Efficacy and safety of a cisplatin and paclitaxel (TP) induction regimen followed by chemoradiotherapy for patients with locally advanced head and neck squamous cell carcinoma (LAHNSCC). ClinicalTrials.gov Identifier: NCT00959387 Running head: cisplatin and paclitaxel induction chemotherapy for LAHNSCC Luciano de Souza Viana, Felipe Coelho de Aguiar Silva, Alexandre Andrade dos Anjos Jacome, Danielle Calheiros Campelo Maia, Marcos Duarte de Mattos, Alexandre Arthur Jacinto, Augusto Elias Mamere, Domingos Boldrini Junior, Renato de Castro Capuzzo, Carlos Roberto Santos, Andre Lopes Carvalho Barretos Cancer Hospital, Brazil Corresponding author: Luciano de Souza Viana Rua Antenor Duarte Vilela, 1331, Bairro Dr. Paulo Prata, Barretos, São Paulo, Brazil. ZIP CODE: 14 784-400 [email protected] +55 17 3321 6600 ext6953 +55 17 3321 6600 Funding: Barretos Cancer Hospital Disclaimers: No potential conflicts of interest This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process which may lead to differences between this version and the Version of Record. Please cite this article as an ‘Accepted Article’, doi: 10.1002/hed.24137 This article is protected by copyright. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Efficacy and safety of a cisplatin and paclitaxel (TP) induction regimen followed
by chemoradiotherapy for patients with locally advanced head and neck squamous
cell carcinoma (LAHNSCC).
ClinicalTrials.gov Identifier: NCT00959387
Running head: cisplatin and paclitaxel induction chemotherapy for LAHNSCC
Luciano de Souza Viana, Felipe Coelho de Aguiar Silva, Alexandre Andrade dos Anjos
Jacome, Danielle Calheiros Campelo Maia, Marcos Duarte de Mattos, Alexandre Arthur
Jacinto, Augusto Elias Mamere, Domingos Boldrini Junior, Renato de Castro Capuzzo,
Carlos Roberto Santos, Andre Lopes Carvalho
Barretos Cancer Hospital, Brazil
Corresponding author:
Luciano de Souza Viana
Rua Antenor Duarte Vilela, 1331, Bairro Dr. Paulo Prata, Barretos, São Paulo,
Brazil. ZIP CODE: 14 784-400
+55 17 3321 6600 ext6953
+55 17 3321 6600
Funding: Barretos Cancer Hospital
Disclaimers: No potential conflicts of interest
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/hed.24137
This article is protected by copyright. All rights reserved.

2
ABSTRACT
Background: The purpose of this phase II trial was to evaluate the tolerability, safety
and efficacy of a non-5-FU-based induction chemotherapy followed by
chemoradiotherapy (CRT) for patients with locally advanced head and neck squamous
cell carcinoma (LAHNSCC).
Methods: Sixty patients with stage III-IV HNSCC were treated with induction TP
(paclitaxel 175mg/m2; cisplatin 80mg/m
2 – 3 cycles) followed by CRT (cisplatin
100mg/m2; D1, 22 and 43 of radiotherapy).
Results: Fifty-six patients (93.3%) completed three-cycles of induction TP (no
treatment-related deaths), 52 (86.7%) completed definitive CRT per protocol (AE grade
≥2 in 53.3%). The overall response rate (ORR) after induction TP was 82.5% for
patients with resectable disease (RD) and 55.5% for unresectable disease (UD)
(p=0.023), and complete response rate after CRT was 70.0% for patients with RD and
30.0% for UD (p=0.005).
Conclusion: Induction TP followed by cisplatin based-CRT was well tolerated, safe
and had high ORR in selected patients with LAHNSCC.
KEY WORDS: head and neck cancer; induction chemotherapy; chemoradiation
therapy; organ preservation; squamous cell carcinoma
Page 2 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

3
INTRODUCTION
Head and neck squamous cell carcinoma (HNSCC) is the sixth most common cancer
worldwide.(1) Its treatment is complex and evolving. In general, early-stage disease
may be managed with single-modality treatment while an advanced stage (about 60% of
clinical presentation) needs a multidisciplinary approach.(2)
Over the last 30 years, much has been learned regarding the role of
chemotherapy, radiation therapy, and combined-modality treatment with
chemoradiation (CRT) in the therapy of locally advanced head and neck cancer.(3) As
the taxanes have been proven to have significant single-agent activity in advanced
disease there is increasing interest in the incorporation of taxanes into induction
regimens in the treatment of patients with locally advanced HNSCC (LAHNSCC).(4-
11)
The results reported in the TAX 323 (6) and TAX 324 (12) trials indicate that
the TPF regimen (docetaxel, cisplatin and 5-fluorouracil) improves overall survival
comparing with the PF regimen (cisplatin and 5-fluorouracil), and the TPF regimen is
globally the most accepted induction regimen for the treatment of LAHNSCC (10).
However, this new regimen has been associated with high toxicity rates, and patients
frequently do not tolerate cisplatin during concurrent radiotherapy.(6, 12-14)
Although sequential treatment with an aggressive induction chemotherapy (IC)
regimen leads to high response rates and enhanced complete response rates prior to
chemoradiotherapy, recently, the DeCIDE(15), PARADIGM(16) and the Spanish Head
and Neck Cancer Cooperative Group(14) trial failed to demonstrate overall survival
benefit from the addition of IC to definitive chemoradiotherapy. The use of
chemoradiotherapy regimens that are not generally considered the standard of care, the
early termination of the trial (17) and the number of patients that did not receive CRT
Page 3 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

4
after induction due to toxicity(14) are possibility reasons for the lack of difference in
survival in these trials. Therefore, the standard of care for most clinicians is a
multidisciplinary approach with cisplatin-based concurrent chemoradiotherapy.(14)
Recent publication of the randomized phase II TREMPLIN trial suggests that
sequential therapy using TPF regimen during induction phase followed by concurrent
therapy based on cisplatin is feasible and safe. But, a key observation of authors of this
trial was that CRT or bioradiotherapy (BRT) based on cetuximab was difficult to deliver
after TPF based IC because of limiting acute toxicity.(18)
The head and neck patients are often a relatively unfit group with significant
comorbidity and from a poor socio-economic class. There is significant concern that the
benefits of TPF may be lost in a non-trial cohort of patients who are likely to be less
fit.(19) This concern is warranted, as a retrospective study reported 15.3% mortality
during IC with a TPF regimen in LAHNSCC patients of low socioeconomic status and
high tumor burden. Furthermore, the administration of IC precluded 38.2% of these
patients from initiating or completing the planned definitive therapy (20). Similarly,
Sanders and co-authors also reported high toxicity rates during retrospective analysis of
sequential TPF chemotherapy followed by concurrent chemoradiotherapy in
LAHNSCC. In this study, 32% of patients were admitted as an emergency after TPF
chemotherapy, two patients had a fatal event while on TPF (1 cerebrovascular accident
and 1 neutropenic sepsis) and only 64% of patients received at least two cycles during
concurrent chemotherapy. As a result, the authors have suggested that strict criteria
should be enforced to eligibility for induction chemotherapy with TPF.(19, 21)
Preliminary data from a prospective study of the Dutch Head and Neck Society
named CONDOR study was presented at the American Society for Clinical Oncology
(ASCO) 2013 Annual Meeting. The authors concluded that after IC with TPF cisplatin-
Page 4 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

5
containing concomitant CRT is not feasible in LAHNSCC, because the total planned
dose of cisplatin could only be administered in 32% of the patients due to severe
toxicity (unpublished data).
Consequently, extensive efforts are ongoing to identify alternative schemes that
are less toxic than but as effective as the TPF regimen for LAHNSCC and safely allow
the use of definitive concurrent treatment based on cisplatin and radiotherapy.(22-29)
This phase II trial was designed to evaluate the feasibility of delivering cisplatin
concurrent with radiotherapy after 3 cycles of an IC regimen based on the combination
of cisplatin plus paclitaxel in LAHNSCC patients with a high tumor burden.
PATIENTS AND METHODS
Study Design
This was a prospective, single center, open-label, non-randomized phase II trial.
The study was approved by the Local Research Ethic Committee and was conducted in
accordance with the Declaration of Helsinki, Good Clinical Practice, and local ethical
and legal requirements. All patients signed an informed consent document prior to
enrollment in the study.
Eligibility Criteria
Patients were eligible if they had histologically confirmed locally advanced
stage III or IVa-b (M0) squamous cell carcinoma of the larynx, oral cavity, oropharynx
or hypopharynx. All patients were required to have measurable disease by Response
Evaluation Criteria in Solid Tumors (RECIST, version 1.1), an ECOG-PS ≤ 2 (Eastern
Cooperative Oncology Group Performance Status), age of at least ≥ 18 years and
Page 5 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

6
adequate liver, renal and bone marrow function. Oral cavity patients were included only
if they had unresectable disease.
Patients were excluded from the study if they had previously received
chemotherapy, radiotherapy or surgery (except diagnostic biopsy) for the primary tumor
or lymph nodes, or if they were using concurrent investigational, biological or immune
therapies. Other exclusion criteria included a history of another malignancy, presence of
a serious concomitant illness, a psychiatric illness that would preclude providing
informed consent.
Interventions
The allocation of all patients according to their resectability status, as defined by
the primary site and staging of the tumor (according to 6th edition of the AJCC criteria),
was performed by a multidisciplinary team consisting of medical oncologist, head and
neck surgeon, radiologist and radiation oncologist before starting IC.
The tumor was classified as unresectable if exists at least one of the following
condition: T4b staging; massive invasion of the carotid artery due to primary tumor or
lymph nodes metastasis; tumor fixation to the clavicle or involvement of the
nasopharynx.(30) In order to minimize the subjectivity of the resectability classification
(resectable or unresectable disease), tumors that would require extensive surgery were
still classified as resectable tumors, although the morbidity may create a compromised
quality of life of questionable additional value.(31)
Treatment Characteristics and Dose Modifications
Induction chemotherapy
Page 6 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

7
Chemotherapy consisted of intravenous paclitaxel (175 mg/m2) and cisplatin (80
mg/m2) on day 1 every 3 weeks for 3 cycles, unless disease progression, unacceptable
toxicity or consent withdrawal. Chemotherapy dose modification guidelines were
consistent with standard clinical practice. Cisplatin had to be replaced by carboplatin if
the patients developed peripheral neuropathy or ototoxicity of grade 2 or greater. A
cycle could be delayed for up to 2 weeks to allow the severity of grade 3 or greater toxic
events to decrease to a severity of grade 1 or lower (with the exception of alopecia).
Delays beyond 2 weeks required discontinuation of chemotherapy.
Concurrent treatment
Radiotherapy and cisplatin (100 mg/m2) were initiated at a minimum interval of
3 weeks and no later than 7 weeks after cycle 3 of IC. Cisplatin was administered
intravenously on days 1, 22 and 43. Cisplatin was reduced to 70 mg/m2 for grade 2
neurotoxicity or grade 2 myelosupression and was discontinued for grade 3
neurotoxicity. Weekly cisplatin (30 mg/m2) was accepted as a suitable option, at the
discretion of the attending physicians (before CRT or during this treatment; i.e.,
declining performance status related to toxicity). For patients unable to tolerate cisplatin
(neurotoxicity or CrCl < 50 mL/min) after IC, weekly carboplatin (AUC 1,5) was
administered. Subsequent cycles were delayed up to 2 weeks if there was evidence of
ongoing dehydration or serum creatinine levels 25% above the pretreatment value at day
22. A delay of subsequent cycles beyond day 35 necessitated withdrawal from
chemotherapy treatment. No dose re-escalations were permitted.
For patients with grades 3–4 mucositis, radiation therapy was delayed until these
reduced to less than grade 2 toxicities. Moreover, all patients received supportive care
Page 7 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

8
during radiotherapy, including dietary measures, local antiseptics and laser therapy as
preventive and curative support for oral mucositis.
Radiotherapy
Radiation treatment was delivered with 6 MV photon beams from a linear
accelerator with a standard fractionated radiotherapy of 70 Gy in 35 fractions for the
primary tumor (2 Gy/day, 5 days/week for 7 weeks). The dose administered to
uninvolved lymph nodes was at least 50 Gy and involved lymph nodes were to receive
60 to 70 Gy (2 Gy/day, 5 days/week), depending on whether an elective neck dissection
was indicated after IC. A combination of lateral-opposed portals, anterior and lateral
wedged fields or other field arrangements was used to treat the primary tumor and the
lymph nodes in the upper neck. A single anterior field was used to treat the neck below
the fields for the primary tumor. All fields were treated on each treatment day, and the
absorbed target dose of the photon fields was at least 95% and not more than 107% of
the specified centrally absorbed dose. Spinal cord sparing was performed at 46 Gy.
Gross tumor volume (GTV) was defined as the primary gross tumor or involved
node(s), and this measure was based on clinical, radiological and endoscopic
examinations at baseline (before IC). An additional margin of 1.0 cm was added to the
GTV to create the CTV. Intensity-modulated radiation therapy (IMRT) was not used.
Surgery
Patients with resectable disease and no response after IC were eligible for
salvage surgery within 4 to 6 weeks of the last scheduled dose of chemotherapy, prior to
starting CRT.
Page 8 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

9
Patients with documented persistent/residual disease after 6-8 weeks of
completing CRT were also eligible to undergo salvage surgery (for the primary tumor or
the neck).
Assessments
Clinical tumor response was determined by clinical evaluation and imaging
studies (performed at baseline, 2 weeks after the third cycle of IC and 6-8 weeks after
the end of radiotherapy). An independent review of radiologic data was performed.
Efficacy
The overall response rate (ORR) was defined as the proportion of patients whose
best overall response was either a complete response (CR) or a partial response (PR),
according to RECIST 1.1 criteria. Complete response (CR) was defined as the
disappearance of all clinically and radiological evident tumors.
Safety
Clinical and laboratory parameters were assessed to evaluate safety and toxicity.
Adverse events were assessed by National Cancer Institute - Common Terminology
Criteria for Adverse Events (NCI-CTCAE, version 3.0).
Acute radiation effects were defined as effects occurring within 90 days from the
beginning of radiotherapy. The relative dose intensity was calculated as the ratio of the
dose intensity actually delivered to the planned dose.
Follow-up and Outcomes
Page 9 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

10
Patients were monitored every 3 months during the first 2 years and every 6
months thereafter. Physical examination, radiographic disease assessment (CT/MRI
scan of head and neck and chest) and fiberoptic endoscopy of the upper digestive tract
were performed during regular monitoring or when disease progression/recurrence was
suspected or until a subject began a new anti-cancer therapy, whichever was sooner. OS
was calculated as the time of study entry to the date of death. Progression-free survival
(PFS) was calculated as the date of assignment to recurrence/progression or death
resulting from any cause. If the patient had no evidence of the aforementioned events,
survival was censored at the time of the last documented evaluation of efficacy/contact
or death resulting from another cause.
All deaths occurring during treatment or within 30 days after the completion of
treatment were considered possibly treatment-related unless tumor progression was
previously documented.
Human Papillomavirus Testing
p16 immunohistochemistry (IHC) was performed on formalin-fixed paraffin
embedded (FFPE) tissue sections cut at 4 mm thick using the CINtec® p16INK4A
assay, according to the manufacturer’s instructions (CINtec® Histology Kit, Ventana
Medical Systems, Inc., Tucson, Arizona, USA). Positive cases were considered for
staining in ≥ 75% of tumor cells.
Statistic Considerations
The primary endpoints were tolerability and safety of chemoradiotherapy based
on cisplatin following IC with TP regimen. Secondary endpoints were ORR, PFS and
overall survival rates.
Page 10 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

11
The following assumptions were made for this phase II sample size. In the
RTOG 91-11 study, the authors reported that 93% of patients randomized to concurrent
therapy based on cisplatin and radiotherapy received at least 2 cycles of chemotherapy
(70% received all 3 planned cycles of cisplatin, and 23% received 2 cycles) (32). Then,
54 patients were required to accept the hypothesis that at least 83% of the patients
submitted to 3 cycles of TP induction chemotherapy would be able to complete the
concurrent planned treatment (at least 2 cycles of bolus cisplatin or 5 courses of weekly
cisplatin or carboplatin and all radiotherapy planned), with a power of 80% (β = 0.20)
and a one-sided significance level of α = 0.05. The estimated rate of early dropout or
loss at follow-up was 10%. Therefore, this study was designed to enroll 20 qualified
patients in each group, defined as having resectable oropharynx tumors; resectable
hypopharynx or larynx tumors; and unresectable disease (total of 60 patients).
Descriptive statistics, including the mean, standard deviation, median, range and
percentage, were used to describe patient demographic and clinical characteristics. Chi-
square or Fisher’s exact tests were used to test differences in categoric variables, and
the Wilcoxon rank sum test or Kruskal-Wallis tests were used to detect differences in
continuous variables. The exact binominal test was used to test the significance of the
observed CR rate. Survival analysis was conducted using the Kaplan-Meier method and
log-rank test. Hazard ratio (HR) was calculated using the Cox proportional hazards
model. All multivariate model were tested including all covariates with p-value <0.20 in
the univariate analysis.
A two-sided level of significance of 0.05 was applied to all tests. Analyses were
performed by using the IBM SPSS statistical software package version 19.0 (SPSS,
Chicago, IL).
Page 11 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

12
RESULTS
Patients
From July 31, 2009, to Nov 12, 2010, a total of 64 patients were enrolled in the
study. Four patients failed the screening (2 due to elevated serum creatinine and 2 due to
systemic metastases diagnosed during the screening period). A CONSORT diagram of
the patient composition is shown in Figure 1 and the baseline demographic and clinical
characteristics of the patients are summarized in Table 1.
Treatment Characteristics
Tolerability
The study met its primary objective [56 patients (93.3%) received all three-
cycles of IC and 52 patients (86.7%) completed at least 2 cycles of concurrent bolus
cisplatin or 5 courses of weekly cisplatin or carboplatin and the planned dose of
radiotherapy], demonstrating that a majority of patients received the full course of
induction and concurrent treatment planned per the protocol (i.e., the number of
chemotherapy cycles and dose intensity) (Table 2).
Seven patients (11.6%) discontinued the planned treatment. The reasons for
discontinuation were as follows: disease progression in 3 patients (1 during induction
chemotherapy; 2 during CRT), 2 AEs related to treatment (1 death), withdrawal of
consent by 1 patient, and noncompliance with the study protocol by 1 patient.
Safety
Table 3 displays the most frequent AEs by NCI-CTCAE version 3.0 grade 2-5
during IC and CRT.
Adverse events related to induction chemotherapy
Page 12 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

13
During this phase, all patients presented alopecia, 75.0% of which were grade 2.
The other most common non-hematological toxicities were fatigue and
nausea/vomiting. Grade 2 fatigue occurred in 13 patients (21.7%); 1 patient presented
grade 3 fatigue. Thirteen patients (21.7%) reported grade 2 nausea/vomiting, and 2
patients had grade 3 nausea/vomiting. Grade 2 peripheral neuropathy occurred in only 1
patient.
The most common grade 2 or higher hematological toxicity was neutropenia
(grade 2 in 6.7%, grade 3 in 1.7% and grade 4 in 1.7% of patients).
Treatment delays of more than 7 days occurred in 4 patients (6.7%), and only 1
patient (1.7%) required discontinuation of treatment due a serious AE (left femoral
acute arterial occlusion that was properly treated by vascular surgical intervention and
evolved with no sequelae).
Only 7 patients (11.7%) had AEs of grade 3 or higher during IC. No deaths were
reported during IC.
Adverse events related to CRT
The most common non-hematological toxicities were xerostomia, anorexia,
nausea/vomiting, radiodermatitis, stomatitis/mucositis, dysgeusia, fatigue and peripheral
neuropathy.
The most common grade 2 or higher hematological toxicity was neutropenia
(grade 2, 3, or 4 in 14.0%, 14.0% and 3.5% of patients, respectively), and only 1 patient
had febrile neutropenia during CRT.
Thirty-two patients (56.1%) displayed some grade 3 or 4 AEs, and 1 death was
deemed to be treatment-related.
Page 13 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

14
Efficacy
Table 4 displays the response assessment rates by RECIST 1.1 criteria after IC
and CRT considering resectability status.
Among the 40 patients classified as having potentially resectable disease, the
ORR was 82.5% after IC and 28 patients (70.0%) achieved CR after CRT. Of the 23
patients who presented a PR by RECIST 1.1 criteria after IC, 17 (73.9%) achieved CR
after CRT in the potentially resectable disease group.
Among the 20 patients classified as having unresectable disease, the ORR was
55.0% after IC and 6 (30.0%) achieved CR. Of the 10 patients with a PR after
induction, 4 patients (40.0%) achieved CR after CRT in the unresectable disease group.
Predictive Factors for Favorable Response to IC
Univariate analysis were performed and the covariates significantly associated
with presence of complete or partial response were: age (p = 0.038), T stage (p = 0.037),
resectability status (p = 0.023) and level of serum calcium (p = 0.038). All other
variables related to the patient (gender, performance status and smoking status), tumor
(primary site, tumor grading, N stage and HPV status) and treatment (cycles of
chemotherapy, cisplatin vs carboplatin) were not significant predictors of response to IC
(p > 0.05 in each case; data not shown).
In the multivariate analysis the only independent variable able to predict the
response after IC was the resectability status (OR 3.86; 95% CI, 1.17-12.81; p = 0.028).
Thus the risk to achieve a complete or partial response is 3.86-fold higher for a patient
with resectable disease than for a patient with unresectable disease.
Predictive Factors for Favorable Response to CRT
Page 14 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

15
Univariate analysis were performed and the covariates associated significantly
with presence of complete response were: response after IC (p < 0.001), resectability
status (p = 0.005), T stage (p = 0.005) and N stage (p = 0.021). Treatment intensity
(complete vs incomplete; p = 0.146) and gender (p = 0.139) were also tested in the
multivariate analysis. All other covariates were not significant predictors of response to
IC (p > 0.05 in each case; data not shown).
In the multivariate analysis the independent variable able to predict the complete
response after CRT were the presence of response (CR or PR) after IC (OR 111.70;
95% CI, 6.72-1,857.28; p = 0.001), T stage [T1-T3 versus T4; (OR 5.44; 95% CI, 1.06-
27.84; p = 0.042)] and N stage [N0-1versus N2-3; (OR 9.37; 95% CI, 1.01-86.58; p =
0.049)].
Salvage Surgery
Salvage neck dissections were performed before CRT in 3 patients due a poor
response rate in the neck. After CRT, 8 patients (6 in the resectable group and 2 in the
unresectable group) underwent salvage surgery due to residual disease (3 neck
dissections, 2 primary site resections, and 3 both neck and primary site salvage surgery).
Progression-Free Survival and Overall Survival
After a median follow-up of 30 months, 33 patients died (27 deaths related to
disease progression, 1 death due to toxicity, 3 deaths due to comorbidities, 1 death after
salvage surgery due to residual head and neck carcinoma and 1 death after surgery for a
second primary tumor). Five patients remain alive with disease and 22 patients are alive
with no evidence of disease (19 cases in the resectable group and 3 cases in the
unresectable group; p < 0.001).
Page 15 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

16
The median PFS was 23.0 months for patients with resectable disease and 8.0
months for patients with unresectable disease [resectable versus unresectable disease;
(HR 2.81; 95% CI, 1.48-5.33; p = 0.002)]. The median OS was 13.0 months for
unresectable disease and it was not reached for patients with resectable disease (HR
3.80; 95% CI, 1.89-7.64; p < 0.001)]. (Figure 2 and Table 5).
Others Secondary Endpoints
Table 5 displays the pattern of first relapse, some functional outcomes (feeding
tube dependence, pneumonia and tracheostomy events), risk and causes of early deaths
according to their resectability status.
The pattern of first failure was as follows: early disease progression (< 6 months
after study enrollment), n = 12 (4 and 8 patients had resectable and unresectable disease,
respectively; p < 0.001); persistent locoregional disease after CRT, n =11; locoregional
recurrence, n = 15; locoregional and distant metastases, n = 2; and second primary
tumor, n = 8. Among the 17 patients who relapsed, 4 (23.5%) underwent salvage
surgery.
DISCUSSION
This phase II non-randomized trial was designed to establish a tolerable and safe
outpatient regimen using cisplatin and paclitaxel for IC followed by concurrent CRT
based on cisplatin for LAHNSCC patients of low socioeconomic status and high tumor
burden.
The combination of platinum and taxane is the backbone of several IC regimens
for LAHNSCC (8, 10, 33). As a safer and more tolerable induction regimen, some
authors maintain that cisplatin and docetaxel, with a range of options for the third drug.
5FU has been replaced by capecitabine (29), ifosfamide (24, 26), cetuximab (23) and
Page 16 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

17
gemcitabine (34). Other authors have replaced docetaxel with paclitaxel (24, 25, 27, 28)
or split the docetaxel dose (biweekly docetaxel) (35) to reduce hematological toxicity,
while others omit the third agent (36).
By contrast, the TPF regimen affects the administration of definitive
locoregional treatment in the majority of patients with LAHNSCC.(22, 37) The
TREMPLIN trial showed that only 45% of patients receiving 3 cycles of induction TPF
chemotherapy completed concomitant chemoradiotherapy.(15) We strongly believe that
the better tolerance profile reported in our study is due to omission of the 5-Fluorouracil
agent during IC need to be better evaluated in further study.
Prestwich et al.(38) reported treating selected patients with LAHNSCC with 3
cycles of induction TPF followed by concurrent three-weekly bolus cisplatin (100
mg/m2) chemoradiotherapy. Between March 2006 and February 2010, only 66 patients
with non-metastatic stage IV head-and-neck squamous cell carcinoma were included.
During TPF, grade 3 toxicity occurred in 18 patients (27%) and unplanned admissions
in 6 (9%). Sixty-two patients (94%) received radical radiotherapy, but only 3 patients
(5%) received the planned concurrent cisplatin therapy (29% and 61% of patients
received 1 and 2 cycles of cisplatin, respectively).(38)
The superior survival observed in the North American TPF compared to the
European TPF arms may be due to the inclusion of resectable patients with better
prognosis, a consequence of the more intensive TPF regimen or a result of the addition
of CRT as part of the treatment plan. It is possible that all three of these factors
contributed to the end result to some extent.(10)
Although IC has a proven role in organ preservation and might reduces the
incidence of distant metastases, its efficacy in prolonging overall survival has not been
Page 17 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

18
demonstrated,(16, 39) and the role of IC prior to concurrent chemoradiotherapy remains
controversial.(17, 33, 40-42)
The DeCIDE and PARADIGM trials sought to address whether the addition of
IC to definitive chemoradiotherapy improved survival. Unfortunately, in both trials,
patients in the induction arms were treated with chemoradiotherapy regimens that are
not generally considered the standard of care, and a large number of biologically distinct
HPV-positive patients were included. Both studies terminated early due to poor accrual,
failing to meet their primary endpoint.(17, 18, 33, 39-42)
The TP regimen used in this study proved to be safe and tolerable with low
toxicity during the induction phase, permitting CRT based on cisplatin in the majority
of patients included. The efficacy of the TP regimen was also promising in these
predominantly HPV-negative patients (ORR after IC with TP regimen was 82.5% for
patients with resectable disease and 55.5% for unresectable disease) that are comparable
to previous reports regarding intensive IC as a TPF regimen (TPF regimen showed ORR
of 68% in TAX 323 trial and ORR of 72% in TAX 324 trial) (6, 12)
In this study, encouraging functional outcomes were observed compared to the
existing literature considering the conventional standard fractionated radiotherapy used
(2 Gy per day; 5 days per week), which claim feeding tube dependence rates of 15% to
30%.(43-45) Likewise, the pneumonia rates within two years after study inclusion were
12.5% and 5.0% in resectable and unresectable disease, respectively. However,
attention has recently focused on new technology in radiation oncology (such as IMRT).
Target delineation has become more complex to selectively decrease radiation dose to
specified anatomic structures responsible for a functional swallow. Recent reports have
proposed a variety of dose thresholds or constraints to these swallowing-related
Page 18 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

19
structures, which may guide IMRT planning with the aim of reducing dysphagia and
consequently decrease the feeding tube dependence.(46)
The most common pattern of relapse in the present study was locoregional
failure, which is comparable to the finding that patients treated with induction regimens
display a lower rate of systemic recurrence (8, 47). Early disease progression (< 6
months after study enrollment) was diagnosed in 12 patients (4 and 8 patients had
resectable and unresectable disease, respectively; p < 0.001), locoregional recurrence
was noticed in 15 patients and only two patients had both locoregional and distant
metastases. All these locorregional recurrence happened in-field of previous
radiotherapy. There is limited published literature regarding patterns of disease
recurrence after conventional radiotherapy for HNSCC. This has been best documented
in several IMRT series.(48) As the success of radiotherapy depends on the accurate
delineation of the clinical target volume, it is important to document the patterns of
disease recurrence in order to continued efforts to improve therapy to enhance
locorregional control.(49)
Another important observation in this study was the difference in response rate
between groups of patients according to resectability status. Several studies have made
no distinction between resectable and unresectable disease, and the definitions of
resectable and unresectable disease vary among practitioners due to the lack of well-
established criteria to uniformly classify the status of resectability in LAHNSCC (30).
Our study used undoubted technical unresectability condition to classify the disease as
unresectable.(30, 31) In clinical practice, the definition of resectability allows clinicians
to plan different strategies for patients with LAHNSCC. Thereby, the resectability status
was used in this phase 2 trial to allow different strategies during the treatment, including
salvage surgery for resectable tumor that failure to IC. However, a large fraction of
Page 19 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

20
resectable tumors can be treated non-surgically (CRT with or without IC) in an effort to
preserve organ anatomy and function and some patients with unresectable disease might
become candidates for salvage surgery.(50)
The stage TNM and HPV status is actually the most accepted important
prognostic factor in patients with squamous cell cancer in the head and neck region.(51)
Even though some authors had showed that response to IC predicts response to
CRT(21), as regards predictive factors of response to induction chemotherapy in
patients with HPV negative LAHNSCC, no factor is currently validated. Surprisingly,
this study showed that the resectability status was an independent variable able to
predict the response after IC, and the presence of response to IC, T stage and N stage
were statistically significant predictive factor of response to CRT. The resectability
status as predict for response to IC may be partly explained by reason to exist some
degree of overlap between resectability status and TNM stage as these two covariates to
evaluate the extent of disease. Although it has been published that hypercalcemia in
head and neck malignancy determine poor median of overall survival(52), this is the
first time that the presence of high value of level of serum calcium at baseline was
correlated with significant lower chance to response to IC (p = 0.038) in univariate
analysis (data not confirmed in multivariate analysis). Future advances are expected in
order to identify prognostic and predictive biomarkers for efficacy and toxicity.(53, 54)
This small, single institutional non-randomized trial has its limitations. First, the
higher proportion of patients with oropharyngeal cancer may have affected the response,
although only two patients were never smokers and only two patients were p16 positive.
The low number of patients with p16 overexpression in this study impaired our analysis
exploring the effect of HPV on prognosis and/or as a predictive factor. In addition,
chronic toxicity was not evaluated because the aim of this study was to determine the
Page 20 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

21
tolerability and efficacy of a TP regimen followed by concurrent therapy. Some patients
received carboplatin during CRT, which is not as effective as cisplatin as a direct
antitumor agent (55, 56).
Moreover, the safety and tolerability observed during IC and CRT in this study
may be explained by patient selection, improved control of emesis, and greater
awareness of hydration and hydration protocols as supportive care during radiotherapy,
including dietary measures, local antiseptics and laser therapy for oral mucositis.
Currently, the standard of care for most patients is a multidisciplinary approach
with concomitant chemotherapy plus radiotherapy,(32, 39, 57-59) but the addition of IC
remains an appropriate approach for advanced disease with a high risk of local or distant
failure.(7)
In summary, a TP regimen (cisplatin plus paclitaxel) followed by CRT based on
cisplatin is safe, well tolerated and had high ORR in patients with LAHNSCC (stage III
and IV M0).
Conflict of Interest Statement: We declare that we have no conflict of interest
Acknowledgements: This study was funded by Barretos Cancer Hospital
Page 21 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

22
REFERENCES
1. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer
statistics. CA Cancer J Clin. 2011 Mar-Apr;61(2):69-90.
2. Denaro N, Russi EG, Adamo V, Merlano MC. State-of-the-art and emerging
treatment options in the management of head and neck cancer: news from 2013.
Oncology. 2014;86(4):212-29.
3. Haddad R, Tishler RB, Norris CM, et al. Docetaxel, cisplatin, 5-fluorouracil
(TPF)-based induction chemotherapy for head and neck cancer and the case for
sequential, combined-modality treatment. Oncologist. 2003;8(1):35-44.
4. Pointreau Y, Atean I, Calais G. How does TPF improve survival over PF?
Lancet Oncol. 2011 May;12(5):420-1; author reply 1-2.
5. Pointreau Y, Atean I, Fayette J, Calais G, Lefebvre JL. Induction chemotherapy
in head and neck cancer: a new paradigm. Anticancer Drugs. 2011 Aug;22(7):613-20.
6. Vermorken JB, Remenar E, van Herpen C, et al. Cisplatin, fluorouracil, and
docetaxel in unresectable head and neck cancer. N Engl J Med. 2007 Oct
25;357(17):1695-704.
7. Cruz JJ, Ocana A, Navarro M, Barco ED, Fonseca E. New options in the
treatment of locally advanced head and neck cancer: role for induction chemotherapy.
Cancer Treat Rev. 2008 May;34(3):268-74.
8. Hanna GJ, Haddad RI, Lorch JH. Induction chemotherapy for locoregionally
advanced head and neck cancer: past, present, future? Oncologist. 2013;18(3):288-93.
9. Pignon JP, Bourhis J, Domenge C, Designe L. Chemotherapy added to
locoregional treatment for head and neck squamous-cell carcinoma: three meta-analyses
of updated individual data. MACH-NC Collaborative Group. Meta-Analysis of
Chemotherapy on Head and Neck Cancer. Lancet. 2000 Mar 18;355(9208):949-55.
Page 22 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

23
10. Posner M, Vermorken JB. Induction therapy in the modern era of combined-
modality therapy for locally advanced head and neck cancer. Semin Oncol. 2008
Jun;35(3):221-8.
11. Levy A, Blanchard P, Bellefqih S, et al. Feasibility of radiotherapy or
chemoradiotherapy after taxane-based induction chemotherapy for nonoperated locally
advanced head and neck squamous cell carcinomas. Anticancer Drugs. 2014
Nov;25(10):1220-6.
12. Posner MR, Hershock DM, Blajman CR, et al. Cisplatin and fluorouracil alone
or with docetaxel in head and neck cancer. N Engl J Med. 2007 Oct 25;357(17):1705-
15.
13. Billan S, Kaidar-Person O, Atrash F, et al. Toxicity of induction chemotherapy
with docetaxel, cisplatin and 5-fluorouracil for advanced head and neck cancer. Isr Med
Assoc J. 2013 May;15(5):231-5.
14. Hitt R, Grau JJ, Lopez-Pousa A, et al. A randomized phase III trial comparing
induction chemotherapy followed by chemoradiotherapy versus chemoradiotherapy
alone as treatment of unresectable head and neck cancer. Ann Oncol. 2014
Jan;25(1):216-25.
15. Cohen EE, Karrison TG, Kocherginsky M, et al. Phase III randomized trial of
induction chemotherapy in patients with N2 or N3 locally advanced head and neck
cancer. J Clin Oncol. 2014 Sep 1;32(25):2735-43.
16. Haddad R, O'Neill A, Rabinowits G, et al. Induction chemotherapy followed by
concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent
chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): a
randomised phase 3 trial. Lancet Oncol. 2013 Mar;14(3):257-64.
Page 23 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

24
17. Loo SW, Geropantas K, Roques TW. DeCIDE and PARADIGM: nails in the
coffin of induction chemotherapy in head and neck squamous cell carcinoma? Clin
Transl Oncol. 2013 Mar;15(3):248-51.
18. Lefebvre JL, Pointreau Y, Rolland F, et al. Induction chemotherapy followed by
either chemoradiotherapy or bioradiotherapy for larynx preservation: the TREMPLIN
randomized phase II study. J Clin Oncol. 2013 Mar 1;31(7):853-9.
19. Sanders IW, Haslett K, Correa P, et al. Sequential TPF chemotherapy followed
by concurrent chemoradiotherapy in locally advanced head and neck cancer--a
retrospective analysis of toxicity and outcomes. Scott Med J. 2014 Feb;59(1):50-5.
20. Caudell JJ, Hamilton RD, Otto KJ, Jennelle RL, Pitman KT, Vijayakumar S.
Induction docetaxel, Cisplatin, and 5-Fluorouracil precludes definitive
chemoradiotherapy in a substantial proportion of patients with head and neck cancer in
a low socioeconomic status population. Am J Clin Oncol. 2014 Aug;37(4):332-6.
21. Lefebvre JL, Ang KK. Larynx preservation clinical trial design: key issues and
recommendations--a consensus panel summary. Head Neck. 2009 Apr;31(4):429-41.
22. Adelstein DJ, Moon J, Hanna E, et al. Docetaxel, cisplatin, and fluorouracil
induction chemotherapy followed by accelerated fractionation/concomitant boost
radiation and concurrent cisplatin in patients with advanced squamous cell head and
neck cancer: A Southwest Oncology Group phase II trial (S0216). Head Neck. 2010
Feb;32(2):221-8.
23. Bauman J, Langer C, Quon H, et al. Induction chemotherapy with cetuximab,
carboplatin and paclitaxel for the treatment of locally advanced squamous cell
carcinoma of the head and neck. Exp Ther Med. 2013 Apr;5(4):1247-53.
24. Chitapanarux I, Tharavichitkul E, Lorvidhaya V, Sittitrai P, Pattarasakulchai T.
Induction chemotherapy with paclitaxel, ifosfamide, and cisplatin followed by
Page 24 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

25
concurrent chemoradiotherapy for unresectable locally advanced head and neck cancer.
Biomed Imaging Interv J. 2010 Jul-Sep;6(3):e23.
25. Dietz A, Rudat V, Dreyhaupt J, et al. Induction chemotherapy with paclitaxel
and cisplatin followed by radiotherapy for larynx organ preservation in advanced
laryngeal and hypopharyngeal cancer offers moderate late toxicity outcome (DeLOS-I-
trial). Eur Arch Otorhinolaryngol. 2009 Aug;266(8):1291-300.
26. Hancock SB, Krempl GA, Canfield V, et al. Treatment of base of tongue cancer
with paclitaxel, ifosfamide, and cisplatinum induction chemotherapy followed by
chemoradiotherapy. Laryngoscope. 2008 Aug;118(8):1357-61.
27. Herman LC, Chen L, Garnett A, et al. Comparison of carboplatin-paclitaxel to
docetaxel-cisplatin-5-flurouracil induction chemotherapy followed by concurrent
chemoradiation for locally advanced head and neck cancer. Oral Oncol. 2014
Jan;50(1):52-8.
28. Hitt R, Lopez-Pousa A, Martinez-Trufero J, et al. Phase III study comparing
cisplatin plus fluorouracil to paclitaxel, cisplatin, and fluorouracil induction
chemotherapy followed by chemoradiotherapy in locally advanced head and neck
cancer. J Clin Oncol. 2005 Dec 1;23(34):8636-45.
29. Perri F, Muto P, Argenone A, et al. Induction chemotherapy with docetaxel,
cisplatin and capecitabine, followed by combined cetuximab and radiotherapy in
patients with locally advanced inoperable squamous cell carcinoma of the head and
neck: a phase I-II study. Oncology. 2013;84(4):251-4.
30. Fu KK, Phillips TL, Silverberg IJ, et al. Combined radiotherapy and
chemotherapy with bleomycin and methotrexate for advanced inoperable head and neck
cancer: update of a Northern California Oncology Group randomized trial. J Clin Oncol.
1987 Sep;5(9):1410-8.
Page 25 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

26
31. Yousem DM, Gad K, Tufano RP. Resectability issues with head and neck
cancer. AJNR Am J Neuroradiol. 2006 Nov-Dec;27(10):2024-36.
32. Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and
radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003
Nov 27;349(22):2091-8.
33. Paccagnella A, Ghi MG, Loreggian L, et al. Concomitant chemoradiotherapy
versus induction docetaxel, cisplatin and 5 fluorouracil (TPF) followed by concomitant
chemoradiotherapy in locally advanced head and neck cancer: a phase II randomized
study. Ann Oncol. 2010 Jul;21(7):1515-22.
34. El Deen DA, Toson EA, El Morsy SM. Gemcitabine-based induction
chemotherapy and concurrent with radiation in advanced head and neck cancer. Med
Oncol. 2012 Dec;29(5):3367-73.
35. Bae WK, Hwang JE, Shim HJ, et al. Multicenter phase II study of weekly
docetaxel, cisplatin, and S-1 (TPS) induction chemotherapy for locally advanced
squamous cell cancer of the head and neck. BMC Cancer. 2013;13:102.
36. Kies MS, Holsinger FC, Lee JJ, et al. Induction chemotherapy and cetuximab for
locally advanced squamous cell carcinoma of the head and neck: results from a phase II
prospective trial. J Clin Oncol. 2010 Jan 1;28(1):8-14.
37. Strojan P, Grasic Kuhar C, Zumer B, et al. TPF induction chemotherapy and
concomitant irradiation with cisplatin and cetuximab in unresectable squamous cell
carcinoma of the head and neck. Head Neck. 2014 Nov;36(11):1555-61.
38. Prestwich RJ, Oksuz DC, Dyker K, Coyle C, Sen M. Feasibility and efficacy of
induction docetaxel, cisplatin, and 5-fluorouracil chemotherapy combined with cisplatin
concurrent chemoradiotherapy for nonmetastatic Stage IV head-and-neck squamous cell
carcinomas. Int J Radiat Oncol Biol Phys. 2011 Nov 15;81(4):e237-43.
Page 26 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

27
39. Dieumegard B, Grandjouan S, Sabourin JC, et al. Extensive molecular screening
for hereditary non-polyposis colorectal cancer. Br J Cancer. 2000 Feb;82(4):871-80.
40. Rapidis AD, Trichas M, Stavrinidis E, et al. Induction chemotherapy followed
by concurrent chemoradiation in advanced squamous cell carcinoma of the head and
neck: final results from a phase II study with docetaxel, cisplatin and 5-fluorouracil with
a four-year follow-up. Oral Oncol. 2006 Aug;42(7):675-84.
41. Urba SG, Moon J, Giri PG, et al. Organ preservation for advanced resectable
cancer of the base of tongue and hypopharynx: a Southwest Oncology Group Trial. J
Clin Oncol. 2005 Jan 1;23(1):88-95.
42. Fabregas JC, Loaiza-Bonilla A, Talebi TN, et al. Concurrent chemoradiotherapy
versus induction chemotherapy followed by chemoradiotherapy (sequential approach) in
the management of head and neck cancer. Expert Rev Anticancer Ther. 2013
Sep;13(9):1065-72.
43. Ackerstaff AH, Balm AJ, Rasch CR, et al. First-year quality of life assessment
of an intra-arterial (RADPLAT) versus intravenous chemoradiation phase III trial. Head
Neck. 2009 Jan;31(1):77-84.
44. Shiley SG, Hargunani CA, Skoner JM, Holland JM, Wax MK. Swallowing
function after chemoradiation for advanced stage oropharyngeal cancer. Otolaryngol
Head Neck Surg. 2006 Mar;134(3):455-9.
45. Langerman A, Maccracken E, Kasza K, Haraf DJ, Vokes EE, Stenson KM.
Aspiration in chemoradiated patients with head and neck cancer. Arch Otolaryngol
Head Neck Surg. 2007 Dec;133(12):1289-95.
46. Batth SS, Caudell JJ, Chen AM. Practical considerations in reducing swallowing
dysfunction following concurrent chemoradiotherapy with intensity-modulated
radiotherapy for head and neck cancer. Head Neck. 2014 Feb;36(2):291-8.
Page 27 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

28
47. Ma J, Liu Y, Yang X, Zhang CP, Zhang ZY, Zhong LP. Induction chemotherapy
in patients with resectable head and neck squamous cell carcinoma: a meta-analysis.
World J Surg Oncol. 2013;11:67.
48. Oksuz DC, Prestwich RJ, Carey B, et al. Recurrence patterns of locally
advanced head and neck squamous cell carcinoma after 3D conformal (chemo)-
radiotherapy. Radiat Oncol. 2011;6:54.
49. Vorwerk H, Hess CF. Guidelines for delineation of lymphatic clinical target
volumes for high conformal radiotherapy: head and neck region. Radiat Oncol.
2011;6:97.
50. Denaro N, Russi EG, Merlano MC. Strategies for non-resectable head and neck
cancer. Curr Treat Options Oncol. 2013 Dec;14(4):492-504.
51. O'Sullivan B, Huang SH, Siu LL, et al. Deintensification candidate subgroups in
human papillomavirus-related oropharyngeal cancer according to minimal risk of
distant metastasis. J Clin Oncol. 2013 Feb 10;31(5):543-50.
52. Bradley PJ, Hoskin D. Hyercalcaemia in head and neck squamous cell
carcinoma. Curr Opin Otolaryngol Head Neck Surg. 2006 Apr;14(2):51-4.
53. Laban S, Wang CJ, Munscher A, Tribius S, Schafhausen P, Knecht R. Molecular
targeting agents in the context of primary chemoradiation strategies. Head Neck. 2013
May;35(5):738-46.
54. Yokota T. Is biomarker research advancing in the era of personalized medicine
for head and neck cancer? Int J Clin Oncol. 2014 Apr;19(2):211-9.
55. Douple EB, Richmond RC, O'Hara JA, Coughlin CT. Carboplatin as a
potentiator of radiation therapy. Cancer Treat Rev. 1985 Sep;12 Suppl A:111-24.
56. Yang LX, Douple E, Wang HJ. Irradiation-enhanced binding of carboplatin to
DNA. Int J Radiat Biol. 1995 Dec;68(6):609-14.
Page 28 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

29
57. Lefebvre JL, Andry G, Chevalier D, et al. Laryngeal preservation with induction
chemotherapy for hypopharyngeal squamous cell carcinoma: 10-year results of EORTC
trial 24891. Ann Oncol. 2012 Oct;23(10):2708-14.
58. Lefebvre JL. Larynx preservation. Curr Opin Oncol. 2012 May;24(3):218-22.
59. Lefebvre JL. Laryngeal preservation in head and neck cancer: multidisciplinary
approach. Lancet Oncol. 2006 Sep;7(9):747-55.
Page 29 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

1
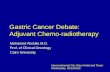
Figure 1
Assessed for elegibility
(n = 64)
Excluded (n = 4)
Did not meet
inclusion criteria
Included (n = 60)
Locally advanced head and neck carcinoma
• resectable oropharynx (n = 20)
• resectable hypopharynx/larynx (n = 20)
• unresectable disease (n = 20)
Resectable disease Unresectable disease
Induction chemotherapy (IC)
Surgical salvage if applicable
Induction chemotherapy
To anticipate CRT if applicable
Chemoradiotherapy (CRT)
Salvage surgery in case of resectable residual disease
Induction phase: n = 60 Concomitant phase: n = 57 Excluded from CRT: n = 3 (1 consent withdrawal; 1 noncompliance; 1 progression of disease and declining performance status for CRT)
En
rollm
en
t A
llo
cati
on
T
reatm
en
t A
naly
sis
Follow-up
Page 30 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

1
Figure 2
Page 31 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

1
Table 1. Characteristics of the 60 patients included in the study.
Variable No. of
patients %
Median Age (years) 56 (37-76)
Gender M 56 93.3
F 4 6.7
ECOG-PS 0 2 3.4
1 53 88.3
2 5 8.3
Primary site Oral Cavity 3 5.0
Oropharynx 32 53.3
Hypopharynx 8 13.3
Larynx 17 28.4
Tracheostomy Yes (baseline) 2 3.3
Tumor grade G1 9 15.0
G2 41 68.3
G3 9 15.0
T classification T2 4 6.7
T3 35 58.3
T4 21 35.0
N classification N0 13 21.7
N1 8 13.3
N2 30 50.0
N3 9 15.0
Stage III 18 30.0
IV 42 70.0
Resectability status* Resectable 40 66.6
Unresectable disease 20 33.3
Smoking status Current 43 71.7
Former 15 25.0
Never 2 3.3
HPV status** Positive (p16+) 2*** 3.33
Negative 50 83.33
Unevaluable 8 13.34
* Twenty patients with oropharynx tumors, 20 patients with non-oropharynx tumors and 20 patients with
unresectable tumors (2 patient had synchronous head and neck carcinoma).
** HPV status was determined retrospectively using archival tumor specimens.
*** Both patients presented oropharynx tumors, were current heavy smokers, male and stage IV.
Page 32 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

Table 2. Treatment administered during induction phase and concurrent treatment.
Parameter Induction Phase (n = 60) Combined Phase (n = 57)
Cisplatin
Median cumulative dose (mg/m2) 233.72 229.97
Median relative dose intensity % 97.38 76.65
Paclitaxel
Median cumulative dose (mg/m2) 520.23 NA
Median relative dose intensity % 99.09 NA
Carboplatin instead of cisplatin 4 (6.7%) 8 (14.0%)
Patients with ≥ 1 dose held for ≥ 7 days 4 (6.7%) 17 (29.8%)
Patients with dose reductions 4 (6.7%) 27 (47.4%)
Cycles of chemotherapy (every 3 weeks)
0 cycles 0 1 (1.8%)
1 cycles 1 (1.7%)† 2 (3.5%)
2 cycles 3 (5.0%)† 17 (29.8%)
††
3 cycles 56 (93.3%) 29 (50.9%)
Weekly session of chemotherapy
≥ 5 weeks sessions of carboplatin NA 7 (12.2%)
< 5 weeks sessions of carboplatin NA 1 (1.8%)
Weekly cisplatin NA 0 (0%)
Completed platin-dose during CRT 53 (92.9%)
Radiotherapy
Total dose ≥ 66 Gy NA 54 (94.7%)
RT major deviation NA 10* (17.5%)
Completed planned IC followed by CRT 52 (86.7%)
Legend. RT, radiotherapy; NA, Not applicable; IC, induction chemotherapy; CRT, concurrent
chemoradiotherapy
*Treatment interruption > 10 days in 8 patients (14.0%). †
Four patients received less than 3 cycles of IC [1 due to toxicity, 1 due to disease progression (unresectable
disease) and 2 due to incorrect anticipation of concurrent chemoradiotherapy] that was not specified in the
protocol. ††
Two patients received 100mg/m2 of cisplatin at the first cycle and further three sessions of weekly cisplatin
(30mg/m2).
Page 33 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

Table 3. Most common AE/SAEs associated with the treatment (NCI-CTCAE v.3.0).
AE TP Induction Chemotherapy (n = 60) Chemoradiotherapy (n = 57)
Grade 2 Grade 3 Grade 4 Grade 5 Grade 2 Grade 3 Grade 4 Grade 5
No. of patients (%) by grade of toxicity No. of patients (%) by grade of toxicity
Hematological
Anemia 7 (11.7) 1 (1.7) 0 0 20 (35.0) 1 (1.7) 0 0
Lymphopenia 0 0 1 (1.7) 0 8 (14.0) 6 (10.5) 0 0
Thrombocytopenia 0 0 0 0 1 (1.7) 1 (1.7) 0 0
Neutropenia 4 (6.7) 1 (1.7) 1 (1.7) 0 8 (14.0) 8 (14.0) 2 (3.5) 0
Febrile neutropenia 0 0 1 (1.7) 0 0 0 1 (1.7) 0
Non-Hematological
Alopecia 45 (75.0) 0 0 0 40 (70.1) - - 0
Nausea/vomiting 13 (21.7) 2 (3.3) 0 0 23 (40.3) 4 (7.0) 0 0
Diarrhea 3 (5.0) 0 0 0 3 (5.2) 0 0 0
Anorexia 5 (8.4) 0 0 0 25 (43.8) 2 (3.5) 0 0
Dysgeusia 0 0 0 0 17 (29.8) 0 0 0
Fatigue 13 (21.7) 1 (1.7) 0 0 13 (22.8) 8 (14.0) 0 0
Myalgia 7 (11.7) 0 0 0 0 0 0 0
Peripheral neuropathy 1 (1.7) 0 0 0 4 (7.0) 0 0 0
Stomatitis/Mucositis 0 0 0 0 15 (26.3) 10
(17.5) 1 (1.7) 0
Xerostomia 0 0 0 0 29 (50.8) 0 0 0
Radiodermatitis - - - - 18 (31.5) 0 0 0
Infection 1 (1.7) 0 1 (1.7) 0 0 0 0 0
Acute arterial occlusion 0 0 1 (1.7) 0 0 0 0 0
Increased serum
creatinine 1 (1.7) 0 0 0 1 (1.7) 1 (1.7) 0 0
Sudden death - - - 0 - - - 1 (1.7)
Legend: AE, adverse event; TP, paclitaxel and cisplatin chemotherapy
Page 34 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

Table 4. Response assessment rates by RECIST 1.1 criteria after induction
chemotherapy (IC) and concurrent chemoradiotherapy (CRT) considering resectability
status (n = 60).
Response assessment (RECIST 1.1)
After IC
No. of patients (%)
After CRT
No. of patients (%)
CR PR SD PD
Not
evaluable*
Resectable
disease
(n = 40)
CR 10 (25.0) 10 (25.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
PR 23 (57.5) 17 (42.5) 3 (7.5) 0 (0.0) 2 (5.0) 1 (2.5)
SD 4 (10.0) 1 (2.5) 2 (5.0) 1 (2.5) 0 (0.0) 0 (0.0)
PD 3 (7.5) 0 (0.0) 1 (2.5) 0 (0.0) 2 (5.0) 0 (0.0)
Unresectable
disease
(n = 20)
CR 1 (5.0) 1 (5.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
PR 10 (50.0) 5 (25.0) 1 (5.0) 0 (0.0) 3 (15.0) 1 (5.0)
SD 6 (30.0) 0 (0.0) 3 (15.0) 0 (0.0) 3 (15.0) 0 (0.0)
PD 3 (15.0) 0 (0.0) 0 (0.0) 0 (0.0) 2 (10.0) 1 (5.0)
Legend. CR: complete response; PR: partial response; SD: stable disease; PD: progression of disease; IC:
induction chemotherapy; CRT: concurrent chemotherapy and radiotherapy.
*A total of 3 patients were not evaluated after the concurrent therapy phase (1 consent withdrawal; 1
noncompliance; 1 progression of disease and declining performance status for CRT).
Page 35 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.

Table 5. Secondary endpoints.
Resectable
disease (n = 40)
Unresectable
disease (n = 20)
p value***
3 year OS
62.5%
15.0%
0.001
OS median (months) NR 13.0
3 year PFS
47.5%
15.0%
< 0.001
PFS median (months) 23.0 8.0
Early Deaths* 4 (10%) 7 (35%) 0.031
Disease progression 3 (7.5%) 6 (30%)
Surgery related 1 (2.5%) 0
Treatment related (during CRT) 0 1 (5.0%)
No evidence of disease at the end of the planned
treatment†
33 (82.5%) 8 (40.0%) <0.001
Pattern of first failure
23 (57.5%) 17 (85.0%) 0.015
Early disease progression**
3 (7.5%) 6 (30.0%)
Persistent locorregional disease after CRT
2 (5.0%) 5 (25.0%)
Locorregional recurrence††
11 (27.5%) 5 (25.0%)
Locorregional and distant metastases 2 (5.0%) 0
Systemic recurrence 1 (2.5%) 0
Second primary tumor††† 6 (15.0%) 2 (10.0%)
Death without progression 5 (12.5%) 1 (5.0%)
Tracheostomy at last follow-up 11 (27.5%) 4 (20%) 0.326
2 years feeding tube dependence 6 (15%) 3 (15%) 1.000
2 years pneumonia event 5 (12.5%) 1 (5.0%) 0.792
* Deaths within the first year ** Progression within the first 6 months after study enrollment *** Chi-square or Fisher’s exact test.
NR = not reached † Including patients with complete response after the end of treatment and patients submitted to salvage surgery due to
residual disease †† Four patients with locorregional recurrence (25.0%) underwent salvage surgery. ††† The second primary tumors sites were: head and neck carcinoma (n=3), esophageal carcinoma (n=2), gastrointestinal
cancer (n=2) and lung cancer (n=1)
Page 36 of 36
John Wiley & Sons, Inc.
Head & Neck
This article is protected by copyright. All rights reserved.
Related Documents