1 23 Surgical Endoscopy And Other Interventional Techniques Official Journal of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) and European Association for Endoscopic Surgery (EAES) ISSN 0930-2794 Surg Endosc DOI 10.1007/s00464-015-4104-2 Efficacy of intracorporeal reinforcing sutures for anastomotic leakage after laparoscopic surgery for rectal cancer Kiyoshi Maeda, Hisashi Nagahara, Masatsune Shibutani, Hiroshi Ohtani, Katsunobu Sakurai, Takahiro Toyokawa, Kazuya Muguruma, et al.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1 23
Surgical EndoscopyAnd Other Interventional TechniquesOfficial Journal of the Society ofAmerican Gastrointestinal andEndoscopic Surgeons (SAGES) andEuropean Association for EndoscopicSurgery (EAES) ISSN 0930-2794 Surg EndoscDOI 10.1007/s00464-015-4104-2
Efficacy of intracorporeal reinforcingsutures for anastomotic leakage afterlaparoscopic surgery for rectal cancer
Kiyoshi Maeda, Hisashi Nagahara,Masatsune Shibutani, Hiroshi Ohtani,Katsunobu Sakurai, Takahiro Toyokawa,Kazuya Muguruma, et al.

1 23
Your article is protected by copyright and all
rights are held exclusively by Springer Science
+Business Media New York. This e-offprint is
for personal use only and shall not be self-
archived in electronic repositories. If you wish
to self-archive your article, please use the
accepted manuscript version for posting on
your own website. You may further deposit
the accepted manuscript version in any
repository, provided it is only made publicly
available 12 months after official publication
or later and provided acknowledgement is
given to the original source of publication
and a link is inserted to the published article
on Springer's website. The link must be
accompanied by the following text: "The final
publication is available at link.springer.com”.

Efficacy of intracorporeal reinforcing sutures for anastomoticleakage after laparoscopic surgery for rectal cancer
Kiyoshi Maeda • Hisashi Nagahara • Masatsune Shibutani • Hiroshi Ohtani •
Katsunobu Sakurai • Takahiro Toyokawa • Kazuya Muguruma • Hiroaki Tanaka •
Ryosuke Amano • Kenjiro Kimura • Kenji Sugano • Teturo Ikeya •
Yasuhito Iseki • Kosei Hirakawa
Received: 28 October 2014 / Accepted: 27 January 2015
� Springer Science+Business Media New York 2015
Abstract
Background The aim of the present study was to inves-
tigate the efficacy of intracorporeal reinforcing sutures for
preventing anastomotic leakage (AL) after laparoscopic
surgery for rectal cancer.
Methods This was a retrospective single-institution study
consisting of 201 consecutive patients who underwent la-
paroscopic proctectomy with double-stapling anastomosis
for primary rectal cancer between August 2007 and
December 2013. The data for patients who received in-
tracorporeal reinforcing sutures were compared with those
of patients who did not receive reinforcing sutures. Patient-
, tumor- and surgery-related variables were collected and
examined using univariate and multivariate analyses.
Results The overall incidence of AL was 9.0 % (18/201).
No significant correlations were observed between the
various clinicopathological factors and the use of rein-
forcing sutures. The multivariate analyses revealed the
distance of the tumor from the anal verge, tumor size and
presence of reinforcing sutures to be independent risk
factors for AL. We classified the patients into two risk
groups using a combination of the tumor site and tumor
size: a low-risk group (patients without any risk factors,
n = 134) and a high-risk group (patients with one or two
risk factors, n = 67). The frequency of AL was sig-
nificantly lower (p \ 0.02) in the patients treated with
reinforcing sutures than in those treated without reinforcing
sutures in the high-risk group. However, no significant
differences were observed in the low-risk group.
Conclusions The use of intracorporeal reinforcing sutures
may reduce the incidence of AL. A prospective randomized
trial is required to evaluate the effects of reinforcing su-
tures in preventing AL.
Keywords Laparoscopic surgery � Rectal cancer �Anastomotic leakage � Reinforcing suture
Several recent randomized trials have demonstrated that la-
paroscopic colectomy is similar to conventional open sur-
gery in terms of oncologic safety and is associated with
improved short-term perioperative outcomes [1–3]. La-
paroscopic rectal surgery is technically more difficult than
laparoscopic colectomy, due to difficulties related to rectal
excision and anastomosis within the narrow pelvic space.
However, an increasing number of recent studies have shown
that laparoscopic rectal surgery is safe and feasible [4–6].
Anastomotic leakage (AL) is a major problem in pa-
tients undergoing rectal cancer surgery. This complication
often requires reoperation, thus resulting in a prolonged
hospital stay as well as high morbidity and mortality. The
incidence of AL has been reported to range from 3.6 to
21 % [7–15]. Leakage can be the result of a combination of
technical, local and systemic factors, and several risk fac-
tors, including old age, a male sex, smoking habit, diabetes
mellitus, obesity, intraoperative blood loss, a longer dura-
tion of surgery, the use of more than three cartridges for
rectal transection, larger tumor size, lower tumor location
and bulky tumors, have been reported [8–15]. The double-
stapled anastomotic technique is widely used in colorectal
surgery because it allows the anastomosis to be made
very low in the pelvis and preserves the anal sphincter.
K. Maeda (&) � H. Nagahara � M. Shibutani � H. Ohtani �K. Sakurai � T. Toyokawa � K. Muguruma � H. Tanaka �R. Amano � K. Kimura � K. Sugano � T. Ikeya � Y. Iseki �K. Hirakawa
Department of Surgical Oncology, Graduate School of Medicine,
Osaka City University, 1-4-3 Asahimachi, Abeno-ku, Osaka,
Japan
e-mail: [email protected]
123
Surg Endosc
DOI 10.1007/s00464-015-4104-2
and Other Interventional Techniques
Author's personal copy

However, this technique creates stapled corners known as
‘‘dog ears,’’ which are made by crossing at least two staple
lines, potentially forming vulnerable areas. The staple line
may also become weakened via friction created by hard
stools, thus increasing the risk of anastomotic failure. In
order to address this problem, various methods have been
suggested, including the placement of intracorporeal rein-
forcing sutures at the staple line. We hypothesized that
placing the sutures to support the circular-stapled anasto-
mosis may reduce AL.
Patients and methods
Patients
We retrospectively collected and reviewed patient charac-
teristics and perioperative data after obtaining approval
from our institutional review board. Between August 2007
and December 2013, a total of 201 consecutive patients
who underwent laparoscopic proctectomy with double-
stapling anastomosis for primary rectal cancer at the
Department of Surgical Oncology, Osaka City University
Hospital, were evaluated. The location of each tumor was
within 15 cm from the anal verge. The eligibility criteria
included rectal cancer with histologically proven adeno-
carcinoma. The exclusion criteria were as follows: ab-
dominoperineal resection, Hartman’s procedure, creation
of a diverting stoma at the time of surgery, emergency
surgery, intersphincteric resection and trans-anal hand-
sewn anastomosis, total abdominal colectomy and
ileorectal anastomosis, and a history of preoperative che-
motherapy or radiation therapy. We divided the eligible
201 patients into two groups: comprising those who re-
ceived reinforcing sutures (n = 91) and those who did not
(n = 110).
Surgical procedure
All procedures were performed or supervised by two senior
surgeons (K.M. and H.N.) specialized in laparoscopic
colorectal surgery. We have routinely utilized intracorpo-
real reinforcing sutures since April 2011. Therefore, most
of the patients with reinforcing sutures underwent surgery
between 2012 and 2013. A schematic view of the rein-
forcing suture technique is shown in Fig. 1. Following
rectal division using an endo-linear stapler, end-to-end
anastomosis was performed using a circular stapler and
reinforcing sutures using 4-0 PDS (Ethicon Inc, New Jer-
sey, USA) were placed intracorporeally. Two to four in-
terrupted sutures were placed along the staple line, and the
two corners made by crossing the circular and linear staple
lines were always included. The distance from the anal
verge was determined on colonoscopy. Air leakage tests
were performed in all patients following anastomosis and
placement of the reinforcing sutures. A temporary diverting
stoma was considered in patients with several risk factors,
such as a positive air leakage test, incomplete circular
stapling donut or doubtful blood supply.
According to our hospital protocol, the patients under-
went mechanical preparation, regardless of whether the
procedure was emergent or elective. A second-generation
cephalosporin was used as a prophylactic antibiotic
(20 mg/kg). The antibiotic was administered 30 min before
surgery and thereafter every 3 h during the procedure.
Definition of anastomotic leakage
Clinical AL was defined as the presence of signs of leakage
(ex, discharge of gas, pus or feces through the pelvic drain,
peritonitis or pus discharge through the rectum) and con-
firmed on diagnostic imaging modalities, such as computed
tomography or retrograde colonography using water-sol-
uble contrast medium. Asymptomatic AL was not assessed
because routine contrast enemas were not performed after
Fig. 1 Intracorporeal view of the anastomosis and reinforcing
sutures. A Reinforcing sutures were placed at the crossing point of
the staple lines. Black arrow anastomosis White Arrow staple line.
B Two to four interrupted sutures were placed along the staple line.
Black arrows reinforcing sutures
Surg Endosc
123
Author's personal copy

surgery. All patients diagnosed with AL in this study were
identified within 14 days.
Variables
The following 21 parameters were evaluated as potential
risk factors for AL: age at the time of surgery (C75 or
\75 years), gender, body mass index (BMI C25 or
\25 kg/m2), ASA score, past history of previous laparo-
tomy, presence of myocardial infarction, chronic obstruc-
tive pulmonary disease (COPD), diabetes mellitus, tumor
site (]5 or\5 cm from the anal verge), tumor size (C4 or
\4 cm in diameter), depth of tumor invasion, regional
lymph node metastasis, operative time (C240 or
\240 min), amount of intraoperative blood loss (C600 or
\600 ml), number of stapler firings, ligation of the left
colic artery, preoperative serum C-reactive protein (CRP)
level (C1.0 or \1.0 g/ml), preoperative serum albumin
level (C3.5 or\3.5 g/ml) and the placement of reinforcing
sutures at the staple line.
All blood samples were collected either 1 or 2 weeks be-
fore surgery. The cutoff levels for the operative time and
amount of intraoperative blood loss, tumor site (distance from
the anal verge) and tumor size (tumor maximal diameter) were
determined as median values. A BMI of C25 kg/m2 is con-
sidered to reflect obesity in Japanese patients [16]; therefore,
the cutoff value for the BMI was set at 25 kg/m2.
Statistical analysis
The statistical analyses were performed using the JMP 10
software program (SAS Institute Japan, Tokyo, Japan).
Univariate analyses were performed using the Chi-square
test, Fisher’s exact test and the Mann–Whitney U test. All
variables with a p value of\0.05 in the univariate analyses
were included in a multivariate logistic regression analysis.
A p value of \0.05 was considered to be statistically
significant.
Results
Patient characteristics
The clinical characteristics of the 201 patients are sum-
marized in Table 1. The mean age at surgery was 67 years
(range 31–90). The majority of patients were classified as
having an ASA of 1 or 2 (94.5 %). A preoperative BMI of
more than 25 was observed in 46 (22.9 %) patients. With
respect to comorbidities, ischemic heart disease was
Table 1 Patient characteristics
Number
of patients
Age (years)
Median (range) 67 (31–90)
Gender
Male 118
Female 83
BMI
Median (range) 22.8 (14.3–32.8)
ASA score
1, 2 190
3 11
Previous laparotomy
Absent 163
Present 38
Myocardial infarction
Absent 182
Present 19
Chronic obstructive pulmonary disease
Absent 194
Present 7
Diabetes mellitus
Absent 159
Present 42
Tumor site (from anal verge, cm)
Median (range) 5.1 (3.0–13.5)
Tumor size (diameter, cm)
Median (range) 39.5 (4.0–90.0)
Depth of tumor invasion
T1, 2 76
T3, 4 125
Lymph node metastases
Absent 132
Present 69
Intra-operative blood loss (ml)
Median (range) 60.6 (5–960)
Number of stapler firing
C3 6
\3 195
Ligation of left colic artery
No 83
Yes 118
Operation time (min)
Median (range) 238 (131–425)
Preoperative serum CRP level (g/dl)
C1 13
\1 188
Surg Endosc
123
Author's personal copy

observed in 19 (9.5 %) patients, diabetes mellitus was
observed in 42 (20.9 %) patients and chronic obstructive
pulmonary disease was observed in seven (3.5 %) patients.
Forty-five patients (22.1 %) presented with rectal cancer
within 5 cm from the anal verge.
The correlations between the various clinicopathological
factors and the presence of reinforcing sutures are shown in
Table 2. There were no significant differences between the
two groups.
The overall incidence of AL was 9.0 % (18/201).
Among these patients, re-laparotomy was required in five
cases; all five patients received a protective stoma and then
quickly recovered. The remaining 13 patients recovered
with conservative treatment. The median time to hospital
discharge was 37 days (range 21–67), and there were no
deaths related to AL.
We classified the patients into two groups based on the
period in which the surgery was performed. One hundred
and eleven patients who underwent surgery between 2007
and 2011 were classified into the early period group, and
the other 90 patients who underwent surgery between 2012
and 2013 were classified into the late period group
(Table 3). The median operative time for reinforcing su-
tures and the frequency of AL were compared among these
groups. As a result, the operative time for reinforcing su-
tures tended to be shorter in the late period group than in
the early period group; however, there were no significant
differences between the two groups. Otherwise, although
the frequency of AL was lower in the late period group
than in the early period group, there were no significant
differences between the two groups.
The results of univariate analyses of the risk factors
potentially associated with AL are shown in Table 4. Ten
factors (BMI of C25, diabetes mellitus, tumor site from the
anal verge of C5 cm, tumor diameter of C4 cm, operative
time of C4 h, operative blood loss of C60 ml, number of
stapler firings C3, depth of tumor invasion CT3 and use of
reinforcing sutures) were found to be significantly corre-
lated with AL. Regarding the correlation between the in-
cidence of AL and the presence of reinforcing sutures, the
rate of AL was 3.3 % (3/91) in the patients treated with
reinforcing sutures, which was significantly (p \ 0.01)
lower than that observed in the patients without reinforcing
sutures (13.6 %, 15/110). Meanwhile, the multivariate
Table 1 continued
Number
of patients
Preoperative serum albumin level (g/dl)
C3.5 189
\3.5 12
BMI body mass index
Table 2 Correlations between various clinicopathological factors
and the use of reinforcing sutures
Variables Reinforcing sutures p value
Yes No
(n = 91) (n = 110)
Age (years)
C75 24 24 0.45
\75 67 86
Gender
Male 52 66 0.68
Female 39 44
BMI
C25 17 29 0.2
\25 74 81
ASA score
1, 2 87 103 0.76
3 4 7
Previous laparotomy
Absent 74 89 0.94
Present 17 21
Myocardial infarction
Absent 83 99 0.77
Present 8 11
COPD
Absent 89 105 0.60
Present 2 5
Diabetes mellitus
Absent 76 83 0.16
Present 15 27
Tumor site (from anal verge, cm)
C5 66 90 0.12
\5 25 20
Tumor size (cm)
C4 20 23 0.85
\4 71 87
Depth of tumor invasion
T1, 2 38 38 0.29
T3, 4 53 72
Lymph node metastases
Absent 61 71 0.71
Present 30 39
Intra-operative blood loss (ml)
C60 16 25 0.37
\60 75 85
Number of stapler firing
C3 1 5 0.31
\3 90 105
Ligation of left colic artery
No 43 40 0.12
Yes 48 70
Surg Endosc
123
Author's personal copy
analyses revealed a tumor site from the anal verge of
B5 cm, tumor size of C4 cm and the absence of reinforc-
ing sutures to be independent risk factors for AL (Table 5).
We classified the patients into two risk groups using a
combination of tumor-related risk factors (tumor site from
the anal verge of B5 cm and tumor size of C4 cm). The
patients were classified into the low-risk group (patients
without any risk factor, n = 134) and high-risk group
(patients with one or two risk factors, n = 67). Moreover,
the frequency of AL was compared between the patients
treated with and without reinforcing sutures (Table 6). The
frequency of AL was significantly lower (p \ 0.02) in the
patients treated with reinforcing sutures than in the patients
treated without reinforcing sutures in the high-risk group.
However, there were no differences in the low-risk group.
Discussion
Anastomotic leakage is a major problem in rectal cancer
surgery, and it is associated with both postoperative mor-
bidity and mortality. Even now, the effects of leakage on
the oncologic outcomes are not clear, although some re-
ports have suggested that AL results in increased rates of
local recurrence and a poor survival [16–18]. Several risk
factors for AL in patients with laparoscopic rectal surgery
have been identified in previous reports [8–15]. In the
current study, we found the tumor size, tumor site from the
anal verge and use of reinforcing sutures to be independent
risk factors for symptomatic AL.
Various methods have been applied to reduce the inci-
dence of AL in patients with these risk factors. Park et al.
[14] and Tan et al. [19] reported that diverting stomas are
mandatory in patients with two or more risk factors.
Meanwhile, Ito et al. [20] reported that vertical rectal
transection via an additional suprapubic site could be used
to avoid multiple stapler firings, resulting in a decreased
rate of AL, and Xiao et al. [21], Zhao et al. [22] and
Nishigori et al. [23] reported that trans-anal decompression
tubes are useful for preventing AL. Recently, Gadiot et al.
[24] examined patients who undergoing left-sided colec-
tomy, sigmoidectomy and anterior resection and reported
that the placement of sutures at the site of anastomosis to
reduce traction resulted in a reduction of AL. All of these
reports examined patients treated with double-stapling
anastomosis. Double-stapling anastomosis is a widely used
and useful technique; however, it creates weak points,
made by crossing staple lines. In the present study, we
examined the efficacy of placing intracorporeal reinforcing
sutures at the crossing staple line for reducing the rate of
AL. As a result, although there were no significant differ-
ences in the low-risk group, the frequency of AL was
significantly lower in the patients treated with reinforcing
sutures than in those treated without reinforcing sutures in
the high-risk group. Therefore, reinforcing sutures are
thought to be useful for reducing AL in the high-risk pa-
tients, although they may be unnecessary in the low-risk
patients. In the case of open surgery, it is difficult to apply
reinforcing sutures, especially in patients treated with very
low anterior resection, due to the limited visual field re-
sulting from the narrow pelvic field. Otherwise, laparo-
scopic surgery has the advantage of providing better
magnified visualization with endoscopy; therefore, it is
easier to place reinforcing sutures under laparoscopic ver-
sus open surgery. Even under laparoscopic visualization,
placing reinforcing sutures is technically difficult in some
cases, especially in high-risk patients. Although the use of
a diverting stoma requires at least once additional surgery,
which can impact the patient’s quality of life, several
studies [14, 19] reported that the frequency of AL is sig-
nificantly lower in patients with a diverting stoma. There-
fore, a diverting stoma should be created in patients whom
reinforcing sutures cannot be accomplished.
The present study has several limitations. First, this
study was not randomized, and there may have been se-
lection bias in the decision to place reinforcing sutures. A
prospective randomized trial is, therefore, needed to eval-
uate the effects of reinforcing sutures on AL. Second, most
of the patients with reinforcing sutures belonged to the late
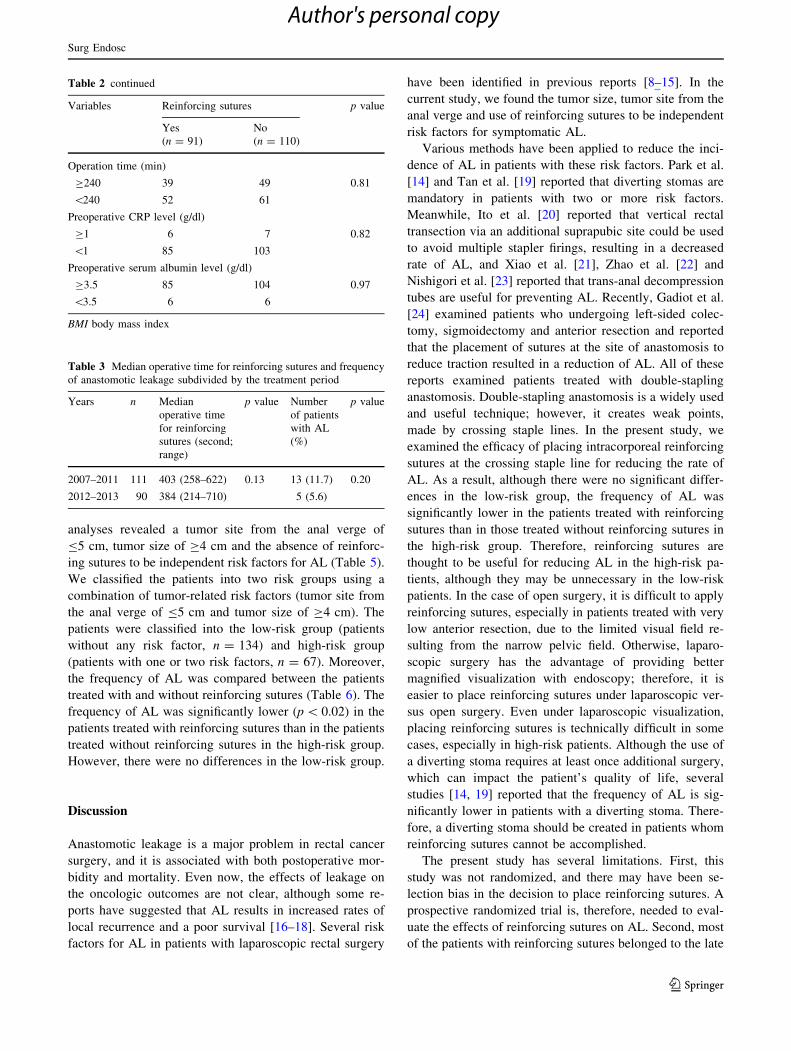
Table 2 continued
Variables Reinforcing sutures p value
Yes No
(n = 91) (n = 110)
Operation time (min)
C240 39 49 0.81
\240 52 61
Preoperative CRP level (g/dl)
C1 6 7 0.82
\1 85 103
Preoperative serum albumin level (g/dl)
C3.5 85 104 0.97
\3.5 6 6
BMI body mass index
Table 3 Median operative time for reinforcing sutures and frequency
of anastomotic leakage subdivided by the treatment period
Years n Median
operative time
for reinforcing
sutures (second;
range)
p value Number
of patients
with AL
(%)
p value
2007–2011 111 403 (258–622) 0.13 13 (11.7) 0.20
2012–2013 90 384 (214–710) 5 (5.6)
Surg Endosc
123
Author's personal copy

period group. The laparoscopic surgical skills may have
been better in the late period than in the early period.
Although the learning curve for laparoscopic surgery may
have slightly affected to the reduction in the frequency of
AL in the late period group, the rate of AL was not sig-
nificantly different between the early period group and the
late period group.
In conclusion, our findings demonstrate that the use of
intracorporeal reinforcing sutures may reduce the incidence
Table 4 Univariate analyses according to the correlations between
various clinicopathological factors and the presence of anastomotic
leakage
Variables Anastomotic leakage p value
Present Absent
(n = 18) (n = 183)
Age (years)
C75 15 78 0.22
\75 3 105
Gender
Male 15 138 0.45
Female 3 45
BMI
C25 10 145 0.02
\25 8 38
ASA score
1, 2 16 174 0.27
3 2 9
Previous laparotomy
Absent 19 149 0.80
Present 5 34
Myocardial infarction
Absent 15 167 0.27
Present 3 16
COPD
Absent 18 178 0.40
Present 0 5
Diabetes mellitus
Absent 10 149 0.01
Present 8 34
Tumor site (from anal verge; cm)
C5 8 148 0.004
\5 10 35
Tumor size (cm)
C4 12 71 0.02
\4 6 112
Depth of tumor invasion
T1, 2 0 75 0.006
T3, 4 18 108
Lymph node metastases
Absent 10 121 0.35
Present 8 61
Intra-operative blood loss (ml)
C60 8 33 0.0008
\60 10 150
Number of stapler firing
C3 3 3 0.0004
\3 15 180
Ligation of left colic artery
No 4 76 0.23
Yes 14 107
Table 4 continued
Variables Anastomotic leakage p value
Present Absent
(n = 18) (n = 183)
Operation time (min)
C240 16 72 \0.0001
\240 2 111
Reinforcing suture of the staple line
No 15 95 0.01
Yes 3 88
Preoperative serum CRP level (g/dl)
C1 0 13 0.24
\1 18 110
Preoperative serum albumin level (g/dl)
C3.5 16 173 0.33
\3.5 2 10
BMI body mass index
Table 5 Multivariate analyses according to the correlations between
various clinicopathological factors and the presence of anastomotic
leakage
Variables Multivariate analysis p value
Odds ratio 95 % CI
BMI
C25 versus \25 1.80 0.58–5.63 0.31
Diabetes mellitus
Present versus absent 2.07 0.65–6.52 0.21
Tumor site (from anal verge, cm)
\5 versus C5 7.13 2.61–17.4 0.01
Tumor size (cm)
C4 versus \4 4.89 1.36–8.87 0.02
Depth of tumor invasion
T3, 4 versus T1, 2 2.69 0.73–9.86 0.12
Operation time (min)
C240 versus \240 2.24 0.61–8.28 0.22
Number of stapler firing
C3 versus \3 1.16 0.15–7.73 0.88
Reinforcing suture of the staple line
No versus yes 4.65 1.36–13.2 0.02
BMI body mass index
Surg Endosc
123
Author's personal copy

of AL. However, a prospective randomized trial is still
needed to evaluate the effects of reinforcing sutures for
preventing AL.
Disclosures Drs Kiyoshi Maeda, Hisashi Nagahara, Masatsune
Shibutani, Hiroshi Otani, Kenji Sugano, Ikeya Tetsuro, Yoshihito
Iseki, Katsunobu Sakurai, Takahiro Toyokawa, Kazuya Muguruma,
Hiroaki Tanaka, Ryosuke Amano, Kenjiro Kimura and Kosei Hi-
rakawa have no conflicts of interest or financial ties to disclose.
References
1. Leung KL, Kwok SP, Lam SC, Lee JF, Yiu RY, Ng SS, Lai PB,
Lau WY (2004) Laparoscopic resection of rectosigmoid carci-
noma: prospective randomized trial. Lancet 363:1187–1192
2. Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AM,
Heath RM, Brown JM (2005) Short-term endpoints of conven-
tional vs laparoscopic-assisted surgery in patients with colorectal
cancer (MRC CLASICC trial): multicenter, randomised con-
trolled trial. Lancet 350:2050–2059
3. Patankar SK, Larach SW, Ferrara A, Willamson PR, Gallagher
JT, Dejesus S, Narayanan S (2003) Prospective comparison of
laparoscopic vs. open resection for colorectal adenocarcinoma
over a ten-year period. Dis Colon Rectum 46:601–611
4. Zhou ZG, Hu M, Li Y, Lei WZ, Yu YY, Cheng Z, Li L, Shu Y,
Wang TC (2004) Laparoscopic vs open total mesorectal excision
with anal sphincter preservation for low rectal cancer. Surg En-
dosc 18:1211–1215
5. Kujan J, Valero G, Hernmandez Q, Sanchez A, Frutos MD,
Parrilla P (2009) Randomized clinical trial comparing laparo-
scopic or open surgery in patients with rectal cancer. Br J Surg
96:982–989
6. Milson JW, de Oliveria O, Trencheva KI Jr, Panddey S, Lee SW,
Sonoda T (2009) Long-term outcomes of patients undergoing
curative laparoscopic surgery for mid and low rectal cancer. Dis
Colon Rectum 52:1215–1222
7. Cong ZJ, Hu LH, Bian ZQ, Ye GY, Yu MH, Gao YH, Li ZS, Yu
ED, Zhong M (2013) Systematic review of anastomotic leakage
rate according to an International Grading System following
anterior resection for rectal cancer. PLoS One 8(9):e75519.
doi:10.1371/journal.Pone.0075519
8. Taflamps P, Christodoulakins M, Tsiftsis D (2009) Anastomotic
leakage after low anterior resection for rectal cancer: facts, Ob-
scurity and Fiction. Surg Today 39:183–188
9. Trencheva K, Morrissey KP, Wells M, Mancuso CA, Lee SW,
Sonoda T, Michelassi F, Charlson ME, Milson JW (2013) Iden-
tifying important predictors of anastomotic leak after colon and
rectal resection: prospective study on 616 patients. Ann Surg
257:108–113
10. Caulfield H, Hyman NH (2013) Anastomotic leak after low an-
terior resection: a spectrum of clinical entities. JAMA Surg
148:177–182
11. Akiyoshi T, Ueno M, Fukunaga Y, Nagayama S, Fujimoto Y,
Konishi T, Kuroyanagi H, Yamaguchi T (2012) Incidence of and
risk factors for anastomotic leakage after laparoscopic anterior
resection with intra corporeal rectal transaction and double-sta-
pling technique anastomosis for rectal cancer. Am J Surg
202:259–264
12. Yamamoto S, Fujita S, Akasu T, Inada R, Moriya Y, Yamamoto
S (2012) Risk factors for anastomotic leakage after laparoscopic
surgery for rectal cancer using a stapling technique. Surg La-
parosc Endosc Perctan Tech 22:239–243
13. Kawada K, Hasegawa S, Hida K, Hirai K, Okoshi K, Nomura A,
Kawamura J, Nagayama S, Sakai Y (2014) Risk factors for
anastomotic leakage after laparoscopic low anterior resection
with DST anastomosis. Surg Endosc 28:2988–2995
14. Park JS, Choi GS, Kim SH, Kim HR, Kim NK, Lee KY, Kang
SB, Kim JY, Lee KY, Kim BC, Bae BN, Son GM, Lee SH, Kang
H (2013) Multicenter analysis of risk factors for anastomotic
leakage after laparoscopic rectal cancer excision. Ann Surg
257:665–671
15. Kim JS, Cho SY, Min BS, Kim NK (2009) Risk factors for
anastomotic leakage after laparoscopic intracorporeal colorectal
anastomosis with double stapling technique. J Am Coll Surg
209:694–701
16. Branagan P, Finnis D (2005) Prognosis after anastomotic leakage
in colorectal surgery. Dis Colon Rectum 48:1021–1026
17. Walker KG, Bell SW, Rickard MJ (2004) Anastomotic leakage is
predictive of diminished survival after anterior resection after
potentially curative resection for colorectal cancer. Ann Surg
240:255–259
18. Krarup PM, Nordholm-Carstensen A, Jorgensen LN, Harling H
(2014) Anastomotic leak increases distant recurrence and long-
term mortality after curative resection for colonic cancer—a na-
tionwide cohort study. Ann Surg 259:930–938
19. Tan WS, Tang CL, Shi L, Eu KW (2009) Meta-analysis of de-
functioning stomas in low anterior resection for rectal cancer. Br
J Surg 96:462–472
20. Ito M, Sugito M, Kobayashi A, Nishizawa Y, Tsunoda Y, Saito N
(2008) Relationship between multiple numbers of stapler firings
during rectal division and anastomotic leakage after laparoscopic
rectal resection. Int J Colorectal Dis 23:703–707
21. Xiao L, Zhang WB, Jiang PC, Bu XF, Yan Q, Zhang YJ, Yu F
(2010) Can transanal tube placement after anterior resection for
rectal carcinoma reduce anastomotic leakage rate? A single-insti-
tution prospective randomized study. World J Surg 35:1367–1377
22. Zhao WT, Hu FL, Li YY, Li HJ, Luo WM, Sun F (2013) Use of a
transanal drainage tube for prevention of anastomotic leakage and
bleeding after anterior resection for rectal cancer. World J Surg
37:227–232
Table 6 Correlations between
the frequency of anastomotic
leakage and use of reinforcing
sutures subdivided according to
the risk group
AL anastomotic leakage
Reinforcing suture AL Frequency of AL (%) p value
Present Absent
High risk
Yes 2 32 5.9
No 10 23 30.3 0.02
Low risk
Yes 2 55 3.5
No 4 73 5.2 0.88
Surg Endosc
123
Author's personal copy

23. Nishigori H, Ito M, NIshizawa Y, Kobayashi A, Sugito M, Saito
N (2014) Effectiveness of a transanal tube for the prevention of
anastomotic leakage after rectal cancers surgery. World J Surg
38:1843–1851
24. Gadiot RPM, Dunker MS, Mearadji A, Hannaerts GHH (2011)
Reduction of anastomotic failure in laparoscopic antitraction
sutures. Surg Endosc 25:68–71
Surg Endosc
123
Author's personal copy
Related Documents



![Right and Wrong Approaches To Colorectal Anastomotic ...through the anastomosis was defined as anastomotic stenosis.[8] Anastomotic stenosis occurring after per-forming anastomosis](https://static.cupdf.com/doc/110x72/60ff5ab4e7dbf06e7d5abd91/right-and-wrong-approaches-to-colorectal-anastomotic-through-the-anastomosis.jpg)







