planned with the due consideration of associated
dosha and involvement of avarana in the pathogenesis. Lashuna rasayana is effective
in both margavaranaja as well as dhatu kshayaja vata vyadhi. With this understanding
the study is planned to evaluate the effect of Lashuna rasayana in patients suffering
from Manibandha marmabhighata. The study proved favorable response to this
conservative management with near complete remission of the clinical symptoms.
Also the medication is equally safe with no any adverse effects even in patients
having pitta involved in the prakriti. Thus the study also gives more scope for further
clinical studies in patients suffering from Manibandha marmabhighata. More clinical
studies may be planned with different dosage schedule of Lashuna rasayana to
establish more evidences to this conservative management of Manibandha
marmabhighata.
Conclusion
Efficacy of lashuna rasayana in manibandha marmabhighata Page 89
CONCLUSION
15 patients diagnosed as Manibandha marmabhighata / Carpal tunnel syndrome
were treated with oral administration of Lashuna rasayana in a dose of 12 g for fifteen
days. Following conclusions are drawn from the study.
Manibandha marmabhighata is a vataja nanatmaja vyadhi; margavaranja and
dhatu kshayaja are the clinical variants; supti, ruk, shosha and kuntata or hand
are the symptoms; matches with Carpal tunnel syndrome; Lashuna rasayana is
a treatment option.
Statistically significant reduction was recorded in the mean severity score of
carpal tunnel syndrome by 12.667 from the initial score of 44.467.
The reduction in the mean score of functional disability by 9.267 from the
baseline value of 34.600 is statistically significant.
The mean VAS pain score at base line was 8.133 that came down to 4.0
following the medication and is statistically significant.
The reduction in the mean VAS score for numbness to 4 from the base line
value of 8.133 is statistically significant.
At baseline the mean hand grip strength was 5.600 Kg. that improved to
12.133 Kg and is statistically significant.
12 patients had average improvement, 2 patients had moderate improvement
and in 1 patient there was no improvement.
Summary
Efficacy of lashuna rasayana in manibandha marmabhighata Page 90
SUMMARY
Marmabhighata is looked differently in surgical and medical schools of
thought. Surgical school of thought describes the marmabhighata with the rationality
of external injury and surgical interventions. Medical school of thought emphasized
the internal injury causing marmabhighata and medial management of the same. Thus
the marmabhighata is regarded as an important etiology of vata vyadhi. Manibandha
marmabhighata presents with features of affliction of sandhi marma in general and
manibandha marma in particular. Supti / numbness, Ruk / pain, Vastushukairavakirna
/ tinging, Shosha / muscle atrophy, Parvashopha / swelling of the finger joints and
Kuntata / paralysis of the hand are the symptoms of Manibandha marmabhighata.
These clinical symptoms also tally the manifestations of Carpal tunnel syndrome.
Shodhana, shamana ,brimhana and rasayana form the principle of treatment of vata
vyadhi and is planned with the due consideration of associated dosha and involvement
of avarana in the pathogenesis. Lashuna rasayana is effective in both margavaranaja
as well as dhatu kshayaja vata vyadhi. With this understanding the study is planned to
evaluate the effect of Lashuna rasayana in patients suffering from Manibandha
marmabhighata.
OBJECTIVES OF THE STUDY-
Efficacy of a Lashuna rasayana on disease severity in patients suffering from
Manibandha marmabhighata / Carpal tunnel syndrome
Effect on functional disability in patients of Manibhandha marmabhighata /
Carpal tunnel syndrome treated with Lashuna rasayana.
Summary
Efficacy of lashuna rasayana in manibandha marmabhighata Page 91
MATERIALS AND METHODS –
Source of data -15 patients diagnosed as Manibandha marmabhighata / Carpal tunnel
syndrome were taken for study from OPD and IPD of Sri Dharmasthala
Manjunatheshwara Ayurveda Hospital, Kuthpady, 574118. The freeze dried powder
of lashuna is obtained in the 500 mg capsule from the Sri Dharmasthala
Manjunatheshwara Ayurveda Pharmacy.
Method of collection of data- A specific proforma was prepared incorporating all
points of history taking, physical signs, and symptoms as mentioned in Ayurveda as
well as bio medicine.
Design of the study-
Study Type : Interventional
Actual Enrollment : 15 participants
Allocation : Non-Randomized
Endpoint Classification : Efficacy Study
Intervention Model : Single Group Assignment
Masking : Open Label
Primary Purpose : Treatment
Study Start Date : October 2017
Study Completion Date : February 2018
The patients were selected irrespective of gender, cast, race, religion, based
on the diagnostic inclusion and exclusion criteria. All the parameter of signs,
symptoms is scored as enlisted in the assessment criteria and the result obtained was
statistically analyzed by the paired t test.
Summary
Efficacy of lashuna rasayana in manibandha marmabhighata Page 92
Diagnostic criteria-Signs and symptoms Manibandha marmabhighata / carpal tunnel
syndrome (paresthesia in the distribution of median nerve distal to wrist, weak hand
grip, wasting of muscles at the thenar eminence and positive tinels and phalen sign)
Inclusion Criteria-
Subjects with a clinical diagnosis of Manibandha marmabhighata / Carpal
tunnel syndrome.
Subjects must be between 16 to 70 years of age (both ages inclusive).
Subjects of both genders.
Having signed a written informed consent form,
Exclusion Criteria-
Patients with uncontrolled Diabetes Mellitus & Hypertension.
Patients with Fracture of wrist.
Subjects with history of excessive menstruation.
Patients who are pregnant by patient report or intending to become pregnant
during the study.
Patients that have been previously diagnosed with cervical radiculopathy,
Outcome measures-
Primary outcome measures
Questionnaire of Levine et al for Clinical Assessment of Carpal Tunnel
Syndrome [Time Frame: Baseline, day 17].
Summary
Efficacy of lashuna rasayana in manibandha marmabhighata Page 93
Secondary outcome measures:
Change in Grip strength (Dynamometer) [Time Frame: Baseline, day 17].
Change in Visual Analog Scale for pain [Time Frame: Baseline, day 17].
Participants Assessment of numbness Over Time by the method of visual
analog scale (VAS) ranging from 0 (best) to 10 (worst) cm
[Time Frame: Baseline, day 17]
Intervention:
Koshtashodhana on Day 1 : Oral administration of Eranda taila in empty
stomach, in a dose of 20 ml in the morning
along with 100 ml of warm water as after drink
LashunaRasayana on Day 2
to 16
: Oral administration of Lashuna rasayana in a
dose of 12 g in empty stomach half an hour
before breakfast along with 100 ml of milk as
after drink.
Pitta virechana on Day 17
:Oral administration of Eranda taila in empty
stomach, in a dose of 20 ml in the morning
along with 100 ml of warm water as after drink.
Follow up duration: 30 days
Total duration of study: 47days.

Summary
Efficacy of lashuna rasayana in manibandha marmabhighata Page 94
Observation & Results
Among the 15 patients, maximum number of patients, 6.66 % were between
the age group of 16 -30 years followed by the age group of 31 to 50 years i.e. 33.33
%. 60% patient belonged to age group of 51-70years. 86.66% were females followed
13.33 % of males. A maximum of 86.66% of the patients were belonging to the Hindu
religion. In contrast to this 13.33% of the patients were of Christian community.
93.33%% were married. 6.66% were widow. 66.66% of patients were house wives by
profession. The remaining 13.33% of the patients were engaged in business.20% were
employees. 60% belonged to the category of middle class. 20% of patients were in the
category of upper middle socio economic status and other20% of patients were of
upper socioeconomic status. Only 26.66% of the patients were restricted to vegetarian
diet, and the remaining 73.33% of the patients had the dietary habit of taking mixed
diet. 80% of the patients had sound sleep. Remaining20% of the patients complained
of disturbed sleep for different reasons. Erroneous habit of day sleep was identified in
80% of the patients among the 15 patient. Remaining 20 %of the patients were not
resorting to the day sleep. Only 13.33% of the patients had the addiction of
consuming tobacco. 100% of the patients had the habit of taking coffee or tea
regularly. Remaining 86.66% of patients admitted that they had no any addictions.
20% of the patients gave the family history of Carpal tunnel syndrome, while the rest
80% didn’t have any history. 60% had their body weight between 40 to 60 kg.
6.66%of the patients had their body weight more than 91 kg. 13.33% of the patient
had their body weight between 71-80kgand 20% between 61-70 kg. 66.66 % of
patients had BMI between 20-24.4. 26.66% had BMI between 25-29.9 where as 6.66
% of the patients had BMI between 30-34.9. 46.66% each showed vata pitta prakriti
and vatakapha prakriti and 6.66% showed pitta kapha prakriti. 80 % had madhyama
Summary
Efficacy of lashuna rasayana in manibandha marmabhighata Page 95
sara, 20 % of the patients belonged to Avara sara. 46.66 % had madhyama type of
samhanana, about 46.66 % patients had avarasamhanana and 13.33% had pravara
samhanana. 66.66 % patients had madhyama satva, 26.66 % had avara satva where as
6.66% of the patients belonged to the category of pravara satva. 41.66 % had
madhyama vyayamashakti and 58.33% had avaravyayama. 26.66 % had
avaravyayamashakti and in comparison to this, 73.33 % had
madhyamaabhyavaranashakti. 80 % of the total number had madhyamajaranashakti,
contrary to this, 13.33 % of the patients had avarajarana Shakti and 6.66% had
pravarajaranashakthi.,73.33% had the progressive onset of the Manibandha
marmabhighata. 26.66% had sudden onset. 1oo% of the patients gave the data of
presence of ruja, and supta. Out of 15 patients in the study 80% are suffering from
Manibandha marmabhighata due to apatarpana and the other 20% due to
santarpananidana.
Effect of Lashuna rasayana in Manibandha marmabhighata.
The mean score of severity before the intervention was 44.467 (±SE 1.546)
that came down to 31.800 (±SE1.303) following medication with Lashuna rasayana.
Thus a reduction into the severity score of 12.667 was recorded in this study. Also the
improvement was statistically significant when analyzed by the Wilcoxon Signed
Rank Test with p <0.001. At the baseline the mean score of functional disability status
was 34.600 (0.616) that came down to 25.333 (0.715) following Lashuna rasayana
thus recording an improvement by 9.267 is functional disability status score. Again
when analyzed by the statistical test of significance, this improvement was highly
significant with p <0.001. The mean VAS pain score in 15 patients at base line was
8.133 that came down to 4.0 following the medication. Thus an improvement of 4.333
Summary
Efficacy of lashuna rasayana in manibandha marmabhighata Page 96
in the mean VAS pain score was recorded. The initial VAS score was 8.133 (±SE
0.654) before beginning the Lashuna rasayana. After the intervention the numbness
recorded was 4.133 (±SE 0.376) thus showing a decrease in severity of numbness
VAS score of 4. Also the improvement was statistically significant when analyzed by
the Wilcoxon Signed Rank Test with p <0.001. At baseline the mean hand grip
strength was 5.600 Kg. After the Lashuna rasayana this improved to 12.133 Kg. Thus
an improvement of 6.53 Kg in the hand grip strength was recorded in the study.
Analysis of the statistical significance was done by adapting the paired t test, it
showed that the improvement in the hand grip strength was statistically significant
with p value of <0.001. The study revealed that 13.33 % of patients had moderate
remission and 80 % of patients have recorded average remission. Also 6.66 % of
patients showed poor remission.
CONCLUSION
The study proved favorable response to the conservative management of
Manibandha marmabhighata with Lashuna rasayana administered in a dose of 12 g
OD for 15 days and recorded a statistically significant, near complete remission of the
clinical symptoms. Also the medication is equally safe with no any adverse effects
even in patients having pitta involved in the prakriti.
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 97
REFERENCES
1. Jadavaji Tikamji Acharyaeditor. Charaka Samhitha, Varanasi:chaukhambha
Prakashan; Reprint 2013.pp.738.p112
2. Jadavaji Tikamji Acharya editor. Susruta Samhitha, Varanasi:chaukhambha
Sanskrit Prakashan; Reprint 2010.pp.824.p373
3. Jadavaji Tikamji Acharya editor. Susruta Samhitha, Varanasi:chaukhambha
Sanskrit Prakashan; Reprint 2010.pp.824.p370
4. Jadavaji Tikamji Acharya editor. Charaka Samhitha, Varanasi:chaukhambha
Prakashan;Reprint 2013.pp.738.p816
5. Jadavaji Tikamji Acharya editor.Charaka Samhitha, Varanasi:chaukhambha
Prakashan;Reprint 2013.pp.738.p613
6. F.Charles Brunicarcardi, Dana K. Anderson, Timothy R.Billiar, David L .Dunn,
John G. Hunter, Jeffrey B. Matthews, Raphael E.Pollock. Schwartz’s Principles
of Surgery. United states of America: Mc Graw Hill Medical, ed 9th .2010,
p1627.
7. Rishi kumar P.R.S. Sharma & Ram Chandra, editor. Atharvaveda Vol 1 to 8.
Muradabad: Sanatana Dharma Yantralaya; 1988. (7:2/123/1)
8. N. S. Sontakke, editor. Rigveda, commentary by – Shri Marsyachandra, Vedic
Samshodhana Mandal Tilak Smarak mandir ; Vol 1 to 10 (1:11/61/6)
9. N. S. Sontakke, editor. Rigveda, commentary by – Shri Marsyachandra, Vedic
Samshodhana Mandal Tilak Smarak mandir ; Vol 1 to 10 (1:17/116/15)
10. Rishi kumar P.R.S. Sharma & Ram Chandra, editor. Atharvaveda Vol 1 – 8.
Muradabad: Sanatana Dharma Yantralaya; 1988. (8:2/3/17)
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 98
11. Rishi kumar P.R.S. Sharma & Ram Chandra, editor. Atharvaveda Vol 1 to 8.
Muradabad: Sanatana Dharma Yantralaya; 1988. (7/36/2,1/17/1)
12. Rishi kumar P.R.S. Sharma & Ram Chandra, editor. Atharvaveda Vol 1 to 8.
Muradabad: Sanatana Dharma Yantralaya; 1988. (1/90/1)
13. Rishi kumar P.R.S. Sharma & Ram Chandra, editor. Atharvaveda Vol 1 to 8.
Muradabad: Sanatana Dharma Yantralaya; 1988. (10/2/11)
14. Rishi kumar P.R.S. Sharma & Ram Chandra, editor. Atharvaveda Vol 1 to 8.
Muradabad: Sanatana Dharma Yantralaya; 1988. (10/8/43)
15. Rishi kumar P.R.S. Sharma & Ram Chandra, editor. Atharvaveda Vol 1 to 8.
Muradabad: Sanatana Dharma Yantralaya; 1988. (7/10/123/1)
16. Rishi kumar P.R.S. Sharma & Ram Chandra, editor. Yajurveda Vol 1 to 8.
Muradabad: Sanatana Dharma Yantralaya; 1988. (8/3/17)
17. Rishi kumar P.R.S. Sharma & Ram Chandra, editor. Yajurveda Vol 1 to 8.
Muradabad: Sanatana Dharma Yantralaya; 1988. (2/33/6)
18. Ram Chandra Shastri Kinjawarkar, editor. Garbhopanishad; 108 Upanishada,
Mathura: Jagadeesh Prasad Bhutiya Bambai Bhusthan Press. Pp: 2949, p: 1933.
19. Valmiki. Motilal Jalan, editor. Ramayana, I part. Gorakhpur: Geeta Press. 1960.
63:45-53.
20. Veda Vyasa. Swami Jagadishwaranand Saraswati, editor.Mahabharatha.Arya
Sahitya Bhavan; 2008. Pp-1312, p-876.
21. Veda Vyasa. Swami Jagadishwaranand Saraswati, editor.Mahabharatha.Arya
Sahitya Bhavan; 2008. Pp-1312, p-1287.
22. Jadavaji Tikamji Acharya editor. Charaka Samhitha, Varanasi:chaukhambha
Prakashan;Reprint 2013.pp.738.p816
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 99
23. Sushruta. Yadavji Trikamji Acharya, editor. Sushruta Samhita with Nibandha
Sangraha of Dalhanacharya. 8th ed. Varanasi: Chaukhambha Orientalia; 2008.
Pp824, p- 369.
24. Vruddha Jeevaka. Kasyapa Samhita or Vruddha Jeevaka Tantra, revised by
Vatsya with Sanskrit introduction by Nepal Rajaguru Pandit Hemaraja Sharma.
7th ed. Varanasi: Chaukhambha Sanskrit Samsthan; 2000 Pp- 364, p- 76.
25. Vriddha Vagbhata. Shiv Prasad Sharma, editor. Ashtanga Sangraha with
Sasilekha commentary of Indu. 1st ed Varanasi: Chaukhambha Sanskrit series
office; 2006. Pp- 965, p- 319.
26. Harisadasivasastri Paradakara Bhisagacarya, editor. Ashtanga Hrudayam with
Sarvangasundara of Arunadatta & Ayurvedarasayana of Hemadri. Varanasi:
Chaukhambha Orientalia; 2005. Pp-956, p- 409.
27. K.R.Srikanta Murthy Editor. Madhava Nidanam, Varanasi: Chaukhambha
Orientalia; Reprint Edition,2009.pp320.p143.
28. Anantaram Sharma Editor. Madhavanidhanam, Varanasi: Chaukhamba Sanskrit
Pratishthan;2007.pp530.p491.
29. Vardhaman Parshwanath Shastri. The Kalyana Karakam of Ugradityacharya,
Varanasi: Shet Govindji Raoji Doshi;1940.pp748.p.31.
30. Fauci, Braunwald, Kasper, Hauser, Longo, Jameson, Loscalzo. Harrison s
Principles of Internal Medicine;pp.2754.p2154.
31. Busul.Bhavaprakasa of Bhavamishra, Varanasi:Chaukambha orientalia; First
2006.pp742.p44.
32. Busulu Sitaram. Bhavaprakasa of Bhavamishra, Varanasi: Chaukambha
orientalia; First 2006.pp742.p45.
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 100
33. Siddhi Nandam Mishra. Rasaratna Samuchchayah, Varanasi: Chaukambha
orientalia; First edition 2011.pp697.p401.
34. David Frawley, Subhash Ranade, Avinash Lele. Ayurveda and Marma Therapy,
Delhi:Chaukhamba Sanskrit Pratisththan;2005.pp259.p9.
35. David Frawley, Subhash Ranade, Avinash Lele. Ayurveda and Marma Therapy,
Delhi:Chaukhamba Sanskrit Pratisththan;2005.pp259.p7.
36. Historical review of Carpal tunnel syndrome(Internet), Available from
https://link.springer.com
37. Carpal tunnel syndrome, syndrome of partial thenar atrophy, and W.Russel Brain
: a historical perspective(internet), Available from www.ncbi.nlm.nih.gov
38. A Value of Gilliatt′s pneumatic tourniquet test for diagnosis of Carpal tunnel
syndrome, Available from www.ncbi.nlm.nih.gov.pubmed
39. Electrodiagnosis of Carpal tunnel syndrome jnnp.bmj:com›jnnp›23.full.pdf.
40. Raja Radhakanthadeva .Shabdhakalpadruma.Delhi:NAG Pulblishers; volume
3,Reprint 1987.pp792.p576.
41. Raja Radhakanthadeva .Shabdhakalpadruma.Delhi:NAG Pulblishers; volume 3,
Reprint 1987.pp792.p574.
42. Raja Radhakanthadeva .Shabdhakalpadruma.Delhi:NAG Pulblishers; volume 3,
Reprint 1987.pp792.p392.
43. Raja Radhakanthadeva .Shabdhakalpadruma.Delhi:NAG Pulblishers; volume 3,
Reprint 1987.pp792.p576.
44. Jadavji Trikamji Acharya editor.Susruta Samhita, Varanasi: Chaukhambha
Sanskrit Sansthan; Reprint 2010.pp.824.p372-373.
45. Jadavji Trikamji Acharya editor.Susruta Samhita, Varanasi: Chaukhambha
Sanskrit Sansthan; Reprint 2010.pp.824.p417.
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 101
46. Amarasimha. Haragovinda Shastri, editor. Amarakosha. Varanasi: Choukambha
Sanskrit Sansthan; 2006, Pp- 667, p-656
47. Jadavji Trikamji Acharya editor.Susruta Samhita, Varanasi: Chaukhambha
Sanskrit Sansthan; Reprint 2010.pp.824.p369.
48. Jadavji Trikamji Acharya editor.Susruta Samhita, Varanasi: Chaukhambha
Sanskrit Sansthan; Reprint 2010.pp.824.p371.
49. Raja Radhakanthadeva .Shabdhakalpadruma.Delhi:NAG Pulblishers; volume 1,
Reprint .pp315.p72.
50. Jadavji Trikamji Acharya editor.Charaka Samhita, Varanasi: Chaukhambha
Orientalia; Reprint edition 2011.pp.738.p201-202.
51. Jadavji Trikamji Acharya editor.Charaka Samhita, Varanasi: Chaukhambha
Orientalia; Reprint edition 2011.pp.738.p75.
52. Jadavji Trikamji Acharya editor.Charaka Samhita, Varanasi: Chaukhambha
Orientalia; Reprint edition 2011.pp.738.p713..
53. Sidney I Landau.Webster′s Student dictionary.New Delhi: CBS Publishers &
distributors;Reprint 2001.pp.863.p108.
54. Siddharth N Shah editor.API Textbook of Medicine, Mumbai: The Association
of Phyisicians of India;8th
edition.pp1624.p1251.
55. Jadavji Trikamji Acharya editor.Charaka Samhita, Varanasi: Chaukhamba
Krishnadas Academy;Reprint2010.pp738.p617.
56. Jadavji Trikamji Acharya editor.Charaka Samhita, Varanasi: Chaukhamba
Krishnadas Academy;Reprint2010.pp738.p677-684.
57. Jadavji Trikamji Acharya editor.Charaka Samhita, Varanasi: Chaukhamba
Sanskrit Sansthan;5th
edition 2001.pp738.p548.
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 102
58. Jadavji Trikamji Acharya editor.Sushruta Samhita, Varanasi: Chaukhamba
Sanskrit Sansthan;Reprint2014.pp824.p83-84.
59. Jadavji Trikamji Acharya editor.Sushruta Samhita, Varanasi: Chaukhamba
Sanskrit Sansthan;Reprint2010.pp824.p73-74.
60. Fauci, Braunwald, Kasper, Hauser, Longo, Jameson, Loscalzo.Harrison s
Principles of Internal Medicine;pp.2754.p2154.
61. Jadavji Trikamji Acharya editor.Charaka Samhita, Varanasi: Chaukhamba
Krishnadas Academy, Reprint2010.pp738.p617.
62. Fauci, Braunwald, Kasper, Hauser, Longo, Jameson, Loscalzo.Harrison s
Principles of Internal Medicine,pp.2754.p2154.
63. Jadavji Trikamji Acharya editor.Sushruta Samhita, Varanasi: Chaukhamba
Sanskrit Sansthan;Reprint2014.pp824.p372-373.
64. Jadavji Trikamji Acharya editor.Sushruta Samhita, Varanasi: Chaukhamba
Sanskrit Sansthan;Reprint2014.pp824.p375.
65. Jadavji Trikamji Acharya editor.Sushruta Samhita, Varanasi: Chaukhamba
Sanskrit Sansthan;Reprint2014.pp824.p369-370.
66. Jadavji Trikamji Acharya editor.Sushruta Samhita, Varanasi: Chaukhamba
Sanskrit Sansthan;Reprint2014.pp824.p370-371.
67. Jadavji Trikamji Acharya editor.Charaka Samhita, Varanasi: Chaukhamba
Krishnadas Academy;Reprint2010.pp738.p686.
68. Moreswara Kunte, Krsna Ramchandra Sstri Navare.Astangahrdayam,
Varanasi:Chaukhambha Orientalia;Reprint 10th
edition,pp956.p415.
69. Moreswara Kunte, Krsna Ramchandra Sstri Navare.Astangahrdayam,
Varanasi:Chaukhambha Orientalia;Reprint 10th
edition,pp956.p415.
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 103
70. Moreswara Kunte, Krsna Ramchandra Sstri Navare. Astangahrdayam,
Varanasi:Chaukhambha Orientalia;Reprint 10th
edition,pp956.p415.
71. Siddharth N Shah editor.API Textbook of Medicine, Mumbai: The Association
of Phyisicians of India;8th
edition.pp1624.p1251.
72. Siddharth N Shah editor.API Textbook of Medicine, Mumbai: The Association
of Phyisicians of India;8th
edition.pp1624.p1251.
73. Siddharth N Shah editor.API Textbook of Medicine, Mumbai: The Association
of Phyisicians of India;8th
edition.pp1624.p1251.
74. Fauci, Braunwald, Kasper, Hauser, Longo, Jameson, Loscalzo.Harrison s
Principles of Internal Medicine;pp.2754.p2154.
75. Fauci, Braunwald, Kasper, Hauser, Longo, Jameson, Loscalzo.Harrison s
Principles of Internal Medicine,pp.2754.p2154.
76. The carpal-compression test. An instrumented device for diagnosing Carpal
tunnel syndrome (Internet),Available from https:www.ncbi.nlm.nih.gov›pubmed
77. LynnS.Bickley.Guide to Physical examination & History taking, New
Delhi:Wolters Kluwer (India) Pvt. Ltd:Reprint 2010.pp964.p604.
78. Carpal tunnel syndrome (Internet), Available from
https://www.ncbi.nlm.nih.gov›articles.
79. Jadavji Trikamji Acharya editor.Susruta Samhita, Varanasi: Chaukhambha
Sanskrit Sansthan; 5th
edition 2001.pp.738.p319.
80. Brahmanand Tripathi editor.Astanga Hrdayam, Varanasi:Chaukhamba Sanskrit
Pratishthan;Reprint 201;.pp1295.p164.
81. Jadavji Trikamji Acharya editor.Charaka Samhitha.Varanasi:Chaukhambha
Orientalia;Reprint 2011;pp738.p617-618.
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 104
82. Jadavji Trikamji Acharya editor.Charaka Samhitha.Varanasi:Chaukhambha
Orientalia;Reprint 2011;pp738.p79-80.
83. Laxmidhar Dwivedi editorSusruta Samhitha.Varanasi:Chaukhambha Sanskrit
Series Office; second edition2002;Volume 2.pp788.p.245
84. Laxmidhar Dwivedi editor Susruta Samhitha.Varanasi:Chaukhambha Sanskrit
Series Office; second edition2002;Volume 2.pp788.p.226
85. Jadavji Trikamji Acharya editor.Sushruta Samhita, Varanasi: Chaukhamba
Sanskrit Sansthan, Reprint2014.pp824.p83-84.
86. Brahmanand Tripathi editor.Astanga Hrdayam, Varanasi:Chaukhamba Sanskrit
Pratishthan;Reprint 201;.pp1295.p171.
87. Brahmanand Tripathi editor.Astanga Hrdayam, Varanasi:Chaukhamba Sanskrit
Pratishthan;Reprint 201;.pp1295.p165.
88. Jadavji Trikamji Acharya editor.Charaka Samhitha.Varanasi:Chaukhambha
Orientalia;Reprint 2011;pp738.p88.
89. Jadavji Trikamji Acharya editor.Charaka Samhitha.Varanasi:Chaukhambha
Orientalia;Reprint 2011;pp738.p66-67
90. Moreswara Kunte, Krsna Ramchandra Sstri Navare. Astangahrdayam,
Varanasi:Chaukhambha Orientalia; Reprint 10th
edition,pp956.p415.
91. Median nerve entraptment (Internet), Available at
http://emedicine.medscape.com.
92. Jadavji Trikamji Acharya editor. Sushruta Samhita, Varanasi:Chaukhambha
Sanskrit Sansthan; Reprint2017.pp724.p376.
93. Jadavji Trikamji Acharya editor. Sushruta Samhita, Varanasi:Chaukhambha
Sanskrit Sansthan;Reprint2017.pp724.p371
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 105
94. Jadavji Trikamji Acharya editor. Sushruta Samhita, Varanasi:Chaukhambha
Sanskrit Sansthan;Reprint2017.pp724.p371.
95. Jadavji Trikamji Acharya editor.Carak Samhita, Varanasi:Chaukhamba
Krishnadas Academy;Reprint 2010,pp.738.p628.
96. Jadavji Trikamji Acharya editor. Carak Samhita, Varanasi:Chaukhamba
Krishnadas Academy;Reprint 2010,pp.738.p686.
97. Jadavji Trikamji Acharya editor.Carak Samhita, Varanasi:Chaukhamba
Krishnadas Academy;Reprint 2010,pp.738.p119.
98. Jadavji Trikamji Acharya editor.Carak Samhita, Varanasi:Chaukhamba
Krishnadas Academy;Reprint 2010,pp.738.p599.
99. Shivprasad Sharma editor.Astangasamgraha, Varanasi:Chaukhambha Sanskrit
Series Office;3rd
edition 2012.pp935.p114.
100. Jadavji Trikamji Acharya editor. Charaka Samhita. Varanasi: Chaukhambha
Surbharati Prakashan; 2014. pp. 738.p.621
101. Brahmashankara Shastri editor. Yogaratnakara- Vidyotini. Purvardha.
Varanasi: Chaukhambha Prakashan; pp.573.p.416
102. Kaviraj Govind Das Sen editor. Bhaishajya Ratnavali- Siddhiprada. Varanasi:
Chaukhambha Surbharati Prakashan, 2009.pp. 1196. P. 571
103. Basavaraja. Basavarajeeyam, Varanasi; Chaukhambha Sanskrit Prasthan, 2005.
Pp. 423; p. 117
104. Shivprasad Sharma editor.Astangasamgraha, Varanasi:Chaukhambha Sanskrit
Series Office;3rd
edition 2012.pp935.p923-928.
105. Lucas. Dravyagunavignana, volume 2, Varanasi:chaukambhavishvabharati,
p422-425.
References
Efficacy of lashuna rasayana in manibandha marmabhighata. Page 106
106. Lucas. Dravyagunavignana, volume 2, Varanasi:chaukambhavishvabharati,
p387-392.
107. Shivprasad Sharma editor.Astangasamgraha, Varanasi:Chaukhambha Sanskrit
Series Office;4rd
edition 2012.pp935.p924.
108. Shivprasad Sharma editor.Astangasamgraha, Varanasi:Chaukhambha Sanskrit
Series Office; 3rd
edition 2012.pp935.p928
ªÀÄt¨sÀAzÀ ªÀĪÀiÁð©üWÁvÀ gÉÆÃUÀzÀ ªÉÄÃ¯É ®±ÀÄ£ÀgÀ¸ÁAiÀÄ£À ¥ÀæAiÉÆÃUÀzÀCzsÀåAiÀÄ£À²æà zsÀªÀÄð¸ÀܼÀ
ªÀÄAdÄ£ÁxÉñÀégÀDAiÀÄĪÉðÃzÀ ªÀĺÁ«zÁå®AiÀÄ, PÀÄvÁàr,GqÀĦ
C¨sÀåyð ¸ÀªÀÄäw ¥ÀvÀæ
___________________ JA§ £Á£ÀÄ F ªÉÄîÌAqÀAiÉÆÃd£ÉAiÀÄ ¸ÁgÁA±ÀzÀ «ªÀgÀuÉ ¥ÀqÉ¢zÀÄÝ, ¸ÀéEZÉÒ¬ÄAzÀ
F AiÉÆÃd£ÉAiÀÄ°è M¼À¥ÀqÀ®Ä M¦àzÉÝãÉ. F CzsÀåAiÀÄ£ÀzÀ°è £À£Àß ¨sÁUÀªÀ»¸ÀÄ«PÉ £À£ÀUÉ
¯Á¨sÀzÁAiÀÄPÀªÁUÀ§ºÀÄzÀÄJAzÀÄ £Á£ÀÄ w½¢zÉÝãÉ. EzÀgÀGzÉÝñÀ ¸ÁzsÀPÀ, ¨ÁzsÀPÀUÀ¼À£ÀÄß £À£ÀßvÀȦÛUÉvÀPÀÌAvÉ £À£ÀUÉ
«ªÀj¸À®ànÖzÉ.F ªÀÄÆ®PÀ F AiÉÆÃd£ÉAiÀÄ°èM¼À¥ÀqÀ®Ä £Á£ÀÄ ¸ÀªÀÄäw ¸ÀÆa¸ÀÄwÛzÉÝãÉ. £Á£ÀÄ
AiÀiÁªÀÅzÉÃPÁgÀtªÀ£ÀÄßPÉÆqÀzÉà F AiÉÆÃd£É¬ÄAzÀAiÀiÁªÀÅzÉà ¸ÀAzÀ¨sÀðzÀ°è »AzÉ §gÀĪÀD¢üPÁgÀªÀ£ÀÄß ºÉÆA¢gÀĪÀ
§UÉÎ w½¢zÉÝãÉ.
¢£ÁAPÀ:
¸ÀÞ¼À :
ªÀåQÛAiÀÄ ºÀ¸ÁÛPÀëgÀªÉÊzÀågÀ ºÀ¸ÁÛPÀëgÀ
PATIENT CONSENT FORM
I ………………………….. aged…………….. years R/O………………………….. is
exercising my free power of choice, hereby give my consent to be included as a trial subject in
the clinical research subject “ EFFICACY OF LASHUNA RASAYANA IN SUBJECTS
WITH CARPAL TUNNEL SYNDROME(MANIBHANDHA MARMABHIGHATA”. I
understand that I may be treated with drug for the disease with which I am suffering. I have
been informed to my satisfaction the aim, objective of the clinical trial, ingredients of the trial
drug treatment and follow up including laboratory investigations to monitor and safeguard my
body functions as and when required. I am also aware of the right to opt out of the trial at any
time during the course of my treatment. I will not make any compensatory claim for any
hazardous effects on me during the treatment.
Date…………… Patient’s signature
Patient has signed the declaration and has given consent.
Signature of research scholar
107
SHRI DHARMASTALA MANJUNATHESHWARA COLEGE OF
AYURVEDA AND HOSPITAL, UDUPI
DEPARTMENT OF POST GRADUATE STUDIES IN
KAYA CHIKITSA AND MANASA ROGA
CASE PROFORMA FOR MANIBHANDHA MARMABHIGHATA
Patient Inclusion/Exclusion Form Case Number ( )
Name: Age: yrs
Sex: M/F
Address:
Sl Patient details Criteria Eligible Not
Eligible
01 Signed informed consent Required
02 Symtoms:
Pain at wrist:
Paresthesia of thumb
Paresthesia of forefinger:
No
Site right wrist left wrist
All
03 Major criteria
a)Tinel/ signYes / No
b) Phalen signYes / No
04 Fracture of wristYes / No No
04 Cervical RadiculopathyYes / No No
05 H/O of excessive menstruation Yes / No No
06 Uncontorolleddiabetismellitus/hypertensionYes
/ No
No
07 Pregnant Yes / No No
08 Planning to conceive in 6 months Yes / No No
09 Lactating Yes / No No
12 Duration: Years < 10
years
13 Age: Years >16-
70Yrs
ACCEPTED REJECTED
108
ªÀÄt¨sÀAzÀ ªÀĪÀiÁð©üWÁvÀ gÉÆÃUÀzÀ ªÉÄÃ¯É ®±ÀÄ£ÀgÀ¸ÁAiÀÄ£À ¥ÀæAiÉÆÃUÀzÀCzsÀåAiÀÄ£À²æà zsÀªÀÄð¸ÀܼÀ
ªÀÄAdÄ£ÁxÉñÀégÀDAiÀÄĪÉðÃzÀ ªÀĺÁ«zÁå®AiÀÄ, PÀÄvÁàr,GqÀĦ
C¨sÀåyð ¸ÀªÀÄäw ¥ÀvÀæ
___________________ JA§ £Á£ÀÄ F ªÉÄîÌAqÀAiÉÆÃd£ÉAiÀÄ ¸ÁgÁA±ÀzÀ «ªÀgÀuÉ ¥ÀqÉ¢zÀÄÝ,
¸ÀéEZÉÒ¬ÄAzÀ F AiÉÆÃd£ÉAiÀÄ°è M¼À¥ÀqÀ®Ä M¦àzÉÝãÉ. F CzsÀåAiÀÄ£ÀzÀ°è £À£Àß ¨sÁUÀªÀ»¸ÀÄ«PÉ £À£ÀUÉ
¯Á¨sÀzÁAiÀÄPÀªÁUÀ§ºÀÄzÀÄJAzÀÄ £Á£ÀÄ w½¢zÉÝãÉ. EzÀgÀGzÉÝñÀ ¸ÁzsÀPÀ, ¨ÁzsÀPÀUÀ¼À£ÀÄß
£À£ÀßvÀȦÛUÉvÀPÀÌAvÉ £À£ÀUÉ «ªÀj¸À®ànÖzÉ.F ªÀÄÆ®PÀ F AiÉÆÃd£ÉAiÀÄ°èM¼À¥ÀqÀ®Ä £Á£ÀÄ ¸ÀªÀÄäw
¸ÀÆa¸ÀÄwÛzÉÝãÉ. £Á£ÀÄ AiÀiÁªÀÅzÉÃPÁgÀtªÀ£ÀÄßPÉÆqÀzÉà F AiÉÆÃd£É¬ÄAzÀAiÀiÁªÀÅzÉà ¸ÀAzÀ¨sÀðzÀ°è »AzÉ
§gÀĪÀD¢üPÁgÀªÀ£ÀÄß ºÉÆA¢gÀĪÀ §UÉÎ w½¢zÉÝãÉ.
¢£ÁAPÀ:
¸ÀÞ¼À :
ªÀåQÛAiÀÄ ºÀ¸ÁÛPÀëgÀªÉÊzÀågÀ ºÀ¸ÁÛPÀëgÀ
PATIENT CONSENT FORM
I ………………………….. aged…………….. years R/O………………………….. is
exercising my free power of choice, hereby give my consent to be included as a trial
subject in the clinical research subject “ EFFICACY OF LASHUNA RASAYANA
IN SUBJECTS WITH CARPAL TUNNEL SYNDROME(MANIBHANDHA
MARMABHIGHATA”. I understand that I may be treated with drug for the disease
with which I am suffering. I have been informed to my satisfaction the aim, objective
of the clinical trial, ingredients of the trial drug treatment and follow up including
laboratory investigations to monitor and safeguard my body functions as and when
required. I am also aware of the right to opt out of the trial at any time during the
course of my treatment. I will not make any compensatory claim for any hazardous
effects on me during the treatment.
Date…………… Patient’s signature
Patient has signed the declaration and has given consent.
Signature of research scholar
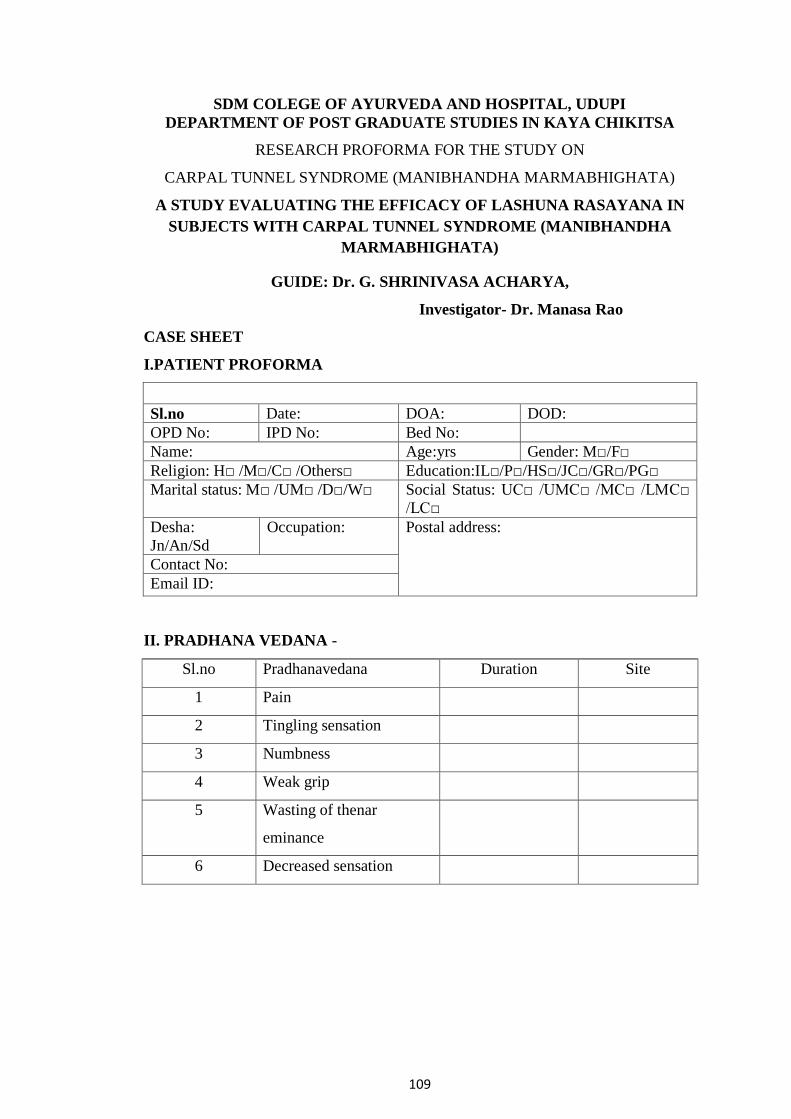
109
SDM COLEGE OF AYURVEDA AND HOSPITAL, UDUPI
DEPARTMENT OF POST GRADUATE STUDIES IN KAYA CHIKITSA
RESEARCH PROFORMA FOR THE STUDY ON
CARPAL TUNNEL SYNDROME (MANIBHANDHA MARMABHIGHATA)
A STUDY EVALUATING THE EFFICACY OF LASHUNA RASAYANA IN
SUBJECTS WITH CARPAL TUNNEL SYNDROME (MANIBHANDHA
MARMABHIGHATA)
GUIDE: Dr. G. SHRINIVASA ACHARYA,
Investigator- Dr. Manasa Rao
CASE SHEET
I.PATIENT PROFORMA
Sl.no Date: DOA: DOD:
OPD No: IPD No: Bed No:
Name: Age:yrs Gender: M□/F□
Religion: H□ /M□/C□ /Others□ Education:IL□/P□/HS□/JC□/GR□/PG□
Marital status: M□ /UM□ /D□/W□ Social Status: UC□ /UMC□ /MC□ /LMC□
/LC□
Desha:
Jn/An/Sd
Occupation: Postal address:
Contact No:
Email ID:
II. PRADHANA VEDANA -
Sl.no Pradhanavedana Duration Site
1 Pain
2 Tingling sensation
3 Numbness
4 Weak grip
5 Wasting of thenar
eminance
6 Decreased sensation
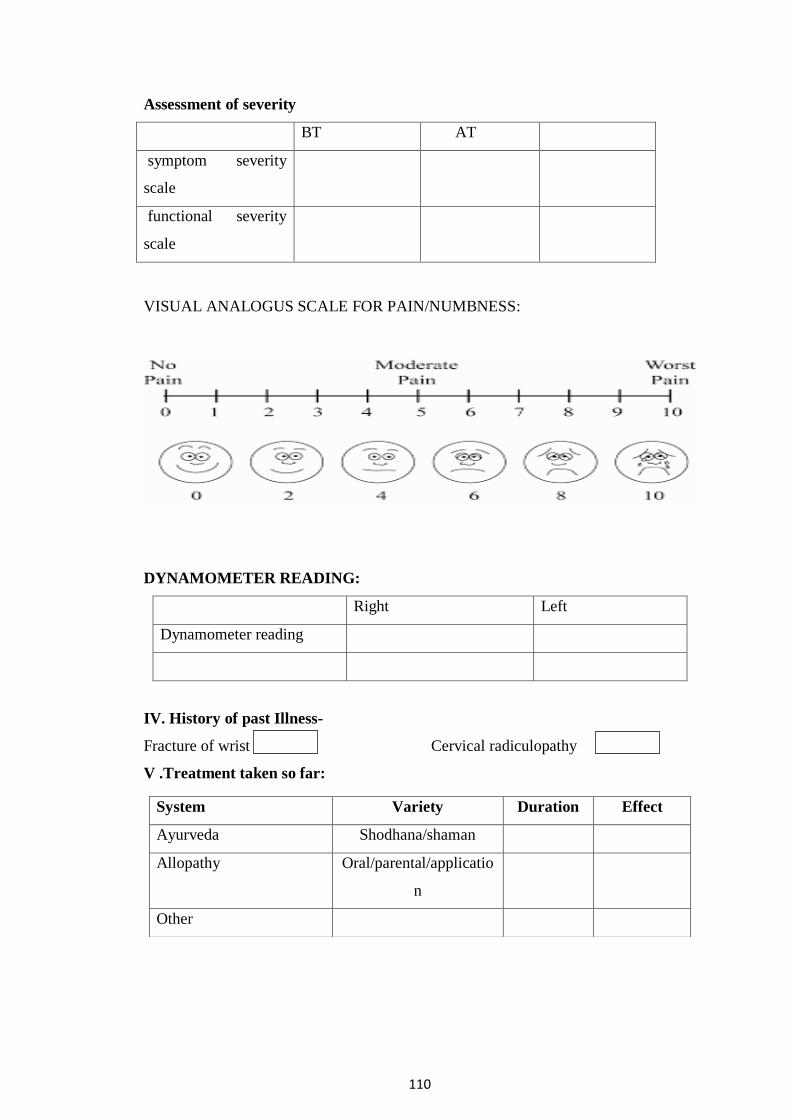
110
Assessment of severity
BT AT
symptom severity
scale
functional severity
scale
VISUAL ANALOGUS SCALE FOR PAIN/NUMBNESS:
DYNAMOMETER READING:
Right Left
Dynamometer reading
IV. History of past Illness-
Fracture of wrist Cervical radiculopathy
V .Treatment taken so far:
System Variety Duration Effect
Ayurveda Shodhana/shaman
Allopathy Oral/parental/applicatio
n
Other
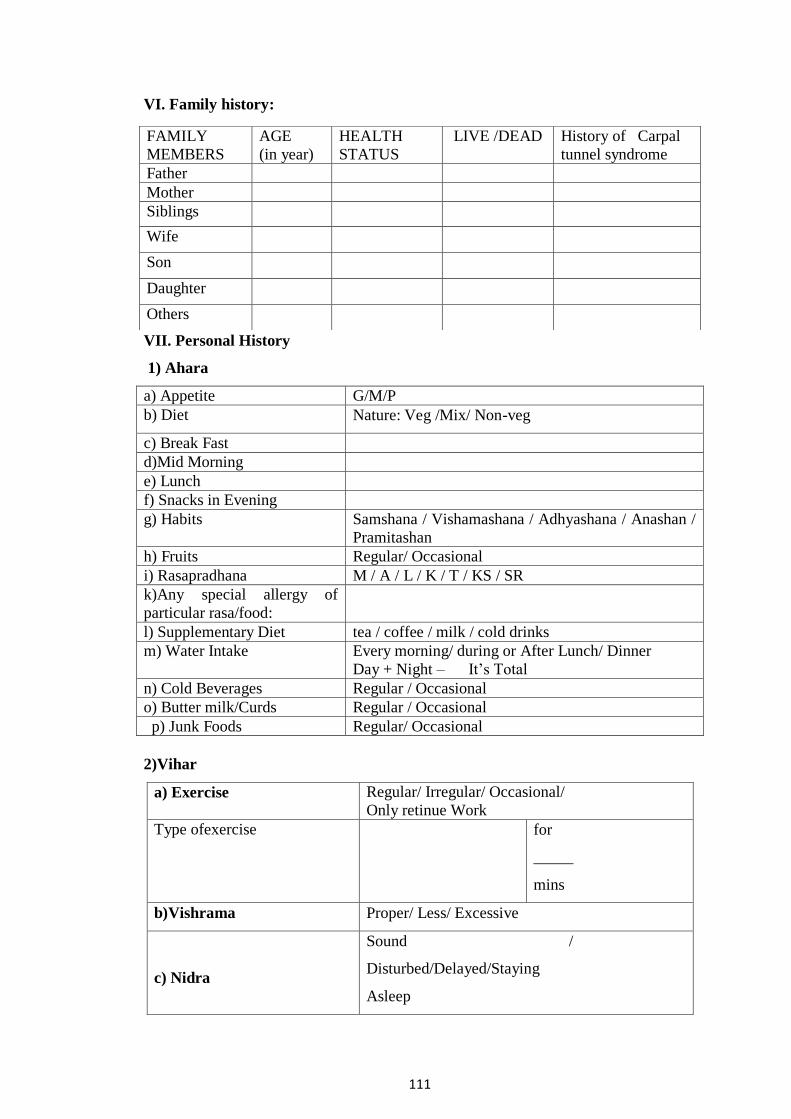
111
VI. Family history:
VII. Personal History
1) Ahara
a) Appetite G/M/P
b) Diet Nature: Veg /Mix/ Non-veg
c) Break Fast
d)Mid Morning
e) Lunch
f) Snacks in Evening
g) Habits Samshana / Vishamashana / Adhyashana / Anashan /
Pramitashan
h) Fruits Regular/ Occasional
i) Rasapradhana M / A / L / K / T / KS / SR
k)Any special allergy of
particular rasa/food:
l) Supplementary Diet tea / coffee / milk / cold drinks
m) Water Intake Every morning/ during or After Lunch/ Dinner
Day + Night – It’s Total
n) Cold Beverages Regular / Occasional
o) Butter milk/Curds Regular / Occasional
p) Junk Foods Regular/ Occasional
2)Vihar
a) Exercise Regular/ Irregular/ Occasional/
Only retinue Work
Type ofexercise for
_____
mins
b)Vishrama Proper/ Less/ Excessive
c) Nidra
Sound /
Disturbed/Delayed/Staying
Asleep
FAMILY
MEMBERS
AGE
(in year)
HEALTH
STATUS
LIVE /DEAD History of Carpal
tunnel syndrome
Father
Mother
Siblings
Wife
Son
Daughter
Others
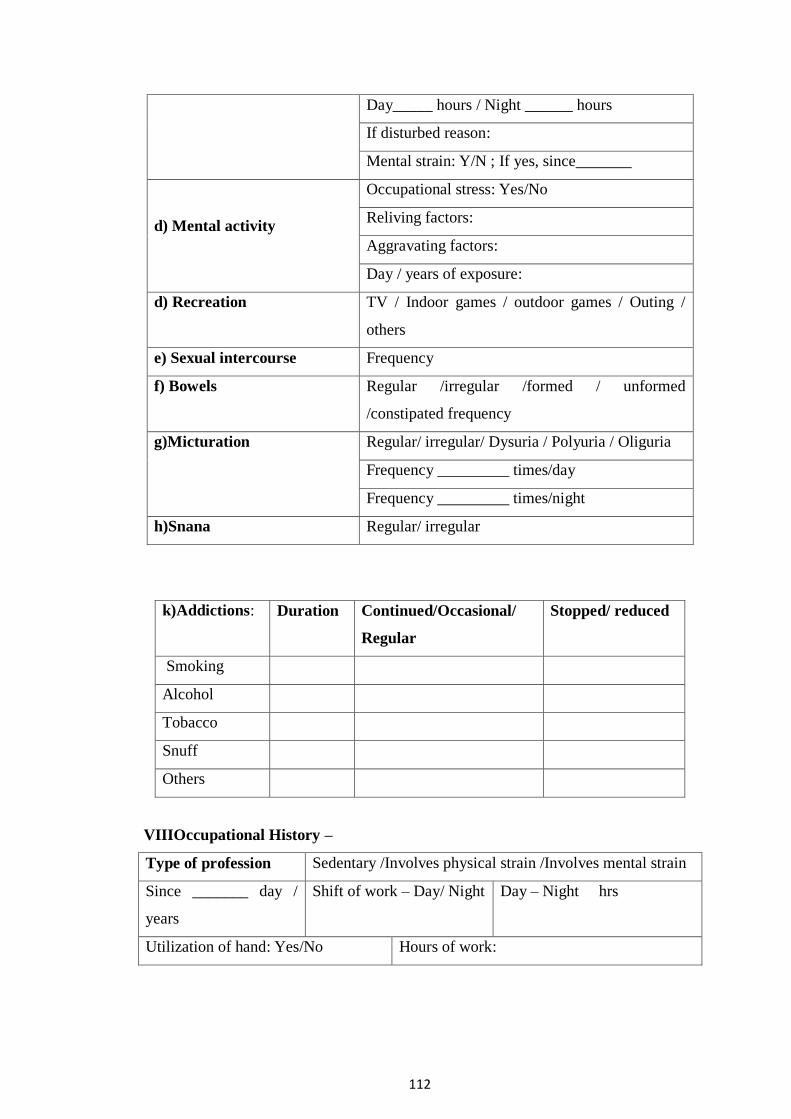
112
Day_____ hours / Night ______ hours
If disturbed reason:
Mental strain: Y/N ; If yes, since_______
d) Mental activity
Occupational stress: Yes/No
Reliving factors:
Aggravating factors:
Day / years of exposure:
d) Recreation TV / Indoor games / outdoor games / Outing /
others
e) Sexual intercourse Frequency
f) Bowels Regular /irregular /formed / unformed
/constipated frequency
g)Micturation Regular/ irregular/ Dysuria / Polyuria / Oliguria
Frequency _________ times/day
Frequency _________ times/night
h)Snana Regular/ irregular
k)Addictions: Duration Continued/Occasional/
Regular
Stopped/ reduced
Smoking
Alcohol
Tobacco
Snuff
Others
VIIIOccupational History –
Type of profession Sedentary /Involves physical strain /Involves mental strain
Since _______ day /
years
Shift of work – Day/ Night Day – Night hrs
Utilization of hand: Yes/No Hours of work:
113
IX. Gynecological history
Menarche: Bleeding days: Menopause:
Menstrual cycle:Regular□ / Irregular□ Obstretic history: P__G__L__D__A__
Menorrhagia□/Metrorrhagia□/Dysmenorrhoea□/Leucorrhoea□
History of contraception: Present □/ Absent□ Temporary : Mechanical □/
Chemical □/Oral □/Local□ / I.U.C.D□ Permanent : Tubectomy□/
Hysterectomy
X. Vital signs
Pulse :_____ per min B.P :__________mm of Hg Temperature : ______F
Heart rate :_______ per
min
Respiratory rate : ______
per min
X.Dashavidha pareeksha
Prakrithi V/P/K/VP/PK/VK/ Sama
Vikriti V / P / K
Satva P / M / A
Sara P / M / A
Samhanana P / M / A
Pramana P / M / A Height__ cms Wt____ Kg
Satmya P / M / A
Vyayamashakthi Purvakalina : P/M /A
Adyatana: P/M/A
Aharashakthi
Abhyavarnashakthi Purvakalina : P/M /A
Adyatana: P/M/A
JaranaShakthi Purvakalina : P/M/A
Adyatana:P/M/A
Vaya Bala/Madhyama / Vriddha
X.Astasthana pareeksha
Nadi
Mala
Mootra

114
Jihwa
Shabda
Sparsha
Drik
Akriti
XI. General Physical examination.
Built & nourishment: well
/mod /poor.
Pallor: P / A Cyanosis: P /
A
Icterus: P / A
Lymphadenopathy: P/A Edema: present/absent; pitting /non pitting ;
Region:
Ht: _____c.m Wt: _____ kg BMI:____kg/m2
Deformities: Tempreure: Throat: Thyroid: Normal /
abnormal
XII. Systemic Examination-
System Findings
Integumentary
Respiratory
Cardiovascular
Per abdomen
Urogenital
Musculo skeletal
Examination of hand-
INSPECTION:
RIGHT LEFT
Drooping of wrist
Wasting of thenar
eminance
Swelling
Inflamation

115
PALPATION-
RIGHT LEFT
Tenderness
Temperature
Tenal sign
Phelen sign
Pressure provocation test
Range of movement-
RIGHT LEFT
Pronation
Supination
Flexion
Extension
Rotation
Abduction
Routine Hematological Investigation.
Results LFT LIPID
PROFILE OTHERS
XIV. Nidanapanchaka:
1.Nidana –
2.Poorvaroopa-
3.Roopa-
4.Upasaya-
5.Anupasaya-
4) SAMPRAPTI GHATAKA
Nidana :
Dosha :
Dushya :
Srotas :
Srotodusti:
Ama :
Udbhavasthana :
116
Sancharasthana:
Vyaktasthana :
Rogamarga :
5) VYADHI VINISCHAYA:
6) SADHYASADHYATA:
7) UPADRAVA:
XV. CHIKITSA:
Koshtha Shodhana on day 1: Oral administration of Eranda taila in empty
stomach, in a dose of 20 ml in the morning along with 100ml warm water as after
drink.
Lashuna rasayana on day 2 to day 16: Oral administration of 12 g of Lashuna
rasayana with 100ml of milk in empty stomach, about half an hour before
breakfast.
Pitta virechana on day 17: oral administration of Eranda taila in empty stomach, in
a dose of 20 ml in the morning along with 100ml of warm water as after drink.
Diet ®imen :
Avoid hot oily spicy food
Rest
Adverse effect during treatment – yes/no
FOLLOW UP INTERVEIW:
XVI. ASSESSMENT CRITERIA:
Primary
outcome
B.T A.T Secondary outcome B.T. A.T
Symptom severity
score
Change Grip in strength
(Dynamometer)
Functional status
score
Change in visual analog
scale for pain
Change in visual analog
scale for numbess
117
VISUAL ANALOGUS SCALE;
Parameters Before treatment After treatment
Pain
Numbness
Adverse effect during treatment: yes/no
If yes:
Signature of the Guide Signature of the Scholar
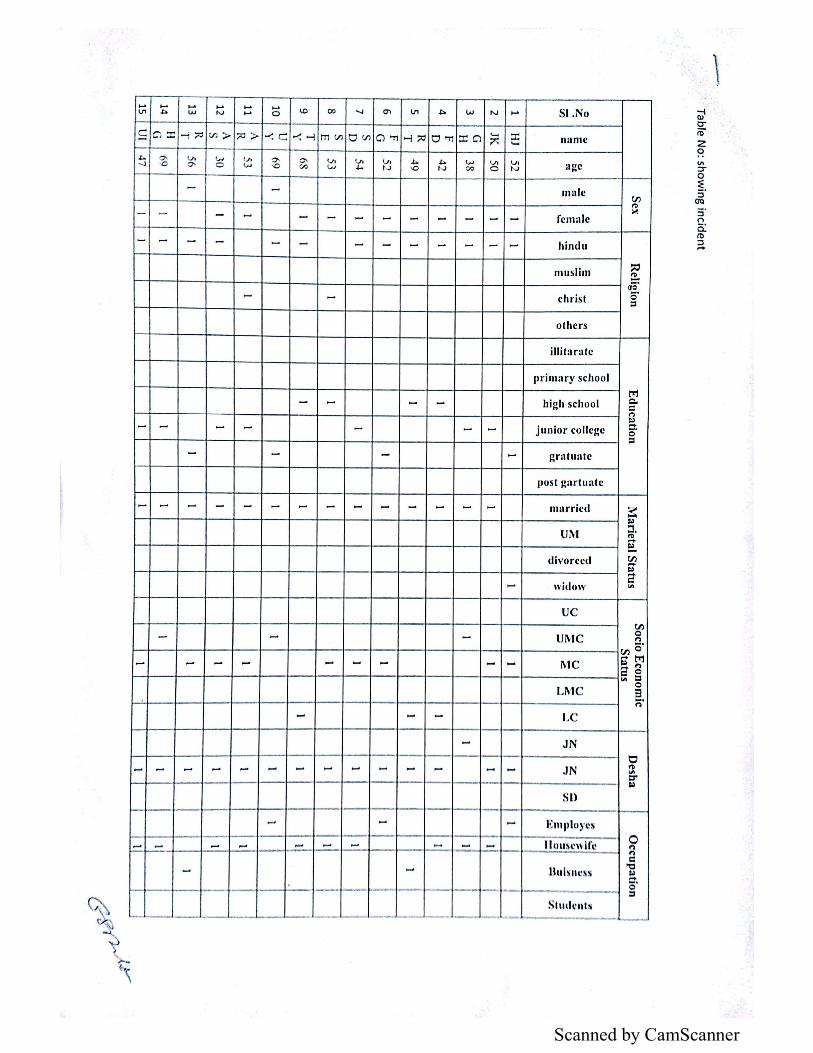
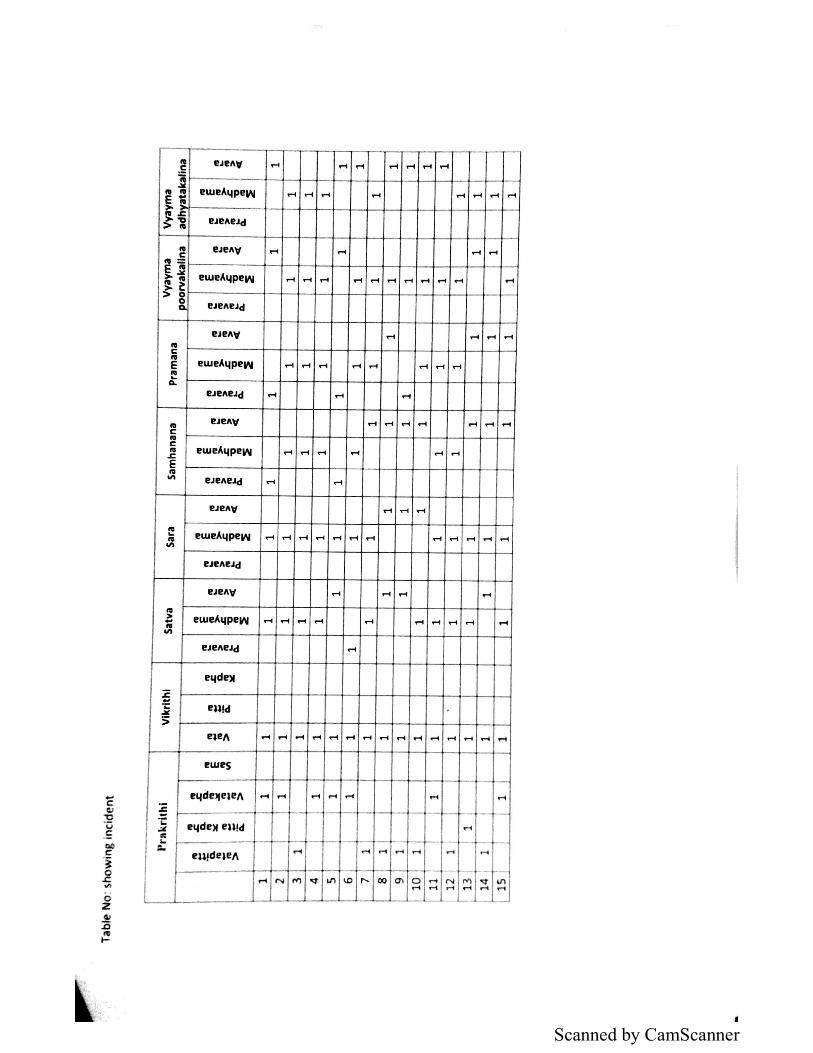
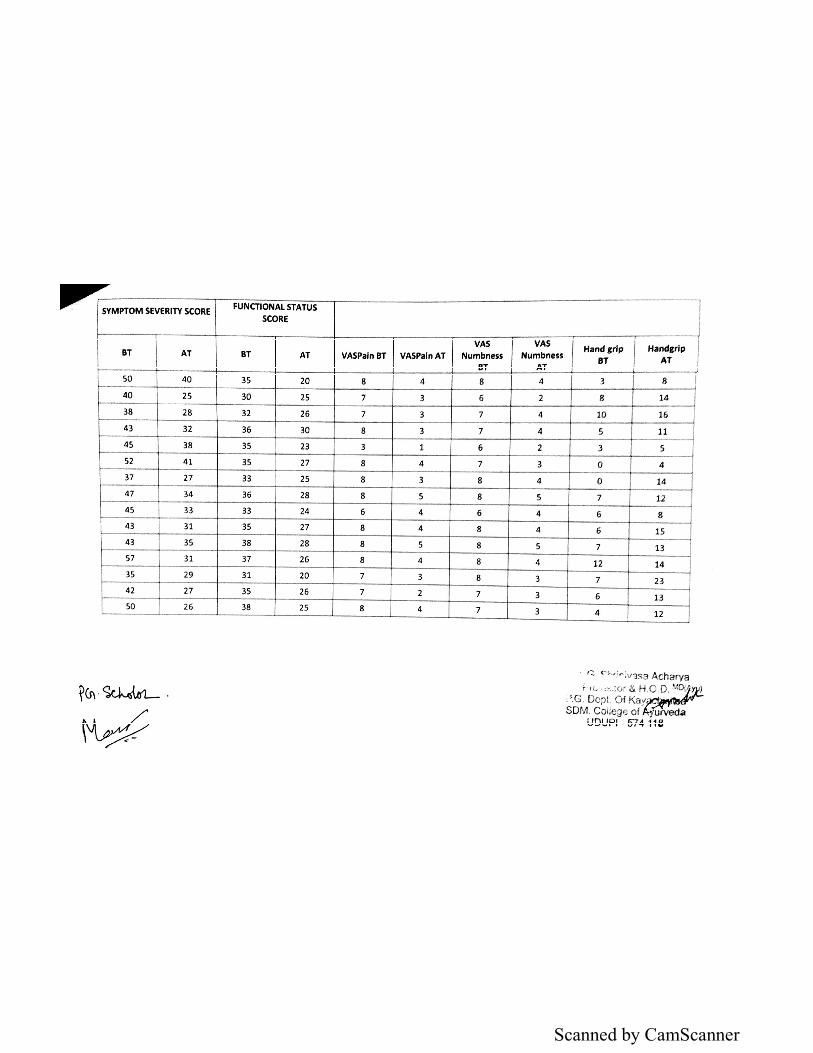
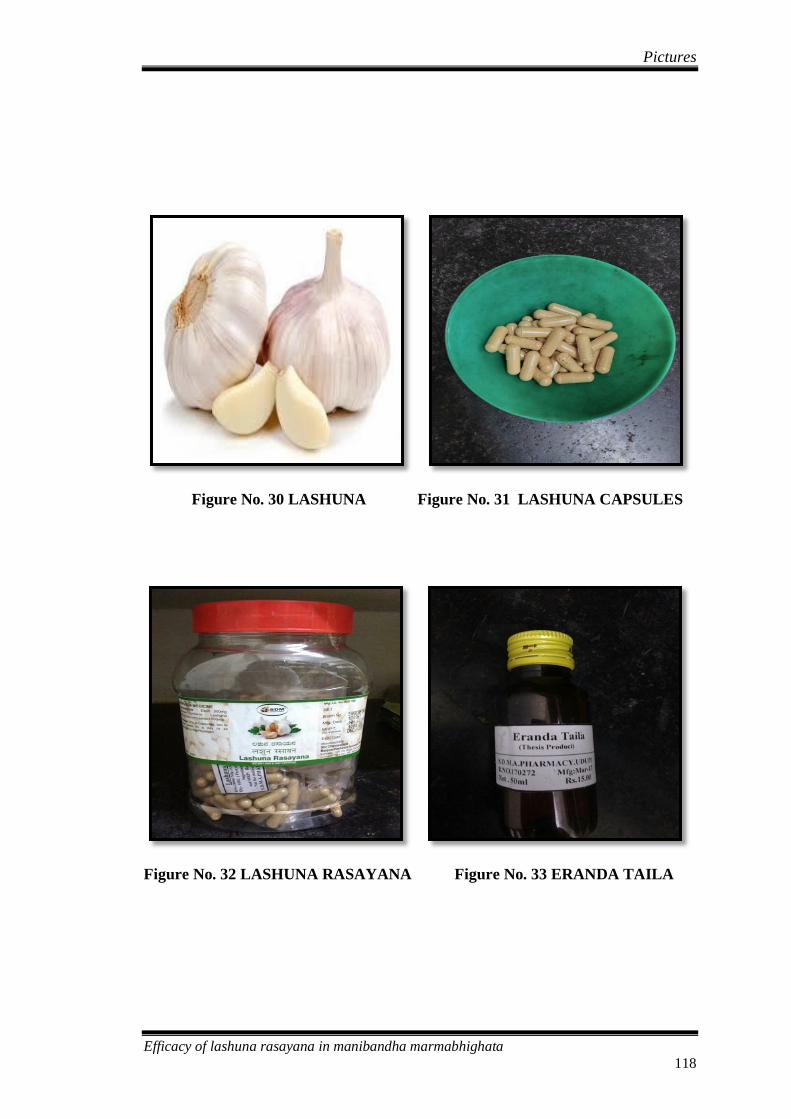
Pictures
Efficacy of lashuna rasayana in manibandha marmabhighata
118
Figure No. 30 LASHUNA Figure No. 31 LASHUNA CAPSULES
Figure No. 32 LASHUNA RASAYANA Figure No. 33 ERANDA TAILA
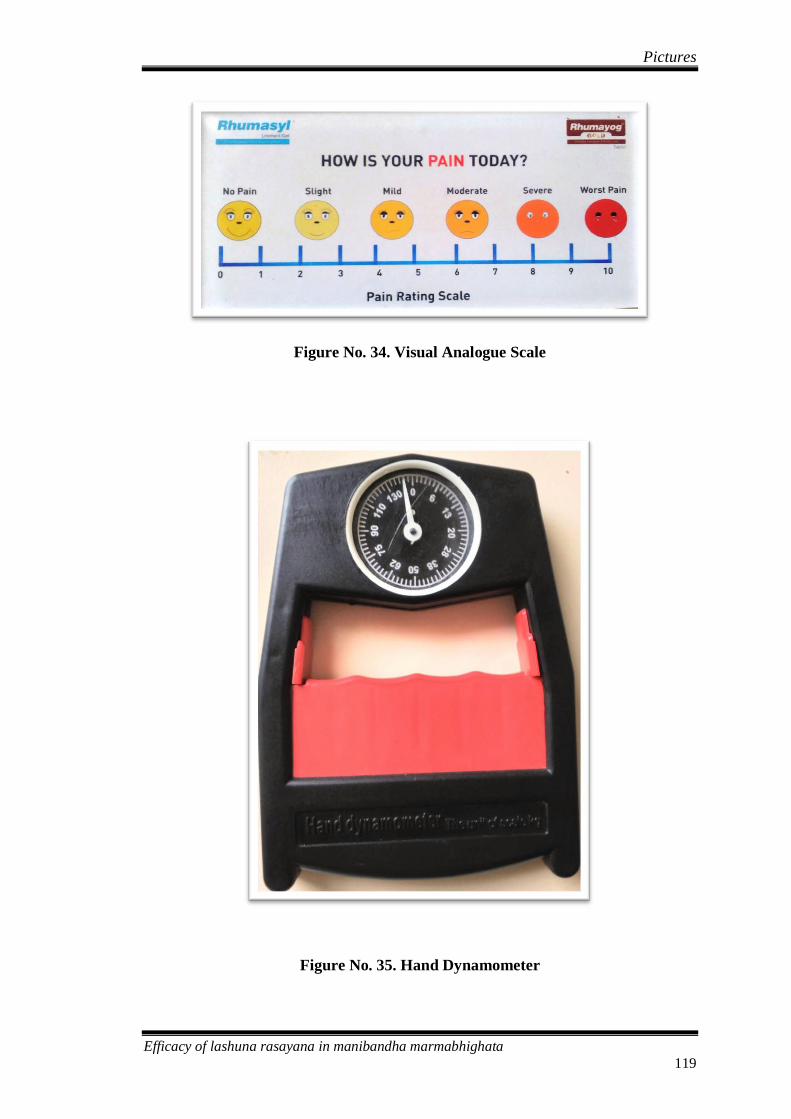
Pictures
Efficacy of lashuna rasayana in manibandha marmabhighata
119
Figure No. 34. Visual Analogue Scale
Figure No. 35. Hand Dynamometer
Related Documents











